

Abstract
The aim of this study was to examine the role of walking in explaining associations between perceived and objective measures of walkability and cognitive function among older adults. The study employed a cross-sectional design analyzing existing data. Data were obtained from the Adult Changes in Thought Activity Monitor study. Cognitive function and perceived walkability were measured by a survey. Objective walkability was measured using geographic information systems (GIS). Walking was measured using an accelerometer. We tested the mediating relationship based on 1,000 bootstrapped samples. Perceived walkability was associated with a 0.04 point higher cognitive function score through walking (p = .006). The mediating relationship accounted for 34% of the total relationship between perceived walkability and cognitive function. Walking did not have a significant indirect relationship on the association between objective walkability and cognitive function. Perceived walkability may be more relevant to walking behavior than objective walkability among older adults. Greater levels of perceived walkability may encourage older adults to undertake more walking, and more walking may in turn improve cognitive function in older adults.
Keywords: Built environment, Cognitive function, Walking, Mediation analysis, Older adults
Introduction
Growing evidence suggests that neighborhood environment can be positively associated with health behaviors (e.g., physical activity) and health outcomes (e.g., mental health) (Bird et al., 2018). Living in a neighborhood that lacks essential factors such as services, parks, and sidewalks can increase the risk of cardiovascular conditions and cancer in residents (Bird et al., 2018, Michael and Yen, 2014). However, the potential role of neighborhood environments on older adults’ cognitive function has been given little attention (Besser et al., 2017, Wu et al., 2015a, Cerin, 2019). A few studies investigated the role and found positive associations between neighborhood walkability and cognitive function. Walkability in the current study refers to a measure of the degree to which neighborhoods can entice and support walking (Forsyth, 2015, Mooney et al., 2020). For instance, people living in areas with high land-use mix have a lower risk of cognitive impairment (Wu et al., 2017) and dementia (Wu et al., 2015b). Higher street connectivity (i.e., how well streets are interconnected) is related to a lower risk of cognitive impairment (Koohsari et al., 2019) and better cognitive function (Watts et al., 2015, Ng et al., 2018). A walkability index, developed using a weighted composite score of residential density, street connectivity, and land-use mix, is also associated with better cognitive function (Ng et al., 2018) and better neuroimaging outcomes (Cerin et al., 2017b). It is important to understand the ways in which neighborhood factors are embodied to affect cognitive function.
An ecological model of cognitive health suggests multiple pathways from built and natural environment to cognitive health and one of the mechanisms is through lifestyle behaviors such as physical activity (Cerin, 2019). Walkability is associated with promoting daily walking, which is in turn linked to better cognitive function. Walking might partially explain the connection between neighborhood walkability and cognitive function in older adults. A positive association between walkability and walking has been observed among older adults (Kerr et al., 2012, Barnett et al., 2017, Rosso et al., 2021). For example, residential density, walkability index, land use mix, public transport, parks, and recreational destinations were positively associated with walking among older adults (Cerin et al., 2017a). Walking is a promising modifiable factor that can be targeted to improve and preserve cognitive function through reducing cardiovascular risk factors and modifying brain metabolism and structure in older adults (Kirk-Sanchez and McGough, 2014). Walking is the most popular and convenient physical activity for older adults, because it does not require special skills or equipment, and its intensity can be easily adjusted based on one’s physical ability (Morris and Hardman, 1997, Notthoff and Carstensen, 2014).
Despite the importance of understanding this mechanism, only few studies have investigated the mediating relationship of walkability on cognitive health through physical activity in older adults (Clarke et al., 2012, Koohsari et al., 2019, Ng et al., 2018). However, these studies performed mediation analysis by determining whether a significant association between walkability and cognitive health remained or was attenuated after adjusting for physical activity, rather than by conducting a formal statistical analysis to estimate an indirect relationship and corresponding confidence interval. A study performed a mediation analysis of physical activity on the association between walkability and brain imaging using the bootstrap-based product of coefficients test, but the study was conducted only among individuals with mild cognitive impairment or Alzheimer’s disease (Cerin et al., 2017b). Thus, the result may differ among older adults with normal cognitive function.
Moreover, most studies included objective walkability, measured by geographic information system (GIS) or neighborhood audits, but not subjective walkability. Lawton’s ecological model of aging postulated a role of individual perception of physical environment on manifestation of behaviors as a result of person-environment interactions (Lawton, 1982; Lawton 1989). A few studies have nonetheless found low to moderate agreement between objective and subjective measures (e.g., survey) of neighborhood environments (Gebel et al., 2009, Michael et al., 2006). Perceptions of physical neighborhood environments (called “perceived neighborhood attributes” hereafter) are influenced by individual judgment and may differ from objective measures. Perceived neighborhood attributes may be distinctly related to walking as well as to cognitive function from objective neighborhood characteristics.
The aims of this study were to: 1) examine the association between perceived and objective walkability and cognitive function in older adults, and 2) test if walking is a mediator in associations between walkability and cognitive function (Figure 1). We hypothesized that having greater perceived walkability and living in areas with greater objective walkability would be associated with better cognitive function, and that walking would partially or fully mediate these associations.
Figure 1.
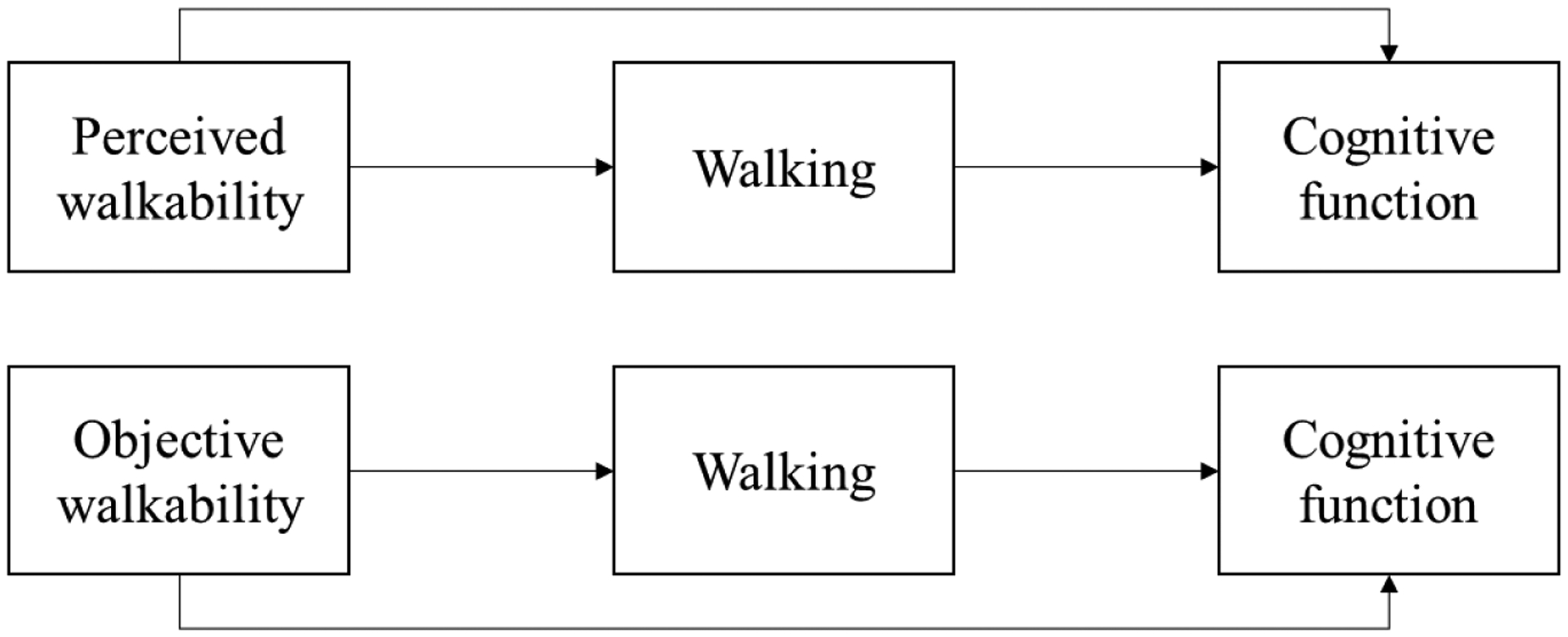
Pathways from perceived and objective walkability to cognitive function through walking.
Methods
Design and Participants
This is a cross-sectional study that analyzed existing data collected as part of the Adult Changes in Thought Activity Monitor (ACT-AM) study. Its parent study, the ACT study, is a prospective cohort study that began in 1994 to investigate the incidence of dementia and related risk factors among community-dwelling older adults (Kukull et al., 2002). Adults aged 65 and above without dementia were randomly selected from the King County members of Kaiser Permanente Washington (KPWA) in the state of Washington state, USA. The cohort was expanded in 2000 and continuous enrollments were initiated in 2004 to compensate for dropouts due to development of dementia, loss to follow-up, or death (Marcum et al., 2019, Mez et al., 2017). Biennial follow-ups were arranged for the cohort members.
The ACT-AM study was launched in 2016 to better understand physical activity patterns among older adults (Rosenberg et al., 2020). Those who were wheelchair-bound, had critical illnesses, and resided in nursing homes were excluded from the study. Participants were asked to wear activity monitoring devices (Actigraph wGT3X+ and activPAL micro) and to log their detailed device wear and sleep times for seven days. In the present analysis, ACT-AM study participants who had valid physical activity data (i.e., data for more than 10 hours of out-of-bed time for at least four days) were included. Participants who resided outside King County, Washington State, USA were excluded due to limited availability of objective walkability data. A total of 829 participants were eligible for this study. After excluding missing data on cognitive function (n = 11) and race/ethnicity (n = 4), 814 observations were included in the analysis. The majority of participants lived in urban areas. This study was approved by the University of Washington Institutional Review Board (STUDY00007736).
Measures
Outcome: Cognitive function
Cognitive function was measured with the Cognitive Ability Screening Instrument (CASI), consisting of nine domains: attention, concentration, orientation, short-term memory, long-term memory, language abilities, visual construction, list-generating fluency, and abstraction and judgment. The total score that can be used to identify potential dementia, rather than domain specific scores, was selected. The total score ranges from 0 to 100 with a higher score indicating better cognitive function (Teng et al., 1994). Outcome data were collected once between 2018 and 2019 except for one case measured in 2017.
Exposures: Perceived and objective walkability
Walkability in this study is defined as the degree to which places encourage and support walking (Forsyth, 2015, Mooney et al., 2020). Perceived neighborhood walkability was measured using a neighborhood environment index from the Physical Activity Neighborhood Environment Scale (PANES), which was developed based on adult participants (Sallis et al., 2010). In the PANES survey, a home neighborhood is defined as a surrounding area within a 10 to 15-minute walking distance from home. This study included six core questions from the PANES questionnaire about residential density, land-use mix, transit access, sidewalk coverage, bicycling infrastructure, and recreation facilities (Sallis et al., 2009). Residential density was measured by inquiring about the main type of housing in a participant’s neighborhood. Detached single-family housing was considered as having low residential density, and other types of housing such as condos, townhouses, or apartments were regarded as having high residential density. Land-use mix was assessed by checking whether essential service establishments, such as shops, markets, or other places to buy things from, were located within a short walking distance of home. Regarding transit access, participants were asked whether there was a transit stop within walking distance from home. Sidewalk coverage referred to the existence of paved paths for pedestrians on most streets in the participant’s neighborhood, and bicycling infrastructure pertained to existence of facilities supporting bicycling in or near the participant’s neighborhood. Recreation facilities were measured by asking whether the neighborhood had several free or low-cost recreational facilities, such as parks, trails, and recreation centers. All questions except the one about residential density had four response options: 1 (strongly disagree), 2 (somewhat disagree), 3 (somewhat agree), and 4 (strongly agree). The responses to the six questions were dichotomized (1 and 2 to 0, signifying low; 3 and 4 to 1, signifying high) and then summed to construct a perceived walkability index, as in prior papers (Sallis et al., 2009, Sallis et al., 2010). The possible range was 0 to 6 with a higher score indicating greater walkability in the neighborhood. The data were collected at one time between 2016 and 2019. Cronbach’s α in this sample was 0.54.
An objective walkability index for each participant’s home neighborhood was created using GIS for spatial data processing. An 800 m Euclidean buffer, corresponding to a 10 to 15-minute walking distance, was created for each central point of the census block (i.e., the smallest geographic unit used to collect decennial census data) in which participants resided; the actual residence locations were not used to protect participant identities. An 800m buffer was used because the median walking trip distance was found to be 729 m in older adults living in a medium-sized city (Prins et al., 2014). Because they were based on GIS measurements within the buffer, objective neighborhood walkability index values were identical for individuals living in the same census block. Of the 713 census blocks within the study area, only 75 census blocks (10.5%) had more than two participants.
The objective walkability index was created using a weighted composite index of land-use mix, residential density, and intersection density and each variable was standardized and weighted by 6, 1, and 1, respectively because the formula showed the greatest explanatory power of the variation in physical activity in previous work (Frank et al., 2005). A higher score indicates greater walkability. This walkability index is considered to capture a walkable environment more comprehensively compared to Walk Score ®, which has been widely used, but is based only on points of interest (Walk Score, n.d.), but does not consider other factors within the neighborhood (Frank et al., 2021). Land-use mix was developed using the 2016 King County Assessor’s data for parcels, with reclassifying predominant use into residential, commercial, office, or none of the three land-use types. Data were processed using an area-based entropy formula that describes the evenness in the distribution of areas with residential, commercial, and office land-uses (Frank, 1994, Frank et al., 2005). Residential density was calculated using housing unit counts within buffer area in square meters (count/m2), also using 2016 King County Assessor’s data. Intersection density was measured using the number of three-way intersections divided by the buffer area in square meters (count/m2), from 2016 US Census TIGER/Line road data. Data for both residential and intersection density were converted from vector format using the selected buffer size to SmartMaps, which is a spatial data format developed for efficient data extraction for area-level variables at any point location within the study area (Hurvitz and Moudon, 2012).
Mediator: Walking
Walking was quantified as average daily step counts for each participant using a thigh-worn accelerometer (activPAL micro, PAL Technologies, Glasgow, Scotland, UK), a validated device for measuring steps in older adults (Hergenroeder et al., 2018). The detailed methods are published elsewhere (Rosenberg et al., 2020). Briefly, consenting participants were asked to wear the device for seven days and to keep a log for the times at which they went to sleep at night and got up in the morning; accelerometer data recorded during sleeping bouts were not included in the analyses. All steps were counted regardless of when (weekends vs. weekdays) and where (home neighborhoods vs. other areas) they were taken.
Other covariates and descriptive variables
Other covariates included age (65–74 years [reference], 75–84 years, ≥ 85 years), sex assigned at birth (female [reference], male), race/ethnicity (non-White race or Hispanic ethnicity [reference], non-Hispanic White), and education (< 12 years [reference], 12–15 years, > 15 years). Additionally, self-rated health (excellent, very good, good, fair, poor) and duration of residence (1–5 years, 6–10 years, 11–20 years, and ≥ 21 years) were added to describe sample that may be helpful to generalize the findings from this study to other settings or interpret the findings. All variables except the duration of residence were measured once from 2016 to 2018 (mostly between 2016 and 2017). The duration of residence was calculated from the history of their address since enrollment in the study.
Statistical Analysis
Descriptive statistics for all individual- and neighborhood-level variables were calculated. We assessed any violation of linear regression assumptions. We found slightly skewed distribution of walking and cognitive function variables, but given the large sample size (i.e., greater than 500), we expect impact on statistical inference to be minimal due to the Central Limit Theorem (Lumley et al., 2002). We did not find obvious evidence of violation of linearity assumption based on plots of residuals against fitted values of outcome variables in all models. We assumed that perceived and objective walkability capture different aspects of actual neighborhood environments. Therefore, for both perceived and objective neighborhood walkability, unadjusted and adjusted linear regression models were fitted between walkability and cognitive function (exposure and outcome), walking and cognitive function (mediator and outcome), and walkability and walking (exposure and mediator) to assess associations among exposures, mediator, and outcome. In the analysis with perceived walkability as exposure, 680 cases were included due to missing perceived walkability values from the survey (n = 134). Accounting for 15 missing objective values, 799 observations were included in the analysis with objective walkability as an exposure. In all adjusted models, age, education, race/ethnicity, and sex at birth were controlled. For mediation analysis, a model-based approach was applied (Tingley et al., 2014). Two models were developed: a mediator model specifying the conditional distribution of the mediator, given the exposure and confounders; and an outcome model specifying the conditional distribution of the outcome, given the exposure, mediator, and confounders (Dobra et al., 2020). After these two models were applied, the size of the mediation relationship on the association between walkability and cognitive function was estimated (i.e., indirect relationship). Subsequently, the bias-corrected and accelerated (BCa) confidence intervals were computed for the estimate based on 1,000 simulations (i.e., bootstrapping). The mediation R package version 4.5.0 was utilized. All statistical analyses were performed using R version 3.6.2 (R Foundation for Statistical Computing, Vienna, Austria) and the GIS analysis was conducted using ArcGIS Pro version 2.4 (Esri Inc, Redlands, CA). Processing of vector data to SmartMaps was performed using R 3.6.0 with the sf, raster, and velox packages, and PostgreSQL 11.6 with the PostGIS 2.5 spatial extension.
Results
Table 1 presents the sample descriptive statistics. The mean age was 77 years (SD = 6.7) with slightly more than half the participants being female (n = 470, 57.7%). The majority of participants were non-Hispanic White (n = 724, 88.9%) and highly educated (greater than 15 years, n = 615, 75.6%). Most participants had lived at their home addresses for at least six years (n = 738, 90.7%) and regarded their health either good (n = 252, 31.0%) or very good (n = 351, 43.1%). The mean CASI score was 95.2 (SD = 4.7). On average, the perceived walkability score was 4.17 (SD = 1.49) and the objective walkability score was −0.13 (SD = 7.3) with a range from −11.3 to 23.0. The Pearson correlation coefficient for the association between perceived and objective walkability was 0.37.
Table 1.
Individual-level and neighborhood-level characteristics (N = 814).
| Characteristics | Mean (SD) or n (%) |
|---|---|
| Individual-level characteristic | |
| Age group | |
| 65–74 year | 343 (42.1) |
| 75–84 year | 348 (42.8) |
| ≥ 85 year | 123 (15.1) |
| Sex at birth | |
| Female | 470 (57.7) |
| Male | 344 (42.3) |
| Race/ethnicity | |
| Hispanic or non-White | 90 (11.1) |
| Non-Hispanic White | 724 (88.9) |
| Education | |
| < 12 year | 12 (1.5) |
| 12–15 year | 187 (23.0) |
| > 15 year | 615 (75.6) |
| Self-rated health | |
| Poor | 8 (1.0) |
| Fair | 41 (5.0) |
| Good | 252 (31.0) |
| Very good | 351 (43.1) |
| Excellent | 162 (19.9) |
| Duration of residence | |
| 1–5 year | 76 (9.3) |
| 6–10 year | 128 (15.7) |
| 11–20 year | 244 (30.0) |
| ≥ 21 year | 366 (45.0) |
| Cognitive function (possible range 0–100)a | 95.19 (4.73) |
| Neighborhood-level characteristic | |
| Perceived walkability (possible range 0–6)a | 4.17 (1.49) |
| Objective walkabilitya,b | −0.13 (7.26) |
Higher cognitive function, perceived walkability, and objective walkability scores indicate better cognitive function, greater perceived walkability, and greater objective walkability.
The range of the objective walkability score in our data was −11.3 to 23.0.
Table 2 shows the association of both perceived and objective walkability with cognitive function. Higher perceived walkability was linked to better cognitive function (p < .01), while objective walkability was not associated with cognitive function. A one-point increase in perceived walkability was associated with a 0.29 points higher cognitive function score. However, the association between perceived walkability and cognitive function was no longer statistically significant after including the potential confounders (i.e., age, education, race/ethnicity, and sex at birth).
Table 2.
Association of perceived and objective walkability with cognitive function (total relationship).
| Model 1a B (S.E.) |
Model 2a B (S.E.) |
Model 3b B (S.E.) |
Model 4b B (S.E.) |
|
|---|---|---|---|---|
| Perceived walkability | 0.290 (0.105)** |
0.143 (0.099) |
||
| Objective walkability | −0.003 (0.023) |
−0.003 (0.021) |
||
| Age: 75–84 year (ref. = age: 65–74 years) |
−1.366 (0.312)*** |
−1.325 (0.329)*** |
||
| Age: ≥ 85 year (ref. = age: 65–74 years) |
−4.026 (0.484)*** |
−4.983 (0.471)*** |
||
| Education: 12–15 years (ref. = education: < 12 years) |
3.107 (1.469)* |
1.685 (1.275) |
||
| Education: > 15 years (ref. = education: < 12 years) |
4.581 (1.447)** |
3.279 (1.260)** |
||
| Non-Hispanic White (ref. = Hispanic or non-White) |
0.948 (0.472)* |
1.346 (0.479)** |
||
| Male (ref. = female) |
−0.578 (0.297) |
−0.537 (0.310) |
S.E. = standard error, ref. = reference category.
p < 0.05,
p < 0.01,
p<0.001
Sample size for models 1 and 2 is 680.
Sample size for models 3 and 4 is 799.
Table 3 reports the relationship between walking (steps/day) and cognitive function. Walking (steps/day) was positively associated with cognitive function after adjusting for age, education, race/ethnicity, and sex at birth (model 2, p = .015). For a daily increase of 1,000 steps, the cognitive function score was higher by 0.1 points after accounting for the confounders. The significant association between walking and cognitive function persisted after separately including each potential mediator (i.e., model 3 for perceived walkability and model 4 for objective walkability).
Table 3.
Association between walking (mediator) and cognitive function (outcome) (N = 814).
| Model 1 B (S.E.) |
Model 2 B (S.E.) |
Model 3a B (S.E.) |
Model 4b B (S.E.) |
|
|---|---|---|---|---|
| Walking (steps/day) | 0.0003 (0.00005)*** |
0.0001 (0.00005)* |
0.0001 (0.00005)* |
0.0001 (0.00005)* |
| Age: 75–84 year (ref. = age: 65–74 years) |
−1.174 (0.33)*** |
−1.236 (0.316)*** |
−1.17 (0.335)*** |
|
| Age: ≥ 85 year (ref. = age: 65–74 years) |
−4.540 (0.484)*** |
−3.733 (0.498)*** |
−4.643 (0.490)*** |
|
| Education: 12–15 years (ref. = education: < 12 years) |
1.718 (1.277) |
3.195 (1.464)* |
1.692 (1.271) |
|
| Education: > 15 years (ref. = education: < 12 years) |
3.216 (1.262)* |
4.562 (1.442)** |
3.187 (1.256)* |
|
| Non-Hispanic White (ref. = Hispanic or non-White) |
1.285 (0.481)** |
0.845 (0.472) |
1.277 (0.479)** |
|
| Male (ref. = female) |
−0.635 (0.308)* |
−0.594 (0.296)* |
−0.571 (0.309) |
|
| Perceived walkability | 0.107 (0.100) |
|||
| Objective walkability | −0.005 (0.002) |
S.E. = standard error, ref. = reference category.
p < 0.05,
p < 0.01,
p<0.001
Sample size for models 3 is 680.
Sample size for models 4 is 799.
Table 4 indicates a positive relationship between perceived walkability and walking after accounting for confounders (p < .001). A one-point increase in the perceived walkability score was associated with 338.4 more daily steps after controlling for confounders. There was no significant association between objective walkability and walking.
Table 4.
Association of perceived and objective walkability (exposure) with walking (mediator).
| Model 1a B (S.E.) |
Model 2a B (S.E.) |
Model 3b B (S.E.) |
Model 4b B (S.E.) |
|
|---|---|---|---|---|
| Perceived walkability | 426.2 (86.5)*** |
338.4 (83.3)*** |
||
| Objective walkability | 11.6 (16.8) |
14.9 (15.8) |
||
| Age: 75–84 year (ref. = age: 65–74 years) |
−1210.0 (263.1)*** |
−1395.1 (249.8)*** |
||
| Age: ≥ 85 year (ref. = age: 65–74 years) |
−2738.7 (408.5)*** |
−2971.8 (357.3)*** |
||
| Education: 12–15 years (ref. = education: < 12 years) |
−817.8 (1239.8) |
−57.0 (966.5) |
||
| Education: > 15 years (ref. = education: < 12 years) |
177.5 (1221.3) |
804.2 (955.3) |
||
| Non-Hispanic White (ref. = Hispanic or non-White) |
961.1 (398.2)* |
599.0 (363.3) |
||
| Male (ref. = female) |
142.5 (250.5) |
291.7 (234.9) |
S.E. = standard error, ref. = reference category.
p < 0.05,
p < 0.01,
p<0.001
Sample size for models 1 and 2 is 680.
Sample size for models 3 and 4 is 799.
Table 5 presents the analysis result of walking as a mediator in the associations between perceived walkability and cognitive function and objective walkability and cognitive function. The estimate, indicating the size of the indirect relationship of perceived walkability on cognitive function through walking was 0.035 (p = .006). The mediating relationship accounted for 34% of the total relationship between perceived walkability and cognitive function. However, walking had no indirect relationship on the association between objective walkability and cognitive function, as it was not a mediator there.
Table 5.
Mediation relationship of walking between perceived and objective walkability and cognitive function.
| Perceived walkability (n = 680) | Objective walkability (n = 799) | |||
|---|---|---|---|---|
| Est. (95% CI) | P value | Est. (95% CI) | P value | |
| Average daily steps (count/day) | 0.035 (0.010, 0.070) | 0.006** | 0.002 (−0.001, 0.010) | 0.300 |
Est. = estimate indicating the size of mediation relationship.
p < 0.01
All models adjusted for age, education, race/ethnicity, and sex at birth.
Discussion
The current study adds evidence to suggest a relationship between walkability and cognitive function, and fills the research gap on the mediator of their association among community-dwelling older adults. Walkability was assessed using both perceived and objective measures (i.e., a questionnaire and GIS data, respectively) to account for the possible different associations with cognitive function (Ng et al., 2018).
First, we tested if greater walkability was associated with better cognitive function in older adults. We found a significant association between perceived walkability and cognitive function in the unadjusted model but not in the adjusted model. This implies that variations in perceived walkability are substantially accounted for by individual characteristics such as age. To the best of our knowledge, a perceived walkability index measured using a survey has not been examined with regard to cognitive function in older adults, but the individual features composing the perceived walkability index have been investigated regarding cognitive function. A cross-sectional study of 402 adults aged 55 years and older was conducted in Singapore (Ng et al., 2018). The authors found that cognitive function was associated with perceived land-use mix (i.e., the presence of diverse stores and facilities in a neighborhood) but not with residential density and street connectivity (Ng et al., 2018), measured by the Neighborhood Environment Walkability Scale (NEWS) (Nyunt et al., 2015). Future studies should examine perceived neighborhood features seperately and the perceived walkability as a composite index with cognitive function to understand which perceived neighborhood features and how perceived walkability are linked to cognitive function in older adults.
In the current study, objective walkability was not associated with cognitive function. Guo et al. (2019) investigated the association of neighborhood environmental characteristics, including the Walk Score walkability index (objective measure) that was created using weighted distance to nearby frequently visited amenities (Duncan et al., 2011), with cognitive function and dementia in Hong Kong residents aged 65 years or older. The authors indicated that the objective walkability index at the census tract level was not associated with cognitive function measured by the Mini-Mental State Examination (MMSE), but was associated with a lower risk of dementia among older adults (Guo et al., 2019). On the other hand, Ng et al. (2017) conducted a cross-sectional study in Singapore using a neighborhood definition of a Euclidean 500-meter buffer around the home address (Ng et al., 2018). The authors found a significant relationship between objective walkability (measured using a combined score of land-use mix, residential density, and street connectivity) and cognitive function in 402 adults aged 55 years and older. The inconsistency in findings may be due to different neighborhood definitions, environmental characteristics, study areas, and characteristics of participants such as age.To understand the effects of objective walkability on cognitive function, further studies are needed.
Second, we examined whether walking (i.e., number of daily steps) mediates the association between both perceived and objectively measured walkability, and cognitive function in older adults. Before performing a formal statistical mediation analysis, we explored associations between walkability and walking, as well as between walking and cognitive function. We found that perceived walkability was associated with walking which was, in turn, related to cognitive function accounting for perceived walkability and potential confounders. This is consistent with previous research. Perceived residential density, street connectivity, and land-use mix were associated with the physical activity of transportation in adults aged 55 years or older living in Singapore (Nyunt et al., 2015). Perceived walkability was related to walking time in Chinese adults aged 60 years or older (Yu et al., 2017). Physical activity is a well-known modifiable factor for cognitive function (Kirk-Sanchez and McGough, 2014).
Unlike with perceived walkability, we did not find a significant association between objective walkability and walking. It is possible that there was little variability in objective walkability in the study region, King County, Washington State, USA. A study conducted in Atlanta quantified objective walkability using the same formula used in this study reported larger standard deviation and broader range, 11.3 and −14.7 to 30.5, respectively (Frank et al., 2005) compared to our study, 7.26 for standard deviation and −11.3 to 23.0 for range. This might limit the ability to find an association. It is also possible that all participants resided in neighborhoods that were relatively supportive of walking. Based on this exploratory analysis, we expected to find an indirect relationship of walking on the association between perceived walkability and cognitive function, but not on the association between objective walkability and cognitive function.
By convention, mediation analysis is conceptualized such that mediation can be tested in the presence of a total effect (i.e., a significant association between exposure and outcome) (Baron, 1986). Recent methodological research recommends assessing an indirect effect regardless of the presence of a significant total effect if there are theoretical reasons to support the existence of an indirect effect (Hayes, 2009, Rucker et al., 2011). Although we could not find a significant association in adjusted models for perceived walkability and cognitive function as well as objective walkability and cognitive function, an indirect relationship was analyzed, given theoretical link between walkability and congitive function through walking (Cerin, 2019). As expected, we found that walking partially mediated the association between perceived walkability and cognitive function. To the best of our knowledge, no other studies have formally tested the indirect relationship of daily steps on the association between perceived walkability and cognitive function among older adults. The partial mediating relationship through walking may indicate presence of potential other mediators such as social engagement and cognitive activities. Future studies can consider to test multiple mediators to explain the association between walkability and cognitive function.
Our study did not detect an indirect effect of objective walkability on cognitive function through walking. Our finding is generally inconsistent with previous studies that have shown promising results of physical activity as a mediator for the association between objective walkability and cognitive function. A study examined whether self-reported leisure time and transport-related physical activity were mediators for the association between objective walkability (using a composite index of residential density, street connectivity, and land-use mix) and brain imaging outcomes (Amyloid β burden, ventricular volume, hippocampal volume, and gray matter volume) among 127 individuals with mild cognitive impairment or Alzheimer’s disease (74.9 years old on average) in Australia (Cerin et al., 2017b). The authors reported that only a small portion of the cross-sectional associations, but no longitudinal associations (18 months follow-up), were explained by self-reported physical activity (Cerin et al., 2017b). A cross-sectional study investigated the roles of physical activity and sedentary behaviors in the associations of neighborhood features in 1-km street network buffer with cognitive function among 4,141 adults (mean age of 61.1 years) in Australia (Cerin et al., 2021). Interestingly, significance and direction of mediating relationships were different depending on types of physical activity. For instance, engagement in transportation walking mediated positive association between neighborhood environment (i.e., percent of commercial land use, street connectivity) and memory, while frequency of transportation walking mediated negative association between non-commercial land use mix and memory, indicating of smaller gain on memory from frequency of transportation walking related to the neighborhood environment. The authors also did not find significant mediating relationships through walking for leisure-time, resistance training, and sitting for transport or leisure-time. In the current study, objective walkability was not associated with walking. Additionally, all steps were counted, regardless of purpose (e.g., for transport or leisure) and whether or not they were taken within the home neighborhood. The mixed types of walking and a potential mismatch between home neighborhood environmental characteristics and where walking occurred may explain the lack of finding a significant indirect effect of walking on the association between objective walkability and cognitive function (Chaix et al., 2017).
This study had several limitations. First, because this is a cross-sectional study, causal relationships cannot be drawn. There is a possibility for residual confounding and residential self-selection. The potential bias was not able to fully controlled for due to limited data availability (e.g., cross-sectional data and limited available variables such as a preference to live in high walkable areas). These factors could distort the associations between variables. There is also a possibility of reverse relationships among variables: older adults with greater cognitive capacity might be more inclined to engage in walking. Further longitudinal studies are required to establish a temporal sequence among exposure, mediator, and outcome, as well as to control for residential self-selection by examining associations among changes in those variables over time. Second, all steps taken during walking time were counted regardless of location and purpose (i.e., recreational or utilitarian). Walking that occurred outside of a neighborhood could be affected by factors other than the walkability of the home neighborhood. Third, our participants were healthy, highly educated, and predominantly White, and resided in King County, WA. The characteristics of our sample may limit generalizability. Lastly, the perceived and objective walkability measures were not validated among older adults. Adding other built environment features that are associated with older adults’ walking or cognitive function to the walkability index may improve the walkability measures. Also, internal consistency for the perceived walkability measure was lower than acceptable range. This could have affected the results drawn in this study.
Conclusions
Our study indicated that perceived walkability, but not objective walkability, can be indirectly associated with cognitive function through walking. If individuals think that streets have complete sidewalks and public transplortation is readily available, they are more likely engage in walking in that area, thereby improving cognitive function. This study contributes to acquiring a better understanding of the mechanism of the association between walkability and cognitive function in older adults. A better understanding of this mechanism may assist policy makers, researchers, and interventionists in identifying which pathway interventions should be targeted to improve cognitive function among older adults. Our finding implies that older adults who have better perceptions of their neighborhood are more likely to benefit from an intervention modifying infrastructure to increase objective walkability. Modifying neighborhood infrastructure is necessary but not sufficient to improve cognitive function in older adults. Educational or social support programs to improve perceived walkability are also needed to promote cognitive function.
Perceived walkability was associated with objectively measured walking.
Walking mediated the association of perceived walkability with cognitive function.
Walking did not mediate the association of objective walkability with cognition.
Perceived walkability may be more relevant to walking behavior in older adults.
An increase in perceived walkability may reduce risk of cognitive aging.
Acknowledgements
The first author received the Healthy Aging Research Scholarship from the de Tornyay Center for Healthy Aging at University of Washington and King County Nurses Association Scholarship and was funded by the National Institute on Aging (DP1AG069874). We thank Adult Changes in Thought study investigators and participants (UO1 AG006781; U19 AG066567) and Dr. Anne Vernez Moudon of the University of Washington Urban Form Lab for help with SmartMap data access.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Declaration of competing interest
No potential conflict of interest reported by the authors.
References
- Barnett DW, Barnett A, Nathan A, Van Cauwenberg J, Cerin E, 2017. Built environmental correlates of older adults’ total physical activity and walking: a systematic review and meta-analysis. Int J Behav Nutr Phys Act, 14, 103. 10.1186/s12966-017-0558-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baron RM, Kenny DA, 1986. The moderator-mediator variable distinction in social phychological research: conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology 51, 1173–1182. 10.1037//0022-3514.51.6.1173 [DOI] [PubMed] [Google Scholar]
- Besser LM, Mcdonald NC, Song Y, Kukull WA, Rodriguez DA, 2017. Neighborhood Environment and Cognition in Older Adults: A Systematic Review. Am J Prev Med 53, 241–251. 10.1016/j.amepre.2017.02.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bird EL, Ige JO, Pilkington P, Pinto A, Petrokofsky C, Burgress-Allen J, 2018. Built and natural environment planning principles for promoting health: an umbrella review. BMC Public Health 18 (1), 930. 10.1186/s12889-018-5870-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cerin E, 2019. Building the evidence for an ecological model of cognitive health. Health Place 60, 102206. 10.1016/j.healthplace.2019.102206 [DOI] [PubMed] [Google Scholar]
- Cerin E, Barnett A, Shaw JE, Martino E, Knibbs LD, Tham R, Wheeler AJ, Anstey KJ, 2021. From urban neighbourhood environments to cognitive health: a cross-sectional analysis of the role of physical activity and sedentary behaviours. BMC Public Health, 21, 2320. 10.1186/s12889-021-12375-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cerin E, Nathan A, Van Cauwenberg J, Barnett DW, Barnett A, 2017a. The neighbourhood physical environment and active travel in older adults: a systematic review and meta-analysis. Int J Behav Nutr Phys Act, 14, 15. 10.1186/s12966-017-0471-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cerin E, Rainey-Smith SR, Ames D, Lautenschlager NT, Macaulary SL, Fowler C, Robertson JS, Rowe CC, Maruff P, Martins RN, Masters CL, Ellis KA, 2017b. Associations of neighborhood environment with brain imaging outcomes in the Australian Imaging, Biomarkers and Lifestyle cohort. Alzheimers Dement 13, 388–398. 10.1016/j.jalz.2016.06.2364 [DOI] [PubMed] [Google Scholar]
- Chaix B, Duncan D, Vallée J, Vernez-Moudon A, Benmarhnia T, Kestens Y The “Residential” Effect Fallacy in neighborhood and health studies: Formal definition, empirical identification, and correction. Epidemiology 28 (6), 789–797. doi: 10.1097/EDE.0000000000000726 [DOI] [PubMed] [Google Scholar]
- Clarke PJ, Ailshire JA, House JS, Morenoff JD, King K, Melendez R, Langa KM, 2012. Cognitive function in the community setting: the neighbourhood as a source of ‘cognitive reserve’? Journal of Epidemiology and Community Health 66 (8), 730–736. 10.1136/jech.2010.128116 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dobra A, Buhikire K, Voss JG, 2020. Identifying mediating variables with graphical models: an application to the study of causal pathways in people living with HIV. Journal of Applied Statistics 47, 1298–1314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Duncan DT, Aldstadt J, Whalen J, Melly SJ, Gortmaker SL, 2011. Validation of walk score for estimating neighborhood walkability: an analysis of four US metropolitan areas. Int J Environ Res Public Health 8, 4160–4179. 10.3390/ijerph8114160 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Forsyth A, 2015. What is a walkable place? The walkability debate in urban design. Urban Design International 20, 274–292. 10.1057/udi.2015.22 [DOI] [Google Scholar]
- Frank L, 1994. Impacts of Mixed Used and Density on Utilization of Three Modes of Travel: Single-Occupant Vehicle, Transit, Walking. Transportation Research Record 1466, 44–52. [Google Scholar]
- Frank LD, Appleyard BS, Ulmer JM, Chapman JE, Fox EH, 2021. Comparing walkability methods: Creation of street smart walk score and efficacy of a code-based 3D walkability index. Journal of Transport & Health, 21, 101005. 10.1016/j.jth.2020.101005 [DOI] [Google Scholar]
- Frank LD, Schmid TL, Sallis JF, Chapman J, Saelens BE, 2005. Linking objectively measured physical activity with objectively measured urban form: Findings from SMARTRAQ. American Journal of Preventive Medicine 28, 117–125. 10.1016/j.amepre.2004.11.001 [DOI] [PubMed] [Google Scholar]
- Gebel K, Bauman A, Owen N, 2009. Correlates of non-concordance between perceived and objective measures of walkability. Ann Behav Med 37, 228–38. 10.1007/s12160-009-9098-3 [DOI] [PubMed] [Google Scholar]
- Guo Y, Chan CH, Chang Q, Liu T, Yip PSF, 2019. Neighborhood environment and cognitive function in older adults: A multilevel analysis in Hong Kong. Health Place 58, 102146. 10.1016/j.healthplace.2019.102146 [DOI] [PubMed] [Google Scholar]
- Hayes AF, 2009. Beyond Baron and Kenny: Statistical Mediation Analysis in the New Millennium. Communication Monographs 76, 408–420. 10.1080/03637750903310360 [DOI] [Google Scholar]
- Hergenroeder AL, Barone Gibbs B, Kotlarczyk MP, Kowalsky RJ, Perera S, Brach JS, 2018. Accuracy of Objective Physical Activity Monitors in Measuring Steps in Older Adults. Gerontol Geriatr Med 4, 2333721418781126. 10.1177/2333721418781126 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hurvitz PM, Moudon AV, 2012. Home versus nonhome neighborhood: quantifying differences in exposure to the built environment. Am J Prev Med 42, 411–7. 10.1016/j.amepre.2011.11.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kerr J, Rosenberg D, Frank L, 2012. The Role of the Built Environment in Healthy Aging:Community Design, Physical Activity, and Health among Older Adults. Journal of Planning Literature 27, 43–60. 10.1177/0885412211415283 [DOI] [Google Scholar]
- Kirk-Sanchez NJ, Mcgough EL, 2014. Physical exercise and cognitive performance in the elderly: current perspectives. Clin Interv Aging 9, 51–62. 10.2147/CIA.S39506 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koohsari MJ, Nakaya T, Mccormack GR, Shibata A, Ishii K, Yasunaga A, Oka K, 2019. Cognitive Function of Elderly Persons in Japanese Neighborhoods: The Role of Street Layout. Am J Alzheimers Dis Other Demen 34, 381–389. 10.1177/1533317519844046 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kukull WA, Higdon R, Bowen JD, Mccormick WC, Teri L, Schellenberg GD, Van Belle G, Jolley L, Larson EB, 2002. Dementia and Alzheimer disease incidence: a prospective cohort study. Arch Neurol 59, 1737–1746. 10.1001/archneur.59.11.1737 [DOI] [PubMed] [Google Scholar]
- Lawton MP, 1982. Competence, environmental press, and the adaptation of older people. In Lawton M, Windley PG, Byerts TO (Eds.). Aging and the environment: Theoretical approaches (pp. 33–59). New York: Springer. [Google Scholar]
- Lawton MP, 1989. Behavior-relevant ecological factors. In Schaie KW, Schooler C (Eds.). Social structure and aging: Psychological processes (pp.57–78). Hillsdale, NJ: Lawrence Erlbaum Associates. [Google Scholar]
- Lumley T, Diehr P, Emerson S, Chen L, 2002. The importance of the normality assumption in large public health data sets. Annu Rev Public Health, 23, 151–69. doi: 10.1146/annurev.publhealth.23.100901.140546 [DOI] [PubMed] [Google Scholar]
- Marcum ZA, Walker RL, Jones BL, Ramaprasan A, Gray SL, Dublin S, Crane PK, Larson EB, 2019. Patterns of antihypertensive and statin adherence prior to dementia: findings from the adult changes in thought study. BMC Geriatr 19, 41. 10.1186/s12877-019-1058-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mez J, Marden JR, Mukherjee S, Walter S, Gibbsons LE, Gross AL, Zahodne LB, Gilsanz P, Brewster P, Nho K, Crane PK, Larson EB, Glymour MM, 2017. Alzheimer’s disease genetic risk variants beyond APOE ε4 predict mortality. Alzheimers Dement (Amst) 8, 188–195. 10.1016/j.dadm.2017.07.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Michael Y, Beard T, Choi D, Farquhar S, Carlson N, 2006. Measuring the influence of built neighborhood environments on walking in older adults. J Aging Phys Act 14, 302–12. 10.1123/japa.14.3.302 [DOI] [PubMed] [Google Scholar]
- Michael YL, Yen IH, 2014. Aging and place--neighborhoods and health in a world growing older. J Aging Health 26, 1251–1260. 10.1177/0898264314562148 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mooney SJ, Hurvitz PM, Moudon AV, Zhou C, Dalmat R, Saelens BE, 2020. Residential neighborhood features associated with objectively measured walking near home: Revisiting walkability using the Automatic Context Measurement Tool (ACMT). Health Place 63, 102332. 10.1016/j.healthplace.2020.102332 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morris JN, Hardman AE, 1997. Walking to health. Sports Med 23, 306–332. 10.2165/00007256-199723050-00004 [DOI] [PubMed] [Google Scholar]
- Ng TP, Nyunt MSZ, Shuvo FK, Eng JY, Yap KB, Hee LM, Chan N SP, Scherer S, 2018. The Neighborhood Built Environment and Cognitive Function of Older Persons: Results from the Singapore Longitudinal Ageing Study. Gerontology 64, 149–156. 10.1159/000480080 [DOI] [PubMed] [Google Scholar]
- Notthoff N, Carstensen LL, 2014. Positive messaging promotes walking in older adults. Psychol Aging 29, 329–341. 10.1037/a0036748 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nyunt MS, Shuvo FK, Eng JY, Yap KB, Scherer S, Hee LM, Chan SP, Ng TP, 2015. Objective and subjective measures of neighborhood environment (NE): relationships with transportation physical activity among older persons. Int J Behav Nutr Phys Act 12, 108. 10.1186/s12966-015-0276-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prins RG, Pierik F, Etman A, Sterkenburg RP, Kamphuis CB, van Lenthe FJ, 2014. How many walking and cycling trips made by elderly are beyond commonly used buffer sizes: results from a GPS study. Health Place. 27, 127–33. doi: 10.1016/j.healthplace.2014.01.012 [DOI] [PubMed] [Google Scholar]
- Rosenberg D, Walker R, Greenwood-Hickman MA, Bellettiere J, Xiang Y, Richmire K, Higgins M, Wing D, Larson EB, Crane PK, Lacroix AZ, 2020. Device-assessed physical activity and sedentary behavior in a community-based cohort of older adults. BMC Public Health 20, 1256. 10.1186/s12889-020-09330-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosso AL, Harding AB, Clarke PJ, Studenski SA, Rosano C, 2021. Associations of Neighborhood Walkability and Walking Behaviors by Cognitive Trajectory in Older Adults. Gerontologist, 61, 1053–1061. doi: 10.1093/geront/gnab005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rucker DD, Preacher KJ, Tormala ZL, Petty RE, 2011. Mediation Analysis in Social Psychology: Current Practices and New Recommendations. Social and Personality Psychology Compass 5, 359–371. 10.1111/j.1751-9004.2011.00355.x [DOI] [Google Scholar]
- Sallis JF, Bowles HR, Bauman A, Ainsworth BE, Bull FC, Craig CL, Sjostrom M, De Bourdeaudhuij I, Lefevre J, Matsudo V, Matsudo S, Macfarlane DJ, Gomez LF, Inoue S, Murase N, Volbekiene V, Mclean G, Carr H, Heggebo LK, Tomten H, Bergman P, 2009. Neighborhood environments and physical activity among adults in 11 countries. Am J Prev Med 36, 484–490. 10.1016/j.amepre.2009.01.031 [DOI] [PubMed] [Google Scholar]
- Sallis JF, Kerr J, Carlson JA, Norman GJ, Saelens BE, Durant N, Ainsworth BE, 2010. Evaluating a brief self-report measure of neighborhood environments for physical activity research and surveillance: Physical Activity Neighborhood Environment Scale (PANES). J Phys Act Health 7, 533–540. 10.1123/jpah.7.4.533 [DOI] [PubMed] [Google Scholar]
- Teng EL, Hasegawa K, Homma A, Imai Y, Larson E, Graves A, Sugimoto K, Yamaguchi T, Sasaki H, Chiu D, et al. , 1994. The Cognitive Abilities Screening Instrument (CASI): a practical test for cross-cultural epidemiological studies of dementia. Int Psychogeriatr 6, 45–62. 10.1017/s1041610294001602 [DOI] [PubMed] [Google Scholar]
- Tingley D, Yamamoto T, Hirose K, Keele L, Imai K, 2014. mediation: R Package for Causal Mediation Analysis 59 (5). 1–38. 10.18637/jss.v059.i05 [DOI] [Google Scholar]
- Walk Score (n.d.). Walk Score methodology. https://www.walkscore.com/methodology.shtml. Accessed October 24, 2022
- Watts A, Ferdous F, Moore KD, Burns JM, 2015. Neighborhood Integration and Connectivity Predict Cognitive Performance and Decline. Gerontol Geriatr Med 1. 2333721415599141. 10.1177/2333721415599141 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wu YT, Prina AM, Brayne C, 2015a. The association between community environment and cognitive function: a systematic review. Soc Psychiatry Psychiatr Epidemiol 50, 351–362. 10.1007/s00127-014-0945-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wu YT, Prina AM, Jones A, Matthews FE, Braynes C, 2017. The Built Environment and Cognitive Disorders: Results From the Cognitive Function and Ageing Study II. Am J Prev Med 53, 25–32. 10.1016/j.amepre.2016.11.020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wu YT, Prina AM, Jones AP, Barnes LE, Matthews FE, Brayne C, Medical Research Council Cognitive Function and Ageing Study, 2015b. Community environment, cognitive impairment and dementia in later life: results from the Cognitive Function and Ageing Study. Age Ageing 44, 1005–1011. 10.1093/ageing/afv137 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yu R, Cheung O, Lau K, Woo J, 2017. Associations between Perceived Neighborhood Walkability and Walking Time, Wellbeing, and Loneliness in Community-Dwelling Older Chinese People in Hong Kong. Int J Environ Res Public Health 14, 1199. 10.3390/ijerph14101199 [DOI] [PMC free article] [PubMed] [Google Scholar]