

Abstract
Introduction
During the COVID-19 pandemic, an accelerated uptake of remote monitoring strategies, replacing traditional face-to-face care, has been observed. However, data on the effects of remote care interventions for patients with rheumatic and musculoskeletal diseases remain scarce and interpretation is hampered by study heterogeneity and research quality concerns. High-quality evidence is required to guide future implementation in clinical practice, with health economic analyses identified as an important knowledge gap. Randomised controlled trials (RCTs) comparing telemonitoring with conventional care for patients with spondyloarthritis (SpA) are currently lacking.
Methods and analysis
TeleSpA is a pragmatic, multicentre RCT investigating the effectiveness and cost-effectiveness of combined asynchronous telemonitoring and patient-initiated follow-up for patients with SpA, compared with conventional care. Two-hundred patients will be recruited at two hospitals and randomised (1:1) to the study intervention or standard care. The primary endpoint is a reduction in the number of follow-up visits by ≥25% in the intervention compared with standard care group, during a 1-year period. Secondary endpoints are (a) non-inferiority of the study intervention with regard to health outcomes, quality of care and patient-reported experience with care; and (b) cost-effectiveness of the intervention, evaluated through a prospective trial-based cost-utility analysis. In addition, experiences with the study intervention will be assessed among patients and healthcare providers, and factors associated with primary and secondary endpoints will be identified.
Ethics and dissemination
This study was approved by the Medical Research Ethics Committee of the Academic Hospital Maastricht/Maastricht University (NL71041.068.19/METC 19-059). Results will be disseminated through publications in peer-reviewed journals and conference presentations.
Trial registration number
Keywords: Telemedicine, HEALTH ECONOMICS, Organisation of health services, Rheumatology, RHEUMATOLOGY
STRENGTHS AND LIMITATIONS OF THIS STUDY.
To our knowledge, TeleSpA is the first randomised controlled trial to investigate the effectiveness of asynchronous telemonitoring combined with patient-initiated care in patients with spondyloarthritis.
Pragmatic and multicentre trial design, augmenting the reliability of inferences regarding feasibility of the study intervention in a real-life care setting.
A prospective trial-based cost-effectiveness analysis, using health utilities obtained through both generic and disease-specific outcome measures, will balance (savings in) costs against health outcomes and address an important knowledge gap in the field of telemedicine.
The follow-up period of 1 year does not allow investigating long-term effects.
Limited sample size for patient-reported experience with care, reducing statistical power for this secondary outcome.
Introduction
Spondyloarthritis (SpA) represents a group of inter-related, chronic rheumatic diseases comprising axial SpA (including radiographic and non-radiographic axial SpA), arthritis associated with psoriasis (psoriatic arthritis (PsA)), arthritis associated with inflammatory bowel disease (IBD), reactive arthritis and undifferentiated SpA. Symptoms typically start in the third decade of life and can involve inflammatory back pain, arthritis, dactylitis and enthesitis as well as extramusculoskeletal manifestations that include psoriasis, IBD and uveitis. Based on clinical features and the pattern of joint involvement, patients can be classified as having ‘axial SpA’ when inflammation primarily affects the spine and/or sacroiliac joints, or ‘peripheral SpA’ in case of predominant peripheral joint involvement.1
SpA is estimated to affect 1% of the population worldwide, but prevalence varies widely in different regions and populations.2 3 In many patients, the disease follows a chronic disabling course, leading to a lower quality of life, absenteeism and work disability. Combined with the financial cost of a lifelong need for specialised health services and antirheumatic therapies, this carries a substantial socioeconomic burden for countries across the globe.4–7
Current management guidelines emphasise the importance of individualised care and regular monitoring, ideally incorporating a specific set of evaluations including patient-reported outcome measures (PROMs) and validated measures of disease activity.8 9 In particular, recommended/emerging ‘treat-to-target’ and tight disease-control strategies require more frequent monitoring and systematic assessment of composite disease activity scores.9–11 Furthermore, as part of good clinical practice in general, care provided should not only be effective and safe, but also timely, efficient, equitable and patient-centred—incorporating patients’ preferences, needs and values.12
Complying with these recommendations poses important challenges in daily practice. First, many rheumatology clinics currently face capacity issues due to an increasing demand for health services and a shortage of rheumatologists, an imbalance that is expected to grow in the coming decade.13 14 As a result, waiting lists and difficulties in providing timely access to care in case of fluctuating disease activity or side-effects threaten to compromise the quality of care.15 16 At the same time, traditional physician-driven monitoring strategies may lead to patients repeatedly presenting for routine outpatient follow-up when they are feeling well and specialist review is unlikely to result in clinical actions. Both patients and clinicians may find such visits unnecessary or inefficient.17–19 Finally, despite well-recognised benefits in terms of patient-centredness, the implementation and impact of routine registration of PROMs are limited by a lack of integrated instruments, non-disease-specific tools and time constraints.20–22
With healthcare expenditure and workforce shortages projected to increase, finding sustainable solutions for these issues is paramount but most countermeasures require years to accomplish due to regulatory barriers and the length of medical educations.16 23 24 Meanwhile, improving healthcare efficiency may safeguard access to care for rheumatology outpatients, ameliorate workflow management for medical staff and potentially decrease costs. More recently, the COVID-19 pandemic abruptly necessitated rheumatologists worldwide to adopt alternative ways of care delivery to reduce or replace physical encounters in order to mitigate the risk of SARS-CoV-2 transmission among vulnerable patient populations.25 This caused a surge of interest in digital health applications and telemedicine with a rapid uptake of alternative follow-up strategies, some of which can potentially contribute towards reducing patient–caregiver contacts in the long term.
Prior to the pandemic, data from several randomised controlled trials (RCTs) already indicated that telemonitoring could be a promising alternative to face-to-face care for rheumatology patients, but the evidence remains limited and validity of conclusions is uncertain due to methodological bias and study heterogeneity.26 27 Specifically, ‘asynchronous’ telehealth solutions that facilitate self-monitoring for patients without relying on real-time interactions with healthcare providers may reduce the number of necessary follow-up appointments while maintaining disease control and patient safety, as demonstrated in rheumatoid arthritis (RA) and IBD.28–31
Favourable experiences with telemedicine supported by electronic PROMs (ePROMs) have since been reported for patients with rheumatic diseases during the pandemic, yet this exclusively constitutes qualitative research or retrospective observational data from provisional care interventions in times of crisis, rendering the validity of study findings uncertain beyond this context.32–34 Before a more definitive shift away from traditional follow-up paradigms can be justified in a usual care setting, more high-quality RCTs comparing telemonitoring with routine care for specific disease entities in terms of disease control, equity of care and patient satisfaction are required, with a lack of economic analyses additionally identified as a specific knowledge gap.26 35 36
Multiple RCTs in RA also illustrated that regular follow-up planning by rheumatologists is not necessary, but can be at the discretion of the patient or general practitioner.18 37–39 Already before the upsurge of telehealth, patient-initiated follow-up (PIFU) has been shown to reduce healthcare resource utilisation, improve self-efficacy and increase satisfaction compared with the traditional pre-booked appointment system.18 38 39 In RA, PIFU resulted in similar improvements in disease activity compared with traditional appointments.37 Furthermore, two RCTs in RA and one RCT among patients with RA and PsA treated with methotrexate indicated that self-monitoring combined with PIFU can reduce healthcare utilisation while maintaining clinical and psychological well-being.30 40 41 Apart from the latter study, no RCTs are available on PIFU nor the effect of telemonitoring on disease activity, resource utilisation or associated costs among patients with SpA.
Since 2016, a disease-specific web-based eHealth system for patients with SpA (‘SpA-Net’) has been used in the Netherlands that allows for remote collection of ePROMs during everyday practice. The development, usability and acceptability of SpA-Net have been described elsewhere.42 We hereby provide the protocol for a pragmatic multicentre RCT, in which remote care (asynchronous telemonitoring) provided through SpA-Net combined with PIFU will be compared with standard care, aiming at more efficient care. The trial will test the hypothesis that asynchronous telemonitoring, combined with PIFU, can reduce the number of outpatient consultations for patients with SpA compared with standard care without compromising health outcomes (disease activity, physical functioning, health-related quality of life), patient experience with care and quality of care. Concomitantly, a trial-based cost-utility analysis is conducted to detect between-group differences in healthcare utilisation and associated healthcare and societal costs, and to examine cost-effectiveness of the study intervention. In addition, experiences with the study intervention and SpA-Net are assessed among patients and healthcare providers.
Methods and analysis
Study design and setting
This is a multicentre, pragmatic RCT, completed with a trial-based cost-utility analysis. The study will be conducted at two participating hospitals, located in different geographical regions in the Netherlands: the Maastricht University Medical Centre+ (MUMC+), an academic hospital and referral centre for SpA care, and Medisch Spectrum Twente, a large non-academic teaching hospital.
Population and recruitment
Patients will be recruited at the rheumatology outpatient clinics in both participating centres. All patients with a scheduled outpatient visit and considered eligible by their treating rheumatologist with respect to the inclusion and exclusion criteria (box 1) will receive an invitation letter and information brochure explaining the study, 1–4 weeks before the next visit.
Box 1. Inclusion and exclusion criteria.
Inclusion criteria:
Age ≥18 years.
Diagnosis of axial and/or peripheral spondyloarthritis according to treating rheumatologist.
Disease duration ≥2 years, in order to be familiar with signs, symptoms and medication.
Stable disease, defined as being in an acceptable symptom state according to patient,46 AND treating rheumatologist AND no changes to treatment expected in the next 3 months.
Access to a computer, tablet and/or smartphone for the entire duration of the study.
Exclusion criteria:
Insufficient mastery of the Dutch language.
Lacking capacity to provide informed consent.
Limited life expectancy (eg, terminal illness).
Ongoing (or planned) pregnancy during the study period, as this might affect treatment, follow-up planning and healthcare resource use.
Patients participating in other research project(s), with an exception for strictly observational studies that do not entail additional healthcare utilisation and/or absence from paid work.
Patients can communicate their willingness to participate before (by mail, email or telephone) or during the scheduled outpatient visit. Inclusion and exclusion criteria will be checked by the attending rheumatologist during the visit, after which a researcher confirms eligibility and verifies whether information is understood before signing the informed consent form (ICF). Upon the patients’ request, signing of the ICF can be postponed by 1 week to provide additional time for consideration. For patients who refuse to participate or do not respond, age, sex, diagnosis, educational level and reasons for non-participation (when disclosed) will be collected.
Study objectives
Primary objective
To determine whether asynchronous telemonitoring combined with PIFU (ie, the study intervention) leads to fewer outpatient visits compared with standard care.
Secondary objectives
To confirm that the study intervention does not compromise perceived quality of care and health outcomes compared with standard care.
To evaluate how changes in healthcare and societal costs will relate to changes in overall preferences for health (health utility).
To assess experiences with care and SpA-Net among patients and to compare these between the two study groups.
To assess experiences with the study intervention and SpA-Net among healthcare providers.
To determine whether self-management skills are important for successful (ie, reducing the number of outpatient visits without compromising quality of care or health outcomes) application of the study intervention.
Randomisation
Patients are randomised after signing the ICF subsequent to their scheduled visit, which will then be considered the baseline visit. Randomisation (1:1; intervention vs standard care) is performed by the web-based software program ALEA using the minimisation method described by Pocock and Simon,43 designed to minimise imbalance between treatment groups on predefined prognostic factors, while incorporating a random component to limit predictability in compliance with the International Conference on Harmonisation (ICH) E9 guidelines.44 On randomisation, medical centre, SpA subtype (axial, peripheral or combined) and treatment (biological vs no biological) are taken into account. When the highest imbalance between groups for any of these factors exceeds 2, an OR of 0.9 is assigned to the group allocation resulting in the lowest imbalance. Due to the nature of the intervention, neither patients nor clinicians can be blinded to the group allocation.
SpA-Net
SpA-Net has been described extensively elsewhere.42 Briefly, it is an ongoing, disease-specific, prospective web-based registry for monitoring SpA in daily practice. Clinical characteristics, outcome measures, results of clinical examinations and laboratory investigations are collected in SpA-Net at every outpatient visit (an example for enthesitis is shown in figure 1). Results over time are graphically visualised in a dashboard, using colour coding to aid quick interpretation (figure 2). These comprehensive up-to-date individual patient data are readily available to the healthcare provider during consultations, and an excerpt of this for patients (figure 3), facilitating informed treatment decision-making.
Figure 1.
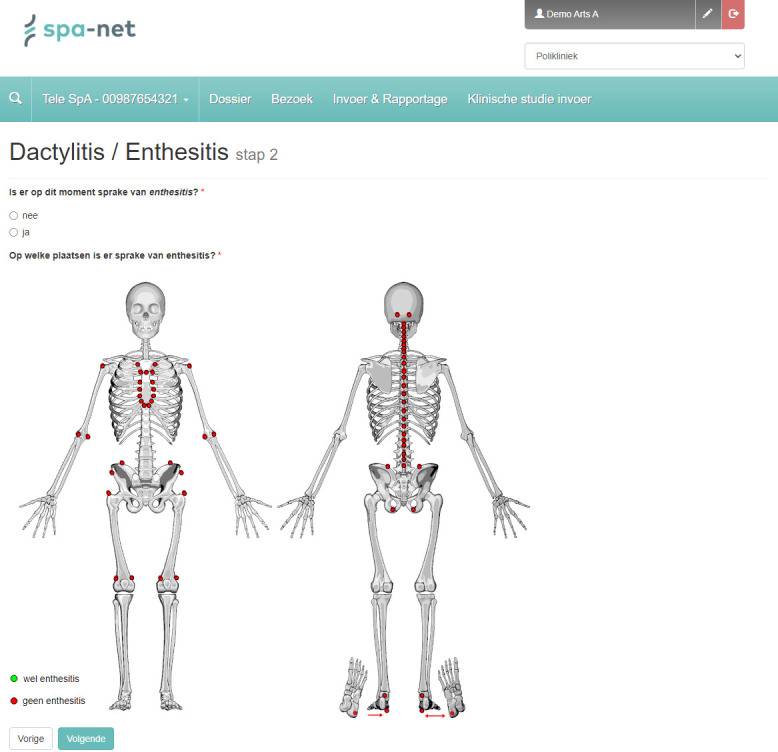
Example of data entry in SpA-Net for healthcare providers. If signs of enthesitis are present, healthcare providers can specify the affected entheses in SpA-Net.
Figure 2.
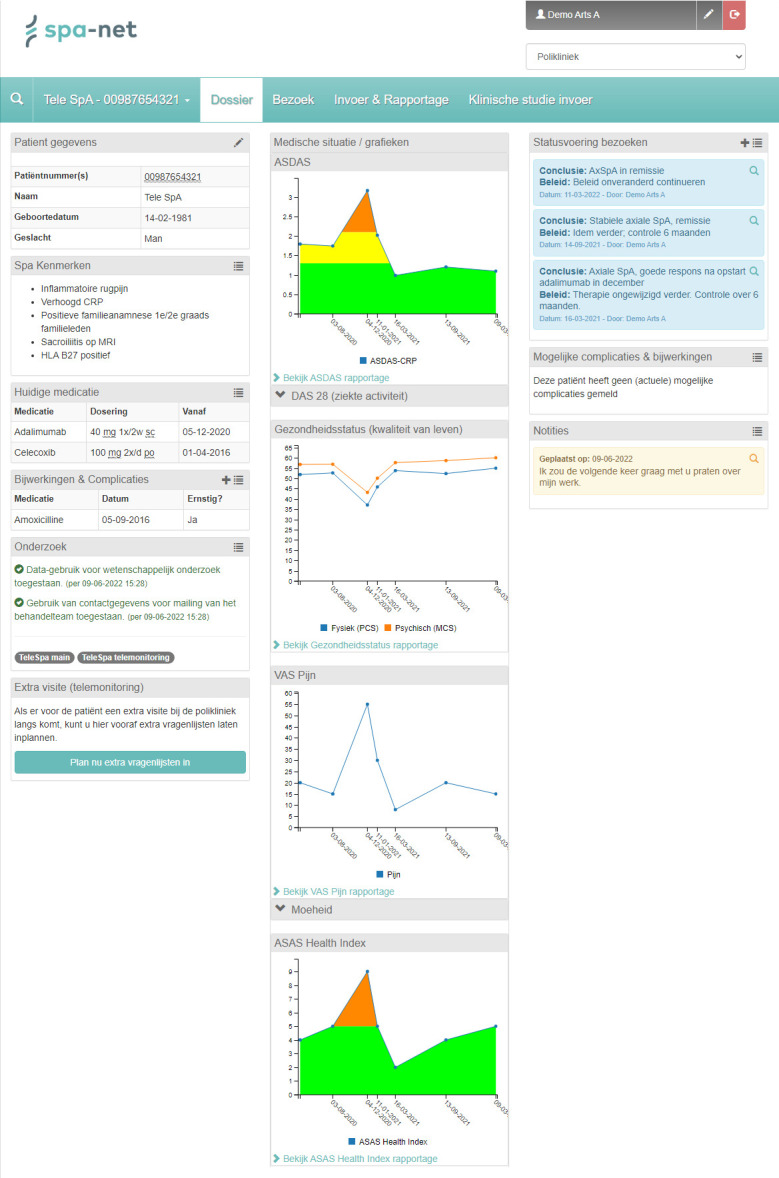
Example of SpA-Net interface for healthcare providers. For healthcare providers, the SpA-Net dashboard environment is divided into three columns. The first column displays patients’ personal information, presence or history of SpA features, current medication and history of medication-related adverse events. The second column contains graphical summaries of the following ePROMs and disease activity measures: ASDAS, SF-36, VAS Pain, VAS Fatigue (accessible in a drop-down box ‘˅’), ASAS Health index. The third column contains summaries of most recent visits, complications or side-effects reported by patients and patient’s notes or questions. ASAS, Assessment of SpondyloArthritis International Society; ASDAS, Ankylosing Spondylitis Disease Activity Score; CRP, C reactive protein; ePROMs, electronic patient-reported outcome measures; MCS, SF-36 Mental Component Scale; PCS, SF-36 Physical Component Scale; SF-36, 36-Item Short-Form Health Survey; SpA, spondyloarthritis; VAS, Visual Analogue Scale.
Figure 3.
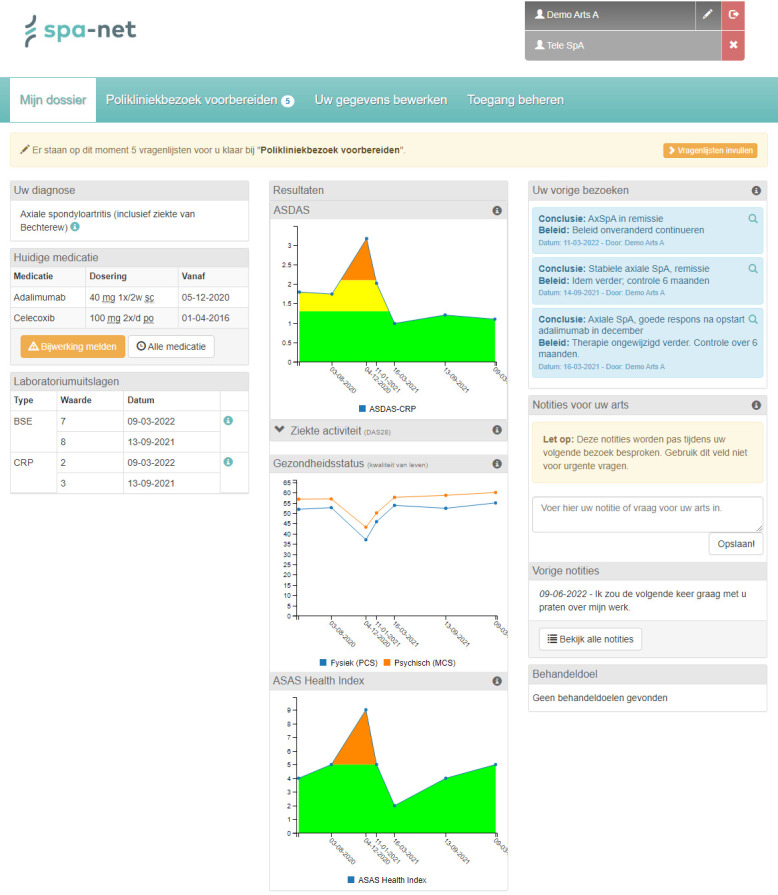
Example of SpA-Net interface from the patient’s perspective. A horizontal notification bar (in yellow) allows patients to quickly access questionnaires as soon as these become available. Below, information is presented in three columns. The first column displays the patient’s diagnosis, current medication (with an additional feature to report side-effects) and recent laboratory results. The second column includes multiple graphs depicting results from questionnaires. The third column displays summaries of the rheumatologist’s notes regarding the most recent outpatient visits, and offers a space where patients can leave questions or notes for their healthcare provider or set personal treatment goals. Lay-term explanations for all items in these three columns are available through an information icon (lower case ‘i’). ASAS, Assessment of SpondyloArthritis International Society; ASDAS, Ankylosing Spondylitis Disease Activity Score; BSE, erythrocyte sedimentation rate; CRP, C reactive protein; MCS, SF-36 Mental Component Scale; PCS, SF-36 Physical Component Scale; SF-36, 36-Item Short-Form Health Survey.
Study intervention and procedures
All participants will have a scheduled outpatient visit at baseline and after 1 year. In the standard care group, additional follow-up visits are scheduled at the discretion of the treating rheumatologist. Before each visit, patients complete questionnaires in SpA-Net and routine blood tests (including C reactive protein) are obtained as per standard care at the respective study site. During the visit, clinical examination by a rheumatologist or specialised rheumatology nurse will take place.
In the intervention group, no additional pre-booked appointments are provided. Instead, ‘remote monitoring’ will take place after 6 months. Two weeks prior to the planned remote monitoring, these patients will receive a reminder email to complete questionnaires in SpA-Net and to have routine blood tests. Rheumatologists receive an automated email notification as soon as all questionnaires have been answered. Responses to questionnaires and laboratory results are subsequently reviewed by the rheumatologist. Rheumatologists’ notes are visible to patients and, at minimum, need to include a summarised interpretation of the patient’s results as well as a treatment and follow-up plan. If needed, a physical visit or telephone consultation can be planned (on request via SpA-Net, telephone or email) by the patient, replacing the remote monitoring procedure, or by the rheumatologist when specialist review or treatment changes are indicated based on the results of ePROMs, disease activity measures and/or blood tests.
Patients in both groups will be instructed that at any time, extra ‘direct access’ visits (provided within 7 days) can be scheduled in case of disease flares or therapy-related side-effects as part of the study project. In this study, no investigational medicinal products are used. All patients receive treatment as indicated from their treating rheumatologists, in accordance with current management recommendations.8 9 45
Outcome measures
Information on the number of outpatient visits in the year prior to and during the study period will be collected from the electronic medical file. In SpA-Net, multiple variables are routinely measured in regular care (table 1). Additionally for the TeleSpA Study, all included patients will complete questionnaires on whether their symptom state is acceptable,46 experience with care (patient-reported experience measure (PREM), assessing overall experience with care and specific aspects including timeliness, emotional support, patient-centredness and safety),47 a Self-Management Screening (SeMaS),48 and questionnaires on health resource utilisation, work productivity, unpaid productivity loss, medication adherence, disease flares (self-reported) and experience with SpA-Net (general satisfaction, ease of use, added value) (see online supplemental file 1).
Table 1.
List of variables and questionnaires collected throughout the study
| Variable | Baseline | 6 months* | 1 year* | Extra visits† |
| Demographics‡ | X | X | ||
| Lifestyle (smoking, alcohol use)‡ | X | X | ||
| Educational level‡ | X | |||
| Work status‡ | X | X | ||
| Diagnosis according to rheumatologist‡ | X | |||
| Symptom duration‡ | X | |||
| Presence or history of SpA features‡ | X | X§ | X | X |
| Comorbidities‡ | X | X§ | X | X |
| Number of outpatient visits in previous year | X | X | ||
| Medication use (NSAID, DMARD, biological)‡ | X | X | X | X |
| Side effects, complications‡ | X | X§ | X | X |
| Presence of tender and swollen joints, dactylitis, enthesitis‡ | X | X§ | X | X |
| Presence of psoriasis (body surface area) | X | X§ | X | X |
| CRP‡ | X | X | X | X |
| Disease activity (BASDAI, ASDAS)‡ | X | X | X | X |
| Patient global assessment of disease activity (VAS)‡ | X | X | X | X |
| Disease activity according to physician (VAS)‡ | X | X§ | X | X |
| Quality of life (SF-36, EQ-5D-5L, ASAS-HI)‡ | X | X | X | X |
| Patient-acceptable symptom state according to patient | X | X | X | X |
| Patient-acceptable symptom state according to physician | X | X§ | X | X |
| Disease flare(s) according to patient | X | X | ||
| Patient-reported experience with care‡ | X | X | ||
| Healthcare utilisation | X | X | X | |
| Work productivity | X | X | X | |
| Experience with SpA-Net | X | X | ||
| Self-management (SeMaS) | X | |||
| Medication adherence (VAS) | X | X |
*A 2-month interval before and after the 6-month and 1-year period will be accepted for this measurement.
†Extra visits can be a regular visit in the standard care group or a non-scheduled visit in either group.
‡Variables already collected in SpA-Net as part of standard care, prior to study.
§Variable not measured in intervention group, unless physical outpatient visit takes place.
ASAS-HI, Assessment of SpondyloArthritis International Society Health Index; ASDAS, Ankylosing Spondylitis Disease Activity Score; BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; CRP, C reactive protein; DMARD, disease-modifying antirheumatic drug; EQ-5D-5L, EuroQol 5-dimensions 5-level; NSAID, non-steroidal anti-inflammatory drug; SeMaS, Self-Management Screening Questionnaire; SF-36, 36-Item Short-Form Health Survey; SpA, spondyloarthritis; VAS, Visual Analogue Scale (0–100 mm).
bmjopen-2022-067445supp001.pdf (211.3KB, pdf)
During physical visits, the rheumatologist will indicate whether the patient is in an acceptable symptom state. If patients indicate pain, swelling or skin abnormalities during a visit, an independent examination of joint (66/68 joint count), skin (body surface area affected by psoriasis) and entheseal involvement will be performed by a trained assessor, except when physical visits are replaced by a telephone or video call. At the end of the study, all rheumatology healthcare providers (ie, rheumatologists, fellows and dedicated nurses) involved in the treatment and/or follow-up of study subjects will receive a questionnaire investigating their experience with the intervention (general satisfaction, safety, effectiveness, patient-centredness, timeliness, efficiency, equitability, flexibility, time and resource-saving capacities) as well as SpA-Net (general satisfaction, ease of use, added value).
To evaluate quality of care, the dimensions ‘timely care’ (time to care when having a flare) and ‘patient-centredness’ will be operationalised by the PREM.47 ‘Patient safety’ is evaluated through the number of complications and side-effects during follow-up. ‘Effectiveness of care’ is evaluated with measures of disease activity, functioning and health-related quality of life, and ‘efficiency of care’ through the number of rheumatology outpatient visits per year and a health economic analysis. ‘Equitability of care’ will be evaluated through subgroup analyses for sex, age, education level, diagnosis, disease duration and therapy.
During the study, all telephone calls will be registered per patient to detect potential shifts in the rheumatologist’s workload.
Sample size
We hypothesise that the study intervention is superior for the primary outcome. In 2016, the average number of outpatient visits for patients with SpA per year was 2.5 (SD 1.4) in the MUMC+. Based on prior research indicating that approximately one-third of routine SpA outpatient visits are considered unnecessary by rheumatologists,49 we expect to reduce the number of visits by at least 25% in the intervention group. A sample size of 80 patients per group is required to detect this difference with a power of 0.80 and alpha of 0.05. Assuming a 20% drop-out during follow-up, 100 patients per group will be recruited. This sample size is also sufficient to test non-inferiority for all secondary objectives with a power of 0.80 and one-sided alpha of 0.025, except for patient-reported experience with care (table 2). Sample sizes for non-inferiority endpoints were calculated using the method described by Flight and Julious for continuous outcomes,50 and the method described by Chow et al for proportional outcomes.51 All other sample size calculations were performed using G*Power (V.3.1).52
Table 2.
Sample size calculations for secondary objectives
| Continuous | Mean | SD | δNI | n |
| ASDAS (N=349) | 2.22 | 1.00 | 0.90 | 20 |
| BASDAI (N=564) | 4.17 | 2.24 | 2.00 | 20 |
| Pain (VAS) (N=763) | 38.33 | 26.19 | 20.00 | 27 |
| Patient global (VAS) (N=687) | 40.26 | 26.07 | 15.00 | 38 |
| Physician global (VAS) (N=711) | 14.30 | 16.12 | 10.00 | 41 |
| Categorical | Proportion | δNI | n | |
| Overall experience with care (N=276) | 0.90 | −0.10 | 141 |
All values calculated are based on data from SpA-Net retrieved on 29 October 2018. The number of patients with available data is provided in the first column. Stable values are assumed for the standard care group.
ASDAS, Ankylosing Spondylitis Disease Activity Score; BASDAI, Bath Ankylosing Spondylitis Disease Activity Index; n, sample size needed per group; VAS, Visual Analogue Scale (range: 0–100 mm); δNI, non-inferiority limit or margin.
Study endpoints
Primary endpoint
The primary endpoint is defined as at least 25% reduction in the number of rheumatology outpatient visits in the intervention group compared with the standard care group, within a 1-year period. Due to the COVID-19 pandemic, these outpatient visits may also take place through telephone or video calls.
Secondary endpoints
Non-inferiority of the study intervention compared with standard care with respect to health outcomes and overall experience with rheumatology care (box 2).
Cost-effectiveness of the study intervention compared with standard care (incremental cost-utility ratio, incremental net monetary benefit (iNMB)).
Predictive value of screening for self-management skills with regard to attaining both the primary and secondary non-inferiority endpoints (intervention group only).
Box 2. Rationale for non-inferiority margins.
Ankylosing Spondylitis Disease Activity Score: non-inferiority defined as an increase of ≤0.9, based on the 2018 Assessment of SpondyloArthritis International Society (ASAS) consensus definition of clinically important worsening.69
Bath Ankylosing Spondylitis Disease Activity Index: non-inferiority defined as an increase of <2.0, in accordance with the most conservative preliminary definition of clinically important worsening (‘flare’) based on the 2016 ASAS consensus report,70 and with what is most commonly regarded as a clinically relevant change by rheumatologists in clinical practice.71
Patient global assessment of disease activity: non-inferiority defined as an increase of ≤15 mm on a 0–100 mm Visual Analogue Scale (VAS), which is situated between the minimally clinically important difference for patient-reported worsening for patients with psoriatic arthritis and spondyloarthritis (SpA), respectively.72 73
Physician global VAS: non-inferiority defined as an increase of ≤10 mm, based on what is considered a clinically relevant change by rheumatologists in clinical practice.
Pain VAS: non-inferiority defined as an increase of ≤20 mm, which is based on the most conservative preliminary definition of clinically important worsening (‘flare’) according to the 2016 ASAS consensus report,70 and closely approximates findings of a study that assessed worsening of VAS-reported pain in adults with SpA, irrespective of pain levels reported at baseline.72
Overall experience with care: in 2018, approximately 90% of patients with SpA in the Maastricht University Medical Centre+ were satisfied with the care provided. Non-inferiority is defined as a decrease of ≤10%.
Statistical analysis
Patient demographics and other baseline characteristics
Descriptive statistics on prespecified demographic (age, sex, educational level, work status) and clinical (diagnosis, symptom duration, SpA features, medication use, number of outpatient visits in previous year) parameters will be reported. In addition, baseline characteristics will be summarised for the following variables: Ankylosing Spondylitis Disease Activity Score,53 Bath Ankylosing Spondylitis Disease Activity Index,54 patient global assessment of disease activity (Visual Analogue Scale (VAS)), disease activity according to physician (VAS), pain (VAS), EuroQol 5-dimensions 5-level (EQ-5D-5L),55 36-Item Short-Form Health Survey,56 Assessment of SpondyloArthritis International Society Health Index (ASAS-HI),57 SeMaS,48 experience with SpA-Net and patient-reported experience with care (PREM).47 All baseline characteristics will be reported for the total population, as well as for both patient groups separately.
Intention-to-treat and per-protocol analyses
The primary outcome will be analysed in the intention-to-treat (ITT) population. Outcomes for secondary non-inferiority and health economic analysis endpoints will be analysed in the ITT and the per-protocol population. All other analyses will be performed in the ITT population.
Primary endpoint
The difference in number of outpatient visits after 1 year of follow-up will be compared with analysis of variance (ANOVA). Given that the population is randomised, an equal distribution of baseline characteristics is to be expected. In case differences between the two groups exist on baseline, post-hoc analyses adjusting for these differences will be done (analysis of covariance).
Secondary endpoints
Differences in quality of care, health outcomes, experience with SpA-Net and overall care will be analysed with ANOVA. Post-hoc, subgroup analyses (male/female, young/older, peripheral/axial disease, early/longstanding disease, biological users/non-biological users) and predictive analyses with respect to self-management skills and successful application of the study intervention will be done with linear mixed-effects models with each endpoint as dependent variable and time, group and their interaction as fixed effects. P values will be adjusted for multiple testing. Descriptive statistics will be used to summarise experience with the study intervention and SpA-Net among healthcare providers.
Economic appraisal
A trial-based health economic evaluation (incremental cost-utility and iNMB analysis) will be performed in accordance with the International Society for Pharmacoeconomics and Outcomes Research guidelines,58 as well as the Dutch guidelines for economic evaluations in healthcare.59 Analyses will be done from a Dutch healthcare and societal perspective.
Self-reported health resource utilisation and loss of productivity in paid and unpaid work due to any health problem will be evaluated for three separate 6-month recall periods (including at baseline, see table 1). Total resource consumption and loss of productivity in paid and unpaid work will be reported as the sum of resources used or days of lost production during the 12-month study period. In case significant differences are detected between groups in healthcare utilisation and/or productivity losses at baseline, this will be accounted for.
Total healthcare costs are calculated by multiplying volumes (resource use) with unit costs according to Dutch costing guidelines.59 Costs of antirheumatic medication (non-steroidal anti-inflammatory drugs, glucocorticoids, conventional and targeted synthetic disease-modifying antirheumatic drugs (DMARDs), biological DMARDs) will be based on the Dutch national drug database (G-standard) accounting for type, dose and frequency of administration.
For paid productivity loss, the friction cost approach was chosen per Dutch national guidelines. Costs of paid productivity loss are calculated by dividing self-reported hours of paid work per week by the number of working days per week, multiplying the result by the reported amount of missed days at work due to illness and the cost per missed hour of paid work.59 A friction period of 85 days is considered.60 61 Costs of unpaid productivity loss (hours needed by housekeeping aid to complete unpaid work that remains unfinished due to illness) will be measured using questions extracted from the Institute for Medical Technology Assessment Productivity Cost Questionnaire.62 Travel costs for physical visits to the rheumatology department will be valued according to Dutch costing guidelines.60
To determine incremental health effects (ΔE), health utility scores retrieved from both the generic standardised EQ-5D-5L and disease-specific ASAS-HI measures will be integrated over time (area under the curve method) to calculate quality-adjusted life years (QALYs),55 57 using Dutch tariffs.63 64 To address uncertainty and the highly skewed nature of cost data, bootstrapping will be performed to construct 95% CIs around the mean cost differences. Point estimates and bootstrap samples will be plotted on cost-effectiveness planes and cost-effectiveness acceptability curves will be constructed as a summary measure of uncertainty for cost-effectiveness estimates. The willingness-to-pay or willingness-to-accept threshold (λ) will be set at €20.000 per QALY to interpret the incremental cost-utility ratios and calculate the iNMB (iNMB=(ΔE×λ)–incremental costs). Sensitivity analyses will be performed to test the robustness of the results, such as including costs of presenteeism and discounted medication prices for biological DMARDs.
Missing data
Data completeness will be checked at every visit and if missing, direct action (phone calls, email) will take place. Missing data will be addressed using multiple imputation.
Ethics and dissemination
The study will be conducted in accordance with the Declaration of Helsinki and Dutch legislation (Medical Research Involving Human Subjects Act) as well as good clinical practice. This study was approved by the Medical Research Ethics Committee of the Academic Hospital Maastricht/Maastricht University (reference NL71041.068.19/METC 19-059). Results will be disseminated through conference presentations and publications in peer-reviewed journals.
Safety reporting
In this study, no investigational medicinal products are used and treatment is provided as per standard care. It is not to be expected that (serious) adverse events ((S)AEs) will occur due to the intervention. Side-effects and complications from treatment are registered in routine care, and reported directly to the Dutch pharmacovigilance institute through SpA-Net. Clinical and laboratory assessments performed in this study are already part of routine care. At any time, participants can contact the outpatient clinic and extra visits can be scheduled within 7 days.
(Serious) adverse events
Adverse events (AEs) and SAEs are defined according to Articles 2.57 and 2.58 of the European Regulation 2017/745.65 All (S)AEs reported spontaneously by the subject or observed by the research team, which are suspected to be related to the study intervention, will be recorded and reported in compliance with Dutch regulations. Elective hospital admissions will not be considered SAEs.
Monitoring and quality assurance
Monitoring will be performed by the Clinical Trial Centre Maastricht in accordance with ICH Good Clinical Practice guidelines and local regulations.
Data deposition
All study data will remain available in SpA-Net for 15 years and can only be used for other (ongoing or future) research projects if permission is granted by the individual participants on the ICF. SpA-Net data storage and maintenance meet all Dutch and European legal requirements, and are in line with regulations on the protection of personal data, including the NEN7510, ISO2700 and European general data protection regulations.66
Patient and public involvement
In 2019, a knowledge agenda was released by the Dutch Society for Rheumatology.67 This document was composed in cooperation with patient organisations, and lists the 10 most important research priorities in the field of rheumatology according to patients and healthcare providers, selected from 1077 different knowledge gaps. Of these, assessing the value of eHealth in comparison with standard care was identified as the most important research question.
Patients with rheumatic and musculoskeletal diseases (RMDs), including SpA, are often subjected to lifelong periodical follow-up at specialised outpatient clinics. Cumulatively, this incurs significant time investments and travel expenses and might entail recurring practical difficulties for patients who are functionally impaired. In our practice, multiple patients have therefore asked whether routine follow-up is truly necessary. The introduction of SpA-Net in 2016 further stimulated some patients to propose replacing physical outpatient visits by remote monitoring through SpA-Net. On that line, patients were involved in the development of the research questions and initial conceptualisation of the study intervention. Additionally, a preliminary version of the research proposal and recruitment procedure was evaluated by two patient research partners that have been involved in previous research projects, including the development of SpA-Net. Their feedback was incorporated into the final protocol. All participants will receive a summary of results via email within 1 year after termination of the study. A separate report will be provided (in Dutch) to the Dutch Arthritis Foundation, the largest rheumatology patient organisation in the Netherlands, for dissemination.
Discussion
To our knowledge, TeleSpA will be the first RCT to investigate the effectiveness of telemonitoring combined with PIFU in patients with SpA with stable disease. This project will contribute to answering research questions that have been granted the highest priority by both rheumatology patients and healthcare providers in the Netherlands,67 and will address multiple unmet needs in the field of remote care for patients with RMDs that were recently identified by a dedicated European Alliance of Associations for Rheumatology task force.36
In general, the implementation of PIFU services may however raise specific safety concerns, the most prominent of which include an inherent risk for loss to follow-up, untimely care due to patients’ reluctance or inability to contact or access health services, and diagnostic delays when conditions do not immediately lead to subjective symptoms (eg, haematological or renal disorders due to medication toxicity or as a part of systemic/multiorgan manifestations of rheumatic disease) or patients fail to recognise when seeking medical review would be beneficial. Importantly, TeleSpA was specifically designed to mitigate these risks. First and foremost, by selecting patients who would theoretically be suitable for, and benefit from, PIFU in real-life care. Second, loss to follow-up will be prevented by scheduled telemonitoring (in turn supported by reminder emails, and telephone contact with the study team in case of incomplete data) and end-of-study visits, serving as safety nets and allowing for continued care planning. Finally, the availability of ‘direct access’ visits, which can be requested in multiple ways, aims to decrease barriers for patients and guarantees timely access to care. Both patient profiles and precautions are in line with recent guidance for implementing PIFU in adult rheumatology services published by the National Health Service in the UK.68 In addition, information retrieved from TeleSpA may lead to additional insights (eg, the value of self-management screening) that could help guide the design and implementation of similar care interventions elsewhere.
This study has several strengths. The utilisation of a disease-specific eHealth platform (SpA-Net) that has been in use since 2016 and for which the usability and acceptability have previously been established,42 as well as the pragmatic and multicentre trial design, will increase the reliability of inferences regarding feasibility of the study intervention in a real-life care setting. In addition, the prospective trial-based cost-utility analysis, based on utility values obtained through both generic and disease-specific outcome measures, will generate comprehensive data related to an important knowledge gap in the field of telemedicine.26 35 36 The trial design is also subject to some specific limitations. The limited sample size reduces statistical power for the secondary outcome related to patient-reported experience with care as well as exploratory subgroup analyses. Due to the limited follow-up period of 1 year, this study will unfortunately not provide information about long-term effects.
If successful in reducing the amount of routine outpatient visits without compromising health outcomes, patient experience with care and quality of care, this project will not only generate evidence to support the fast-paced adoption of similar remote care interventions currently observed in rheumatology practice, but will also provide an evidence-based, pragmatic intervention that can be rapidly translated into real-life care in the Netherlands to safeguard accessibility and flexibility of care for both patients with SpA and healthcare providers.
Supplementary Material
Footnotes
Contributors: KH, AB, HEV and AvT designed the study. KH, AB, HEV and AvT are responsible for data acquisition and/or data management. KH and AvT were involved in drafting the manuscript. All authors revised the manuscript critically for important intellectual content and approved the final manuscript. AvT is a senior author.
Funding: This work was supported by a grant from the Dutch Arthritis Foundation (project number 19-2-203). In addition, development of SpA-Net was financially supported by grants from ZonMw (project number 836042001) and the Dutch Arthritis Foundation, and was sponsored by AbbVie, Biogen, Celgene, Janssen-Cilag, MSD, Novartis, Pfizer and UCB.
Disclaimer: None of these parties had a role in the study design or in the collection, analysis or interpretation of the data, the writing of the manuscript or the decision to submit the manuscript for publication. Publication of this article was not contingent upon approval by any of these parties.
Competing interests: KH declared no competing interests. AB received departmental research grants from AbbVie and consulting fees or honorarium from Galapagos, Hy2Care and Novartis, all unrelated to the current research project. HEV received research grants from Sanofi and consulting fees or honorarium from AbbVie, Novartis, Pfizer, UCB, Janssen and Galapagos, all outside the current research project. AvT received unrestricted research grants from Novartis, Pfizer and UCB, and received consulting fees from Novartis and Galapagos.
Patient and public involvement: Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review: Not commissioned; externally peer reviewed.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Ethics statements
Patient consent for publication
Not required.
References
- 1.Rudwaleit M. New approaches to diagnosis and classification of axial and peripheral spondyloarthritis. Curr Opin Rheumatol 2010;22:375–80. 10.1097/BOR.0b013e32833ac5cc [DOI] [PubMed] [Google Scholar]
- 2.Akkoc N. Are spondyloarthropathies as common as rheumatoid arthritis worldwide? A review. Curr Rheumatol Rep 2008;10:371–8. 10.1007/s11926-008-0060-3 [DOI] [PubMed] [Google Scholar]
- 3.Reveille JD, Witter JP, Weisman MH. Prevalence of axial spondylarthritis in the United States: estimates from a cross-sectional survey. Arthritis Care Res (Hoboken) 2012;64:905–10. 10.1002/acr.21621 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Malinowski KP, Kawalec P. The indirect costs of ankylosing spondylitis: a systematic review and meta-analysis. Expert Rev Pharmacoecon Outcomes Res 2015;15:285–300. 10.1586/14737167.2015.1001370 [DOI] [PubMed] [Google Scholar]
- 5.Palla I, Trieste L, Tani C, et al. A systematic literature review of the economic impact of ankylosing spondylitis. Clin Exp Rheumatol 2012;30:S136–41. [PubMed] [Google Scholar]
- 6.Boonen A, Brinkhuizen T, Landewé R, et al. Impact of ankylosing spondylitis on sick leave, presenteeism and unpaid productivity, and estimation of the societal cost. Ann Rheum Dis 2010;69:1123–8. 10.1136/ard.2009.116764 [DOI] [PubMed] [Google Scholar]
- 7.Strömbeck B, Englund M, Bremander A, et al. Cost of illness from the public payers’ perspective in patients with ankylosing spondylitis in rheumatological care. J Rheumatol 2010;37:2348–55. 10.3899/jrheum.100099 [DOI] [PubMed] [Google Scholar]
- 8.van der Heijde D, Ramiro S, Landewé R, et al. 2016 update of the ASAS-EULAR management recommendations for axial spondyloarthritis. Ann Rheum Dis 2017;76:978–91. 10.1136/annrheumdis-2016-210770 [DOI] [PubMed] [Google Scholar]
- 9.Smolen JS, Schöls M, Braun J, et al. Treating axial spondyloarthritis and peripheral spondyloarthritis, especially psoriatic arthritis, to target: 2017 update of recommendations by an international task force. Ann Rheum Dis 2018;77:3–17. 10.1136/annrheumdis-2017-211734 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Machado PM, Deodhar A. Treat-to-target in axial spondyloarthritis: gold standard or fools’ gold? Curr Opin Rheumatol 2019;31:344–8. 10.1097/BOR.0000000000000625 [DOI] [PubMed] [Google Scholar]
- 11.Coates LC, O’Dwyer J, Meads D, et al. Treat-to-target in psoriatic arthritis—cost-effective in the biosimilar era. The Lancet Rheumatology 2022;4:e390–1. 10.1016/S2665-9913(22)00101-1 [DOI] [PubMed] [Google Scholar]
- 12.Institute of Medicine Committee on Quality of Health Care in A . Crossing the quality chasm: A new health system for the 21st century. Washington (DC): National Academies Press (US), [Google Scholar]
- 13.Battafarano DF, Ditmyer M, Bolster MB, et al. 2015 American College of rheumatology workforce study: supply and demand projections of adult rheumatology workforce, 2015-2030. Arthritis Care Res (Hoboken) 2018;70:617–26. 10.1002/acr.23518 [DOI] [PubMed] [Google Scholar]
- 14.Barber CEH, Jewett L, Badley EM, et al. Stand up and be counted: measuring and mapping the rheumatology workforce in Canada. J Rheumatol 2017;44:248–57. 10.3899/jrheum.160621 [DOI] [PubMed] [Google Scholar]
- 15.Kiltz U, Landewé RBM, van der Heijde D, et al. Development of ASAS quality Standards to improve the quality of health and care services for patients with axial spondyloarthritis. Ann Rheum Dis 2020;79:193–201. 10.1136/annrheumdis-2019-216034 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.British Society for Rheumatology . Rheumatology workforce: a crisis in numbers. workforce policy report 2021. London, 2021: 1–46. [Google Scholar]
- 17.Hehir M, Hewlett S, Mitchell K, et al. What happens in rheumatoid arthritis (RA) outpatient clinics? Rheumatology Suppl 2001;40 Suppl 1:146. 10.1093/rheumatology/40.suppl_1.138 [DOI] [Google Scholar]
- 18.Hewlett S, Kirwan J, Pollock J, et al. Patient initiated outpatient follow up in rheumatoid arthritis: six year randomised controlled trial. BMJ 2005;330:171. 10.1136/bmj.38265.493773.8F [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.McBain H, Newman S, Shipley M, et al. Experiences of a patient-initiated self-monitoring service in inflammatory arthritis: a qualitative exploration. Musculoskeletal Care 2018;16:278–86. 10.1002/msc.1232 [DOI] [PubMed] [Google Scholar]
- 20.Bartlett SJ, De Leon E, Orbai A-M, et al. Patient-reported outcomes in RA care improve patient communication, decision-making, satisfaction and confidence: qualitative results. Rheumatology (Oxford) 2020;59:1662–70. 10.1093/rheumatology/kez506 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Rivera SC, Kyte DG, Aiyegbusi OL, et al. The impact of patient-reported outcome (pro) data from clinical trials: a systematic review and critical analysis. Health Qual Life Outcomes 2019;17:156. 10.1186/s12955-019-1220-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Solomon DH, Rudin RS. Digital health technologies: opportunities and challenges in rheumatology. Nat Rev Rheumatol 2020;16:525–35. 10.1038/s41584-020-0461-x [DOI] [PubMed] [Google Scholar]
- 23.Miloslavsky EM, Bolster MB. Addressing the rheumatology workforce shortage: a multifaceted approach. Semin Arthritis Rheum 2020;50:791–6. 10.1016/j.semarthrit.2020.05.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Vonk RAA, Hilderink HBM, Plasmans MHD, et al. Health care expenditures foresight 2015-2060: quantitative preliminary study at the request of the scientific council for government policy (WRR). part 1: future projections: national institute for public health and the environment (RIVM). 2020: 37–53. [Google Scholar]
- 25.Mikuls TR, Johnson SR, Fraenkel L, et al. American College of rheumatology guidance for the management of rheumatic disease in adult patients during the COVID-19 pandemic: version 3. Arthritis Rheumatol 2021;73:e1–12. 10.1002/art.41596 [DOI] [PubMed] [Google Scholar]
- 26.Nelson AJ, Anderson ME. A systematic review exploring pre-COVID-19 telehealthcare models used in the management of patients with rheumatological disease. Rheumatol Adv Pract 2021;5:rkab073. 10.1093/rap/rkab073 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Marques A, Bosch P, de Thurah A, et al. Effectiveness of remote care interventions: a systematic review Informing the 2022 EULAR points to consider for remote care in rheumatic and musculoskeletal diseases. RMD Open 2022;8:e002290. 10.1136/rmdopen-2022-002290 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Seppen BF, den Boer P, Wiegel J, et al. Asynchronous mhealth interventions in rheumatoid arthritis: systematic scoping review. JMIR Mhealth Uhealth 2020;8:e19260. 10.2196/19260 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Nguyen NH, Martinez I, Atreja A, et al. Digital health technologies for remote monitoring and management of inflammatory bowel disease: a systematic review. Am J Gastroenterol 2022;117:78–97. 10.14309/ajg.0000000000001545 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Müskens WD, Rongen-van Dartel SAA, Vogel C, et al. Telemedicine in the management of rheumatoid arthritis: maintaining disease control with less health-care utilization. Rheumatol Adv Pract 2021;5:rkaa079. 10.1093/rap/rkaa079 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Myasoedova E, Crowson CS, Giblon RE, et al. Optimization of flare management in patients with rheumatoid arthritis: results of a randomized controlled trial. Clin Rheumatol 2019;38:3025–32. 10.1007/s10067-019-04664-5 [DOI] [PubMed] [Google Scholar]
- 32.Chevallard M, Belloli L, Ughi N, et al. Use of telemedicine during the COVID-19 pandemic in patients with inflammatory arthritis: a retrospective study on feasibility and impact on patient-reported outcomes in a real-life setting. Rheumatol Int 2021;41:1253–61. 10.1007/s00296-021-04863-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Bos WH, van Tubergen A, Vonkeman HE. Telemedicine for patients with rheumatic and musculoskeletal diseases during the COVID-19 pandemic; a positive experience in the Netherlands. Rheumatol Int 2021;41:565–73. 10.1007/s00296-020-04771-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Bateman J, Cleaton N. Managing patients using telerheumatology: lessons from a pandemic. Best Pract Res Clin Rheumatol 2021;35:101662. 10.1016/j.berh.2021.101662 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Krusche M. Telemedicine: a solution for everyone? Nat Rev Rheumatol 2022;18:187–8. 10.1038/s41584-022-00763-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.de Thurah A, Bosch P, Marques A, et al. 2022 EULAR points to consider for remote care in rheumatic and musculoskeletal diseases. Ann Rheum Dis 2022;81:1065–71. 10.1136/annrheumdis-2022-222341 [DOI] [PubMed] [Google Scholar]
- 37.Fredriksson C, Ebbevi D, Waldheim E, et al. Patient-initiated appointments compared with standard outpatient care for rheumatoid arthritis: a randomised controlled trial. RMD Open 2016;2:e000184. 10.1136/rmdopen-2015-000184 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Hewlett S, Mitchell K, Haynes J, et al. Patient-initiated hospital follow-up for rheumatoid arthritis. Rheumatology (Oxford) 2000;39:990–7. 10.1093/rheumatology/39.9.990 [DOI] [PubMed] [Google Scholar]
- 39.Kirwan JR, Mitchell K, Hewlett S, et al. Clinical and psychological outcome from a randomized controlled trial of patient-initiated direct-access hospital follow-up for rheumatoid arthritis extended to 4 years. Rheumatology (Oxford) 2003;42:422–6. 10.1093/rheumatology/keg130 [DOI] [PubMed] [Google Scholar]
- 40.McBain H, Shipley M, Olaleye A, et al. A patient-initiated DMARD self-monitoring service for people with rheumatoid or psoriatic arthritis on methotrexate: a randomised controlled trial. Ann Rheum Dis 2016;75:1343–9. 10.1136/annrheumdis-2015-207768 [DOI] [PubMed] [Google Scholar]
- 41.Seppen B, Wiegel J, Ter Wee MM, et al. Smartphone-assisted patient-initiated care versus usual care in patients with rheumatoid arthritis and low disease activity: a randomized controlled trial. Arthritis Rheumatol 2022;74:1737–45. 10.1002/art.42292 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Webers C, Beckers E, Boonen A, et al. Development, usability and acceptability of an integrated ehealth system for spondyloarthritis in the Netherlands (spa-net). RMD Open 2019;5:e000860. 10.1136/rmdopen-2018-000860 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Pocock SJ, Simon R. Sequential treatment assignment with balancing for prognostic factors in the controlled clinical trial. Biometrics 1975;31:103–15. 10.2307/2529712 [DOI] [PubMed] [Google Scholar]
- 44.ICH harmonised tripartite guideline. Statistical principles for clinical trials. International conference on harmonisation E9 expert working group. Stat Med 1999;18:1905–42. [PubMed] [Google Scholar]
- 45.Coates LC, Gossec L, Ramiro S, et al. New grappa and EULAR recommendations for the management of psoriatic arthritis. Rheumatology (Oxford) 2017;56:1251–3. 10.1093/rheumatology/kew390 [DOI] [PubMed] [Google Scholar]
- 46.Maksymowych WP, Richardson R, Mallon C, et al. Evaluation and validation of the patient acceptable symptom state (pass) in patients with ankylosing spondylitis. Arthritis Rheum 2007;57:133–9. 10.1002/art.22469 [DOI] [PubMed] [Google Scholar]
- 47.Beckers E, Webers C, Boonen A, et al. Validation and implementation of a patient-reported experience measure for patients with rheumatoid arthritis and spondyloarthritis in the Netherlands. Clin Rheumatol 2020;39:2889–97. 10.1007/s10067-020-05076-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Eikelenboom N, Smeele I, Faber M, et al. Validation of self-management screening (semas), a tool to facilitate personalised counselling and support of patients with chronic diseases. BMC Fam Pract 2015;16:165. 10.1186/s12875-015-0381-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Hermans K, Boonen A, van Tubergen A. Are all routine spondyloarthritis outpatient visits considered useful by rheumatologists? An exploratory clinical practice study. J Rheumatol 2022;49:1214–20. 10.3899/jrheum.220037 [DOI] [PubMed] [Google Scholar]
- 50.Flight L, Julious SA. Practical guide to sample size calculations: non-inferiority and equivalence trials. Pharm Stat 2016;15:80–9. 10.1002/pst.1716 [DOI] [PubMed] [Google Scholar]
- 51.Chow S, Shao J, Wang H, et al. Sample size calculations in clinical research. 3rd ed. Boca Raton: Taylor & Francis, 2018: 77–8. [Google Scholar]
- 52.Faul F, Erdfelder E, Lang A-G, et al. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods 2007;39:175–91. 10.3758/bf03193146 [DOI] [PubMed] [Google Scholar]
- 53.van der Heijde D, Lie E, Kvien TK, et al. ASDAS, a highly discriminatory ASAS-endorsed disease activity score in patients with ankylosing spondylitis. Ann Rheum Dis 2009;68:1811–8. 10.1136/ard.2008.100826 [DOI] [PubMed] [Google Scholar]
- 54.Garrett S, Jenkinson T, Kennedy LG, et al. A new approach to defining disease status in ankylosing spondylitis: the Bath ankylosing spondylitis disease activity index. J Rheumatol 1994;21:2286–91. [PubMed] [Google Scholar]
- 55.Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res 2011;20:1727–36. 10.1007/s11136-011-9903-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Ware JE, Sherbourne CD. The mos 36-ltem short-form health survey (SF-36). Medical Care 1992;30:473–83. 10.1097/00005650-199206000-00002 [DOI] [PubMed] [Google Scholar]
- 57.Kiltz U, van der Heijde D, Boonen A, et al. The ASAS health index (ASAS HI)-a new tool to assess the health status of patients with spondyloarthritis. Clin Exp Rheumatol 2014;32:S–105. [PubMed] [Google Scholar]
- 58.Ramsey SD, Willke RJ, Glick H, et al. Cost-effectiveness analysis alongside clinical trials II-an ISPOR good research practices task force report. Value Health 2015;18:161–72. 10.1016/j.jval.2015.02.001 [DOI] [PubMed] [Google Scholar]
- 59.Hakkaart-van Roijen L, van der Linden N, Bouwmans C, et al. Kostenhandleiding: methodologie van kostenonderzoek en referentieprijzen voor economische evaluaties in de gezondheidszorg. 2016. Available: https://www.zorginstituutnederland.nl/over-ons/publicaties/publicatie/2016/02/29/richtlijn-voor-het-uitvoeren-van-economische-evaluaties-in-de-gezondheidszorg [Accessed 11 Feb 2019].
- 60.Kanters TA, Bouwmans CAM, van der Linden N, et al. Update of the dutch manual for costing studies in health care. PLoS One 2017;12:e0187477. 10.1371/journal.pone.0187477 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Koopmanschap MA, Rutten FF, van Ineveld BM, et al. The friction cost method for measuring indirect costs of disease. J Health Econ 1995;14:171–89. 10.1016/0167-6296(94)00044-5 [DOI] [PubMed] [Google Scholar]
- 62.Bouwmans C, Krol M, Severens H, et al. The imta productivity cost questionnaire: a standardized instrument for measuring and valuing health-related productivity losses. Value Health 2015;18:753–8. 10.1016/j.jval.2015.05.009 [DOI] [PubMed] [Google Scholar]
- 63.M Versteegh M, M Vermeulen K, M A A Evers S, et al. Dutch tariff for the five-level version of EQ-5D. Value Health 2016;19:343–52. 10.1016/j.jval.2016.01.003 [DOI] [PubMed] [Google Scholar]
- 64.Essers I, Hiligsmann M, Kiltz U, et al. Development of one general and six country-specific algorithms to assess societal health utilities based on ASAS HI. RMD Open 2019;5:e000872. 10.1136/rmdopen-2018-000872 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.European parliament and Council of the European Union . Regulation (EU) 2017/745 of the european parliament and of the council of 5 april 2017 on medical devices: EUR-lex; 2017. 2020. Available: http://data.europa.eu/eli/reg/2017/745/2020-04-24 [Accessed 18 May 2022].
- 66.European parliament and Council of the European Union . Regulation (EU) 2016/679 of the european parliament and of the council of 27 april 2016 on the protection of natural persons with regard to the processing of personal data and on the free movement of such data 2016. 2016. Available: http://data.europa.eu/eli/reg/2016/679/2016-05-04 [Accessed 18 May 2022].
- 67.Dutch society for rheumatology . KennisAgenda reumatologie. Utrecht: Nederlandse Vereniging voor Reumatologie, 2019: 18–9. [Google Scholar]
- 68.National Health Service . Implementing patient-initiated follow-up (PIFU) in adult rheumatology services. 2022. Available: https://www.england.nhs.uk/wp-content/uploads/2022/05/B0943-implementing-patient-initiated-follow-up-services-in-adult-rheumatology-services.pdf [Accessed 02 Nov 2022].
- 69.Molto A, Gossec L, Meghnathi B, et al. An assessment in spondyloarthritis International Society (ASAS) -endorsed definition of clinically important worsening in axial spondyloarthritis based on ASDAS. Ann Rheum Dis 2018;77:124–7. 10.1136/annrheumdis-2017-212178 [DOI] [PubMed] [Google Scholar]
- 70.Gossec L, Portier A, Landewé R, et al. Preliminary definitions of “ flare ” in axial spondyloarthritis, based on pain, BASDAI and ASDAS-CRP: an ASAS initiative. Ann Rheum Dis 2016;75:991–6. 10.1136/annrheumdis-2015-208593 [DOI] [PubMed] [Google Scholar]
- 71.Essers I, Boonen A, Busch M, et al. Fluctuations in patient reported disease activity, pain and global being in patients with ankylosing spondylitis. Rheumatology (Oxford) 2016;55:2014–22. 10.1093/rheumatology/kew303 [DOI] [PubMed] [Google Scholar]
- 72.Wheaton L, Pope J. The minimally important difference for patient-reported outcomes in spondyloarthropathies including pain, fatigue, sleep, and health assessment questionnaire. J Rheumatol 2010;37:816–22. 10.3899/jrheum.090086 [DOI] [PubMed] [Google Scholar]
- 73.Kwok T, Pope JE. Minimally important difference for patient-reported outcomes in psoriatic arthritis: health assessment questionnaire and pain, fatigue, and global visual analog scales. J Rheumatol 2010;37:1024–8. 10.3899/jrheum.090832 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjopen-2022-067445supp001.pdf (211.3KB, pdf)