

Highlights
-
•
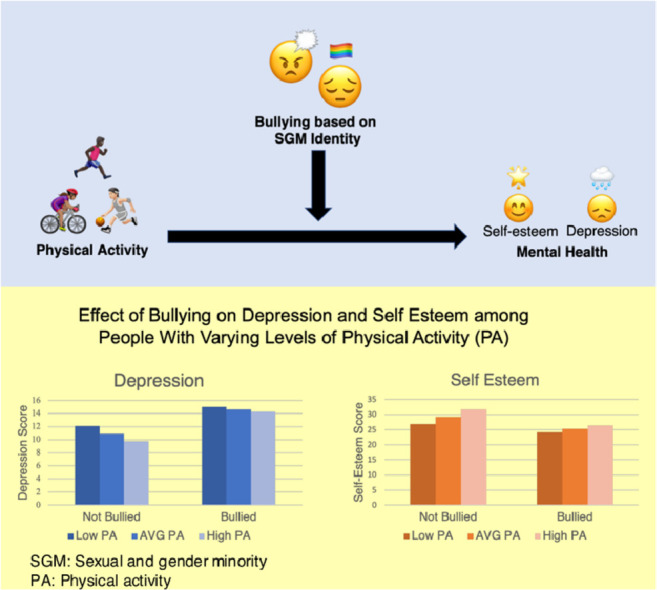
Bullying based on youth's sexual and gender identity is positively associated with depression and negatively associated with self-esteem.
-
•
Physical activity is associated with better mental health but only in non-bullied sexual and gender minority youth.
-
•
Bullying history should be addressed if seeking to implement physical activity interventions to improve mental health among sexual and gender minority youth.
Keywords: Bullying, Depression, Exercise, LGBTQ, Self-esteem, Youth
Abstract
Background
Sexual and gender minority youth frequently experience bullying, which often contributes to higher depressive symptoms and lower self-esteem. Given that physical activity (PA) can mitigate depressive symptoms and improve self-esteem, we examined the moderating effect of PA on the relationship between bullying and mental health among sexual and gender minority youth.
Methods
Data from the Lesbian, Gay, Bisexual, Transgender, and Queer National Teen Survey (n = 9890) were analyzed. Hierarchical regression analyses examined the influence of history and frequency of being bullied, PA, and the interaction of these variables on depressive symptoms and self-esteem. Simple slopes analyses were used to probe significant interactions.
Results
Results indicated the importance of accounting for bullying history when examining effects of PA on mental health. PA was negatively related to depression (t = –4.18, p < 0.001) and positively related to self-esteem (t = 12.11, p < 0.001). Bullying frequency was positively related to depression (t = 19.35, p < 0.001) and negatively related to self-esteem (t = –12.46, p < 0.001). There was a significant interaction between bullying frequency and PA for depression (t = 4.45, p < 0.001) and self-esteem (t = –4.69, p < 0.001). Post hoc analyses suggested that the positive effects of PA on mental health may be limited to those not bullied because it had a negligible effect on those who were bullied.
Conclusion
Results suggest that sexual and gender minority youth exercise interventions aiming to improve mental health should first address bullying history; otherwise, their effectiveness may be limited to those who have been bullied.
Graphical abstract
1. Introduction
Sexual and gender minority (SGM) students, or those identifying as lesbian, gay, bisexual, transgender, and questioning (LGBTQ), are significantly more at risk for bullying, teasing, perceived discrimination, and violent events than their non-LGBTQ peers.1, 2, 3, 4 Despite a decline in school-related violence victimization over the past 20 years, rates of LGBTQ students being bullied at school have not declined.5 One study of LGBTQ students found that a majority were harassed at school based on their sexual orientation and over half were harassed based on gender identity.2 In the same study, nearly half of LGBTQ students reported that they had experienced cyberbullying, or harassment on the Internet, in the past year.2 Bullying based on sexual orientation and gender identity continues to be a significant problem for LGBTQ youth and can impact their mental health. Given the potential mental health impacts of bullying, it is worth exploring how physical activity (PA) can improve depression and self-esteem among this vulnerable population.
1.1. The minority stress model and effects of discrimination on mental health
The minority stress model posits that LGBTQ individuals face higher levels of mental health disorders than non-LGBTQ individuals, in part due to the social stressors from stigma and prejudice related to being LGBTQ.6 Furthermore, the minority stress model categorizes LGBTQ-specific prejudice into multiple categories, which include external prejudice events such as discrimination or violence and expectations of these events.3,6 Not only does being bullied contribute to poorer mental health, but it can also contribute to worry about bullying occurring again.
Perceived discrimination and bullying based on sexual orientation are associated with increased depressive symptoms.1,3,4 More specifically, bullying has been found to contribute to LGBTQ youth suicidal tendencies and lack of school belongingness.7, 8, 9 LGBTQ youth who experience higher levels of victimization based on their sexual orientation report higher levels of depression than their LGBTQ peers who report lower levels of victimization, suggesting that the more victimization they face, the more severe depression they experience.2 Negative self-schemas and low self-esteem may also result from stigma-related stress, which can contribute to depression in minority groups.10 Being bullied and frequency of being bullied negatively impact LGBTQ youth's mental health.
High self-esteem has been shown to be a protective factor against depression and suicidal tendencies in LGBTQ youth.1,7 However, many LGBTQ youth report lower levels of self-esteem compared to their non-LGBTQ peers.11,12 LGBTQ youth who report higher levels of in-school victimization and discrimination based on sexual orientation and gender expression report lower levels of self-esteem compared to both their heterosexual peers and LGBTQ peers who had not experienced victimization or discrimination.2,13 Given that bullying based on being LGBTQ can lead to poor mental health, it is imperative to explore the relationships among bullying, exercise, and mental health for this vulnerable population.
1.2. PA
PA has been shown to reduce feelings of sadness and depression and increase self-esteem in adolescents.14, 15, 16, 17, 18, 19 One systematic review found a medium effect size (d = –0.50) for exercise on depression among youth and a small-to-medium effect size (d = –0.48) for exercise on clinical depression among youth.20 For youth, participation in physical education classes has been associated with a lower risk of sadness.15 Importantly, for LGBTQ youth, participation in sports can contribute to decreased feelings of hopelessness.21 Exercise has also been shown to have a positive effect on self-esteem among healthy adolescents.22 A recent meta-analysis found small-to-medium effect sizes for PA interventions on both self-concept (Hedges’ g = 0.49) and self-worth (Hedges’ g = 0.31).23 Despite the multiple benefits of PA, many youths are insufficiently active.24 The U.S. Department of Health and Human Services recommends that youth ages 5‒17 years engage in at least 60 min of PA daily.25 Many LGBTQ youth are insufficiently active and report engaging in less moderate-to-vigorous PA in general than their heterosexual peers.26 This could be due to their lower levels of athletic self-esteem or a reluctance to engage in sports due to feelings of exclusion, isolation, or unsafety because of their sexual orientation or gender identity.2,26,27 The benefits of PA for improving mental health in a diverse range of populations is well established; therefore, it is worth exploring how PA may influence depression among LGBTQ youth.
1.3. The current study
Previous research has established that PA can reduce depression symptoms and increase self-esteem in many populations, including high school youth. The links between perceived discrimination, bullying, and teasing based on SGM identity and mental health is also well established. However, to the best of our knowledge, no studies have examined the effect that PA has on the relationship between bullying based on SGM identity and depression and self-esteem.
In order to bridge this gap, this study used a large national sample of SGM youth to better understand the moderating effect of PA on the relationship between bullying and depression and between bullying and self-esteem in SGM youth. This study tested the following hypotheses: (1) bullying based on being SGM would be positively related to depression severity and negatively related to self-esteem; (2) PA levels would be negatively related to depression severity and positively related to self-esteem; and (3) PA would moderate the effect of bullying on depression and self-esteem such that, as levels of PA increase, the relationships between bullying and depression and bullying and self-esteem would be weakened. The term “SGM youth” will be used henceforth to describe the population studied here. “LGBTQ” will still be used to describe previous research that used this terminology.
2. Methods
2.1. Procedures
This study used data from the LGBTQ National Teen Survey, a nationwide survey assessing health behaviors, school experiences, victimization, and family relationships of SGM adolescents in the United States. Data were collected through an anonymous online survey on Qualtrics.com. Recruitment of SGM adolescents took place on Twitter, Instagram, SnapChat, Reddit, and Facebook. Social media influencers shared the survey, and the Human Rights Campaign shared the link with their community partners. Eligible participants were between 13 and 17 years old, resided in the United States at the time they took the survey, and were English-speaking. Participants were offered a chance to win a gift card to a popular online retailer for completing the survey, and all participants could receive Human Rights Campaign wristbands. The University of Connecticut Institutional Review Board approved all study protocols. Online informed assent was obtained from all youth participants in the study. A waiver of parental consent related to this study was obtained from the Institutional Review Board.
Further details about recruitment, data collection, screening procedures, and the sample composition are reported elsewhere.28 The full sample for this survey as originally collected was n = 17,112; however, in this study we limited the sample to those who responded to at least one of the survey items related to bullying, resulting in a sample size of n = 9890. All demographic data and results are based on this limited sample.
2.2. Measures
2.2.1. Demographics
For this analysis, participants’ sexual orientation, gender identity, sex assigned at birth, age, race/ethnicity, and body mass index (BMI) (calculated from reported height and weight) were included. For gender identity and race/ethnicity, participants could choose all options that applied.
For sexual orientation, participants were asked “How do you describe your sexual identity?” Participants chose one of the following: “gay or lesbian”, “bisexual”, “straight, that is, not gay”, or “something else”. If a participant chose “something else”, the options of “queer”, “pansexual”, “asexual”, “questioning”, or “other” were presented. Participants who chose “other” were presented with an open-ended text entry. For this analysis, all text entries were labeled as “other”.
To assess gender identity, participants were asked “What is your current gender identity?” Participants could select “Male”, “Female”, “Trans male/Trans boy”, “Trans female/Trans girl”, “Non-binary”, “Genderqueer/Gender non-conforming”, or “Different identity”. If participants selected “Different identity”, they were prompted to write in their gender identity. Participants were asked “What sex were you assigned at birth?” and were given the choices “Male” or “Female”. For this analysis, a new variable with the categories “Cis-male”, “Cis-female”, “Trans male/Trans boy”, “Trans female/Trans girl”, “assigned male at birth (AMAB)/Non-binary”, and “assigned female at birth (AFAB)/Non-binary” was created. Participants categorized as “Cis-male” and “Cis-female” selected a gender identity that was congruent with their sex assigned at birth.
2.2.2. PA
PA was measured using the Godin Leisure-Time Exercise Questionnaire, a common self-report measure of PA that has been tested on and published about in studies with adolescent populations.29, 30, 31 Participants indicated how many times per week they engaged in strenuous, moderate, and mild exercise for a period of 15 min or more, with definitions provided for each category (mild exercise is minimal effort activity, moderate exercise is activity that is not exhausting, and strenuous exercise is activity where one's heart beats rapidly). Response choices included “never”, “1‒2 times a week”, “3‒4 times a week”, and “5 or more times a week”. A PA score was calculated by multiplying the frequency of each level of exercise (Never = 0, 1‒2 times = 1, 3‒4 times = 2, 5 or more times = 3) by metabolic equivalent values for each level of activity and summing the products of each component (3 × mild + 5 × moderate + 9 × strenuous = leisure-time PA score).29,30 This scale has been used across multiple studies and has demonstrated consistent concurrent validity.32,33
2.2.3. Depression
Depression was measured using the Kutcher Adolescent Depression Scale 11,34,35 an 11-item self-report instrument that measures frequency of depression symptoms in adolescents aged 12‒17 years. Items included statements such as “Irritable, losing your temper easily, feeling pissed off, losing it”, and “Feelings of worthlessness, hopelessness, letting people down, not being a good person”. Respondents indicated the frequency over the past week that they experienced each statement on a 4-point scale: 0 (hardly ever), 1 (much of the time), 2 (most of the time), and 3 (all of the time). A single item asking about self-harm and suicide was excluded from this survey in order to waive parental consent. Responses were summed (Cronbach's α = 0.90), and scores could range from 0 to 30, with higher scores indicating more depression symptoms. The scale as designed does not categorize participants based on specific ranges of scores.
2.2.4. Self-esteem
Self-esteem was measured using 18 items from 3 scales. Facets of multiple scales that assessed both self-esteem and beliefs about control over life experiences were combined to form a more comprehensive measure. All items from the Rosenburg Self-Esteem Scale, which is the most commonly used for scale for self-esteem in LGBTQ youth, were used and included statements such as “All in all, I am inclined to feel that I am a failure” and “I take a positive attitude towards myself”.36 The majority of items from the Pearlin Mastery Scale and 2 items from the Levenson Multidimensional Locus of Control Scale were used.37,38 Respondents indicated how much they agreed with each statement on a 4-point scale: 0 (strongly disagree), 1 (disagree), 2 (agree), and 3 (strongly agree). Some items were reverse scored. Total scores were calculated by summing all items, and higher scores indicated higher self-esteem (possible range 0‒54). Because multiple scales were combined, there are no standardized diagnostic cut-offs for specific scores. Cronbach's α for the 18 self-esteem items was 0.91.
2.2.5. Bullying
Bullying was measured with 2 items. Participants were asked, “Have you ever been teased or bullied because of your actual or perceived LGBTQ identities at school?” Answer choices included “Yes, because I am LGBTQ and I have told others”, “Yes, because someone thought I was LGBTQ”, and “No”. For this analysis, the first 2 choices were condensed to “Yes” to make the response dichotomous. If participants responded “Yes” to the first question, then a second question to assess for frequency of bullying in the past year was displayed: “Has this happened to you within the past year?” Response choices ranged from Never = 0 to Very Often = 4. Only 2 items were selected due to lack of consensus on a multi-item scale that is universally applied to measure bullying, as well as survey space limitations.
2.2.6. Statistical analyses
Data were analyzed using SPSS Version 26.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were calculated for sexual orientation, gender identity, race/ethnicity, age (birth year), and BMI. Multiple regression analyses were performed to examine predictors of depression and self-esteem, with the independent variables of level of PA, bullying based on being LGBTQ, and the interaction of these 2 variables. These regression analyses all contained several demographic variables used as controls, including sexual orientation, gender identity, race/ethnicity, age, and BMI. All categorical variables that were non-dichotomous were dummy coded. There was no dummy coding for race/ethnicity and gender identity because participants could select multiple options. Analyses were first run to examine the effect of PA on depression and self-esteem. Next, the impact of bullying (independent of PA) was examined by including either the variable of whether or not participants had ever been bullied or how frequently they had been bullied in the past year. To examine the moderating effect of PA on the relationship between bullying and mental health, analyses were run containing the independent variables of PA, bullying (whether or not respondents had ever been bullied or how frequently they were bullied in the past year), and an interaction term created by multiplying one of the bullying variables (having ever been bullied and frequency of bullying in the past year) with PA. All continuous variables were mean centered, and all variables met multicollinearity assumptions. Simple slopes analyses were completed to obtain further detail about any significant interactions found.
3. Results
Demographic information (n = 9890) is listed in Table 1. The most common sexual orientations were gay/lesbian (38.2%) and bisexual (33.5%). The sample was predominantly White (76.2%), with 16.2% identifying as Hispanic/Latino, 8.5% as African American, 7.2% as Asian American, 4.2% as American Indian or Alaskan Native, and 3.4% as other.
Table 1.
Sample demographics and baseline measures.
| n | % | |
|---|---|---|
| Age (year) | ||
| 13 | 733 | 7.4 |
| 14 | 1443 | 14.6 |
| 15 | 2041 | 20.6 |
| 16 | 2575 | 26.0 |
| 17 | 3098 | 31.3 |
| Race | ||
| White | 7538 | 76.2 |
| Black | 845 | 8.5 |
| American Indian/Alaska Native | 417 | 4.2 |
| Asian American | 711 | 7.2 |
| Hispanic/Latino | 1591 | 16.2 |
| Other | 340 | 3.4 |
| Sexual orientation | ||
| Gay/lesbian | 3782 | 38.2 |
| Bisexual | 3311 | 33.5 |
| Heterosexual | 158 | 1.6 |
| Something else | 2639 | 26.7 |
| Queer | 402 | 4.1 |
| Pansexual | 1292 | 13.1 |
| Asexual | 451 | 4.6 |
| Questioning | 217 | 2.2 |
| Other | 276 | 2.8 |
| Did not specify | 1 | <0.1 |
| Gender identity | ||
| Cis-male | 2276 | 23.0 |
| Cis-female | 4273 | 42.8 |
| Trans-male | 849 | 8.6 |
| Trans-female | 113 | 1.1 |
| AMAB/NB | 255 | 2.6 |
| AFAB/NB | 2160 | 21.8 |
| Sex assigned at birth | ||
| Male | 2644 | 26.7 |
| Female | 7246 | 73.3 |
| Bullying in last year | 6458 | 65.3 |
Note: Some categories do not total 100% (9890) because of rounding (age, gender identity) or respondents could select multiple options (race, sexual orientation).
Abbreviations: AFAB = assigned female at birth; AMAB = assigned male at birth; NB = non-binary.
Depression scores ranged from 0 to 30 (13.36 ± 7.61, mean ± SD), and self-esteem scores ranged from 0 to 54 (26.46 ± 10.15). PA scores ranged from 0 to 51 (19.33 ± 13.48). Only 14.3% of the sample reported engaging in moderate or strenuous PA for at least 6 days per week, suggesting that the majority of the sample did not meet suggested PA guidelines for adolescents.25 More than 18% reported engaging in no moderate or strenuous PA each week. Almost two-thirds of participants (65.3%) reported ever being teased or bullied due to being LGBTQ. The average frequency of bullying in the past year was 1.92 ± 1.11, which indicates that for those students who were bullied in past year, most reported being bullied “sometimes”.
Regression results are provided in Table 2, Table 3, Table 4, Table 5 and are discussed in further details in the sections below. To improve readability, these tables only include standardized estimates and statistical significance for each predictor; full regression tables are available upon request. Many demographic variables were consistently related to the outcomes across the various models. For sexual orientation, individuals who identified as bisexual, pansexual, and asexual frequently had significantly higher depression scores and lower self-esteem scores compared to people who identified as gay/lesbian. Conversely, individuals who identified as straight had statistically lower depression scores and higher self-esteem scores. For gender identity, cis-males had significantly lower depression scores and higher self-esteem scores than all other gender identities (cis-females, trans-males, trans-females, and those who identify as non-binary). American Indian, Hispanic/Latino, and other individuals had higher depression scores, and Asian American individuals had consistently lower self-esteem scores. As BMI increased, participants had significantly higher depression scores and lower self-esteem scores. Finally, as age increased, individuals had higher depression scores and lower self-esteem scores.
Table 2.
Summary of regression analysis (β) for the effects of physical activity, ever being bullied, and their interaction on depression.
| Variable | Model 1 | Model 2 | Model 3 |
|---|---|---|---|
| Sexual orientation (Ref. = gay/lesbian) | |||
| Bisexual | 0.049⁎⁎⁎ | 0.029* | 0.047⁎⁎⁎ |
| Straight | –0.029⁎⁎ | –0.034⁎⁎ | –0.027⁎⁎ |
| Queer | –0.002 | –0.007 | –0.003 |
| Pansexual | 0.062⁎⁎⁎ | 0.051⁎⁎⁎ | 0.060⁎⁎⁎ |
| Asexual | 0.037⁎⁎ | 0.018 | 0.036⁎⁎ |
| Questioning | 0.014 | 0.003 | 0.014 |
| Other | 0.038⁎⁎⁎ | 0.034⁎⁎ | 0.037⁎⁎⁎ |
| BMI | 0.096⁎⁎⁎ | 0.099⁎⁎⁎ | 0.091⁎⁎⁎ |
| Gender identity (Ref. = cis-male) | |||
| Cis-female | 0.181⁎⁎⁎ | 0.137⁎⁎⁎ | 0.177⁎⁎⁎ |
| Trans-male | 0.223⁎⁎⁎ | 0.238⁎⁎⁎ | 0.220⁎⁎⁎ |
| Trans-female | 0.047⁎⁎⁎ | 0.046⁎⁎⁎ | 0.045⁎⁎⁎ |
| AMAB/NB | 0.288⁎⁎⁎ | 0.295⁎⁎⁎ | 0.282⁎⁎⁎ |
| AFAB/NB | 0.061⁎⁎⁎ | 0.068⁎⁎⁎ | 0.059⁎⁎⁎ |
| Race/ethnicity | |||
| White | –0.031* | –0.016 | –0.027 |
| African American | 0.013 | 0.008 | 0.012 |
| Native American | 0.035⁎⁎ | 0.044⁎⁎⁎ | 0.036⁎⁎⁎ |
| Asian American | 0.019 | 0.010 | 0.020 |
| Hispanic/Latino | 0.029* | 0.031* | 0.028* |
| Other | 0.027⁎⁎ | 0.035⁎⁎ | 0.029⁎⁎ |
| Age (year) | 0.043⁎⁎⁎ | 0.057⁎⁎⁎ | 0.047⁎⁎⁎ |
| Physical activity | –0.043⁎⁎⁎ | – | –0.112⁎⁎⁎ |
| Ever bullied | 0.211⁎⁎⁎ | 0.216⁎⁎⁎ | |
| Ever bullied × physical activity | 0.069⁎⁎⁎ | ||
| Adjusted R2 | 0.122 | 0.160 | 0.165 |
| Overall model significance | F(21, 8426) = 56.68⁎⁎⁎ | F(21, 8426) = 77.80⁎⁎⁎ | F(23, 8424) = 73.47⁎⁎⁎ |
p < 0.05,
p < 0.01,
p < 0.001.
Abbreviations: AFAB = assigned female at birth; AMAB = assigned male at birth; BMI = body mass index; NB = non-binary; Ref. = reference.
Table 3.
Summary of regression analysis (β) for the effects of physical activity, ever being bullied, and their interaction on self-esteem.
| Variable | Model 1 | Model 2 | Model 3 |
|---|---|---|---|
| Sexual orientation (Ref. = gay/lesbian) | |||
| Bisexual | –0.044⁎⁎⁎ | –0.060⁎⁎⁎ | –0.058⁎⁎⁎ |
| Straight | 0.043⁎⁎⁎ | 0.043⁎⁎⁎ | 0.036⁎⁎ |
| Queer | –0.002 | –0.008 | –0.005 |
| Pansexual | –0.068⁎⁎⁎ | –0.077⁎⁎⁎ | –0.075⁎⁎⁎ |
| Asexual | –0.040⁎⁎⁎ | –0.057⁎⁎⁎ | –0.054⁎⁎⁎ |
| Questioning | –0.026* | –0.036⁎⁎ | –0.035⁎⁎ |
| Other | –0.039⁎⁎⁎ | –0.043⁎⁎⁎ | –0.041⁎⁎⁎ |
| BMI | –0.075⁎⁎⁎ | –0.080⁎⁎⁎ | –0.068⁎⁎⁎ |
| Gender identity (Ref.= cis male) | |||
| Cis-female | –0.118⁎⁎⁎ | –0.157⁎⁎⁎ | –0.149⁎⁎⁎ |
| Trans-male | –0.212⁎⁎⁎ | –0.205⁎⁎⁎ | –0.198⁎⁎⁎ |
| Trans-female | –0.046⁎⁎⁎ | –0.050⁎⁎⁎ | –0.044⁎⁎⁎ |
| AMAB/NB | –0.279⁎⁎⁎ | –0.280⁎⁎⁎ | –0.268⁎⁎⁎ |
| AFAB/NB | –0.067⁎⁎⁎ | –0.063⁎⁎⁎ | –0.060⁎⁎⁎ |
| Race/ethnicity | |||
| White | –0.015 | –0.002 | –0.007 |
| African American | 0.016 | 0.010 | 0.013 |
| Native American | –0.029⁎⁎ | –0.020 | –0.023* |
| Asian American | –0.023* | –0.029* | –0.031⁎⁎ |
| Hispanic/Latino | 0.002 | 0.002 | 0.004 |
| Other | –0.011 | –0.002 | –0.007 |
| Age (year) | –0.093⁎⁎⁎ | –0.076⁎⁎⁎ | –0.088⁎⁎⁎ |
| Physical activity | 0.124⁎⁎⁎ | – | –0.171⁎⁎⁎ |
| Ever bullied | –0.161⁎⁎⁎ | 0.214⁎⁎⁎ | |
| Ever bullied × physical activity | –0.099⁎⁎⁎ | ||
| Adjusted R2 | 0.134 | 0.144 | 0.165 |
| Overall model significance | F(21, 8482) = 63.57⁎⁎⁎ | F(21, 8520) = 68.44⁎⁎⁎ | F(23, 8480) = 72.88⁎⁎⁎ |
p < 0.05,
p < 0.01,
p < 0.001.
Abbreviations: AFAB = assigned female at birth; AMAB = assigned male at birth; BMI = body mass index; NB = non-binary; Ref. = reference.
Table 4.
Summary of regression analysis (β) for the effects of physical activity, bullying frequency, and their interaction on depression.
| Variable | Model 1 | Model 2 | Model 3 |
|---|---|---|---|
| Sexual orientation (Ref. = Gay/lesbian) | |||
| Bisexual | 0.049⁎⁎⁎ | 0.032* | 0.032* |
| Straight | –0.029⁎⁎ | –0.031⁎⁎ | –0.028* |
| Queer | –0.002 | –0.003 | –0.005 |
| Pansexual | 0.062⁎⁎⁎ | 0.049⁎⁎ | 0.048⁎⁎ |
| Asexual | 0.037⁎⁎ | 0.019 | 0.019 |
| Questioning | 0.014 | 0.006 | 0.007 |
| Other | 0.038⁎⁎⁎ | 0.028* | 0.028* |
| BMI | 0.096⁎⁎⁎ | 0.105⁎⁎⁎ | 0.098⁎⁎⁎ |
| Gender identity (Ref. = cis-male) | |||
| Cis-female | 0.181⁎⁎⁎ | 0.144⁎⁎⁎ | 0.138⁎⁎⁎ |
| Trans-male | 0.223⁎⁎⁎ | 0.214⁎⁎⁎ | 0.210⁎⁎⁎ |
| Trans-female | 0.047⁎⁎⁎ | 0.040⁎⁎ | 0.039⁎⁎ |
| AMAB/NB | 0.288⁎⁎⁎ | 0.286⁎⁎⁎ | 0.278⁎⁎⁎ |
| AFAB/NB | 0.061⁎⁎⁎ | 0.067⁎⁎⁎ | 0.064⁎⁎⁎ |
| Race/ethnicity | |||
| White | –0.031* | –0.022 | –0.017 |
| African American | 0.013 | 0.009 | 0.009 |
| Native American | 0.035⁎⁎ | 0.037⁎⁎ | 0.040⁎⁎ |
| Asian American | 0.019 | 0.016 | 0.017 |
| Hispanic/Latino | 0.029* | 0.031* | 0.032* |
| Other | 0.027⁎⁎ | 0.028* | 0.030* |
| Age (year) | 0.043⁎⁎⁎ | 0.012 | 0.016 |
| Physical activity | –0.043⁎⁎⁎ | – | –0.069⁎⁎⁎ |
| Bullying frequency | 0.239⁎⁎⁎ | 0.241⁎⁎⁎ | |
| Bullying frequency × physical activity | 0.054⁎⁎⁎ | ||
| Adjusted R2 | 0.122 | 0.176 | 0.180 |
| Overall model significance | F(21, 8426) = 56.68⁎⁎⁎ | F(21, 5711) = 58.06⁎⁎⁎ | F(23, 5530) = 53.86⁎⁎⁎ |
p < 0.05,
p < 0.01,
p < 0.001.
Abbreviations: AMAB = assigned male at birth; AFAB = assigned female at birth; BMI = body mass index; NB = non-binary; Ref. = reference.
Table 5.
Summary of regression analysis (β) for the effects of physical activity, bullying frequency, and their interaction on self-esteem
| Variable | Model 1 | Model 2 | Model 3 |
|---|---|---|---|
| Sexual orientation (Ref. = Gay/lesbian) | |||
| Bisexual | –0.044⁎⁎⁎ | –0.047⁎⁎ | –0.046⁎⁎ |
| Straight | 0.043⁎⁎⁎ | 0.045⁎⁎ | 0.038⁎⁎ |
| Queer | –0.002 | –0.006 | –0.003 |
| Pansexual | –0.068⁎⁎⁎ | –0.068⁎⁎⁎ | –0.066⁎⁎⁎ |
| Asexual | –0.040⁎⁎⁎ | –0.043⁎⁎ | –0.041⁎⁎ |
| Questioning | –0.026* | –0.030* | –0.029* |
| Other | –0.039⁎⁎⁎ | –0.036⁎⁎ | –0.035⁎⁎ |
| BMI | –0.075⁎⁎⁎ | –0.086⁎⁎⁎ | –0.073⁎⁎⁎ |
| Gender identity (Ref. = cis-male) | |||
| Cis-female | –0.118⁎⁎⁎ | –0.129⁎⁎⁎ | –0.118⁎⁎⁎ |
| Trans-male | –0.212⁎⁎⁎ | –0.201⁎⁎⁎ | –0.193⁎⁎⁎ |
| Trans-female | –0.046⁎⁎⁎ | –0.045⁎⁎⁎ | –0.041⁎⁎ |
| AMAB/NB | –0.279⁎⁎⁎ | –0.280⁎⁎⁎ | –0.266⁎⁎⁎ |
| AFAB/NB | –0.067⁎⁎⁎ | –0.068⁎⁎⁎ | –0.064⁎⁎⁎ |
| Race/ethnicity | |||
| White | –0.015 | –0.005 | –0.015 |
| African American | 0.016 | 0.013 | 0.015 |
| Native American | –0.029⁎⁎ | –0.022 | –0.027* |
| Asian American | –0.023* | –0.026 | –0.028* |
| Hispanic/Latino | .002 | 0.001 | .001 |
| Other | –0.011 | 0.003 | .008 |
| Age (year) | –0.093⁎⁎⁎ | –0.057⁎⁎⁎ | –0.065⁎⁎⁎ |
| Physical activity | 0.124⁎⁎⁎ | – | 0.143⁎⁎ |
| Bullying frequency | –0.156⁎⁎⁎ | –0.165⁎⁎⁎ | |
| Bullying frequency × physical activity | –0.058⁎⁎⁎ | ||
| Adjusted R2 | 0.134 | 0.141 | 0.163 |
| Overall model significance | F(21, 8482) = 63.57⁎⁎⁎ | F(21, 5766) = 46.22⁎⁎⁎ | F(23, 5512) = 47.74⁎⁎⁎ |
p < 0.05,
p < 0.01,
p < 0.001.
Abbreviations: AFAB = assigned female at birth; AMAB = assigned male at birth; BMI = body mass index; NB = non-binary; Ref. = reference.
3.1. PA and mental health
The model examining the effect of PA on depression was significant (F(21, 8426) = 56.68, p < 0.001) (Model 1 in Table 2). The variable of PA was significantly related to depression (t = –4.176, p < 0.001; sr2 = 0.002; 95% confidence interval (95%CI): –0.04 to 0.01); as PA increased, depression decreased. PA level was also positively related to self-esteem; the full model was significant F(21, 8482) = 63.57, p < 0.001, as was as the PA variable (t = 12.11, p < 0.001; sr2 = 0.02, 95%CI: 0.08‒0.11) (Model 1 in Table 3).
3.2. Bullying and mental health
Overall, the model examining the effect of ever being bullied on depression was statistically significant (F(21, 8426) = 77.80, p < 0.001) (Model 2 in Table 2). Ever being bullied was significantly related to depression (t = 20.17, p < 0.001; sr2 = 0.05, 95%CI: 3.05–3.71) such that those who were ever bullied had higher levels of depression. For the regression examining the impact of frequency of bullying (Model 2 in Table 4), the overall model was also significant (F(21, 5711) = 58.06, p < 0.001). Frequency of bullying in the past year was positively related to depression (Table 4), t = 19.35, p < 0.001; sr2 = 0.05; 95%CI: 1.47‒1.81) such that more frequent bullying led to higher depression levels.
In examining self-esteem, the model with the independent variable of ever being bullied based on being LGBTQ was significant (F(21, 8520) = 68.44, p < 0.001) (Model 2 in Table 3). Ever being bullied was significantly related to self-esteem (t = –15.23, p < 0.001; sr2 = 0.02; 95%CI: –3.87 to –2.99) such that individuals who reported being bullied had lower self-esteem. For the regression examining the impact of frequency of bullying, the overall model was also significant (F(21, 5766) = 46.22, p < 0.001) (Model 2 in Table 5). Frequency of bullying in the past year was negatively related to self-esteem (t = –12.46, p < 0.001; sr2 = 0.02; 95%CI: –1.66 to –1.21) (Table 4) such that individuals who were bullied more frequently had lower self-esteem.
3.3. The interaction between PA and bullying as a predictor of mental health
There were significant interaction effects between PA and bullying on depression and self-esteem, but not in the expected direction. For the variable of ever being bullied, the overall model for depression was significant (F(23, 8424) = 73.47, p < 0.001) (Model 3 in Table 2), as was the model for self-esteem (F(23, 8480) = 72.88, p < 0.001) (Model 3 in Table 3). The independent variables of PA (t = –6.56, p < 0.001; sr2 = 0.004; 95%CI: –0.08 to –0.04), bullying (t = 20.65, p < 0.001; sr2 = 0.04; 95%CI: 3.13 – 3.79), and the interaction term (t = 4.09, p < 0.001; sr2 = 0.002; 95%CI: 0.03‒0.07) were all significantly related to depression. Similarly, the independent variables of PA (t = 12.54, p < 0.001; sr2 = 0.02; 95%CI: 0.14‒0.19), bullying (t = –16.35, p < 0.001; sr2 = 0.03; 95%CI: –4.09 to –3.21), and the interaction term (t = –5.82, p < 0.001; sr2 = 0.003; 95%CI: –0.13 to –0.06) were significant predictors of self-esteem.
Simple slopes analyses were conducted to probe the significant interactions. Results indicated that the relationships between bullying and depression and bullying and self-esteem were stronger with increased levels of PA (Table 6). However, a visual examination of the data (Supplementary Fig. 1) indicated that while increased PA was associated with lower depression and higher self-esteem among individuals who reported not experiencing bullying, the positive effects of PA were less pronounced among those who reported experiencing bullying. To further probe this finding, regression analyses were re-run while limiting the sample to only those who had not experienced bullying and then comparing the regression coefficients and effect sizes. Among individuals who had never experienced bullying, PA was a significant predictor of depression (t = –6.65, p < 0.001; β = –0.119; sr2 = 0.013; 95%CI: –0.08 to –0.05) and self-esteem (t = 11.71, p < 0.001; β = 0.204; sr2 = 0.04; 95%CI: 0.13‒0.18). Among those who had experienced bullying, PA was also a significant predictor of depression (t = –1.97, p < 0.05; β = –0.025; sr2 = 0.001; 95%CI: –0.03 to 0.00) and self-esteem (t = 7.56, p < 0.001; β = 0.096; sr2 = 0.009; 95%CI: 0.05‒0.09), but it had a much weaker effect. Thus, while the relationship between bullying and mental health is stronger as individuals have higher levels of PA, this result appears to be due to the fact that PA has a strong impact among individuals who had not been bullied but almost no effect among individuals who had experienced bullying.
Table 6.
Summary of unstandardized simple slopes for moderating effects of physical activity.
| Simple slopes of bullying variables at 3 points of physical activity score |
||||||
|---|---|---|---|---|---|---|
| Depression |
Self-esteem |
|||||
| Predictor | 1SD below | Mean | 1SD above | 1SD below | Mean | 1SD above |
| Ever bullied | 1.45⁎⁎⁎ | 1.86⁎⁎⁎ | 2.27⁎⁎⁎ | −1.33⁎⁎⁎ | −2.02⁎⁎⁎ | −2.72⁎⁎⁎ |
| Frequency of bullying | 1.50⁎⁎⁎ | 1.88⁎⁎⁎ | 2.27⁎⁎⁎ | −1.35⁎⁎⁎ | −1.85⁎⁎⁎ | −2.35⁎⁎⁎ |
p < 0.001.
For the analysis containing the variable examining frequency of bullying, the overall model was significant for depression (F(23, 5530) = 53.86, p < 0.001) and self-esteem (F(23, 5512) = 47.74, p < 0.001) (Model 3 in Table 4). For depression, the variables of bullying frequency (t = 19.18, p < 0.001; sr2 = 0.06; 95%CI: 1.49‒1.83), PA (t = –5.57, p < 0.001; sr2 = 0.005; 95%CI: –0.05 to –0.03), and their interaction (t = 4.45, p < 0.001; sr2 = 0.003; 95%CI: 0.02‒0.04) were all statistically significant predictors. Similarly, the independent variables of bullying frequency (t = –12.97, p < 0.001; sr2 = 0.03; 95%CI: –1.74 to –1.28), PA (t = 11.41, p < 0.001; sr2 = 0.01; 95%CI: 0.09‒0.13), and the interaction term (t = –4.69, p < 0.001; sr2 = 0.003; 95%CI: –0.05 to –0.02) were significant predictors of self-esteem (Model 3 in Table 5).
Simple slopes analysis revealed that, like the previous analysis, the relationships between bullying and depression and bullying and self-esteem were stronger as the level of PA increased (Table 6). However, when conducting a visual inspection of the data (Supplementary Fig. 2), it became apparent that increased PA was indeed associated with decreased depression scores and higher self-esteem scores among those who reported more infrequent bullying. However, as bullying frequency increased, the effects of PA on depression and self-esteem were almost nonexistent. To further probe this finding, the regression analyses were re-run when limiting the data, first to individuals with scores below the mean for frequency of bullying and next to individuals with scores at the mean or higher for frequency of bullying. Among individuals who scored below the mean for bullying, PA was a significant predictor of depression (t = –6.15, p < 0.001; sr2 = 0.016; β = –0.130; 95%CI: –0.10 to –0.05) and self-esteem (t = 9.05, p < 0.001; sr2 = 0.03; β = 0.19; 95%CI: 0.11‒ 0.17). Among individuals who scored at the mean or higher for frequency of bullying, PA had a statistically significant but weaker effect on self-esteem (t = 3.71, p < 0.001; sr2 = 0.003; β = 0.06; 95%CI: 0.02–0.06) and did not have a significant effect on depression.
4. Discussion
Most of our findings were consistent with our hypotheses. Depression levels were positively related to bullying based on being LGBTQ, while self-esteem was negatively related to bullying based on being LGBTQ. A history of being bullied and frequency of bullying were significant predictors of depression and self-esteem. These results are consistent with previous research that found a relationship between being bullied based on LGBTQ identity and increased depression and lower self-esteem.1,2,4,39 Results are also consistent with the minority stress theory, which states that individuals with marginalized identities who experience perceived discrimination are at risk for poor mental health.3
PA levels were negatively related to depression and positively related to self-esteem. The more active youth were, the lower their reported levels of depression were. These findings aligned with previous research, which found that youth who exercise tend to experience less depression than those who do not exercise.14,15 The physiological effects of PA, such as the “endorphin hypothesis”, which states that the release of endorphins may reduce pain and increase feelings of euphoria, could explain decreases in depression symptoms in youth who exercise.40 The link between social connection and better mental health outcomes is well established; therefore, social interactions while exercising might also contribute to reduced depression symptoms in youth who exercise.41,42
Our predictions that PA would moderate the effects of bullying on depression and self-esteem were partially supported. Surprisingly, results indicated that as PA increased, the relationships between bullying and depression and bullying and self-esteem became stronger. Upon further examination, it appeared that bullying may moderate the effect of PA on depression and self-esteem, instead of the predicted relationship, which posited that PA would moderate the effect of bullying on depression/self-esteem. Specifically, whereas increased PA led to lower levels of depression in youth who had not been bullied, it had a very weak or no effect on depression among youth who were bullied. Those who reported being bullied had higher levels of depression, and their depression scores remained high regardless of activity level. Likewise, as PA increased, the relationship between bullying and self-esteem weakened. For non-bullied youth, increased levels of PA were positively related to self-esteem, but for youth who had been bullied, PA had little to no effect on self-esteem.
These findings contradict the existing literature, which found that youth who participate in PA and sports are less likely to report being bullied and feeling depressed, and are more likely to report higher self-esteem than those who are not physically active.21,43, 44, 45 Most of this research, however, has been conducted with heterosexual and cisgender populations, or with populations where sexual and gender identity were not examined. A consistent body of literature has found that the majority of LGBTQ individuals report some sort of homophobic or heterosexist behavior or language, discrimination, and lack of support from teachers in grade school physical education settings.27,46 The unwelcoming environment, rife with opportunities for bullying, could discourage SGM youth from wanting to participate in PA and sports. Unsurprisingly, LGBTQ youth report not wanting to participate in high school athletics due to not feeling safe.47 Even though PA has the ability to reduce depression and increase self-esteem, concerns about bullying, safety, and discrimination likely have a greater influence on SGM youth's desire not to participate in sports and exercise than the potential to reduce depression.
In all models, the control variables of gender identity, age, and BMI were significant predictors of depression. These findings are similar to previous literature in that BMI was related to self-esteem and depressive symptoms in adolescents, though the direction of this relationship remains unclear.48 Students who identify as a gender minority tend to experience more depressive symptoms and suicidality than their cisgender peers.49, 50, 51 Non-binary individuals in particular report lower levels of self-esteem.52 Identifying as Native American or Hispanic/Latino were significant predictors of depression in all models. Regarding race/ethnicity, our results are consistent with previous research, which found that Hispanic/Latino and Native American/Pacific Islander youth are at an increased risk for depression and suicidality.53 Identifying as bisexual, heterosexual, pansexual, or asexual was a significant predictor of depression in all models. Previous research has found that individuals with emerging sexual identities experience higher rates of anxiety and depression than their heterosexual, gay, and lesbian counterparts.51 While our results were congruent with the literature, further research on demographic control variables is needed to determine the unique interaction among each variable and bullying, PA, and mental health.
Future research should examine the interaction between overall school environment on bullying, self-esteem, and depression symptoms in SGM youth. Previous research has found that being bullied at school can lead to youth skipping school, which is associated with lower levels of PA.54 If SGM students are bullied in school, they likely will not seek out activities, such as team sports, that might encourage bullying. Since our study did not examine school-based sport participation in particular, future research should examine differences in school-based and non-school-based athletic participation among SGM youth in order to explore students’ experiences of bullying in different sport settings. Future research should also examine what sports or exercise might be more accepting for SGM youth.
Recruitment occurred online, which limited reach to youth with Internet access, potentially excluding low-income youth, homeless youth, or youth without social media profiles. Recruitment occurred through “mainstream” SGM organizations and social media influencers, who tend to have predominantly cisgender and White followers. Thus, given that the majority of the sample identified as White, recruitment efforts may have missed youth of color and youth who do not follow SGM accounts, limiting the generalizability of the sample. The survey recruited SGM youth and might have missed youth who do not identify as SGM. The survey design was cross-sectional; therefore, causality could not be determined. Our analysis combined bullying based on both known and perceived SGM identity and, as a result, we were unable to describe differences between the two perceived causes of bullying. Future research should employ a longitudinal design to determine if one factor (bullying, PA, or depression) precedes another. All survey items were self-report and, thus, participant recall might have been inaccurate. Future research could use wearable technology to measure PA, ask further questions about perceived causes of bullying, and use diagnostic interviews with self-report measures to assess for depression.
5. Conclusion
Youth who are bullied and youth who exercise less report higher levels of depression and lower self-esteem than youth who exercise more and youth who are not bullied. In addition to the need for increased PA in youth, these results highlight the need for continued anti-bullying and anti-discrimination initiatives in schools. For participants who have never been bullied, results of this study align with previous research in that exercise appears to decrease levels of depression while increasing self-esteem, but for SGM youth who have been bullied, exercise has less of an effect on depression or self-esteem levels. While exercise can still have many positive effects on both physical and mental health, our results reveal the importance of taking into account SGM youths’ history of bullying before initiating an exercise intervention if the primary goal is improving mental health. Alternatively, in order to improve both mental and physical health for this vulnerable population, it may be beneficial to integrate mental health support with an exercise intervention in order to better address history of SGM identity-based bullying.
Acknowledgments
This research uses data from the LGBTQ National Teen Study, designed by Ryan J. Watson and Rebecca M. Puhl in collaboration with the Human Rights Campaign, and supported by the Office for Vice President of Research at the University of Connecticut. The authors acknowledge the important contributions of Ellen Kahn, Gabe Murchison, and Liam Miranda in their support, conceptualization, and management related to the LGBTQ National Teen Study. This work was supported through funding by the National Institute on Drug Abuse (Grant No. K01DA047918) awarded to Ryan J. Watson.
Authors’ contributions
SJK created the tables and wrote the introduction, methods, and discussion sections; CL ran the analyses, wrote the results section, created the tables, and provided edits; RJW collected the data and reviewed the manuscript. All authors have read and approved the final version of the manuscript, and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Peer review under responsibility of Shanghai University of Sport.
Supplementary materials associated with this article can be found in the online version at doi:10.1016/j.jshs.2020.11.013.
Supplementary materials
References
- 1.Hall WJ. Psychosocial risk and protective factors for depression among lesbian, gay, bisexual, and queer youth: A systematic review. J Homosex. 2018;65:263–316. doi: 10.1080/00918369.2017.1317467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kosciw JG, Greytak EA, Giga NM, Villenas C, Danischewski DJ. GLSEN; New York, NY: 2016. The 2015 national school climate survey: The experiences of lesbian, gay, bisexual, transgender, and queer youth in our nation's schools. [Google Scholar]
- 3.Meyer IH. In: The health of sexual minorities: Public health perspectives on lesbian, gay, bisexual and transgender populations. Meyer IH, Northridge ME, editors. Springer; Boston, MA: 2007. Prejudice and discrimination as social stressors; pp. 242–267. [Google Scholar]
- 4.Almeida J, Johnson RM, Corliss HL, Molnar BE, Azrael D. Emotional distress among LGBT youth: The influence of perceived discrimination based on sexual orientation. J Youth Adolesc. 2009;38:1001–1014. doi: 10.1007/s10964-009-9397-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.O'Malley Olsen E, Vivolo-Kantor AM, Kann L, Milligan CN. Trends in school-related victimization of lesbian, gay, and bisexual youths—Massachusetts, 1995–2015. Am J Public Health. 2017;107:1116–1118. doi: 10.2105/AJPH.2017.303761. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Meyer IH. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychol Bull. 2003;129:674–697. doi: 10.1037/0033-2909.129.5.674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Peter T, Taylor C. Buried above ground: A university-based study of risk/protective factors for suicidality among sexual minority youth in Canada. J LGBT Youth. 2014;11:125–149. [Google Scholar]
- 8.Burton CM, Marshal MP, Chisolm DJ, Sucato GS, Friedman MS. Sexual minority-related victimization as a mediator of mental health disparities in sexual minority youth: A longitudinal analysis. J Youth Adolesc. 2013;42:394–402. doi: 10.1007/s10964-012-9901-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Poteat VP, Mereish EH, DiGiovanni CD, Koenig BW. The effects of general and homophobic victimization on adolescents' psychosocial and educational concerns: The importance of intersecting identities and parent support. J Couns Psychol. 2011;58:597–609. doi: 10.1037/a0025095. [DOI] [PubMed] [Google Scholar]
- 10.Hatzenbuehler ML. How does sexual minority stigma “get under the skin”? A psychological mediation framework. Psychol Bull. 2009;135:707–730. doi: 10.1037/a0016441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ziyadeh NJ, Prokop LA, Fisher LB, et al. Sexual orientation, gender, and alcohol use in a cohort study of U.S. adolescent girls and boys. Drug Alcohol Depend. 2007;87:119–130. doi: 10.1016/j.drugalcdep.2006.08.004. [DOI] [PubMed] [Google Scholar]
- 12.Plöderl M, Fartacek R. Suicidality and associated risk factors among lesbian, gay, and bisexual compared to heterosexual Austrian adults. Suicide Life Threat Behav. 2005;35:661–670. doi: 10.1521/suli.2005.35.6.661. [DOI] [PubMed] [Google Scholar]
- 13.Kosciw JG, Palmer NA, Kull RM, Greytak EA. The effect of negative school climate on academic outcomes for LGBT youth and the role of in-school supports. J Sch Violence. 2013;12:45–63. [Google Scholar]
- 14.Paluska SA, Schwenk TL. Physical activity and mental health: Current concepts. Sports Med. 2000;29:167–180. doi: 10.2165/00007256-200029030-00003. [DOI] [PubMed] [Google Scholar]
- 15.Brosnahan J, Steffen LM, Lytle L, Patterson J, Boostrom A. The relation between physical activity and mental health among Hispanic and non-Hispanic white adolescents. Arch Pediatr Adolesc Med. 2004;158:818–823. doi: 10.1001/archpedi.158.8.818. [DOI] [PubMed] [Google Scholar]
- 16.Pascoe MC, Parker AG. Physical activity and exercise as a universal depression prevention in young people: A narrative review. Early Interv Psychiatry. 2019;13:733–739. doi: 10.1111/eip.12737. [DOI] [PubMed] [Google Scholar]
- 17.Dale LP, Vanderloo L, Moore S, Faulkner G. Physical activity and depression, anxiety, and self-esteem in children and youth: An umbrella systematic review. Ment Health Phys Act. 2019;16:66–79. [Google Scholar]
- 18.Calfas KJ, Taylor WC. Effects of physical-activity on psychological variables in adolescents. Pediatr Exerc Sci. 1994;6:406–423. [Google Scholar]
- 19.Eime RM, Young JA, Harvey JT, Charity MJ, Payne WR. A systematic review of the psychological and social benefits of participation in sport for children and adolescents: Informing development of a conceptual model of health through sport. Int J Behav Nutr Phys Act. 2013;10:98. doi: 10.1186/1479-5868-10-98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Wegner M, Amatriain-Fernández S, Kaulitzky A, Murillo-Rodriguez E, Machado S, Budde H. Systematic review of meta-analyses: Exercise effects on depression in children and adolescents. Front Psychiatry. 2020;11:81. doi: 10.3389/fpsyt.2020.00081. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Taliaferro LA, Rienzo BA, Miller MD, Pigg Jr RM, Dodd VJ. High school youth and suicide risk: Exploring protection afforded through physical activity and sport participation. J Sch Health. 2008;78:545–553. doi: 10.1111/j.1746-1561.2008.00342.x. [DOI] [PubMed] [Google Scholar]
- 22.Rasmussen M, Laumann K. The academic and psychological benefits of exercise in healthy children and adolescents. EJPE. 2013;28:945–962. [Google Scholar]
- 23.Liu M, Wu L, Ming Q. How does physical activity intervention improve self-esteem and self-concept in children and adolescents? Evidence from a meta-analysis. PLoS One. 2015;10 doi: 10.1371/journal.pone.0134804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Kann L, McManus T, Harris WA, et al. Youth risk behavior surveillance - United States, 2017. MMWR Surveill Summ. 2018;67:1–114. doi: 10.15585/mmwr.ss6708a1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.U.S. Department of Health and Human Services . 2nd ed. U.S. Department of Health and Human Services; Washington, DC: 2018. Physical activity guidelines for Americans. [Google Scholar]
- 26.Calzo JP, Roberts AL, Corliss HL, Blood EA, Kroshus E, Austin SB. Physical activity disparities in heterosexual and sexual minority youth ages 12–22 years old: Roles of childhood gender nonconformity and athletic self-esteem. Ann Behav Med. 2014;47:17–27. doi: 10.1007/s12160-013-9570-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Greenspan SB, Griffith C, Hayes CR, Murtagh EF. LGBTQ + and ally youths’ school athletics perspectives: a mixed-method analysis. J LGBT Youth. 2019;16:403–434. [Google Scholar]
- 28.Watson RJ, Wheldon CW, Puhl RM. Evidence of diverse identities in a large national sample of sexual and gender minority adolescents. J Res Adolesc. 2020;30:431–442. doi: 10.1111/jora.12488. [DOI] [PubMed] [Google Scholar]
- 29.Godin G, Shephard RJ. A simple method to assess exercise behavior in the community. Can J Appl Sport Sci. 1985;10:141–146. [PubMed] [Google Scholar]
- 30.Godin G. The Godin-Shephard leisure time physical activity questionnaire. Health Fit J Can. 2011;4:18–22. [Google Scholar]
- 31.Nelson MC, Neumark-Stzainer D, Hannan PJ, Sirard JR, Story M. Longitudinal and secular trends in physical activity and sedentary behavior during adolescence. Pediatrics. 2006;118:e1627–e1634. doi: 10.1542/peds.2006-0926. [DOI] [PubMed] [Google Scholar]
- 32.Godin G, Jobin J, Bouillon J. Assessment of leisure time exercise behavior by self-report: A concurrent validity study. Can J Public Health. 1986;77:359–362. [PubMed] [Google Scholar]
- 33.Jacobs DR, Jr, Ainsworth BE, Hartman TJ, Leon AS. A simultaneous evaluation of 10 commonly used physical activity questionnaires. Med Sci Sports Exerc. 1993;25:81–91. doi: 10.1249/00005768-199301000-00012. [DOI] [PubMed] [Google Scholar]
- 34.Brooks SJ, Krulewicz SP, Kutcher S. The Kutcher adolescent depression scale: assessment of its evaluative properties over the course of an 8-week pediatric pharmacotherapy trial. J Child Adolesc Psychopharmacol. 2003;13:337–349. doi: 10.1089/104454603322572679. [DOI] [PubMed] [Google Scholar]
- 35.Brooks SJ, Kutcher S. Diagnosis and measurement of adolescent depression: A review of commonly utilized instruments. J Child Adolesc Psychopharmacol. 2001;11:341–376. doi: 10.1089/104454601317261546. [DOI] [PubMed] [Google Scholar]
- 36.Rosenberg M. Wesleyan University Press; Middletown, CT: 1989. Society and the adolescent self-image. Revised edition. [Google Scholar]
- 37.Pearlin LI, Schooler C. The structure of coping. J Health Soc Behav. 1978;19:2–21. [PubMed] [Google Scholar]
- 38.Levenson H. Multidimensional locus of control in psychiatric patients. J Consult Clin Psychol. 1973;41:397–404. doi: 10.1037/h0035357. [DOI] [PubMed] [Google Scholar]
- 39.Roberts AL, Rosario M, Slopen N, Calzo JP, Austin SB. Childhood gender nonconformity, bullying victimization, and depressive symptoms across adolescence and early adulthood: An 11-year longitudinal study. J Am Acad Child Adolesc Psychiatry. 2013;52:143–152. doi: 10.1016/j.jaac.2012.11.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Dishman RK, O'Connor PJ. Lessons in exercise neurobiology: The case of endorphins. Ment Health Phys Act. 2009;2:4–9. [Google Scholar]
- 41.Kawachi I, Berkman LF. Social ties and mental health. J Urban Health. 2001;78:458–467. doi: 10.1093/jurban/78.3.458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Doré I, O'Loughlin JL, Beauchamp G, Martineau M, Fournier L. Volume and social context of physical activity in association with mental health, anxiety and depression among youth. Prev Med. 2016;91:344–350. doi: 10.1016/j.ypmed.2016.09.006. [DOI] [PubMed] [Google Scholar]
- 43.Waasdorp TE, Mehari KR, Milam AJ, Bradshaw CP. Health-related risks for involvement in bullying among middle and high school youth. J Child Fam Stud. 2019;28:2606–2617. [Google Scholar]
- 44.Sibold J, Edwards E, Murray-Close D, Hudziak JJ. Physical activity, sadness, and suicidality in bullied US adolescents. J Am Acad Child Adolesc Psychiatry. 2015;54:808–815. doi: 10.1016/j.jaac.2015.06.019. [DOI] [PubMed] [Google Scholar]
- 45.Dishman RK, Hales DP, Pfeiffer KA, et al. Physical self-concept and self-esteem mediate cross-sectional relations of physical activity and sport participation with depression symptoms among adolescent girls. Health Psychol. 2006;25:396–407. doi: 10.1037/0278-6133.25.3.396. [DOI] [PubMed] [Google Scholar]
- 46.Morrow RG, Gill DL. Perceptions of homophobia and heterosexism in physical education. Res Q Exerc Sport. 2003;74:205–214. doi: 10.1080/02701367.2003.10609082. [DOI] [PubMed] [Google Scholar]
- 47.Kulick A, Wernick LJ, Espinoza MAV, Newman TJ, Dessel AB. Three strikes and you're out: Culture, facilities, and participation among LGBTQ youth in sports. Sport Educ Soc. 2019;24:939–953. [Google Scholar]
- 48.Boutelle KN, Hannan P, Fulkerson JA, Crow SJ, Stice E. Obesity as a prospective predictor of depression in adolescent females. Health Psychol. 2010;29:293–298. doi: 10.1037/a0018645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Gower AL, Rider GN, Coleman E, Brown C, McMorris BJ, Eisenberg ME. Perceived gender presentation among transgender and gender diverse youth: Approaches to analysis and associations with bullying victimization and emotional distress. LGBT Health. 2018;5:312–319. doi: 10.1089/lgbt.2017.0176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Eisenberg ME, Gower AL, McMorris BJ, Rider GN, Shea G, Coleman E. Risk and protective factors in the lives of transgender/gender nonconforming adolescents. J Adolesc Health. 2017;61:521–526. doi: 10.1016/j.jadohealth.2017.04.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Borgogna NC, McDermott RC, Aita SL, Kridel MM. Anxiety and depression across gender and sexual minorities: Implications for transgender, gender nonconforming, pansexual, demisexual, asexual, queer, and questioning individuals. Psychol Sex Orientat Gend Divers. 2019;6:54–63. [Google Scholar]
- 52.Thorne N, Witcomb GL, Nieder T, Nixon E, Yip A, Arcelus J. A comparison of mental health symptomatology and levels of social support in young treatment seeking transgender individuals who identify as binary and non-binary. Int J Transgend. 2018;20:241–250. doi: 10.1080/15532739.2018.1452660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Bostwick WB, Meyer I, Aranda F, et al. Mental health and suicidality among racially/ethnically diverse sexual minority youths. Am J Public Health. 2014;104:1129–1136. doi: 10.2105/AJPH.2013.301749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Demissie Z, Lowry R, Eaton DK, Hertz MF, Lee SM. Associations of school violence with physical activity among U.S. high school students. J Phys Act Health. 2014;11:706–711. doi: 10.1123/jpah.2012-0191. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.