

Abstract
Introduction Surgical resection of lesions occupying the incisural space is challenging. In a comparative fashion, we aimed to describe the anatomy and surgical approaches to the tentorial incisura and to the rostral brainstem via the intradural subtemporal approach and its infratentorial extensions.
Methods Six fresh human head specimens (12 sides) were prepared for the microscopic dissection of the tentorial incisura using the intradural subtemporal approach and its infratentorial extensions. Endoscope was used to examine the anatomy of the region inadequately exposed with the microscope. Image-guided navigation was used to confirm bony structures visualized around the petrous apex.
Results Standard subtemporal approach provides surgical access to the supratentorial brainstem above the pontomesencephalic sulcus and to the lateral surface of the cerebral peduncle. The linear or triangular tentorial divisions can provide access to the infratentorial space below the pontomesencephalic sulcus. The triangular tentorial flap in comparison with the linear incision obstructs the exposure of anterior incisural space and of the prepontine cistern. Visualization of the brainstem below the trigeminal nerve can be achieved by the anterior petrosectomy.
Conclusion Infratentorial extension of the intradural subtemporal approach is technically demanding due to critical neurovascular structures and a relatively narrow corridor. In-depth anatomical knowledge is essential for the selection of the appropriate operative approach and safe surgical resections of lesions.
Keywords: subtemporal approach, skull base, tentorial incisura, brainstem, anterior petrosectomy
Introduction
The incisural space is located between the brainstem and the free edge of the tentorium. It is divided into three compartments: anterior, middle, and posterior incisural space. The divisions are established based on the external surface landmarks of the brainstem. 1 The roof of the anterior and middle incisural space is formed by the optic chiasm and optic tract, respectively. These spaces contain the basilar artery and its branches and the oculomotor and trochlear nerves. Lesions located within the incisural space can be classified as primarily supra- or infratentorial based on their relationship to the free edge of the tentorium. Pathological lesions can extend across supra- and infratentorial compartments using incisura as the anatomical corridor.
Surgical approach to incisural lesions is challenging requiring a thorough appreciation of the complex neurovascular and skull base anatomy. The location of the cranial nerves and vasculature is further distorted by lesions which increases the complexity of these procedures. With the lesion primarily in the ambient cistern and rostral to the trigeminal nerve, the intradural subtemporal approach is the primary operative route. With further caudal extension of the lesion, operative options include division of the tentorium or performing an anterior petrosectomy. 2 3 4 5 To obviate the excessive temporal retraction needed in a basic temporal craniotomy the extended middle fossa approach with anterior petrosectomy and anterior clinoidectomy can be performed. 6
Although the anatomy of these approaches has been previously described 3 5 7 8 9 10 11 12 13 while approaching lesions like brainstem cavernous malformations, basilar aneurysms, meningiomas, this study aimed to clarify the indications, anatomical and technical nuances pertinent to these approaches in a comparative fashion using anatomical dissections.
Materials and Methods
Six fresh human head specimens (12 sides) were prepared for dissection at the Surgical Neuroanatomy Laboratory of the Department of Neurological Surgery at University of Pittsburgh School of Medicine. The research was approved by the Committee for Oversight of Research Involving the Dead (CORID) at the University of Pittsburgh. The common carotid arteries, vertebral arteries, and internal jugular veins were isolated, cannulated, and injected with red and blue silicone. Specimens were positioned initially with the sagittal suture parallel to the floor and the vertex angled inferiorly to provide maximal visualization along the tentorial surface and tentorial incisura.
Open Microsurgical Visualization
A standard temporal craniotomy down to the level of the middle fossa was performed (level with the posterior root of the zygomatic arch) in all specimens initially. The extensions of the subtemporal approach via use of the linear tentorial incision and triangular tentorial flap as well as combination of the tentorial incision with anterior petrosectomy were examined in stepwise dissections. All observations were recorded from a surgeon's perspective. Special attention was paid to the exposed anatomical structures limiting visualization and working space in each approach.
Endoscopic Visualization
Rod lens endoscopes (Karl Storz, 4 mm, 18 cm, Hopkins II, 0 and 45 degrees) attached to a high-definition camera and a digital video recorder system were used to examine the anatomy of the region that was inadequately exposed or not exposed at all due to the limited view obtained with the microscope.
Results
Standard Subtemporal Approach
Surgical Anatomy in General
A temporal craniotomy with bone drilled flush to the middle cranial fossa is performed to obtain a basal and wide exposure of the tentorial incisura while preserving the vein of the Labbé ( Fig. 1A ). The intradural subtemporal approach provides exposure of the anterior incisural space and the anterior part of the middle incisural space ( Fig. 1B ). Anatomical configuration of the vein of Labbé complex and the parahippocampal gyrus is the main factor limiting the exposure of the superior part of the arachnoid cisterns within the tentorial incisura. The vein of Labbé is defined as the largest vein connecting the superficial sylvian vein with the transverse sinus. It arises in the middle of the sylvian fissure and crosses the temporal lobe to empty into the transverse sinus. 14 The place of crossing is the main factor limiting the exposure. The arachnoid around the vein of Labbé and other temporobasal bridging veins can be dissected free to extend the width of brain retraction ( Fig. 1A ). 15 In rare cases with an anterior location of the vein of Labbé, resection of a small part of the inferior temporal gyrus around the vein of Labbé can avoid excessive stretching of the vein. 16 In cases with long interdural segment of the vein of Labbé, the dural flap enclosing the vein can be dissected free from the skull base to also safely maximize the exposure. 17
Fig. 1.
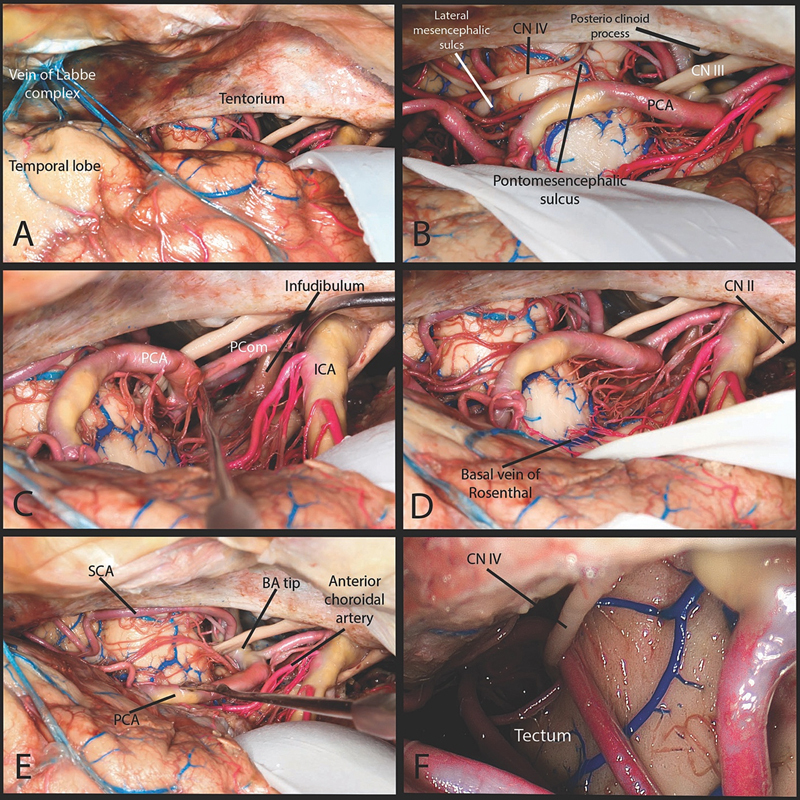
Subtemporal approach. ( A ) A temporal craniotomy was performed. Wide opening of the arachnoid spaces around tentorial incisura exposes underlying structures. The arachnoid dissection around the vein of Labbé complex is performed to maximize safe retraction. ( B ) The anterior and the anterior part of the middle incisural space is exposed. The anterior part of tentorial free edge starting at the anterior and posterior clinoid process was visualized. The free edge of the tentorium was easily followed up to the lateral mesencephalic sulcus. The pontomesencephalic sulcus was identified at the level of the tentorium. ( C ) Within the anterior incisural space the infundibulum from the hypothalamus to the pituitary was visualized. The oculomotor nerve was easily seen within the arachnoid spaces between the posterior cerebral artery (PCA) and superior cerebellar artery (SCA) and where it enters the cavernous sinus within the oculomotor triangle. ( D ) Extensive retraction of the medial temporal lobe was required to visualize the basal vein of Rosenthal. ( E ) The basilar tip, P1, posterior communicating, P2, SCA were exposed in all specimens. The origin and most of the cisternal segment of the anterior choroidal artery could also be exposed through the subtemporal approach. In all specimens the lateral mesencephalic vein was visualized. ( F ) From a subtemporal view the origin of trochlear nerve cannot be seen even with the use of endoscope. BA, basilar artery; CN, cranial nerve; ICA, internal carotid artery; PCA, posterior cerebral artery; Pcom, posterior communicating artery; SCA, superior cerebellar artery.
Visualized Neurovascular Structures
The standard subtemporal approach provides visualization and surgical access to the supratentorial brainstem above the pontomesencephalic sulcus and to the lateral surface of the cerebral peduncle. Visualization of the brainstem below the tentorial incisura with this approach is very limited and to achieve that one has to consider the division of the tentorium via techniques, as detailed later.
Cranial Nerves
The anterior incisural space is crossed by the infundibulum of the pituitary gland on its way from the hypothalamus. The optic nerve, the chiasm, and the optic tract form the superior border of the midbrain and of the anterior and middle incisural spaces. Within the anterior incisural space, the cisternal segment of the oculomotor nerve is easily visualized within its arachnoid layers prior to entrance into the roof of the cavernous sinus ( Fig. 1C ). Visualization of the trochlear nerve always requires some arachnoid dissection within the middle incisural space. The trochlear nerve emerges in the posterior incisural space below and lateral to the inferior colliculus and passes forward parallel to the oculomotor nerve. From a subtemporal approach, visualization of the origin of the trochlear nerve and its initial cisternal segment is not feasible without an endoscope ( Fig. 1F ). This segment of the trochlear nerve is the longest of the five described segments with a mean length of 35 mm. 18 The precise starting point of the tentorial segment is challenging due to arachnoidal adhesions around the nerve. Trochlear nerve usually reaches the free margin of the tentorium at the level of the posterior edge of the cerebral peduncle. From here it passes along the inferior surface of the tentorium within a groove prior to be finally encased within the tentorial dural canal. Precise identification of the entrance of the trochlear nerve into the tentorial tunnel is important from the point of view of performing an appropriately placed tentorial division. Tentorial segment is approximately 9 mm and extends from the entrance of the trochlear nerve into the tentorium up to its entrance into the roof of the cavernous sinus. 19 From an extracranial perspective the start of the tentorial segment can be found approximately 1.5 cm posterior to an imaginary line drawn from external to the internal acoustic meatus. Both meatus lie in the same coronal plane. 20
Vascular Structures
The anterior part of the anterior incisural space involves the supraclinoid internal carotid artery and its posterior branches while the posterior part is occupied by the termination of the basilar artery ( Fig. 1C–E ). Along and above the free edge of the tentorium, the P2 segment of the posterior cerebral artery can be identified. Extensive retraction of the medial temporal lobe is required to visualize the basal vein of Rosenthal ( Fig. 1D ).
Surgical Techniques for Increasing the Caudal Access with the Intradural Subtemporal Approach
Linear Technique for Tentorial Incision 3
This technique was described by MacDonald et al, in 1998. The trochlear nerve is initially identified and dissected free form the arachnoid attachments ( Fig. 2B ). Precise tentorial entry point of the trochlear nerve is identified and the incision starts just posterior to it ( Fig. 2B ). Incision runs posterolaterally in a trajectory parallel to the superior petrosal sinus ( Fig. 2A, B ). The incision can be extended laterally to the confluence of the superior petrosal sinus and the transverse sinus. This approach can be extended by a second incision which is perpendicular to the first one and runs lateral to the trigeminal nerve ( Fig. 2F ). It transects the superior petrosal sinus which is present within the lateral margin of the tentorium and runs along the petrous ridge to join the junction of the transverse and sigmoid sinuses.
Fig. 2.
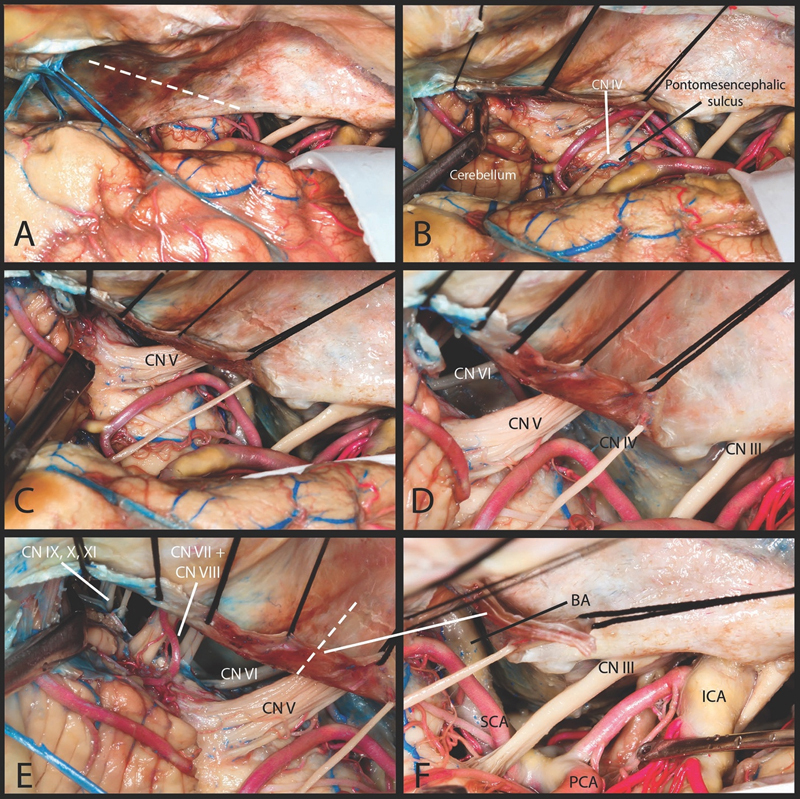
Linear technique. ( A ) The incision starts at the point just posterior to the tentorial entry point of the trochlear nerve. Incision runs parallel to the superior petrosal sinus. ( B ) This incision allows for visualization of the brain stem below the pontomesencephalic sulcus. The lateral surface of the pons can be visualized. Posteriorly the superomedial surface of the cerebellar hemisphere is also visualized. ( C ) The entry zone of the trigeminal nerve as well as its whole length within the prepontine cistern on its way to Meckel's cave is visualized. ( D ) Inferior to the trigeminal nerve the abducens nerve was identified. ( E ) Further lateral extension of the incision allows visualization of the facial, cochlear and vestibular nerves on their way to the internal acoustic meatus. More laterally retraction of cerebellum allows lower cranial nerves to be seen. ( F ) This approach can be extended by second incision which is perpendicular to the first one. CN, cranial nerve; ICA, internal carotid artery; PCA, posterior cerebral artery; SCA, superior cerebellar artery.
Visualized Neuroanatomical Structures: Linear Technique
The linear tentorial incision provides visualization and surgical access to the infratentorial space, especially to the brainstem below the pontomesencephalic sulcus and to the lateral surface of the pons around the trigeminal nerve entry zone ( Fig. 2B, C ). This approach provides excellent approach to the intrinsic ventrolateral pathologies of the brainstem through the epitrigeminal safe entry zone. Visualization of the brainstem below the trigeminal nerve with this approach is very limited and to achieve that one has to consider the anterior petrosectomy.
Cranial Nerves
A standard subtemporal approach without tentorial division does not expose the trigeminal and the abducens nerve. This incision provides the visualization of the trigeminal nerve from its entry zone at the anterolateral aspect of the pons up to the petrous apex where it enters the Meckel's cave ( Fig. 2E ). Retraction of the cerebellar hemisphere can help identify the abducens nerve within the prepontine cistern and below the trigeminal nerve. The abducens nerve emerges from the pontomedullary sulcus and ascends in the prepontine cistern to reach the inferior petrosal sinus where it enters below the petrosphenoidal ligament (Gruber's ligament) ( Fig. 2D ). A further lateral extension of the incision allows the visualization of the facial, cochlear, and vestibular nerves on their way to the internal acoustic meatus. More laterally, posterior retraction of the cerebellar hemisphere exposes the lower cranial nerves ( Fig. 2E ).
Vascular Structures
Tentorial incision and reflection allows for visualization of the superior cerebellar artery and the part of the basilar trunk located below it ( Fig. 2B ). The superior cerebellar artery arises from the basilar artery within the anterior incisural space and courses laterally under the free edge of the tentorium and parallel to the posterior cerebral artery. The segment of the anterior inferior cerebellar artery within the prepontine cistern is also visualized ( Fig. 2D ). The origin of the anterior inferior cerebellar artery from the basilar artery is not seen. In none of the dissected specimens tentorial-meningeal branches of the posterior cerebral artery and superior cerebellar arteries could be seen. These branches have been reported to be identified in up to 25% of all studied specimens and can cause bleeding with tentorial reflection. 21 22
Triangular Technique for Tentorial Division 23
This incision starts from the free edge of the tentorium at the level of posterior surface of the cerebral peduncle which is located posterior to the tentorial entry point of fourth nerve ( Fig. 3A ). The end point of the incision is located at the petrous ridge and superior petrosal sinus. The incision line over the tentorium should create an angle of approximately 45 degrees in relation to the petrous ridge ( Fig. 3B ). This creates a triangular tentorial flap which is everted over the superior petrosal sinus ( Fig. 3C ). A blunt hook is used to elevate the tentorium to protect infratentorial structures and to identify the petrous ridge and the superior petrosal sinus ( Fig. 3B ).
Fig. 3.
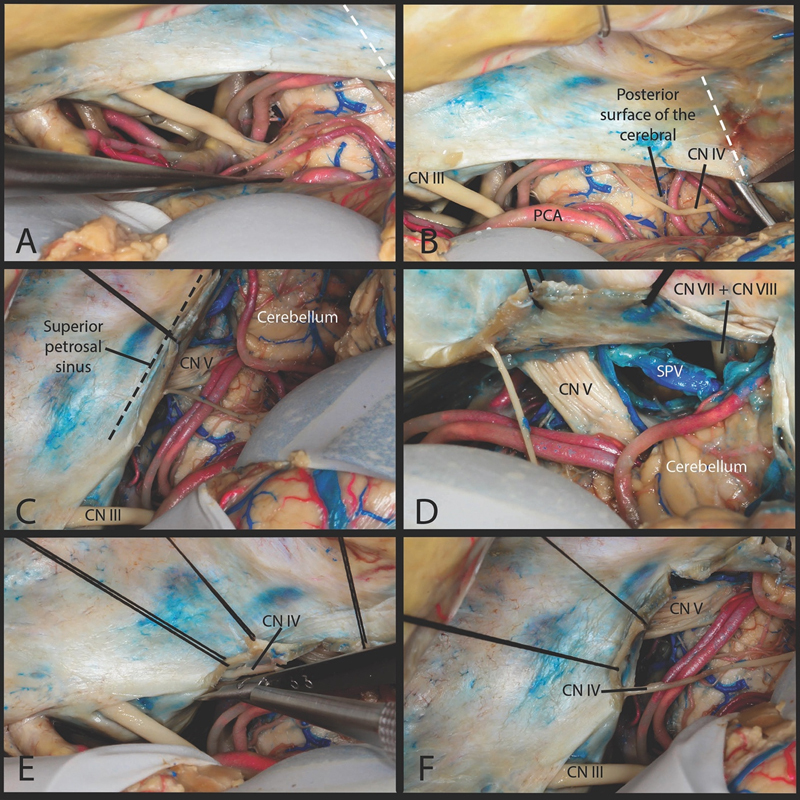
Triangular technique. ( A ) The subtemporal approach. ( B ) The incision starts from the edge of the tentorium at the level of posterior surface of the cerebral peduncle. The end point of the incision is located at the petrous ridge and superior petrosal sinus. ( C ) This creates triangular tentorial flap which is everted over the superior petrosal sinus. This part of the tentorium everted around the superior petrosal sinus obstructed the view of the prepontine cistern. ( D ) Looking laterally only a small course of the facial/cochlear nerve was visualized within the cerebellopontine angle. ( E ) To achieve maximal anterolateral reflection of the tentorial flap we dissected the trochlear nerve fully from its tentorial canal as far as its entrance into the cavernous sinus. ( F ) View after releasing the trochlear nerve from its tentorial canal. CN, cranial nerve; PCA, posterior cerebral artery; SPV, superior petrosal vein.
Triangular versus Linear Technique for Tentorial Division
In comparison with the linear incision technique, the triangular tentorial flap (everted over the superior petrosal sinus) obstructs the view of anterior incisural space and of the prepontine cistern ( Fig. 3C ). Further only a short proximal segment of the facial and vestibulocochlear nerves is visualized ( Fig. 3D ). The lower cranial nerves are not seen with this approach. With this technique to achieve maximal anterolateral reflection of the tentorial flap, it is useful to dissect the trochlear nerve free from its tentorial canal stopping proximal to its entrance into the cavernous sinus. This can be achieved by opening the medial wall and gentle mobilization of the nerve from the tentorial canal ( Fig. 3E ). 2 A working corridor is therefore, created above and below the trochlear nerve ( Fig. 3F ). The tentorial triangular flap can also be resected by adding a cut parallel to the superior petrosal sinus.
Anterior Petrosectomy 4 5
Visualization of the brainstem below the trigeminal nerve with a more ventral perspective can be achieved by the anterior petrosectomy. Most commonly, the extradural anterior petrosectomy is performed. It starts with peeling of the middle fossa dura in posterior to anterior direction to expose the petrous part of the temporal bone and Kawase's triangle. Anatomical landmarks like greater superficial petrosal nerve (GSPN, anterior border), arcuate eminence (lateral border), petrous ridge (posterior border), and lateral border of the mandibular nerve (medial border) are clearly identified before drilling.
In case of inadequate exposure of the infratentorial structures after tentorial incision, intradural subtemporal approach can be extended by intradural modification of the standard extradural anterior petrosectomy. The tentorial incision has to be extended through the superior petrosal sinus and is directed lateral to the mandibular nerve ( Fig. 4B ). Due to lack of anatomical landmarks from the intradural perspective, the location of the mandibular nerve is checked with a dissector. The use of image guidance with this procedure is very helpful. The petrous apex is drilled lateral to the mandibular nerve ( Fig. 4C ). With a complete anterior petrosectomy, the inferior petrosal sinus is identified at the inferior border ( Fig. 4D ). The dura over the posterior fossa is cut and supratentorial and infratentorial exposure is achieved ( Fig. 4E, F ).
Fig. 4.
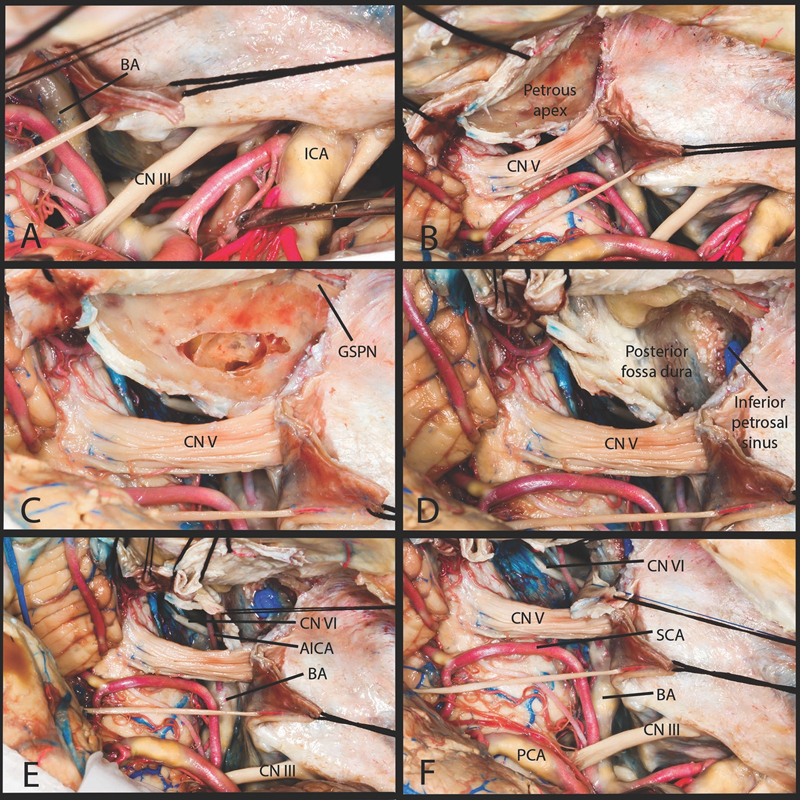
Intradural anterior petrosectomy. ( A ) The tentorium over the superior petrosal sinus has to be cut. ( B ) The dura over the petrous apex is stripped away. ( C ) The petrous apex is drilled lateral to the mandibular nerve. ( D ) The inferior border of apical petrosectomy is marked by the inferior petrosal sinus. ( E ) Anterior petrosectomy provides a more anterior and inferior exposure of the infratentorial structures. ( F ) The dura over the posterior fossa is cut to create a single opening. AICA, anterior inferior cerebellar artery; BA, basilar artery; CN, cranial nerve; ICA, internal carotid artery; PCA, posterior cerebral artery; SCA, superior cerebellar artery.
Anterior Petrosectomy versus Tentorial Division in the Standard Subtemporal Approach
Extension of the approach via anterior petrosectomy provides more ventral and caudal exposure of the infratentorial brainstem. In particular, it provides a working corridor between the trigeminal and the vestibulocochlear nerve ( Fig. 4E, F ). Additionally the whole course of the abducens nerve from the pontomedullary sulcus up to the Gruber's ligament can be appreciated ( Fig. 4F ). Visualized vascular structures include the basilar trunk and the anterior inferior cerebellar artery origin ( Fig. 4F ).
Comparison of Intradural with Extradural Anterior Petrosectomy 5 24 25
With extradural anterior petrosectomy, the injury to the temporal lobe, vein of Labbé, and temporal bridging veins is minimal. On the other hand, dissection of the dura of the middle fossa may cause traction on the GSPN with the risk of facial nerve palsy. Extradural petrosectomy is more difficult to perform in a tailored fashion as the whole bony exposure has to be performed before the dural opening. The main advantage of the intradural approach is a chance to perform a tailored approach for the size of the lesion. The main disadvantages are related to the lack of bony anatomical landmarks and spread of bone dust from drilling in the intradural space in the posterior fossa.
Discussion
Subtemporal Approach and Preoperative Considerations
The location of the lesion within the incisural space relative to the tentorium dictates the choice of the surgical approach. If the preoperative coronal MR images demonstrate a lesion located within the anterior and middle incisural spaces (primarily supratentorial), it can be approached via the intradural subtemporal approach. Injury to the vein of Labbé and other temporobasal bridging veins may lead to morbidity by causing venous infarction. The pattern of superficial venous anatomy can be studied in the preoperative MR venography in anticipation for surgery.
Anatomical Consideration Surrounding the Infratentorial Extension
To protect the trochlear nerve, the tentorial incision is located posterior to its tentorial entry point. The trochlear nerve has the longest intracranial course and also the smallest diameter among all intracranial nerves making it vulnerable to intraoperative injury. Identification and protection of the infratentorial structures and superior petrosal sinus during tentorial incision can be achieved with the use of a blunt hook which is used to elevate the tentorium. Intraoperative superior petrosal vein (SPV)occlusion usually does not cause venous infraction and edema but preservation of the large caliber veins should be attempted whenever possible to decrease operative morbidity. 26 Tanriover et al, proposed a classification of the SPV in relation to the Meckel's Cave and the internal acoustic meatus. 27 In the type 3 (the SPV empties medially into the Meckel's cave) and in type 2 (drainage located between the Meckel's cave medially and the internal acoustic canal laterally), the exposure of the infratentorial structures may require the sacrifice of the vein. Before sacrificing the superior petrosal sinus, preoperative analysis of the venography should be done to exclude rare cases of basal vein of Rosenthal draining into the petrosal vein and then into the superior petrosal sinus. 28
With respect to the blood supply of the tentorium, the medial tentorial artery (artery of Bernasconi-Cassinari) arising from meningohypophyseal trunk was the most constant artery. It is often seen on imaging in pathological lesions arising around the tentorial incisura. 29 Both posterior cerebral and superior cerebellar arteries may also supply medial areas of the tentorium with branches from these arteries being found in about one quarter of all patients. 21 22 The tentorial branch of the posterior cerebral artery, artery of Davidoff and Schechter, runs under the free edge of the tentorium. 22 The branch from the superior cerebellar artery, artery of Wollschlaeger and Wollschlaeger, arises from the lateral pontomesencephalic segment with a small size of 1 mm or less making its cadaveric dissection difficult. 21 These branches should be kept in mind as troublesome bleeding can be encountered during eversion of the tentorial flap. These branches can also be potentially avulsed from the parent artery.
Extensions of the Subtemporal Approach
When the exposure of the upper incisural space is limited, the subtemporal approach can be combined with the transtemporal transchoroidal approach. 30
The exposure of the infratentorial part of the lesion is limited by the tentorium. The optimal incision over the tentorium should provide wide exposure of the posterior fossa structures with minimal risk of injury to the neurovascular structures. Simple retraction of the free edge of the tentorium with the spatula or with a stich may in some cases be sufficient. This can be further extended by short (10 mm) cut running perpendicular to the tentorial free edge. 31 As described above, two main techniques of tentorial incision are used. To achieve a more ventral and caudal exposure of the brainstem, each tentorial incision technique can be combined with the anterior petrosectomy. Intradural anterior petrosectomy compared with the extradural petrosectomy can provide an opportunity to perform a tailored petrosectomy to address the lesion.
Indications for These Approaches
The subtemporal approach provides the shortest and the most direct access to the posterior cerebral artery. This approach, often without infratentorial extension can be applied to treat the posterior cerebral artery aneurysms up to the P3 segment of the artery. 9 Meningiomas located in the middle incisural space and anterolateral to the brainstem are commonly approached by some authors with the subtemporal approach 10 32 especially when tumors are located closer to the midline above and medial to internal acoustic canal. 8 33 Petroclival meningiomas can also be resected with addition of the apical petrosectomy. 5 25
Subtemporal transtentorial approach provides excellent visualization of the trigeminal nerve entry zone including the epitrigeminal safe entry zone to the ventrolateral pons. 13 Recently Ogiwara et al, found it useful in cases of recurrent trigeminal neuralgia who were operated on with the standard retrosigmoid approach or when the offending vessel was distal to the root entry zone or on its anterolateral side. 11 In trigeminal schwannomas extending from the middle fossa through the porus trigeminus into the posterior fossa, the tumor medial to the internal acoustic canal can also be approached. 34
With respect to accessing the retroinfudibular/retrochiasmatic region, the location of the parasellar tumor in relation to the optic chiasm and to the pituitary stalk has to be taken into consideration during selection of the surgical approach. Retroinfudibular/retrochiasmatic craniopharyngiomas often are found to extend toward the posterior fossa. Standard microscopic anterolateral approaches have been used but often visualization of retrochiasmatic space requires surgeon to work between neurovascular structures in a deep and narrow operating field. The subtemporal approach provides access to the retroinfudibular/retrochiasmatic tumors using corridors between the oculomotor nerve and the internal carotid artery and also between the posterior cerebral and the posterior communicating artery. 35 Alternatively endoscopic endonasal transsphenoidal approach can also be used to reach the tumor in the retrochiasmatic/retoroinfudibular space with the transposition of the pituitary gland and posterior clinoidectomy. 36
The tentorial incision also reveals the superior surface of the cerebellum which provides direct approach with short working distance to the tumors located within the anteromedial and superior part of the cerebellar hemisphere. 37
Conclusion
The tentorial incisura is a complex area containing many critical neurovascular structures. Infratentorial extension of the intradural subtemporal approach is technically demanding due to those structures and the long and narrow corridor. In-depth anatomical knowledge is essential for safe and successful operation in this area with additional appreciation of distortion of the neurovascular structures with pathological lesions in the incisural space.
Footnotes
Conflict of Interest None declared.
References
- 1.Ono M, Ono M, Rhoton A L, Jr, Barry M. Microsurgical anatomy of the region of the tentorial incisura. J Neurosurg. 1984;60(02):365–399. doi: 10.3171/jns.1984.60.2.0365. [DOI] [PubMed] [Google Scholar]
- 2.McLaughlin N, Martin N A.Extended subtemporal transtentorial approach to the anterior incisural space and upper clival region: experience with posterior circulation aneurysms Neurosurgery 2014100115–23., discussion 23–24 [DOI] [PubMed] [Google Scholar]
- 3.MacDonald J D, Antonelli P, Day A L. The anterior subtemporal, medial transpetrosal approach to the upper basilar artery and ponto-mesencephalic junction. Neurosurgery. 1998;43(01):84–89. doi: 10.1097/00006123-199807000-00054. [DOI] [PubMed] [Google Scholar]
- 4.Kawase T, Shiobara R, Toya S.Anterior transpetrosal-transtentorial approach for sphenopetroclival meningiomas: surgical method and results in 10 patients Neurosurgery 19912806869–875., discussion 875–876 [PubMed] [Google Scholar]
- 5.Steiger H J, Hänggi D, Stummer W, Winkler P A. Custom-tailored transdural anterior transpetrosal approach to ventral pons and retroclival regions. J Neurosurg. 2006;104(01):38–46. doi: 10.3171/jns.2006.104.1.38. [DOI] [PubMed] [Google Scholar]
- 6.Fernandez-Miranda J C. Extended Middle fossa approach with anterior petrosectomy and anterior clinoidectomy for resection of spheno-cavernous-tentorial meningioma: the Hakuba-Kawase-Dolenc approach: 3-dimensional operative video. Oper Neurosurg (Hagerstown) 2017;13(02):281. doi: 10.1093/ons/opw019. [DOI] [PubMed] [Google Scholar]
- 7.Drake C G. Bleeding aneurysms of the basilar artery. Direct surgical management in four cases. J Neurosurg. 1961;18:230–238. doi: 10.3171/jns.1961.18.2.0230. [DOI] [PubMed] [Google Scholar]
- 8.Goel A. Extended lateral subtemporal approach for petroclival meningiomas: report of experience with 24 cases. Br J Neurosurg. 1999;13(03):270–275. doi: 10.1080/02688699943673. [DOI] [PubMed] [Google Scholar]
- 9.Goehre F, Lehecka M, Jahromi B R. Subtemporal approach to posterior cerebral artery aneurysms. World Neurosurg. 2015;83(05):842–851. doi: 10.1016/j.wneu.2015.01.042. [DOI] [PubMed] [Google Scholar]
- 10.Hashemi M, Schick U, Hassler W, Hefti M. Tentorial meningiomas with special aspect to the tentorial fold: management, surgical technique, and outcome. Acta Neurochir (Wien) 2010;152(05):827–834. doi: 10.1007/s00701-009-0591-z. [DOI] [PubMed] [Google Scholar]
- 11.Ogiwara T, Goto T, Kusano Y. Subtemporal transtentorial approach for recurrent trigeminal neuralgia after microvascular decompression via the lateral suboccipital approach: case report. J Neurosurg. 2015;122(06):1429–1432. doi: 10.3171/2014.10.JNS132643. [DOI] [PubMed] [Google Scholar]
- 12.Steňo J, Bízik I, Steňová J, Timárová G.Subtemporal transtentorial resection of cavernous malformations involving the pyramidal tract in the upper pons and mesencephalon Acta Neurochir (Wien) 2011153101955–1962., discussion 1962 [DOI] [PubMed] [Google Scholar]
- 13.Zenonos G A, Fernandes-Cabral D, Nunez M, Lieber S, Fernandez-Miranda J C, Friedlander R M. The epitrigeminal approach to the brainstem. J Neurosurg. 2018;128(05):1512–1521. doi: 10.3171/2016.12.JNS162561. [DOI] [PubMed] [Google Scholar]
- 14.Rhoton A L., Jr The cerebral veins. Neurosurgery. 2002;51 04:S159–S205. [PubMed] [Google Scholar]
- 15.Sugita K, Kobayashi S, Yokoo A. Preservation of large bridging veins during brain retraction. Technical note. J Neurosurg. 1982;57(06):856–858. doi: 10.3171/jns.1982.57.6.0856. [DOI] [PubMed] [Google Scholar]
- 16.Heros R C. Brain resection for exposure of deep extracerebral and paraventricular lesions. Surg Neurol. 1990;34(03):188–195. doi: 10.1016/0090-3019(90)90073-x. [DOI] [PubMed] [Google Scholar]
- 17.Kyoshima K, Oikawa S, Kobayashi S. Preservation of large bridging veins of the cranial base: technical note. Neurosurgery. 2001;48(02):447–449. doi: 10.1097/00006123-200102000-00047. [DOI] [PubMed] [Google Scholar]
- 18.Joo W, Rhoton A L., Jr Microsurgical anatomy of the trochlear nerve. Clin Anat. 2015;28(07):857–864. doi: 10.1002/ca.22602. [DOI] [PubMed] [Google Scholar]
- 19.Iaconetta G, de Notaris M, Benet A.The trochlear nerve: microanatomic and endoscopic study Neurosurg Rev 20133602227–237., discussion 237–238 [DOI] [PubMed] [Google Scholar]
- 20.Tubbs R S, Oakes W J. Relationships of the cisternal segment of the trochlear nerve. J Neurosurg. 1998;89(06):1015–1019. doi: 10.3171/jns.1998.89.6.1015. [DOI] [PubMed] [Google Scholar]
- 21.Umeoka K, Takusakawa Y, Kominami S, Kobayashi S, Morita A. The meningeal branches of the superior cerebellar artery: a surgical observation study. J Neurosurg. 2016;124(01):244–247. doi: 10.3171/2014.12.JNS141190. [DOI] [PubMed] [Google Scholar]
- 22.Griessenauer C J, Loukas M, Scott J A, Tubbs R S, Cohen-Gadol A A. The artery of Davidoff and Schechter: an anatomical study with neurosurgical case correlates. Br J Neurosurg. 2013;27(06):815–818. doi: 10.3109/02688697.2013.798856. [DOI] [PubMed] [Google Scholar]
- 23.Goel A. Tentorial dural flap for transtentorial surgery. Br J Neurosurg. 1995;9(06):785–786. doi: 10.1080/02688699550040765. [DOI] [PubMed] [Google Scholar]
- 24.Gupta S K, Salunke P. Intradural anterior petrosectomy for petroclival meningiomas: a new surgical technique and results in 5 patients: technical note. J Neurosurg. 2012;117(06):1007–1012. doi: 10.3171/2012.9.JNS12429. [DOI] [PubMed] [Google Scholar]
- 25.Ichimura S, Hori S, Hecht N, Czabanka M, Vajkoczy P. Intradural anterior transpetrosal approach. Neurosurg Rev. 2016;39(04):625–631. doi: 10.1007/s10143-016-0711-1. [DOI] [PubMed] [Google Scholar]
- 26.Koerbel A, Gharabaghi A, Safavi-Abbasi S. Venous complications following petrosal vein sectioning in surgery of petrous apex meningiomas. Eur J Surg Oncol. 2009;35(07):773–779. doi: 10.1016/j.ejso.2008.02.015. [DOI] [PubMed] [Google Scholar]
- 27.Tanriover N, Abe H, Rhoton A L, Jr, Kawashima M, Sanus G Z, Akar Z. Microsurgical anatomy of the superior petrosal venous complex: new classifications and implications for subtemporal transtentorial and retrosigmoid suprameatal approaches. J Neurosurg. 2007;106(06):1041–1050. doi: 10.3171/jns.2007.106.6.1041. [DOI] [PubMed] [Google Scholar]
- 28.Fernández-Miranda J C, de Oliveira E, Rubino P A, Wen H T, Rhoton A L., JrMicrovascular anatomy of the medial temporal region: part 1: its application to arteriovenous malformation surgeryNeurosurgery 2010;67(suppl operative 3):ons237–ons276, discussion ons276 [DOI] [PubMed]
- 29.Tubbs R S, Nguyen H S, Shoja M M, Benninger B, Loukas M, Cohen-Gadol A A. The medial tentorial artery of Bernasconi-Cassinari: a comprehensive review of its anatomy and neurosurgical importance. Acta Neurochir (Wien) 2011;153(12):2485–2490. doi: 10.1007/s00701-011-1195-y. [DOI] [PubMed] [Google Scholar]
- 30.Ulm A J, Tanriover N, Kawashima M, Campero A, Bova F J, Rhoton A., JrMicrosurgical approaches to the perimesencephalic cisterns and related segments of the posterior cerebral artery: comparison using a novel application of image guidance Neurosurgery 200454061313–1327., discussion 1327–1328 [DOI] [PubMed] [Google Scholar]
- 31.Hernesniemi J, Ishii K, Karatas A.Surgical technique to retract the tentorial edge during subtemporal approach: technical note Neurosurgery 20055704E408, discussion E408 [DOI] [PubMed] [Google Scholar]
- 32.Nanda A, Patra D P, Savardekar A. Tentorial meningiomas: reappraisal of surgical approaches and their outcomes. World Neurosurg. 2018;110:e177–e196. doi: 10.1016/j.wneu.2017.10.115. [DOI] [PubMed] [Google Scholar]
- 33.Li D, Tang J, Ren C, Wu Z, Zhang L W, Zhang J T.Surgical management of medium and large petroclival meningiomas: a single institution's experience of 199 cases with long-term follow-up Acta Neurochir (Wien) 201615803409–425., discussion 425 [DOI] [PubMed] [Google Scholar]
- 34.Taha J M, Tew J M, Jr, van Loveren H R, Keller J T, el-Kalliny M. Comparison of conventional and skull base surgical approaches for the excision of trigeminal neurinomas. J Neurosurg. 1995;82(05):719–725. doi: 10.3171/jns.1995.82.5.0719. [DOI] [PubMed] [Google Scholar]
- 35.Wong R H, De Los Reyes K, Alikhani P. The subtemporal approach to retroinfundibular craniopharyngiomas: a new look at an old approach. Oper Neurosurg (Hagerstown) 2015;11(04):495–503. doi: 10.1227/NEU.0000000000000972. [DOI] [PubMed] [Google Scholar]
- 36.Fernandez-Miranda J C, Gardner P A, Snyderman C H. Craniopharyngioma: a pathologic, clinical, and surgical review. Head Neck. 2012;34(07):1036–1044. doi: 10.1002/hed.21771. [DOI] [PubMed] [Google Scholar]
- 37.Ammerman J M, Lonser R R, Oldfield E H. Posterior subtemporal transtentorial approach to intraparenchymal lesions of the anteromedial region of the superior cerebellum. J Neurosurg. 2005;103(05):783–788. doi: 10.3171/jns.2005.103.5.0783. [DOI] [PubMed] [Google Scholar]