

Abstract
Background
Authors from low and middle-income country (LMIC) institutions are under-represented in publications of research based in LMICs. This case study of publications from authors within the Medical Research Council International Statistics and Epidemiology Group (MRC-ISEG), a global health research group affiliated to the London School of Hygiene & Tropical Medicine in the UK, aims to describe patterns in authorship and factors associated with under-representation.
Methods
Papers were included if they were published between January 2016 and December 2020 inclusive, included an author from the MRC-ISEG and described work conducted in a LMIC. Authors’ affiliations were classified using World Bank country income classifications into LMIC affiliations only, high-income country (HIC) affiliations only and mixed LMIC/HIC affiliations. Multinomial logistic regression analysis was used to assess associations of author affiliation category with authorship position, and whether patterns varied by journal impact factor quartile and multiple versus single-country studies.
Results
A total of 882 papers, including 10 570 authors describing research conducted in 61 LMICs, were included. Compared with authors of HIC-only affiliation, those with LMIC-only affiliation were less likely to be in first authorship position (relative risk ratio (RRR)=0.51, 95% CI 0.44 to 0.60) and mixed HIC/LMIC affiliation authors were more likely (RRR=2.80, 95% CI 2.35 to 3.34). Compared with authors of HIC-only affiliation, those with LMIC-only affiliation were less likely to be in last authorship position (RRR=0.20, 95% CI 0.16 to 0.24) and those with mixed HIC/LMIC affiliations were more likely (RRR=1.95, 95% CI 1.65 to 2.30). The proportion of senior authors with LMIC-only affiliation was lowest for the highest impact journals, and in multicountry versus single-country studies.
Conclusion
Alongside increasing research capacity within LMICs, HIC institutions should ensure that LMIC-affiliated researchers are properly represented in global research. Academics working in global health should be judged on their involvement in representative collaborative research rather than individual achievements in authorship position.
Keywords: epidemiology
WHAT IS ALREADY KNOWN ON THIS TOPIC
Existing literature has highlighted inequalities in authorship among publications describing research conducted in low and middle-income country (LMIC) settings, with a lack of LMIC author representation particularly in first and last authorship positions.
Further understanding of the nature and predictors of authorship inequalities is needed.
WHAT THIS STUDY ADDS
This paper describes patterns in authorship and factors associated with under-representation in senior authorship positions in publications from the UK-based Medical Research Council International Statistics and Epidemiology Group (MRC-ISEG) over a 5-year period.
In addition to showing that LMIC-affiliated authors are under-represented in leading authorship positions in MRC-ISEG publications, the findings suggest that LMIC representation in senior authorship positions is lower in the highest journal impact factor publications and in multicountry studies versus single-country studies.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
These results demonstrate the urgent need to address inequalities in global health research collaborations.
Capacity strengthening initiatives to increase funding, training and opportunities for LMIC researchers, and increased recognition of equitable research should be prioritised.
Introduction
Global health initiatives commonly involve partnerships between countries, institutions and governments to codevelop public health strategies. Such actions often include research partnerships that bring together researchers from both high-income countries (HICs) and low and middle-income countries (LMICs) to address public health problems that disproportionately affect populations in LMICs.
These partnerships are important because the high burden of diseases in LMICs has not been matched by adequate funding and capacity to address existing gaps in research. Despite accounting for over 80% of the world’s population and 92% of global disease burden, only 10% of funds for global health research are budgeted for health research in LMICs.1 International scientific collaborations between researchers in HICs and LMICs provide opportunities for leadership from LMIC researchers to address public health problems prevalent in LMICs.1 2 However, inequities in research production and ownership have persisted.3–5
Global health collaborations have been described as potentially exploitative of LMIC researchers and communities,6 7 with under-representation of LMIC authors in written research outputs even when the research is conducted and hosted in LMICs. Guidelines from the International Committee of Medical Journal Editors (ICMJE) specify that authorship is assigned in descending order of contribution with the first author being the lead contributor of the research and the last author also having prominent leadership responsibility and ownership of the published manuscript compared with individuals in other authorship roles. Bibliometric analyses have highlighted inequities in terms of research authorship positions in research conducted in LMICs,8–10 and have shown that first and last authorship positions are more frequently held by HIC than LMIC researchers.3 11 12 The relatively small number of researchers in LMICs has been suggested to be one of the reasons why such imbalances in research outputs exist.13 For example, it is estimated that Africa has 198 researchers per million inhabitants compared with the UK and USA that have 4000 per million.13 Possible explanations for this could be a lack of academic and economic resources and poorer research infrastructure in sub-Saharan African (SSA) countries.14 Research has highlighted the need for high-income institutions, funding agencies and journals to promote research from within SSA which is equitable and collaborative.15
While increasing research highlights the inequities of authorship position related to LMIC/HIC affiliation, gaps exist in understanding the nature and predictors of authorship inequalities. This bibliometric analysis, focusing on a global health research group affiliated with a HIC institution, sought to understand whether author affiliation is associated with authorship position, and to assess the impact of study and paper characteristics on this relationship. Research has noted different authorship practices are dependent on the discipline in which the paper is focused,16 this paper explores authorship within statistics and epidemiology, a discipline in which authorship inequalities have not previously been widely researched.
Methods
The Medical Research Council International Statistics and Epidemiology Group (MRC-ISEG) is a group of 35 statisticians and epidemiologists at the London School of Hygiene & Tropical Medicine (LSHTM) who work mainly on the epidemiology, prevention and treatment of HIV, tuberculosis, malaria, emerging and neglected tropical diseases and statistical methodology in LMICs.17 MRC-ISEG members are predominantly based in London, although members are also based in several LMICs. The focus of MRC-ISEG is primarily to conduct research; however, the group also plays a role in capacity strengthening, including leading initiatives such as the MRC-funded ISEG Fellowship scheme which supports researchers from SSA to study an MSc in Medical Statistics at LSHTM. It also runs The European & Developing Countries Clinical Trials Partnership (EDCTP) funded East and Southern African Consortium for Outbreak Epidemiology Training programme, a collaboration with six African institutions which supports public health practitioners from SSA to study an MSc in Epidemiology at LSHTM.
A database was generated to collect information about peer-reviewed publications which included MRC-ISEG authors between January 2016 and December 2020. The database was built from Elements software (Symplectic, UK) which collates publication data from LSHTM-affiliated staff. The database included the paper’s title, journal name, authors, authorship positions and affiliations for each author. The data set was exported to Excel (Microsoft, USA), where titles and abstracts were screened independently by two authors (ELW, KT) to identify papers which met the inclusion criteria. Papers that were published during the timeframe, included an author from the MRC-ISEG and described work conducted in an LMIC were eligible for inclusion. Papers were excluded if they were duplicates, methodology papers, systematic reviews or were not peer-reviewed research articles (eg, abstracts, books, commentaries, conference presentations, reports, reviews or letters). The only papers which included work conducted in both HIC and LMIC settings were systematic reviews and were therefore excluded.
The title and abstract of eligible papers were used to classify papers based on location of research (single country or multicountry). Journal impact factor (IF) data were collected from Journal Citation Reports. For the 5.4% of papers whose journal IF could not be obtained from Journal Citation Reports, their journal IF was identified directly from the journal website or through online searching. This variable was then split into four quartiles.
Based on World Bank country income classifications,18 each individual author affiliation was classified as being from a low-income country, lower middle-income country, upper middle-income country or HIC. Authors with multiple affiliations were categorised as LMIC affiliations only, HIC affiliations only and mixed LMIC/HIC affiliations.
The number and proportion of authors in each affiliation group was tabulated overall and separately by authorship position (first, last, second, other). Only 16 (1.8%) papers had less than four authors; for papers with only one author they were classified as first, for papers with two authors they were classified as first and last, respectively, and for papers with three authors they were classified as first, second and last. To quantify how authorship affiliation category impacted authorship position, relative risk ratios (RRR) were estimated using multinomial logistic regression models with authorship position (first, second, last, other) as the outcome and author affiliation (LMIC only, LMIC/HIC, HIC only) as the main independent variable, allowing for authorship clustering by paper using robust SEs. Reference groups were ‘Other’ authorship position for the outcome and ‘HIC-only’ affiliation for the main independent variable. To analyse effect modification between author affiliation and study characteristics, interaction terms were included in the regression models. All analyses and data visualisation were done in Stata V.16.1 (StataCorp, USA) and Excel.
Patient and public involvement
Patients and the public were not involved in the design, conduct or dissemination of this study.
Results
A total of 1079 papers published by ISEG members from 1 January 2016 to 31 December 2020 were identified from the Elements database. Of these, 11 duplicates and a further 186 papers were excluded (figure 1), so that a total of 882 papers were included in the final analysis data set (figure 1), describing research conducted in a total of 61 countries.
Figure 1.

Selection process for included papers. LMIC, low and middle-income country; MRC-ISEG, Medical Research Council International Statistics and Epidemiology Group.
Most papers (669; 75.9%) were observational studies, with the remaining 213 intervention studies (table 1). Almost all the intervention studies included randomisation (204; 95.8%), thus no comparisons between non-randomised and randomised intervention studies were made. Overall, 17 (1.9%) papers reported multicountry research. There were a mean of 8.9 authors per paper, and this was similar by study characteristics (table 1).
Table 1.
Study characteristics of included papers
| Study characteristic | n (%) | Mean number of authors per paper | SD |
| Author affiliation | |||
| All authors LMIC only | 11 (1.2) | 9.31 | 1.75 |
| Mixed LMIC/HIC authors | 829 (94.0) | 9.17 | 1.62 |
| All authors HIC only | 42 (4.8) | 9.22 | 1.68 |
| Journal impact factor | |||
| Lowest quartile (0–2.27) | 224 (25.4) | 8.67 | 1.42 |
| Low quartile (2.27–3.30) | 233 (26.4) | 8.60 | 1.49 |
| High quartile (3.30–5.23) | 207 (23.5) | 8.78 | 1.80 |
| Highest quartile (5.23–91.3) | 218 (24.7) | 9.03 | 1.98 |
| Country of study | |||
| Single | 865 (98.1) | 9.35 | 1.35 |
| Multiple | 17 (1.9) | 9.03 | 2.35 |
| Study country category (of single-country studies) | |||
| Low income | 281 (42.1) | 8.60 | 2.07 |
| Lower middle income | 266 (39.8) | 8.68 | 1.67 |
| Upper middle income | 121 (18.1) | 8.94 | 1.57 |
| Study topic | |||
| Emerging and neglected diseases* | 193 (21.9) | 9.33 | 1.47 |
| HIV/RSH† | 242 (27.4) | 9.44 | 1.31 |
| Malaria | 209 (23.7) | 9.02 | 2.29 |
| Tuberculosis | 64 (7.3) | 9.34 | 1.30 |
| Multiple | 19 (2.2) | 9.34 | 1.38 |
| Other | 155 (17.5) | 9.20 | 1.54 |
| Study design | |||
| Intervention | 213 (24.1) | 9.02 | 1.43 |
| Observational | 669 (75.9) | 8.68 | 1.78 |
*Neglected tropical diseases, mental health, eye health and disease outbreaks.
† Reproductive and sexual health
HIC, high-income country; LMIC, low and middle-income country.
Of the 882 eligible papers, 42 (4.8%) had only HIC-affiliated authors and 840 (94.0%) had a mix of HIC-affiliated and LMIC-affiliated authors. There were a total of 10 570 (non-unique) authors, of whom 8073 (76.4%) had only one affiliation, 2113 (20.0%) had two affiliations, 340 (3.2%) had three affiliations and 44 (0.4%) had four or more affiliations. Based on all affiliations reported by each author, 4555 (43.1%) authors had LMIC-only affiliations, 4767 (45.1%) had HIC-only affiliations and 1247 (11.8%) had mixed LMIC/HIC affiliations.
Figure 2 displays the proportions of authors by affiliation, stratified by authorship position. There was strong evidence of differences in authorship position by affiliation with the proportion of LMIC-only-affiliated authors being lower for first (27%) and last (14%) authorship positions than for second (42%) and other (48%) positions (p<0.001). As shown in table 2, LMIC-only-affiliated authors, compared with HIC-only authors, were associated with a decreased likelihood of being first or last author compared with ‘other’ authorship positions (first authorship position: RRR=0.51, 95% CI 0.44 to 0.60; last authorship position: RRR=0.20, 95% CI 0.16 to 0.24). However, mixed LMIC/HIC author affiliations, compared with HIC-only affiliations, were associated with an increased likelihood of first or last authorship position (first authorship position: RRR=2.80, 95% CI 2.35 to 3.34; last authorship position: RRR=1.95, 95% CI 1.65 to 2.30).
Figure 2.
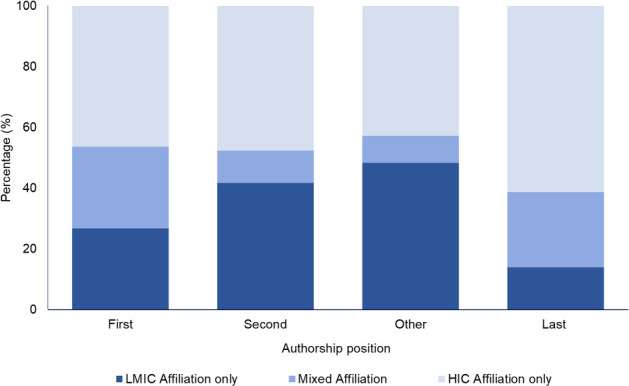
Overall author affiliation by authorship position. HIC, high-income country; LMIC, low and middle-income country.
Table 2.
Relative risk ratios (compared with other authorship position) for the association between author affiliation and authorship position
| Affiliation group | Authors (n) | First author | Second author | Last author |
| HIC affiliation only | 4763 | Reference group | Reference group | Reference group |
| LMIC affiliation only | 4556 | 0.51 (0.44–0.60) | 0.78 (0.67–0.90) | 0.20 (0.16–0.24) |
| Mixed LMIC/HIC affiliations | 1251 | 2.80 (2.35–3.34) | 1.07 (0.85–1.36) | 1.95 (1.65–2.30) |
HIC, high-income country; LMIC, low and middle-income country.
There was strong evidence of effect modification by journal IF for the association between authorship affiliation and authorship position (p=0.01; online supplemental figure 1). The proportion of LMIC-only-affiliated authors in first or last authorship position decreased with increasing journal impact quartile.
bmjgh-2022-011053supp001.pdf (499KB, pdf)
Being a LMIC-only-affiliated author, compared with a HIC-affiliated author, was associated with a decreased likelihood of being in last authorship. The reduction in RRR generally becomes greater with increasing journal IF quartile (lowest journal IF quartile: RRR=0.28, 95% CI 0.20 to 0.38; low journal IF quartile: RRR=0.23, 95% CI 0.16 to 0.33; high journal IF quartile: RRR=0.12, 95% CI 0.08 to 0.20; highest journal IF quartile: RRR=0.15, 95% CI 0.10 to 0.24). RRRs for first authorship position followed a similar pattern. For mixed LMIC/HIC author affiliations, RRRs for first and last authorship positions were all greater than 1; RRRs for first authorship position of mixed LMIC/HIC affiliated authors compared with HIC-only-affiliated authors decreased with increasing IF quartile, while RRRs for last authorship position increased with increasing IF quartile (table 3).
Table 3.
Relative risk ratios (compared with other authorship position) for the association between author affiliation and authorship position, stratified by journal impact factor
| Affiliation group | First author | Second author | Last author |
| Lowest <2.6 | |||
| HIC affiliation only | Reference group | Reference group | Reference group |
| LMIC affiliation only | 0.61 (0.46–0.83) | 0.95 (0.72–1.26) | 0.28 (0.20–0.38) |
| Mixed LMIC/HIC affiliations | 3.16 (2.19–4.57) | 0.67 (0.35–1.30) | 1.70 (1.16–2.50) |
| Low 2.6–3.3 | |||
| HIC affiliation only | Reference group | Reference group | Reference group |
| LMIC affiliation only | 0.64 (0.47–0.88) | 0.87 (0.66–1.16) | 0.23 (0.16–0.33) |
| Mixed LMIC/HIC affiliations | 2.99 (2.16–4.15) | 1.35 (0.91–2.03) | 1.80 (1.31–2.47) |
| High 3.3–5.3 | |||
| HIC affiliation only | Reference group | Reference group | Reference group |
| LMIC affiliation only | 0.37 (0.25–0.53) | 0.56 (0.41–0.78) | 0.12 (0.08–0.20) |
| Mixed LMIC/HIC affiliations | 2.99 (2.10–4.27) | 1.16 (0.73–1.84) | 1.80 (1.27–2.57) |
| Highest >5.3 | |||
| HIC affiliation only | Reference group | Reference group | Reference group |
| LMIC affiliation only | 0.42 (0.31–0.58) | 0.72 (0.53–0.97) | 0.15 (0.10–0.24) |
| Mixed LMIC/HIC affiliations | 2.25 (1.56–3.24) | 0.99 (0.61–1.61) | 2.53 (1.88–3.41) |
HIC, high-income country; LMIC, low and middle-income country.
There was also evidence of effect modification by single-country versus multiple-country studies (p=0.001). The proportion of both LMIC-only and mixed LMIC/HIC-affiliated authors in first, second and last positions, respectively, compared with ‘other authors’ was consistently higher in single-country studies compared with multicountry studies (online supplemental figure 2 and online supplemental table 1). LMIC-only-affiliated authors were least likely to be in first or last authorship position in multicountry studies (first authorship position: RRR=0.24, 95% CI 0.17 to 0.35; last authorship position: RRR=0.11, 95% CI 0.07 to 0.19). Mixed LMIC/HIC-affiliated authors were more likely than HIC-only authors to be first authors in single-country studies (RRR=3.65, 95% CI 2.98 to 4.47) than in multicountry studies (RRR=1.01, 95% CI 0.66 to 1.56). A similar pattern is seen for last authorship position.
bmjgh-2022-011053supp002.pdf (58.2KB, pdf)
Discussion
In this case study of publications describing work conducted in LMICs and including authors from a global health research group affiliated to a HIC institution, we found that the proportion of LMIC-only-affiliated authors in first and last authorship positions was considerably lower than in second and other authorship positions. Representation of LMIC-only authors in senior (first and last) authorship roles was poorer for papers published in higher impact journals, and for multicountry compared with single-country studies. Despite all the papers describing research conducted in LMIC settings, we found that only 55% of all authors had any LMIC institutional affiliation.
Our findings add to the increasing body of evidence from other literature investigating authorship inequities in global health research.14 19 20 In a recent systematic review of authorship in collaborative health research in Africa, 54% of all authors and 53% of first authors were from the country of the paper’s focus, with lower representation where collaborators were from the USA, Canada or Europe, dropping to 41% when authors were affiliated to a top US university.14 It has also been shown that inequities in the distribution of authorship position got worse during the period 2008–2019, particularly within last authorship position.21 While previous research has reported that the lack of local authorship has ranged from 28% to 70% of publications,22 23 our research group had only 5% of papers with no local authors.
Our findings support previous literature demonstrating that first and last authorship positions are dominated by HIC authors compared with LMIC authors, with second authorship position showing a more equal distribution of author affiliations,20 and that last authorship position typically has the lowest representation of LMIC authors.24 We found that these results held, regardless of journal IF and whether it was a single-country or multicountry study. Further, we found that representation of LMIC-only-affiliated authors in first and last authorship positions reduced with increasing journal IF. These findings reflect other literature that has found a poorer representation of LMIC authors in higher IF journals.25 26 Without information on submission statistics, it is not possible to determine whether this is due to differences in submission patterns, differences in acceptance patterns or both. However, representation of LMIC scientists is lower among journal editors and reviewers,27 28 which could influence acceptance rates. Exploring whether citations of a paper are associated with authorship affiliation was not possible in this case study due to the recent publication timeframe within which included papers were published. However, in recent literature, it has been noted that the relative citation ratio for both first and last authors was lower for SSA authors compared with USA-affiliated authors.29
The poorer representation of LMIC-only and mixed LMIC/HIC-affiliated authors in multicountry studies compared with single-country studies is consistent with research that found ‘authorship parasitism’, in which one benefits at the expense of another, is not common generally, except for within multicountry studies.30 These findings have been argued to reflect the inherent international hierarchy of global health research.19 The higher RRRs for mixed LMIC/HIC affiliation authors compared with HIC-only-affiliated authors in single-country studies could be due to mixed LMIC/HIC-affiliated authors typically being more senior and therefore having ownership of single-country studies. However, in multicountry studies, there is more competition for senior authorship position and so HIC-only-affiliated authors may be more likely to take a leadership position, particularly if funding for the research has come from a HIC. These results could also be linked to the effect modification by journal IF, studies that are multicountry are more likely to be studies that require greater funding, which could be more likely to come from a HIC. These larger multicountry studies could therefore be more likely to be published in a higher impact journal. Unfortunately, due to there being only 17 multicountry studies within this analysis we were unable to explore this theory further.
The structural and systemic causes of publishing inequities, and the underlying inequities in global health research that they likely reflect, are long-standing and multifactorial. Inequalities have been attributed to both technical advances and developed research structures in HICs which allow authors from HICs to develop strong research networks, secure funding and often contribute to the majority of the write-up of a paper.14 In addition, open access fees also create a barrier in publishing research, potentially disadvantaging authors with LMIC-only affiliations in publishing papers particularly in high-impact journals. Despite some journals waiving fees for papers with a lead LMIC author, research analysing 272 journals found that only 51% offered a waiver to LMIC authors.31 Written agreements between HIC and LMIC collaborators can ensure there is co-ownership of research study data and that LMIC authors are able to propose papers that they will first author. However, these agreements are still dependent on the principal investigator, who may often be affiliated to a HIC institution only, approving these suggestions and also creating an environment in which LMIC researchers feel empowered to suggest leading papers. Furthermore, limitations with ICMJE guidelines could also contribute to authorship inequalities, with language barriers being a key factor which could result in an author not meeting the authorship guidelines, despite their notable contributions to the conceptualisation and conduct of the research underlying the paper.16
However, authorship inequalities could also result from inherent inequity. There is an underlying conflict between HIC authors focusing on individual success commonly required for their career progression, compared with collaborating on truly equitable research where LMIC scientists are leading research and are properly represented throughout the whole research process. HIC researchers themselves should take responsibility for embracing equitable research practices. However, this should be supported by HIC institutions developing policies where academics are recognised for their commitment to collaborative and equitable research as opposed to individual achievements. LMIC authors being undervalued at the stage of publication has been labelled as ‘neo-colonial science’22 and requires a commitment to capacity strengthening in LMICs and reconsideration of the values of HIC academic institutions to address these sources of inequality. It is the responsibility of funders, governments and academic institutions to ensure capacity strengthening efforts and equitable partnerships are integrated into all global health research as a priority.32 Research collaborations, where the funding is routed through a HIC institution as opposed to going directly to LMIC institutions in the country where the research is being conducted, limit LMIC institutions from enhancing their own research funding infrastructure and capacity. Thus, global health funders should prioritise provision of resources directly to LMIC institutions. As a university, LSHTM has introduced new core values, which include integrity in working together, these values need to be put into practice with commitment to representative authorship. MRC-ISEG also supports LMIC coauthors, particularly PhD students and early career researchers, to develop experience with navigating paper development and submission.
Our case study had several limitations. First, we used information on author affiliation rather than nationality, as nationality is not recorded on publication databases. The results may not therefore represent associations with nationality. Second, the data extracted from Elements did not capture data on joint first or last authorship. The second-named joint first author was classified as holding second authorship position, and the penultimate author as ‘other’ authorship position. However, the prevalence of joint authorship is low, and we expect the impact to be small and not associated with affiliation. In addition, data on other characteristics that might be associated with authorship patterns, such as funding source or author gender, were not available. The presence/absence and nature of agreements between HIC and LMIC authors on each study would have been useful to investigate in this analysis; however, data on this were not accessible from the database from which we extracted the data set. Since we only included papers from a relatively short time period, we were unable to access temporal trends in authorship patterns. It also needs to be acknowledged that institutional affiliation may not be able to fully capture the power dynamics that LMIC authors experience within academia, issues of gender, race and identity are likely to create complex power inequalities beyond just authorship position. We also recognise that this is a case study of a HIC-affiliated research group, resulting in a lack of generalisability to other disciplines and research conducted in other areas; our results may not be directly comparable to other work on the topic. However, the fact that we reviewed only papers on studies conducted in LMIC countries and found that 5% of papers do not have any LMIC authors indicates that these issues are likely to be more broadly experienced than just within the MRC-ISEG, as demonstrated by the increasing literature on this topic.
Conclusion
Our results demonstrate that the representation of LMIC-only-affiliated authors is considerably poorer in senior authorship positions compared with HIC-only-affiliated authors. Authors with mixed LMIC/HIC affiliations were more likely than HIC-only-affiliated authors to be in either first or last position. The association between author affiliation and authorship position was exacerbated in papers of higher journal IF and of studies based in multiple countries. While authorship alone does not ensure collaborations are equitable, it is a good indicator of who is benefiting from research. These findings demonstrate the need for HIC institutions to value equal collaboration. In addition to institution and government-level capacity strengthening initiatives, it needs to be recognised that increasing LMIC representation relies on the core values of research institutes prioritising collaborative and equitable research. The success and credit given to academics should be shifted away from individual success and focus on ways in which they have engaged in equitable research that has fairly represented authors from LMIC settings. Efforts should be made by all stakeholders to shift the unequal power dynamic that typically results in LMIC researchers being undervalued and under-represented.
Acknowledgments
We thank Andy Reid from LSHTM for extracting the publication data from Elements software. KT, JB, HAW and ELW were part funded by an award from the UK Medical Research Council (MRC) (grant reference: MR/R010161/1, HAW); this award is jointly funded by the UK MRC and the UK Foreign, Commonwealth & Development Office (FCDO) under the MRC/FCDO Concordat agreement and is also part of the EDCTP2 programme supported by the European Union.
Footnotes
Handling editor: Seye Abimbola
IS and KT contributed equally.
Contributors: IS and KT conceptualised the contents of the paper, cleaned and analysed the data and drafted the paper. JB and TM contributed to the drafting and editing of the paper. HAW contributed to the conceptualisation and editing of the paper. ELW contributed to the conceptualisation of the paper, cleaning and analysing of the data and editing of the paper. KT is guarantor and accepts full responsibilty for the work.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Patient and public involvement: Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review: Not commissioned; externally peer reviewed.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Not applicable.
References
- 1.Franzen SRP, Chandler C, Lang T. Health research capacity development in low and middle income countries: reality or rhetoric? A systematic meta-narrative review of the qualitative literature. BMJ Open 2017;7:e012332. 10.1136/bmjopen-2016-012332 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ralaidovy AH, Adam T, Boucher P. Resource allocation for biomedical research: analysis of investments by major funders. Health Res Policy Syst 2020;18:20. 10.1186/s12961-020-0532-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.González-Alcaide G, Park J, Huamaní C, et al. Dominance and leadership in research activities: collaboration between countries of differing human development is reflected through authorship order and designation as corresponding authors in scientific publications. PLoS One 2017;12:e0182513. 10.1371/journal.pone.0182513 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hasnida A, Borst RA, Johnson AM, et al. Making health systems research work: time to shift funding to locally-led research in the south. Lancet Glob Health 2017;5:e22–4. 10.1016/S2214-109X(16)30331-X [DOI] [PubMed] [Google Scholar]
- 5.Badenhorst A, Mansoori P, Chan KY. Assessing global, regional, National and sub-national capacity for public health research: a bibliometric analysis of the web of science (TM) in 1996-2010. J Glob Health 2016;6:010504. 10.7189/jogh.06.010504 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Crane J. Scrambling for Africa? universities and global health. Lancet 2011;377:1388–90. 10.1016/S0140-6736(10)61920-4 [DOI] [PubMed] [Google Scholar]
- 7.Mbaye R, Gebeyehu R, Hossmann S, et al. Who is telling the story? A systematic review of authorship for infectious disease research conducted in Africa, 1980-2016. BMJ Glob Health 2019;4:e001855. 10.1136/bmjgh-2019-001855 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Pineda P, Gregorutti G, Streitwieser B. Emerging decolonialized research collaboration: the max planck society and the leibniz association in latin america. J Stud Int Educat 2020;24:59–78. 10.1177/1028315319888891 [DOI] [Google Scholar]
- 9.Kelaher M, Ng L, Knight K, et al. Equity in global health research in the new millennium: trends in first-authorship for randomized controlled trials among low- and middle-income country researchers 1990-2013. Int J Epidemiol 2016;45:2174–83. 10.1093/ije/dyw313 [DOI] [PubMed] [Google Scholar]
- 10.Lawrence DS, Leeme T, Mosepele M, et al. Equity in clinical trials for HIV-associated cryptococcal meningitis: a systematic review of global representation and inclusion of patients and researchers. PLoS Negl Trop Dis 2021;15:e0009376. 10.1371/journal.pntd.0009376 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Adedokun BO, Olopade CO, Olopade OI. Building local capacity for genomics research in Africa: recommendations from analysis of publications in sub-Saharan Africa from 2004 to 2013. Glob Health Action 2016;9:31026. 10.3402/gha.v9.31026 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Garbern SC, Hyuha G, González Marqués C, et al. Authorship representation in global emergency medicine: a bibliometric analysis from 2016 to 2020. BMJ Glob Health 2022;7:e009538. 10.1136/bmjgh-2022-009538 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Simpkin V, Namubiru-Mwaura E, Clarke L, et al. Investing in health R & D: where we are, what limits us, and how to make progress in Africa. BMJ Glob Health 2019;4:e001047. 10.1136/bmjgh-2018-001047 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hedt-Gauthier BL, Jeufack HM, Neufeld NH, et al. Stuck in the middle: a systematic review of authorship in collaborative health research in Africa, 2014-2016. BMJ Glob Health 2019;4:e001853. 10.1136/bmjgh-2019-001853 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Rees CA, Ali M, Kisenge R, et al. Where there is no local author: a network bibliometric analysis of authorship parasitism among research conducted in sub-saharan africa. BMJ Glob Health 2021;6:e006982. 10.1136/bmjgh-2021-006982 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Smith E, Hunt M, Master Z. Authorship ethics in global health research partnerships between researchers from low or middle income countries and high income countries. BMC Med Ethics 2014;15:42. 10.1186/1472-6939-15-42 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.MRC international statistics and epidemiology group 2022. Available: https://www.lshtm.ac.uk/research/centres-projects-groups/mrc-international-statistics-and-epidemiology-group#welcome [Accessed 9 Feb 2022].
- 18.GNI per capita, atlas method (current US$) 2020. Available: https://data.worldbank.org/indicator/NY.GNP.PCAP.CD [Accessed 22 May 2022].
- 19.Schneider H, Maleka N. Patterns of authorship on community health workers in low-and-middle-income countries: an analysis of publications (2012-2016). BMJ Glob Health 2018;3:e000797. 10.1136/bmjgh-2018-000797 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Pingray V, Ortega V, Yaya S, et al. Authorship in studies conducted in low-and-middle income countries and published by reproductive health: advancing equitable global health research collaborations. Reprod Health 2020;17:18. 10.1186/s12978-020-0858-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Hart KL, Perlis RH. Authorship inequality: a bibliometric study of the concentration of authorship among a diminishing number of individuals in high-impact medical journals, 2008-2019. BMJ Open 2021;11:e046002. 10.1136/bmjopen-2020-046002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Farid Dahdouh-Guebas JA. Rita van moll & nico koedam neo-colonial science by the most industrialised upon the least developed countries in peer-reviewed publishing. Scientometrics 2003. [Google Scholar]
- 23.Ghani M, Hurrell R, Verceles AC, et al. Geographic, subject, and authorship trends among LMIC-based scientific publications in high-impact global health and general medicine journals: a 30-month bibliometric analysis. J Epidemiol Glob Health 2021;11:92–7. 10.2991/jegh.k.200325.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Dimitris MC, Gittings M, King NB. How global is global health research? A large-scale analysis of trends in authorship. BMJ Glob Health 2021;6:e003758. 10.1136/bmjgh-2020-003758 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Chersich MF, Blaauw D, Dumbaugh M, et al. Local and foreign authorship of maternal health interventional research in low- and middle-income countries: systematic mapping of publications 2000-2012. Global Health 2016;12:35. 10.1186/s12992-016-0172-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Keiser J, Utzinger J, Tanner M, et al. Representation of authors and editors from countries with different human development indexes in the leading literature on tropical medicine: survey of current evidence. BMJ 2004;328:1229–32. 10.1136/bmj.38069.518137.F6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Guetter CR, Vervoort D, Luc JGY, et al. Female and country representation on editorial boards of cardiothoracic surgery journals. Semin Thorac Cardiovasc Surg 2022;34:1233–5. 10.1053/j.semtcvs.2021.08.015 [DOI] [PubMed] [Google Scholar]
- 28.Pike KM, Min S-H, Poku OB, et al. A renewed call for international representation in editorial boards of international psychiatry journals. World Psychiatry 2017;16:106–7. 10.1002/wps.20389 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Akudinobi EA, Kilmarx PH. Bibliometric analysis of sub-Saharan African and US authorship in publications about sub-Saharan Africa funded by the Fogarty international center, 2008-2020. BMJ Glob Health 2022;7:e009466. 10.1136/bmjgh-2022-009466 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Rees CA, Lukolyo H, Keating EM, et al. Authorship in paediatric research conducted in low- and middle-income countries: parity or parasitism? Trop Med Int Health 2017;22:1362–70. 10.1111/tmi.12966 [DOI] [PubMed] [Google Scholar]
- 31.Gardner UG, Thompson PS, Burton J, et al. Article processing charge waiver policies as a barrier to oncology scholarship in low- and lower-middle-income countries. JCO Glob Oncol 2021;7:1413–7. 10.1200/GO.21.00143 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Adegnika AA, Amuasi JH, Basinga P, et al. Embed capacity development within all global health research. BMJ Glob Health 2021;6:e004692. 10.1136/bmjgh-2020-004692 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjgh-2022-011053supp001.pdf (499KB, pdf)
bmjgh-2022-011053supp002.pdf (58.2KB, pdf)
Data Availability Statement
All data relevant to the study are included in the article or uploaded as supplementary information.