

Abstract
Background:
It is known that giant cell arteritis (GCA) and polymyalgia rheumatica (PMR) often occur together. So far, the prevalence of GCA in newly diagnosed PMR patients has not been evaluated in a prospective ultrasound study.
Objective:
The aim of this study was to assess the prevalence of GCA using vascular ultrasound in patients with newly diagnosed PMR.
Design:
A consecutive cohort of newly diagnosed PMR patients was prospectively evaluated for the presence of GCA with the use of systematic musculoskeletal and vascular ultrasound examination.
Methods:
Overall, 60 patients with newly diagnosed PMR were prospectively enrolled. Symptoms and laboratory findings were collected. All patients underwent ultrasound of shoulder and hip joints, and vascular ultrasound evaluating the facial, temporal, carotid, vertebral and axillary arteries. Patients were diagnosed with GCA if they had ultrasound imaging findings of GCA. Patients with PMR (PMR-group) and patients with PMR and GCA (PMR–GCA-group) were compared, and a C-reactive protein (CRP) cut-off value was evaluated.
Results:
GCA was diagnosed in 28 of 60 PMR patients (46%). The PMR-group consisted of 20 (62.5%) females with a mean age of 69 (±9.9) years, while the PMR–GCA-group consisted of 11 (39.3%) females with a mean age of 74 (±8.4) years. In 13 of 28 patients (46%) in the PMR–GCA-group, GCA was subclinical and only diagnosed by ultrasound. The PMR–GCA-group showed higher values of joint effusion and significantly higher CRP values. A CRP cut-off value of 26.5 mg/litre (reference range 0–5 mg/litre) yielded a sensitivity of 66% with a specificity of 73% for GCA.
Conclusion:
GCA was found in 46% of newly diagnosed PMR patients; 22% of the patients with PMR had asymptomatic GCA. Joint effusions were higher in the PMR–GCA-group, with significant results for the hip joint. A CRP cut-off value of ⩾26.5 mg/litre in PMR can help in the identification of subclinical GCA.
Keywords: C-reactive protein, cut-off value, giant cell arteritis, joint effusion, polymyalgia rheumatica, prevalence, ultrasound
Introduction
Polymyalgia rheumatica (PMR) is an inflammatory disease of the elderly with characteristic clinical symptoms of stiffness and pain of neck and shoulder area and the pelvic girdles.1 Incidences are between 41 and 113 cases per 100,000 of European people above 50 years of age.2 Giant cell arteritis (GCA) is the most common form of systemic vasculitis in elderly, typically affecting medium and large extracranial vessels. The incidence of GCA is lower than for PMR, with incidences between 18 to 29 cases per 100,000 people above 50 years of age.2 GCA can present with various clinical symptoms, such as headache, scalp tenderness, jaw claudication or visual impairment.3 PMR and GCA are associated with elevated inflammatory laboratory markers, especially C-reactive protein (CRP).
It is well known that PMR and GCA frequently coexist.4,5 According to recent studies, GCA is frequently underdiagnosed in PMR patients and may be the cause of therapy-resistant PMR.6–8 The use of other imaging techniques, in particular 18F-fluorodeoxyglucose positron emission tomography (18F-FDG-PET), has revealed that a third of patients with PMR without symptoms or signs of GCA can have an occult large vessel involvement.9 Given the two conditions are treated differently, it is imperative to establish the correct diagnosis. The prevalence of GCA in patients presenting with PMR has not been well studied.
Correct identification of those diseases can be challenging, as symptoms and signs of GCA and PMR may vary and are unspecific (i.e. headache and shoulder pain).10,11 Evaluation of laboratory parameters can be helpful, but acute phase reactants can be elevated due to other inflammatory processes as well. In recent years, CRP has become the most accurate parameter, due to higher sensitivity.12
Ultrasound as an imaging modality plays an important role in the diagnosis of GCA and PMR and increases diagnostic specificity; it is non-invasive, easy to use, reliable and widely available.13–15 Further ultrasound is easily accessible at point-of-care and low in costs, which makes it the ideal method for fast-track diagnosis.16,17 Compared to temporal artery biopsy, ultrasound provides a higher sensitivity.18,19
The purpose of this prospective study was to assess the prevalence of vascular abnormalities consistent with GCA in patients with newly diagnosed PMR using the Outcome Measures in Rheumatology (OMERACT) definitions for GCA with established cut-off values.18–20 We compared clinical, laboratory and ultrasound variables in patients with PMR only and those with PMR and GCA. Finally, we assessed CRP values to establish a cut-off value to distinguish between patients with PMR only and patients with PMR and GCA.
Methods
Study population
All consecutive patients with newly diagnosed PMR who presented to the Department of Rheumatology at the University Hospital Bonn, Germany between 1 October 2018 and 31 January 2021 were included. Patients were referred to our clinic by themselves, their local rheumatologists or their primary care physicians.
Patients had to meet the following inclusion criteria: age above 50 years, elevated inflammatory laboratory markers (CRP > 5 mg/litre), a glucocorticoid (GC) intake of 7 days or less given data that suggest false-negative results after a longer GC intake.21 There was no limit on the maximum intake of GC prior to inclusion in the study. European League Against Rheumatism/American College of Rheumatology (EULAR/ACR) 2012 classification criteria were used to classify PMR in these patients.15 Diagnosis of PMR was verified by an experienced board-certified rheumatologist (VSS or PK). All patients with diagnosis of PMR were evaluated with ultrasound of the shoulder and hip joints, and vascular ultrasound. Diagnosis of GCA was also made by an experienced board-certified rheumatologist (VSS or PK) according to clinical, laboratory and imaging parameters. Patients who did not have GCA symptoms but had abnormalities on vascular ultrasound examination were considered having GCA. All of the patients also fulfilled the extended ACR classification criteria, which include imaging.6 Diagnosis of GCA was based on clinical parameters and ultrasound findings only. Ultrasound of the temporal and axillary artery is recommended as first imaging modality in the EULAR recommendation on imaging in large-vessel vasculitis (LVV).13 All ultrasounds were performed by rheumatologists (VSS and PK) with extensive expertise, and as a result, ultrasound abnormalities were considered sufficient for diagnosis of GCA and a temporal artery biopsy was not pursued.
Patients were then split into two groups: The PMR-group included patients who had been diagnosed with PMR only and the PMR–GCA-group which comprised patients who also had a GCA diagnosis.
PMR patients who were found to have GCA, were treated as GCA.
Six months later, each patient was contacted and examined to assess any changes in diagnosis.
The reporting of this study conforms to the Standards for Reporting Diagnostic accuracy studies (STARD).22
Clinical evaluation
At the time of recruitment, demographic data, previous treatment with GC, cardiovascular risk factors, duration of symptoms, and PMR and GCA symptoms and signs were obtained using a questionnaire. Duration and amount of GC intake were obtained from every patient. CRP, haemoglobin, leucocyte and thrombocyte counts, rheumatoid factor (RF) and anti-citrullinated peptide antibodies (ACPA) were the laboratory markers examined at inclusion. The erythrocyte sedimentation rate (ESR) was not assessed since current studies indicate that evaluation of ESR does not increase diagnostic accuracy.12
Ultrasound examination
All patients underwent an ultrasound examination of shoulder and hip joints, and a core set of arteries typically affected in GCA according to EULAR recommendations.13 For all examinations, a GE Logiq S8 XDclear ultrasound machine with software version R3 manufactured in 2018 was used. For shoulder and hip joints, axillary, vertebral and carotid arteries, a multifrequency linear ultrasound probe with a range from 6 to 15 MHz was used; for all other small arteries, a multifrequency ultrasound probe with a range from 8 to 18 MHz was applied. The parameters B-Mode frequency, image depth and focus points were adjusted individually for every patient to provide the best possible picture.
All ultrasound examinations were performed by experienced rheumatologists (VSS and PK) with 13 and 14 years of ultrasound experience [German Society for Ultrasound in Medicine (DEGUM)/European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB) levels II and III], who have previously proven to be reliable ultrasonographers17 or by a medical student (LCB) under the supervision of one of the two rheumatologists.
The ultrasound examiners were blinded to clinical data and symptoms.
Vascular ultrasound
The following arteries were examined in both planes (transversal and longitudinal) for signs of vasculitis: axillary artery, vertebral artery, common carotid artery, common superficial temporal artery with frontal and parietal branches and facial artery.23 Intima-media thickness (IMT) values of all above-mentioned arteries were measured in diastole using B-mode. Highest IMT values were recorded. All measurements were performed on the wall distal to the ultrasound probe in a rectangular position from the beginning of the medial-adventitial structure close to the wall of the vessel to the intima-structure close to the lumen.
Vessels were considered abnormal if IMT of the arteries extended respective cut-off values19,20 and OMERACT ultrasound definitions for acute GCA were met.23
Musculoskeletal ultrasound
Shoulder joints were evaluated for the presence and extent of effusion around the biceps tendon and for glenohumeral effusion, as well as for subacromial-subdeltoid bursitis. Hip joints were examined for effusion in the trochanteric bursae and for hip capsular effusion, respectively. The biceps tendon was examined in longitudinal and transversal section, and the glenohumeral area was scanned in transversal section. Effusion of the hip joint and the trochanteric bursae was measured in longitudinal section. All joint effusions were evaluated at the point of their widest extent and in total area (Figures 1 and 2). Joint effusions were defined as findings of hypo- or anechoic joint capsule distension in ultrasound examination.
Figure 1.

Ultrasound images and measuring techniques of the shoulder joint. (a) Biceps tendon in transversal section, measurement of the effusion at the widest extent. (b) Biceps tendon in transversal section, measurement of the effusion in total area. (c) Biceps tendon in longitudinal section, measurement of the effusion at the widest extent. (d) Biceps tendon in longitudinal section, measurement of the effusion in total area. (e) Glenohumeral joint, measurement of the effusion at the widest extent. (f) Glenohumeral joint, measurement of the effusion in total area.
Figure 2.

Ultrasound images and measuring techniques of the hip joint. (a) Trochanteric bursae, measurement of the effusion at the widest extent. (b) Trochanteric bursae, measurement of the effusion in total area. (c) Hip joint, measurement of the effusion in total area.
Statistical analysis
Statistical analysis was performed using SPSS, version 26 (IBM) and R, version 4.0.3. For quantitative parameters, mean values, standard deviation and ranges were calculated. For categorical data, Pearson’s chi-square test was applied. When normality could not be assumed, the Mann–Whitney U test was applied. Otherwise, metric data were tested using t-tests. Statistical significance level was defined at p < 0.05. Receiver operating characteristic curve (ROC) analyses were applied to evaluate the discriminatory ability. The optimal cut point was determined with respect to the Youden’s index.
Results
A total of 117 patients with PMR were referred to our department; however, 57 had to be excluded owing to prolonged pre-treatment with GC (>7 days). Overall, 60 patients with first diagnosis of PMR were included. Twenty-eight patients had vascular abnormalities on ultrasound that were consistent with a diagnosis of GCA. Therefore, the prevalence of GCA in this cohort was 46%. The diagnosis remained unchanged at re-evaluation in 6 months. An additional patient in the PMR-group developed GCA, which was diagnosed by ultrasound on a follow-up visit one month after inclusion. One patient of the PMR-group presented to our clinic reporting temporal loss of vision, which was later identified as non-vasculitic anterior ischemic optic neuropathy (AION).
Clinical and laboratory parameters
A comparison of the 32 patients (54%) in the PMR-group and 28 patients (46%) in the PMR–GCA-group is displayed in Table 1. Patients in the PMR-group were younger (mean age 69 years) compared to the PMR–GCA-group (mean age 74 years), (p = 0.03). The PMR-group had a mean duration of symptoms of 10 weeks compared to 16 weeks for the PMR–GCA-group (p = 0.08). The PMR-group had a lower mean GC intake of 0.4 days, compared to the PMR–GCA-group with a mean GC intake of 1.5 days (p = 0.05). The PMR–GCA-group had a higher mean GC intake due to the initiation of pulse therapy in case of visual symptoms.
Table 1.
Demographic and clinical data.
| PMR-group (n = 32) | PMR–GCA-group (n = 28) | p value | |
|---|---|---|---|
| Patient characteristics | |||
| Age, years | 69 (±9.9) | 74 (±8.4) | 0.03 |
| Female | 20 (62.5%) | 11 (39.3%) | 0.12 |
| Symptom duration, weeks | 9.5 (±9.3) | 16.4 (17.9) | 0.08 |
| GC intake, days | 1.43 (±2.16) | 0.4 (1.06) | 0.05 |
| Initial GC intake, mean amount ± SD (mg) | 17.2 (±45.4) | 81.8 (±226) | 0.14 |
| Cardiovascular risk factors | |||
| Obesity | 4 (12%) | 4 (14%) | 1 |
| Arterial hypertension | 15 (47%) | 18 (64%) | 0.11 |
| Diabetes mellitus | 2 (6%) | 7 (25%) | 0.32 |
| Smoking | 8 (25%) | 6 (21%) | 0.12 |
| Peripheral artery occlusive disease | 1 (3%) | 1 (4%) | 0.21 |
| Atherosclerosis | 10 (31%) | 12 (43%) | 0.11 |
| Coronary heart disease | 4 (12%) | 3 (11%) | 0.50 |
| History of myocardial infarction | 2 (6%) | 2 (7%) | 0.59 |
| History of stroke or transient ischemic attack | 5 (15%) | 4 (14%) | 0.48 |
| General symptoms | |||
| Fever | 0 (0%) | 2 (7%) | 0.41 |
| Night sweats | 5 (15.6%) | 5 (17.9%) | 1 |
| Weight loss | 6 (18.8%) | 5 (17.9%) | 1 |
| Fatigue | 1 (3.1%) | 4 (14.3%) | 0.17 |
| PMR-specific characteristics | |||
| Morning stiffness | 31 (97%) | 23 (82%) | 0.08 |
| Pain of pelvic girdle | 32 (100%) | 27 (96%) | 0.47 |
| Absence of affection of other joints | 31 (97%) | 28 (100%) | 1 |
| Absence of RF and ACPA antibodies | 31 (97%) | 27 (96%) | 1 |
| EULAR/ACR 2012 criteria points ⩾ 5 | 31 (97%) | 25 (89%) | 0.44 |
| EULAR/ACR 2012 criteria points, M (SD) | 5.44 (±0.88) | 5.28 (±0.90) | 0.44 |
| GCA-specific symptoms | |||
| Visual impairment | 1 (4%) | 7 (25%) | 0.07 |
| Temporal headache | 3 (9%) | 10 (36%) | 0.03 |
| Jaw claudication | 3 (9%) | 10 (36%) | 0.11 |
| Scalp tenderness | 0 (0%) | 1 (4%) | 0.09 |
| Laboratory parameters | |||
| Leucocytes, 103/µl, M (SD) | 9.89 (±2.5) | 9.22 (±3.0) | 0.38 |
| Thrombocytes, 103/µl, M (SD) | 349 (±123) | 321 (±103) | 0.37 |
| Haemoglobin, mg/dl, M (SD) | 12.6 (±1.5) | 12.3 (±1.5) | 0.55 |
| CRP, mg/litre, M (SD) | 29.5 (±31.6) | 53.8 (±42.3) | 0.02 |
ACPA, anti-citrullinated peptide antibodies; ACR, American College of Rheumatology; EULAR, European League Against Rheumatism; GCA, giant cell arteritis; PMR, polymyalgia rheumatic; RF, rheumatoid factor; SD, standard deviation.
PMR–GCA-group: patients with diagnosis of PMR and GCA; PMR-group: patients with diagnosis of PMR; Visual impairment: amaurosis, diplopia, vision loss and blurred vision.
Table 1 displays the clinical parameters for both groups. The mean number of PMR EULAR/ACR 2012 criteria points met was 5.4 (SD ± 0.86) in the PMR-group and 5.3 (SD ± 0.88) in the PMR–GCA-group (p = 0.44). The mean number of GCA symptoms was 0.3 (SD ± 0.73) in the PMR-group and 1.35 (SD ± 1.74) in the PMR–GCA-group, respectively (p = 0.004). In total, 22 (79%) patients in the PMR–GCA-group reported two or fewer GCA symptoms and 13 patients (46%) reported no specific GCA symptoms at all.
Mean CRP was 29.5 mg/dl (SD ± 31.61) in the PMR-group and 53.8 mg/dl (SD ± 42.27) in the PMR–GCA-group at a reference range of < 5 mg/litre. CRP values were significantly higher (p = 0.018) in the PMR–GCA-group compared to the PMR-group (Table 1). The other laboratory parameters examined did not differ substantially between the two groups. A CRP cut-off value of 26.5 mg/litre was found to distinguish the PMR-group from the PMR–GCA-group, offering a sensitivity of 66% and a specificity of 73%. Calculated area under the curve (AUC) was found to be 0.670 (confidence interval 0.520–0.821, Figure 3).
Figure 3.
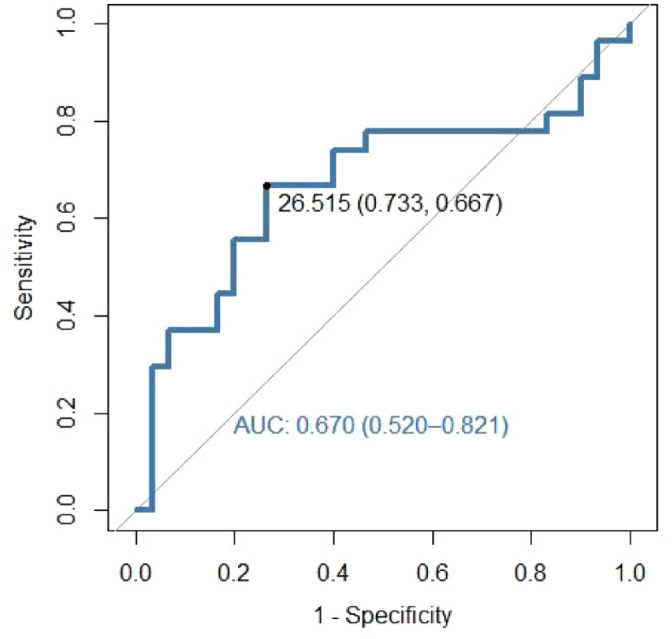
ROC for cut-off value of CRP.
Ultrasound assessment
Vascular ultrasound
In the PMR–GCA-group, a mean of 8.61 (SD ± 3.14) vessels per patient was affected. No pathological vascular abnormality suggestive of GCA was identified in the PMR-group. The axillary arteries were affected in 82% (23/28) of the PMR–GCA patients, and the common branches of the superficial temporal arteries were affected in 71% (20/28). Every patient in this group presented with at least one elevated IMT value and pathological ultrasound morphology of either the axillary or superficial temporal artery. No correlation was found between the extent of cranial symptoms and involvement of cranial vessels. Table 2 displays the total numbers and frequencies of pathological arteries and the vasculitic affection in the PMR–GCA-group.
Table 2.
Absolute counts and relative frequencies of affected arteries and vasculitic affection.
| PMR–GCA-group (n = 28) | |
|---|---|
| Axillary artery | 23 (82%) |
| Carotid artery | 24 (86%) |
| Vertebral artery | 13 (46%) |
| Superficial temporal artery | 20 (71%) |
| TA frontal branch | 21 (75%) |
| TA parietal branch | 22 (78%) |
| Facial artery | 19 (68%) |
| Affection of extracranial arteries only | 1 (3.5%) |
| Affection of cranial arteries only | 1 (3.5%) |
| Affection of extracranial and cranial arteries | 26 (93%) |
TA, temporal artery; GCA, giant cell arteritis; PMR, polymyalgia rheumatica.
PMR–GCA-group: patients with diagnosis of PMR and GCA.
Musculoskeletal ultrasound
Table 3 displays the number of patients with joint effusion and the mean values of measured effusion in broadest extent and overall area. Figures 1 and 2 show the measuring techniques that were applied to assess joint or bursal effusions.
Table 3.
Ultrasound findings of the joints in each cohort.
| PMR-group (n = 32) | PMR–GCA-group (n = 28) | p value | |
|---|---|---|---|
| Mean values of joint effusions of the shoulder and hip joint | |||
| Effusion around the biceps tendon in longitudinal section, mean area (SD), cm2 | 0.161 (±0.11) | 0.266 (±0.24) | 0.07 |
| Effusion around the biceps tendon in transversal section, mean area (SD), cm2 | 0.13 (±0.09) | 0.17 (±0.13) | 0.18 |
| Glenohumeral effusion, mean area (SD), cm2 | 0.18 (±0.15) | 0.32 (±0.43) | 0.16 |
| Trochanteric effusion, mean area (SD), cm2 | 0.14 (±0.34) | 0.11 (±0.30) | 0.59 |
| Effusion of the hip joint, mean area (SD), cm2 | 0.11 (±0.10) | 0.23 (±0.29) | 0.04* |
| Effusion around the biceps tendon in longitudinal section, mean extent (SD), mm | 1.84 (±0.81) | 2.4 (±1.25) | 0.07 |
| Effusion around the biceps tendon in transversal section, mean extent (SD), mm | 2.36 (±1.59) | 3.02 (±1.65) | 0.18 |
| Glenohumeral effusion, mean extent (SD), mm | 6.41 (±2.86) | 8.40 (±4.70) | 0.07 |
| Trochanteric effusion, mean extent (SD), mm | 2.71 (±6.45) | 3.16 (±6.23) | 0.67 |
| Absolute counts and frequencies of patients having joint effusions of at least one side | |||
| Effusion of the biceps tendon | 28 (88%) | 21 (75%) | 0.61 |
| Glenohumeral effusion | 29 (91%) | 23 (82%) | 1 |
| Trochanteric effusion | 5 (15%) | 6 (21%) | 1 |
| Effusion of the hip joint | 31 (97%) | 26 (93%) | 0.60 |
GCA, giant cell arteritis; PMR, polymyalgia rheumatica; SD, standard deviation.
PMR-group: patients with diagnosis of PMR.
PMR–GCA-group: patients with diagnosis of PMR and GCA.
p ⩽ 0.05.
A higher proportion of patients in the PMR-group had effusions of the biceps tendon and the glenohumeral joint compared to the PMR–GCA-group (Table 2), but results were not significant (p > 0.05), while the mean values of the widest extent and total area were higher in the PMR–GCA-group than in the PMR-group (Table 2). Effusion of the trochanteric bursa was rare in both groups. Subacromial-subdeltoid bursitis was not found in any of the patients.
Differences in biceps, glenohumeral and trochanteric effusions were found to be not significant (p > 0.05) between the two groups. Results in overall area of hip joint effusion were found to be statistically significant (p = 0.04).
Discussion
The purpose of this study was to evaluate the prevalence of findings of LVV consistent with GCA in patients with newly diagnosed PMR using vascular ultrasound. In our study cohort, the prevalence of GCA was 46%. Importantly, in 13 patients (46%) of the PMR–GCA-group, GCA was only diagnosed by ultrasound as typical GCA symptoms were absent. Ultrasound characteristics that separated the two groups included vasculitis of either the temporal or axillary artery, the presence of effusions in the biceps tendon and glenohumeral joints which was higher for the PMR-group, and, the area of hip joint effusion which was relatively greater in the PMR–GCA-group. A CRP cut-off value of 26.5 mg/litre was found to distinguish patients with PMR from patients with PMR and GCA, with moderate sensitivity and specificity.
The diagnosis of PMR is a clinical one without any confirmatory test and the evaluation of suspected PMR requires consideration for several conditions, inflammatory and non-inflammatory, including GCA. In a retrospective study of patients with PMR, 7.4% developed GCA after an average of 27 months with 17% presenting with visual loss and 18% being diagnosed based on large-vessel imaging, highlighting the importance of early detection.24 Few imaging studies, mainly using PET, have evaluated the prevalence of subclinical GCA in patients being evaluated for a diagnosis of PMR with estimates of GCA ranging from 14 to 50%.5,25–29 One study evaluated the temporal arteries in 102 patients with PMR and found findings of concurrent active GCA in 8%.29
Compared to other studies, the prevalence of GCA in PMR patients was relatively high in our cohort. Our study is the first to date to include systematic ultrasound examinations of several vessels and joints in consecutive newly diagnosed PMR patients with very short or no GC intake, which may explain the high prevalence of abnormalities found. Another factor to consider is that about half of the patients were recruited directly at our university hospital, which might explain for the higher GCA prevalence in our patients. Furthermore, we scored every abnormal ultrasound finding as GCA based on established definitions, regardless of whether patients had GCA symptoms. We decided to not perform temporal artery biopsy in the asymptomatic patients of the cohort as it is invasive and often has little effect on diagnostic sensitivity.30 Furthermore, many patients also had involvement of the axillary arteries and it is unlikely that these were also false-positive results. No additional imaging was performed in these patients since ultrasound is the preferred imaging technique according to recent EULAR recommendations.13
In the PMR–GCA-group, every patient showed at least one pathological axillary or superficial temporal artery and most of the patients presented with both extracranial and cranial vasculitic affection. Other studies with bigger cohorts show that axillary and superficial temporal artery are the most commonly affected arteries in GCA.19,20 However, the prevalence of vasculitic affection of respective arteries observed was lower compared to our cohort. The majority of patients (78%) in the PMR–GCA-group presented with two or fewer characteristic GCA symptoms, while 46% were asymptomatic, suggesting a high proportion of subclinical GCA in PMR patients.
There is ongoing controversy about whether patients with these subclinical vascular abnormalities should be treated as GCA.6 It may be that the subset of patients with GCA, PMR is the presenting manifestation. In the clinical trial of tocilizumab in GCA, 23% of patients included with newly diagnosed disease and 20% of the population overall had symptoms of PMR alone.31 In this subset, of 51 patients, 18% had a positive biopsy and 82% had large-vessel imaging findings of vasculitis.31 Without vascular ultrasound examination, GCA would not have been identified in the 28 patients in our study. Using GC doses typically reserved for PMR and the potential for ischemic complications resulting from untreated GCA, especially in patients with temporal artery involvement, we decided to treat all these patients as GCA but whether this is the correct approach can only be addressed in a prospective, randomized clinical trial.6,24,32,33 During a 6-month follow-up period, only one of the patients from the PMR-group developed GCA, suggesting this was an effective method for early detection of patients with GCA.
However, a subset of patients in the PMR-group had symptoms of GCA, as headache or jaw claudication. These patients could be considered having undetected GCA. The ultrasound examination of the temporal artery is the gold standard according to the recent EULAR recommendations for imaging in LVV.13 We did not perform temporal artery biopsy in these patients. If ultrasound is negative, temporal artery biopsy would not have revealed more information, as we used an 18-MHz ultrasound probe revealing an image resolution of approximately 140 µm for the superficial temporal arteries and also were able to examine the superficial temporal artery in its full length using ultrasound. Ultrasound cut-off values together with the OMERACT ultrasound definitions,34 which were also applied, already displayed a sensitivity over 99% in a study performed by Schäfer et al.19
Joint effusions were found to be greater in extent in the PMR–GCA-group, while the frequency of joint effusions was higher in the PMR-group. Schmidt et al.35 examined shoulder joints of a comparable healthy control group. For effusions of the glenohumeral joint, an upper normal limit of 3.1 mm was defined. Compared to our cohort, the values for glenohumeral effusions were much higher in our population, with 6.41 mm in the PMR-group and 8.4 mm in the PMR–GCA-group, respectively. Furthermore, no effusions around the biceps tendon were described in this study, compared to a frequency of 88% (28/32) in the PMR-group and 75% (21/28) in the PMR–GCA-group in our cohort. In our cohort, no subacromial-subdeltoid bursitis was found in any of the patients. To date, there is no reliable data on the findings of subacromial-subdeltoid bursitis in PMR patients. The absence of this bursitis could be influenced by GC intake. However, the total amount and time of GC intake was very small in our cohort, in median 1.43 days in the PMR-group and 0.4 days in the PMR–GCA-group (Table 1). Another epidemiologic study of Gonzalez-Gay et al.36 proved that PMR together with GCA was a more severe disease compared to isolated PMR, with significant abnormalities in laboratory parameters and clinical symptoms.
Other studies, such as a comprehensive review by Mackie et al.,37 indicate a lower frequency of musculoskeletal abnormalities in PMR patients. The definition of joint effusions, however, differed throughout these studies. We did not use a cut-off value in our cohort to score joint effusions, but instead labelled every hypo- or anechoic structure detected in respective joints as an effusion. Furthermore, the patients were checked at the time of initial diagnosis with extremely little GC intake and shortly after the onset of symptoms, which limits the impact of treatment and symptom duration on our findings.
Laboratory parameters that may distinguish patients with PMR from those who may also have concurrent GCA are currently unknown. Based on our findings, we established a CRP cut-off value to discriminate between patients with PMR only and patients with PMR and GCA. The cut-off value was set at 26.5 mg/litre, offering moderate sensitivity and specificity. Van Sleen et al.38 also found angiopoietin-2 to be another reliable laboratory marker for GCA offering good sensitivity and specificity. However, this marker is rarely examined in daily clinical practice; therefore, the CRP cut-off value together with clinical parameters and ultrasound findings may be helpful to discriminate between PMR and GCA, although CRP elevation can often be unspecific. Furthermore, no ESR was evaluated in this study. A study performed by Kermani et al.12 proved that additional evaluation of ESR does not improve diagnostic specificity compared to the evaluation of CRP alone, so we decided to not evaluate ESR in this study.
The strengths of our study include the prospective study design with standardized data collection. All patients in the study were on GC treatment for less than 7 days which should minimize the impact of treatment on ultrasound findings. There was systematic and comprehensive ultrasound evaluation which included the shoulders and hips in addition to examining multiple arterial beds. Finally, we also re-evaluated the diagnosis of PMR at 6 months. Our study has few limitations to consider. The lack of a control group without PMR leaves the comparison of our findings to healthy subjects open. We did not compare our findings of vasculitic affection in the PMR–GCA-group to patients with GCA only. Therefore, it is unknown, whether patients with PMR and GCA present with a different pattern of affected arteries compared to patients with GCA only. The aorta also was not assessed and therefore, the prevalence of asymptomatic aortitis could not be evaluated. Furthermore, the number of the patients in our study is rather small compared to other studies, keeping in mind that most of the other studies were retrospective. We only included patients with little to no GC intake, which significantly reduced the number of eligible patients. Our study cohort can be considered representative due to the referral of patients from local rheumatologists and general practitioners, although it might be biased by patients presenting directly to our university hospital in case of severe symptoms.
Conclusion
The overall prevalence of GCA in our cohort of consecutive newly diagnosed PMR patients was 46%. The extent of joint effusions was relatively higher in patients with PMR and GCA compared to patients with PMR only, but only significant for the hip joint.
The diagnosis of GCA could only be determined by vascular ultrasound in a significant number of our patients (46%) who had PMR and GCA. Until previously, vascular ultrasound examinations in PMR patients remained infrequent. For everyday clinical practice, our results demonstrate that a routine ultrasound assessment of a core set of extracranial vessels, particularly the axillary and temporal arteries, which were affected in all of our patients, is advised to rule out the presence of subclinical GCA. Furthermore, a CRP cut-off value was calculated to discriminate between patients with PMR and patients with PMR and GCA, which can assist in distinguishing patients with PMR from those with GCA and PMR.
As we examined a cohort with definitive diagnosis of PMR with very short GC treatment, our study could already lead to a different approach in PMR patients, scanning every PMR patient for the presence of GCA. Further studies with larger cohorts are needed to confirm this observation and validate the proposed CRP cut-off value.
Acknowledgments
The authors thank all general practitioners and local rheumatologists for referral of a part of the patients included in this study. They thank all patients for participating.
Footnotes
ORCID iDs: Lara C. Burg  https://orcid.org/0000-0002-5379-9149
https://orcid.org/0000-0002-5379-9149
Pantelis Karakostas
https://orcid.org/0000-0001-8421-2745
Tanaz A. Kermani
https://orcid.org/0000-0002-7335-7321
Valentin S. Schäfer
https://orcid.org/0000-0002-6591-5936
Contributor Information
Lara C. Burg, Clinic of Internal Medicine III, Department of Oncology, Haematology, Rheumatology and Clinical Immunology, University Hospital Bonn, Venusberg-Campus 1, 53127 Bonn, Germany.
Pantelis Karakostas, Clinic of Internal Medicine III, Department of Oncology, Haematology, Rheumatology and Clinical Immunology, University Hospital Bonn, Bonn, Germany.
Charlotte Behning, Institute of Medical Biometry, Informatics and Epidemiology, University Hospital Bonn, Bonn, Germany.
Peter Brossart, Clinic of Internal Medicine III, Department of Oncology, Haematology, Rheumatology and Clinical Immunology, University Hospital Bonn, Bonn, Germany.
Tanaz A. Kermani, Division of Rheumatology, David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, CA, USA
Valentin S. Schäfer, Clinic of Internal Medicine III, Department of Oncology, Haematology, Rheumatology and Clinical Immunology, University Hospital Bonn, Bonn, Germany
Declarations
Ethics approval and consent to participate: The study was conducted in accordance with the Declaration of Helsinki and was reviewed and approved by the Ethics Committee of the University Hospital Bonn, Germany (Lfd. Nr.097/18). Written informed consent was obtained from every patient prior to inclusion.
Consent of publication: Not applicable.
Author contributions: Lara C. Burg: Conceptualization; Data curation; Formal analysis; Methodology; Project administration; Validation; Writing – original draft; Writing – review & editing.
Pantelis Karakostas: Methodology; Writing – review & editing.
Charlotte Behning: Data curation; Formal analysis; Methodology; Software; Writing – review & editing.
Peter Brossart: Methodology; Writing – review & editing.
Tanaz A. Kermani: Conceptualization; Methodology; Writing – review & editing.
Valentin S. Schäfer: Conceptualization; Data curation; Investigation; Methodology; Project administration; Supervision; Validation; Writing – review & editing.
Funding: The authors received no financial support for the research, authorship, and/or publication of this article.
TAK is a chairperson in a safety board for Abatacept for giant cell arteritis. All other authors declare no conflicts of interests.
Availability of data and materials: The full de-identified patient data and study protocol will be available on approval of a reasonable request and may only be used for the analysis mentioned in the request. Requests should be addressed to the corresponding author.
References
- 1. Gonzalez-Gay MA, Vazquez-Rodriguez TR, Lopez-Diaz MJ, et al. Epidemiology of giant cell arteritis and polymyalgia rheumatica. Arthritis Rheum 2009; 61: 1454–1461. [DOI] [PubMed] [Google Scholar]
- 2. Dejaco C, Brouwer E, Mason JC, et al. Giant cell arteritis and polymyalgia rheumatica: current challenges and opportunities. Nat Rev Rheumatol 2017; 13: 578–592. [DOI] [PubMed] [Google Scholar]
- 3. Warrington KJ, Matteson EL. Management guidelines and outcome measures in giant cell arteritis (GCA). Clin Exp Rheumatol 2007; 25(Suppl. 47): 137–141. [PubMed] [Google Scholar]
- 4. Dejaco C, Duftner C, Dasgupta B, et al. Polymyalgia rheumatica and giant cell arteritis: management of two diseases of the elderly. Aging Health 2011; 7: 633–645. [Google Scholar]
- 5. Henckaerts L, Gheysens O, Vanderschueren S, et al. Use of 18F-fluorodeoxyglucose positron emission tomography in the diagnosis of polymyalgia rheumatica –a prospective study of 99 patients. Rheumatology 2018; 57: 1908–1916. [DOI] [PubMed] [Google Scholar]
- 6. Dejaco C, Duftner C, Buttgereit F, et al. The spectrum of giant cell arteritis and polymyalgia rheumatica: revisiting the concept of the disease. Rheumatology 2017; 56: 506–515. [DOI] [PubMed] [Google Scholar]
- 7. Koster MJ, Matteson EL, Warrington KJ. Large-vessel giant cell arteritis: diagnosis, monitoring and management. Rheumatology 2018; 57(Suppl. 2): ii32–ii42. [DOI] [PubMed] [Google Scholar]
- 8. Floris A, Piga M, Chessa E, et al. Long-term glucocorticoid treatment and high relapse rate remain unresolved issues in the real-life management of polymyalgia rheumatica: a systematic literature review and meta-analysis. Clin Rheumatol 2021; 41: 19–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. González-Gay MA, Matteson EL, Castañeda S. Polymyalgia rheumatica. Lancet 2017; 390: 1700–1712. [DOI] [PubMed] [Google Scholar]
- 10. Robinette ML, Rao DA, Monach PA. The immunopathology of giant cell arteritis across disease spectra. Front Immunol 2021; 12: 623716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Ling ML, Yosar J, Lee BW, et al. The diagnosis and management of temporal arteritis. Clin Exp Optom 2020; 103: 572–582. [DOI] [PubMed] [Google Scholar]
- 12. Kermani TA, Schmidt J, Crowson CS, et al. Utility of erythrocyte sedimentation rate and C-reactive protein for the diagnosis of giant cell arteritis. Semin Arthritis Rheum 2012; 41: 866–871. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Dejaco C, Ramiro S, Duftner C, et al. EULAR recommendations for the use of imaging in large vessel vasculitis in clinical practice. Ann Rheum Dis 2018; 77: 636–643. [DOI] [PubMed] [Google Scholar]
- 14. Camellino D, Cimmino MA. Imaging of polymyalgia rheumatica: indications on its pathogenesis, diagnosis and prognosis. Rheumatology 2012; 51: 77–86. [DOI] [PubMed] [Google Scholar]
- 15. Dasgupta B, Cimmino MA, Maradit-Kremers H, et al. 2012 provisional classification criteria for polymyalgia rheumatica: a European League Against Rheumatism/American College of Rheumatology collaborative initiative. Ann Rheum Dis 2012; 71: 484–492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Figus FA, Skoczyńska M, McConnell R, et al. Imaging in polymyalgia rheumatica: which technique to use? Clin Exp Rheumatol 2021; 39: 883–888. [PubMed] [Google Scholar]
- 17. Karakostas P, Dejaco C, Behning C, et al. Point-of-care ultrasound enables diagnosis of giant cell arteritis with a modern innovative handheld probe. Rheumatology 2021; 60: 4434–4436. [DOI] [PubMed] [Google Scholar]
- 18. Chrysidis S, Duftner C, Dejaco C, et al. Definitions and reliability assessment of elementary ultrasound lesions in giant cell arteritis: a study from the OMERACT Large Vessel Vasculitis Ultrasound Working Group. RMD Open 2018; 4: e000598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Schäfer VS, Juche A, Ramiro S, et al. Ultrasound cut-off values for intima-media thickness of temporal, facial and axillary arteries in giant cell arteritis. Rheumatology 2017; 56: 1479–1483. [DOI] [PubMed] [Google Scholar]
- 20. Ješe R, Rotar Tomšič ŽM, Hočevar A. The cut-off values for the intima-media complex thickness assessed by colour Doppler sonography in seven cranial and aortic arch arteries. Rheumatology 2021; 60: 1346–1352. [DOI] [PubMed] [Google Scholar]
- 21. Bosch P, Dejaco C, Schmidt WA, et al. Ultrasound for diagnosis and follow-up of chronic axillary vasculitis in patients with long-standing giant cell arteritis. Ther Adv Musculoskelet Dis 2021; 13: 1759720X21998505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Bossuyt PM, Reitsma JB, Bruns DE, et al. STARD 2015: an updated list of essential items for reporting diagnostic accuracy studies. BMJ 2015; 351: h5527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Schäfer VS, Chrysidis S, Schmidt WA, et al. OMERACT definition and reliability assessment of chronic ultrasound lesions of the axillary artery in giant cell arteritis. Semin Arthritis Rheum 2021; 51: 951–956. [DOI] [PubMed] [Google Scholar]
- 24. Liozon E, de Boysson H, Dalmay F, et al. Development of giant cell arteritis after treating polymyalgia or peripheral arthritis: a retrospective case-control study. J Rheumatol 2018; 45: 678–685. [DOI] [PubMed] [Google Scholar]
- 25. Moosig F, Czech N, Mehl C, et al. Correlation between 18-fluorodeoxyglucose accumulation in large vessels and serological markers of inflammation in polymyalgia rheumatica: a quantitative PET study. Ann Rheum Dis 2004; 63: 870–873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Camellino D, Paparo F, Morbelli SD, et al. Clinical and FDG-PET/CT correlates in patients with polymyalgia rheumatica. Clin Exp Rheumatol 2022; 40: 78–85. [DOI] [PubMed] [Google Scholar]
- 27. Prieto -Peña D, Martínez -Rodríguez I, Loricera J, et al. Predictors of positive 18F-FDG PET/CT-scan for large vessel vasculitis in patients with persistent polymyalgia rheumatica. Semin Arthritis Rheum 2019; 48: 720–727. [DOI] [PubMed] [Google Scholar]
- 28. Yamashita H, Kubota K, Takahashi Y, et al. Whole-body fluorodeoxyglucose positron emission tomography/computed tomography in patients with active polymyalgia rheumatica: evidence for distinctive bursitis and large-vessel vasculitis. Mod Rheumatol 2012; 22: 705–711. [DOI] [PubMed] [Google Scholar]
- 29. Schmidt WA, Gromnica-Ihle E. Incidence of temporal arteritis in patients with polymyalgia rheumatica: a prospective study using colour Doppler ultrasonography of the temporal arteries. Rheumatology 2002; 41: 46–52. [DOI] [PubMed] [Google Scholar]
- 30. Luqmani R, Lee E, Singh S, et al. The role of ultrasound compared to biopsy of temporal arteries in the diagnosis and treatment of giant cell arteritis (TABUL): a diagnostic accuracy and cost-effectiveness study. Health Technol Assess 2016; 20: 1–238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Tuckwell K, Collinson N, Dimonaco S, et al. Newly diagnosed vs. relapsing giant cell arteritis: baseline data from the giacta trial. Semin Arthritis Rheum 2017; 46: 657–664. [DOI] [PubMed] [Google Scholar]
- 32. Clifford AH, Cohen Tervaert JW. Cardiovascular events and the role of accelerated atherosclerosis in systemic vasculitis. Atherosclerosis 2021; 325: 8–15. [DOI] [PubMed] [Google Scholar]
- 33. Hernández-Rodríguez J, Font C, García-Martínez A, et al. Development of ischemic complications in patients with giant cell arteritis presenting with apparently isolated polymyalgia rheumatica: study of a series of 100 patients. Medicine 2007; 86: 233–241. [DOI] [PubMed] [Google Scholar]
- 34. Schäfer VS, Chrysidis S, Dejaco C, et al. Assessing vasculitis in giant cell arteritis by ultrasound: results of OMERACT patient-based reliability exercises. J Rheumatol 2018; 45: 1289–1295. [DOI] [PubMed] [Google Scholar]
- 35. Schmidt WA, Schicke B, Krause A. Schultergelenkerguss: welcher ultraschallschnitt ist der beste? Ultraschall Med 2008; 29(Suppl. 5): 250–255. [DOI] [PubMed] [Google Scholar]
- 36. González-Gay MA, García-Porrúa C, Vázquez-Caruncho M. Polymyalgia rheumatica in biopsy proven giant cell arteritis does not constitute a different subset but differs from isolated polymyalgia rheumatica. J Rheumatol 1998; 25: 1750–1755. [PubMed] [Google Scholar]
- 37. Mackie SL, Koduri G, Hill CL, et al. Accuracy of musculoskeletal imaging for the diagnosis of polymyalgia rheumatica: systematic review. RMD Open 2015; 1: e000100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. van Sleen Y, Boots AMH, Abdulahad WH, et al. High angiopoietin-2 levels associate with arterial inflammation and long-term glucocorticoid requirement in polymyalgia rheumatica. Rheumatology 2020; 59: 176–184. [DOI] [PubMed] [Google Scholar]