

Abstract
Objective
We performed a systematic review and meta-analysis of epidemiological data of injuries in professional male football.
Method
Forty-four studies have reported the incidence of injuries in football. Two reviewers independently extracted data and assessed trial quality using the Strengthening the Reporting of Observational Studies in Epidemiology statement and Newcastle Ottawa Scale. Studies were combined in a pooled analysis using a Poisson random effects regression model.
Results
The overall incidence of injuries in professional male football players was 8.1 injuries/1000 hours of exposure. Match injury incidence (36 injuries/1000 hours of exposure) was almost 10 times higher than training injury incidence rate (3.7 injuries/1000 hours of exposure). Lower extremity injuries had the highest incidence rates (6.8 injuries/1000 hours of exposure). The most common types of injuries were muscle/tendon (4.6 injuries/1000 hours of exposure), which were frequently associated with traumatic incidents. Minor injuries (1–3 days of time loss) were the most common. The incidence rate of injuries in the top 5 European professional leagues was not different to that of the professional leagues in other countries (6.8 vs 7.6 injuries/1000 hours of exposure, respectively).
Conclusions
Professional male football players have a substantial risk of sustaining injuries, especially during matches.
INTRODUCTION
A professional football team with a 25-player squad typically suffers about 50 injuries that cause time loss from play each season, which equates to two injuries per player per season.1
Player match availability has a strong correlation (r>0.85) with team success (ie, ranking position, games won, goals scored, total points).2 3 Injuries are also a financial burden to football clubs—the average cost of a player in a professional top team being injured for 1 month is calculated to be around €500.000.4
Therefore, it is important to quantify the injury incidence in professional football.5 6 There have been a number of prospective cohort studies investigating injuries sustained by football players since the end of the 1970s,1 and the publication of a consensus statement on injury definitions and data collection procedures in 20067 has improved the consistency and quality of research within the field. In the latter two decades (1998–2018) several epidemiological studies have been published describing injury patterns over one8–11 or numerous1 12–14 seasons and during tournaments with national teams15–18 in male football players. However, despite the large number of studies reporting the incidence and severity of football-related injuries,1 8 19–21 no studies have combined and meta-analysed such epidemiological data.22 Identifying the most common and severe injuries as well as where (anatomical location) and when (matches or training sessions) they usually occur would lead coaches, physical trainers, physiotherapists and physicians to prioritise the application of specific measures to prevent or reduce the risk of sustaining such injuries.
Therefore, we conducted a systematic review and meta-analysis quantifying the incidence of injuies in professional male football. Our secondary purpose was to carry out subanalyses to determine the overall effects regarding location of injuries, type of injuries, severity of injuries, overuse and traumatic injuries, new and recurrent injuries, level of play and national leagues (clubs) and international tournaments (national teams).
METHOD
To conduct this study, guidelines for reporting meta-analysis of observational studies in epidemiology (Preferred Reporting Items for Systematic Reviews and Meta-Analyses [PRISMA] guidelines) were followed.23 The PRISMA checklist is presented in online supplementary appendix 1.
Study selection
To be included in the meta-analysis, the studies had to fulfil the following criteria: (1) Injury must be defined in terms of time loss (ie, injury that results in a player being unable to take full part in future football training or match play).7 24 (2) Participants had to be professional male football players (ie, players who belong to teams engaged in professional national football leagues).19 (3) The study had to be a full-text article published in a peer-reviewed journal before March 2018. (4) Eligible studies must report either incidence rate or prevalence among the surveyed players or provide sufficient data from which these figures could be calculated through standardised equations. Studies using injury definitions other than time loss were excluded. Literature reviews, abstracts, editorial commentaries and letters to the editor were also excluded. Finally, some authors were contacted to provide missing data or to clarify if data were duplicated in other publications. Incomplete data, or data from an already included study, were excluded.
Search strategy
Potential studies were identified by using a systematic search process. First, the following bibliographical databases were searched: PubMed, Scopus, Excerpta Medica Database (EMBASE), Allied and Complementary Medicine Database (AMED), Google Scholar and the Cochrane Library with the following search terms included in Boolean search strategies: (soccer (tiab) OR soccer (mesh) OR football (tiab) OR football (mesh)) AND (injury (tiab) OR injury (mesh) OR injuries (tiab) OR injuries (mesh)) AND (professional (tiab) OR professional (mesh) OR elite (tiab) OR elite (mesh)). The search was limited to publication dates (to 28 February 2018). Second, several specialised electronic journals were also searched, including: British Journal of Sports Medicine, American Journal of Sports Medicine, British Medical Journal, Scandinavian Journal of Medicine & Science in Sports, European Journal of Sports Sciences. Finally, the reference lists of the studies recovered were hand-searched to identify potentially eligible studies not captured by the electronic searches.
Two reviewers independently (AL-V and IRP): (1) Screened the title, abstract and reference list of each study to locate potentially relevant studies, and once hard copies of the screened documents were obtained. (2) Reviewed them in detail to identify articles that met the selection criteria. A third external reviewer (FAR) was consulted to resolve discrepancies regarding the selection process.
Data extraction
With the aim of guaranteeing the maximum possible objectivity, a codebook was produced that specified the standards followed in coding each of the characteristics of the studies. The codebook can be obtained from the corresponding author on request. The moderator variables of the eligible studies were coded and grouped into three categories: (1) General study descriptors (eg, authors, year of publication and study design). (2) Description of the study population (eg, sample size, age and level of play). (3) Epidemiological data (eg, injury and exposure data, distribution of injuries by anatomical location, type of injury, injury severity). If applicable, the authors of included studies were contacted to provide clarifications or access to raw data. Operational definitions used in the meta-analysis are shown in online supplementary appendix 2. Online supplementary appendix 3 also displays the moderator variables coded separately by category.
The purpose of the current meta-analysis was to determine the overall effects of: (1) Football-related injury incidence (overall vs training vs match injuries rates). (2) Location of injuries (lower extremity vs trunk vs upper extremity vs head and neck). (3) Type of injuries (fractures and bone stress vs joint (non-bone) and ligament vs muscle and tendon vs contusions vs laceration and skin lesion vs central/peripheral nervous system vs undefined/other). (4) Severity of injuries (slight/minimal (1–3 days) vs minor/mild (4–7 days) vs moderate (8–28 days) vs major/severe (>28 days)). (5) Mechanism of injury (overuse vs traumatic injuries). (6) New versus recurrent injuries. (7) Level of play (top-5 European professional leagues vs other professional leagues). (8) National leagues versus international tournaments (tournaments with national teams).
Quality assessment
The reporting quality of included studies was assessed using an adapted version of the ‘Strengthening the Reporting of Observational Studies in Epidemiology’ (STROBE) statement by Vom Elm et al.25 Thus, all included studies were rated on 11 specific criteria which were derived from items 5, 6, 7, 8, 9, 12, 14 and 15 of the original checklist. This 11-item checklist provides guidance on the reporting of observational studies to facilitate critical appraisal and interpretation of results.
Furthermore, to assess risk of bias of external validity quality, an adapted version of the Newcastle Ottawa Scale (NOS) for cohort studies was used. The original NOS is a quality assessment tool for cohort and case-control studies which contains eight items categorised into three domains (selection, comparability and exposure) and uses a star rating system to indicate the quality of a study (maximum of nine stars).26 The instrument was modified for the purpose of this review (the incidence of injuries) and the population of football players. Two of the eight items were deleted. Item 2 was excluded because a selection of the non-exposed cohort was irrelevant as long as the total study population was exposed to football play and item 5 (comparability of cohorts on the basis of the design or analysis) was excluded because it was linked to item 2. Two new items were added to the original scale (items 1 and 3). Therefore, the criteria adopted to assess risk of bias were: (1) Description or type of football players. (2) Definition of injury. (3) Representativeness of the exposed cohort. (4) Ascertainment of exposure. (5) Demonstration that the outcome of interest was not present at the start of study. (6) Assessment of outcome. (7) Whether follow-up was long enough for outcomes to occur. (8) Adequacy of follow-up of cohorts. An article could be awarded a maximum of one star for each item if appropriate methods had been clearly reported. Thus, a total of eight stars could be given to an article. The higher the number of stars given to an article the lower the risk of bias. Similarly, modified versions of this checklist have been used previously in systematic reviews investigating the epidemiology of injuries in other cohorts of athletes.27 28 Online supplementary appendix 4 displays a brief description of each item of the adapted version of the NOS tool used in this study.
The data extraction and quality assessment (including risk of bias of external validity) were conducted by two reviewers (AL-V and IR-P). To assess the intercoder reliability of the coding process, these two reviewers (AL-V and IR-P) coded 22 studies randomly (50%) (including quality assessment). For the quantitative moderator variables intraclass correlation coefficients (ICC3,1) were calculated, while for the qualitative moderator variables Cohen’s κ coefficients were applied. On average, the ICC was 0.89 (range: 0.78–1.0) and the κ coefficient was 0.90 (range: 0.81–1.0), which can be considered highly satisfactory, as proposed by Orwin and Vevea.29 Inconsistencies between the two coders were resolved by consensus, and when these were due to ambiguity in the coding book, this was corrected. As before, any disagreement was resolved by mutual consent in consultation with a third reviewer (FA).
Statistical analysis
Injury incidence rates per 1000 hours of player exposures were extracted from the included studies. If injury incidence rates were not specifically reported, they were, if possible, calculated from the available raw data using the following formulas:
* Match duration, using the factor 1.5, based on standard 90 min match play. For example, a hypothetical study reporting that a football team comprising 20 players sustained a total of 6 injuries within the season (38 matches), the application of the second formula would estimate an incidence of 9.6 injuries per 1000 hours of match exposure.
Data were modelled by a random effects Poisson regression model, as previously described.30 The response variable was the number of observed injuries, offset by the log of the number of exposure hours. A random effects term was included to account for the correlation arising from using multiple rows of data from the same study. Factors of interest were included as random effects. A weighting factor used was: study exposure time (hours)/mean study exposure time (hours). The possible influence of the following variables on the model was analysed independently through univariate and multivariate analyses: registration period; year of the study publication, age of the players, STROBE score, NOS stars and number of teams included in the study. Only those studies that rigorously and clearly followed the definitions of injury described by Fuller7 were included in the subanalyses.
Heterogeneity was evaluated using the I2 statistic, which represents the percentage of total variation across all studies due to between-study heterogeneity.31 All statistical analyses were performed using the statistical software package R V.2.4.1 (The R Foundation for Statistical Computing) and the ‘metafor’ package.32
For injury incidence data, the overall estimated means for each random effect factor were obtained from the model and then back-transformed to give incidence rates, along with 95% CIs.
RESULTS
Descriptive characteristics of the studies
A total of 2013 references were identified with all search strategies, from which 537 were excluded in the first screening as duplicates (26.6 %). One thousand three hundred and eleven studies (65.1 %) were eliminated after reading the title and abstract. Another 23 studies did not report injury incidence rates or were focused on specific types of injuries (eg, ankle sprains, hamstrings muscle strains) (1.1%). Ninety-eight did not comply methodologically with the established criteria such as injury definition, participants observed (amateur players or children) and data duplication (4.7 %).
The search process identified 44 articles (resulting in 56 cohort groups as seven studies had more than one group) that met the inclusion criteria.8–10 13 15–19 21 33–66 Figure 1 shows the flow chart of the selection process of the studies. The studies were carried out between 1989 and 2018 and comprised players from both tournaments (world15 16 18 43 44 54 55 and continental17 21 62 tournaments) and professional football leagues in many countries.42 46 49 52 57 66 Online supplementary appendix 5 provides a descriptive summary of the characteristics of the included studies.
Figure 1.
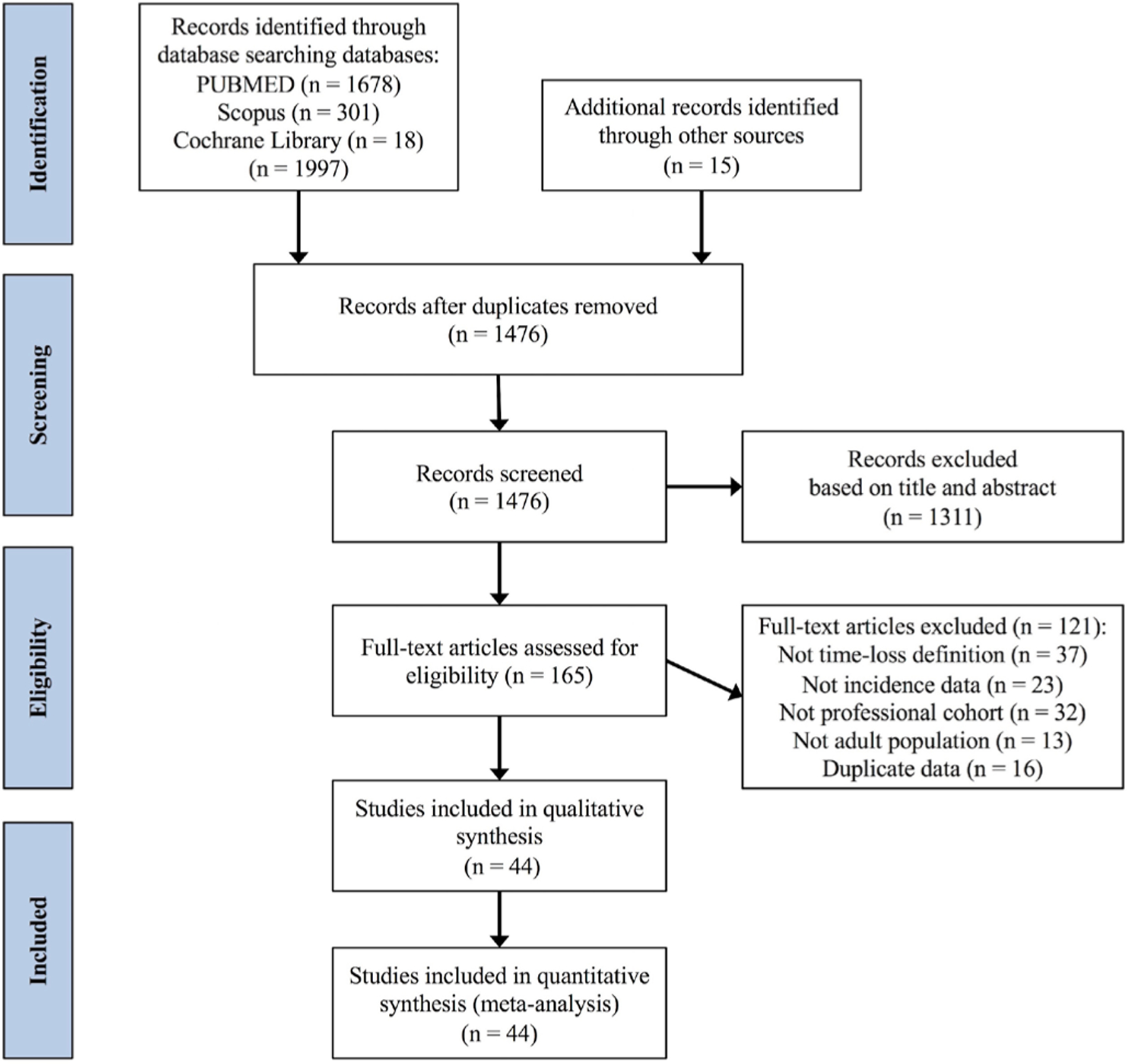
Flow chart of the selection of studies for the meta-analysis.
With regards to the reporting quality of the studies, the mean score obtained with the STROBE quality scale was 7.7 (minimum: 3, maximum: 11). In general, more recent studies (published from 2007 to 2017) had more information reported (8.5, 95% CI=7.9 to 8.8) than older (published before 2007) studies (6.3, 95% CI=6.0 to 7.0). The detailed data are presented in online supplementary appendix 6. Regarding NOS, the mean score obtained was 7.0 (minimum: 5, maximum: 8). The detailed data are presented in online supplementary appendix 7.
Findings: meta-analyses
In the different meta-analyses carried out, the effect sizes exhibited a moderate to large heterogeneity (based on the Q statistics and the I2 indices), supporting the decision of applying random-effects models.
Neither the registration period (ie, the period of time/year when the data collection process was carried out), nor the year of publication of the study, age, STROBE score, NOS stars and number of teams’ variables had an impact on injury incidence rates and hence, the subsequent subanalyses were not adjusted to these variables.
Injury incidence: overall, training and match
Thirty-four studies (43 cohorts) reported overall injury incidence,8–10 13 17 19 21 33 35–39 41 42 44–49 51–53 56–61 63–66 30 studies (39 cohorts) reported training injury incidence9 10 13 17 21 33 35–37 39 40 42 43 45–49 51 52 56–61 63–66 and 40 studies (52 cohorts) reported match injury incidence9 10 13 15–18 21 33–37 39–52 54–66 that could be combined in the meta-analysis. These studies comprised 29 991 (overall), 12 089 (training) and 14 974 (match) injuries.
The random effect models for injury incidence showed an overall incidence of 8.1 injuries per 1000 hours of exposure (95% CI 7.2 to 9.0, I2=99.1%), a training incidence of 3.7 injuries per 1000 hours of training exposure (95% CI 3.1 to 4.4, I2=98%) and a match incidence of 36.0 injuries per 1000 hours of match exposure (95% CI 31.3 to 40.8, I2=98.9%). Figures 2–4 display a summary of the reported overall, training and match injury incidence rates of the analysed studies, respectively.
Figure 2.
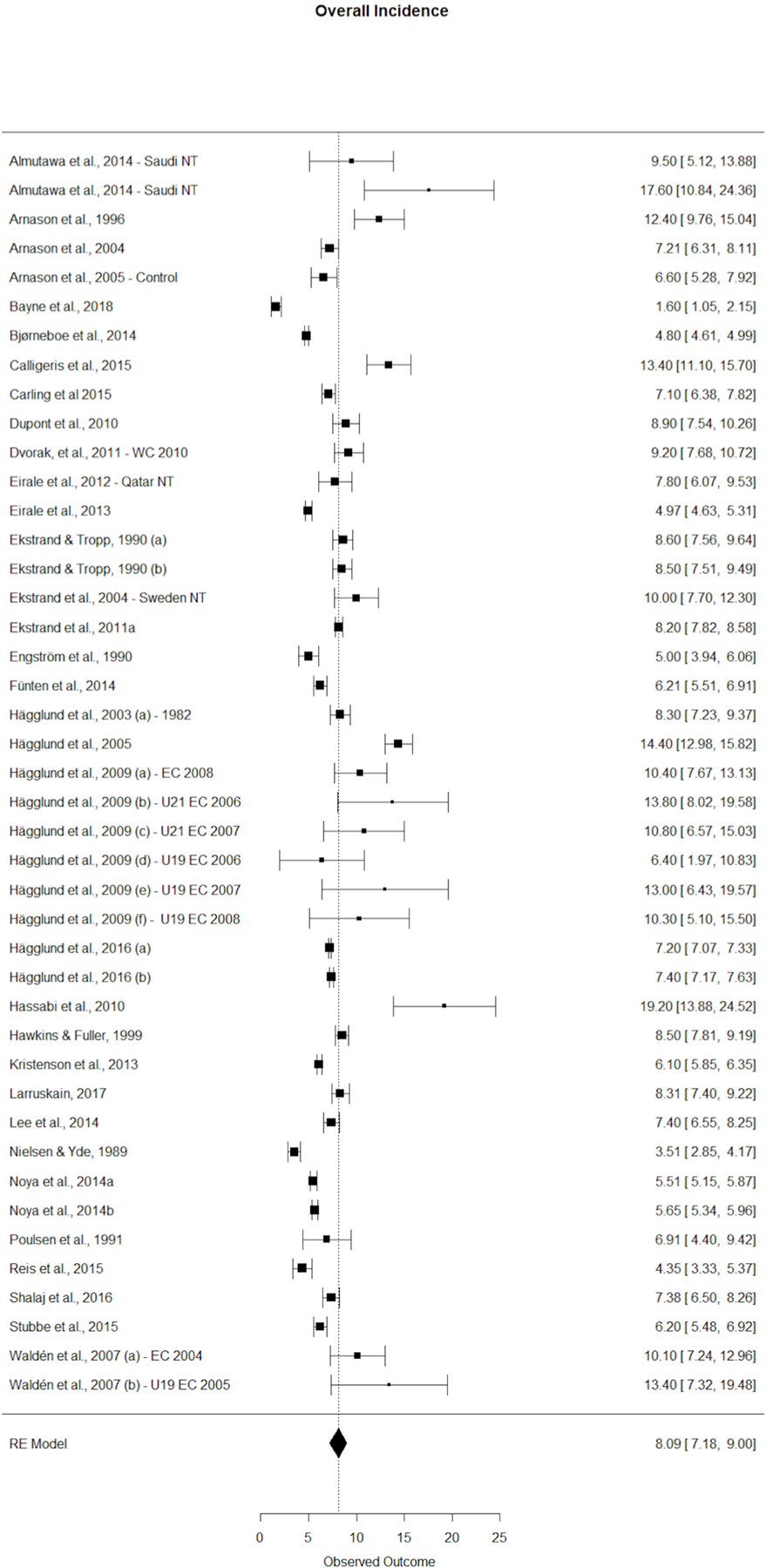
Overall injury incidence forest plot with 95% CIs. EC, Europe tournament; NT, national team; U, under; WC, world tournament.
Figure 4.
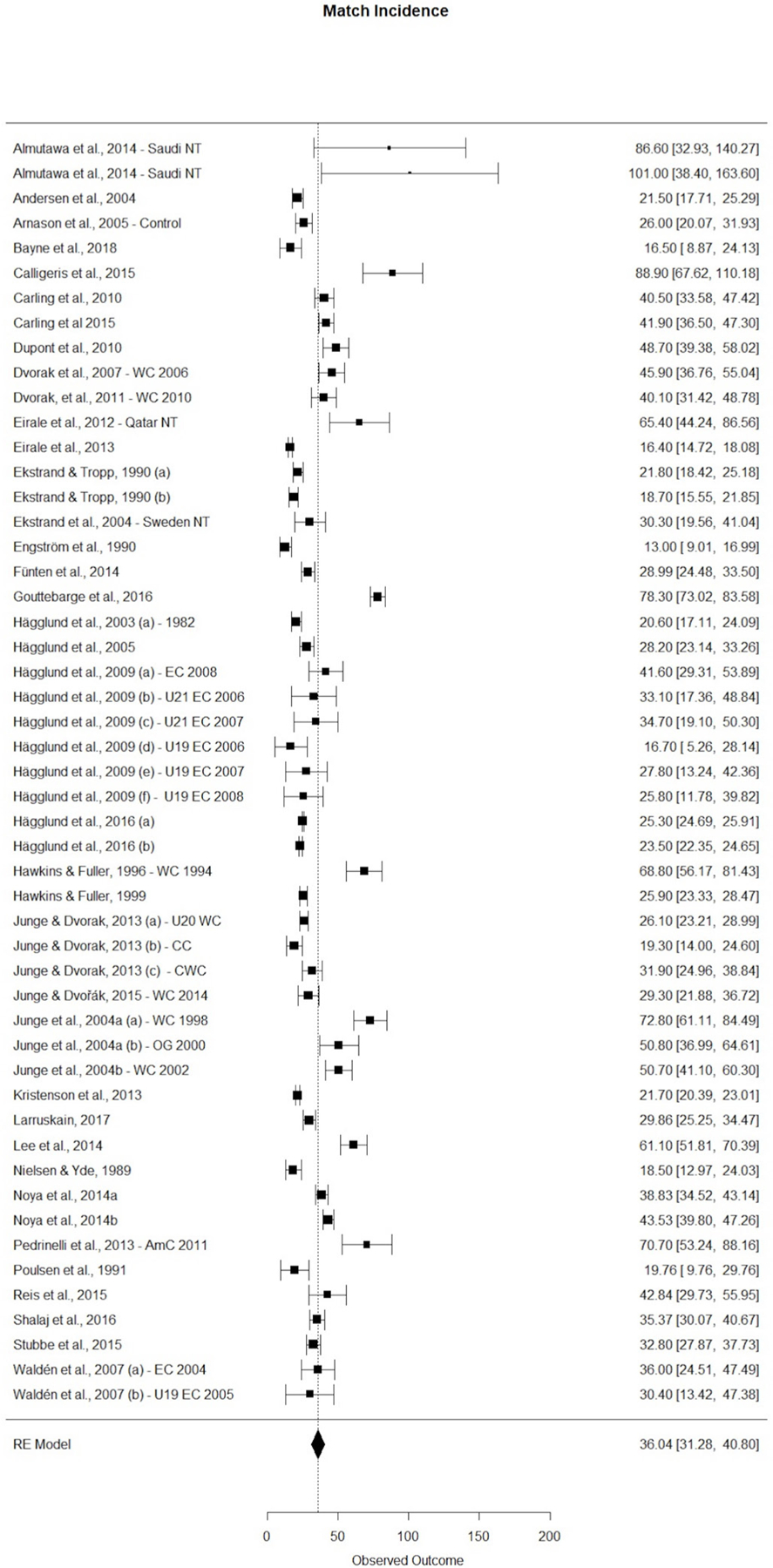
Match injury incidence forest plot with 95% CIs. AMC, American tournament; CC, confederation tournaments; CWC, clubs world tournaments; EC, Europe tournament; nt, national team; OG, Olympic games; U, under; WC, world tournament.
Location of injury
Twenty-five studies (26 cohorts) reported injury location (ie, lower extremity, trunk, upper extremity, head and neck) and lower extremities region categories (ie, thigh, hip/groin, knee, lower leg/Achilles tendon, ankle and foot/toe) according to Fuller et al7 which were pooled in the meta-analysis.1 8 13 17 19 35–38 40 42 43 45 46 48 49 51 53 57 58 60 61 63 65 66 Lower extremity injuries had the highest incidence rates (6.8 per 1000 hours of exposure, 95% CI 5.7 to 7.8, I2=98.86) compared with the other body regions. The trunk was the second most commonly injured region (0.4 per 1000 hours of exposure, 95% CI 0.3 to 0.5, I2=97.67), the upper extremity was the third most commonly injured region (0.3 per 1000 hours of exposure, 95% CI 0.2 to 0.4, I2=98.32) and head and neck injuries had the lowest incidence rates (0.2 per 1000 hours of exposure, 95% CI 0.1 to 0.2, I2=96.3).
Regarding lower extremity injuries, six anatomical regions were analysed. The mean incidence per 1000 player hours of exposure with 95% CIs were in descending order: thigh (1.8, 95% CI 1.5 to 2.2, I2=91.78); knee (1.2, 95% CI 1.0 to 1.4, I2=91.86); ankle (1.1, 95% CI 0.9 to 1.2, I2=92.58); hip/groin (0.9, 95% CI 0.7 to 1.0, I2=95.32); lower leg/Achilles tendon (0.8, 95% CI 0.6 to 1.0, I2=93.01) and foot/toe (0.4, 95% CI 0.3 to 0.5, I2=91.4) (figure 5).
Figure 5.
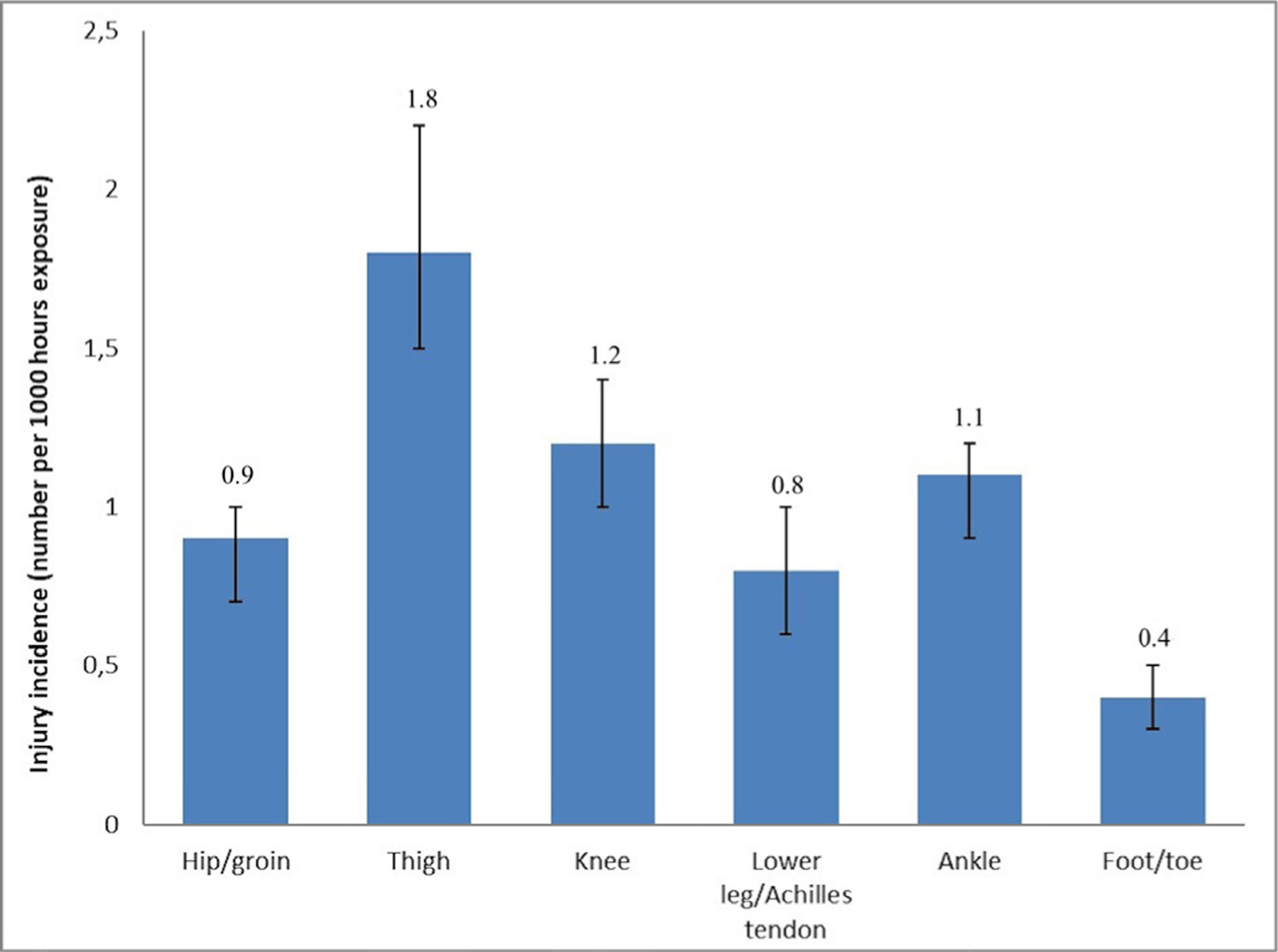
Injury incidence rates (with 95% CIs) by location of lower extremity injuries.
Type of injury
Twenty-four studies (26 cohorts) were included in the pooled analysis.1 8 13 17 19 35 37–39 43 45 46 48 49 51 53 57 58 60 61 63–66 The mean incidence is presented per 1000 hours of exposure with 95% CIs. The most common type of injury grouping was muscle/tendon (4.6, 95% CI 3.8 to 5.4, I2=98.71), followed by contusions (1.4, 95% CI 1.1 to 1.8, I2=97.65), undefined/other injuries (0.6, 95% CI 0.3 to 0.9, I2=97.92), joint (non-bone) and ligament (0.4, 95% CI 0.2 to 0.6, I2=98.02), fracture and bone stress (0.2, 95% CI 0.1 to 0.3, I2=98.16), laceration and skin lesions (0.05, 95% CI 0.02 to 0.08, I2=98.52) and the least common injury type grouping was central/peripheral nervous system injuries (0.04, 95% CI 0.02 to 0.06; I2=98.19) (figure 6).
Figure 6.
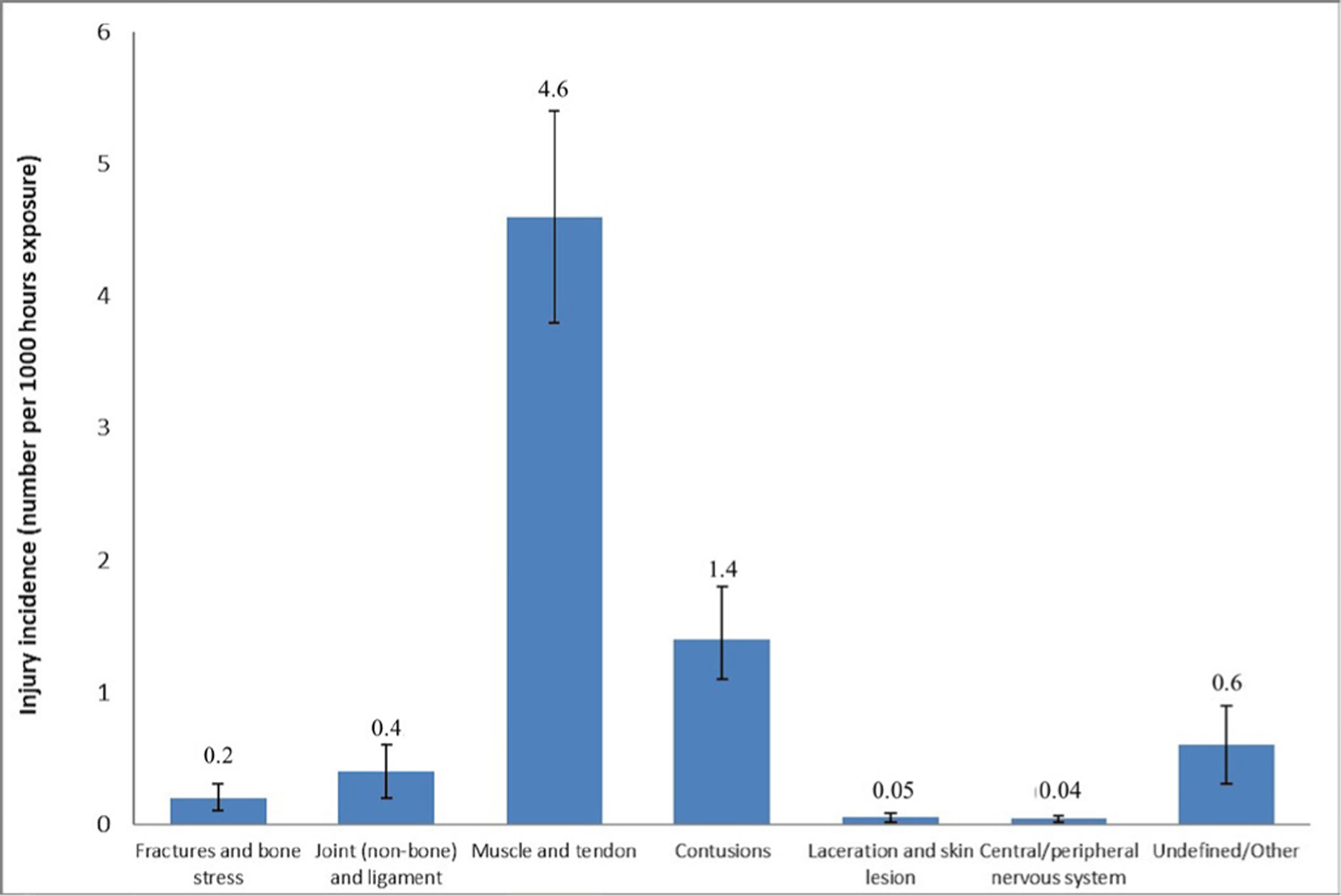
Injury incidence (with 95% CIs) by type of injury.
Severity of injury
Concerning severity of injuries, 21 studies (28 cohorts) were included in the pooled analysis.1 10 13 17 21 33 37 40 42 43 45 46 49 51 57 58 60 61 64–66 Minimal injuries (3.1 per 1000 hours of exposure, 95% CI 2.4 to 3.9, I2=98.75) were the most usual injuries, followed by moderate (2.0 per 1000 hours of exposure, 95% CI 1.7 to 2.4, I2=92.58), minor (1.7 per 1000 hours of exposure, 95% CI 1.4 to 2.1, I2=94.73) and severe (0.8 per 1000 hours of exposure, 95% CI 0.6 to 1.0, I2=91.63) injuries (online supplementary appendix 8).
Mechanism of injury
Twenty studies (26 cohorts) were involved in the meta-analysis to compare overuse injuries versus traumatic injuries.8 9 17 19 21 35 38 39 42 45 46 49 51 57 58 60 61 64–66 The incidence in traumatic injuries (5.9, 95% CI 4.7 to 7.1, I2=99.32) was higher than in overuse injuries (2.4, 95% CI 1.9 to 3.0, I2=98.31).
New versus recurrent injuries
Fifteen studies (21 cohorts) were included in an analysis which compared the incidence of new versus recurrent injuries.13 21 35 39 42 43 45 46 51 52 57 58 61 64 66 The incidence rate of new injuries (7.0 per 1000 hours of exposure, 95% CI 6.0 to 8.1, I2=98.84) was higher than recurrent injuries incidence rate (1.3 per 1000 hours of exposure, 95% CI 0.8 to 1.8, I2=98.53).
Level of play
For level of play, 32 studies were divided into two groups: (1) Top-5 European professional leagues as ranked by Union of European Football Associations (UEFA) in 2018 (https://www.uefa.com/memberassociations/uefarankings/index.html) (La Liga (Spain), Premier League (England), Serie A (Italy), Bundesliga (Germany) and Ligue1 (France)). (2) Other professional leagues in the world (outside the top-5 European professional leagues). Seven studies were performed in clubs belonging to the top-5 European professional leagues and reported overall13 40 41 49 57 60 61 training13 40 49 57 60 61 and match13 40 41 49 57 60 61 incidence rates, respectively. Alternatively, 25 studies were conducted in the professional leagues outside of the top-5 European professional leagues, and also reported overall,8 10 19 35–39 46–48 51–53 56 58 59 63–66 training10 35–37 39 46–48 51 52 56 58 59 63–66and match10 34–37 39 46–48 50–52 56 58 59 63–66 incidence rates. The overall incidence rate in professional leagues was not significantly different than in the top-5 European leagues (7.6, 95% CI 6.2 to 9.0 vs 6.8, 95% CI 5.8 to 7.9, respectively). The mean incidence rates in training and match were in descending order: top-5 European leagues match: 35.5 (30.0 to 40.9, I2=90.23), other professional leagues match: 31.9 (23.2 to 40.6, I2=97.23), other professional leagues training: 3.9 (2.9 to 5.0, I2=98.01) and top-5 European professional leagues training: 3.6 (3.2 to 4.0, I2=91.23).
National leagues versus international tournaments
For this comparison, 44 studies were divided into two groups: (1) National leagues—studies in football clubs of professional leagues. (2) International tournaments—studies in national teams during international tournaments. Twenty-eight, 24 and 27 studies carried out in football clubs reported overall,8 10 13 19 35–40 42 46–49 51–53 56–61 63–66 training,10 13 35–37 39 40 42 46–49 51 52 56–61 63–66 and match10 13 34–37 39–42 46–52 56–61 63–66 incidence rates. On the other hand, 6, 6 and 13 studies in national teams reported overall,9 17 21 33 43 45 training9 17 21 33 43 45 and match9 15–18 21 33 43–45 55 62 incidence rates. Incidence rates in international tournaments were higher than in national leagues (9.8, 95% CI 8.8 to 10.8 vs 7.5, 95% CI 6.5 to 8.4, for international tournaments and national leagues). In particular, the mean incidence rates in training and match were in descending order: international match: 41.1 (33.9 to 48.2, I2=90.69); national match: 32.3 (26.7 to 37.9, I2=96.43); national training: 3.8 (3.2 to 4.5, I2=98.37); and international training: 3.5 (2.2 to 4.7, I2=91.71).
DISCUSSION
The purposes of this study were to perform a systematic review and meta-analysis quantifying the incidence of injuries in professional male football as well as to conduct subanalyses to determine the overall effects regarding location of injuries, type of injuries, severity of injuries, overuse and traumatic injuries, new and recurrent injuries, level of play and national leagues (clubs) and international tournaments (national teams).
Injury incidence: overall, training and match
This meta-analysis indicates that the incidence rate per 1000 hours of exposure for professional male football players (8.1 injuries per 1000 hours of exposure) is lower than the injury incidence rate provided for professional male rugby players (12.6 injuries per 1000 hours of exposure).67 The incidence rates in the current meta-analysis are similar to injury incidence rates provided in individual studies for amateur football players (5.1–10.9 injuries per 1000 hours of exposure),68–70 college ice hockey players (9.1 injuries per 1000 hours of exposure)71 and senior handball players (6.3 injuries per 1000 hours of exposure).72 Fortunately, although injuries occur frequently in professional football players, the majority appear to be of minimal severity (1–3 days lost from sport play).
In line with most team sports (eg, basketball,73 handball,72 rugby)67 match/game injury incidence in football was notably higher (almost 10 times) than the injury rate obtained for training sessions. A number of studies have attributed these differences in injury incidence rates between match and training to several factors, including the higher physical demands on players during matches in comparison with training sessions, the number of contacts and collisions during matches, and fatigue generated during the course of the match.1 74 75 Furthermore, the variability and uncertainly generated in the players when competing against rivals in a match compared with teammates in training may potentiate these differences. Although still under debate, it has been suggested that training session design (ie, workload, intensity, duration), when possible, should mimic match demands so that players are better prepared for what they face during matches.76 Although the limited number of studies published did not permit us to describe the pattern of injury incidence during the course of a football match, the current evidence shows that the incidence rates of some injuries tend to increase towards the end of each half.1 14 16 44 74 77 The finding of a higher incidence of injuries in the second part of each half in comparison with other match periods may indicate that fatigue is implicated in injury aetiology, however, factors contributing to this (eg, hydration, nutrition, neuromuscular compromise and biomechanical alterations to technique) require further investigation.
Location of injury
As expected, lower extremity injuries were by far the most frequent location for an injury with an incidence rate of 6.8 injuries per 1000 hours of exposure. The thigh was the most commonly injured anatomical region followed by the knee. Furthermore, the most common type of injury grouping was muscle/tendon injuries. Due to the lack of studies reporting incidence rates separately for different muscle groups (eg, gluteus, hamstrings, quadriceps, abductors, adductors, triceps surae), a subanalysis aimed at identifying the most injured muscle group was not possible. However, previous epidemiological studies have consistently reported that hamstring muscles are the muscle group most frequently injured in professional football players.66 74 78 As previous studies exploring the location and type of football-related injuries have only reported incidence rates and not the average number of days lost from football (time loss), it was not possible for us to calculate the injury burden (the cross-product of severity (consequences) and incidence (likelihood)) to build a risk matrix. The risk matrix would have helped to identify the importance of each type of football-related injury and may provide information to help prioritise injury prevention measures used in professional football environments. Recently, Bahr et al79 built a risk matrix based on data from the UEFA Elite Club Injury Study and suggested that injury reduction in the areas of the hamstring, groin, knee and ankle are priorities for coaching, medical and fitness staff, while concussions represent less of a health burden. According to Ekstrand et al,80 the measures designed to reduce the injury burden should address the traditionally proposed modifiable injury risk factors (eg, eccentric strength deficits,81–83 poor flexibility,84 85 altered muscle architecture,86 87 player load and match frequency)8 88 and some new external factors such as the stability of the club in terms of coaching, medical staff and management, players adherence and coach compliance to the injury prevention programme.89
Overuse versus traumatic injuries
In this study most of the football-related injuries had a traumatic mechanism, with an incidence rate of 5.9 injuries per 1000 hours of exposure, twice that of the incidence reported in overuse injuries (2.4 injuries per 1000 hours of exposure). In particular, being tackled or colliding with an opponent (ie, during a jump) appear to be the most common injury incidents, representing approximately 50% of all traumatic injuries, followed closely by the injury incidents caused during non-contact actions such as sprinting and cutting (30% of all cases of traumatic injuries).90 As it has been documented for young players,91 92 the application of football-specific neuromuscular training programmes with the aim of optimising players’ motor competency, joint stability and delaying the onset of fatigue might reduce the relative risk of injury due to acute overload of soft tissues.
New versus recurrent injuries
As expected, recurrent injuries incidence is lower than the new injuries rate (1.3 vs 7.0 injuries per 1000 hours of exposure). However, the recurrent rate identified in the present study may be considered high. It has been recently shown that most recurrent injuries (mainly lower extremity muscle and tendon injuries) occur within 2 months after return to play.52 This may reflect a premature return to train/play and incomplete or inadequate rehabilitation. The lack of evidence-based criteria for a safe return to train/play alongside the fact that team managers and coaches may be tempted to let injured players return to play important matches or to let them play with ongoing minor symptoms might be two reasons behind the high recurrent injuries incidence rates. Future studies should extend our current knowledge in relation to improving the decision-making process for a safe return to training/play by developing learning algorithms or artificial intelligence-based models that allow the identification of when a player is fully and effectively rehabilitated before returning to training/play.93
Level of play
The results of this study also highlight that the incidence rates overall, during training and match play were similar between top-5 level European leagues and the rest of the professional leagues. These findings suggest that although there may be differences in the number and density (ie, match congestion) of matches played across the season between teams engaged in top-5 level European leagues and teams from other professional leagues, that this does not lead to a greater injury incidence rate. These findings were unexpected because a number of teams engaged in top-5 level European leagues must face a higher recurrence of exposure to periods of short (i.e. ≤3 days elapsed between consecutive match exposures) and long-term match congestion (i.e. >7.5 hours of match play exposure within 30 days) across the season (due to organisational reasons of their national leagues and their simultaneous participation in other national (eg, FA Cup and Football League Cup in England) and European (ie, UEFA Europa League and UEFA Champion League) tournaments) in comparison with their counterparts from other (eg, Scandinavian leagues), but not all, professional leagues94 and hence, a priori we predicted a higher incidence of injuries. However, a recently published 14 years prospective study, with 2672 male professional football players included and more than 130 000 match observations, found no associations between total match injury rates and high short-term and long-term match congestion periods95 which is in line with the results in the current meta-analysis. A possible explanation for these similar match incidence rates between top-5 level European leagues and the rest of the professional leagues could be linked to player rotation policies carried out in top-level teams (eg, sporadic exposure over the season, players only competing in one out of two matches in cycles played in a short time frame,<75 min exposure time) that might have diluted the real risk of injury.96
National leagues versus international tournaments
Finally, the present meta-analysis has also shown that the incidence rate during international matches (41.1 injuries per 1000 hours of exposure) was higher than during national matches (32.3 injuries per 1000 hours of exposure). The higher density of matches played, the mental stress and anxiety generated in the players, and the fact that international competitions are usually played during summer periods (at the end of a long season where accumulated fatigue may play a part and during hot and dry climate conditions) have been suggested as contributing factors for this increase in the number of injuries.94 97
LIMITATIONS
Like other meta-analyses conducted in sports medicine settings,67 98 variations in injury and severity definitions associated with older studies resulted in heterogeneous estimates of the main meta-analysis. Only those studies that rigorously and clearly followed the definitions of injury described by Fuller7 were included in the subanalyses. Also when different epidemiological data were used (eg, hours of athlete exposure, total number of injuries, number of matches played) and therefore various methods of data collection, we applied standardised formulas to account for this discrepancy. Nevertheless, even when our inclusion criteria for subanalysis and standardised formulas were applied, the degree of inconsistency of the results across studies was still very high (I1 >90%). Consequently, variations in injury definitions and lack of uniform data collection methods may not have been the unique sources of inconsistency in the results. Other potential sources of inconsistency may have been the differences existing among the national leagues in terms of climatic regions (cooler and warmer areas),37 periods of fixed match congestion,41 42 numbers of matches and in-season breaks49 as well as the level of professionalism.52 Additionally, the sample size of studies included was not sufficient to investigate interactive effects within factors (eg, playing position by level of play) or whether injury rates are associated with a violation of the competition rules (a variable that has not been thoroughly explored). This could, for example, help to assess whether the protective equipment used by players (shin pads) reduces injury risk or if other equipment is needed for certain positions (eg, a helmet for the goalkeeper to protect themselves against concussions). Furthermore, the lack of studies that reported the average number of days lost from football, caused by specific types of injuries, did not allow us to present data on injury burden. Another limitation that should be mentioned is that this study was not eligible for inclusion in the International Prospective Register of Systematic Reviews database because the systematic review had progressed beyond the point of completing data extraction when the official registration process was addressed. Consequently, it was not possible to make a comparison between the predictive outcomes and those finally published in order to analyse any discrepancy. In our analysis separate incidence rates reported in studies that covered multiple seasons or cups were considered as independent when multiple comparisons were conducted. In this instance the same player may have been counted more than once over the different seasons. However, for each separate incidence rate recorded, the same player was counted only one time. Unfortunately only one author corresponded when asked for additional information subsequently limiting the data we had access to.
CONCLUSIONS
Professional male football players are exposed to a substantial risk of sustaining injuries, especially during matches. Although most injuries had a traumatic mechanism (injuries with sudden onset and known cause), fortunately most of them appear to be of minimal severity. As might be expected, the lower extremity is more frequently injured, and the most common type of injury is muscle/tendon strain. Recurrent injuries were less frequent than new injuries, although re-injury rates have implications for return to train/play management. Future studies should focus on introducing and evaluating preventative measures that target the most common diagnoses, namely, muscle/tendon injuries highlighted in this meta-analysis, in order to reduce the number and severity of injuries within male professional football players.
Supplementary Material
Figure 3.
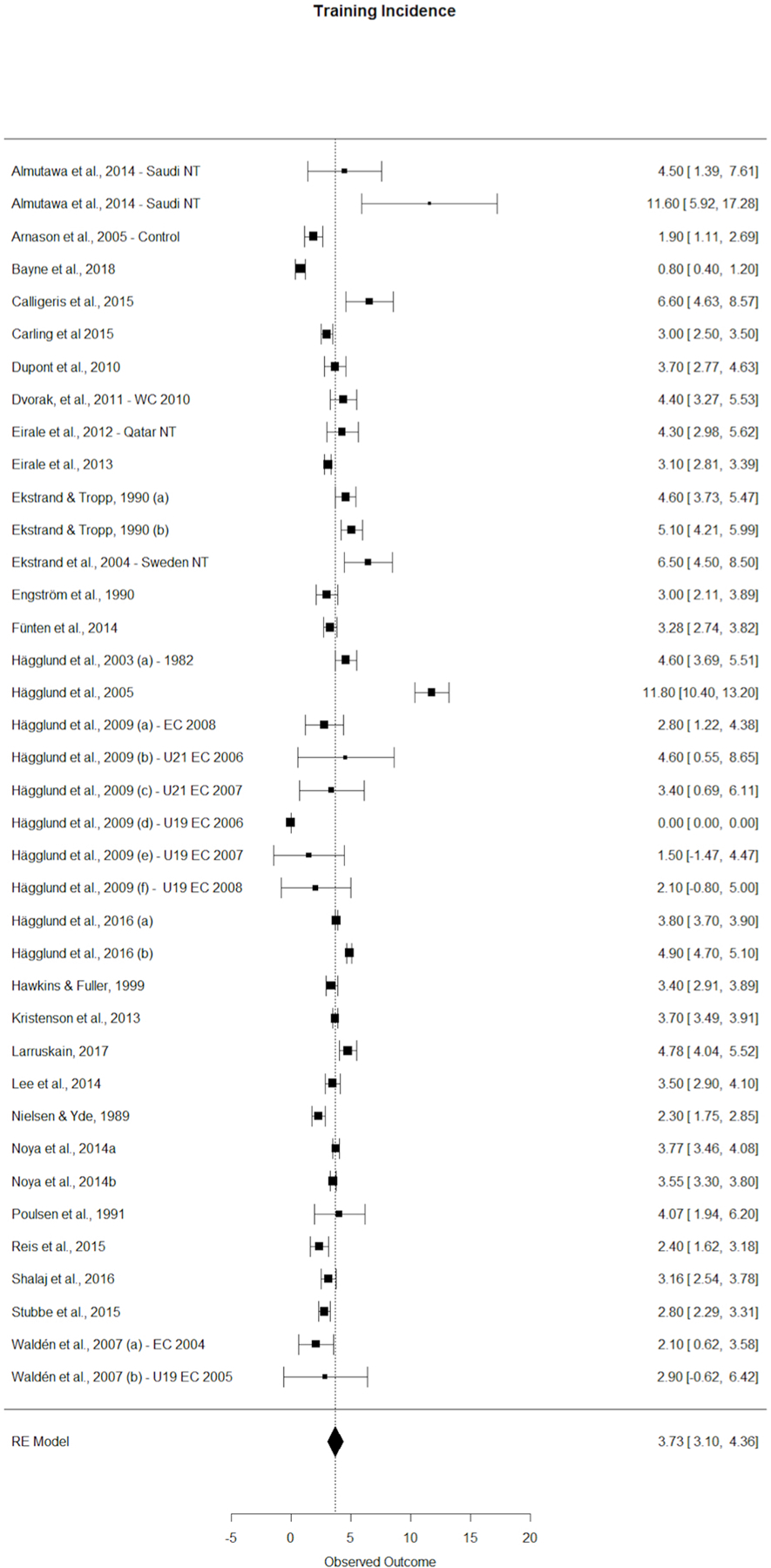
Training injury incidence forest plot with 95% CIs. EC, Europe tournament; NT, national team; U, under; WC, world tournament.
What is already known?
Injuries are one of the biggest problems in modern football.
Some types of injuries have increased in the past few decades.
Professional male football players are exposed to a substantial risk of sustaining injuries, especially during matches.
What are the new findings?
Match injury incidence is almost 10 times higher than the training injury incidence rate.
Although most injuries have a traumatic mechanism, most appear to be of minimal severity.
It is confirmed that the lower extremity is more frequently injured, and the most common types of injuries are muscle/tendon strains.
Injury incidence rates between the top-5 level European leagues and the rest of the professional leagues overall, in training and match play are similar.
Funding
AL-V was supported by a predoctoral grant given by Ministerio de Educación, Cultura y Deporte (FPU) from Spain. FAR was supported by a postdoctoral grant given by Seneca Foundation (postdoctoral fellowships funded by the regional sub program focuses on the postdoctoral development, 20366/PD/17) from Spain.
Footnotes
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
REFERENCES
- 1.Ekstrand J, Hägglund M, Waldén M. Injury incidence and injury patterns in professional football: the UEFA injury study. Br J Sports Med 2011;45:553–8. [DOI] [PubMed] [Google Scholar]
- 2.Hägglund M, Waldén M, Magnusson H, et al. Injuries affect team performance negatively in professional football: an 11-year follow-up of the UEFA champions League injury study. Br J Sports Med 2013;47:738–42. [DOI] [PubMed] [Google Scholar]
- 3.Eirale C, Tol JL, Farooq A, et al. Low injury rate strongly correlates with team success in Qatari professional football. Br J Sports Med 2013;47:807–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ekstrand J Keeping your top players on the pitch: the key to football medicine at a professional level. Br J Sports Med 2013;47:723–4. [Google Scholar]
- 5.Finch C A new framework for research leading to sports injury prevention. Journal of Science and Medicine in Sport 2006;9:3–9. [DOI] [PubMed] [Google Scholar]
- 6.van Mechelen W, Hlobil H, Kemper HCG. Incidence, severity, aetiology and prevention of sports injuries. Sports Medicine 1992;14:82–99. [DOI] [PubMed] [Google Scholar]
- 7.Fuller CW, Ekstrand J, Junge A, et al. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Scand J Med Sci Sports 2006;16:83–92. [DOI] [PubMed] [Google Scholar]
- 8.Arnason A, Sigurdsson SB, Gudmundsson A, et al. Risk factors for injuries in football. Am J Sports Med 2004;32(1_suppl):5–16. [DOI] [PubMed] [Google Scholar]
- 9.Ekstrand J, Waldén M, Hägglund M. Risk for injury when playing in a National football team. Scand J Med Sci Sports 2004;14:34–8. [DOI] [PubMed] [Google Scholar]
- 10.Hägglund M, Waldén M, Ekstrand J. Exposure and injury risk in Swedish elite football: a comparison between seasons 1982 and 2001. Scand J Med Sci Sports 2003;13:364–70. [DOI] [PubMed] [Google Scholar]
- 11.Waldén M, Hägglund M, Ekstrand J. UEFA champions League study: a prospective study of injuries in professional football during the 2001–2002 season. British Journal of Sports Medicine 2005;39:542–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hägglund M, Waldén M, Ekstrand J. Previous injury as a risk factor for injury in elite football: a prospective study over two consecutive seasons. British Journal of Sports Medicine 2006;40:767–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hawkins RD, Fuller CW. A prospective epidemiological study of injuries in four English professional football clubs. British Journal of Sports Medicine 1999;33:196–203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hawkins RD et al. The association football medical research programme: an audit of injuries in professional football. Br J Sports Med 2001;35:43–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Junge A, Dvorak J, Graf-Baumann T. Football injuries during the World Cup 2002. Am J Sports Med 2004;32(1_suppl):23–7. [DOI] [PubMed] [Google Scholar]
- 16.Junge A, Dvorak J, Graf-Baumann T, et al. Football injuries during FIFA Tournaments and the Olympic games, 1998–2001. Am J Sports Med 2004;32(1_suppl):80–9. [DOI] [PubMed] [Google Scholar]
- 17.Waldén M, Hägglund M, Ekstrand J. Football injuries during European championships 2004–2005. Knee Surg Sports Traumatol Arthrosc 2007;15:1155–62. [DOI] [PubMed] [Google Scholar]
- 18.Junge A, Dvořák J. Football injuries during the 2014 FIFA World Cup. Br J Sports Med 2015;49:599–602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ekstrand J, Hägglund M, Fuller CW. Comparison of injuries sustained on artificial turf and grass by male and female elite football players. Scand J Med Sci Sports 2011;21:824–32. [DOI] [PubMed] [Google Scholar]
- 20.Hägglund M, Waldén M, Ekstrand J. Injuries among male and female elite football players. Scand J Med Sci Sports 2009;19:819–27. [DOI] [PubMed] [Google Scholar]
- 21.Hägglund M, Waldén M, Ekstrand J. UEFA injury study--an injury audit of European Championships 2006 to 2008. British Journal of Sports Medicine 2009;43:483–9. [DOI] [PubMed] [Google Scholar]
- 22.Burke LM, Peeling P. Methodologies for investigating performance changes with supplement use. Int J Sport Nutr Exerc Metab 2018;20:1–11. [DOI] [PubMed] [Google Scholar]
- 23.Hutton B, Catalá-López F, Moher D. The PRISMA statement extension for systematic reviews incorporating network meta-analysis: PRISMA-NMA. Medicina Clínica 2016;147:262–6. [DOI] [PubMed] [Google Scholar]
- 24.Hägglund M et al. Methods for epidemiological study of injuries to professional football players: developing the UEFA model. Br J Sports Med 2005;39:340–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.von Elm E, Altman DG, Egger M, et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. International Journal of Surgery 2014;12:1495–9. [DOI] [PubMed] [Google Scholar]
- 26.Wells G, Shea B, O’Connell D, et al. The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in metaanalyses Canada: Department of Epidemiology and Community Medicine, University of Ottawa, Canada. University of Ottawa, 2013. [Google Scholar]
- 27.Saragiotto BT, Yamato TP, Hespanhol Junior LC, et al. What are the main risk factors for running-related injuries? Sports Med 2014;44:1153–63. [DOI] [PubMed] [Google Scholar]
- 28.Videbæk S, Bueno AM, Nielsen RO, et al. Incidence of Running-Related Injuries Per 1000 h of running in Different Types of Runners: A Systematic Review and Meta-Analysis. Sports Med 2015;45:1017–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Orwin RG, Vevea JL. Evaluating coding decisions. The handbook of research synthesis and meta-analysis 2009;2:177–203. [Google Scholar]
- 30.Bagos PG, Nikolopoulos GK. Mixed-effects poisson regression models for meta-analysis of follow-up studies with constant or varying durations. Int J Biostat 2009;5.20104258 [Google Scholar]
- 31.Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta-analysis. Statist. Med 2002;21:1539–58. [DOI] [PubMed] [Google Scholar]
- 32.Viechtbauer W Conducting Meta-Analyses in R with the metafor Package. J Stat Softw 2010;36:1–48. [Google Scholar]
- 33.Almutawa M, Scott M, George KP, et al. The incidence and nature of injuries sustained on grass and 3rd generation artificial turf: A pilot study in elite Saudi National Team footballers. Physical Therapy in Sport 2014;15:47–52. [DOI] [PubMed] [Google Scholar]
- 34.Andersen TE et al. Video analysis of injuries and incidents in Norwegian professional football. British Journal of Sports Medicine 2004;38:626–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Árnason Á, Gudmundsson Á, Dahl HA, et al. Soccer injuries in Iceland. Scand J Med Sci Sports 1996;6:40–5. [DOI] [PubMed] [Google Scholar]
- 36.Arnason A, Engebretsen L, Bahr R. No effect of a video-based awareness program on the rate of soccer injuries. Am J Sports Med 2005;33:77–84. [DOI] [PubMed] [Google Scholar]
- 37.Bayne H, Schwellnus M, van Rensburg DJ, et al. Incidence of injury and illness in South African professional male soccer players: a prospective cohort study. J Sports Med Phys Fitness 2018;58. [DOI] [PubMed] [Google Scholar]
- 38.Bjørneboe J, Bahr R, Andersen TE. Gradual increase in the risk of match injury in Norwegian male professional football: a 6-year prospective study. Scand J Med Sci Sports 2014;24:189–96. [DOI] [PubMed] [Google Scholar]
- 39.Calligeris T, Burgess T, Lambert M. The incidence of injuries and exposure time of professional football Club players in the premier soccer League during football season. S Afr J SM 2015;27:16–19. [Google Scholar]
- 40.Carling C, McCall A, Le Gall F, et al. The impact of in-season national team soccer play on injury and player availability in a professional Club. Journal of Sports Sciences 2015;33:1751–7. [DOI] [PubMed] [Google Scholar]
- 41.Carling C, Orhant E, LeGall F. Match injuries in professional soccer: inter-seasonal variation and effects of competition type, match congestion and positional role. Int J Sports Med 2010;31:271–6. [DOI] [PubMed] [Google Scholar]
- 42.Dupont G, Nedelec M, McCall A, et al. Effect of 2 soccer matches in a week on physical performance and injury rate. Am J Sports Med 2010;38:1752–8. [DOI] [PubMed] [Google Scholar]
- 43.Dvorak J, Junge A, Derman W, et al. Injuries and illnesses of football players during the 2010 FIFA World Cup. British Journal of Sports Medicine 2011;45:626–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Dvorak J, Junge A, Grimm K, et al. Medical report from the 2006 FIFA World Cup Germany. British Journal of Sports Medicine 2007;41:578–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Eirale C, Hamilton B, Bisciotti G, et al. Injury epidemiology in a National football team of the Middle East. Scand J Med Sci Sports 2012;22:323–9. [DOI] [PubMed] [Google Scholar]
- 46.Eirale C, Tol JL, Smiley F, et al. Does Ramadan affect the risk of injury in professional football? Clinical Journal of Sport Medicine 2013;23:261–6. [DOI] [PubMed] [Google Scholar]
- 47.Ekstrand J, Tropp H. The incidence of ankle sprains in soccer. Foot & Ankle 1990;11:41–4. [DOI] [PubMed] [Google Scholar]
- 48.Engström B, Forssblad M, Johansson C, et al. Does a major knee injury definitely sideline an elite soccer player? Am J Sports Med 1990;18:101–5. [DOI] [PubMed] [Google Scholar]
- 49.Kad F, Faude O, Lensch J, et al. Injury characteristics in the German professional male soccer leagues after a shortened winter break. J Athl Train 2014;49:786–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Gouttebarge V, Hughes Schwab BA, Vivian A, et al. Injuries, matches missed and the influence of minimum Medical standards in the A-League professional football: a 5-year prospective study. Asian J Sports Med 2016;7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Hägglund M, Waldén M, Ekstrand J. Injury incidence and distribution in elite football-a prospective study of the Danish and the Swedish top divisions. Scand J Med Sci Sports 2005;15:21–8. [DOI] [PubMed] [Google Scholar]
- 52.Hägglund M, Waldén M, Ekstrand J. Injury recurrence is lower at the highest professional football level than at national and amateur levels: does sports medicine and sports physiotherapy deliver? Br J Sports Med 2016;50:751–8. [DOI] [PubMed] [Google Scholar]
- 53.Hassabi M, Mohammad-Javad Mortazavi S, Giti M-R, et al. Injury profile of a professional soccer team in the premier League of Iran. Asian J Sports Med 2010;1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Hawkins RD, Fuller CW. Risk assessment in professional football: an examination of accidents and incidents in the 1994 World Cup finals. Br J Sports Med 1996;30:165–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Junge A, Dvorak J. Injury surveillance in the world football Tournaments 1998–2012. Br J Sports Med 2013;47:782–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Kristenson K, Bjørneboe J, Waldén M, et al. The Nordic football injury audit: higher injury rates for professional football clubs with third-generation artificial turf at their home venue. Br J Sports Med 2013;47:775–81. [DOI] [PubMed] [Google Scholar]
- 57.Larruskain J, Lekue JA, Diaz N, et al. A comparison of injuries in elite male and female football players: a five-season prospective study. Scand J Med Sci Sports 2018;28:237–45. [DOI] [PubMed] [Google Scholar]
- 58.JW-Y L, Mok K-M, Chan HC-K, et al. A prospective epidemiological study of injury incidence and injury patterns in a Hong Kong male professional football League during the competitive season. Asia Pac J Sports Med Arthrosc Rehabil Technol 2014;1:119–25. [Google Scholar]
- 59.Nielsen AB, Yde J. Epidemiology and traumatology of injuries in soccer. Am J Sports Med 1989;17:803–7. [DOI] [PubMed] [Google Scholar]
- 60.Noya Salces J, Gómez-Carmona PM, Gracia-Marco L, et al. Epidemiology of injuries in first division Spanish football. J Sports Sci 2014b;32:1263–70. [DOI] [PubMed] [Google Scholar]
- 61.Noya Salces J, Gomez-Carmona PM, Moliner-Urdiales D, et al. An examination of injuries in Spanish professional soccer League. J Sports Med Phys Fitness 2014a;54:765–71. [PubMed] [Google Scholar]
- 62.Pedrinelli A, Filho GARdaC, Thiele ES, et al. Epidemiological study on professional football injuries during the 2011 CopA America, Argentina. Revista Brasileira de Ortopedia 2013;48:131–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Poulsen TD, Freund KG, Madsen F, et al. Injuries in high-skilled and low-skilled soccer: a prospective study. British Journal of Sports Medicine 1991;25:151–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Reis GF, Santos TRT, Lasmar RCP, et al. Sports injuries profile of a first division Brazilian soccer team: a descriptive cohort study. Braz. J. Phys. Ther 2015;19:390–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Shalaj I, Tishukaj F, Bachl N, et al. Injuries in professional male football players in Kosovo: a descriptive epidemiological study. BMC Musculoskelet Disord 2016;17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Stubbe JH, van Beijsterveldt A-MMC, van der Knaap S, et al. Injuries in professional male soccer players in the Netherlands: a prospective cohort study. J Athl Train 2015;50:211–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Williams S, Trewartha G, Kemp S, et al. A meta-analysis of injuries in senior men’s professional Rugby Union. Sports Med 2013;43:1043–55. [DOI] [PubMed] [Google Scholar]
- 68.van Beijsterveldt AMCA-M, Stubbe JH, Schmikli SL, et al. Differences in injury risk and characteristics between Dutch amateur and professional soccer players. J Sci Med Sport 2015;18:145–9. [DOI] [PubMed] [Google Scholar]
- 69.Mallo J, González P, Veiga S, et al. Injury incidence in a Spanish sub-elite professional football team: a prospective study during four consecutive seasons. J Sports Sci Med 2011;10. [PMC free article] [PubMed] [Google Scholar]
- 70.Peterson L, Junge A, Chomiak J, et al. Incidence of football injuries and complaints in different age groups and skill-level groups. Am J Sports Med 2000;28(5_suppl):51–7. [DOI] [PubMed] [Google Scholar]
- 71.Schick DM, Meeuwisse WH. Injury rates and profiles in female ice hockey players. Am J Sports Med 2003;31:47–52. [DOI] [PubMed] [Google Scholar]
- 72.Moller M, Attermann J, Myklebust G, et al. Injury risk in Danish youth and senior elite handball using a new SMS text messages approach. Br J Sports Med 2012;46:531–7. [DOI] [PubMed] [Google Scholar]
- 73.Podlog L, Buhler CF, Pollack H, et al. Time trends for injuries and illness, and their relation to performance in the National Basketball association. Journal of Science and Medicine in Sport 2015;18:278–82. [DOI] [PubMed] [Google Scholar]
- 74.Ekstrand J, Hägglund M, Waldén M. Epidemiology of muscle injuries in professional football (soccer). Am J Sports Med 2011;39:1226–32. [DOI] [PubMed] [Google Scholar]
- 75.Bangsbo J, Mohr M, Krustrup P. Physical and metabolic demands of training and match-play in the elite football player. Journal of Sports Sciences 2006;24:665–74. [DOI] [PubMed] [Google Scholar]
- 76.Gabbett TJ. The training-injury prevention paradox: should athletes be training smarter and harder? Br J Sports Med 2016;50:273–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Rahnama N, Reilly T, Lees A. Injury risk associated with playing actions during competitive soccer. Br J Sports Med 2002;36:354–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Hägglund M. Epidemiology and prevention of football injuries Institutionen för hälsa och samhälle, 2007. [Google Scholar]
- 79.Bahr R, Clarsen B, Ekstrand J. Why we should focus on the burden of injuries and illnesses, not just their incidence. Br J Sports Med 2017. [DOI] [PubMed] [Google Scholar]
- 80.Ekstrand J, Waldén M, Hägglund M. Hamstring injuries have increased by 4% annually in men’s professional football, since 2001: a 13-year longitudinal analysis of the UEFA Elite Club injury study. Br J Sports Med 2016;50:731–7. [DOI] [PubMed] [Google Scholar]
- 81.Croisier J-L, Ganteaume S, Binet J, et al. Strength imbalances and prevention of hamstring injury in professional soccer players. Am J Sports Med 2008;36:1469–75. [DOI] [PubMed] [Google Scholar]
- 82.Petersen J, Thorborg K, Nielsen MB, et al. Preventive effect of eccentric training on acute hamstring injuries in men’s soccer: a cluster-randomized controlled trial. Am J Sports Med 2011;39:2296–303. [DOI] [PubMed] [Google Scholar]
- 83.van Dyk N, Bahr R, Whiteley R, et al. Hamstring and quadriceps isokinetic strength deficits are weak risk factors for hamstring strain injuries. Am J Sports Med 2016;44:1789–95. [DOI] [PubMed] [Google Scholar]
- 84.Henderson G, Barnes CA, Portas MD. Factors associated with increased propensity for hamstring injury in English premier League soccer players. Journal of Science and Medicine in Sport 2010;13:397–402. [DOI] [PubMed] [Google Scholar]
- 85.Fousekis K, Tsepis E, Poulmedis P, et al. Intrinsic risk factors of non-contact quadriceps and hamstring strains in soccer: a prospective study of 100 professional players. British Journal of Sports Medicine 2011;45:709–14. [DOI] [PubMed] [Google Scholar]
- 86.Lees A, Nolan L. The biomechanics of soccer: a review. Journal of Sports Sciences 1998;16:211–34. [DOI] [PubMed] [Google Scholar]
- 87.Timmins RG, Bourne MN, Shield AJ, et al. Short biceps femoris fascicles and eccentric knee flexor weakness increase the risk of hamstring injury in elite football (soccer): a prospective cohort study. Br J Sports Med 2016;50:1524–35. [DOI] [PubMed] [Google Scholar]
- 88.Rahnama N, Reilly T, Lees A, et al. Muscle fatigue induced by exercise simulating the work rate of competitive soccer. Journal of Sports Sciences 2003;21:933–42. [DOI] [PubMed] [Google Scholar]
- 89.McCall A, Dupont G, Ekstrand J. Injury prevention strategies, coach compliance and player adherence of 33 of the UEFA Elite Club Injury Study teams: a survey of teams’ head medical officers. Br J Sports Med 2016;50:725–30. [DOI] [PubMed] [Google Scholar]
- 90.Wong P, Hong Y. Soccer injury in the lower extremities. British Journal of Sports Medicine 2005;39:473–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Emery CA, Meeuwisse WH. The effectiveness of a neuromuscular prevention strategy to reduce injuries in youth soccer: a cluster-randomised controlled trial. British Journal of Sports Medicine 2010;44:555–62. [DOI] [PubMed] [Google Scholar]
- 92.Silvers H, Mandelbaum B, Bizzini M, et al. The efficacy of the FIFA 11+ program in the collegiate male soccer player (USA). Br J Sports Med 2014;48:662.1–662. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.van der Horst N Preventing hamstring injuries in football through enhanced exercise and RTP strategies. Br J Sports Med 2018;0:1–2. [DOI] [PubMed] [Google Scholar]
- 94.Bengtsson H, Ekstrand J, Hägglund M. Muscle injury rates in professional football increase with fixture congestion: an 11-year follow-up of the UEFA champions League injury study. Br J Sports Med 2013;47:743–7. [DOI] [PubMed] [Google Scholar]
- 95.Bengtsson H, Ekstrand J, Waldén M, et al. Muscle injury rate in professional football is higher in matches played within 5 days since the previous match: a 14-year prospective study with more than 130 000 match observations. Br J Sports Med 2017. [DOI] [PubMed] [Google Scholar]
- 96.Carling C, McCall A, Le Gall F, et al. The impact of short periods of match congestion on injury risk and patterns in an elite football Club. Br J Sports Med 2016;50:764–8. [DOI] [PubMed] [Google Scholar]
- 97.Ekstrand J, Waldén M, Hägglund M. A congested football calendar and the wellbeing of players: correlation between match exposure of European footballers before the World Cup 2002 and their injuries and performances during that World Cup. British Journal of Sports Medicine 2004;38:493–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Lystad RP, Gregory K, Wilson J. The epidemiology of injuries in mixed martial arts a systematic review and meta-analysis. Orthop J Sports Med 2014;2. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.