

Abstract
Objectives
Documenting routine practice is significant for better diagnosis, treatment, continuity of care and medicolegal issues. However, health professionals’ routine practice documentation is poorly practised. Therefore, this study aimed to assess health professionals’ routine practice documentation and associated factors in a resource-limited setting.
Methods
An institution-based cross-sectional study design was used from 24 March up to 19 April 2022. Stratified random sampling and a pretested self-administered questionnaire were used among 423 samples. Epi Info V.7.1 and STATA V.15 software were used for data entry and analysis, respectively. Descriptive statistics and a logistic regression model were employed to describe the study subjects and to measure the strength of association between dependent and independent variables, respectively. A variable with a p value of <0.2 in bivariate logistic regression was considered for multivariable logistic regression. In multivariable logistic regression, ORs with 95% CIs and a p value of <0.05 were considered to determine the strength of association between dependent and independent variables.
Results
Health professionals’ documentation practice was 51.1% (95% CI: 48.64 to 53.1). Lack of motivation (adjusted OR (AOR): 0.41, 95% CI: 0.22 to 0.76), good knowledge (AOR: 1.35, 95% CI: 0.72 to 2.97), taking training (AOR: 4.18, 95% CI: 2.99 to 8.28), using electronic systems (AOR: 2.19, 95% CI: 1.36 to 3.28), availability of standard documentation tools (AOR: 2.45, 95% CI: 1.35 to 4.43) were statistically associated factors.
Conclusions
Health professionals’ documentation practice is good. Lack of motivation, good knowledge, taking training, using electronic systems and the availability of documentation tools were significant factors. Stakeholders should provide additional training, and encourage professionals to use an electronic system for documentation practices.
Keywords: documentation, BMJ health informatics, data management, electronic health records, evidence-based nursing
WHAT IS ALREADY KNOWN ON THIS TOPIC
Although routine practice documentation is a legal obligation and crucial for the continuity of patient care, health professionals’ documentation practices are poor, contain errors that further affect patient outcomes and create distorted health information.
WHAT THIS STUDY ADDS
This study assesses routine practice documentation in resource-limited setting including all types of health professionals, and identify associated factors.
Additionally, whether health professionals’ documentation of education and counselling they give to patients and use an electronic system was assessed.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study is crucial for health policy formulators, planners and implementers to enhance health professionals’ motivation for better documentation practice.
This study may motivate health professionals to use an electronic system for documentation practice as much as possible.
The evidence would serve as input for future similar studies.
Introduction
In routine healthcare practice, evidence about the care and treatment of patients, progress notes, assessments and care plans,1 laboratory tests and results, medication and drug prescription information, patient education and counselling2 are some of the routine practices of health professionals. Therefore, documenting the health professionals’ routine practices are important for various purposes.
Documentation is a standard way of keeping ongoing patient care information. It is the relevant facts of routine health information and patient care plans,3 such as professionals’ evaluation and judgement about the patients, evaluation charts, tests, reports, subjective notes or professionals’ reflections.4
Documenting routine practices is essential for the continuity of patient care, legal defence, reimbursement, communication among healthcare professionals and better patient diagnoses and treatments.5 Maintaining routine practice is part of the health professional obligation. Healthcare facilities’ by-laws or policies should require health professionals to complete patient records.6 Whether the documentation is a paper-based or electronic system, it should be patient-focused, accurate, relevant, clear, permanent, confidential and timely. Electronic patient record systems are better for reducing the time spent on documenting patient information and enhancing the quality of documentation.7
Poor documentation practice affects patient management, continuity of patient care and medicolegal issues, which arise from incomplete and inadequate documentation, lack of accuracy and poor quality.8 It leads to adverse patient outcomes, medication errors and patient deaths.9 Distorted health information may influence health professionals’ decision-making capabilities due to inappropriate and misleading documentation practices.10
Globally, poor communication between health professionals is a reason for medical error and patient mortality.9 Many health professionals’ documentation practice is incomplete, inaccurate and of poor quality. According to evidence from the USA, documentation errors are a cause of at least one death and 1.3 million injuries annually.11 Moreover, health professionals’ documentation practice is inadequate such as 33.3% in Indonesia,12 47% in England13 and 50% in Iran.14
In the low-income and middle-income regions, a qualitative study undertaken in Uganda stated that documentation practice is limited by constraints and poor support from the administration.15 In Ghana, 46% of care is provided, and progress notes are not documented after the first day of patient admission.16 In Nigeria, only 44% of health professionals had good documentation knowledge and practice.17
In Ethiopia, documentation is poorly practised and has been reported as being left undone.3 Health professionals’ documentation practice is 47.8% in the Tigray18 and 37.4%3 in Amhara regions. Surprisingly, 88% of the medication provided has been wrongly documented.19 A study report in the Amhara region states that 87% of the medications had documentation errors.19
Age, sex, experience, income, levels of education, health professionals’ knowledge and attitude,3 12 18 motivation, workload and training about documentation20 are factors associated with routine practice documentation.
Documenting health professionals’ routine activities is valuable for sharing knowledge and learning from history. This has a significant impact on better decision-making and accuracy in patient diagnosis and treatment. As per our literature review, studies have not been undertaken in the current study setting. Few studies in similar settings have been carried out with only nursing as a study participants, education and counselling given to the patient were not assessed. So, assessment documentation practice in both medical and non-medical practices, including all health professionals is crucial. Therefore, this study aimed to determine health professionals’ routine practice documentation and associated factors.
Methods
Study design and period
An institutional-based cross-sectional study design was employed among health professionals working in public health facilities in the Ilu Aba bora Zone, from 24 March up to 19 April 2022.
Study setting
Ilu Aba Bora Zone is found in Southwest Ethiopia. The zone is located 600 km away from Addis Ababa, the capital city of Ethiopia. In the zone, there are 44 total health facilities and 2 hospitals (1 general hospital and 1 referral hospital). The public health facilities provide different health services for more than a million of the population in southwest parts of the country coming from Gambela, Southern Nation Nationality and People’s region.
Study population and eligibility criteria
All healthcare professionals working in the public health facilities of Ilu Aba Bora Zone and those who were found during the data collection period were the sources and study population, respectively. Healthcare professionals who were not permanently employed, those who were not present during the study period and who worked as data clerks were excluded.
Sampling size determination
A sample size (n) was determined by using a single population proportion formula, N=(Za/2)2×P(1−P)/d2, where n=the required sample size, (Za/2)2=the value of standard normal distribution or 1.96, p=the prevalence of documentation practice among health professionals and so the default maximum value of 50% was used for P, d=degree of precision or 0.05. Taking this, the required sample size was calculated to be 384. After adding a 10% non-response rate, a total of 423 healthcare professionals participated in this study.
Sampling producer
A stratified simple random sampling method was used. Due to the limited resources, we have to cover all types of health facilities, we have included two hospitals directly and three randomly selected health centres. Once the sample was stratified based on the types of randomly selected health facilities, the sample was allocated to each stratum proportionally. Then, a simple random sampling technique was used to select the study subjects in each public health facility. The list of health professionals was taken from human resource departments. Accordingly, there are 1043 health professionals from 5 randomly selected health facilities. The sampling procedure has been presented in figure 1.
Figure 1.
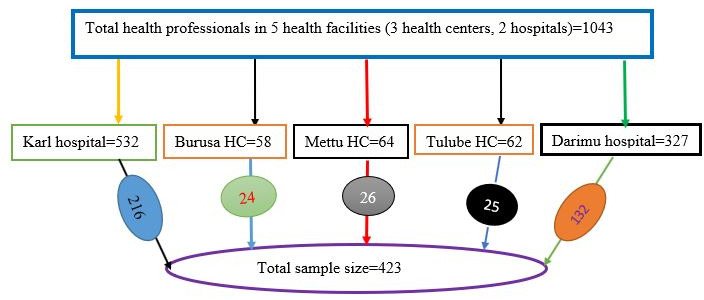
Sampling procedures of study participant selection. HC, health centres.
Operationalisations and measurements
In the healthcare system, patient status, medical diagnoses, planned care, medical interventions or treatments, laboratory tests, result confirmations, medications, patient education and counselling, communication and delivering service are activities of health professionals. All the mentioned activities of health professionals are either medical or non-medical activities (patient education and counselling), but all are routine activities for health professionals. As a result, health professionals use standard documentation tools such as manual records and/or electronic systems to document their routine activities correctly and on time while respecting the rules of ethics.21 Accordingly, health professionals’ routine practice documentation was assessed by using 12 ‘yes’ and ‘no’ questions.3 22 The level of health professionals’ routine practice documentation was determined using the mean value as a cut-off point. Hence, the level of health professionals’ routine practice documentation is good if the score is above or equal to the mean value, and otherwise poor documentation practice.
Knowledge
The study participants’ level of knowledge was measured by using 10 ‘yes’ and ‘no’ options. Health professionals who scored above or equal to the mean score were considered to have good knowledge, and those who scored below the mean value had poor knowledge.3
Attitude
The study participants’ level of attitude was measured by using nine Likert scale questions with responses ranging from 1 ‘strongly agree’ to 5 ‘strongly disagree’.3 18 Health professionals who scored above or equal to the mean score were considered to have a good attitude, otherwise, poor attitude.
Data collection tool and quality assurance
The tool used was developed based on reviewing similar studies.3 18 22 A pretested, self-administered questionnaire was used. Two supervisors and three data collectors received 2 days of intensive training on the study objectives and how to approach study participants. A pretest was done outside the study area with 10% of the study subjects to check the readability and consistency of the questionnaire. The data obtained from the pretest were used to check the validity and reliability of the tool. The Cronbach’s alpha was used to check the reliability of the tool with a value of 83.
Data processing and analysis
The data entry was performed using Epi Info V.7.1 software packages and analysed using STATA V.15 software. Descriptive statistics were computed to describe the sociodemographic characteristics of the healthcare professionals, their knowledge and their attitudes towards routine practice documentation. Bivariable and multivariable binary logistic regression analyses were conducted to measure the association between the dependent and independent variables. In the bivariable regression analysis, variables with a p value of <0.2 were considered for further multivariable logistic regression analysis. The OR with a 95% CI level was assumed to assess the strength of the association between dependent and predictor variables. For all significantly associated variables, a p value <0.05 was used as a cut-off point. A variance inflation factor was performed. Consequently, its value for all predictors was between one and three. This revealed that there was no correlation between the variables. The Hosmer-Lemeshow test was performed to assess the model fitness, and so model was fitted (p=0.271).
Result
Description of study subjects
From 423 participants, 415 responded to a questionnaire with a 98.11% response rate. The mean age of the study subjects was 29.28 (SD±2.21) years with a minimum age of 21 years and a maximum age of 59 years. Half (51.1%) of the study subjects were male. The majority (66.7%) of study subjects were BSc degree holders or below. Of the total respondents, around 6–10 (62.4%) of the study participants had up to 5 years of working experience.
Less than half (32.3%) of the study subjects were trained in routine practice documentation. Of 415 study participants, 235 (56.6%) health professionals earned 4500–7500 Ethiopian Birr per month, and 8–10 (80.2%) health professionals responded that standard documentation tools were available in the working area. One hundred twenty-five (54.22%) health professionals used manual forms for documentation purposes (table 1).
Table 1.
Sociodemographic characteristics of health professionals
| Sociodemographic characteristics | Frequency | Per cent |
| Sex | ||
| Female | 199 | 48.0 |
| Male | 216 | 52.0 |
| Educational status | ||
| Degree and below | 277 | 66.7 |
| Master and above | 138 | 33.3 |
| Age (in years) | ||
| 21–25 | 65 | 15.7 |
| 26–30 | 244 | 58.8 |
| 31–35 | 59 | 14.2 |
| >35 | 47 | 11.3 |
| Month salary (Ethiopian Birr) | ||
| Up to 4500 | 93 | 22.4 |
| Between 4500 and 7500 | 235 | 56.6 |
| >7500 | 87 | 21.0 |
| Experience (in years) | ||
| 1–5 years | 259 | 62.4 |
| Between 6 and 10 years | 88 | 21.2 |
| >10 years | 68 | 16.4 |
| Training for standard documentation tools | ||
| Yes | 134 | 32.3 |
| No | 281 | 67.7 |
| Availability of standard documentation tools | ||
| Yes | 333 | 80.2 |
| No | 82 | 19.8 |
| Types of documentation tools used | ||
| Electronic system | 190 | 45.78 |
| Manual form | 225 | 54.22 |
Health professionals’ routine practice documentation
Overall, 51.1% (95% CI: 46.29% to 53.55%) of health professionals had good routine practice documentation; 6.99% of different laboratory test request forms were not completed and documented; 6.025% of the physicians’ prediagnosis was completed and documented; 5.54% of drug prescription and laboratory result forms were not completed and documented. Documentation incompleteness accounted for 32.52% of health professionals’ poor routine practice documentation (table 2).
Table 2.
Checklists examine health professionals’ routine practice documentation adopted from the Ethiopian health institution reform implementation guidelines
| Sn | Content of items for routine practice documentation | Yes (%) | No (%) |
| 1 | Patients’ admission assessment is documented or attached for the patient admitted | 17 (4.10) | 13 (3.13) |
| 2 | Physicians’ prediagnosis is completed and documented | 14 (3.37) | 25 (6.02) |
| 3 | Different laboratory test request forms completed and documented | 19 (4.58) | 29 (6.99) |
| 3 | The nursing care plan is completed and attached to the patient’s card | 28 (6.75) | 15 (3.61) |
| 4 | Laboratory request accepted and attached to patient card | 21 (5.06) | 14 (3.37) |
| 5 | Laboratory results from filling out (completed) and documented | 15 (3.61) | 23 (5.54) |
| 6 | Laboratory results attached to patient cards | 12 (2.90) | 11 (2.65) |
| 7 | Final diagnosis and treatment results documented | 10 (2.41) | 24 (5.78) |
| 9 | Drug prescription forms completed and documented | 20 (4.82) | 23 (5.54) |
| 10 | Maternal and child health service forms completed and documented | 22 (5.30) | 12 (2.89) |
| 11 | Follow-up form (form for chronic patients) completed and documented | 18 (4.34) | 8 (1.93) |
| 12 | Progress report documented including education and counselling given to the patients | 16 (3.86) | 6 (1.45) |
| Overall health professionals’ routine practice documentation | 212 (51.1) | 203 (48.9) |
Factors associated with routine practice documentation
Bivariate and multivariate logistic regressions were used to measure the association between dependent and independent predictors. In the bivariate logistic regression, p<0.2 was used and sex, age, training, knowledge, attitude, types of documentation tools, availability of standard documentation tools, workload and motivation of study subjects were the candidate variables for the multivariable regression analysis. In the multivariable regression model, knowledge, training, motivation, types and availability of the standard documentation tools were significant factors for routine practice documentation (table 3).
Table 3.
Bivariate and multivariate analysis of factors associated with health professionals’ routine practice documentation (n=415)
| Variables | Routine practice documentation | OR (95% CI) | ||||
| Poor practice | Good practice | COR (95% CI) | AOR (95% CI) | |||
| n | % | n | % | |||
| Sex | ||||||
| Male | 107 | 25.80 | 103 | 24.80 | 0.95 (0.65 to 1.40)* | 0.93 (0.60 to 1.44) |
| Female | 96 | 23.10 | 109 | 26.30 | 1 | 1 |
| Knowledge | ||||||
| Good | 123 | 29.64 | 148 | 35.66 | 1.50 (1.00 to 2.26)* | 1.35 (0.72 to 2.97)† |
| Poor | 80 | 19.28 | 64 | 15.42 | 1 | 1 |
| Age (in years) | ||||||
| 26–30 | 120 | 28.92 | 124 | 29.88 | 0.83 (0.48 to 1.44)* | 1.10 (0.58 to 2.08) |
| 31–35 | 23 | 5.54 | 36 | 8.67 | 1.26 (0.62 to 2.58) | 1.20 (0.52 to 2.77) |
| >35 | 31 | 7.47 | 16 | 3.86 | 0.42 (0.19 to 0.90) | 0.51 (0.21 to 1.34) |
| 21–25 | 29 | 6.99 | 36 | 8.67 | 1 | 1 |
| Motivation | ||||||
| No | 171 | 41.21 | 163 | 39.28 | 0.62 (0.38 to 1.02)* | 0.41 (0.22 to 0.76)† |
| Yes | 32 | 7.71 | 49 | 11.80 | 1 | 1 |
| Attitude | ||||||
| Good | 165 | 39.76 | 182 | 43.86 | 1.40 (0.83 to 2.36)* | 1.09 (0.71 to 2.04) |
| Poor | 38 | 9.15 | 30 | 7.23 | 1 | 1 |
| Training on documentation | ||||||
| Yes | 32 | 7.71 | 102 | 24.57 | 4.96 (3.12 to 7.88)* | 4.18 (2.99 to 8.28)† |
| No | 171 | 41.21 | 110 | 26.51 | 1 | 1 |
| Availability of documentation sheet | ||||||
| Yes | 147 | 35.42 | 186 | 44.82 | 2.73 (1.63 to 4.55)* | 2.45 (1.35 to 4.43)† |
| No | 56 | 13.50 | 26 | 6.26 | 1 | 1 |
| Types of tool used for documentation | ||||||
| Electronic system | 119 | 28.67 | 80 | 19.28 | 2.34 (1.58 to 3.47)* | 2.19 (1.36 to 3.28)† |
| Manual form | 84 | 20.24 | 132 | 31.81 | 1 | 1 |
| Workload | ||||||
| Yes | 130 | 31.33 | 151 | 36.39 | 0.67 (0.33 to 1.36)* | 0.48 (0.21 to 1.10) |
| No | 64 | 15.42 | 70 | 16.86 | 1 | 1 |
Reference category=1.
*Significant in COR.
†Significant in AOR.
AOR, adjusted OR; COR, crude OR.
Health professionals who lack motivation were 59% (adjusted OR (AOR): 0.41, 95% CI: 0.22 to 0.76) less likely to document routine practices. Health professionals who had good knowledge of routine practice documentation were 1.4 (AOR: 1.35, 95% CI: 0.72 to 2.97) times more likely to document routine practice than those who had poor knowledge. Health professionals who were trained in routine practice documentation were 4.2 (AOR: 4.18, 95% CI: 2.99 to 8.28) times more likely to document routine practices than those who were not trained. Health professionals who used electronic systems for routine practice documentation were 2.2 (AOR: 2.19, 95% CI: 1.36 to 3.28) times more likely to document their routine practices than those who used manual forms for documentation. The availability of standard documentation tools were 2.5 (AOR: 2.45, 95% CI: 1.35 to 4.43) times more odds for health professionals to document their routine practices (table 3).
Discussion
This study assesses health professionals’ routine practice documentation and associated factors. Health professionals who had good knowledge about routine practice documentation, training on documentation, using electronic systems for documentation, the availability of standard documentation tools and a lack of motivation towards routine practice documentation were statistically significant factors associated with health professionals’ routine practice documentation.
The study revealed that health professionals’ routine practice documentation was good (51.1%). This finding is higher than previous similar studies, which found 44.2% in Nigeria,17 33.3% in Indonesia12 and 37.4%–48.8% in different parts of Ethiopia.3 18 23 However, the finding is lower than the study done in Jamaica, which reports that health professionals’ documentation practice is 98%.24 This might be due to the utilisation of technologies such as the electronic medical record and district health information system V.2 (DHIS2), the accessibility of required tools for documentation and health professionals’ good commitment to using DHIS2 data.19 Additionally, this variation might be due to the information difference, the time gap between studies, the high patient flow, the shortage of time and the workload of health professionals.
Health professionals who lack motivation were 59% less likely to have documentation practices when compared with those who had gained motivation. This finding is inconsistence with studies done in Ethiopia.23 25 This might be poor professional encouragement, poor financial support, less opportunities for further educational development, poor infrastructures and low hospital management support.25
Health professionals for whom standard documentation tools were available were 2.5 times more likely to document routine practices than those for whom standard documentation tools were not available. This finding is consistence with a study done in Australia,26 Tigray18 and Amhara regions.23 This might be due to familiarisation with standard documentation sheets, and the accessibility of integrated routine health information forms for recording and reporting.27
Health professionals who had good knowledge of routine practice documentation were more likely to document their routine practice. This result is supported by studies done in Ethiopia,3 the USA28 and Australia.29 This might be due to health professionals’ familiarity with documentation guidelines and manual forms that improve health professionals’ knowledge of routine practice documentation.3 Additionally, the reason might be that health professionals understand the importance of documenting routine practice, the viability of reading materials, know that record-keeping is required for medicolegal issues and have good competency in the area of documentation.29 Moreover, spending on documentation courses may promote health professionals’ knowledge.30
Health professionals who were trained in routine practice documentation were 4.2 times more likely to document routine practices than those who were not trained. This evidence is supported by studies done in Ethiopia3 and Iran.30 This might be due to training, which might enhance health professionals’ knowledge and motivation for documentation and provide team-based learning, intrapersonal skills sharing and consultation gained from colleagues. Plus, training may force health professionals to develop a positive attitude towards routine practice documentation.3
Health professionals who used electronic systems for routine practice documentation were 2.2 times more likely to document their routine practices than those who used manual forms. This study is supported by a study done in Ethiopia20 and a study done about maintaining practices and record-keeping.1 This might be due to the capability of electronic systems to reduce the time spent documenting patient care.7 Additionally, record-keeping in the light of recent public inquiries, national interests in shifting from paper to digital storage of data, the capability of electronic health records to generate a complete record of an episode of care and the longitudinal nature of the electronic system might be possible reasons.1 Moreover, a need for real-time access to health information when and where it is needed might be reason why an electronic system could be more likely to be good for documentation.23
Strength and limitation
Since the data were collected at a specific time, social desirability bias may occur. Significant variables may have a temporal relationship. This study assesses the use of electronic systems for documentation as an independent variable. All health professionals were included, and documentation regarding education and counselling was assessed. Hence, the finding is unique as compared with previous studies. Moreover, the mean value was used as a cut-off point to determine level of health professionals’ routine practice documentation to consider the weighted average values.
Conclusions
In this study, health professionals have good routine practice documentation. Knowledge, training, using an electronic system, availability of standard documentation tools and lack of motivation are statistically significant factors for routine practice documentation. Health policy formulators and stakeholders give additional training to health professionals, and encourage them to use an electronic system for documentation. Stakeholders should improve health professionals’ knowledge and motivation of routine practice documentation. Additional high-quality studies are required on a similar topic.
Footnotes
Contributors: AWD had made a substantial contribution in writing the conception, designing the study, analyzing the data, and discussing the findings. SYK and ATD were involved in drafting the manuscript and interpreting the results. AAC and HSN had revised the manuscript. MKH, AAS, ADW, and MDE all made significant contributions to revising the manuscript, and managing the data. All authors read and approved the final manuscript submission for publication.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data availability statement
All the data generated and analysed during this study are included, in the table and text form, in this article. If required, the data will be available on request from the corresponding author. Not applicable.
Ethics statements
Patient consent for publication
Not applicable.
Ethics approval
Ethics approval was obtained from the Institutional Review Committee of the health science college of Mettu University with reference number ARcsu/271/24. Informed verbal and written consent from the study participant was obtained.
References
- 1.Beach J, Oates J. Maintaining best practice in record-keeping and documentation. Nurs Stand 2014;28:45–50. 10.7748/ns2014.05.28.36.45.e8835 [DOI] [PubMed] [Google Scholar]
- 2.Seetharama S. Information generation and utilisation in hospitals: an analytical study. SRELS Journal of Information Management 1980;17:10–8. [Google Scholar]
- 3.Kebede M, Endris Y, Zegeye DT. Nursing care documentation practice: the unfinished task of nursing care in the University of gondar Hospital. Inform Health Soc Care 2017;42:290–302. 10.1080/17538157.2016.1252766 [DOI] [PubMed] [Google Scholar]
- 4.Akhu-Zaheya L, Al-Maaitah R, Bany Hani S. Quality of nursing documentation: paper-based health records versus electronic-based health records. J Clin Nurs 2018;27:e578–89. 10.1111/jocn.14097 [DOI] [PubMed] [Google Scholar]
- 5.Bargaje C. Good documentation practice in clinical research. Perspect Clin Res 2011;2:59–63. 10.4103/2229-3485.80368 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Singh P, John S. Analysis of health record documentation process as per the national standards of accreditation with special emphasis on tertiary care hospital. Int J Health Sci Res 2017;7:286–92. [Google Scholar]
- 7.Kent P, Morrow K. Better documentation improves patient care. Nurs Stand 2014;29:44–51. 10.7748/ns.29.14.44.e9267 [DOI] [PubMed] [Google Scholar]
- 8.Considine J, Trotter C, Currey J. Nurses’ documentation of physiological observations in three acute care settings. J Clin Nurs 2016;25:134–43. 10.1111/jocn.13010 [DOI] [PubMed] [Google Scholar]
- 9.Collins SA, Cato K, Albers D, et al. Relationship between nursing documentation and patients’ mortality. Am J Crit Care 2013;22:306–13. 10.4037/ajcc2013426 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lewandowsky S, Ecker UKH, Seifert CM, et al. Misinformation and its correction: continued influence and successful debiasing. Psychol Sci Public Interest 2012;13:106–31. 10.1177/1529100612451018 [DOI] [PubMed] [Google Scholar]
- 11.Krishna R, Khyati G. Nursing errors in the documentation: a review. Ruas-Uas JMC 2017;3:1–5. [Google Scholar]
- 12.Motea P, Rantetampang A, Pongtikuc A. The factor relates to the job performance of nurses with health nursing documentation at paniai general hospital papuan province. Int J Sci Basic Appl Res (IJSBAR) 2016;30:231–47. [Google Scholar]
- 13.Ball JE, Murrells T, Rafferty AM, et al. “ care left undone ” during nursing shifts: associations with workload and perceived quality of care. BMJ Qual Saf 2014;23:116–25. 10.1136/bmjqs-2012-001767 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Torki S, Tavakoli N, Khorasani E. Improving the medical record documentation by quantitative analysis in a training Hospital. J Earth Environ Health Sci 2015;1:22. 10.4103/2423-7752.159923 [DOI] [Google Scholar]
- 15.Nakate GM, Dahl D, Petrucka P, et al. The nursing documentation dilemma in uganda: neglected but necessary. A case study at mulago national referral hospital. OJN 2015;05:1063–71. 10.4236/ojn.2015.512113 [DOI] [Google Scholar]
- 16.Avoka Asamani J, Delasi Amenorpe F, Babanawo F, et al. Nursing documentation of inpatient care in eastern Ghana. Br J Nurs 2014;23:48–54. 10.12968/bjon.2014.23.1.48 [DOI] [PubMed] [Google Scholar]
- 17.Oseni OM, Adejumo PO. Nurses’ reported practice and knowledge of wound assessment, assessment tools and documentation in a selected hospital in Lagos, Nigeria. Afr J Med Med Sci 2014;43:149–57. [PubMed] [Google Scholar]
- 18.Tasew H, Mariye T, Teklay G. Nursing documentation practice and associated factors among nurses in public hospitals, tigray, ethiopia. BMC Res Notes 2019;12:612. 10.1186/s13104-019-4661-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Feleke SA, Mulatu MA, Yesmaw YS. Medication administration error: magnitude and associated factors among nurses in ethiopia. BMC Nurs 2015;14:53. 10.1186/s12912-015-0099-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Semachew A. Implementation of nursing process in clinical settings: the case of three governmental hospitals in ethiopia, 2017. BMC Res Notes 2018;11:173. 10.1186/s13104-018-3275-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.WHO . Guide for documenting and sharing best practices in health programmes. 2008. Available: https://www.afro.who.int/sites/default/files/2017-06/Guide_for_documenting_and_Sharing_Best_Practice_-_english_0.pdf
- 22.Andualem A, Asmamaw T, Sintayehu M, et al. Knowledge, attitude, practice and associated factors towards nursing care documentation among nurses in west gojjam zone public hospitals, amhara ethiopia, 2018. Clin J Nurs Care Pract 2018;3:001–13. 10.29328/journal.cjncp.1001010 [DOI] [Google Scholar]
- 23.Kasaye MD, Beshir MA, Endehabtu BF, et al. Medical documentation practice and associated factors among health workers at private hospitals in the amhara region, ethiopia 2021. BMC Health Serv Res 2022;22:465. 10.1186/s12913-022-07809-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Blake-Mowatt C, Lindo JLM, Bennett J. Evaluation of registered nurses’ knowledge and practice of documentation at a Jamaican Hospital. Int Nurs Rev 2013;60:328–34. 10.1111/inr.12040 Available: http://doi.wiley.com/10.1111/inr.2013.60.issue-3 [DOI] [PubMed] [Google Scholar]
- 25.Dagne T, Beyene W, Berhanu N. Motivation and factors affecting it among health professionals in the public hospitals, central ethiopia. Ethiop J Health Sci 2015;25:231–42. 10.4314/ejhs.v25i3.6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Tower M, Chaboyer W, Green Q, et al. Registered nurses’ decision-making regarding documentation in patients’ progress notes. J Clin Nurs 2012;21:2917–29. 10.1111/j.1365-2702.2012.04135.x [DOI] [PubMed] [Google Scholar]
- 27.Hansen RL, Fossum M. Nursing documentation of pressure ulcers in nursing homes: comparison of record content and patient examinations. Nurs Open 2016;3:159–67. 10.1002/nop2.47 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Keenan GM, Yakel E, Tschannen D, et al. Documentation and the nurse care planning process. patient safety and quality: an evidence-based handbook for nurses. 2008. [PubMed]
- 29.Daskein R, Moyle W, Creedy D. Aged-care nurses’ knowledge of nursing documentation: an australian perspective. J Clin Nurs 2009;18:2087–95. 10.1111/j.1365-2702.2008.02670.x [DOI] [PubMed] [Google Scholar]
- 30.Ghazanfari Z, Sheykhpour-Khani M, Haghdoost A-A. Nurse’s knowledge and practice of the principles of nursing documentation at hospitals of kerman university of medical sciences. Iran Journal of Nursing 2009;22:15–22. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All the data generated and analysed during this study are included, in the table and text form, in this article. If required, the data will be available on request from the corresponding author. Not applicable.