

Abstract
Background:
A traumatic arteriovenous fistula of the scalp due to hair transplantation (AVFHT) is a rare fistulous communication between branches of the arteries and draining veins in the scalp’s subcutaneous tissue. Its incidence is unknown and its clinical manifestations may range from a pulsatile mass to seldom epilepsy. Surgery and interventional approaches (percutaneous and endovascular embolization) using coils and embolic agents such as Onyx have been used as treatment options. The authors report a rare case of an AVFHT successfully treated through percutaneous and endovascular embolization using coils and precipitating hydrophobic injectable liquid (PHIL) embolic agent. This is possibly the first reported case using PHIL embolic agent to treat an AVFHT.
Case Description:
The patient presented with a painful and disabling scalp swelling in the right parieto-occipital region 2 years after a hair transplant in 2011. A computed tomography angiography showed an arteriovenous fistula between branches of the right superficial temporal artery and branches of the right occipital artery to the right superficial temporal vein that was successfully embolized using coils and PHIL. The patient was discharged after a smooth recovery and 1 month later remained healthy.
Conclusion:
Percutaneous and endovascular embolization using PHIL embolic agent can be an alternative treatment for AVFHT.
Keywords: Angiography, Arteriovenous fistula, Intervention, Liquid embolic material, Precipitating hydrophobic injectable liquid

INTRODUCTION
An arteriovenous fistula of the scalp (misnomered cirsoid aneurysm) is a rare fistulous communication between branches of the external carotid artery and draining veins in the scalp’s subcutaneous tissue.
Its clinical manifestations range from a painful deforming pulsatile mass (94%), headaches (25%), and tinnitus (20%) to even seldom epilepsy.[6]
They account for 8.1% of all arteriovenous malformations; nevertheless, their exact incidence is unknown. Although predominantly spontaneous (60.2%), they also may occur secondary to trauma or iatrogeny, like secondary to hair transplantation procedures.[1,6]
Traumatic arteriovenous fistulas of the scalp due to hair transplantation (AVFHT) are extremely rare; by 2019, only 15 cases were reported in the literature, of which only five were treated exclusively with vascular or direct puncture embolization using coils and onyx; however, no case reported the usage of precipitating hydrophobic injectable liquid (PHIL) embolic agent.[3]
PHIL is a new embolic agent approved by the Food and Drug Administration for treating arteriovenous malformations and hypervascular lesions. Its use for AVFHT has not been well established.
Hereby, we report a case of an AVFHT successfully treated using coils and PHIL embolic agent.
CASE DESCRIPTION
A 50-year-old male presented scalp swelling in the right parieto-occipital region 2 years after a hair transplant in 2011 that was initially conservatively treated. The swelling progressively enlarged and became painful and disabling. In 2021, a computed tomography angiography showed subcutaneous right parieto-occipital dilated vessels representing an arteriovenous fistula between parietal branches of the right superficial temporal artery and branches of the right occipital artery to the right superficial temporal vein [Figure 1]. Due to the diagnostic imaging findings and clinical course of the disease, the patient was diagnosed with AVFHT.
Figure 1:
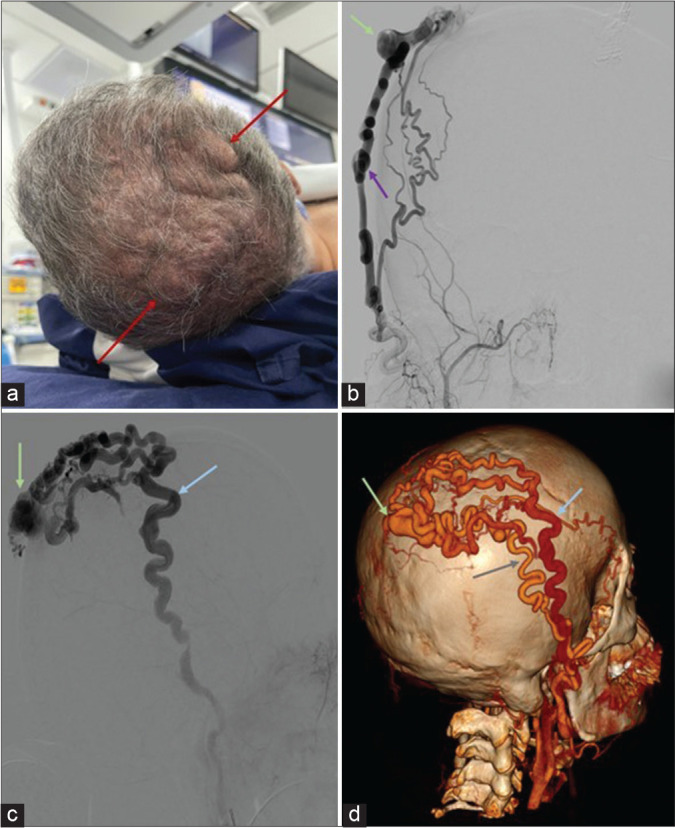
(a) Multiple subcutaneous right parieto-occipital dilated vessels (red arrows). (b) Arterial phase angiography showing feeders from the right occipital artery (purple arrow) to the arteriovenous fistula (green arrow). (c) Venous phase angiography showing the arteriovenous fistula (green arrow) and dilated right superficial temporal vein (blue arrow). (d) Volume rendering reconstruction showing the arteriovenous fistula (green arrow), superficial temporal artery (grey arrow), and dilated superficial temporal vein (blue arrow).
The fistula was embolized using coils and PHIL liquid embolic fluid through micro-catheter direct percutaneous puncture; additionally, proximal right superficial temporal and occipital arteries selective embolizations with coils were carried out, achieving occlusion of the fistula and afferent arteries [Figure 2]. One month later, the patient remains healthy.
Figure 2:

(a) Resolution of dilated vessels on physical examination (red arrow). (b) Volume rendering reconstruction showing the embolization materials in the fistula, right occipital, and right superficial temporal arteries (green arrows).
DISCUSSION
Although hair transplantation using the punch-graft technique is considered safe and effective, remaining a popular cosmetic treatment, as more than 1.2 billion people suffer from baldness, AVFHT can be a rare complication of this procedure when both an artery and vein are damaged.[2]
Most AVFHT reported cases show the malformation originating from the superficial temporal artery, less commonly from the occipital artery or both, as in our case.[3]
Surgery has been the mainstay of treatment for AVFHT, with low recurrence; nevertheless, endovascular approaches using several embolic agents such as Onyx embolic fluid and coils have also been used as an alternative single treatment option or associated with surgical treatment.[2,4] Surgical resection of large lesions can be complicated with considerable bleeding and require reconstructive skin procedures; therefore, endovascular embolization is becoming increasingly popular.[2,4]
PHIL has advantages over other embolic agents used to treat AVFHT. It is delivered in pre-filled syringes that do not require shaking before its use, making its administration faster. It is also pale in color, reducing the risk of skin staining, characteristic of Onyx; moreover, iodine is covalently bonded in PHIL, leading to less glare artifact on computed tomography. In superficial arteriovenous malformations, PHIL also has deeper penetration with its different concentrations, achieving embolization of the nidus and arterial feeders when approaching from the venous side, making it a potentially safe and helpful embolic agent when treating AVFHTs, like in our case.[5]
We used endovascular approaches (percutaneous puncture and transarterial approaches), utilizing PHIL and coils to treat our patient. No procedure-related complications and no symptoms recurred during follow-up. We strongly encourage reporting more cases like ours to strengthen the available evidence in the literature on the use of PHIL as an embolizing agent to treat AVFHTs.
CONCLUSION
Percutaneous and endovascular embolization using PHIL embolic agent can be an alternative treatment for AVFHT.
Footnotes
How to cite this article: Quiroz Alfaro AJ, Herrera Ortíz AF, Mejia JA, Cardona Ortegon JD, Gutierrez LC, Dussan Tovar CA, et al. Traumatic scalp arteriovenous fistula post capillary implantation successfully treated using PHIL embolic agent. Surg Neurol Int 2023;14:12.
Contributor Information
Alejandro José Quiroz Alfaro, Email: alejandro.quiroz@urosario.edu.co.
Andrés Felipe Herrera Ortíz, Email: afherreraor@gmail.com.
Juan Andres Mejia, Email: juanandresmejia@gmail.com.
Jose David Cardona Ortegon, Email: josecaor@unisabana.edu.co.
Laura Camila Gutierrez, Email: lauracami13.gutierrez@gmail.com.
Catalina Andrea Dussan Tovar, Email: doctor.dussan@gmail.com.
Miguel Zarate, Email: zaratemiguel4@gmail.com.
Sebastian Ramiro Gil-Quiñones, Email: sgil9602@gmail.com.
Marlon Yesid Barrera Montañez, Email: marlonbarreramont@gmail.com.
Lorena Fernández Beaujon, Email: lorefebe@gmail.com.
Orlando Manuel Diaz Daza, Email: odiaz@houstonmethodist.org.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
REFERENCES
- 1.Bernstein J, Podnos S, Leavitt M. Arteriovenous fistula following hair transplantation. Dermatol Surg. 2011;37:873–5. doi: 10.1111/j.1524-4725.2011.02027.x. [DOI] [PubMed] [Google Scholar]
- 2.Dabus G, Pizzolato R, Lin E, Kreusch A, Linfante I. Endovascular treatment for traumatic scalp arteriovenous fistulas: Results with Onyx embolization. J Neurointerv Surg. 2014;6:405–8. doi: 10.1136/neurintsurg-2013-010724. [DOI] [PubMed] [Google Scholar]
- 3.Liounakos JI, Urakov T, Snelling B, Peterson EC. Scalp arteriovenous fistula following hair transplantation: A case report and review of the literature. Clin Med Rev Case Rep. 2018;5:200. [Google Scholar]
- 4.Perez-Meza D, Niedbalski R. Complications in hair restoration surgery. Oral Maxillofac Surg Clin North Am. 2009;21:119–48. vii. doi: 10.1016/j.coms.2008.10.010. [DOI] [PubMed] [Google Scholar]
- 5.Prashar A, Butt S, Shaida N. Introducing PHIL (precipitating hydrophobic injectable liquid)-a new embolic agent for the body interventional radiologist. Diagn Interv Radiol. 2020;26:140–2. doi: 10.5152/dir.2019.19063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sofela A, Osunronbi T, Hettige S. Scalp Cirsoid aneurysms: Case illustration and systematic review of literature. Neurosurgery. 2020;86:E98–107. doi: 10.1093/neuros/nyz303. [DOI] [PubMed] [Google Scholar]