

Minor rectal neuroendocrine tumors (NETs) can be resected endoscopically using various procedures. Nevertheless, there remains controversy with regard to which of the possible endoscopic approaches is the most effective 1 2 3 . As revealed by relevant reports, endoscopic submucosal dissection (ESD) is an effective and safe technique for the treatment of rectal NETs; however, ESD requires physicians to have more surgical skills and operative times are longer than for other endoscopic resection techniques 2 . A pretraction-assisted ESD technique for small rectal NETs was therefore created to simplify the process and facilitate the operation ( Video 1 ).
Video 1 Pretraction-assisted endoscopic submucosal dissection for a rectal neuroendocrine tumor.
A NET of approximately 8 mm in size was found in the rectum about 5 cm from the anus. Endoscopic ultrasonography (EUS) suggested that the lesion was confined to the submucosa. In a pretraction-assisted ESD method, a DualKnife was used to mark the area around the lesion with a margin of approximately 5 mm. Submucosal injection was performed sufficiently around the lesion. Prior to submucosal dissection, a metal clip was used to secure a line to the marked point on the anal side of the lesion ( Fig. 1 a ). The line was then dragged to the opposite wall from the lesion and secured with another metal clip ( Fig. 1 b ). The line was subsequently pulled from outside the body to maintain the required tension. With the use of pretraction, the submucosal area could be thoroughly exposed by cutting through the mucosal layer ( Fig. 1 c ). During dissection, the external traction was adjusted as required to ensure adequate exposure of the submucosa and, simultaneously, dissection was be performed alongside the upper part of the muscle layer ( Fig. 1 d ).
Fig. 1.
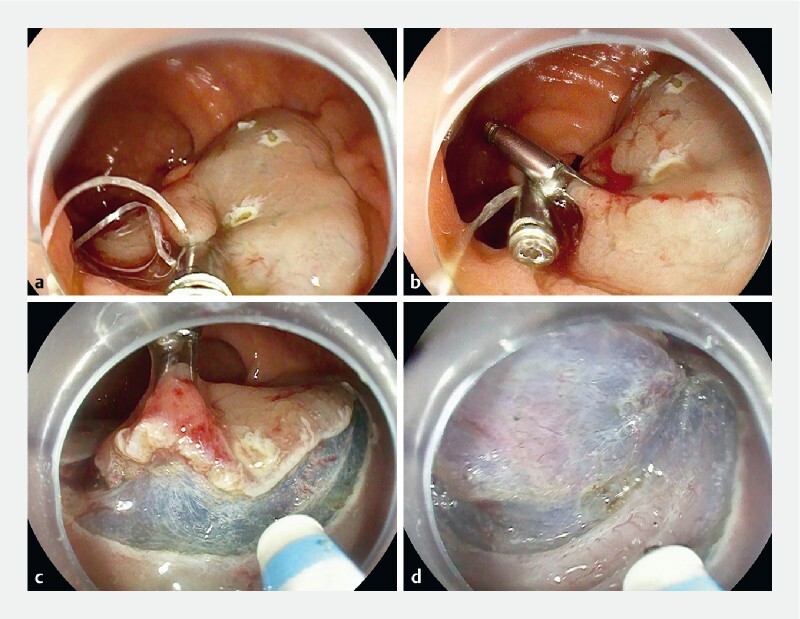
Endoscopic images showing: a the first clip with the line anchored at the anal side of the lesion; b a second clip attached to the line on the opposite side of the bowel wall, creating preliminary traction; c good exposure of the submucosa, which is easily achieved with sufficient traction; d dissection being performed along the uppermost portion of the muscle layer to guarantee negative margins.
This pretraction method allows the lesion to be dissected speedily, meaning it is not only unnecessary to perform additional submucosal injections, but also that en bloc resection without any complications is possible.
Endoscopy_UCTN_Code_TTT_1AQ_2AC
Footnotes
Competing interests The authors declare that they have no conflict of interest.
Endoscopy E-Videos : https://eref.thieme.de/e-videos .
Endoscopy E-Videos is an open access online section, reporting on interesting cases and new techniques in gastroenterological endoscopy. All papers include a high quality video and all contributions are freely accessible online. Processing charges apply (currently EUR 375), discounts and wavers acc. to HINARI are available. This section has its own submission website at https://mc.manuscriptcentral.com/e-videos
References
- 1.Sun P, Zheng T, Hu C et al. Comparison of endoscopic therapies for rectal neuroendocrine tumors: endoscopic submucosal dissection with myectomy versus endoscopic submucosal dissection. Surg Endosc. 2021;35:6374–6378. doi: 10.1007/s00464-021-08622-8. [DOI] [PubMed] [Google Scholar]
- 2.Toriyama K, Yamamura T, Nakamura M et al. An evaluation of resectability among endoscopic treatment methods for rectal neuroendocrine tumors <10 mm. Arab J Gastroenterol. 2021;22:104–110. doi: 10.1016/j.ajg.2021.05.007. [DOI] [PubMed] [Google Scholar]
- 3.Zhang J, Liu M, Li H et al. Comparison of endoscopic therapies for rectal carcinoid tumors: endoscopic mucosal resection with circumferential incision versus endoscopic submucosal dissection. Clin Res Hepatol Gastroenterol. 2018;42:24–30. doi: 10.1016/j.clinre.2017.06.007. [DOI] [PubMed] [Google Scholar]