

Abstract
Objective:
Conflict poses multiple relational and health risks. Dyadic stress theories suggest satisfaction and communication alter cardiovascular and autonomic function, key pathways from troubled relationships to poor health. However, “we-talk,” a positive communication pattern, can strengthen relationships and promote health. We examined how each spouse’s satisfaction and we-talk were related to conflict’s physiological, relational, and emotional toll.
Methods:
Married couples (n=107 couples, 214 individuals, ages 40–87), who were mostly white, highly educated, and higher income Americans in different-gender relationships, engaged in 20-minute conflict discussions while wearing monitors to assess heart rate variability (HRV). Spouses rated their closeness immediately after conflict and their conflict rumination 2 hours later. Conflict transcriptions measured we-talk, or the proportion of first-person plural pronouns (we, us, our).
Results:
Satisfied spouses or those in mutually satisfying relationships had higher HRV during conflict (b=0.0001, p=0.049), felt closer immediately after conflict (b=0.07, p<0.001), and ruminated less about the conflict two hours later (b=−0.26, p=0.026). Spouses’ HRV was highest (b=0.0002, p=0.002) and rumination was lowest (b=−0.49, p=0.019) when they or their partners were satisfied and used we-talk more often. Women’s HRV (b=0.0001, p=0.035) and rumination (b=−0.01, p=0.02) benefited when both spouses were satisfied, as did closeness when women were satisfied (b=0.10, p<0.001). Men’s closeness benefited when they (b=0.04, p=0.003) or their wives (b=0.04, p=0.002) were satisfied.
Conclusions:
The combination of mutually satisfying relationships and we-talk was associated with better relational and health outcomes after conflict. These findings are important for middle-aged and older couples whose relationships are central to their health.
Keywords: Marriage, stress, conflict, rumination, health, romantic relationships
Introduction
Happily married spouses have better health than their unhappily married and unmarried peers (1–3). Indeed, married spouses have lower morbidity and mortality than those who are unmarried, and satisfied spouses are three times less likely to develop cardiovascular disease than dissatisfied spouses (4–6). Though a satisfying marriage protects health, a troubled marriage has physiological costs across multiple regulatory systems, notably autonomic and cardiovascular function (2,7). Low heart rate variability (HRV) is associated with multiple cardiovascular risk factors: hypertension, metabolic syndrome, high cholesterol, and atherosclerosis (8–10). While low HRV during rest reflects a lower capacity for cardiac regulation, low HRV during stress reflects poorer flexibility adapting to stressful situations (11). Such stress-related decrements suggest a heighted stress response, wearing on the body and threatening health (12). These health effects intensify as spouses age, with dissatisfied partners reporting higher marital strain and lower HRV concurrently and 10 years later (13,14).
Dyadic stress and coping frameworks, such as the Dyadic Biobehavioral Stress Model (15), Systemic Transactional Model of Dyadic Coping (16,17), and the Communal Coping Model (18), suggest that the way couples manage conflict—a common source of relational stress—influences each partner’s physiological, emotional, and relational health. Given couples’ interdependence, these frameworks discuss how the perceptions and behaviors of one partner can influence the relational and health outcomes of the other partner. This interdependent lens therefore conceptualizes conflict as dyadic, emphasizing each partner’s role—for better or worse—in navigating these difficult conversations. For negative conflict management and communication, studies have shown that relative to less hostile partners, more hostile partners experienced greater heart rate responses to conflict (1,19). In addition, compared to their less negative peers, more negative couples’ HRV dropped during conflict (7). In terms of the emotional and relational aftermath, partners felt less close and experienced greater negative emotional reactivity when they were more negative and less positive during conflict (7). Partners’ post-conflict rumination, a particularly maladaptive emotion regulation strategy, was higher when they expressed more negative emotions during conflict (20).
In contrast, couples’ satisfying relationships and positive communication strategies are protective during conflict. Individuals’ HRV was higher when their partners were more satisfied or used positive communication strategies during conflict (21,22). For instance, spouses resolve conflict more effectively and experience fewer relational and health consequences when they think and talk in relational terms (23,24). This communication pattern, termed we-talk, is shown when spouses use words like “we” rather than “you” or “me,” reflecting the fact that they are thinking about resolving conflict as a couple rather than as two separate individuals (25). Using first-person plural pronouns (we), rather than singular pronouns (I, you, or me), signals that partners see the problem as shared and want to address it together.
A meta-analysis showed partners who use more we-talk have better relationship functioning and health relative to those using we talk less often (25). Partners also felt more comfortable talking about a sensitive topic when they each thought in relational terms and saw problems as shared, correlating with better relationship and health perceptions in each partner (26,27). Using an index of autonomic and somatic measures, spouses’ physiological reactivity to conflict was lower when individuals and their partners used we-talk more often relative to less often (24). Interestingly, a partner’s we-talk was more strongly associated with physiological reactivity compared to a person’s own we-talk; this finding illustrates the health benefits of a partner thinking and talking in relational terms.
In addition, women experience greater physiological and emotional reactivity to relational stress and conflict than men (28,29). The interpersonal orientation hypothesis suggests women not only monitor their relationships more often than men, but they also include their relationships in their self-perceptions and identities, often due to gendered socialization in American culture (30,31). In contrast, men’s sense of self is more independent and less relationship focused. Relationship conflict may signal to women that their relationships are in peril, resulting in greater physiological, relational, and emotional distress (32). However, a partner’s we-talk may relate to lower conflict responses in women because we-talk represents a strong couple identity and interdependent relationship (24).
As couples’ relationships become even more important for their health with age, it is important to understand how each partner can help reduce conflict’s relational and health impact in adulthood. Studies addressing the effects of each partner’s satisfaction and we-talk—a global protective mechanism combined with a context-specific protective mechanism—would help illustrate how partners help increase or decrease each other’s conflict-related risks. Although couples’ satisfying relationships and we-talk have each been related to more positive conflict responses (21–23), their joint and synergistic effects have not been examined. It is worthwhile to understand how they combine to exacerbate or reduce conflict’s negative relational and health effects. For instance, partners may benefit most if they are satisfied and use we-talk during conflict, or they might be worse off if they are less satisfied and use we-talk less often; alternatively, their greater satisfaction or we-talk might help compensate if the other is lacking. Addressing how both global and context-specific protective mechanisms relate to conflict responses might help explain why conflict poses heightened relationship and health risks for some partners, but not for others, offering new insights into marriage’s health impact.
The present study examined how each partner’s satisfaction and we-talk related to conflict’s physiological, relational, and emotional toll in middle-aged and older couples. We assessed couples’ HRV during conflict, momentary closeness immediately after conflict, and conflict rumination 2 hours later. We hypothesized that each partner’s satisfaction would be associated with higher HRV and closeness and lower rumination, and that these effects would be strongest when both spouses were more satisfied. Likewise, we hypothesized that each partner’s we-talk during conflict would be associated with higher HRV and closeness, and lower rumination, and that the effects would be strongest when both spouses used we-talk more often during the conflict. Additionally, we expected that the interaction of partners’ higher satisfaction and we-talk would correspond to higher HRV, greater closeness, and lower rumination. Lastly, we hypothesized that these effects would be stronger for women relative to men, given conflict’s stronger impact on women (28,33).
Method
Participants
Middle-aged and older heterosexual couples (n=107 couples, 214 participants) were recruited for a parent study on molecular aging. Interested couples completed online and in-person screens to determine eligibility. The parent study’s sample size was planned based on the expected power for hypothesized three-way interactions, with exploratory hypotheses examining actor-partner effects and interactions by gender. Given the parent study’s adequate power for similarly sized effects for the current study, it was concluded that the primary hypotheses for the present study were powered. Couples were excluded if they were together fewer than three years, not living together, younger than 40 years old, and had sensory impairments that would interfere with study completion. The parent study also focused on different-gender couples because of statistical power related to gender and actor-partner effects. To reduce bias in HRV data, couples were also excluded if either partner smoked, abused substances, had chronic health problems with lingering symptoms, or used prescription medications other than statins (n=30) and antidepressants (n=49), given their widespread use. Nine participants used beta-blockers, which served as a covariate in the analyses. A total of 576 interested individuals were excluded or did not participate because they or their partner did not meet the stringent health criteria (n=412), their partner was not interested (n=48), they canceled their visit (n=22), or they never enrolled (n=94). All couples were heterosexual, married, and cohabiting with an average relationship duration of 28.62 years (SD=14.06, range=3–63). Participants’ average age was 56.52 years (SD=11.22, range=40–86), and most were white (92.5%), had graduate or professional training (49.1%), worked full time (57%), and had household incomes over $100,000 (57.5%). Table 1 provides additional sociodemographic characteristics. Data were collected between December 2017 and March 2020 (before the COVID-19 shutdown).
Table 1.
Sociodemographic Characteristics of Participants (n=107 couples, 214 participants)
| Mean ± SD (range) or N (%) | |
|---|---|
| Age | 56.52 ± 11.22 (40–86) |
| Relationship length | 28.62 ± 14.06 (3–63) |
| Race | |
| Asian | 6 (2.8%) |
| Black | 8 (3.7%) |
| Native American or Alaskan Native | 1 (0.5%) |
| White | 198 (92.5%) |
| Multiracial | 1 (0.5%) |
| Education | |
| High school | 3 (1.4%) |
| Some college | 24 (11.2%) |
| College graduate | 81 (37.9.0%) |
| Graduate or professional training | 105 (49.1%) |
| Prefer not to answer | 1 (0.05%) |
| Employment status | |
| Full time | 122 (57.0%) |
| Part time | 26 (12.1%) |
| Retired | 57 (26.6%) |
| Disabled | 3 (1.4%) |
| Unemployed | 6 (2.8%) |
| Income | |
| $25,000-$49,999 | 16 (7.5%) |
| $50,000-$74,999 | 35 (16.4%) |
| $75,000-$99,999 | 24 (11.2%) |
| >$100,000 | 123 (57.5%) |
| Prefer not to answer | 16 (7.5%) |
Note. All couples were married, cohabiting, and in different-gender relationships.
Procedure
Participants completed a full-day visit at the Clinical Research Center (CRC), a hospital research unit at the Ohio State University. Couples were told to avoid alcohol and strenuous physical activity two days before the study visit. They began a 12-hour fast at 7:30 p.m. the evening before the visit and then couples arrived at 7:30 a.m. Each person was fitted with a heart rate monitor to obtain HRV data throughout the visit. Following a brief 5-minute resting period, spouses ate a standardized breakfast and completed several self-report questionnaires, including a relationship satisfaction measure, and engaged in a conflict discussion later that morning. After the conflict, spouses completed several cognitive and psychological assessments separately; these were unrelated to the present analyses. At the end of the visit, about 2 hours after the conflict, spouses completed a conflict rumination measure. Study procedures were approved by the Ohio State University Institutional Review Board; participants provided written informed consent before participating.
Conflict Discussion
Couples engaged in a 20-minute marital problem discussion to resolve one or more of their marital issues. To initiate the discussions, an experimenter first conducted a 10- to 20-minute interview to identify the most contentious topics within the marriage for both spouses (28,34). These topics were selected from an inventory each spouse completed about their relationship problems. Couples were then asked to discuss and try to resolve one or more marital issues that the experimenter judged to be the most conflict-producing (e.g., money, communication, or in-laws). The research team remained out of sight during the discussion.
As a manipulation test to assess the conflict’s emotional intensity and severity, participants rated several negative emotions (0=not at all, 100=extremely) before and after the conflict. After the conflict, compared to before the conflict, participants felt more gloomy (mean difference=3.05, SD=17.63, t(212)=2.53, p=0.01)), angry and irritated (mean difference=8.78, SD=21.02, t(212)=6.10, p<0.001)), upset (mean difference=37.23, SD=21.13, t(212)=4.99, p<0.001)), and marginally more sad or blue (mean difference=2.39, SD=20.86, t(212)=1.68, p=0.095)). In addition, participants rated the importance of the conflict topic using a 7-point scale (1=Not very important, 7=Extremely important), which showed 46.7% of participants rated the topic as extremely important (mode=7, M=6.09, SD = 1.05).
Relationship Satisfaction
The 32-item Couples Satisfaction Index (CSI-32) assessed relationship satisfaction (35). Developed using item response theory, the CSI distinguishes between satisfied and dissatisfied partners with greater precision than most commonly used relationship satisfaction scales (35). Cronbach’s α for the CSI-32 was 0.98.
We-Talk
Transcribed conflict discussions were analyzed with the widely used computerized text analysis program Linguistic Inquiry and Word Count-2015 (LIWC2015;(36). LIWC calculates percentages of words, adjusted for total word count, in psychologically relevant categories based on a standardized dictionary. We-talk was calculated as the proportion of first-person plural pronouns (e.g., we, us, our, ourselves) from the total amount of words in the transcript, and indexed as a percentage to easily compare between individuals (37). Higher we-talk scores indicated that spouses used more first-plural pronouns during their conflict discussions.
Momentary Closeness
Immediately after the conflict discussion, participants rated their momentary interpersonal closeness (38). Using a scale from 0 (strongly disagree) to 6 (strongly agree), participants rated two items: “Right now, I feel emotionally distant from my partner” and “Right now, I feel close to my partner.” The first item was reverse-scored, and then the two items were summed to reflect momentary closeness (α=0.91).
Conflict Rumination
Approximately 2 hours after the conflict, participants rated how much they were thinking about the conflict (“Since my partner and I discussed our disagreement a little bit ago, I have been thinking back about the conversation”) using a scale ranging from 0 (not at all) to 100 (very much so).
HRV
HRV was obtained with the Firstbeat Bodyguard 2, a lightweight heart monitor with electrodes placed under the right clavicle and on the left side of the ribcage below the heart (39). The device produces reliable and easily extractable HR and HRV data (39,40). Visual artifact correction was performed on the raw interbeat interval (IBI) data using Kubios HRV software (41). To capture HRV levels during the 5-minute rest period and conflict, we extracted the corresponding IBI series for those windows and calculated a standard time-domain measure of HRV, the root mean square of successive differences (RMSSD) using Kubios software (11). We used 5-minute segments of the conflict discussion to match the 5-minute window of the rest period (Laborde et al., 2017). HRV measurements were natural log-transformed to better approximate the normality of residuals. HRV data shown in the tables and figures represent back-transformed geometric numbers to enhance interpretability.
Covariates
Primary analyses predicting HRV controlled for resting baseline HRV, age, sagittal abdominal diameter, daily physical activity, and beta-blocker use (n=9) given their associations in previous research (7,42). Primary analyses predicting closeness and rumination controlled for age, given documented associations (2,43).
Analytical Plan
Preliminary analyses examined means, standard deviations, correlations, and gender differences in study variables (see Table 2); we also assessed HRV trajectories across baseline and the 20-minute conflict discussions using dyadic multilevel models; time was treated as a categorical variable due to the varying nonlinear trajectories. Gender differences in trajectories were tested using two-way interactions between gender and time.
Table 2.
Correlations among Study Variables
| CSI-32 | Conflict we-talk | Conflict HRV | Closeness | Rumination | Baseline HRV | Age | SAD | Physical activity | Beta-blocker | |
|---|---|---|---|---|---|---|---|---|---|---|
| CSI-32 | 0.62 *** | 0.32*** | 0.13 | 0.73*** | −0.27* | −0.01 | −0.08 | 0.04 | 0.06 | −0.17 |
| Conflict we-talk | 0.14 | 0.44 *** | −0.03 | 0.23* | −0.10 | −0.10 | 0.17 | 0.01 | −0.01 | −0.22* |
| Conflict HRV | −0.11 | 0.28** | 0.19 ** | 0.02 | 0.21 | 0.80*** | −0.17 | −0.15 | 0.26* | 0.09 |
| Closeness (post-conflict) | 0.51*** | 0.19 | −0.18 | 0.48 *** | −0.41*** | −0.15 | −0.02 | 0.04 | 0.06 | −0.11 |
| Rumination (2 hr post-conflict) | −0.13 | −0.30** | −0.03 | −0.14 | 0.07 | 0.18 | 0.06 | −0.02 | −0.01 | −0.05 |
| Baseline HRV | −0.17 | 0.14 | 0.82*** | −0.14 | 0.07 | 0.26 *** | −0.26** | −.026** | 0.26* | 0.09 |
| Age | 0.11 | −0.08 | −0.27** | 0.00 | 0.30** | −0.26* | 0.94 *** | −0.03 | 0.24* | 0.13 |
| SAD | −0.14 | −0.03 | −0.21* | −0.06 | 0.002 | −0.25* | 0.04 | 0.05 | −0.24* | 0.06 |
| Physical activity | −0.17 | −0.11 | −0.01 | −0.20 | 0.16 | 0.02 | 0.40*** | −0.18 | 0.27 *** | 0.04 |
| Beta-blocker | 0.18 | −0.09 | 0.05 | −0.01 | 0.09 | 0.01 | 0.17 | −0.03 | −0.01 | −0.03 |
| Mean ± SD or N (women) | 125.65 ±29.15 | 2.06 ±0.88 | 24.99 ±1.86 | 9.51 ± .33 | 31.92 ±31.54 | 26.48 ±1.82 | 55.68 ±10.76 | 20.73 ±3.17 | 3.35 ± 1.51 | 3 |
| Range or % (women) | 36–158 | 0.17–4.14 | 6.90–117.29 | 0–12 | 0–100 | 6.92–97.98 | 40–86 | 13.92–8.50 | 1–7 | 2% |
| Mean ± SD or N (men) | 131.04±23.39 | 1.88 ±0.94 | 23.17 ±1.79 | 9.79 ±3.17 | 37.14 ±30.90 | 25.10 ±1.88 | 56.92 ±10.90 | 23.34 ±3.15 | 3.46 ±1.81 | 6 |
| Range or % (men) | 43–160 | 0.14–4.35 | 7.06–90.71 | 0–12 | 0–100 | 5.26–158.11 | 40–86 | 17.80–35.00 | 1–7 | 4% |
Note. CSI=couples satisfaction inventory. SAD=sagittal abdominal diameter. Gender coded −1=men, 1=women. Beta-blocker use coded −1=no, 1=yes. Correlations for women are above the diagonal, correlations for men are below the diagonal, and correlations between partners are bolded along the diagonal. HRV data are back-transformed.
p<0.05
p<0.01
p<0.001.
Multilevel modeling (MLM) was used to conduct Actor-Partner Interdependence Models testing the study hypotheses (44). This analytical approach allowed for explicit modeling of the non-independence in married couples’ data. Couples were treated as distinguishable with gender as the distinguishing variable. For models predicting HRV during conflict, we specified that the four HRV measurement samples within the 20-minute period were nested within individuals and couples, and that time was a repeated factor across individuals and couples (i.e., that we had observations for both partners on each sample time; Kenny et al., 2006). As with the preliminary analyses, time was treated as a categorical variable due to the varying nonlinear trajectories. We accounted for the similarity in the spouses’ average HRV by including a random couple-level intercept. We also accounted for the similarity in the residuals of the individuals’ HRV across the specific time points and gender-specific intercepts at the couple level and an unstructured covariance matrix. For models predicting post-conflict closeness and rumination, we accounted for the similarity in the spouses’ outcomes by including a random intercept using a variance components covariance structure; these outcomes had only one observation per person. Below are example equations predicting (1) HRV during conflict with actor and partner satisfaction and we-talk, and (2) Momentary closeness after conflict with actor and partner satisfaction and we-talk.
An additional strength of using MLM is that it accounts for missing data by maximizing the use of existing data. MLM analyses were performed using the MIXED MODELS procedure with restricted maximum likelihood estimation in SPSS version 26. Before the primary analyses, the independent variables (own satisfaction, partner satisfaction, own we-talk, and partner we-talk) and continuous covariates (baseline HRV, age, sagittal abdominal diameter (SAD), and daily physical activity) were grand mean-centered to improve the interpretability of the intercepts; each of these variables was assessed once per person. Dichotomous independent variables and covariates were effects coded (gender: men=−1, women=1; beta-blocker use: no=−1, yes=1); these variables were also assessed one time.
To examine hypotheses that own and partner satisfaction would predict HRV, closeness, and rumination, we first specified models with the main effects of own satisfaction and partner satisfaction and their two-way interaction. Then we included two- and three-way interactions with gender to examine gender differences in how own and partner satisfaction predicted spouses’ outcomes. The same process was used for own and partner we-talk (i.e., initial model with own we-talk, partner we-talk, and their interaction; second model with gender interactions). Next, we added actor and partner effects for both satisfaction and we-talk to test how they each predicted HRV, closeness, and rumination in the same model. Last, we added two- and three-way interactions between own satisfaction, partner satisfaction, own we-talk, and partner we-talk to the models to address their synergistic relationships with the three outcomes; we initially tested their four-way interaction, but it did not predict the outcomes and was thus removed in constructing the final models (ps>0.66); the lower order interactions remained in the models and are presented in text below. We also explored interactions with time for the HRV models, but they did not predict spouses’ HRV (ps>0.23) and were thus removed from the final models. We used the Benjamini–Hochberg false discovery rate method to account for multiple comparisons (45); this method controls the error rate of false positives by considering the number of significant results in a family of tests. As discussed by McDonald (46), a false discovery rate of 0.05 is likely too low for the Benjamini–Hochberg correction, and a rate of 0.10–0.20 is suggested. All associations reported below held after FDR adjustments and fell below an FDR of .15. Tests also held after a more stringent .10 FDR correction, unless otherwise noted. Nonsignificant higher-order interactions were removed when probing lower-order interactions. Continuous interactions were computed as the product of the mean-centered variables (47). Interacting effects were probed at one standard deviation above and below the means for each continuous interacting variable. Analytic code and data are available upon request from the first author.
Results
Preliminary Analyses
Table 2 shows means, standard deviations, and correlations in all study variables for women and men separately, as well as correlations between women and men; only correlations among primary study variables are discussed in text. For women, but not men, greater relationship satisfaction was correlated with more frequent we-talk during conflict (pwomen<0.001; pmen=0.17 ). Women’s and men’s greater relationship satisfaction was correlated with higher post-conflict closeness (ps<0.001); women’s relationship satisfaction also was associated with lower post-conflict rumination (p=0.016). Women’s we-talk during conflict was correlated with higher post-conflict closeness (p=0.020), whereas men’s we-talk was associated with higher conflict HRV (p=0.005) and lower post-conflict rumination (p=0.009). HRV during conflict was not correlated with post-conflict closeness (ps>0.082) or rumination (ps>0.066) for women or men; closeness and rumination were negatively correlated for women (p<0.001), but not men (p=0.24). For correlations between women and men, with the exception of post-conflict rumination (p=0.40), all primary study variables were positively correlated (ps<0.008). There were no gender differences in primary study variables (ps>0.13); for covariates, men had larger sagittal abdominal diameters than women, t(209)=6.00, p<0.001).
Mixed models showed HRV was higher at baseline relative to each conflict timepoint (F(4, 385)=8.27, p<0.001, bs=0.05–0.10, SEs=0.02, ps<0.009, 95% CIs [0.01, 0.13]). During conflict, HRV was higher at 5 minutes compared to 10 minutes (b=0.05, SE=0.02, p=0.003, 95% CI [0.01, 0.08]) and 15 minutes (b=0.04, SE=0.02, p=0.015, 95% CI [0.01, 0.07]); there were no other HRV differences during the conflict (ps>.053). There were no initial gender differences in average HRV (p=0.12) or how HRV changed across the day (p=0.96).
HRV During Conflict
Own and Partner Satisfaction
Own and partner satisfaction’s main effects did not predict HRV during conflict (ps>0.097), but their two-way interaction predicted HRV (b=0.0001, SE=0.00004, p=0.049, 95% CI [0.00003, 0.0001]); this effect survived an FDR of .15 but not .10, though it was qualified by a 3-way interaction below. As shown in Figure 1A, satisfied spouses had higher HRV throughout the conflict than less satisfied spouses if their partner was also satisfied (b=0.005, SE=0.002, p=0.030, 95% CI [0.0001, 0.009]). If a partner was less satisfied, HRV was similar regardless of spouses’ own satisfaction even if they were satisfied themselves (b=0.001, SE=0.002, p=0.69, 95% CI [−0.003, 0.004]). Thus, HRV during conflict was higher if both spouses were satisfied.
Figure 1.
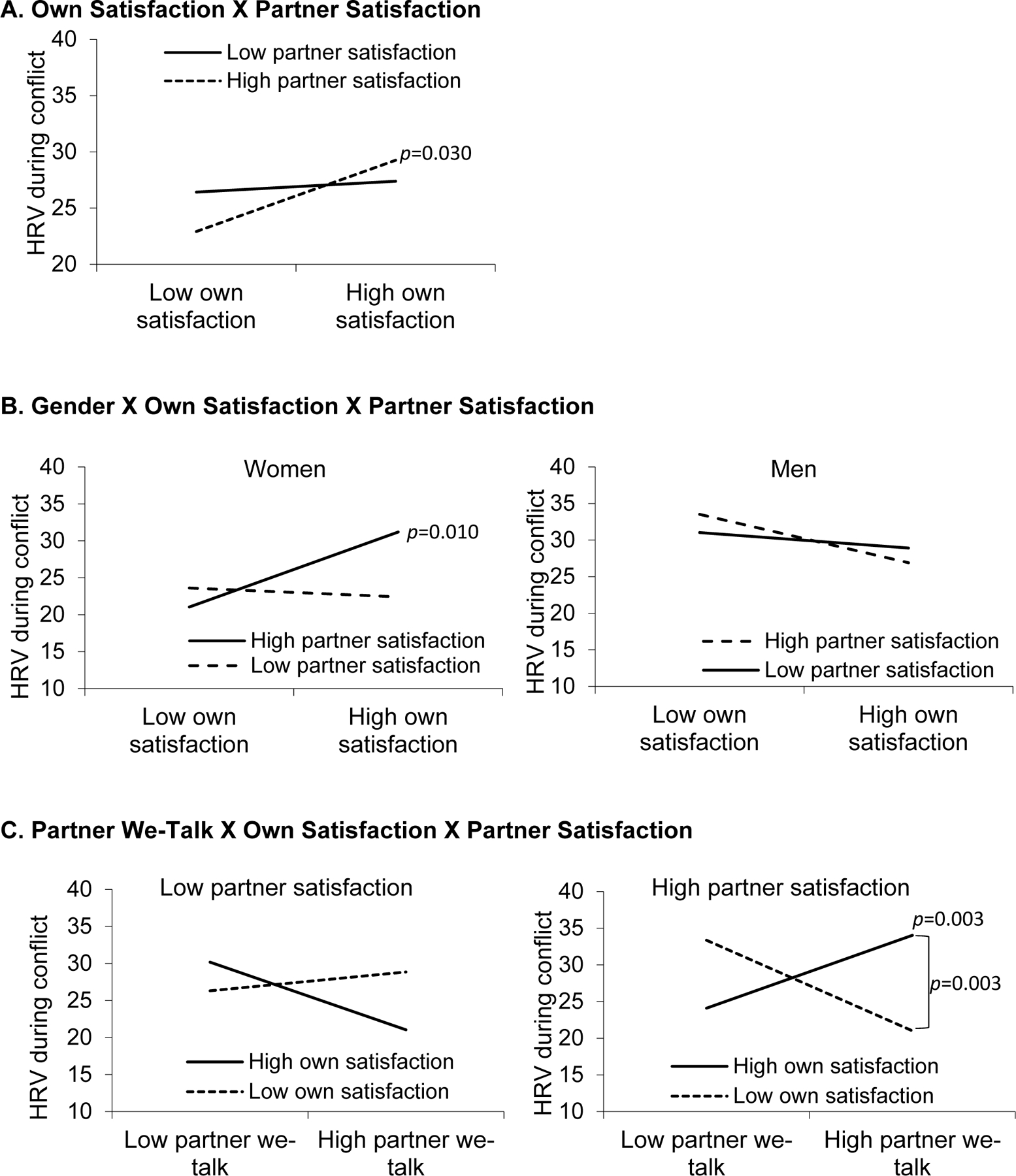
Visual depictions of the interactions predicting HRV during conflict.
When adding interactions with gender, results showed that the 3-way interaction between own satisfaction, partner satisfaction, and gender predicted HRV (b=0.0001, SE=0.0001, p=0.035, 95% CI [0.00001, 0.0002]). As shown in Figure 1B, women’s HRV was highest if both they and their husbands were more satisfied (b=0.007, SE=0.002, p=0.010, 95% CI [0.002, 0.01]). In contrast, there were no differences in women’s HRV only if they or their husbands were satisfied (ps>0.084). Men’s HRV was not different based on their own and their wives’ satisfaction (ps>0.30). Also, women had lower HRV during conflict than men when both spouses (b=−0.137, SE=0.056, p=0.017, 95% CI [−0.25, −0.03]) or women were less satisfied (b=−0.233, SE=0.098, p=0.021, 95% CI [−0.43, −0.04]). There were no gender differences in HRV when both spouses (p=0.17) or women were highly satisfied (p=0.16).
Own and Partner We-Talk
Own and partner we-talk’s main effects and their interaction did not predict HRV during conflict (ps>0.34). Likewise, gender did not moderate effects of own or partner we-talk on HRV (ps>0.056).
Own and Partner Satisfaction and We-Talk
When testing effects of own and partner satisfaction and we-talk, results showed that the three-way interaction between partner we-talk, own satisfaction, and partner satisfaction predicted conflict HRV (b=0.0002, SE=0.0001, p=0.002). As shown in Figure 1C, simple slopes analyses revealed partner we-talk predicted higher HRV if both spouses were more satisfied (b=0.189, SE=0.062, p=0.003), but not if one or both spouses were less satisfied (ps>.052). Among those with high partner we-talk, HRV was higher if they and their spouses were satisfied compared to those with less satisfied spouses (b=0.008, SE=0.004, p=0.003). Thus, HRV was highest when both spouses were satisfied and their partners used we-talk more often. Own we-talk did not moderate the effects of own and/or partner satisfaction on HRV (ps>.13). The interaction between own satisfaction, partner satisfaction, and gender from the previous models still predicted HRV (b=0.0002, SE=0.0001, p=0<0.001, 95% CI [0.00001, 0.0003]). Covariate effects across the models showed that higher baseline HRV predicted greater conflict HRV (p<0.001); no other covariates were related to HRV (ps>0.12).
Momentary Closeness Immediately After Conflict
Own and Partner Satisfaction
Own satisfaction was associated with greater momentary closeness (b=0.07, SE=0.01, p<0.001, 95% CI = [0.06, 0.09]), but partner satisfaction and their interaction did not predict closeness (ps>0.13). When adding gender interactions, results showed gender differences in the effects of own satisfaction (b=0.03, SE=0.01, p=0.004, 95% CI = [0.009, 0.05]) and partner satisfaction (b=−0.03, SE=0.01, p=0.003, 95% CI = [−0.05, −0.01]) on closeness. As shown in Figure 2A and 2B, more satisfied individuals felt closer to their partners after conflict compared to their less satisfied counterparts, and this effect was stronger for women (b=0.10, SE=0.01, p<0.001, 95% CI = [0.07, 0.12]) relative to men (b=0.04, SE=0.01, p=0.003, 95% CI = [0.01, 0.07]). Also, men felt closer to their wives if their wives were more satisfied compared to less satisfied (b=0.04, SE=0.01, p=0.002, 95% CI = [0.01, 0.06]). In contrast, men’s satisfaction was not related to wives’ post-conflict closeness (b=−0.02, SE=0.01, p=0.11, 95% CI = [−0.05, 0.005]).
Figure 2.
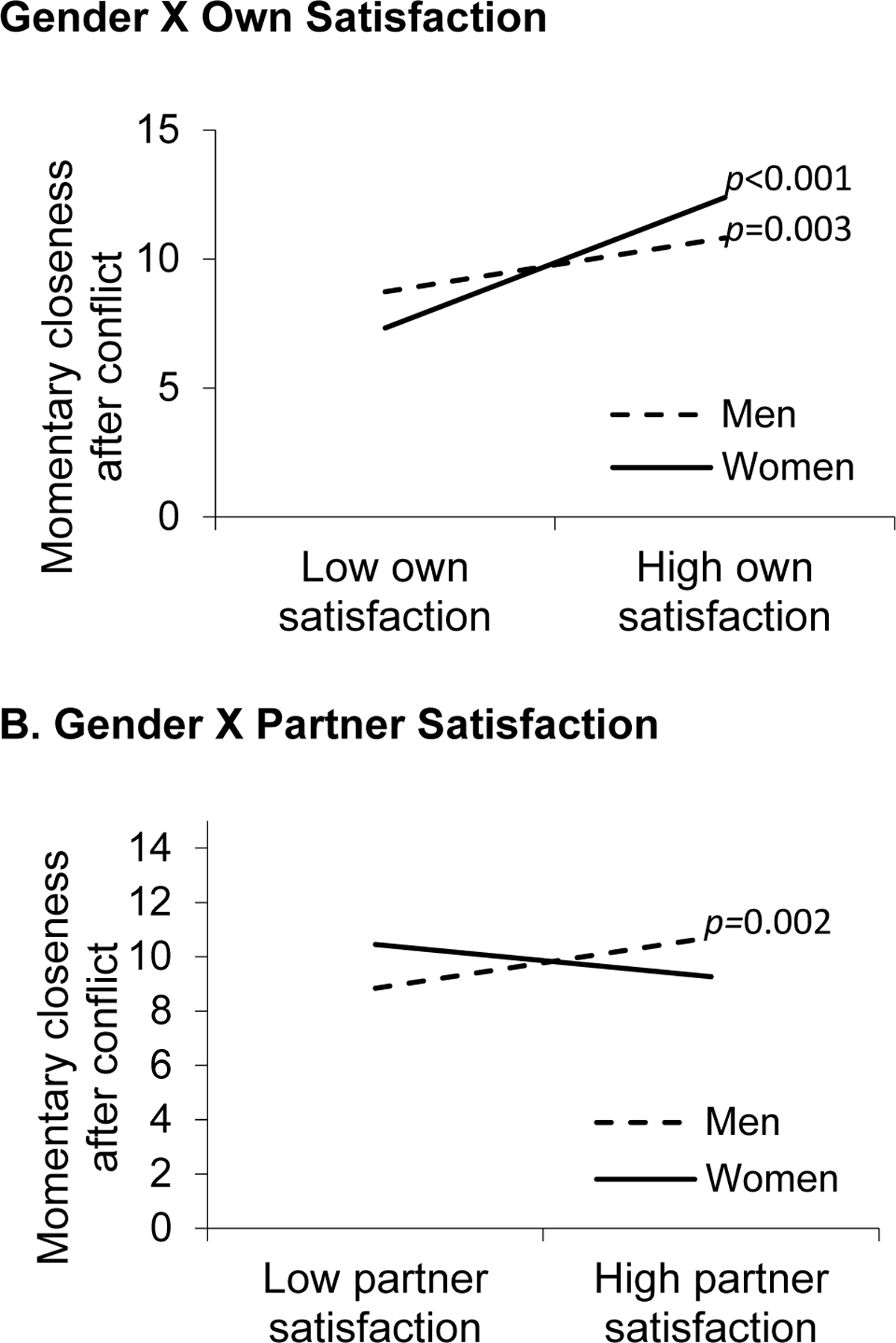
Visual depictions of the interactions predicting momentary closeness immediately after conflict.
Own and Partner We-Talk
Greater partner we-talk was related to higher momentary closeness after conflict (b=0.59, SE=0.24, p=0.014, 95% CI [0.12, 1.07]), whereas own we-talk did not predict momentary closeness (b=0.47, SE=0.24, p=0.053, 95% CI [−0.01, 0.94]). The interaction between own and partner we-talk did not predict closeness (p=0.25), nor did interactions with gender (ps>0.22).
Own and Partner Satisfaction and We-Talk
Own and partner we-talk were no longer related to momentary closeness with own and partner satisfaction in the model (ps>0.63). Interactions between own/partner satisfaction and own/partner we-talk did not predict closeness (ps>0.062). The previously discussed two-way gender interactions with own satisfaction (b=0.03, SE=0.01, p=0.004, 95% CI = [0.008, 0.05]) and partner satisfaction (b=−0.03, SE=0.01, p=0.003, 95% CI = [−0.05, −0.01]) still predicted momentary closeness. For covariates, age was not related to spouses’ post-conflict closeness across the models (ps>0.59)
Rumination 2 Hours After Conflict
Own and Partner Satisfaction
We tested how own and partner satisfaction, along with their interaction, predicted conflict rumination 2 hours after conflict. The own satisfaction effect showed that satisfied spouses had lower rumination relative to less satisfied spouses (b=−0.26, SE=0.11, p=0.026, 95% CI = [−0.49, −0.03]); this effect held after an FDR of .15 but not .10, though it was qualified by interactions below. Partner satisfaction was not related to rumination (p=0.22) nor was the own by partner satisfaction interaction (p=0.061).
When testing gender differences, results showed the three-way interaction between gender, own satisfaction, and partner satisfaction predicted rumination (b=−0.01, SE=0.003, p=0.017, 95% CI = [−0.01, −0.001]). As shown in Figure 3A, in women with satisfied husbands, their own conflict rumination was lower if women themselves were also satisfied (b=−0.56, SE=0.17, p=0.001, 95% CI = [−0.88, −0.23]). If their husbands were less satisfied, women’s rumination was higher and did not change even if they were satisfied (b=0.03, SE=0.20, p=0.87, 95% CI = [−0.36, 0.43]). Men’s rumination did not change based on their own and/or their wives’ satisfaction (ps>0.40). In addition, women’s rumination was lower than men’s when both spouses were satisfied (b=−10.20, SE=4.83, p=0.038, 95% CI = [−19.83, −0.57]).
Figure 3.
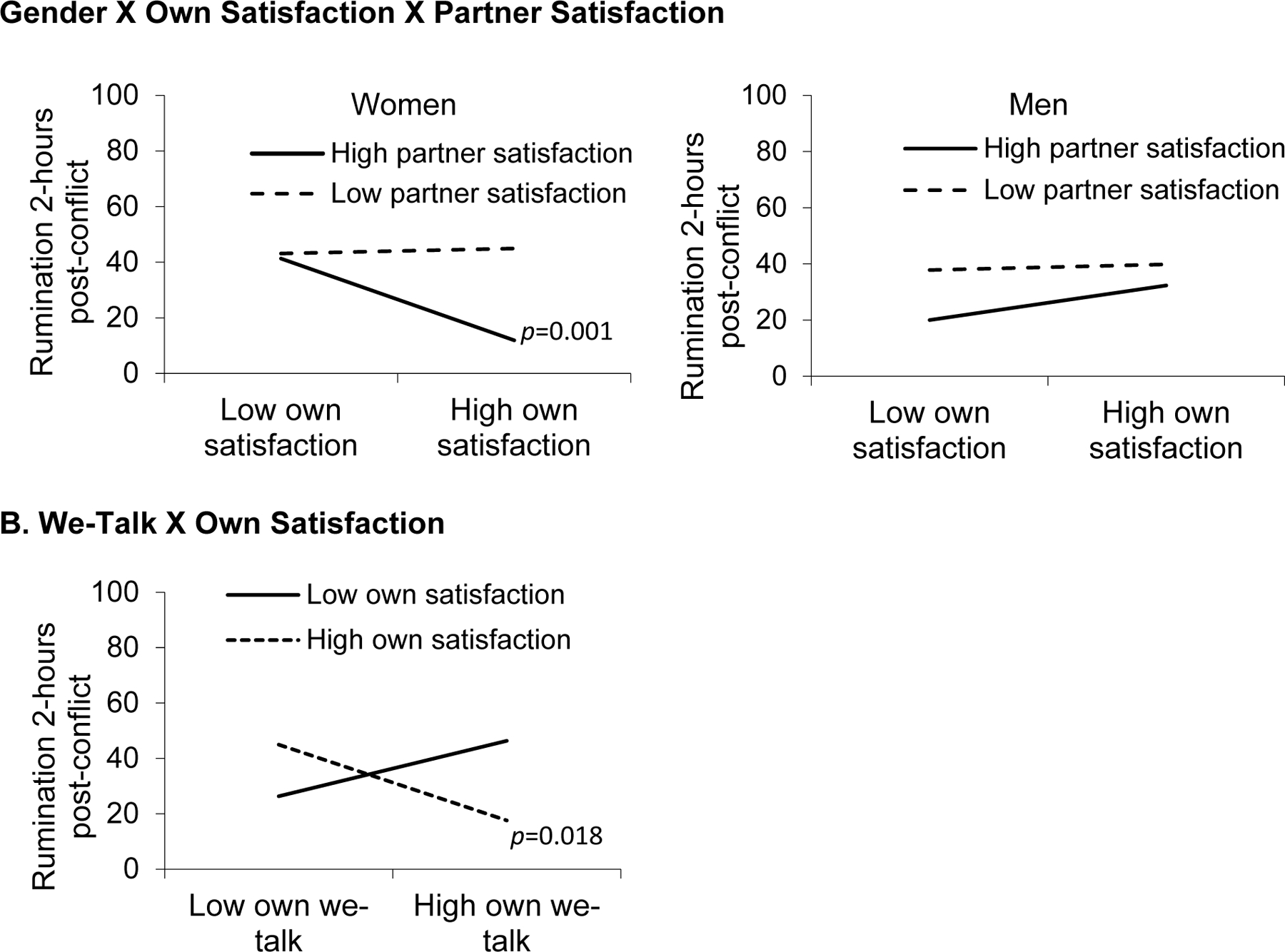
Visual depictions of the interactions predicting rumination 2 hours after conflict.
Own and Partner We-Talk
Greater own we-talk was related to lower rumination 2 hours after conflict (b=−6.45, SE=3.09, p=0.039, 95% CI [−12.56, −0.34]); this effect held after an FDR of .15 but not .10, though it was qualified by an interaction reported below. Partner we-talk was unrelated to post-conflict rumination (p=0.49). The interaction between own and partner we-talk did not predict rumination (p=0.64), nor did interactions with gender (ps>0.44).
Own and Partner Satisfaction and We-Talk
When adding both satisfaction and we-talk to the model, results revealed a two-way interaction between own satisfaction and own we-talk on rumination (b=−0.49, SE=0.21, p=0.019, 95% CI [−0.90, −0.08]). As shown in Figure 3B, satisfied spouses had lower rumination if they used we-talk more often compared to less often (b=−14.96, SE=6.23, p=0.018, 95% CI [−27.28. −2.63]). In contrast, we-talk did not predict less satisfied spouses’ rumination (b=10.93, SE=6.95, p=0.12, 95% CI [−2.82, 24.67]). Thus, conflict rumination was lower in spouses who were more satisfied and used we-talk more often during the conflict. Interactions between partner satisfaction and own/partner we-talk were not related to rumination (ps>0.21), nor were the interactions between own satisfaction, partner satisfaction, and own/partner we-talk (ps>0.21). The previously discussed three-way interaction between gender, own satisfaction, and partner satisfaction still predicted rumination (b=−0.01, SE=0.003, p=0.022, 95% CI = [−0.01, −0.001]).
Discussion
In accord with dyadic stress theories, this study demonstrated that both individuals’ own and their partners’ relationship satisfaction and we-talk during conflict were associated with better physiological, relational, and emotional responses. When individuals or their partners were more satisfied, they had higher HRV during conflict, felt closer immediately after conflict, and ruminated less about the conflict 2 hours later. In contrast, those in less satisfying relationships had lower HRV, lower closeness, and greater rumination. Couples’ satisfying relationships were particularly beneficial for women, helping offset conflict’s physiological, relational, and emotional toll. In addition, spouses’ HRV was higher and rumination was lower if they or their partners were more satisfied and used we-talk more often. Couples who were less satisfied and used we-talk less often had lower HRV during conflict and greater rumination 2 hours after conflict. The combination of mutually satisfying relationships and talking in relational terms may relate to reduced physiological and emotional responses to conflict in middle-aged and older couples.
When examining couples’ relationship satisfaction, each partner’s satisfaction and gender were key. Satisfied spouses had higher HRV during conflict if their partners were also satisfied. Also, satisfied spouses felt closer immediately after conflict and ruminated less about conflict 2 hours later than less satisfied spouses. In contrast, those with less satisfied partners had lower HRV during conflict, and less satisfied spouses also felt less close and ruminated more after conflict. Accordingly, happy spouses and those in mutually satisfying relationships may experience fewer physiological, relational, and emotional consequences after conflict than unhappy and mutually dissatisfied spouses. Consistent with prior research and theory, these findings illustrate a satisfying relationship’s wide-ranging impact (2,15). Extending the literature, this research reveals the importance of assessing each partner’s satisfaction in understanding physiological, relational, and emotional paths from strong relationships to better health.
Gender effects revealed that mutually satisfying relationships particularly benefited women. Women’s HRV was highest and rumination was lowest if they and their husbands were satisfied. Likewise, women had lower HRV and higher rumination than men except when both spouses were satisfied. Thus, women reaped the most physiological and emotional benefits when both spouses were satisfied. In addition, when women were satisfied, they and their husbands felt closer after conflict, suggesting both partners profited from women’s high satisfaction. Men’s satisfaction, however, was not associated with their wives’ post-conflict closeness. These gender differences are consistent with the research showing that conflict negatively affects women’s health more than men’s (28,29), yet revealed women’s health also benefitted more from their mutually satisfying relationships than did men’s. Women with unhappy partners may experience greater physiological and emotional stress during and after conflict, even when they are happy themselves. Yet, a mutually satisfying relationship may help counteract conflict’s physiological and emotional effects on women. Men, in contrast, may reap more relational benefits from having a satisfied spouse. Men rely on their partners for support, especially as they age, and conflict may cause concern about their relationships (48). However, a satisfied spouse may help reduce their relationship worries and promote feelings of relational and emotional closeness even after conflict. These findings highlight the importance of a partner’s satisfaction for women’s physiological and emotional well-being and men’s relational well-being during and after conflict.
In addition to satisfaction, couples’ we-talk during conflict moderated their physiological, relational, and emotional responses. Spouses’ HRV was highest when both couple members were more satisfied and their partners used we-talk more often during conflict. If one or both spouses were less satisfied, a partner’s we-talk did not predict individuals’ own HRV. Likewise, spouses’ rumination was lower 2 hours after conflict if they were more satisfied and used we-talk more often during conflict. In contrast, less satisfied spouses’ rumination was similar regardless of their we-talk during conflict. These findings are notable because they suggest relationships may need to be satisfying for spouses to gain we-talk’s physiological and emotional benefits during and after conflict. We-talk did not interact with satisfaction to predict momentary closeness right after conflict, suggesting that we-talk may be more important for reducing conflict’s physiological and emotional effects. Taken together, these findings extend prior work by illustrating relationship satisfaction and we-talk’s synergistic relational and health effects. Spouses’ we-talk during conflict may signal that they see the problem as shared and want to address it together (25). Thus, during contentious conversations, satisfied couples may be even better off when they think and talk in relational terms. These findings help explain how conflict takes a toll on some couples’ relationships and health but not on others, as well as demonstrate how talking in relational terms provides greater physiological and emotional benefits in marriages.
This study has implications for dyadic stress theories and research on couples’ relationships and health. Dyadic stress models illustrate that spouses influence each other’s health, particularly in during stressful situations (2,15). Indeed, the Dyadic Biobehavioral Stress Model suggests that each partner’s communication strategies during stress confer risks or benefits that influence disease risk and healthy aging. The present study identified each partner’s satisfaction and we-talk during conflict as key predictors of better physiological, relational, and emotional health. These findings are especially important for couples as their lives become increasingly intertwined with age and are at greater risk for age-related health problems and disease (49,50). HRV decreases with stress and age, and low HRV underlies serious conditions and signals cardiovascular decline and early disease risk (8,51,52). Low HRV during marital conflict may reflect poorer cardiac flexibility and reduced regulatory capacity, increasing marital stress-related health risks (12). In addition, older adults’ divorce rates are increasing, despite average divorce rates remaining stable in recent years (53). Conflict is a common yet difficult part of married life. Talking in relational terms may help promote couples’ relationships and health despite conflict and age-related risks. This positive communication strategy may strengthen couples’ shared identities, curb negative emotions, and protect their health.
One strength of this study is the dyadic approach to addressing conflict’s effects—a key method to address marriage’s health impact (54). Having both partners allowed us to examine how their satisfaction and we-talk were related to each other’s physiological, relational, and emotional responses, and identify key gender differences. We were also able to examine gender differences, which showed that men’s relationships benefitted the most when their wives were more satisfied relative to less satisfied, whereas women’s physiological and emotional health benefitted most when they and their husbands were satisfied compared to less satisfied. This study also considered how global relationship perceptions and conflict-specific communication patterns contributed to conflict responses. Spouses’ satisfaction provided the lens through which partners see their relationships, while their we-talk provided a window into how they talk in daily life. Findings suggested both elements were important for understanding conflict’s relational and health toll. This study also adds to the growing literature illustrating pathways from strong relationships to better health, notably among middle-aged and older couples, an understudied group whose relationships are central to their health (2).
A limitation of this study was the fact that couples were primarily white, highly educated, and higher income Americans in different-gender relationships and in good health. Studies including same-gender couples would help tease apart gender effects related to a person’s own gender and a partner’s gender. Likewise, though significant effort went into recruiting less happy couples, the sample was highly satisfied with their relationships. The current findings may underestimate effects and be more pronounced in couples with greater marital strife. To reduce chronic disease- and medication-related confounds, the sample was recruited for their good health; future work should include fewer health restrictions to test generalizability. Additionally, the parent study was powered to test three-way hypotheses, but power might have played a role in higher order (e.g., four-way) interactions. Even so, these findings inform future work and should be examined in larger, more diverse samples.
Limitations around measurement include that the post-conflict rumination and momentary closeness measures were one- and two-item measures, respectively, and the rumination item may not reflect maladaptive thoughts. Though rumination and closeness were correlated in the expected directions with relationship satisfaction and we-talk, and also negatively correlated with each other, longer measures may capture these experiences more precisely. It is also possible that asking partners about the conflict while still in the lab where the discussion took place affected their responses. Likewise, it is worthwhile to consider if not thinking about the discussion is adaptive or maladaptive. Similarly, couples’ conflicts may look different in daily life than in a laboratory setting. Research suggests laboratory studies provide more conservative estimates (55); thus, the effects in this study may be stronger if captured in couples’ natural settings. Future work might include daily designs to examine conflict in couples’ natural environments, while also examining intra-individual, within-person differences in partners’ daily conflict experiences and responses. These questions provide an interesting avenue for research addressing conflict’s relational and health aftermath.
This study demonstrated how aging couples’ relationship satisfaction and we-talk were associated with lower physiological, relational, and emotional responses to conflict. Satisfied spouses or those in mutually satisfying relationships had higher HRV during conflict, felt closer immediately after conflict, and ruminated less about the conflict 2 hours later. Spouses’ HRV was highest and rumination was lowest when they or their partners were satisfied and used we-talk more often. Both spouses also benefitted from women’s satisfaction: when women were more satisfied relative to less satisfied, they and their husbands felt closer after conflict. Likewise, women had higher HRV, felt closer, and ruminated less when they or their husbands were more satisfied; also, women’s HRV and rumination were similar to men’s only when both spouses were satisfied. Thus, a mutually satisfying relationship may help shield women from greater conflict reactivity. This research contributes to research and theory on how couples’ relationships enhance or hinder health, and the findings show a satisfying marriage’s relational and health benefits may be strongest when both spouses are satisfied.
Funding:
Work on this project was supported by Ohio State University Presidential Postdoctoral Scholars Fellowship to the first author, and NIH grants KL2TR002530, UL1TR002529, UL1TR001070, UL1TR002733, R01 AG057032, T32 CA229114, and TL1TR002735.
Abbreviations:
- CSI
couples satisfaction inventory
- HRV
Heart rate variability
- LIWC
Linguistic Inquiry and Word Count
- MLM
Multilevel modeling
- SAD
Sagittal abdominal diameter
Footnotes
Declaration of Conflicting Interests: The author(s) declared that there were no conflicts of interest with respect to the authorship or the publication of this article.
References
- 1.Robles TF, Slatcher RB, Trombello JM, McGinn MM. Marital quality and health: A meta-analytic review. Psychological bulletin 2014;140:140–87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kiecolt-Glaser JK, Wilson S. Lovesick: How couples’ relationships influence health. Annual Review of Clinical Psychology 2017;8:421–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Holt-Lunstad J, Robles TF, Sbarra DA. Advancing social connection as a public health priority in the United States. American Psychologist 2017;72:517–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Orth-Gomér K, Wamala SP, Horsten M, Schenck-Gustafsson K, Schneiderman N, Mittleman MA. Marital Stress Worsens Prognosis in Women With Coronary Heart Disease The Stockholm Female Coronary Risk Study. Journal of the American Medical Association [Internet] 2000;23:3008–14. Available from: https://jamanetwork.com/ [DOI] [PubMed] [Google Scholar]
- 5.Liu H, Waite L. Bad marriage, broken heart? Age and gender differences in the link between marital quality and cardiovascular risks among older adults. Journal of Health and Social Behavior 2014;55:403–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Troxel WM, Matthews KA, Gallo LC, Lewis Kuller H. Marital Quality and Occurrence of the Metabolic Syndrome in Women. Archives of Internal Medicine [Internet] 2005;165:1022–27. Available from: https://jamanetwork.com/ [DOI] [PubMed] [Google Scholar]
- 7.Wilson SJ, Bailey BE, Jaremka LM, Fagundes CP, Andridge R, Malarkey WB, Gates KM, Kiecolt-Glaser JK. When couples’ hearts beat together: Synchrony in heart rate variability during conflict predicts heightened inflammation throughout the day. Psychoneuroendocrinology 2018;93:107–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Thayer JF, Åhs F, Fredrikson M, Sollers JJ, Wager TD. A meta-analysis of heart rate variability and neuroimaging studies: Implications for heart rate variability as a marker of stress and health Vol. 36, Neuroscience and Biobehavioral Reviews. 2012. p. 747–56. [DOI] [PubMed] [Google Scholar]
- 9.Turner AI, Smyth N, Hall SJ, Torres SJ, Hussein M, Jayasinghe SU, Ball K, Clow AJ. Psychological stress reactivity and future health and disease outcomes: A systematic review of prospective evidence. Psychoneuroendocrinology [Internet] 2020;114:104599. Available from: 10.1016/j.psyneuen.2020.104599 [DOI] [PubMed] [Google Scholar]
- 10.Thayer JF, Yamamoto SS, Brosschot JF. The relationship of autonomic imbalance, heart rate variability and cardiovascular disease risk factors Vol. 141, International Journal of Cardiology. 2010. p. 122–31. [DOI] [PubMed] [Google Scholar]
- 11.Laborde S, Mosley E, Thayer JF. Heart rate variability and cardiac vagal tone in psychophysiological research - Recommendations for experiment planning, data analysis, and data reporting Vol. 8, Frontiers in Psychology. Frontiers Research Foundation; 2017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kiecolt-Glaser JK, Renna ME, Shrout MR, Madison AA. Stress Reactivity: What Pushes Us Higher, Faster, and Longer—and Why It Matters. Current Directions in Psychological Science 2020;29:492–98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Smith TW, Cribbet MR, Nealey-Moore JB, Uchino BN, Williams PG, MacKenzie J, Thayer JF. Matters of the Variable Heart: Respiratory Sinus Arrhythmia Response to Marital Interaction and Associations With Marital Quality. Journal of Personality and Social Psychology 2011;100:103–19. [DOI] [PubMed] [Google Scholar]
- 14.Donoho CJ, Seeman TE, Sloan RP, Crimmins EM. Marital status, marital quality, and heart rate variability in the MIDUS cohort. Journal of Family Psychology 2015;29:290–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Shrout MR. The Health Consequences of Stress in Couples: A Review and New Integrated Dyadic Biobehavioral Stress Model. Brain, Behavior, & Immunity - Health [Internet] 2021;16. Available from: 10.1016/j.bbih.2021.100328 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bodenmann G A systemic-transactional conceptualization of stress and coping in couples. Swiss Journal of Psychology 1995;54:34–49. [Google Scholar]
- 17.Bodenmann G Dyadic coping and its significance for marital functioning 2005. [Google Scholar]
- 18.lyons renee, mickelson kristin, sullivan michael, coyne james. coping as a communal process. Journal of Social and Personal Relationships 1998; [Google Scholar]
- 19.Robles TF, Kiecolt-Glaser JK. The physiology of marriage: Pathways to health. Physiology and Behavior 2003;79:409–16. [DOI] [PubMed] [Google Scholar]
- 20.Wilson SJ, Andridge R, Peng J, Bailey BE, Malarkey WB, Kiecolt-Glaser JK. Thoughts after marital conflict and punch biopsy wounds: Age-graded pathways to healing. Psychoneuroendocrinology 2017;85:6–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Helm JL, Sbarra DA, Ferrer E. Coregulation of respiratory sinus arrhythmia in adult romantic partners. Emotion 2014;14:522–31. [DOI] [PubMed] [Google Scholar]
- 22.Ditzen B, Neumann ID, Bodenmann G, von Dawans B, Turner RA, Ehlert U, Heinrichs M. Effects of different kinds of couple interaction on cortisol and heart rate responses to stress in women. Psychoneuroendocrinology 2007;32:565–74. [DOI] [PubMed] [Google Scholar]
- 23.Wilson SJ, Jaremka LM, Fagundes CP, Andridge R, Kiecolt-Glaser JK. Does it matter whether we or I talk about us? Distinguishing we-talk in couples’ conflict discussions and partners’ private thoughts before and after conflict. Journal of Social and Personal Relationships 2021; [Google Scholar]
- 24.Seider BH, Hirschberger G, Nelson KL, Levenson RW. We Can Work It Out: Age Differences in Relational Pronouns, Physiology, and Behavior in Marital Conflict. Psychology and Aging 2009;24:604–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Karan A, Rosenthal R, Robbins ML. Meta-analytic evidence that we-talk predicts relationship and personal functioning in romantic couples. Journal of Social and Personal Relationships 2019;36:2624–51. [Google Scholar]
- 26.Shrout MR. Couples and nonvisible chronic illness: An integrated model of dyadic Coping. Dissertation 2019;23:2019. [Google Scholar]
- 27.Manne SL, Siegel S, Kashy D, Heckman CJ. Cancer-specific relationship awareness, relationship communication, and intimacy among couples coping with early stage breast cancer. Journal of social and personal relationships [Internet] 2014;31:314–34. Available from: http://www.scopus.com/inward/record.url?eid=2-s2.0-84898951235&partnerID=tZOtx3y1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kiecolt-Glaser JK, Newton TL. Marriage and health: His and hers. Psychological Bulletin 2001;127:472–503. [DOI] [PubMed] [Google Scholar]
- 29.Wanic R, Kulik J. Toward an Understanding of Gender Differences in the Impact of Marital Conflict on Health. Sex Roles 2011;65:297–312. [Google Scholar]
- 30.Orbuch TL, Bauermeister JA, Brown E, Mckinley BD. Early Family Ties and Marital Stability Over 16 Years: The Context of Race and Gender. Family Relations 2013;62:255–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Cross SE, Madson L. Models of the Self: Self-Construals and Gender. Psychological Bulletin 1997;122:5–37. [DOI] [PubMed] [Google Scholar]
- 32.Smith TW, Berg CA, Florsheim P, Uchino BN, Pearce G, Hawkins M, Henry NJM, Beveridge RM, Skinner MA, Olsen-Cerny C. Conflict and Collaboration in Middle-Aged and Older Couples: I. Age Differences in Agency and Communion During Marital Interaction. Psychology and Aging 2009;24:259–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Shrout MR, Brown RD, Orbuch TL, Weigel DJ. A multidimensional examination of marital conflict and subjective health over 16 years. Personal Relationships 2019;26:490–506. [Google Scholar]
- 34.Kiecolt-Glaser JK, Loving TJ, Stowell JR, Malarkey WB, Lemeshow S, Dickinson SL, Glaser R. Hostile marital interactions, proinflammatory cytokine production, and wound healing. Archives of General Psychiatry 2005;62:1377–84. [DOI] [PubMed] [Google Scholar]
- 35.Funk JL, Rogge RD. Testing the ruler with item response theory: Increasing precision of measurement for relationship satisfaction with the couples satisfaction index. Journal of Family Psychology 2007;21:572–83. [DOI] [PubMed] [Google Scholar]
- 36.Pennebaker JW, Boyd RL, Jordan K, Blackburn K. The development and psychometric properties of LIWC2015 Austin, TX; 2015. [Google Scholar]
- 37.Lin WF, Chen LH, Li TS. Are “We” Good? A Longitudinal Study of We-Talk and Stress Coping in Dual-Earner Couples. Journal of Happiness Studies 2016;17:757–72. [Google Scholar]
- 38.Jaremka LM, Collins NL. Current Closeness to Partner Scale University of California Santa Barbara. 2011. [Google Scholar]
- 39.Bogdány T, Boros S, Szemerszky R, Köteles F. Validation of the Firstbeat TeamBelt and BodyGuard2 systems Health tourism View project Nutrition as an intervention View project 2016;4–12. Available from: https://www.researchgate.net/publication/308809187 [Google Scholar]
- 40.Hinde K, White G, Armstrong N. Wearable devices suitable for monitoring twenty four hour heart rate variability in military populations. Sensors 2021;21:1–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Tarvainen MP, Niskanen JP, Lipponen JA, Ranta-aho PO, Karjalainen PA. Kubios HRV - Heart rate variability analysis software. Computer Methods and Programs in Biomedicine [Internet] 2014;113:210–20. Available from: 10.1016/j.cmpb.2013.07.024 [DOI] [PubMed] [Google Scholar]
- 42.Sin NL, Sloan RP, McKinley PS, Almeida DM. Linking daily stress processes and laboratory-based heart rate variability in a national sample of midlife and older adults. Psychosomatic Medicine 2016;78:573–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Senkans S, McEwan TE, Skues J, Ogloff JRP. Development of a Relational Rumination Questionnaire. Personality and Individual Differences [Internet] 2016;90:27–35. Available from: 10.1016/j.paid.2015.10.032 [DOI] [Google Scholar]
- 44.Kenny DA, Kashy DA, Cook WL. Dyadic data analysis. Dyadic data analysis. New York, NY, US: Guilford Press; 2006. (Methodology in the social sciences (Kenny David A., Series Editor).). [Google Scholar]
- 45.Benjamini Y, Hochberg Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing Vol. 57, Source: Journal of the Royal Statistical Society. Series B (Methodological). 1995. [Google Scholar]
- 46.McDonald JH. Handbook of Biological Statistics 3rd ed. Baltimore, Maryland. : Sparky House Publishing; 2014. [Google Scholar]
- 47.Aiken LS, West SG. Multiple regression: Testing and interpreting interactions. Multiple regression: Testing and interpreting interactions Thousand Oaks, CA, US: Sage Publications, Inc; 1991. xi, 212–xi, 212. [Google Scholar]
- 48.Antonucci TC. Social relations: An examination of social networks, social support, and sense of control. In: Handbook of the psychology of aging, 5th ed. San Diego, CA, US: Academic Press; 2001. p. 427–53. [Google Scholar]
- 49.Hoppmann CA, Gerstorf D. Biobehavioral Pathways Underlying Spousal Health Dynamics: Its Nature, Correlates, and Consequences. Gerontology 2014;60:458–65. [DOI] [PubMed] [Google Scholar]
- 50.Carstensen LL. Evidence for a life-span theory of socioemotional selectivity. Current Directions in Psychological Science 1995;4:151–56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Zulfiqar U, Jurivich DA, Gao W, Singer DH. Relation of High Heart Rate Variability to Healthy Longevity. American Journal of Cardiology 2010;105:1181–85. [DOI] [PubMed] [Google Scholar]
- 52.Wilson SJ, Woody A, Padin AC, Lin J, Malarkey WB, Kiecolt-Glaser JK. Loneliness and telomere length: Immune and parasympathetic function in associations with accelerated aging. Annals of Behavioral Medicine 2019;53:541–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Brown SL, Lin I-F. The Graying of Divorce: A Half Century of Change. The Journals of Gerontology: Series B [Internet] 2022;gbac057. Available from: 10.1093/geronb/gbac057 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Pietromonaco PR, Collins NL. Interpersonal mechanisms linking close relationships to health. American Psychologist 2017;72:531–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Heyman RE. Observation of couple conflicts: Clinical assessment applications, stubborn truths, and shaky foundations. Psychological Assessment 2001;13:5–35. [DOI] [PMC free article] [PubMed] [Google Scholar]