

Abstract
What is already known about this topic?
Environmental and occupational lead exposure has generally declined in the past two decades. However, there is no large-scale monitoring of blood lead levels (BLLs) in the Chinese general population.
What is added by this report?
This nationally representative study showed declines of BLLs in all ages of participants; for children aged 3–5 years, down from 78.1 μg/L to 16.9 μg/L, corresponding to 78.4% decrease in the past two decades (2000–2018).
What are the implications for public health practice?
Recommendations for elevated BLLs on screening children at high risk now need to be revisited and updated from 100 μg/L to 50 μg/L in guidelines to conform with the substantial declines in China.
Keywords: blood lead levels, reference value, China National Human Biomonitoring
High exposure to lead is associated with numerous adverse health outcomes, particularly impairment of neural development in children (1). Large-scale biomonitoring is necessary to quantify risk assessments in public health. The United States carries out the National Health and Nutrition Examination Surveys (NHANES) to monitor changes in environmental chemicals. Monitoring of blood lead levels (BLLs) in children led to action on the reduction of exposure from, for example, leaded gasoline and leaded paint (2). Following the recent BLL decline, the US CDC updated the blood lead reference value (BLRV) to 35 µg/L based on the latest two rounds of the NHANES and reported in Morbidity and Mortality Weekly Report (3). In China, the latest national recommendations for BLLs in children, issued in 2006, established a BLRV of 100 μg/L for hyperleademia (4). Recent studies have indicated that BLLs in Chinese children have been declining over the past two decades (5). However, China does not have a suitable definition of elevated BLLs. To this end, the China CDC initiated the China National Human Biomonitoring (CNHBM) in 2017.
The distribution and temporal trends of BLLs during the past two decades in the Chinese population were from the data of a nationally representative study and two previous regional-scale surveys. The 2017/18 survey based on CNHBM, a nationally representative study for tracing the dynamic change of environmental chemicals, included 21,746 samples recruited from 152 counties in 31 provincial-level administrative divisions (PLADs) of China (Supplementary Figure S1, available in http://weekly.chinacdc.cn). Due to 45 participants without available BLLs information, 21,701 participants aged 3–79 years were included in this study. The CNHBM used an advanced computer-assisted personal interviewing (CAPI) online system to conduct a household interview and Epidata (version 3.2, EpiData Association, Odense, Denmark) for data entry and management, collecting the data of age, gender, residence, districts, and so on. Details of covariate definition are shown in Supplementary Methods (available in http://weekly.chinacdc.cn). Details about the study design have been previously reported (6). Approval was obtained from the Ethics Committee of the National Institute of Environmental Health, Chinese Center for Disease Control and Prevention (No.201701). All participants signed written informed consent. The 2000 survey included 6,085 children aged 3–5 years randomly selected from 19 cities (7). The 2009/10 survey included 11,090 participants of the general population aged 6–59 years (8). In 2000, 2009/10, and 2017/18 surveys, venous blood specimens were collected in the morning after an overnight fast for all persons in the local community health centers, frozen, and shipped to China CDC (Beijing) for analysis. Inductively coupled plasma mass spectrometry (ICP-MS) was used to measure lead concentrations in blood samples in the three surveys (Supplementary Methods). The lead measurement in the 2017/18 survey was finished in 2019. The BLLs in each of the three surveys were calibrated using standards prepared from lead nitrate Standard Reference Material obtained from the National Institute of Standards and Technology.
Characteristics of participants in the 2017/18 survey were stratified by quartiles of BLLs. Geometric means and distributions of BLLs and the number of participants with elevated BLLs were calculated by incorporating the weights for the entire Chinese population. The spatial distribution of BLLs in the Chinese population was mapped. The 97.5th percentile of the BLLs in participants of all age groups from CNHBM was chosen as the BLRV (3). Description of the method adopted to estimate the disease burden for children aged 3–5 years and participants aged 6–59 years is presented in Supplementary Methods, respectively. Analyses were done with SAS (version 9.4, SAS Institute Inc., Cary, USA), R (version 3.4.1, R Development Core Team, Vienna, Austria), and ArcGIS (version 3.6.1, Environmental Systems Research Institute Inc., California, USA). All P values were two-sided, and a P value of less than 0.05 was considered significant.
The geometric mean of BLLs of all 21,701 participants aged 3–79 years in the 2017/18 survey was 20.66 μg/L, and the proportion of BLLs over 50 µg/L was 6.0% (Table 1). The spatial distribution of BLLs in the Chinese population in 2017/18 is shown in Figure 1. During the past two decades (2000–2018), the BLLs of children aged 3–5 years were down from 78.1 μg/L to 16.9 μg/L, dropping by 78.4%. For participants aged 6–59 years, the BLLs were 20.41 μg/L in 2017/18, down from 36.9 μg/L in 2009/10, dropping by 44.7%. The lead exposure-related burden of disease measured in DALYs showed clear downward trends over time (Table 2). Based on the BLLs in 2017/18, the BLRV for participants aged 3–5 years was updated to 50 μg/L considering the 97.5th percentile of the BLLs in this population (Table 1). Characteristics of participants in surveys are shown in Supplementary Tables S1–S2 (available in http://weekly.chinacdc.cn). Supplementary Figure S2 (available in http://weekly.chinacdc.cn) compares the proportion of BLLs over 50 μg/L in participants from 2000 to 2018. More details of disease burden are shown in Supplementary Tables S3–S4 (available in http://weekly.chinacdc.cn).
Table 1. Blood lead levels (BLLs) in different age, gender, residence and districts among Chinese population in 2017/18.
| Sub group | <LOD* (%) |
Geometric mean
(95% CI), μg/L |
Median
(95% CI), μg/L |
P90
(95% CI), μg/L |
P95
(95% CI), μg/L |
P97.5
(95% CI), μg/L |
Participants with BLLs ≥35 μg/L, n (%), million† | Participants with BLLs ≥50 μg/L, n (%), million§ | Participants with BLLs ≥100 μg/L, n (%), million¶ |
| Abbreviation: LOD=limit of detection. * The LOD of blood lead was 0.035 μg/L; <LOD (%) was the proportion below LOD. † Participants with BLLs ≥35 μg/L, n (%) were calculated incorporating the sample weights. § Participants with BLLs ≥50 μg/L, n (%) were calculated incorporating the sample weights. ¶ Participants with BLLs ≥100 μg/L, n (%) were calculated incorporating the sample weights. | |||||||||
| Total | 0.27 | 20.66 (19.90–21.46) |
20.72 (20.03–21.42) |
42.82 (40.73–44.91) |
52.72 (50.03–55.41) |
65.80 (60.93–70.67) |
222.4 (16.7) | 79.9 (6.0) | 9.0 (0.7) |
| Age (years) | |||||||||
| 3–5 | 0.36 | 16.87 (16.06–17.72) |
17.01 (16.33–17.68) |
33.87 (31.87–35.87) |
41.67 (38.32–45.02) |
50.95 (44.86–57.03) |
11.8 (8.7) | 3.7 (2.7) | 0.7 (0.5) |
| 6–11 | 0.24 | 16.84 (16.12–17.59) |
17.01 (16.34–17.67) |
31.27 (29.49–33.04) |
38.65 (35.91–41.40) |
45.87 (42.46–49.29) |
11.6 (7.1) | 3.0 (1.8) | 0.1 (0.1) |
| 12–18 | 0.36 | 15.21 (14.53–15.93) |
15.27 (14.71–15.83) |
29.30 (27.18–31.42) |
37.66 (33.73–41.59) |
46.28 (38.59–53.97) |
9.7 (6.1) | 3.2 (2.0) | 0.6 (0.3) |
| 19–39 | 0.36 | 21.32 (20.33–22.36) |
21.65 (20.50–22.79) |
41.79 (39.12–44.45) |
51.15 (47.70–54.61) |
62.64 (55.65–69.63) |
47.9 (16.2) | 15.2 (5.2) | 1.2 (0.4) |
| 40–59 | 0.30 | 24.78 (23.70–25.91) |
25.02 (23.90–26.14) |
49.47 (47.09–51.85) |
58.68 (54.54–62.81) |
71.33 (64.98–77.68) |
84.6 (25.2) | 32.2 (9.6) | 3.3 (1.0) |
| 60–79 | 0.06 | 24.40 (23.32–25.52) |
23.70 (22.75–24.64) |
49.37 (45.49–53.26) |
63.92 (57.30–70.54) |
85.72 (78.31–93.14) |
56.8 (23.8) | 22.6 (9.5) | 3.1 (1.3) |
| Sex | |||||||||
| Men | 0.24 | 24.41 (23.37–25.50) |
24.43 (23.39–25.48) |
47.34 (44.72–49.96) |
57.34 (53.26–61.41) |
71.38 (65.29–77.47) |
154.1 (23.3) | 54.5 (3.8) | 5.2 (0.8) |
| Women | 0.28 | 17.51 (16.86–18.18) |
17.39 (16.90–17.89) |
35.37 (33.31–37.44) |
45.54 (42.46–48.62) |
57.44 (52.24–62.64) |
68.3 (10.2) | 25.4 (8.2) | 3.8 (0.6) |
| Residence | |||||||||
| Urban | 0.26 | 20.50 (19.46–21.59) |
20.70 (19.83–21.57) |
42.61 (39.87–45.35) |
52.25 (48.98–55.52) |
63.10 (55.88–70.33) |
132.8 (16.5) | 46.6 (5.8) | 5.0 (0.6) |
| Rural | 0.29 | 20.92 (19.78–22.11) |
20.81 (19.60–22.02) |
43.09 (39.84–46.34) |
53.35 (48.27–58.42) |
67.48 (61.25–73.71) |
89.6 (17.1) | 33.3 (6.4) | 4.0 (0.8) |
| Districts | |||||||||
| North China | 0.28 | 19.34 (18.21–20.54) |
19.45 (18.28–20.62) |
38.57 (34.24–42.90) |
49.10 (42.41–55.80) |
55.93 (46.99–64.88) |
25.8 (13.5) | 8.3 (4.3) | 1.0 (0.5) |
| Northeast China | 0.11 | 19.39 (17.40–21.61) |
18.93 (16.70–21.16) |
44.14 (36.97–51.30) |
56.15 (47.37–64.94) |
72.30 (48.78–95.83) |
18.2 (16.4) | 7.3(7.1) | 0.7 (0.6) |
| East China | 0.18 | 19.39 (17.90–21.00) |
20.03 (18.94–21.12) |
38.11 (35.36–40.86) |
45.53 (42.22–48.84) |
54.52 (49.59–59.45) |
55.2 (13.4) | 13.8 (3.3) | 1.4 (0.4) |
| South-Central China | 0.09 | 22.22 (20.34–24.28) |
21.63 (19.36–23.89) |
46.97 (41.79–52.14) |
56.06 (48.65–63.47) |
67.70 (56.18–79.22) |
65.0 (20.2) | 26.3 (8.1) | 2.5 (0.8) |
| Southwest China | 0.66 | 23.95 (21.95–26.14) |
23.69 (21.91–25.48) |
51.88 (45.02–58.74) |
70.76 (62.21–79.32) |
89.66 (78.16–101.15) |
40.7 (24.6) | 18.8 (11.2) | 3.1 (1.8) |
| Northwest China | 0.36 | 20.36 (18.70–22.15) |
20.30 (18.85–21.75) |
38.13 (32.54–43.72) |
47.78 (36.45–59.11) |
60.89 (41.25–80.53) |
17.5 (13.9) | 5.4 (4.3) | 0.3 (0.3) |
Figure 1.

The spatial distribution of blood lead levels in Chinese population aged 3 to 79 years in 2017–2018 (N=21,701).
Table 2. Declines in blood lead levels (BLLs) for Chinese population aged 3–59 years during the past two decades.
| Sub-population | Year |
Geometric mean
(95% CI), μg/L |
BLLs ≥50 μg/L, % | Rate of decline, % |
Disease burden, DALYs
(million person-years) |
| Abbreviation: DALYs=disability-adjusted life years. | |||||
| Aged 3–5 years | |||||
| Total | 78.4 | ||||
| 2000 | 78.1 (77.0–79.0) | 84.8 | 16.66 | ||
| 2017–2018 | 16.9 (16.1–17.7) | 2.7 | 0.41 | ||
| Sex | |||||
| Men | 77.7 | ||||
| 2000 | 80.0 (78.5–81.5) | 88.3 | 8.83 | ||
| 2017–2018 | 17.8 (16.4–19.4) | 2.6 | 0.21 | ||
| Women | 78.1 | ||||
| 2000 | 75.9 (74.3–77.5) | 81.2 | 7.83 | ||
| 2017–2018 | 16.6 (15.8–17.5) | 2.7 | 0.20 | ||
| Aged 6–59 years | |||||
| Total | 44.7 | ||||
| 2009–2010 | 36.9 (32.1–14.6) | 29.8 | 9.33 | ||
| 2017–2018 | 20.4 (20.0–20.8) | 4.9 | 6.46 | ||
| Sex | |||||
| Men | 43.1 | ||||
| 2009–2010 | 44.3 (37.8–50.8) | 34.6 | 6.65 | ||
| 2017–2018 | 24.2 (23.2–25.3) | 7.7 | 4.95 | ||
| Women | 44.6 | ||||
| 2009–2010 | 30.3 (24.6–36.0) | 19.5 | 2.70 | ||
| 2017–2018 | 16.8 (16.1–17.4) | 3.2 | 1.50 | ||
| Age (years) | |||||
| 6–11 | 52.4 | ||||
| 2009– 2010 | 35.3 (30.0–41.6) | 23.7 | 0.21 | ||
| 2017–2018 | 16.8 (16.1–17.6) | 1.8 | 0.12 | ||
| 12–18 | 54.4 | ||||
| 2009–2010 | 33.3 (26.1–42.6) | 22.5 | 0.47 | ||
| 2017–2018 | 15.2 (14.5–15.9) | 2.0 | 0.25 | ||
| 19–39 | 40.5 | ||||
| 2009–2010 | 35.8 (28.4–45.2) | 28.9 | 1.90 | ||
| 2017–2018 | 21.3 (20.3–22.4) | 5.2 | 1.23 | ||
| 40–59 | 37.5 | ||||
| 2009–2010 | 39.6 (33.1–47.6) | 32.5 | 6.74 | ||
| 2017–2018 | 24.8 (23.7–25.9) | 9.6 | 4.71 | ||
DISCUSSION
Our study found that both the BLLs among the Chinese population aged 3–5 years and 6–59 years exhibited decreases of varying degrees in the past two decades. Our study demonstrated that the decline in BLLs in the Chinese population was akin to the decline in the USA. Implementation of the elimination of leaded gasoline preceded the observed decline in BLLs. Leaded paint, while a major source of indoor exposure in the United States, was not widely used in the Chinese housing stock, and most residents reside in dwellings built after the banning of leaded paint. Therefore, the BLLs in Chinese residents were closely related to the levels of environmental lead exposure and the formulation of policies related to lead. However, compared with the latest monitoring results of developed countries such as the United States and Canada, the internal exposure to lead in Chinese population was still at a relatively higher level, indicating a higher disease burden and limiting intellectual quotient attainment of children on a population scale (9–10). It has been observed that BLLs in Tibet are higher than in other regions, which may be due to this population’s unique dietary and living habits.
The BLRV is 100 μg/L in China at present, higher than the American standard (35 μg/L) (3) and the World Health Organization (WHO) standard (50 μg/L) (11), and therefore needs updates based on our measurements in the decline of BLLs over the past two decades. However, setting standards is complicated by various literature using inconsistent criteria for BLRV definition. In this study, we established reference values based on blood lead concentrations stratified according to age. Although a lower BLRV increases the burden on the medical system, especially in pediatrics, we cannot deny that a more stringent BLRV would identify at-risk populations as much as possible and give caregivers, communities, and officials more opportunities to act earlier. Measures to improve lead exposure monitoring and prevention interventions for high-risk populations are priorities for future work. Government agencies, employers, and worker-affiliated organizations are responsible for carrying out education in the workplace and community in accordance with the latest guidelines and recommendations.
The strengths of this study include the CNHBM data obtained by the official organization, which firstly permits the characterization of BLLs in a nationally representative sample of the general Chinese population aged 3–79 years. We updated the BLRV based on the current blood lead levels from the results of the nationally representative study with the largest sample size and scope so far. Our study conducted a longitudinal comparison of BLLs among Chinese population through three surveys, focusing on the general population rather than specific groups such as those with high occupational exposure.
This study was subject to some limitations. First, surveys in 2000 and 2009/10 were only regional-scale, though being the largest study of BLLs monitoring in China at the time, and the study samples only covered part of the age group, limiting the comparison of the changing trends of BLLs. Second, our study involved three different cross-sectional studies, with the result that different people were sampled with iterations of the study, so that determination of within-individual temporal trends in BLLs cannot be obtained.
The study demonstrated a substantial decline in BLLs and the disease burden of the entire Chinese population in the past two decades, which provided evidence that China has made significant achievements in controlling lead pollution. Furthermore, there is an urgent need to update a lower BLRV based on the significant reductions in current blood lead levels that are more sensitive to monitor and screen people with high BLLs with significant public health value for prevention of hazards of lead exposure. The study added needed evidence on behalf of populous developing countries. There is no known safe blood lead concentration, and even as BLL declines, governments and public health institutions need to protect future generations if continued efforts to preemptively control or even eliminate lead sources and provide timely interventions for persons at the highest risk for exposure.
SUPPLEMENTARY MATERIALS
Supplementary Methods
Variable Definition
Residences were categorized as rural and urban. Districts were defined as northern, northeastern, eastern, central south, southwest, and northeast. Occupation was defined as the first, secondary and tertiary industries. House type was categorized as cottage, simple building, villa, and other types. Lifestyle variables were cigarette smoking, tea drinking, and alcohol drinking. Cigarette smoking was defined as never, <70 cigarettes/week, 71–105 cigarettes/week, 106–140 cigarettes/week, ≥141 cigarettes/week. Alcohol drinking was defined as never, <2 times/month, 2–4 times/month, 2–3 times/week, and ≥4 times/week. Tea drinking was defined as <once/month, once/month–6 times/week, 7–20 times/week, ≥21 times/week. Dietary habits were constructed as described previously based on food groups including sea fish (never, <once/month, 1–7 times/month, 2 times/week, 3 times/week, ≥4 times/week, missing), sea shell (once/month, 1–7 times/month, 2 times/week, ≥3 times/week, missing), freshwater fish (once/month, 1–3 times/month, once/week, 2 times/week, ≥3 times/week, missing), rice (<4 times/week, 4–6 times/week, 7–13 times/week, 14–20 times/week, ≥21 times/week, missing), meat (<once/month, 1–2 times/month, 3–6 times/week, 7–13 times/week, 14–20 times/week, ≥21 times/week, missing), milk (<once/month, 1–3 times/month, 1–6 times/week, ≥7 times/week, missing), fruits (<once/month, 1–3 times/month, 1–6 times/week, 7–13 times/week, ≥14 times/week, missing), flour (<once/month, 1–3 times/month, 1–6 times/week, 7–13 times/week, ≥14 times/week, missing), tubers (<once/month, 1–3 times/month, 1–2 times/week, ≥3 times/week, missing), beans (<once/month, 1–3 times/month, once/week, 2 times/week, ≥3 times/week, missing), nuts (<once/month, 1–3 times/month, 1–2 times/week, 3–6 times/week, ≥7 times/week, missing).
Blood Lead Measurements
The methods for determining lead in blood (1 μg/L = 0.00483 μmol/L), including quality control and assurance procedures, have been described for each survey. Comparability has been established for the method used in five laboratories. The limits of determination (LOD) for blood lead were 0.8, 0.28, and 0.03 μg/L in the 2000, 2009/10, and 2017/18 surveys, respectively. 2.3% of samples were less than LOD in the 2017/18 surveys. For the calculation of mean lead levels, the LOD/2 was imputed for samples below the LOD. Although there is no safe blood lead level (BLL) for the population, using dichotomous BLL thresholds is advantageous for assessing trends over time. These cut points may be more easily understood than statistically derived cut points such as quartiles. An elevated BLL was defined a priori as 50 µg/L at or above selected values chosen in part because of their prior or potential use in public health policy. Given the multiple hazards of exposure to lead, during a May 2021 meeting of the Lead Exposure and Prevention Advisory Committee (LEPAC), the workgroup recommended that the blood lead reference value (BLRV) be updated from 50 µg/L to 35 µg/L using data derived from the two most recent National Health and Nutrition Examination Surveys (NHANES) cycles (2015–2016 and 2017–2018).
Quality Control in the Laboratory of Blood Lead
We used high-purity reagents for standard solutions and sample preparation. Before analysis and determination, the instrument was tuned with a mass spectrometry tuning solution, and the experiment was carried out after the main technical indicators (low, medium, and high-quality element sensitivity, oxide ratio, and double charge ratio) reached the standard. The nebulizer and sample cone were periodically soaked and cleaned with diluted nitric acid. Calibration curves, certified standard reference materials (external quality control), parallel samples, field blanks, and laboratory reagent blanks were determined for each batch of experiments. The linear correlation coefficient r of the calibration curve was required to be greater than 0.995. The certified reference material was measured once every 30 samples, and the measurement result was within the allowable error range of the reference value; one parallel sample (randomly selected) was measured for every 20 samples. The relative error of the parallel sample was less than 10%. The laboratory reagent blank determination was less than the method’s detection limit. When the measured concentration of the sample exceeded the measurement range of the calibration curve, we reduced the sampling amount or increased the dilution factor and then re-measured.
Methods of Estimating the Burden of Disease Associated with Lead Exposure in Participants Aged 6–59 years
The burden of disease was assessed using the disability-adjusted life years (DALYs) developed by the Global Burden of Disease Study. This study assessed YLLs in the 6–59 age group.
YLLs calculation method: Firstly, based on the literature to find the dose-response relationship between lead and the risk of all-cause mortality, the HR(Ci) values under the exposure level Ci of different age groups and sex groups of Chinese residents were calculated by the hazard ratio (HR). Mortality M in different age and gender groups was collected and calculated according to formula (1) the mortality  in the region if exposure levels were reduced to the theoretical minimum risk value across the region. According to formula (2), the number of premature deaths due to exposure to lead (Mi) can be calculated. This study estimated YLLs according to Equation (3). The HR(Ci) values involved in the formula were estimated by finding the HR values in the dose-response relationship between internal exposure and the risk of all-cause death in the relevant literature, combined with the actual exposure level of Chinese residents. The mortality data of each age group when calculating YLLs comes from the “2016 China Cause of Death Surveillance Dataset”.
in the region if exposure levels were reduced to the theoretical minimum risk value across the region. According to formula (2), the number of premature deaths due to exposure to lead (Mi) can be calculated. This study estimated YLLs according to Equation (3). The HR(Ci) values involved in the formula were estimated by finding the HR values in the dose-response relationship between internal exposure and the risk of all-cause death in the relevant literature, combined with the actual exposure level of Chinese residents. The mortality data of each age group when calculating YLLs comes from the “2016 China Cause of Death Surveillance Dataset”.
 |
1 |
 |
2 |
 |
3 |
Methods of Estimating the Burden of Disease Associated with Lead Exposure in Children Aged 3–5 Years
The burden of disease was calculated based on the method published in 2003 by World Health Organization (WHO). The method indicates that the loss of intelligence quotient (IQ) points can be calculated ideally based on the linear dose-response relationship between BLLs and IQ loss. When the BLL is between 50 and 200 μg/L, the IQ decreases by 1.3 points for every 50 μg/L increase; for BLLs over 200 μg/L, a loss of 3.5 IQ points is assumed. When IQ levels are above 50 points, intelligence in human populations generally approximates a normal distribution. According to the distribution of BLL of Chinese residents obtained from our investigation and the assessment method provided by WHO, the proportion of children aged 3–5 years with different BLLs and the proportion of children with IQ loss caused by lead exposure were calculated respectively on the premise that the IQ distribution in the population was a normal distribution.
The WHO guidelines use the incidence of mild mental retardation (MMR) as a quantified indicator of the health effects caused by lead exposure and assess the burden of MMR disease. MMR occurs when the IQ is below 70 points but above 50 points. Even if IQ points decrease due to various diseases or exposures, they can also remain above 70 because of the higher original IQ. Consequently, assessing the disease burden of MMR requires counting the number of people with an IQ slightly above the threshold of 70 who enter the MMR range through loss of IQ points due to lead exposure. Some infectious and parasitic diseases can also cause MMR, therefore, according to the prevalence of MMR caused by known non-congenital causes in different regions, WHO calculates the adjustment ratio (AR) of MMR. According to the method, the incidence of MMR in each age group was calculated by multiplying the proportion of children with the defined IQ point losses by the respective percentage of the population in that range of BLLs, based on the distributions of BLLs and IQ levels of children. The formula is as follows:
 |
4 |
In formula (1), E1, E2, E3, and E4 represent the proportion of children with BLLs of 50–100 μg/L, 100–150 μg/L, 150–200 μg/L, and >200 μg/L, respectively; P1, P2, P3, and P4 represent the proportion of children with IQ points of 70–70.65, 70–71.95, 70–73.25, and 70–73.50, respectively; AR is the adjustment ratio and the value of China (WHO Western Pacific Region) is 3.03.3.
Disability adjusted life years (DALYs) were used to quantitatively measure the burden of MMR in children caused by lead exposure. The DALYs are the sum of years of life lost due to premature death [years of life lost (YLLs)] and years lived with disability including permanent disability and temporary incapacity [years lived with disability (YLDs)]. Because MMR due to lead exposure in children rarely leads to death, only YLDs were estimated. So we performed the calculation based on the simplified formula for DALYs recommended in the approach of the Global Burden of Diseases, Injuries, and Risk Factors enterprise (GBD 2010):
 |
5 |
In formula (2), I is the number of prevalent cases, it can be obtained by multiplying IMMR by the number of children in that age group; DW is the disability weight; L is the duration of disability. It is generally assumed that intellectual impairment exists early in life and remains throughout life, life expectancy is therefore calculated as the duration of disability. The incidence of MMR, the number of children in 3–5 age group in the sixth national census of China, the average life expectancy data (77.0 years) in the 2018 Statistical Bulletin of China’s Health Development and the disability weight of MMR (0.361) were substituted into the formula for calculation.
Figure S1.
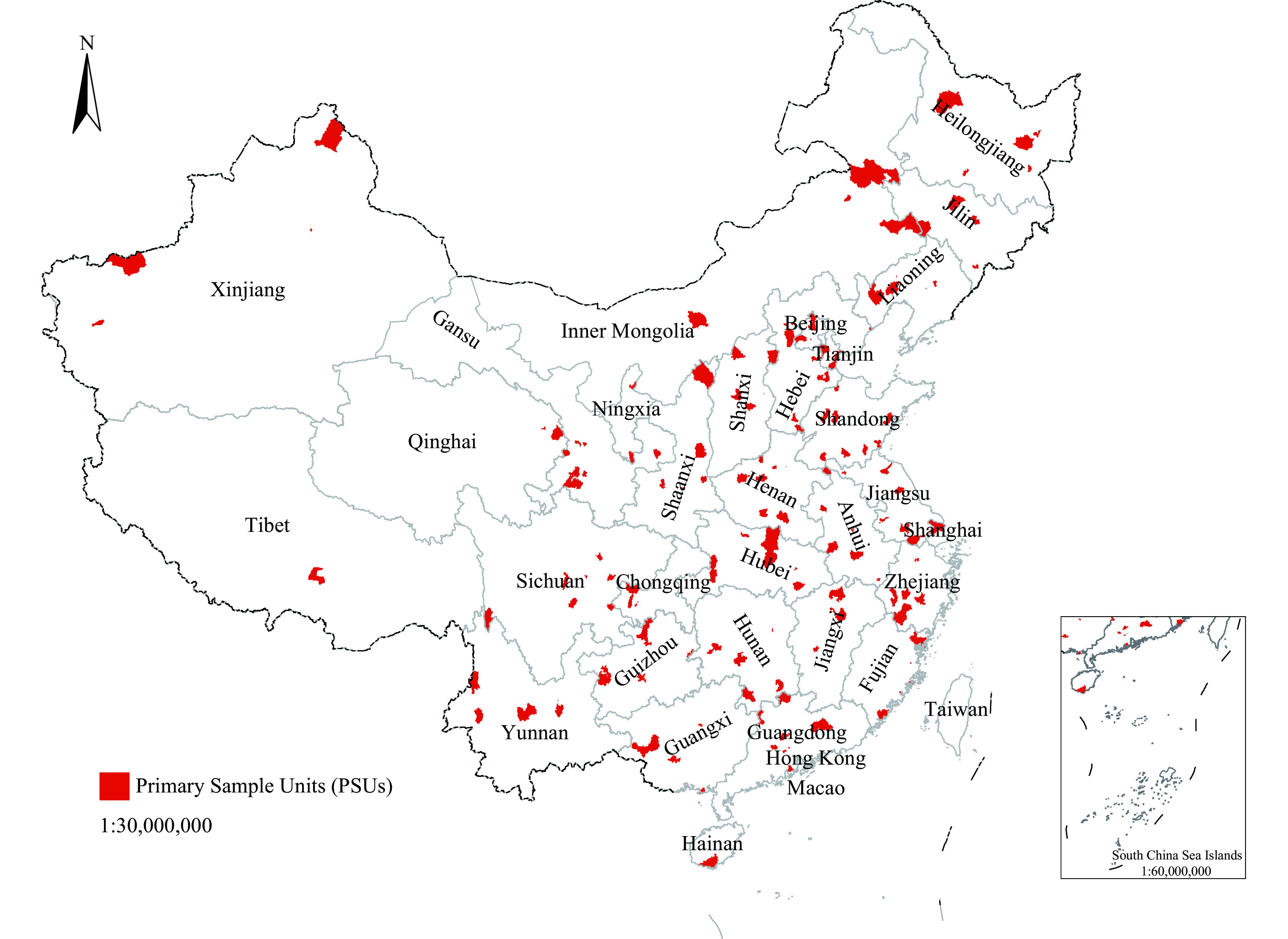
Spatial locations of the monitoring units in China National Human Biomonitoring.
Figure S2.
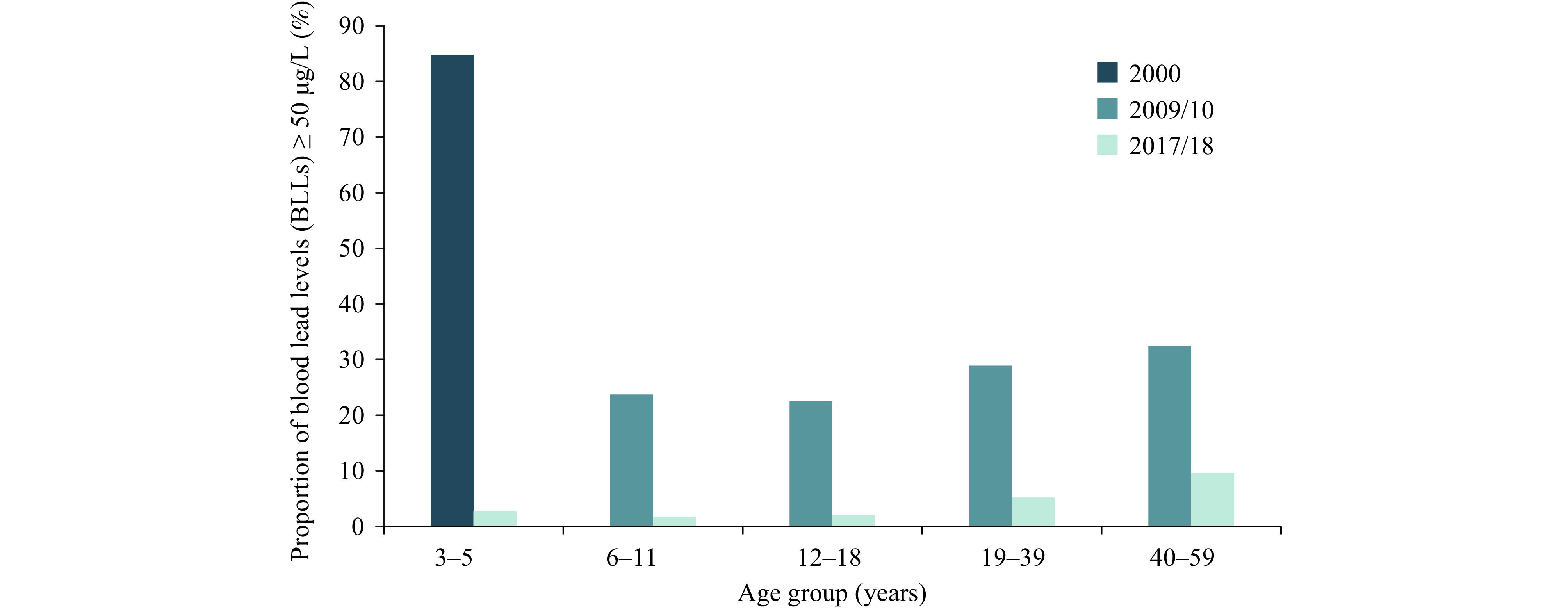
Comparison of proportions of blood lead levels (BLLs) over 50 μg/L in 2000–2018.
Table S1. The blood lead levels of Chinese children aged 3–5 years in 2000.
| Sub group | Frequency |
Geometric mean
(95% CI), μg/L |
P10
(95% CI), μg/L |
P25
(95% CI), μg/L |
Median (95% CI), μg/L |
P75 (95% CI), μg/L |
P90
(95% CI), μg/L |
P95
(95% CI), μg/L |
P99
(95% CI), μg/L |
| Abbreviation: PLADs=provincial level administrative divisions. | |||||||||
| Total | 6,085 | 78.1 (77.0–79.2) |
38.5 (36.5–40.4) |
62.0 (60.8–63.0) |
81.4 (80.5–82.1) |
110.9 (109.0–112.5) |
150.5 (147.0–153.0) |
175.0 (171.0–178.5) |
228.0 (219.5–241.5) |
| Gender | |||||||||
| Male | 3,260 | 80.0 (78.5–81.5) |
41.5 (38.5–43.5) |
63.0 (61.6–64.0) |
82.5 (81.5–83.6) |
114.5 (111.0–117.5) |
152.4 (149.5–156.0) |
176.9 (170.7–183.0) |
226.6 (216.0–238.5) |
| Female | 2,825 | 75.9 (74.3–77.5) |
35.5 (33.0–38.0) |
60.7 (59.1–62.2) |
80.2 (79.0–81.3) |
106.5 (103.8–109.2) |
146.2 (143.0–152.1) |
173.0 (167.0–178.2) |
234.0 (218.0–260.0) |
| PLADs | |||||||||
| Anhui | 837 | 70.5 (68.9–72.1) |
52.0 (49.2–53.6) |
61.0 (59.5–62.5) |
70.0 (68.9–70.9) |
82.0 (79.8–85.0) |
102.5 (98.5–110.1) |
124.5 (114.5–142.0) |
175.2 (168.3–204.5) |
| Gansu | 248 | 116.0 (109.6–122.7) |
65.5 (56.5–74.0) |
85.6 (79.9–93.8) |
118.3 (107.6–125.0) |
156.4 (147.5–176.5) |
211.1 (197.8–229.0) |
241.5 (226.6–266.0) |
268.0 (266.0–299.0) |
| Hainan | 526 | 103.7 (99.6–107.9) |
52.5 (45.1–60.4) |
78.61 (72.7–82.8) |
115.0 (105.8–123.0) |
151.9 (147.0–156.8) |
176.4 (169.1–180.0) |
185.5 (182.7–189.8) |
197.7 (193.0–210.9) |
| Henan | 543 | 128.6 (124.9–132.3) |
83.3 (78.6–88.0) |
107.9 (102.5–111.0) |
134.0 (129.6–139.5) |
160.0 (155.5–163.0) |
190.0 (183.0–202.0) |
215.0 (203.6–222.9) |
259.50 (241.0–283.0) |
| Heilongjiang | 1,105 | 76.9 (75.0–78.8) |
52.2 (48.4–55.7) |
70.7 (67.9–72.7) |
82.0 (81.0–82.6) |
90.7 (88.8–92.1) |
113.5 (108.6–120.0) |
136.0 (128.0–143.6) |
190.30 (176.0–214.5) |
| Hubei | 495 | 55.3 (52.0–58.9) |
17.5 (15.0–20.0) |
40.5 (32.5–49.5) |
66.5 (64.5–68.5) |
86.0 (80.0–90.0) |
116.0 (107.5–125.5) |
135.0 (126.0–149.5) |
228.0 (167.0–328.5) |
| Hunan | 443 | 37.3 (35.1–39.6) |
17.5 (15.5–19.0) |
24.0 (23.0–26.0) |
35.0 (32.5–37.0) |
52.0 (47.5–56.5) |
99.0 (83.0–124.5) |
134.0 (124.5–146.0) |
199.5 (163.0–319.0) |
| Jilin | 893 | 93.7 (91.0–96.6) |
62.0 (58.2–64.4) |
76.5 (74.6–78.2) |
93.5 (90.5–96.0) |
121.0 (117.5–125.0) |
155.8 (146.7–165.4) |
182.0 (172.0–195.5) |
270.0 (234.0–443.4) |
| Ningxia | 995 | 71.9 (70.0–73.8) |
41.0 (38.5–43.5) |
55.5 (53.5–57.5) |
71.5 (69.5–74.1) |
97.0 (93.4–100.0) |
121.5 (118.0–128.0) |
141.5 (134.5–150.5) |
194.0 (170.5–231.0) |
Table S2. The blood lead levels of Chinese population in 2009/10.
| Sub group | Frequency |
Geometric mean (95% CI), μg/L |
P10 (95% CI), μg/L |
P25 (95% CI), μg/L |
Median (95% CI), μg/L |
P75 (95% CI), μg/L |
P90 (95% CI), μg/L |
P95 (95% CI), μg/L |
P99 (95% CI), μg/L |
| * The frequency is too low for bootstrap to resample. | |||||||||
| Total | 11,090 | 36.9 (30.3–44.9) |
17.6 (14.7–20.5) |
25.7 (22.3–29.1) |
37.3 (31.0–43.5) |
55.9 (40.0–71.9) |
83.9 (38.6–129.2) |
109.7 (46.4–173.0) |
211.6 (.–.)* |
| Age, years | |||||||||
| 6–11 | 1,525 | 35.4 (30.0–41.6) |
19.96 (17.1–22.8) |
26.8 (23.0–30.6) |
35.6 (30.6–40.6) |
49.1 (34.8–63.4) |
67.6 (36.8–98.5) |
81.96 (.–.)* |
112.6 (91.0–134.3) |
| 12–18 | 3,573 | 33.3 (26.1–42.6) |
16.8 (13.0–20.6) |
23.6 (19.2–28.0) |
33.8 (26.2–41.4) |
47.8 (26.8–68.8) |
70.7 (.–.)* |
89.6 (.–.)* |
151.5 (.–.)* |
| 19–39 | 3,533 | 35.9 (28.5–45.2) |
17.2 (13.2–21.2) |
25.3 (21.3–29.3) |
36.9 (29.9–44.0) |
55.0 (36.6–73.5) |
84.1 (34.2–134.1) |
109.2 (67.0–151.3) |
176.3 (.–.)* |
| 40–60 | 2,459 | 39.7 (33.1–47.6) |
17.8 (15.2–20.4) |
26.7 (23.8–29.5) |
39.7 (34.1–45.3) |
60.4 (45.2–75.7) |
92.0 (32.2–151.7) |
126.2 (.–.)* |
262.4 (.–.)* |
| Gender | |||||||||
| Female | 5,616 | 29.9 (23.6–38.0) |
14.6 (11.4–17.8) |
21.5 (18.1–25.0) |
30.3 (24.6–36.0) |
45.1 (28.5–61.6) |
69.1 (.– .)* |
88.8 (.–.)* |
166.8 (.–.)* |
| Male | 5,474 | 45.0 (38.0–53.3) |
22.7 (18.9–26.5) |
31.5 (28.0–35.0) |
44.3 (37.8–50.8) |
65.5 (47.1–83.8) |
96.3 (58.8–133.9) |
124.2 (70.0–178.5) |
225.9 (.–.)* |
| Region | |||||||||
| Eastern China | 8,010 | 31.9 (26.6–38.3) |
21.0 (.–.)* |
27.7 (13.6–41.8) |
43.1 (20.7–65.5) |
65.0 (19.4–110.7) |
92.2 (16.6–167.9) |
114.1 (64.4–163.8) |
208.5 (.–.)* |
| Central China | 1,376 | 43.4 (29.2–64.3) |
15.7 (12.5–19.0) |
23.6 (20.4–26.9) |
33.6 (29.4–37.7) |
47.0 (40.3–53.7) |
65.95 (44.6–87.4) |
83.2 (.–.)* |
200.1 (.–.)* |
| Western China | 1,704 | 63.8 (38.5–105.9) |
30.3 (.–.)* |
43.8 (.–.)* |
66.3 (20.2–112.3) |
93.0 (55.3–130.7) |
125.4 (94.9–155.9) |
147.8 (112.0–183.6) |
227.0 (.–.)* |
| City | |||||||||
| Beijing | 568 | 33.9 (32.1– 35.9) |
18.4 (16.2– 20.6) |
26.1 (24.5– 27.6) |
36.2 (34.7–37.8) |
49.8 (47.4–52.2) |
66.3 (61.2–71.5) |
75.9 (70.2–81.7) |
100.2 (81.1–119.2) |
| Chaozhou | 699 | 47.5 (45.5–49.6) |
26.8 (24.7–28.8) |
35.3 (33.5–37.2) |
45.97 (44.1–47.8) |
63.8 (60.0–67.6) |
83.9 (78.2–89.5) |
100.3 (85.97– 114.7) |
269.7 (165.0–374.5) |
| Chengde | 554 | 29.9 (28.4–31.5) |
15.8 (14.4–17.3) |
21.1 (19.9–22.3) |
30.4 (27.7–33.1) |
44.3 (41.1–47.5) |
54.7 (50.7–58.7) |
60.1 (51.4–68.8) |
81.8 (.–.)* |
| Dandong | 492 | 33.0 (31.3–34.8) |
19.4 (18.1–20.7) |
25.8 (24.4–27.2) |
33.8 (32.5–35.2) |
44.0 (40.7–47.2) |
56.2 (50.2–62.2) |
66.1 (56.5–75.6) |
83.9 (.–.)* |
| Haidong | 560 | 44.7 (42.3–47.3) |
22.4 (20.7–24.0) |
30.8 (28.6–33.0) |
42.9 (40.4–45.4) |
62.4 (56.9–67.9) |
95.5 (77.0–114.0) |
130.4 (114.5–146.3) |
177.9 (.–.)* |
| Heze | 313 | 9.8 (8.2–11.8) |
2.3 (0.9–3.6) |
5.9 (4.3–7.6) |
13.9 (11.9–15.8) |
23.5 (20.1–26.8) |
33.1 (28.2–38.0) |
41.3 (29.6–53.0) |
66.4 (.–.)* |
| Jiaozuo | 463 | 60.3 (56.9–64.1) |
32.8 (30.1–35.5) |
40.6 (37.3–43.9) |
57.5 (53.2–61.8) |
82.5 (76.8–88.3) |
108.3 (98.9–117.7) |
135.7 (93.3–178.1) |
311.1 (.–.)* |
| Jinan | 465 | 22.7 (20.9–24.7) |
8.6 (6.5–10.7) |
16.6 (14.7–18.4) |
25.8 (23.6–27.9) |
36.4 (34.4–38.4) |
47.0 (43.4–50.5) |
56.8 (50.2–63.3) |
71.0 (30.9–111.2) |
| Jinzhou | 566 | 31.3 (29.9–32.8) |
17.8 (16.7–19.0) |
23.6 (22.1–25.1) |
30.1 (28.7–31.5) |
42.2 (39.3–45.2) |
55.3 (51.3–59.4) |
63.9 (55.2–72.7) |
81.9 (.–.)* |
| Langfang | 549 | 36.8 (34.6–39.2) |
19.9 (17.9–22.0) |
27.9 (26.3–29.5) |
37.6 (35.3–40.0) |
51.8 (47.7–55.9) |
68.1 (64.2–72.0) |
75.9 (70.6–81.2) |
110.9 (.–.)* |
| Lianyungang | 455 | 34.5 (33.1–36.0) |
22.0 (20.7–23.3) |
27.6 (26.4–28.8) |
34.9 (33.5–36.3) |
43.95 (40.9–47.0) |
55.4 (52.5–58.3) |
60.5 (55.9–65.0) |
76.6 (.–.)* |
| Pingdingshan | 467 | 32.4 (30.5–34.4) |
18.4 (17.0–19.8) |
22.6 (21.4–23.8) |
30.8 (28.4–33.1) |
44.5 (41.4–47.6) |
54.1 (48.1–60.1) |
72.7 (43.9–101.5) |
151.9 (.–.)* |
| Puyang | 446 | 39.96 (37.4–42.7) |
19.4 (18.3–20.5) |
25.1 (23.4–26.9) |
39.1 (34.4–43.8) |
62.8 (57.3–68.2) |
83.6 (75.1–92.1) |
109.1 (92.7–25.5) |
144.8 (.–.)* |
| Qingdao | 313 | 20.4 (18.1–23.0) |
7.1 (5.3–9.0) |
13.2 (11.2–5.2) |
21.9 (18.4–25.4) |
35.4 (29.2–41.6) |
56.1 (50.1–62.1) |
61.3 (52.7–69.9) |
97.0 (.–.)* |
| Qingyuan | 530 | 83.1 (76.3– 90.6) |
34.7 (32.1–37.3) |
47.0 (43.4–50.6) |
76.9 (67.8–86.0) |
136.7 (113.5–159.8) |
227.6 (188.1–267.0) |
298.6 (161.3–435.8) |
604.7 (.–.)* |
| Shenyang | 247 | 25.9 (24.3–27.5) |
14.9 (13.4–16.4) |
19.3 (17.2–21.4) |
27.4 (25.0–29.7) |
33.7 (30.5–36.9) |
44.1 (41.3– 46.9) |
47.8 (43.8–51.2) |
66.1 (.–.)* |
| Shijiazhuang | 543 | 32.1 (30.8–33.3) |
19.4 (18.0–20.7) |
25.1 (23.5–26.6) |
31.3 (29.5–33.1) |
41.6 (39.8–43.4) |
52.9 (48.5– 57.2) |
58.9 (54.3–63.6) |
80.1 (.–.)* |
| Suzhou | 522 | 33.3 (31.7–35.1) |
18.9 (17.1–20.6) |
25.2 (23.7–26.6) |
33.5 (31.7–35.4) |
45.4 (43.5–47.2) |
57.1 (50.8– 63.3) |
68.8 (61.8–75.8) |
85.2 (68.1–102.3) |
| Taizhou | 549 | 35.7 (34.4–37.0) |
23.2 (21.7–24.8) |
28.2 (27.1–29.4) |
35.6 (34.1–37.0) |
44.2 (42.5–46.0) |
55.1 (51.4– 58.8) |
62.7 (56.6–68.9) |
84.3 (.–.)* |
| Xining | 1,144 | 76.0 (73.4–78.6) |
41.6 (38.8–44.4) |
57.4 (54.8–60.0) |
76.3 (73.5–79.1) |
100.4 (96.4–104.4) |
131.7 (122.8– 140.6) |
157.1 (139.7–174. 6) |
261.2 (182.8–339.7) |
| Zhanjiang | 645 | 22.9 (21.1–24.9) |
10.6 (9.0–12.3) |
17.7 (16.5–18.9) |
26.1 (24.8–27.5) |
36.9 (34.4–39.4) |
48.8 (42.7– 55.0) |
60.7 (54.9–66.5) |
91.5 (32.5–150.5) |
Table S3. Burden of disease from lead exposure in Chinese population aged 6–59 years measured in 2000 and 2017/18.
| Age group, years | HR | Weighted mortality, % | Adjusted weighted mortality, % | Population, million | Population of premature deaths | DALYs |
| Abbreviation: HR=hazard ratio; DALYs=disability-adjusted life years. | ||||||
| 6–11 | ||||||
| 2009–2010 | ||||||
| Male | 1.23 | 0.024 | 0.019 | 45.83 | 2,028 | 139,530 |
| Female | 1.23 | 0.015 | 0.012 | 38.71 | 1,097 | 75,453 |
| Total | – | – | – | – | – | 214,984 |
| 2017–2018 | ||||||
| Male | 1.12 | 0.024 | 0.021 | 45.83 | 1,131 | 77,794 |
| Female | 1.11 | 0.015 | 0.014 | 38.71 | 564 | 38,785 |
| Total | – | – | – | – | – | 116,579 |
| 12–18 | ||||||
| 2009–2010 | ||||||
| Male | 1.22 | 0.036 | 0.030 | 65.74 | 4,257 | 265,231 |
| Female | 1.22 | 0.019 | 0.015 | 99.89 | 3,306 | 205,934 |
| Total | – | – | – | – | – | 471,166 |
| 2017–2018 | ||||||
| Male | 1.11 | 0.036 | 0.033 | 65.74 | 2,436 | 151,745 |
| Female | 1.09 | 0.019 | 0.017 | 99.89 | 1,581 | 98,491 |
| Total | – | – | – | – | – | 250,236 |
| 19–39 | ||||||
| 2009–2010 | ||||||
| Male | 1.23 | 0.093 | 0.075 | 136.50 | 23,913 | 1,155,014 |
| Female | 1.23 | 0.038 | 0.030 | 218.83 | 15,492 | 748,246 |
| Total | – | – | – | – | – | 1,903,260 |
| 2017–2018 | ||||||
| Male | 1.16 | 0.093 | 0.080 | 136.50 | 17,318 | 836,466 |
| Female | 1.11 | 0.038 | 0.034 | 218.83 | 8,196 | 395,878 |
| Total | – | – | – | – | – | 1,232,344 |
| 40–59 | ||||||
| 2009–2010 | ||||||
| Male | 1.26 | 0.450 | 0.358 | 198.83 | 183,229 | 5,093,771 |
| Female | 1.26 | 0.151 | 0.120 | 191.58 | 59,334 | 1,649,472 |
| Total | – | – | – | – | – | 6,743,243 |
| 2017–2018 | ||||||
| Male | 1.18 | 0.450 | 0.381 | 198.83 | 136,697 | 3,800,183 |
| Female | 1.13 | 0.151 | 0.134 | 191.58 | 32,919 | 915,159 |
| Total | – | – | – | – | – | 4,715,342 |
| 60–79 | ||||||
| 2009–2010 | ||||||
| Male | – | – | – | – | – | – |
| Female | – | – | – | – | – | – |
| Total | – | – | – | – | – | – |
| 2017–2018 | ||||||
| Male | 1.17 | 2.929 | 2.493 | 78.27 | 341,216 | 2,661,485 |
| Female | 1.14 | 1.408 | 1.233 | 78.34 | 136,747 | 1,066,628 |
| Total | – | – | – | – | – | 3,728,114 |
| Total | ||||||
| 2009–2010 | ||||||
| Male | – | – | – | – | – | 6,653,547 |
| Female | – | – | – | – | – | 2,679,105 |
| Total | – | – | – | – | – | 9,332,652 |
| 2017–2018 | ||||||
| Male | – | – | – | – | – | 7,615,225 |
| Female | – | – | – | – | – | 2,568,477 |
| Total | – | – | – | – | – | 10,183,702 |
Table S4. Burden of disease from lead exposure in Chinese population aged 3–5 years old measured in 2000 and 2017/18.
| Year | No. of participants | Blood lead geometric mean, μg/L | Incidence of mild mental retardation (‰) |
DALYs
(Person-year/1,000 children) |
DALYs
(Person-year) |
| Abbreviation: DALYs=disability-adjusted life years. | |||||
| 2000 | 46,612,176 | 78.1 | 13.87 | 357.4 | 16,659,509 |
| 2017–2018 | 45,202,983 | 16.9 | 0.33 | 9.0 | 408,780 |
REFERENCES
World Health Organization. Assessing the environmental burden of disease at national and local levels: introduction and methods. 2003. https://www.who.int/publications/i/item/9241546204. [2003-7-2].
Fewtrell LJ, Prüss-Üstün A, Landrigan P, Ayuso-Mateos JL. Estimating the global burden of disease of mild mental retardation and cardiovascular diseases from environmental lead exposure. Environ Res 2004;94(2):120 − 33. http://dx.doi.org/10.1016/S0013-9351(03)00132-4.
Yan YZ, Yang SL, Zhou YJ, Song Y, Huang J, Liu ZP, et al. Estimating the national burden of mild intellectual disability in children exposed to dietary lead in China. Environ Int 2020;137:105553. http://dx.doi.org/10.1016/j.envint.2020.105553.
Funding Statement
This work was supported by National Health Commission of the People's Republic of China, the National Institute of Environmental Health of Chinese Center for Disease Control and Prevention, and National Natural Sciences Foundation of China (81872707)
Contributor Information
Xiaoyuan Yao, Email: yaoxy@chinacdc.cn.
Yuxin Zheng, Email: yxzheng@qdu.edu.cn.
Xiaoming Shi, Email: shixm@chinacdc.cn.
References
- 1.Reuben A, Caspi A, Belsky DW, Broadbent J, Harrington H, Sugden K, et al Association of childhood blood lead levels with cognitive function and socioeconomic status at age 38 years and with IQ change and socioeconomic mobility between childhood and adulthood. JAMA. 2017;317(12):1244–51. doi: 10.1001/jama.2017.1712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Centers for Disease Control and Prevention (CDC). Very high blood lead levels among adults - United States, 2002-2011. MMWR Morb Mortal Wkly Rep 2013;62(47):967-71. https://pubmed.ncbi.nlm.nih.gov/24280917/.
- 3.Ruckart PZ, Jones RL, Courtney JG, LeBlanc TT, Jackson W, Karwowski MP, et al Update of the blood lead reference value - United States, 2021. MMWR Morb Mortal Wkly Rep. 2021;70(43):1509–12. doi: 10.15585/mmwr.mm7043a4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ministry of Health. High blood lead and lead poisoning prevention guidelines in children. 2006,17(4):1-2. http://www.nhc.gov.cn/fys/s3585/200602/f8742aef6c654935866fa7cbf4e78d94.shtml. [2022-10-21]. (In Chinese).
- 5.Han ZX, Guo XY, Zhang BM, Liao JG, Nie LS Blood lead levels of children in urban and suburban areas in China (1997-2015): temporal and spatial variations and influencing factors. Sci Total Environ. 2018;625:1659–66. doi: 10.1016/j.scitotenv.2017.12.315. [DOI] [PubMed] [Google Scholar]
- 6.Cao ZJ, Lin SB, Zhao F, Lv YB, Qu YL, Hu XJ, et al Cohort profile: China National Human Biomonitoring (CNHBM) - A nationally representative, prospective cohort in Chinese population. Environ Int. 2021;146:106252. doi: 10.1016/j.envint.2020.106252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Qi QP, Yang YW, Yao XY, Ding L, Wang W, Liu YY, et al. Blood lead level of children in the urban areas in China. Chin J Epidemiol 2002;23(3):162-6. https://d.wanfangdata.com.cn/periodical/ChlQZXJpb2RpY2FsQ0hJTmV3UzIwMjIxMDEzEg96aGx4YngyMDAyMDMwMDIaCHJ0czQ5NnRk. (In Chinese).
- 8.Ding CG, Pan YJ, Zhang AH, Wu BH, Huang HL, Zhu C, et al. Study of distribution and influencing factors of lead and cadmium in whole blood and urine among population in 8 provinces in China. Chin J Prev Med 2014;48(2):91-6. http://rs.yiigle.com/CN112150201402/142256.htm. (In Chinese).
- 9.Crinnion WJ. The CDC fourth national report on human exposure to environmental chemicals: what it tells us about our toxic burden and how it Assist environmental medicine physicians. Altern Med Rev 2010;15(2):101-9. https://pubmed.ncbi.nlm.nih.gov/20806995/.
- 10.Health Canada. Fourth report on human biomonitoring of environmental chemicals in Canada. 2017. https://www.canada.ca/en/health-canada/services/environmental-workplace-health/reports-publications/environmental-contaminants/fourth-report-human-biomonitoring-environmental-chemicals-canada.html. [2022-10-21].
- 11.World Health Organization. WHO guidance to reduce illness due to lead exposure. 2021. https://www.who.int/news/item/27-10-2021-who-guidance-to-reduce-illness-due-to-lead-exposure. [2022-12-1].