

ABSTRACT
Objective:
to identify, in the scientific literature, the defining characteristics and contributing factors (related factors, associated conditions and populations at risk) for nursing diagnosis decreased cardiac output.
Method:
an integrative literature review, conducted between September and October 2020, with an update in March 2022, in the MEDLINE via PubMed, LILACS, SciELO, CINAHL and EMBASE databases. Using acronym PEO, studies published in the last 10 years in Portuguese, English and Spanish were included. A descriptive analysis was carried out to present the elements mapped in the literature.
Results:
analysis of 31 articles identified different elements, highlighting 4 new related factors: hyperglycemic stress, prone position, left lateral position, sleep deprivation. Individuals with a history of cardiovascular disease and males were identified as possible populations at risk.
Final considerations:
the elements for decreased cardiac output, identified in the literature, add evidence that justifies the permanence of this diagnosis in the NANDA-I classification.
Descriptors: Cardiac Output, Nursing Diagnosis, Review, Evidence-Based Nursing, Standardized Nursing Terminology
RESUMO
Objetivo:
identificar, na literatura científica, as características definidoras e fatores contribuintes (fatores relacionados, condições associadas e populações em risco) para o diagnóstico de enfermagem débito cardíaco diminuído.
Método:
revisão integrativa da literatura, conduzida entre setembro e outubro de 2020, com atualização em março de 2022, nas bases de dados MEDLINE via PubMed, LILACS, SciELO, CINAHL e EMBASE. Com uso do acrônimo PEO, foram incluídos estudos publicados nos últimos 10 anos em português, inglês e espanhol. Realizouse análise descritiva para apresentar os elementos mapeados na literatura.
Resultados:
análise de 31 artigos identificou diferentes elementos, com destaque para 4 novos fatores relacionados: estresse hiperglicêmico, posição prona, posição lateral esquerda, privação do sono. Indivíduos com história de doença cardiovascular e do sexo masculino foram apontados como possíveis populações em risco.
Considerações finais:
os elementos para débito cardíaco diminuído, identificados na literatura, agregam evidências que justificam a permanência desse diagnóstico na classificação da NANDA-I.
Descritores: Débito Cardíaco, Diagnóstico de Enfermagem, Revisão, Enfermagem Baseada em Evidência, Terminologia Padronizada em Enfermagem
RESUMEN
Objetivo:
identificar, en la literatura científica, las características definidoras y los factores contribuyentes (factores relacionados, condiciones asociadas y poblaciones de riesgo) para el diagnóstico de enfermería de gasto cardíaco disminuido.
Método:
revisión integrativa de la literatura, realizada entre septiembrey octubre de 2020, con actualización en marzo de 2022, en las bases de datos MEDLINE vía PubMed, LILACS, SciELO, CINAHL y EMBASE. Utilizando la sigla PEO, se incluyeron estudios publicados en los últimos 10 años en portugués, inglés y español. Se realizó un análisis descriptivo para presentar los elementos mapeados en la literatura.
Resultados:
el análisis de 31 artículos identificó diferentes elementos, con énfasis en 4 nuevos factores relacionados: estrés hiperglucémico, posición prona, posición lateral izquierda, privación del sueño. Las personas con antecedentes de enfermedad cardiovascular y los hombres se identificaron como posibles poblaciones en riesgo.
Consideraciones finales:
los elementos para gasto cardíaco disminuido, identificados en la literatura, suman evidencias que justifican la permanencia de este diagnóstico en la clasificación NANDA-I.
Descriptores: Gasto Cardíaco, Diagnóstico de Enfermería, Revisión, Enfermería Basada em la Evidencia, Terminología Normalizada de Enfermería
INTRODUCTION
Standardized language systems in nursing organize the vocabulary scope of concepts and elements related to the phenomena that nurses must identify, treat and assess in health care(1). In the clinical setting, changes in the capacity of the blood volume required for circulation, called cardiac output(2), can produce signs and symptoms resulting from hypoperfusion that are of special interest to nursing.
Decreased cardiac output (DCO) (00029) is a nursing diagnosis (ND) from NANDA International, Inc. (NANDA-I)(3), defined as “an inadequate volume of blood pumped by the heart to meet the metabolic demands of the body”. It is contained in the Activity/Rest domain and has 36 defining characteristics (DC), divided into five groups: altered heart rate/rhythm, altered preload, altered afterload, altered contractility, behavioral/emotional(3). By DC, we understand the set of observable clues or inferences that are grouped as manifestations of an ND. As for associated conditions (conditions not modifiable by a nurse), six are described for DCO: altered contractility, altered heart rate, altered afterload, altered preload, altered heart rhythm and altered stroke volume(3).
Although DCO has been present in the classification since 1975 and has already been the focus of conceptual research regarding its pertinence in the field of nursing(4), to date, previous studies have not identified antecedent elements that show a causal relationship with this human response, called related factors (RF), and that are subject to modification by independent nursing interventions(3). It is also observed that, although DCO is often identified in people with cardiovascular diseases, especially heart failure(5), its diagnostic structure does not include a description of populations at risk, which are defined as a group of people who share common characteristics and who, due to such characteristics, are more susceptible to certain human responses(3).
NANDA-I(3) is the only classification that presents well-defined criteria regarding validity evidence levels of ND present in its structure, defined so far as level of evidence (LoE). Therefore, each ND must present a set of evidence (theoretical and clinical) that allow its correct interpretation, from a set of manifestations for certain clinical contexts(3). In this context, DCO does not present the minimum level of evidence required by NANDA-I to justify its permanence in the classification, and its withdrawal is suggested in the next edition 2024-2026.
Therefore, DCO refinement from the literature allows identifying possible contributing factors (RF, associated conditions, populations at risk) that explain the causal dynamics of this ND as well as the characterization of its occurrence in the scenarios in which it has been identified. In addition to aggregating the evidence necessary for DCO to remain in NANDA-I classification, such information will assist in the clinical reasoning and decision-making of nurses, providing evidence that explains the cause-effect relationships of this ND, which may reflect a greater degree of accuracy in the process of identifying this human response in the clinical context.
OBJECTIVE
To identify, in scientific literature, the DC and contributing factors (RF, associated conditions, and populations at risk) for ND DCO.
METHODS
Ethical aspects
This study was carried out in public domain databases, which does not require submission to a Research Ethics Committee.
Study design
This is an integrative literature review(6), developed in six stages: theme identification; guiding question selection; inclusion and exclusion criteria establishment; definition of the information to be extracted from selected studies; assessment of included studies; and interpretation of results.
Study protocol
To meet the purposes of this review, the following guiding question was used: what are the DC resulting from DCO and what are the possible contributing factors (RF, associated conditions and populations at risk) for the occurrence of this phenomenon? The formulation of the question considered an adaptation of acronym PEO(7), as: P (Population of interest) = general population; E (Exposure of interest) = DC, RF, associated conditions and populations at risk; and O (Outcome) = DCO occurrence.
Data collection took place between September and October 2020, with an update in March 2022, with searches in the electronic databases: MEDLINE via PubMed, Latin American and Caribbean Literature in Health Sciences (LILACS), Cumulative Indexto Nursing and Allied Health Literature (CINAHL), EMBASE and SciELO. The Descriptors in Health Sciences (DeCS), Medical Subject Heading (MeSH), CINAHL and Emtree titles for EMBASE were used. The search strategy followed the criteria of each database with Boolean operators AND and OR, crossed between controlled and uncontrolled descriptors, followed by NOT to exclude studies related to the risk of DCO.
In each base, two strategies were used for a more detailed understanding of the phenomenon of interest(6). In the broad strategy, the objective was to rescue studies that presented possible new elements that precede (contributing factors) or that are a consequence (DC) of the presence of the DCO phenomenon, without the use of descriptors related to nursing. In the restricted strategy, the objective was to rescue studies directly related to DCO, in order to verify how this diagnosis has been presented in nursing and in which contexts and populations (Chart 1). Moreover, the references present in the articles identified and selected by the search strategy were also consulted.
Chart 1. Search strategy used in the databases, Brazil, 2022.
| Controlled descriptors | Uncontrolled descriptors | |
|---|---|---|
| Strategy 1 (broad) | Cardiac Output [MeSH Terms]; Cardiac Output, Low [MeSH Terms]; cardiac output, decreased [Título CINAHAL];‘heart output’ [emtree]; Débito Cardíaco [DeCS]; Baixo Débito Cardíaco [DeCS] | decreased; risk; diminuído; risco |
| Strategy 2 (restricted) | Cardiac Output [MeSH Terms]; Cardiac Output, Low [MeSH Terms]; cardiac output, decreased [Título CINAHAL]; Débito Cardíaco [DeCS]; Baixo Débito Cardíaco [DeCS]; ‘heart output’ [emtree]; NANDA Nursing Diagnoses [Título CINAHAL];‘nursing diagnosis’ [emtree] | decreased; risk; diminuído; risco; nursing diagnos*; Diagnósticos de Enfermagem |
Studies published in the last 10 years were included, without restriction of sample size, in English, Portuguese and Spanish. The time frame is justified by the volume of articles retrieved not related to the scope of this review, such as articles on validation of techniques and/or equipment for measuring cardiac output at the bedside, in addition to experimental studies with animals. Review studies, case studies, textbooks, editorials, protocols, diagnostic performance studies, studies that did not directly describe DCO and studies in which there was no significant and/or explained reduction in cardiac output were also excluded.
Eligible studies were retrieved on the same day to avoid bias as the databases are updated daily. To eliminate possible duplicate articles and speed up the initial screening of the data, the results were loaded into Rayyan® software, which uses a reliable semi-automation process, incorporating a high level of usability and efficiency into the analysis process(8). The results were analyzed blindly and independently by two researchers, graduate students with research in the field of cardiology and nursing diagnoses, and disagreements were resolved by consensus with a third researcher.
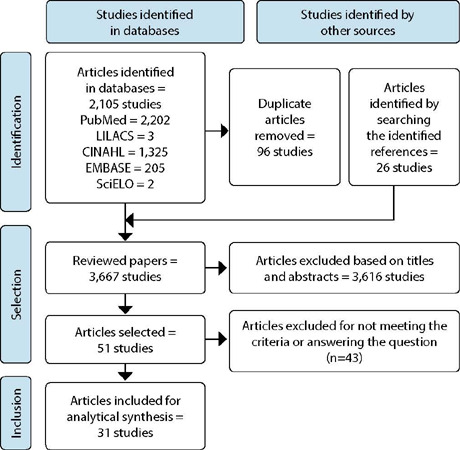
Finally, 51 studies were selected for full reading, of which 31 made up the final sample, as shown in Figure 1, following the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) recommendations(9).
Figure 1. Flowchart of the stages of search and selection of analyzed articles, Brazil, 2022.
Data analysis
The information from the selected articles was organized in a Microsoft Office Excel spreadsheet (2019), containing the essential items of each study: bibliographic data, study objectives, methodological design, sample size and characteristics, DC and possible contributing factors to DCO.
The cross-mapping technique(10) was applied between the terms found in the literature and the elements contained in the NANDA-I for DCO, in order to look for possible similarities. In this process, the following steps were adopted: a) verify semantic equivalence between terms in the literature and terms in NANDA-I for DCO; b) verify the conceptual equivalence between terms in the literature and terms in NANDA-I for DCO; c) highlight terms not matching DCO as possible new DC and contributing factors; d) verify in NANDA-I whether the possible new terms are already described for other diagnoses, considering the standardization of terms in taxonomic structure.
Furthermore, the publications were qualified according to the level of scientific evidence proposed by Fineout-Overholt(11), considering the criteria adopted in this study: level II - evidence derived from at least one well-designed randomized controlled clinical trial; level III - evidence obtained from well-designed clinical trials without randomization; level IV - evidence from well-designed cohort and case-control studies; level VI - evidence derived from a single descriptive or qualitative study.
Data analysis and presentation were performed descriptively. The results were synthesized and grouped in synoptic tables, distributed from the DC and the possible contributing factors to DCO, coded in chronological order (S1, S2,…).
RESULTS
Chart 2 presents a summary of the characterization process and assessment of the level of evidence of selected studies.
Chart 2. Characterization of selected studies using the selection flowchart (N=31), Brazil, 2022.
| Study | Author, year, and country | Design | Objective | LoE | Context | DCO |
|---|---|---|---|---|---|---|
| S1(12) | Garan et al., (2010) - USA | Retrospective longitudinal | Investigate whether peripheral vascular compensatory mechanisms are preserved after orthotopic heart transplantation. | IV | 36 medical records of hospitalized patients in 38 months | Phenomenon |
| S2(13) | Paganin et al., (2010) - Brazil | Cross-sectional | Map the Nursing Interventions Classification interventions with the most prevalent NDs in the first 24 hours of patient admission to the Intensive Care Unit. | VI | 150 medical records of hospitalized individuals | ND |
| S3(14) | Paganin et al., (2010) - Brazil | Cross-sectional | Identify the main ND established in an Intensive Care Unit and compare them between clinical and surgical patients. | VI | 150 medical records of hospitalized individuals | ND |
| S4(15) | Martins, Aliti, Rabelo (2010) - Brazil | Cross-sectional | Validate DCO in patients with decompensated HF hospitalized in Intensive and Emergency Care Units. | VI | 29 hospitalized patients | ND |
| S5(16) | Alessandra, Silla, Marilisia (2011) - Italy | Cross-sectional | Describe the use of nursing terminology in care plans provided to patients in a cardiology rehabilitation unit. | VI | 76 outpatient patients | ND |
| S6(17) | Aliti etal., (2011) - Brazil | Cross-sectional | Identify the signs and symptoms to infer the main ND in patients with decompensated HF. | VI | 303 hospitalized patients | ND |
| S7(18) | Bodetofta et al., (2011) - Sweden | Randomized clinical trial | Check whether inhaling oxygen decreases cardiac output and blood flow. | II | 16 healthy volunteers | Phenomenon |
| S8(19) | Pereira et al., (2011) - Brazil | Cross-sectional | Identify the frequency of ND and DC in patients with cardiovascular diseases and characterize them in terms of sociodemographic and clinical variables. | VI | 30 hospitalized patients | ND |
| S9(20) | Scherb et al., (2011) - USA | Multicentric comparative | Compare the ten most frequent diagnoses, interventions and nursing outcomes in patients hospitalized for HF. | VI | 302 medical records of hospitalized patients | ND |
| S10(21) | Matos et al., (2012) - Brazil | Cross-sectional | Assess the prevalence of DC and to analyze which are the predictive factors of DCO in patients with HF undergoing assessment for heart transplantation. | VI | 38 hospitalized patients using Pulmonary Artery Catheter | ND |
| S11(22) | Kyhl et al., (2013) - Denmark | Non-randomized clinical study | Check whether positive pressure ventilation reduces cardiac output. | III | 18 healthy volunteers | Phenomenon |
| S12(23) | Wajima et al., (2013) - Japan | Randomized clinical trial | Identify and compare hemodynamic parameters for probable hypotension during patient commuting to bed after different types of anesthesia (general, epidural or spinal combined with general). | II | 69 patients hospitalized in the immediate postoperative period of elective surgery | Phenomenon |
| S13(24) | Hargens et al., (2015) - USA | Randomized clinical trial | Determine whether resting hemodynamic variables are altered in individuals with OSA entering cardiac rehabilitation compared to those without apnea. | II | 73 individuals in outpatient cardiac rehabilitation | Phenomenon |
| S14(25) | Kasai et al., (2015) - Canada | Non-randomized clinical trial | Investigate whether, in patients with HF, those with OSA have greater reductions in stroke volume and cardiac output and whether these decreases are proportional to the severity of OSA. | III | 60 outpatient patients | Phenomenon |
| S15(26) | Li et al., (2015) - China | Case-control study | Investigate total peripheral vascular resistance, cardiac output and natriuretic peptide levels in children with PTS during supine, orthostatic and return to supine positions. | IV | 29 children with PTS in the case group and 32 controls | Phenomenon |
| S16(27) | Ma et al., (2015) - USA | Longitudinal | Assess the short-term cardiovascular response to prone position in neonates in neonatal intensive care. | IV | 30 neonates hospitalized for 10 minutes | Phenomenon |
| S17(28) | Souza et al., (2015) - Brazil | Cross-sectional | Assess the clinical usefulness of operational definitions for DC DCO, excessive fluid volume and impaired activity tolerance, and the concomitant presence of these diagnoses in patients with HF decompensation. | VI | 25 hospitalized patients | ND |
| S18(29) | Chikhani et al., (2016) - England | Non-randomized clinical study | Investigate the effect of prone position using surgical pads on hepatic blood flow and cardiovascular behavior in healthy subjects. | III | 10 healthy volunteers | Phenomenon |
| 519(30) | Costa, Linch, Souza (2016) - Brazil | Cross-sectional | Identify the main signs and symptoms of patients with heart disease admitted to an intensive cardiac care unit and infer the main ND. | VI | 77 medical records of hospitalized individuals | ND |
| S20(31) | Galvão et al., (2016) - Brazil | Cross-sectional | Identify priority NDs for patients with decompensated HF admitted to a cardiology emergency room at a university hospital. | VI | 62 hospitalized patients | ND |
| S21(32) | Pereira et al., (2016) -Brazil | Longitudinal | Identify the ND fatigue, DCO and activity intolerance and verify the association of DD with the respective ND in patients hospitalized with HF. | IV | 72 patients followed up during three weeks of hospitalization | ND |
| S22(33) | Sánchez et al., (2016) - Colombia | Cross-sectional | Determine the clinical and construct validity of ND DCO in patients with HF. | VI | 200 hospitalized patients | ND |
| S23(34) | Yang et aI., (2016) - China | Randomized clinical trial | Explore the effects of stress hyperglycemia on cardiac function and prognosis in critically ill intensive care patients. | II | 80 hospitalized patients | Phenomenon |
| S24(35) | Miró et al., (2017) - Italy | Non-randomized clinical study | Investigate changes in left ventricular systolic function due to thoracic epidural anesthesia and changes in hemodynamic variables and left ventricular diastolic function in patients undergoing major abdominal surgery. | III | 24 hospitalized without significant heart disease | Phenomenon |
| S25(36) | Paviotti, Todero, Demarini (2017) - Italy | Longitudinal | Verify the short-term effects of the left lateral position on the cardiovascular parameters of hemodynamically stable newborns. | IV | 32 neonates hospitalized for 10 minutes | Phenomenon |
| S26(37) | Nederend et al., (2018) - Netherlands | Randomized clinical trial | Assess cardiac autonomic nervous system activity and cardiac function in children after aortic coarctation repair and investigate the relationship between the two. | II | 31 outpatient patients | Phenomenon |
| S27(38) | Slomko et al., (2018) - Poland | Randomized clinical trial | Analyze the impact of sleep deprivation on hemodynamic and autonomic parameters in subjects with normal blood pressure, compared with prehypertension and hypertension, at 24, 28 and 32 hours of total sleep deprivation. | II | 30 healthy volunteers | Phenomenon |
| S28(39) | Stewart et al., (2018) - USA | Case-control study | Investigate whether postural hyperventilation is one of the causes of PTS and whether there is associated hyperventilation when there is a reduction in cardiac output. | IV | 58 cases with PTS and 16 healthy controls | Phenomenon |
| S29(40) | Ribeiro et al., (2019) - Brazil | Cross-sectional | Assess ND Frail Elderly Syndrome in older adults with chronic diseases in a health district in the Federal District. | VI | 78 community older adults | ND |
| S30(41) | Zhang et al., (2021) - China | Case-control study | Analyze the associations of cardiac function with inflammatory cytokines, oxidative stress and anemia in patients with uremia. | IV | 43 patients in uremia in the case group and 36 patients in the control group | Phenomenon |
| S31(42) | Perry et al.,(2021)- England | Longitudinal | Describe hemodynamic differences in women with gestational hypertension. | IV | 717 pregnant women followed up during 77 months | Phenomenon |
S - study; LoE - level of evidence; ND - Nursing Diagnosis(s); HF - heart failure; DCO - Decreased Cardiac Output; OSA - obstructive sleep apnea; PTS - Postural Tachycardia Syndrome.
Of the 31 studies analyzed in the review, 17 (55%)(12, 18, 22-27, 29, 34-39, 41) referred to the DCO phenomenon, and 14 (45%)(13-17, 19-21, 28, 30-33,40), to DCO. The studies were mostly carried out in countries in South America (n=12;38%)(13-15, 17, 19, 21, 28, 30-33, 40) and in Europe (n=9;29%)(16, 18, 22, 29, 35-38, 42), with emphasis on Brazilian publications (n=11; 35%)(13-15, 17, 19, 21, 28, 30-32, 40), that were exclusively related to DCO. In publications related to ND, which aimed to identify its occurrence in an isolated way (n=3;21%)(15, 21, 33) or together with other diagnoses (n=i11.79%)(13-14, 16-17, 19-20, 28, 30-32, 40), the breadth in the prevalence estimates is highlighted, which ranged from 6.7%(13-14) to 100%(15-16, 28, 33).
Despite the heterogeneity of the population profiles and methodological designs, the studies showed similarities that they were carried out with samples of people with cardiovascular disorders, such as heart failure (HF) (n=11;35%)(15, 17, 19-21, 25, 28, 31-33, 40), hypertension (n=7;22%)(16, 19, 28-29, 38, 40, 42) or with a history of acute myocardial infarction (n=4; 13%)(16, 24, 30, 40). In addition, males were highlighted as having the highest composition among the samples (n=10;32%)(14-15, 17, 24-25, 28, 31-33, 35). As for the level of evidence, level VI was the most frequent (n=13;42%)(13-17, 19-21, 28, 30-31, 33, 40), followed by level IV studies (n=8;26%)(12, 26-27, 32, 36, 39, 41-42).
Regarding the studies that presented the DC currently described in NANDA-I for DCO, edema (13, 15, 17, 19, 21, 28, 30, 32-33, 40) was the most frequent in the literature (n=10;71%) Jugular vein distension (15, 17, 19, 28, 32-33), dyspnea(15, 17, 19, 30, 32-33) and fatigue (13, 15, 19, 28, 32-33) were present in six publications (43%) each. Other studies have pointed out abnormal skin color (13, 15, 28, 32-33) and decreased ejection fraction (17, 21, 28, 32-33)(n=5; 36%), in addition to clammy skin (13, 15, 28, 33) and presence of S3 heart sound (21, 28, 32-33) (n=4;29%). Bradycardia (21, 30, 33), nocturnal paroxysmal dyspnea (15, 17, 33) heart palpitations (15, 33, 40) altered blood pressure (28, 33, 40) orthopnea (15, 17, 33), tachycardia (21, 30, 33), prolonged capillary refill (13, 28, 33) and cough (15, 28, 33)were presented in three studies (21%) each.
Other DC also described in NANDA-I for DCO were cited with lower prevalence. Electrocardiogram change (13, 28), psychomotor agitation (28, 30), anxiety (28, 30), weight gain (15, 33), decreased peripheral pulses (28, 33), increased central venous pressure (15, 21), presence of S4 heart sound (28, 33), adventitious breath sounds (15, 33) and oliguria (15, 28) were present in two studies (14%) each. Increased pulmonary artery occlusion pressure (21), decreased central venous pressure (21), increased pulmonary vascular resistance (21), decreased pulmonary vascular resistance (21) and increased systemic vascular resistance (21) were cited in one study (7%) each.
The following DC of DCO present in NANDA-I were not found in this review: decreased pulmonary artery occlusion pressure, heart murmur, decreased systemic vascular resistance, decreased cardiac index, decreased stroke volume index, and decreased left ventricular stroke work index. Moreover, some of the DC that were identified in the literature are not present in the structure of DCO, although they are part of other NANDA-I diagnoses, such as arrhythmias (13, 28, 32-33), ascites (28), hepatomegaly (15), restlessness (13), positive hepatojugular reflex (28), altered mental status (28) and altered breathing pattern (28). No new DC were observed other than those already present in the classification.
Regarding associated conditions currently described in NANDA-I for DCO, altered contractility (13, 31), altered heart rate (13, 31) and altered stroke volume (13, 31) were identified in two studies (14%). Still, altered heart rate (31) and altered postload (13) were also cited in one study (7%) each. Finally, the contributing factors (RF, associated conditions and populations at risk) identified in the literature and that did not correspond to DCO in NANDA-I are grouped in Table 1.
Table 1. Possible new contributing factors for diagnosis decreased cardiac output, Brazil, 2022.
| Possible new related factors | Studies |
|---|---|
| Hyperglycemic stress | S23(34) |
| Prone position | S16(27);S18(29) |
| Left side position | S25(36) |
| Sleep deprivation | S27(38) |
| Possible new associated conditions | |
|---|---|
| Obstructive sleep apnea | S13(24); S14(25) |
| Coarctation of the aorta | S26(37) |
| Gestational hypertension | S31(42) |
| Anesthetic procedure | S24(35) |
| Postural tachycardia syndrome | S15(26); S28(39) |
| Transplantation | S1(12) |
| Oxygen therapy | S7(18) |
| Uremia | S30(41) |
| Positive pressure ventilation | S11(22) |
| Possible new populations at risk | |
|---|---|
| Individuals with a history of cardiovascular disease | S4(15); S5(16); S6(17); S8(19); S9(20); S10(21); S13(24); S14(25); S17(28); S19(30); S20(31); S21(32); S22(33); S27(38); S29(38); S31(42) |
| Male | S3(14); S4(15); S6(17); S13(24); S14(25); S17(28); S20(31); S21(32); S22(33); S24(35) |
DISCUSSION
The results of this review allowed the answer to the proposed guiding question, corroborating the main DC representative of DCO already described in NANDA-I(3), as well as the identification of possible new contributing factors to this ND, with emphasis on four RF that can be independently modified by a nurse: hyperglycemic stress (34), prone position (27, 29), left side position (36) and sleep deprivation (38).
The highest prevalence of studies in this review was those conducted in South American countries, which demonstrate their potential for research, despite being developing countries with limitations in the process of translation of evidence(43). This reinforces what is advocated by NANDA-I as an international entity regarding the need for studies on ND in different care contexts, in order to generate evidence for clinical and population validation(44).
Despite previous questions about the independence of DCO as a specific and non-collaborative phenomenon with other subjects(4, 5), the high frequency of studies in nursing(13-17, 19-21, 28, 30-33, 40) suggests that there is a lot of interest in this phenomenon, since it has been described in different practice scenarios, with potential for interventions and positive health outcomes from the specific management of nursing.
Regarding the level of evidence of specific investigations on DCO, the studies that presented DC were mostly cross-sectional and focused on the prevalence of this diagnosis. Although crucial for clinical and social validity in specific subgroups, advances are needed in conducting diagnostic studies focusing on the predictive and prognostic capacity of these DC for further submission to NANDA-I(3, 45).
The group of DC already described in NANDA-I(3), as consequences of changes in preload, were the most frequent, especially edema, fatigue and jugular vein distension. Edema is a sign of HF, as it represents the deficit of the right ventricle in ejecting the entire amount of blood from the venous circulation, leading to increased hydrostatic pressure in the organs and capillaries(2). Fatigue results from inadequate distribution of oxygenated volume by reduced output and inadequate excretion of the products of metabolism. Jugular vein distension reflects the increases in pressure and volume in the right atrium(2, 46).
Regarding contractility, decreased ejection fraction is a result of the amount of blood available in the left ventricle between systole and diastole, being an important characteristic for the classification of HF(47) On the other hand, nocturnal paroxysmal dyspnea occurs due to the addition of daytime fluids that, at night, can return to the blood circulation, causing accumulation in the pulmonary alveoli, reduced gas exchange and increased carbon dioxide, with consequent awakening by patients(2, 46).
In the altered postload group, dyspnea and abnormal skin color stood out. Dyspnea can occur with minimal or moderate activities, being an important predictor of HF severity(46), indispensable for clinical nursing care to people with cardiovascular alterations. In addition to this, abnormal skin color represented by cyaniasis or skin pallor are initial signs of tissue hypoperfusion(48).
Altered heart rate/rhythm was identified by bradycardia, tachycardia and heart palpitations. Bradycardia appears as a result of exhaustion of the heart muscle in generating output. As a consequence, reduced stroke volume can activate the sympathetic nervous system and increase heart rate, generating tachycardia and heart palpitations (2, 46). It is emphasized that DC electrocardiogram change does not describe which alterations should be considered. The reformulation of this characteristic would be relevant for its better understanding and identification in clinical practice.
Finally, behavioral alterations were the least identified in the literature, with anxiety and psychomotor agitation. Both can be identified in a more severe spectrum of DCO, since low output alters cerebral perfusion, creating a vicious cycle of worsening concomitantly with dyspnea (2, 46).
In general, the evidence about the DC extracted from the literature supports the permanence of DCO in NANDA-I classification(3) as a phenomenon identified and researched in different scenarios, adding the minimum necessary evidence. However, when considering the current structure presented in the classification, in which DC are grouped into subleveis and named by components similar to those presented in the associated conditions, this can make it difficult to understand their elements. A restructuring, for example, at different levels of severity, could facilitate the explanation and relationship between diagnostic components.
Consistently, the most frequent DC for DCO indicated in the literature are initial changes in debt that are not restricted to intensive care environments, justifying their applicability to different clinical contexts. For its correct identification, DCO requires a solid training of nurses, which requires transversality of knowledge, which translates into skills for the physical examination, ability to use and interpret diagnostic support technologies and analysis of functional patterns for the applicability of knowledge to nursing.
Although NANDA-I presents DC obtained by direct measurement of DC, which can be identified from the presence of a pulmonary artery catheter installed in individuals (considered the gold standard), advances in clinical and interventional cardiology have prioritized non-invasive or minimally invasive measurement, with a focus on patient safety(46, 48).
The installation of invasive hemodynamic monitoring measures depends on the indication by the medical team beyond patients’ clinical spectrum of severity. These may be justifications for the low frequency or even absence of some of the DC that correspond to measurements necessarily obtained by a pulmonary artery catheter. The non-observation of these signs in the literature points to the need for reformulation or inclusion of new parameters obtained by minimally invasive measures, since they are not being identified in clinical practice, as previously observed in a systematic review of the DC of DCO(5). Furthermore, in the study conducted by Matos et al.(21), increased pulmonary artery occlusion pressure, increased central venous pressure, decreased central venous pressure, and decreased pulmonary vascular resistance did not increase the chances of diagnosis occurring.
There are some DC rescued in the literature that are already present in NANDA-I classification(3), but described in other diagnoses, such as excessive fluid volume. Such signs and symptoms are derived from cardiac congestion due to pump failure and reduced output, with consequent accumulation in body fluid volume, as is the case with HF(47). For this situation, studies of differential analysis can contribute to the identification of DC specific to correlated phenomena(45). In the case of DC arrhythmias, this appears to be a granularity of electrocardiogram change. Studies that develop conceptual and operational definitions are especially useful to help with such impasses.
The studies that identified possible RF or associated conditions are the result of methodological designs with a higher level of evidence, which allow the attribution of cause and effect, representing the second highest frequency found. Studies with greater methodological robustness are needed to add validity of specific causes to DCO, being encouraged to better clarify the relationships between its antecedent elements.
Regarding the possible RF, the presence of hyperglycemic stress (34), prone position (27, 29), left lateral position (36) and sleep deprivation stand out(38) as subject to independent interventions by nurses, with nursing outcomes and interventions available in the Nursing Outcomes Classification (NOC)(49) and Nursing Interventions Classification (NIC)(50).
Patients who present hyperglycemic stress, in intensive care, secondary to trauma, infections, major surgeries, among other causes, present significant changes in hemodynamic parameters, such as reduced cardiac output, as a result of worsening cardiac function. This fact may be due to the reduction in muscle strength and myocardial energy capacity after failure in compensatory mechanisms(34). Interventions for hyperglycemia management (2120) and nutritional therapy (1120) can manage these cases(50).
The reduction in cardiac output from positioning patients in prone position (27, 29) or left lateral position (36) is a direct result of the increase in intrathoracic pressure, which generates a reduction in venous return and consequent reduction in systolic volume(27, 29, 36). Nursing activities related to positioning (0840) can avoid such complications(50).
Periods of sleep deprivation can increase the dominance of the sympathetic nervous system in the body, linking pathophysiological mechanisms of blood pressure control centers, with a consequent reduction in cardiac output(38). Both sleep disorder and sleep deprivation are ND described in NANDA-I that are common in the hospital environment(3). Sleep enhancement (1850) may contribute to the resolution of this agent(50).
Associated conditions already available in NANDA-I and which are related to DCO were rarely mentioned in the included studies, in addition to altered preload, which was not verified in the literature, which confirms the need to review this diagnostic element. The addition of associated conditions identified from this literature review can improve the clinical reasoning of nurses in clinical practice, with the investigation of initial signs and symptoms in specific contexts., with emphasis on obstructive sleep apnea (24-25) and postural tachycardia syndrome (26, 39), which contribute to observable changes in nursing assessment.
Finally, according to the findings of this review, individuals with a history of cardiovascular disease and males are likely to be populations at risk for DCO, sharing common characteristics related to heart pump failure, in addition to being frequent demographic profiles in the clinical investigation contexts observed in this review.
Study limitations
The limitation of time for the search for publications, as well as the search strategies used, are a characteristic limitation of this study design, since there may be other publications outside the stipulated period.
Contributions to nursing
The deepening of DCO knowledge, based on scientific evidence that supports these phenomena, allows the proposal to refine this ND in NANDA-I classification, promoting the strengthening of this diagnostic classification and the advancement of nursing knowledge. In addition, it contributes to better decision-making in the search for better health outcomes, which affects the qualification of clinical practice.
FINAL CONSIDERATIONS
This study made it possible to identify DC and contributing factors for the DCO present in the literature, adding evidence that justifies its permanence in NANDA-I classification, especially by verifying causal factors that are subject to intervention and independent treatment by nursing.
As it is a complex phenomenon, future investigations on the diagnostic concept are necessary for a better understanding of its essential attributes, with a view to solving possible impasses regarding its definition and its constitutive elements that help its identification by practice nurses. It is suggested that, based on these results, new studies of clinical-causal validation and clinical construct are carried out, to strengthen evidence about DCO with higher levels of evidence, especially in non-intensive care settings.
Footnotes
FUNDING
Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - (CAPES).
REFERENCES
- 1.Zhang T, Wu X, Peng G, Zhang Q, Chen L, Cai Z, et al. Effectiveness of standardized nursing terminologies for nursing practice and healthcare outcomes: a systematic review. Int J Nurs Knowl. 2021;32:220–228. doi: 10.1111/2047-3095.12315. [DOI] [PubMed] [Google Scholar]
- 2.Perpetua E, Keegan P. Cardiac Nursing. 7. Philadelphia: Wolters Kluwer Health; 2021. pp. 700–700. [Google Scholar]
- 3.Herdman TH, Kamitsuru S, Lopes CT. Diagnósticos de Enfermagem da NANDA-I: Definições e Classificação 2021-2023. 12. Porto Alegre: Artmed; 2021. pp. 544–544. [Google Scholar]
- 4.Dougherty CM. Reconceptualization of the nursing diagnosis decreased cardiac output. Int J Nurs Terminol Classif. 1997;8:29–36. doi: 10.1111/j.1744-618X.1997.tb00129.x. [DOI] [PubMed] [Google Scholar]
- 5.Souza V, Zeitoun SS, Barros ALBL. Débito cardíaco diminuído: revisão sistemática das características definidoras. Acta Paul Enferm. 2011;24:114–119. doi: 10.1590/S0103-21002011000100017. [DOI] [Google Scholar]
- 6.Toronto CE. In: A step-by-step guide to conducting an integrative review. Toronto C, Remington R, editors. Cham: Springer; 2020. Overview of the integrative review; pp. 1–9. [DOI] [Google Scholar]
- 7.Moola S, Munn Z, Sears K, Sfetcu R, Currie M, Lisy K, et al. Conducting systematic reviews of association (etiology) Int J Evid Based Healthc. 2015;13:163–169. doi: 10.1097/XEB.0000000000000064. [DOI] [PubMed] [Google Scholar]
- 8.Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan: a web and mobile app for systematic reviews. Syst Rev. 2016;5:210–210. doi: 10.1186/s13643-016-0384-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ [Internet] 2021;372(71) doi: 10.1136/bmj.n71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Delaney C, Moorhead S. Synthesis of Methods, Rules, and Issues of Standardizing Nursing Intervention Language Mapping. Int J Nurs Terminol Classif [Internet] 1997;8:152–156. doi: 10.1111/j.1744-618X.1997.tb00471.x. [DOI] [PubMed] [Google Scholar]
- 11.Melnyk BM, Fineout-Overholt E. Evidence-based practiice in nursing and healthcare: a guide to best practice. 4. Wolters Kluwer; 2019. pp. 658–658. [Google Scholar]
- 12.Garan AR, Uriel N, Sayer G, Sims D, Zahner D, Farr M, et al. Alteration in systemic vascular resistance and cardiac output during acute cellular rejection and recovery in heart transplant recipients. J Hear Lung Transplant. 2010;29:382–384. doi: 10.1016/j.healun.2009.08.015. [DOI] [PubMed] [Google Scholar]
- 13.Paganin A, Souza EN, Azzolin K, Rabelo ER. Nursing interventions implemented according to the most prevalent nursing diagnoses in intensive care: cross-sectional study. Online Braz J Nurs. 2010;9:1–16. doi: 10.5935/1676-4285.20103143. [DOI] [Google Scholar]
- 14.Paganin A, Menegat P, Klafke T, Lazzarotto A, Fachinelli TS, Chaves IC, et al. Implantação do diagnóstico de enfermagem em unidade de terapia intensiva: uma análise periódica. Rev Gaúcha Enferm. 2010;31:307–313. doi: 10.1590/S1983-14472010000200015. [DOI] [PubMed] [Google Scholar]
- 15.Martins QCS, Aliti G, Rabelo ER. Decreased cardiac output: clinical validation in patients with decompensated heart failure. Int J Nurs Terminol Classif. 2010;21:156–165. doi: 10.1111/j.1744-618X.2010.01161.x. [DOI] [PubMed] [Google Scholar]
- 16.Alessandra Z, Silla A, Marilisa C. A Retrospective Study of Nursing Diagnoses, Outcomes, and Interventions for Patients Admitted to a Cardiology Rehabilitation Unit. Int J Nurs Terminol Classif [Internet] 2011;22:148–156. doi: 10.1111/j.1744-618X.2011.01184.x. [DOI] [PubMed] [Google Scholar]
- 17.Aliti GB, Linhares JCC, Linch GFC, Ruschel KB, Rabelo ER. Sinais e sintomas de pacientes com insuficiência cardíaca descompensada: inferência dos diagnósticos de enfermagem prioritários. Rev Gaúcha Enferm. 2011;32:590–595. doi: 10.1590/S1983-14472011000300022. [DOI] [PubMed] [Google Scholar]
- 18.Bodetoft S, Carlsson M, Arheden H, Ekelund U. Effects of oxygen inhalation on cardiac output, coronary blood flow and oxygen delivery in healthy individuals, assessed with MRI. Eur J Emerg Med. 2011;18:25–30. doi: 10.1097/MEJ.0b013e32833a295e. [DOI] [PubMed] [Google Scholar]
- 19.Pereira JMV, Cavalcanti ACD, Santana RF, Cassiano KM, Queluci GC, Guimarães TCF. Diagnósticos de enfermagem de pacientes hospitalizados com doenças cardiovasculares. Esc Anna Nery. 2011;15:737–745. doi: 10.1590/S1414-81452011000400012. [DOI] [Google Scholar]
- 20.Scherb CA, Head BJ, Maas ML, Swanson EA, Moorhead S, Reed D, et al. Most frequent nursing diagnoses, nursing interventions, and nursing-sensitive patient outcomes of hospitalized older adults with heart failure: part 1. Int J Nurs Terminol Classif. 2011;22:13–22. doi: 10.1111/j.1744-618X.2010.01164.x. [DOI] [PubMed] [Google Scholar]
- 21.Matos LN, Guimarães TCF, Brandão MAG, Santoro DC. Prevalence of nursing diagnosis of decreased cardiac output and the predictive value of defining characteristics in patients under evaluation for heart transplant. Rev Latino-Am Enfermagem. 2012;20:307–315. doi: 10.1590/S0104-11692012000200013. [DOI] [PubMed] [Google Scholar]
- 22.Kyhl K, Ahtarovski KA, Iversen K, Thomsen C, Vejlstrup N, Engstrøm T, et al. The decrease of cardiac chamber volumes and output during positive-pressure ventilation. Am J Physiol Circ Physiol. 2013;305:H1004–H1009. doi: 10.1152/ajpheart.00309.2013. [DOI] [PubMed] [Google Scholar]
- 23.Wajima Z, Shiga T, Imanaga K, Inoue T. Vigilance of hemodynamic changes immediately after transferring patients is crucial. J Anesth. 2013;27:521–527. doi: 10.1007/s00540-013-1568-x. [DOI] [PubMed] [Google Scholar]
- 24.Hargens TA, Aron A, Newsome LJ, Austin JL, Shafer BM. Effects of obstructive sleep apnea on hemodynamic parameters in patients entering cardiac rehabilitation. J Cardiopulm Rehabil Prev. 2015;35:181–185. doi: 10.1097/HCR.0000000000000102. [DOI] [PubMed] [Google Scholar]
- 25.Kasai T, Yumino D, Redolfi S, Su M, Ruttanaumpawan P, Mak S, et al. Overnight effects of obstructive sleep apnea and its treatment on stroke volume in patients with heart failure. Can J Cardiol. 2015;31:832–838. doi: 10.1016/j.cjca.2015.01.001. [DOI] [PubMed] [Google Scholar]
- 26.Li H, Han Z, Chen S, Liao Y, Wang Y, Liu P, et al. Total peripheral vascular resistance, cardiac output, and plasma c-type natriuretic peptide level in children with postural tachycardia syndrome. J Pediatr [Internet] 2015;166:1385–1389.:e2. doi: 10.1016/j.jpeds.2015.03.032. [DOI] [PubMed] [Google Scholar]
- 27.Ma M, Noori S, Maarek JM, Holschneider DP, Rubinstein EH, Seri I. Prone positioning decreases cardiac output and increases systemic vascular resistance in neonates. J Perinatol. 2015;35:424–427. doi: 10.1038/jp.2014.230. [DOI] [PubMed] [Google Scholar]
- 28.Souza V, Salloum Zeitoun S, Lopes CT, Oliveira APD, Lima Lopes J, Barros ALBL. Clinical usefulness of the definitions for defining characteristics of activity intolerance, excess fluid volume and decreased cardiac output in decompensated heart failure: a descriptive exploratory study. J Clin Nurs. 2015;24:2478–2487. doi: 10.1111/jocn.12832. [DOI] [PubMed] [Google Scholar]
- 29.Chikhani M, Evans DL, Blatcher AW, Jackson AP, Guha IN, Aithal GP, et al. The effect of prone positioning with surgical bolsters on liver blood flow in healthy volunteers. Anaesthesia. 2016;71:550–555. doi: 10.1111/anae.13416. [DOI] [PubMed] [Google Scholar]
- 30.Costa C, Linch GFC, Souza EN. Nursing diagnosis based on signs and symptoms of patients with heart disease. Int J Nurs Knowl. 2016;27:210–214. doi: 10.1111/2047-3095.12132. https://doi.org/ 10.1111/2047-3095.12132 . [DOI] [PubMed] [Google Scholar]
- 31.Galvão PCDC, Gomes ET, Figueirêdo TR, Bezerra SMMS. Diagnósticos de enfermagem aplicados a pacientes com insuficiência cardíaca descompensada. Cogitare Enferm. 2016;21:1–8. doi: 10.5380/ce.v21i2.44646. [DOI] [Google Scholar]
- 32.Pereira JMV, Flores PVP, Figueiredo LS, Arruda CS, Cassiano KM, Vieira GCA, et al. Nursing Diagnoses of hospitalized patients with heart failure: a longitudinal study. Rev Esc Enferm USP. 2016;50:929–936. doi: 10.1590/s0080-623420160000700008. [DOI] [PubMed] [Google Scholar]
- 33.Rojas Sánchez LZ, Hernández Vargas JA, Trujillo Cáceres SJ, Roa Díaz ZM, Jurado Arenales AM, Toloza Pérez YG. Usefulness of the Diagnosis “Decreased Cardiac Output (00029)” in Patients With Chronic Heart Failure. Int J Nurs Knowl. 2017;28:192–188. doi: 10.1111/2047-3095.12148. [DOI] [PubMed] [Google Scholar]
- 34.Yang J, Wu F, Li H, Yue Y. Effects of stress hyperglycemia on cardiac function and prognosis in critical patients of ICU. Int J Clin Exp Med[lnternet] 2016;9(6):12025–12031. [cited 2022 Apr 21] Available from: http://www.ijcem.com/files/ijcem0024047.pdf . [Google Scholar]
- 35.Miró M, Sanfilippo F, Pérez F, Del Valle SG, Gómez-Arnau Jl. Influence of the thoracic epidural anesthesia on the left ventricular function: an echocardiographic study. Minerva Anestesiol. 2017;83:695–704. doi: 10.23736/s0375-9393.16.11582-2. [DOI] [PubMed] [Google Scholar]
- 36.Paviotti G, Todero S, Demarini S. Cardiac output decreases and systemic vascular resistance increases in newborns placed in the left-lateral position. J Perinatol. 2017;37:563–565. doi: 10.1038/jp.2016.251. [DOI] [PubMed] [Google Scholar]
- 37.Nederend I, Geus EJC, Kroft LJM, Westenberg JJM, Blom NA, Harkel ADJ. Cardiac autonomic nervous system activity and cardiac function in children after coarctation repair. Ann Thorac Surg. 2018;105:1803–1808. doi: 10.1016/j.athoracsur.2018.01.084. [DOI] [PubMed] [Google Scholar]
- 38.Stomko J, Zawadka-Kunikowska M, Kujawski S, Klawe JJ, Tafil-Klawe M, Newton JL, et al. Do changes in hemodynamic parameters depend upon length of sleep deprivation? comparison between subjects with normal blood pressure, prehypertension, and hypertension. Front Physiol. 2018;9:1–10. doi: 10.3389/fphys.2018.01374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Stewart JM, Medow MS, Sutton R, Visintainer P, Jardine DL, Wieling W. Mechanisms of Vasovagal Syncope in the Young: Reduced Systemic Vascular Resistance Versus Reduced Cardiac Output. J Am Heart Assoc. 2017;6:1–11. doi: 10.1161/JAHA.116.004417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Ribeiro IA, Lima LR, Volpe CRG, Funghetto SS, Rehem TCMSB, Stival MM. Frailty syndrome in the elderly in elderly with chronic diseases in Primary Care. Rev Esc Enferm USP. 2019;53:1–9. doi: 10.1590/s1980-220x2018002603449. [DOI] [PubMed] [Google Scholar]
- 41.Zhang H, Fan L, Liao H, Tu L, Zhang J, Xu D, et al. Correlations of cardiac function with inflammation, oxidative stress and anemia in patients with uremia. Exp Ther Med [Internet] 2021;21:250–250. doi: 10.3892/etm.2021.9681. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Perry H, Binder J, Gutierrez J, Thilaganathan B, Khalil A. Maternal haemodynamic function differs in pre-eclampsia when it is associated with a small-for-gestational-age newborn: a prospective cohort study. BJOG An Int J Obstet Gynaecol. 2021;128:167–175. doi: 10.1111/1471-0528.16269. [DOI] [PubMed] [Google Scholar]
- 43.Tucker S, McNett M, Melnyk BM, Hanrahan K, Hunter SC, Kim B, et al. Implementation science: application of evidence-based practice models to improve healthcare quality. Worldviews Evidence-Based Nurs. 2021;18:76–84. doi: 10.1111/wvn.12495. [DOI] [PubMed] [Google Scholar]
- 44.Rabelo-Silva ER, Mantovani VM, Pedraza LL, Cardoso PC, Lopes CT, Herdman TH. International collaboration and new research evidence on Nanda International Terminology. Int J Nurs Knowl. 2021;32:103–107. doi: 10.1111/2047-3095.12300. [DOI] [PubMed] [Google Scholar]
- 45.Lopes MVO, Silva VM. In: PRONANDA: Programa de atualização em diagnósticos de enfermagem. Herdman TH, Napoleão AA, Silva VM, editors. Porto Alegre: Artmed; 2016. Métodos avançados de validação de diagnósticos de enfermagem; pp. 31–74. [Google Scholar]
- 46.Huang SJ. Measuring cardiac output at the bedside. Curr Opin Crit Care. 2019;25:266–272. doi: 10.1097/MCC.0000000000000599. [DOI] [PubMed] [Google Scholar]
- 47.Bozkurt B, Coats AJ, Tsutsui H, Abdelhamid M, Adamopoulos S, Albert N, et al. Universal Definition and Classification of Heart Failure. J Card Fail [Internet] 2021;27:387–413. doi: 10.1016/j.cardfail.2021.01.022. [DOI] [PubMed] [Google Scholar]
- 48.Kobe J, Mishra N, Arya V, Al-Moustadi W, Nates W, Kumar B. Cardiac output monitoring: technology and choice. Ann Card Anaesth. 2019;22:6–6. doi: 10.4103/aca.ACA_41_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Moorhead S, Johnson M, Maas ML, Swanson E. Classificação dos resultados de enfermagem (NOC) 6. Rio de Janeiro: Elsevier; 2020. pp. 608–608. [Google Scholar]
- 50.Bulechek GM, Butcher HK, Dochterman JM, Wagner CM. Classificação das intervenções em enfermagem (NIC) 7. Rio de Janeiro: Elsevier; 2020. pp. 440–440. [Google Scholar]