

Abstract
In 1974, the United States established the Safe Drinking Water Act (SDWA) to protect consumers from potential exposure to drinking water contaminants associated with health risks. Each contaminant is assigned a health-based standard meant to reflect the maximum level at which an adverse human health outcome is unlikely; measurements beyond that level have greater potential to result in adverse health outcomes. Although there is extensive research on human health implications following water contaminant exposure, few studies have specifically examined associations between fetal health and municipal drinking water violations. Therefore, the objective of this study is to assess whether SDWA drinking water violations are associated with fetal health outcomes, including preterm birth (PTB), low birth weight (LBW), and term-low birth weight (tLBW), in the Commonwealth of Virginia.
Singleton births (n=665,984) occurring between 2007 and 2015 in Virginia were geocoded and assigned to a corresponding estimated water service area. Health-based (HB) and monitoring and reporting (MR) violations for 12 contaminants were acquired from the US EPA Safe Drinking Water Information System, with exposure defined at the approximate service area level to limit exposure misclassification. A logistic regression model for each birth outcome assessed potential relationships with SDWA violations.
When examining the association between individual MR violations and birth outcomes, Nitrate-Nitrite (OR=1.10; 95% CI= 1.02, 1.18, P=0.01) was positively associated with PTB and the total coliform rule was negatively associated with tLBW (OR=0.93; 95% CI= 0.87, 1.00, P=0.04). These findings indicate that a lack of regular monitoring and reporting by water providers (resulting in monitoring and reporting violations) may be concealing health-based violations as these health concerns cannot be revealed without testing, suggesting a need for additional technical, managerial, and financial support to enable often-underfunded water systems to adhere to monitoring and reporting requirements meant to protect public health.
Keywords: medical geography, environmental health, spatial epidemiology, water quality, birth outcomes, nitrate, nitrite, total coliform
1. Introduction
According to the World Health Organization, half of the world’s population will be living in water-stressed areas by 2025 (WHO, 2019). As of 2019, 2.2 billion people globally are without access to safe drinking water (WHO, 2019), and water scarcity is only projected to grow as global population increases. Worldwide, 842,000 deaths are attributed to unsafe drinking water, sanitation, and hygiene every year (WHO, 2019). Lack of clean drinking water can lead to increases in cholera, typhoid, hepatitis A, dysentery, diarrhea, and polio (WHO, 2019). Significant reductions in these deaths are possible with access to clean drinking water. In addition to the presence of infectious agents associated with gastrointestinal disease, both chronic and acute exposure to metals and organic toxins in water can also affect human health (e.g., lead and neurotoxicity), although the impacts of chronic exposures are often less well-established (US EPA, 2022; Srivastav et al., 2020).
Given the wide variety of potential harmful exposures vectored by water, as well as documented associations between waterborne exposures and complications related to pregnancy, it can be hypothesized that water quality influences the health of a gestating infant (Edwards, 2013; Cao et al., 2016, Sherris et al., 2021, Aschengrau et al., 2020, Blaisdell et al., 2019). Past research documenting potential relationships between drinking water quality and birth outcomes is available but limited. Bove et al. (1996) examined the effects of maternal ingestion of trihalomethanes and disinfection byproducts on birth outcomes in four counties in northern New Jersey. Water quality measurements were assessed at the tap level and results indicated that total trihalomethane (TTHM) levels in drinking water greater than 100 ppb are associated with term-low birth weight (tLBW) (Bove et al., 1996). Dodds et al. (1999) examined the effects of TTHM in drinking water on adverse birth outcomes in Nova Scotia, Canada and found an association between TTHM levels and an elevated risk for stillbirth but did not find an association with birth weight or gestational age (Dodds et al., 1999). Yang et al. (2003) compared birth outcomes within areas with and without arsenic contaminated drinking water in Taiwan and found that arsenic was associated with low birth weight (LBW).
Recent interest in potential connections between birth outcomes and waterborne exposures in the United States has emerged. Hill and Ma (2022) found increased risks to infant health associated with contaminated drinking water stemming from shale gas activity in Pennsylvania. Hill and DiSalvo (2019) examined chemical contaminant violations and birth outcomes in Pennsylvania and found adverse effects at conditions below EPA drinking water standards. Wang et al. (2021) examined birth outcomes in the context of the Flint, Michigan water and found an increased frequency of LBW infants. This previous work supports the need for continued examinations of the impacts of municipal water quality on birth outcomes. A serious constraint on past investigations of the impact of any chronic or acute drinking water exposures on consumer health is the complexity of drinking water consumption patterns, and the lack of publicly available data on household water sources. A recent systematic review by McDonald et al (2022) determined that over half of the states in the US do not have any available delineations of municipal service areas; of those 24 states with delineated boundaries, the majority are incomplete. The authors note that this seriously limits the ability to monitor health impacts and emergent environmental justice concerns within large portions of the US, as available delineations often poorly represent minoritized and rural areas.
The present effort investigates potential relationships between birth outcomes and water quality through application of unique dataset approximating service areas for the entire state of Virginia (Marcillo et al. 2021), which at present lacks any publicly available delineations of water system service areas (McDonald et al. 2022). Exploring potential relationships at the approximated community water system service area level likely reduces exposure misclassification that may exist solely when county boundaries are used. An improved understanding of how drinking water violations potentially impact birth outcomes will assist health officials, drinking water program staff, and policy makers as they work to improve and refine implementation of national drinking water quality standards and public health protection. Therefore, this work examines the following research questions:
Does an association exist between SDWA violations (monitoring and reporting and/or health-based) and adverse birth outcomes within water service areas in Virginia?
If there is an association between violations and adverse birth outcomes in Virginia, where can drinking water program agencies focus their attention to decrease incidence of adverse birth outcomes?
The first research question regarding the presence of an association between water contaminant violations and adverse birth outcomes will be answered through logistic regression to determine whether the target contaminants are associated with the response variable (i.e., preterm birth (PTB), LBW, tLBW). To determine specific regions of concern within Virginia we will evaluate which contaminant violations significantly impact the response variables and where those violations occur.
2. Background
Contaminants of Interest
Past studies suggest that a variety of contaminants, ranging from chemical to microbial, may affect human health and birth outcomes (see table 1). The SDWA currently establishes health-based drinking water standards (i.e., maximum contaminant levels (MCLs), treatment techniques, and maximum residual disinfection limits (MRDL)) for over 90 contaminants. The MCLs enforced by the Environmental Protection Agency (EPA) are meant to reflect the maximum level that limits the risk of human health impacts, but also may reflect the realities of available treatment technology. This study considers two violation types: health-based (HB) and monitoring and reporting (MR). HB violations are issued when a contaminant exceeds its corresponding MCL or when a system fails to follow minimum treatment technique requirements to reduce the contaminant. When a system fails to evaluate water samples, or submit monitoring results, a MR violation is issued.
Table 1:
Summary of literature reviewed by contaminant.
| Contaminant Type | Contaminant | Associated Studies | Findings |
|---|---|---|---|
| Chemical Contaminants | Arsenic | Claus Henn et al., 2016; Almberg et al., 2017; Yang et al., 2003, Ahmad et al. 2001; Huang et al., 2018 | Maternal exposure is associated with LBW and PTB. |
| Atrazine | Rinsky et al., 2012; Almberg et al., 2018 | Exposure increases the risk for PTB and tLBW. | |
| Lead | Ugwuja et al., 2011 | Contaminated drinking water correlated with LBW. | |
| Nitrate | Huang et al., 2018; Sherris et al., 2021; Stayner et al., 2017 | Increased risk for PTB. Increased risk for very PTB and very LBW at concentrations below EPA drinking water standards. | |
| Radionuclides | Radon | Langlois et al., 2016 | Increased prevalence of Down syndrome, cleft lip, and cystic hygroma/lymphangioma when exposed to high levels. |
| Uranium and Radium | Cech et al., 2007 | Elevated levels in drinking water are associated with an increased prevalence of orofacial birth defects. | |
| Microbial and Disinfectant Byproducts | Total Trihalomethanes | Toledano et al., 2005; Bove et al., 1995; Gallagher et al., 1998; Hwang et al., 2003; Yang et al. 2007; Cao et al., 2016 | Excess risk of LBW and very LBW when exposed to high concentrations; Maternal exposure is associated with LBW, tLBW and PTB. |
| Haloacetic Acids | Hinckley et al., 2005 | Increased exposure is associated with tLBW. | |
| Fecal Indicator Bacteria (FIB | Mahande et al., 2016; Jones et al., 2004 | Pregnant women who had amebiasis, caused by a gastrointestinal parasite, were 79% more likely to have a preterm birth; Exposure to FIB during the third trimester of pregnancy developed into E. coli sepsis, leading to the preterm rupture of the amniotic sac. |
Both source water type (e.g., surface vs groundwater) and system size (i.e., number of customers served) can play a role in a public water systems (PWSs) compliance, potentially influencing the likelihood of a violation (Allaire et al., 2018). In general, MR violations are issued more frequently than HB violations, with smaller systems more likely to struggle with compliance (Marcillo & Krometis, 2019; US EPA, 2013). Marcillo and Krometis (2019) found that very small (< 500 people) community water systems in Virginia had more MR violations than large systems; medium systems had more MCL violations. Similarly, the US EPA (2013) noted in the national public water systems compliance report that small PWSs have more occurrences of noncompliance than larger systems. Previous studies posit that lack of resources and staffing constraints may impact a system’s ability to comply with SDWA regulations, potentially contributing to the higher occurrences of monitoring and reporting violations (Fu et al., 2020; Marcillo & Krometis, 2019).
3. Data and Methods
Public Water System Data
PWS data for the Commonwealth of Virginia from 2007 to 2015 was obtained from the Safe Drinking Water Information System (SDWIS) database, which is a publicly available database containing information on all PWS in the United States. From SDWIS, the water system detail and violation report datasets were used. The following variables were acquired from the dataset: PWS ID and name, PWS type, counties and cities served, number of violations per year, rule name, violation type, contaminant name, and date. PWSs that were active in 2016 when the SDWIS data was extracted were included in the analysis. Note that the system had to be active at one point during the study period but did not have to remain active for the entirety of the study period. Only rule and contaminant violations that occurred during the study period and in one of the 662 geocoded service areas were included in the analysis. The following rules were analyzed: Arsenic, Total Coliform Rule, Lead and Copper Rule, Stage 1 Disinfectant Byproduct Rule (DBPR), and Stage 2 DBPR. To parse out rules containing many contaminants (i.e., synthetic organic compound rule, volatile organic compound rule, radionuclide rule, and ground water rule) the following contaminants were analyzed rather than their corresponding rule: atrazine, E. coli in source water, Combined Radium, Combined Uranium, Gross Alpha Excluding Radon and Uranium, Gross Alpha including Radon and Uranium, and Nitrate-Nitrite. Contaminants under the Stage 1 and Stage 2 DBPRs were not analyzed individually due to some systems not specifying contaminant type when a stage 1 or stage 2 DBPR violation was issued.
Service areas for 662 community water systems (CWSs), of all sizes, were estimated by Marcillo et al. (2021), see figure 1, by assigning populations to CWS based on proximity to the system and population served. Zip codes were utilized to determine proximity to CWS, and zip codes closest to a CWS were assigned to the corresponding system until the population that the system served was fully assigned. As previously mentioned, service area delineations are not publicly available for Virginia (McDonald et al., 2022). While the boundaries used here are estimates, and so do present a potential source of exposure misclassification, they allow for a finer scale examination of the research questions as opposed to the utilization of county boundaries, which are often used as approximations in similar work (Ahern et al., 2011). Individuals are more likely to be correctly matched to their water provider with the use of our approximated service area boundaries than with the use of county boundaries, which have no meaningful relationship with an individual’s water provider.
Figure 1:
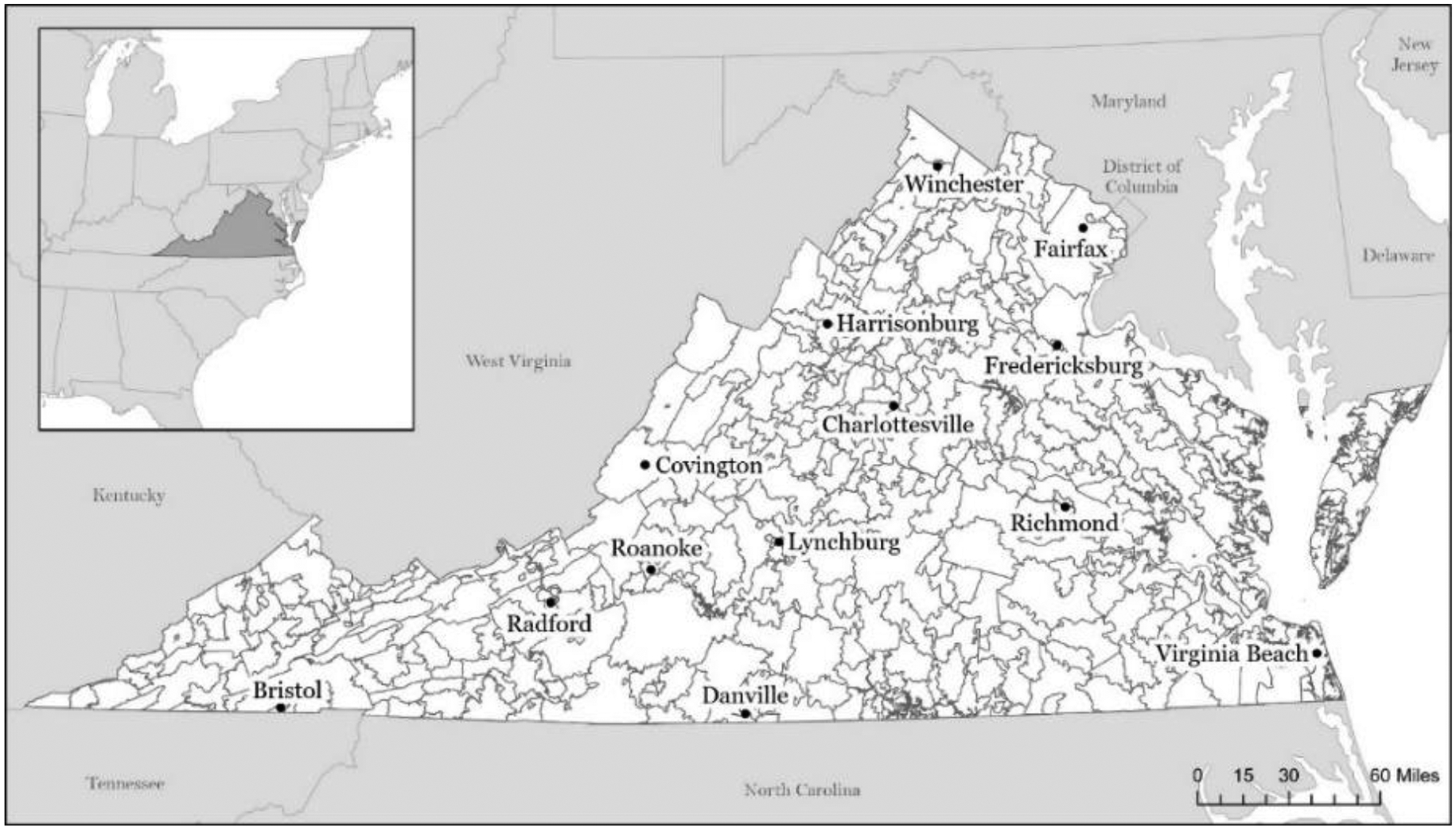
Estimated service area boundaries in Virginia.
Birth Outcome Data
Virginia birth records (n=876,797) from 2007 to 2015 were acquired for the Commonwealth of Virginia from the Virginia Department of Health (VDH). All data analyses were conducted according to protocols to protect confidentiality approved by Virginia Tech IRB (VT IRB #17-1190) and Virginia Department of Health IRB (VDH IRB #40221). The following information was acquired from the birth records: mother’s address, mother’s demographics (age, race, education, if mother is of Hispanic origin), child’s information (weight, gestational length, sex), parity, plurality, payment (Medicaid, private insurance, self-pay, unknown), and tobacco use during pregnancy (see table 3).
Table 3:
Characteristics of births before and after data processing.
| Characteristic | Original Sample Size, n = 876,797, n (%) | Final Sample Size, n = 665,984, n (%) |
|---|---|---|
| Infant Sex | ||
| M | 448211 (51.1) | 340984 (51.2) |
| F | 428558 (48.9) | 325000 (48.8) |
| Invalid | 28 (<.01) | - |
| Mother’s Hispanic Origin | ||
| Hispanic | 115077 (13.1) | 85350 (12.8) |
| Not Hispanic | 760514 (86.7) | 579768 (87.1) |
| Unknown | 1206 (0.1) | 866 (0.1) |
| Race | ||
| White | 571357 (65.2) | 443636 (66.6) |
| Black | 191904 (21.9) | 137113 (20.6) |
| Other | 90457 (10.3) | 85235 (12.8) |
| Invalid | 23079 (2.63) | - |
| Mother’s Age | ||
| 18–35 | 749553 (85.5) | 566007 (85.0) |
| <18 | 15275 (1.7) | 11892 (1.7) |
| >35 | 111967 (12.8) | 88085 (13.3) |
| Invalid | 2 (<.01) | - |
| Mother’s Education | ||
| Some secondary schooling1 | 353652 (40.3) | 261089 (39.2) |
| Some college or college degree | 512906 (58.5) | 397793 (59.7) |
| Unknown | 10239 (1.2) | 7102 (1.1) |
| Payment | ||
| Medicaid | 257833 (29.4) | 186697 (28.0) |
| Private Insurance | 559417 (63.8) | 436281 (65.5) |
| Self-Pay | 47074 (5.4) | 34078 (5.1) |
| Unknown | 12473 (1.4) | 8928 (1.3) |
| Tobacco | ||
| No | 765000 (87.2) | 581151 (87.3) |
| Yes | 50841 (5.8) | 37282 (5.6) |
| Unknown | 60956 (7.0) | 47551 (7.1) |
| Parity | ||
| 1 | 366136 (41.8) | 279594 (42) |
| 2 | 282246 (32.2) | 215172 (32.3) |
| 3 | 140107 (16.0) | 105930 (15.9) |
| 4 or more | 88096 (10.0) | 65288 (9.8) |
| Invalid | 212 (<.01) | - |
Includes high school diploma or GED
Data Processing
For birth records, exposure period was classified by the majority gestational year. To determine majority gestational year, the gestational age and birth date were used to estimate the midpoint of the gestational period (Ruktanonchai et al., 2022; Buttling et al., 2021). The majority gestational year was assigned to the year in which the midpoint occurred. The use of majority gestational year allowed us to match the exposure and birth outcome more closely in time; a birth that occurs in January would therefore be matched with data in the previous year when most exposure during pregnancy would have occurred instead of the year in which the birth took place. Birth records were examined to determine gestational length and birthweight to identify PTB, LBW, and tLBW, which were generated as follows: PTB= <37 weeks of pregnancy, LBW= <2500 grams, tLBW= <2500 grams and ≥37 weeks of pregnancy (von Ehrenstein et al., 2013; WHO, n.d.). Each outcome was given a binary (i.e., 0 or 1) classification. During the study period, the original birth record coding structure changed for self-reported (typically mother reported) fields for race, payment, and education. A new coding structure was created to ensure consistency between the years and prepare the following covariates to be entered into the regression model: mother’s age, race, education, if mother is of Hispanic origin, tobacco use during pregnancy (yes/no), infant’s sex, payment, and parity/birth order. For the race variable, self-reported mother’s race was only recorded for half of the study period. When mother’s race was unavailable, the recorded child’s race was used. Plural births have an increased risk of PTB, LBW, morbidity and perinatal mortality (Warner et al., 2000); thus, they were removed from the analysis, and the study only included singleton births. Birth records with any of the following were removed from the study: incomplete street address, P.O. box address, unknown gestational age, and unknown birth weight (see figure 2), resulting in a final sample size of 665,984. Birth records with complete addresses were geocoded using Esri’s 2013 StreetMap dataset (see table 2).
Figure 2:

Data processing for individual birth records within Virginia. 168,899 birth records were removed due to inability to geocode, this included those with missing, incorrect, or postal office box addresses. 31,702 records were removed due to being a plural birth.
Table 2:
The percentage of geocoded matched street addresses. Match scores range between 85 and 100, with a minimum match score of 85.
| Match Score (%) | Number of Addresses | % of Addresses |
|---|---|---|
| 100 | 588,760 | 87.0% |
| 90 – 99 | 49,966 | 7.4% |
| ≤ 89 | 35,898 | 5.3% |
| Tied1 | 1,816 | 0.27% |
| Total 676,440 |
Tied addresses were reviewed before matching.
To reduce the risk of exposure misclassification compared to studies conducted at the county scale, approximated service areas were used as the unit of analysis for this study. SDWA violations were aggregated at the service area level and were then categorized into (0) having no violations in a service area or (1) having one or more violations during each year. Quantities of violations were not considered due to inconsistencies in sampling frequency between individual water systems. Monitoring frequency varies for each contaminant rule and can also vary due to factors such as system size, water source, or prior violations (EPA, 2020). Each birth record was joined spatially to its corresponding service area and paired to violations that occurred during the majority gestation year for analysis.
Statistical Analyses
Statistical analyses were conducted to determine if an association exists between adverse birth outcomes and water contaminant violations while controlling for covariates. The violations of interest include rules and contaminants regulated by the EPA that have the potential to impact birth outcomes and that occurred at one of the 662 geocoded service areas during the study period. MR and HB violations were examined separately using a logistic regression model for each birth outcome (PTB, LBW, tLBW), for a total of six models. To understand the relationship between the outcome of interest and SDWA violations, odds ratios and confidence intervals (CI) at 95% were calculated to determine significance. All analyses were completed using JMP statistical software.
4. Results
Out of the 665,984 births that were analyzed, 51,261 were PTB (7.7%), 40,638 were LBW (6.1%), and 14,052 were tLBW (2.1%). Demographic characteristics of the original and final sample are provided in Table 3, and demographic characteristics of those exposed and unexposed to SDWA violations are available in Table 4. Within the sample over the nine-year study period, there were 60,983 births that were exposed to at least one MR violation and 53,354 births that were exposed to at least one HB violation. Tables with non-significant results can be found in the appendix.
Table 4:
Characteristics of singleton births exposed and unexposed to SDWA violations in their corresponding service area.
| Characteristic (%) | Monitoring and Reporting | Health-Based | ||
|---|---|---|---|---|
| ≥1 MR Violation Occurred, n = 60,983, n (%) | 0 MR Violation Occurred, n = 605,001, n (%) | ≥1 HB Violation Occurred, n = 53,354, n (%) | 0 HB Violation Occurred, n = 612,630, n (%) | |
| Infant Sex | ||||
| M (51.2) | 309448 (51.1) | 313375 (51.2) | ||
| F (48.8) | 295553 (48.9) | 299255 (48.8) | ||
| Mother’s Hispanic Origin | ||||
| Hispanic (12.8) | 79452 (13.1) | 81557 (13.3) | ||
| Not Hispanic (87.1) | 524778 (86.7) | 530266 (86.6) | ||
| Unknown (0.1) | 771 (.13) | 807 (.1) | ||
| Race | ||||
| White (66.6) | 398952 (65.9) | 405934 (66.3) | ||
| Black (20.6) | 125553 (20.8) | 124728 (20.4) | ||
| Other (12.8) | 80496 (13.3) | 82128 (13.4) | ||
| Mother’s Age | ||||
| 18–35 (85) | 513552 (84.9) | 519161 (84.7) | ||
| <18 (1.7) | 10629 (1.8) | 10692 (1.7) | ||
| >35 (13.3) | 80820 (13.4) | 82777 (13.5) | ||
| Mother’s Education | ||||
| Some secondary schooling1 (39.2) | 234088 (38.7) | 236982 (38.7) | ||
| Some college or college degree (59.7) | 364421 (60.2) | 368924 (60.2) | ||
| Unknown (1.1) | 6492 (1.1) | 6724 (1.1) | ||
| Payment | ||||
| Medicaid (28) | 167113 (27.6) | 168403 (27.5) | ||
| Private Insurance (65.5) | 399292 (66.0) | 404646 (66.1) | ||
| Self-Pay (5.1) | 30271 (5.0) | 31859 (5.2) | ||
| Unknown (1.3) | 8325 (1.4) | 7722 (1.3) | ||
| Tobacco | ||||
| No (87.3) | 529570 (87.5) | 536626 (87.6) | ||
| Yes (5.6) | 32239 (5.3) | 32574 (5.3) | ||
| Unknown (7.1) | 43192 (7.1) | 43430 (7.1) | ||
| Parity | ||||
| 1 (42) | 254277 (42.0) | 257307 (42.0) | ||
| 2 (32.3) | 195936 (32.4) | 198473 (32.4) | ||
| 3 (15.9) | 95964 (15.9) | 97355 (15.9) | ||
| 4 or more (9.8) | 58824 (9.7) | 59495 (9.7) | ||
Includes High School diploma or GED
Monitoring and Reporting Violations
Within the study sample, there were 60,983 births that were exposed to at least one MR violation. Three logistic regression models (one for each outcome) were employed to examine monitoring and reporting violations for 13 contaminants in relation to PTB, LBW, and tLBW.
When examining PTB in relation to individual MR violations, nitrate-nitrite had an OR of 1.10 (95% CI: 1.02–1.18) (see table 5). Confidence intervals for all other violations crossed one and are presented in Table 5. When examining LBW and tLBW in relation to MR violations, all violations were found to be insignificant at a CI of 95%.
Table 5:
Odds ratios (CI 95%) for associations between monitoring and reporting violations and PTB. Adjusted for water system service area, mother’s race, mother’s age, mother’s education, parity, majority gestational year, infant’s sex, and tobacco use during pregnancy. Bold = statistically significant
| SDWA Monitoring and Reporting Violation/Contaminant Name | Preterm Birth | |||
|---|---|---|---|---|
| OR | P | Lower 95 % | Upper 95 % | |
| Arsenic | 1.08 | 0.33 | 0.93 | 1.26 |
| Atrazine | 0.84 | 0.69 | 0.37 | 1.94 |
| Total Coliform Rule1 | 0.98 | 0.40 | 0.95 | 1.02 |
| Combined Radium | 1.08 | 0.30 | 0.93 | 1.26 |
| Combined Uranium | 1.10 | 0.23 | 0.94 | 1.28 |
| Stage 1 DBPR | 0.95 | 0.34 | 0.85 | 1.06 |
| Stage 2 DBPR | 1.04 | 0.28 | 0.97 | 1.13 |
| E. coli in Source Water | 0.93 | 0.27 | 0.82 | 1.06 |
| Gross Alpha Exc.2 | 1.10 | 0.24 | 0.95 | 1.27 |
| Lead and Copper Rule | 1.03 | 0.41 | 0.96 | 1.12 |
| Nitrate-Nitrite | 1.10 | 0.01 | 1.02 | 1.18 |
TCR in this study represents the first published rule and not the revised version that began in 2016.
Gross Alpha Excluding Radon and Uranium.
Health-Based Violations
Within the study sample, there were 53,354 births that were exposed to at least one HB violation. Three logistic regression models (one for each outcome) were employed to examine HB violations for eight contaminants in relation to PTB, LBW, and tLBW. Nitrate-nitrite, gross alpha including radon and uranium, and atrazine were excluded due to insufficient frequency of occurrence.
When examining PTB and LBW in relation to HB violations, no violations were significant at a CI of 95%. When examining tLBW in relation to HB violations, Total Coliform Rule (TCR) was found to be significant with an OR of 0.93 (95% CI: 0.87–1.00); in other words, the occurrence of TCR violations was associated with a decrease in tLBW. No other violations were found to be significant at a CI of 95% (see table 6).
Table 6:
Odds ratios (CI 95%) for associations between health-based violations and tLBW. Adjusted for water system service area, mother’s race, mother’s age, mother’s education, parity, majority gestational year, infant’s sex, and tobacco use during pregnancy. Bold = statistically significant
| SDWA Health-Based Violation/Contaminant Name1 | Term Low Birth Weight | |||
|---|---|---|---|---|
| OR | P | Lower 95 % | Upper 95 % | |
| Arsenic | 0.94 | 0.72 | 0.69 | 1.29 |
| Total Coliform Rule 2 | 0.93 | 0.04 | 0.87 | 1.00 |
| Combined Radium | 1.24 | 0.46 | 0.70 | 2.22 |
| Gross Alpha Exc.3 | 0.99 | 0.99 | 0.24 | 4.05 |
| Stage 1 DBPR4 | 1.01 | 0.92 | 0.88 | 1.16 |
| Lead and Copper Rule | 1.30 | 0.30 | 0.79 | 2.14 |
| Stage 2 DBPR | 1.09 | 0.50 | 0.85 | 1.39 |
Nitrate-nitrite, gross alpha including radon and uranium, and atrazine were excluded due to insufficient frequency of occurrence.
TCR in this study represents the first published rule and not the revised version that began in 2016.
Gross Alpha Excluding Radon and Uranium.
Stage 1 DBPR HB violations were exclusively treatment technique violations.
Distribution of Violations
During the study period, MR violations (n = 1,339) occurred more frequently than HB violations (n = 633), which is in keeping with previous research in Virginia (Marcillo and Krometis, 2019) and nationally (Allaire et al. 2018; Fu et al. 2020). Also, in keeping with state and national trends, violation occurrence increased as system size decreased, with very small (VS) systems having the highest quantity of violations and very large (VL) systems having the least, consistent across both violation types (see figure 3). PWS that utilized ground water as its source water type had more violations across both violation types (see figure 4).
Figure 3:
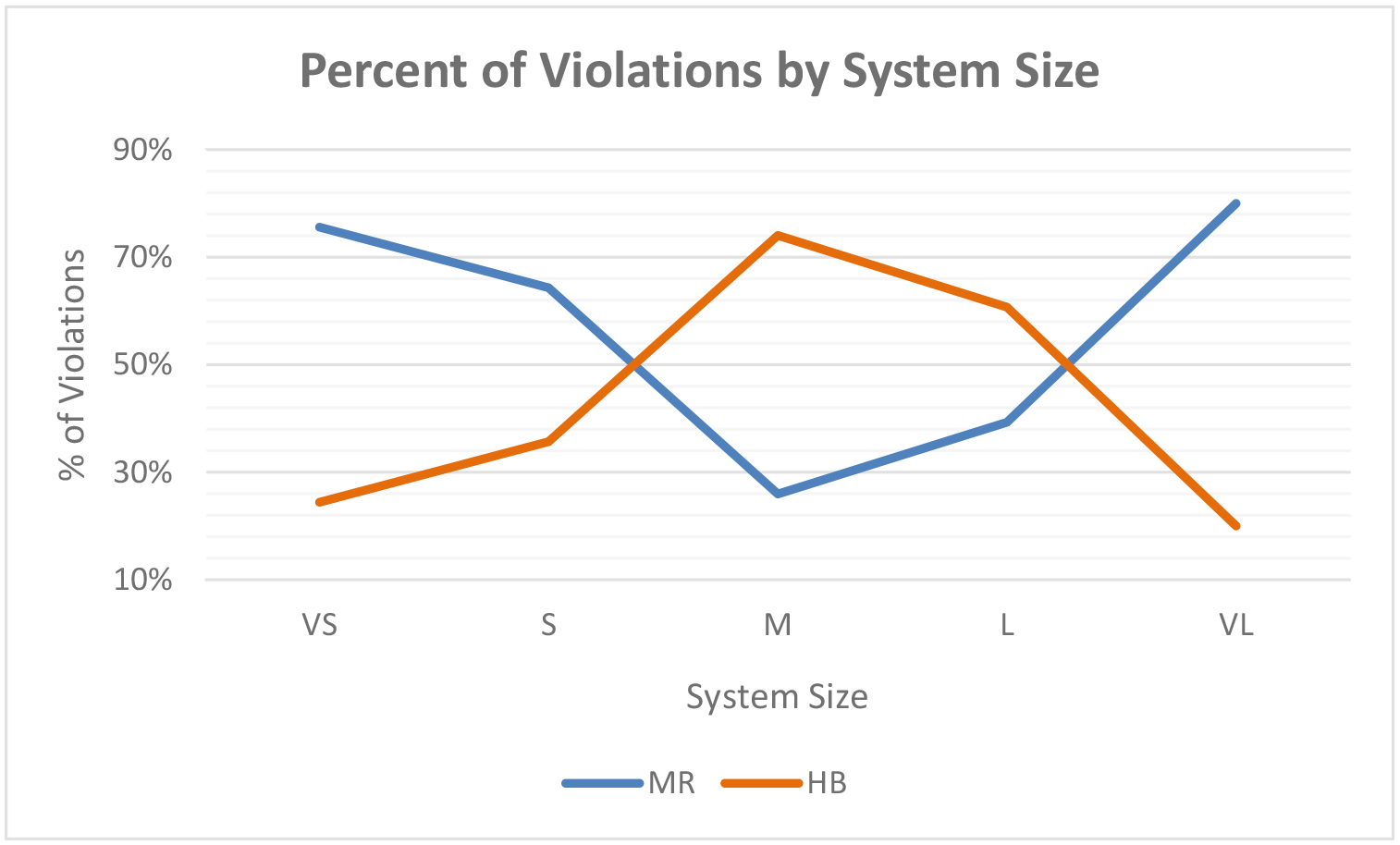
Percent of total violations by system size.
Figure 4:

Percent of total violations by source water type. Ground water systems include ground water and ground water purchased. Surface water systems include surface water, surface water purchased, and ground water under the influence of surface water.
Nitrate-Nitrite (MR)
Nitrate-nitrite violations primarily occurred in northern Virginia near Harrisonburg and Fredericksburg and were mainly concentrated in urban areas and large towns with a few occurring in more rural areas (see figure 5).
Figure 5:

Nitrate-Nitrite (MR) violations in estimated service areas.
Total Coliform Rule (HB)
TCR violations were distributed throughout Virginia (see figure 6). Throughout the study, violations were concentrated on the eastern side of the state with fewer violations as you move south through the state. Violations were mainly concentrated in urban areas and large towns apart from some violations occurring in more rural areas in the south-west.
Figure 6:

Total Coliform Rule (HB) violations in estimated service areas.
5. Discussion
These results suggest that specific SDWA violations are significantly associated with adverse birth outcomes. Nitrate-nitrite MR violations were positively associated with preterm birth, i.e., mothers who lived in a service area that had at least one nitrate-nitrite MR violation were 1.095 times or 9.5% more likely to experience a preterm birth than those that did not live in a service area where the violation occurred. It is critical to note that HB nitrate-nitrite violations occurred too infrequently in this study period to allow for formal analysis (0.01%). Previous examinations of national trends in MR and HB violation reporting suggest that financial incentives might unintentionally encourage under-resourced systems to incur MR violations to avoid the stricter penalties of HB violations (Fu et al., 2020); an explicit examination of this possibility is beyond the goals and data availability of the present study. However, it is noteworthy that this observation is in keeping with previous studies that indicate an association between PTB and nitrate. Sherris et al. (2021) found that maternal ingestion of nitrate contaminated drinking water is associated with increased odds of spontaneous PTB. Similarly, Stayner et al. (2017) found that maternal ingestion of nitrate contaminated drinking water is associated with very PTB (<3.3 pounds).
Results also revealed a negative association between the HB TCR violation and tLBW, as tLBW was 7% less for mothers that lived in a service area where at least one HB TCR violation occurred during the majority year of gestation. Total coliforms are not typically harmful to humans. Instead, they are used as an indicator to determine if disinfection processes are working properly and that the water system is functioning adequately. It is difficult to explain why a HB TCR violation may decrease the risk for tLBW. This finding could be spurious, or it could possibly result from live-birth bias. Since the study only examined live-births, it is not possible to fully examine the impact of exposure to drinking water violations. Another possible explanation for this result is that a HB TCR violation may signal to a system that there is an issue that needs to be addressed rather than potentially going unnoticed when a MR TCR violation is issued. Since no studies have looked at the potential fetal health effects of TCR violations, evidence to support our findings cannot be found, indicating a need for future research.
Limitations and Future Research
Several important limitations exist within the study, which could result in bias. Geocoding addresses presents limitations due to locational error at the individual level. Additionally, geocoded addresses often have a higher error when locating rural addresses as opposed to addresses in a city. Although portions of Virginia are considered rural, much of the population lives in a more easily geocoded urban area.
Majority gestational year was used to define the exposure period, and SDWA violations were aggregated yearly. If exposure occurred during the minority gestational year but not during the majority gestational year, then SDWA violations that occurred in the minority gestational year were not compared to that birth outcome. For example, an infant born at full-term in June of 2012 would be assigned to 2012 for its majority gestational year. The birth record for that infant is paired with the SDWA violations that occurred in 2012. If exposure occurred in December of 2011, then the results of the study could be skewed. Future research examining quarterly SDWA reports, particularly in areas of high adverse birth outcome incidence, is recommended.
Covariates were considered and the study was adjusted to consider all available known covariates. Race was represented differently on original birth records from 2007–2012 and 2013–2015. From 2007–2012 the mother’s race was not recorded so instead child’s race was used. From 2013–2015 mother’s race was recorded and used. It is important to recognize that though mother’s race and child’s race may not be the same, to include race as a potential confounding variable, child’s race was used when mother’s race was unavailable. Additionally, ethnicity of mother was limited to mother’s reported Hispanic origin or not. This study did not take into consideration combinations of reported race and ethnicity. Future studies can benefit from further analysis of reported race and ethnicity to characterize differences based on demographic variables. Additionally, despite the careful consideration of covariates, this study was limited to the covariates stated above and thus, unknown covariates could still exist (e.g., maternal comorbidities).
Water systems often monitor at a frequency proportional to the number of people served, and each violation requires a different monitoring frequency. For example, under the revised TCR, larger systems serving 83,001 – 96,000 people are required to monitor for total coliform at a frequency of 90 samples per month as compared to a frequency of seven samples per month required for a smaller system serving 5,801 – 6,700 people (EPA, n.d.). Because of monitoring differences, violations for this study were represented as binary variables (yes = at least one violation occurred; no = no violations occurred). Due to this limitation, we are unable to consider how a greater frequency of violations impact birth outcomes. These results do reveal a potential risk for adverse birth outcomes when a violation occurs, raising a warning that monitoring and reporting violations may indicate decreased effectiveness of treatment facilities, posing a potential risk to fetal health. Further research is needed to examine the relationship between birth outcomes and individual water contaminant violations; looking individually at each violation type can allow the researcher to see the effect of violation frequency.
As noted previously, service area boundaries in this study are estimates and could therefore potentially introduce exposure misclassification, which is a well-recognized limitation of investigations of waterborne exposures nationally (McDonald et al. 2022). This study also does not take into consideration consumption of bottled water during pregnancy or mothers who moved during their pregnancy. This is noteworthy, as emerging evidence suggests that, particularly post-Flint, reliance on bottled water has increased notably, particularly among Black and Hispanic families (Teodoro et al., 2o22). However, at present consumption patterns are unavailable at household scale. Similarly, the exposure profile of women who rely on tap water might be misclassified if most of their consumption occurs outside the home residence, i.e., at work or school. Truly accurate exposure measures would demand paired household-level water quality monitoring and consumption reports, which is worthy of future consideration but beyond the scope of the present effort. Despite this limitation, we believe the demonstration of significant relationships here does suggest the approach applied is an advance over previous examinations at the county scale and can serve as motivation for individual or community scale examinations at field scale.
6. Conclusion
Our results indicate that nitrate-nitrite MR violations may be associated with the risk for PTB and TCR HB violations may decrease the risk for tLBW. In keeping with previous research, MR violations represented most violation types, and violation frequency increased as system size decreased. Additionally, violations primarily occurred at public water systems reliant on ground water. The two violations that were found to be significant occur primarily in northern Virginia and on the eastern side of the state, decreasing in occurrence as you move south-west, with a few exceptions. By identifying exposure at the service area level, we were able to reduce exposure misclassification that may have been introduced had we relied on political boundaries instead. This research provides valuable insight that drinking water violations may pose a risk to fetal health, and that more research on individual violations is warranted to examine links between health and waterborne exposures related to municipal drinking water violations.
Supplementary Material
Exposure to drinking water violations defined at estimated service area level
Examined preterm birth, low birth weight, and term low birth weight
Monitoring and reporting violations may be concealing health-based violations
Monitoring and reporting nitrate-nitrite violation related to preterm birth
Health-based total coliform rule violation related to healthy birth weight
Funding
This work was supported by the National Institute of Environmental Health Sciences (R21ES028396).
Declaration of interests
Julia Gohlke reports financial support was provided by National Institute of Environmental Health Sciences. Holly Young reports a relationship with United States Environmental Protection Agency that includes: employment. Cristina Marcillo reports a relationship with United States Environmental Protection Agency that includes: employment.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Ahern MM, Hendryx M, Conley J, Fedorko E, Ducatman A, Zullig KJ (2011). The association between mountaintop mining and birth defects among live births in central Appalachia, 1996–2003, Environmental Research, Volume 111, Issue 6, 2011, Pages 838–846, ISSN 0013–9351, 10.1016/j.envres.2011.05.019. [DOI] [PubMed] [Google Scholar]
- Ahmad SA, Salim Ullah Sayed MH, Barua S, Haque Khan M, Faruquee MH, Jalil A, … Kabir Talukder H (2001). Arsenic in drinking water and pregnancy outcomes. Environmental Health Perspectives, 109(6), 629–631. 10.1289/ehp.01109629 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Allaire M, Wu H, & Lall U (2018). National trends in drinking water quality violations. Proceedings of the National Academy of Sciences of the United States of America, 115(9), 2078–2083. 10.1073/pnas.1719805115 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Almberg KS, Turyk ME, Jones RM, Rankin K, Freels S, & Stayner LT (2018). Atrazine contamination of drinking water and adverse birth outcomes in community water systems with elevated atrazine in Ohio, 2006–2008. International Journal of Environmental Research and Public Health, 15(9). 10.3390/ijerph15091889 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Almberg KS, Turyk ME, Jones RM, Rankin K, Freels S, Graber JM, & Stayner LT (2017). Arsenic in drinking water and adverse birth outcomes in Ohio. Environmental Research, 157, 52–59. 10.1016/j.envres.2017.05.010 [DOI] [PubMed] [Google Scholar]
- Aschengrau A, Winter M, Gallagher L, Vieira V, Butler L, Fabian M, … Ozonoff D (2020, February 13). Reproductive and developmental health effects of prenatal exposure to tetrachloroethylene-contaminated drinking water. Retrieved September 12, 2022, from https://pubs.rsc.org/en/content/articlelanding/2020/em/c9em00590k/unauth [DOI] [PMC free article] [PubMed]
- Blaisdell J, Turyk ME, Almberg KS, Jones RM, & Stayner LT (2019). Prenatal exposure to nitrate in drinking water and the risk of congenital anomalies. Environmental Research, 176, 108553. doi: 10.1016/j.envres.2019.108553 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bove FJ (1996). Public Drinking Water Contamination and Birthweight, Prematurity, Fetal Deaths, and Birth Defects. In Toxicology and Industrial Health (Vol. 12). [PubMed] [Google Scholar]
- Bove FJ, Fulcomer MC, Klotz JB, Esmart J, Dufficy EM, & Savrin JE (1995). Public drinking water contamination and birth outcomes. American Journal of Epidemiology, 141(9), 850–862. 10.1093/oxfordjournals.aje.a117521 [DOI] [PubMed] [Google Scholar]
- Buttling LG, McKnight MX, Kolivras KN, Ranganathan S, & Gohlke JM (2021). Maternal proximity to Central Appalachia Surface Mining and birth outcomes. Environmental Epidemiology, 5(1). doi: 10.1097/ee9.0000000000000128 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cao W, Zeng Q, Luo Y, Chen H, Miao D, Li L, … Lu W (2016). Blood biomarkers of late pregnancy exposure to trihalomethanes in drinking water and fetal growth measures and gestational age in a Chinese cohort. Environmental Health Perspectives, 124(4), 536–541. doi: 10.1289/ehp.1409234 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cech I, Burau KD, & Walston J (2007). Spatial distribution of orofacial cleft defect births in Harris County, Texas, 1990 to 1994, and historical evidence for the presence of low-level radioactivity in tap water. Southern Medical Journal, 100(6). https://go.gale.com/ps/anonymous?id=GALE%7CA165821640&sid=googleScholar&v=2.1&it=r&linkaccess=abs&issn=00384348&p=AONE&sw=w [DOI] [PubMed] [Google Scholar]
- Claus Henn B, Ettinger AS, Hopkins MR, Jim R, Amarasiriwardena C, Christiani DC, Coull BA, Bellinger DC, & Wright RO (2016). Prenatal arsenic exposure and birth outcomes among a population residing near a mining-related superfund site. Environmental Health Perspectives, 124(8), 1308–1315. 10.1289/ehp.1510070 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dodds L, King W, Woolcott C, & Pole J (1999). Trihalomethanes in Public Water Supplies and Adverse Birth Outcomes. Retrieved from https://about.jstor.org/terms [PubMed]
- Edwards M (2013). Fetal Death and Reduced Birth Rates Associated with Exposure to Lead-Contaminated Drinking Water. 10.1021/es4034952 [DOI] [PubMed] [Google Scholar]
- EPA. (n.d.) Revised Total Coliform Rule And Total Coliform Rule | Drinking Water Requirements for States and Public Water Systems | US EPA. (n.d.). Retrieved February 29, 2020, from https://www.epa.gov/dwreginfo/revised-total-coliform-rule-and-total-coliform-rule
- Fu G, Liu P, & Swallow S (2020). Effectiveness of Public versus Private Ownership: Violations of the Safe Drinking Water Act (SDWA). Agricultural and Resource Economics Review, 49(2), 291–320. doi: 10.1017/age.2020.4 [DOI] [Google Scholar]
- Gallagher MD, Nuckols JR, Stallones L, & Savitz DA (1998). Exposure to Trihalomethanes and Adverse Pregnancy Outcomes. In Source: Epidemiology (Vol. 9). [PubMed] [Google Scholar]
- Hill E, & DiSalvo R (2019). Public drinking water contamination and birth outcomes. Environmental Epidemiology, 3, 159. doi: 10.1097/01.ee9.0000607520.82579.07 [DOI] [Google Scholar]
- Hill EL, & Ma L (2022). Drinking water, fracking, and infant health. Journal of Health Economics, 82, 102595. doi: 10.1016/j.jhealeco.2022.102595 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hinckley AF, Bachand AM, & Reif JS (2005). Late pregnancy exposures to disinfection by-products and growth-related birth outcomes. Environmental Health Perspectives, 113(12), 1808–1813. 10.1289/ehp.8282 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huang H, Woodruff TJ, Baer RJ, Bangia K, August LM, Jellife-Palowski LL, … Sirota M (2018). Investigation of association between environmental and socioeconomic factors and preterm birth in California. Environment International, 121, 1066–1078. doi: 10.1016/j.envint.2018.07.027 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hwang BF, & Jaakkola JJK (2003). Water Chlorination and Birth Defects: A Systematic Review and Meta-Analysis. Archives of Environmental Health, 58(2), 83–91. 10.3200/AEOH.58.2.83-91 [DOI] [PubMed] [Google Scholar]
- Jones B, Peake K, Morris AJ, McCowan LM, & Battin MR (2004). Escherichia coli: A growing problem in early onset neonatal sepsis. In Australian and New Zealand Journal of Obstetrics and Gynaecology (Vol. 44, Issue 6, pp. 558–561). 10.1111/j.1479-828X.2004.00304.x [DOI] [PubMed] [Google Scholar]
- Langlois PH, Lee M, Lupo PJ, Rahbar MH, & Cortez RK (2016). Residential radon and birth defects: A population-based assessment. Birth Defects Research Part A - Clinical and Molecular Teratology, 106(1), 5–15. 10.1002/bdra.23369 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marcillo CE, Krometis L-AH. Small towns, big challenges: Does rurality influence Safe Drinking Water Act compliance? (2018) AWWA Wat Sci. 2018;e1120. 10.1002/aws2.1120 [DOI] [Google Scholar]
- Marcillo C, Krometis L-A, & Krometis J (2021). Approximating Community Water System Service Areas to Explore the Demographics of SDWA Compliance in Virginia. International Journal of Environmental Research and Public Health, 18(24), 13254. 10.3390/ijerph182413254 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McDonald YJ, Anderson KM, Caballero MD, Ding KJ, Fisher DH, Morkel CP, & Hill EL (2022). A systematic review of geospatial representation of United States community water systems. AWWA Water Science, e1266. 10.1002/aws2.1266 [DOI] [Google Scholar]
- Rinsky JL, Hopenhayn C, Golla V, Browning S, & Bush HM (2012). Atrazine Exposure in Public Drinking Water and Preterm Birth. Public Health Reports, 127(1), 72–80. 10.1177/003335491212700108 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ruktanonchai CW, McKnight MX, Buttling L, Kolivras K, Krometis L, & Gohlke J (2022). Identifying exposure pathways mediating adverse birth outcomes near active surface mines in Central Appalachia. Environmental Epidemiology, 6(3). doi: 10.1097/ee9.0000000000000208 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sherris AR, Baiocchi M, Fendorf S, Luby SP, Yang W, & Shaw GM (2021). Nitrate in drinking water during pregnancy and spontaneous preterm birth: A retrospective within-mother analysis in California. Environmental Health Perspectives, 129(5). doi: 10.1289/ehp8205 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Srivastav A, Patel N, & Chaudhary V (2020, August 23). Disinfection by-products in drinking water: Occurrence, toxicity and abatement. Retrieved September 12, 2022, from https://www.sciencedirect.com/science/article/abs/pii/S0269749120361625?casa_token=HZvO49Uw2E4AAAAA%3A9hIExyv-KKgM_Hl4fZp0BSTCHuVg7EqK-oSVfYaha9w880SKDfnZEP9IjURJd22Ff3j6k66UhA [DOI] [PubMed]
- Stayner LT, Almberg K, Jones R, Graber J, Pedersen M, & Turyk M (2017). Atrazine and nitrate in drinking water and the risk of preterm delivery and low birth weight in four Midwestern states. Environmental Research, 152, 294–303. 10.1016/j.envres.2016.10.022 [DOI] [PubMed] [Google Scholar]
- Teodoro MP, Zuhlke S, Switzer D (2022, August). The Profits of Distrust – Citizen-Consumers, Drinking Water, and the Crisis of Confidence in American Government. Cambridge University Press, 10.1017/9781009244893 [DOI] [Google Scholar]
- Toledano MB, Nieuwenhuijsen MJ, Best N, Whitaker H, Hambly P, de Hoogh C, … Elliott P (2005). Relation of trihalomethane concentrations in public water supplies to stillbirth and birth weight in three water regions in England. Environmental Health Perspectives, 113(2), 225–232. 10.1289/ehp.7111 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ugwuja E, Ejikeme B, Obuna JA (2011, July). Impacts of Elevated Prenatal Blood Lead on Trace Element Status and Pregnancy Outcomes in Occupationally Non-exposed Women | Ugwuja | Int J Occup Environ Med (The IJOEM). (n.d.). Retrieved April 13, 2020, from https://theijoem.com/ijoem/index.php/ijoem/article/view/94/187 [PubMed]
- US EPA | Office of Enforcement and Compliance Assurance. (2013). Providing safe drinking water in America: 2013 National Public Water Systems Compliance Report. EPA Document 305R15001 [Google Scholar]
- US EPA. (2022, February). Potential Well Water Contaminants and Their Impacts. Retrieved September 12, 2022, from https://www.epa.gov/privatewells/potential-well-water-contaminants-and-their-impacts#:~:text=Heavy%20metals%20can%20contaminate%20private,damage%2C%20anemia%2C%20and%20cancer.
- The Standardized Monitoring Framework: A quick reference guide - US EPA. (2020, May). Retrieved October 2, 2022, from https://www.epa.gov/sites/default/files/202005/documents/smf_2020_final_508.pdf
- von Ehrenstein OS, Wilhelm M, & Ritz B (2013). Maternal occupation and term low birth weight in a predominantly Latina population in Los Angeles, California. Journal of Occupational & Environmental Medicine, 55(9), 1046–1051. 10.1097/jom.0b013e31829888fe [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang R, Chen X, & Li X (2021). Something in the pipe: The Flint Water Crisis and health at birth. Journal of Population Economics, 35(4), 1723–1749. doi: 10.1007/s00148-021-008769 [DOI] [Google Scholar]
- WHO. (n.d.) Preterm and low birth weight. (n.d.). Retrieved September 12, 2022, from https://www.who.int/teams/maternal-newborn-child-adolescent-health-andageing/newborn-health/preterm-and-low-birth-weight#:~:text=Preterm%20infants%20are%20born%20at,low%20birth%20weight%20each%20year.
- Yang CY, Chang CC, Tsai SS, Chuang HY, Ho CK, & Wu TN (2003). Arsenic in drinking water and adverse pregnancy outcome in an arseniasis-endemic area in northeastern Taiwan. Environmental Research, 91(1), 29–34. 10.1016/S0013-9351(02)00015-4 [DOI] [PubMed] [Google Scholar]
- Yang CY, Xiao ZP, Ho SC, Wu TN, & Tsai SS (2007). Association between trihalomethane concentrations in drinking water and adverse pregnancy outcome in Taiwan. Environmental Research, 104(3), 390–395. 10.1016/j.envres.2007.01.006 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.