

Abstract
A 50-year-old woman presented to an outside hospital for acute onset bilateral lower limb pain. She was diagnosed with aortoiliac stenosis and underwent stent placement. Post-procedure, she was noted to have altered mental status, truncal ataxia, neck titubation, and incomplete external ophthalmoplegia. She rapidly declined to a stuporous state. She had a history of uterine cancer treated with chemoradiation which was complicated by chronic radiation enteritis. She was also reported to have poor oral intake, recurrent emesis, and weight loss for a month before her presentation. After an extensive work up, she arrived at our facility where an MRI of the brain showed restricted diffusion and T2-FLAIR sequence showed hyperintensities of bilateral cerebellum. T2-FLAIR hyperintensities of bilateral dorsomedial thalami, fornix, and post-contrast-enhancement of mammillary bodies were also noted. The clinical picture with imaging findings was concerning for possible thiamine deficiency. In Wernicke’s encephalopathy, restricted diffusion, T2-FLAIR hyperintensities, and contrast enhancement may be seen in mammillary bodies, dorsomedial thalami, tectal plate, periaqueductal grey matter, and rarely in the cerebellum as well. Her thiamine level was 70 nmol/l (reference range: 70–180 nmol/l). Thiamine levels can be falsely elevated in patients who are on enteral feeds, which was the case in our patient. She was started on high dose thiamine replacement. At time of discharge, repeat MRI brain revealed resolution of cerebellar changes with mild atrophy and patient had subtle neurological improvement including consistent eye opening, tracking, and attending to examiner, as well as mumbling words.
Keywords: Cerebellum, Diffusion restriction, Thiamine, Wernicke
A 50-year-old woman presented to an outside hospital for acute onset bilateral lower limb pain. She was diagnosed with aortoiliac stenosis and underwent stent placement. Post-procedure, she was noted to have altered mental status, truncal ataxia, neck titubation, and incomplete external ophthalmoplegia. She rapidly declined to a stuporous state. She had a history of uterine cancer treated with chemoradiation which was complicated by chronic radiation enteritis. She was also reported to have poor oral intake, recurrent emesis, and weight loss for a month before her presentation. After an extensive work up, she arrived at our facility where a magnetic resonance imaging (MRI) of the brain showed restricted diffusion and T2-fluid attenuated inversion recovery sequences (T2-FLAIR) showed hyperintensities of bilateral cerebellum [Figure 1]. T2-FLAIR hyperintensities of bilateral dorsomedial thalami, fornix, and post-contrast-enhancement of mammillary bodies were also noted [Figure 2]. The clinical picture with imaging findings was concerning for possible thiamine deficiency. In Wernicke’s encephalopathy, restricted diffusion, T2-FLAIR hyperintensities, and contrast-enhancement may be seen in mammillary bodies, dorsomedial thalami, tectal plate, periaqueductal grey matter, and rarely in the cerebellum as well. Her thiamine level was 70 nmol/l (reference range: 70–180 nmol/l). Thiamine levels can be falsely elevated in patients who are on enteral feeds, which was the case in our patient. She was started on high dose thiamine replacement. At time of discharge, repeat MRI brain revealed resolution of cerebellar changes with mild atrophy and patient had subtle neurological improvement including consistent eye opening, tracking, and attending to examiner, as well as mumbling words.
Figure 1:
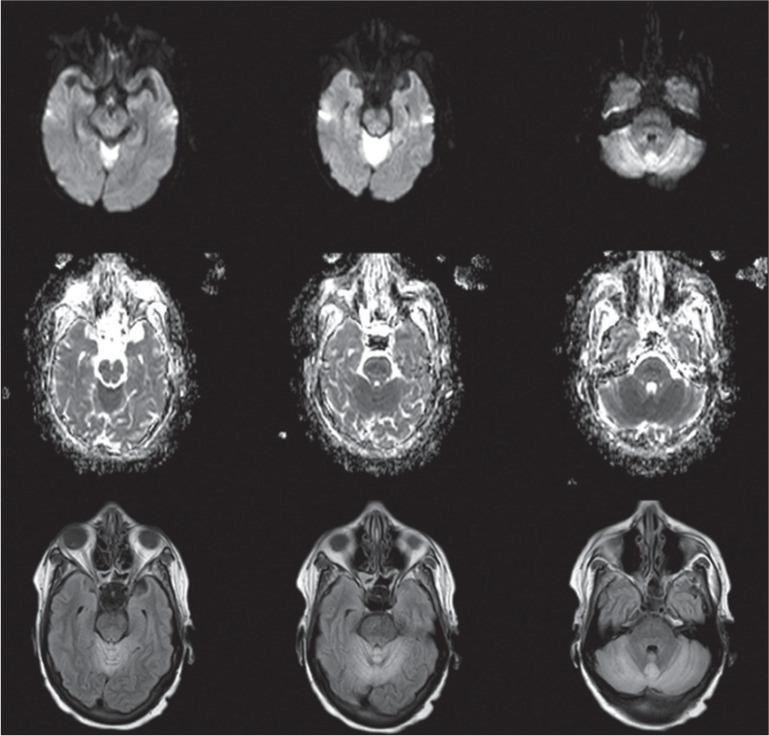
Diffusion-weighted images are seen in the first row. Apparent Diffusion Coefficient images are seen in the second row. These show restricted diffusion of bilateral cerebellum. T2-fluid attenuated inversion recovery images (T2-FLAIR) are seen in the third row and it shows hyperintensities involving bilateral cerebellum.
Figure 2:
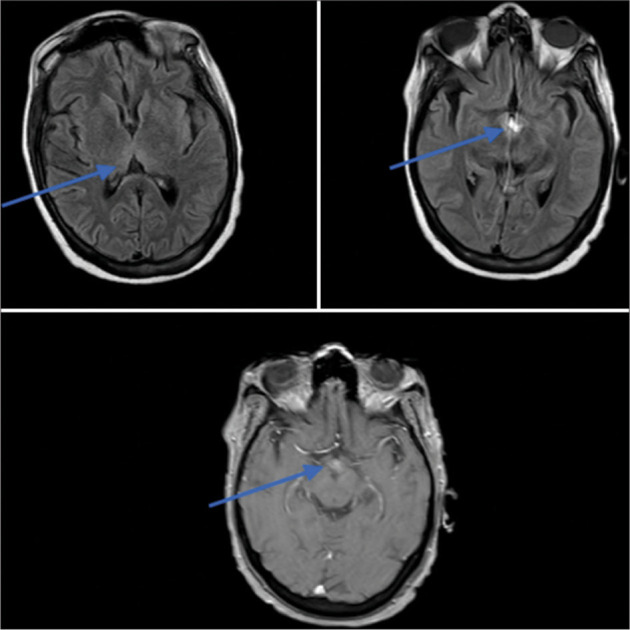
Blue arrow indicates T2-FLAIR hyperintensities involving bilateral dorsomedial thalami (top left), fornix (top right) and post-contrast enhancement of the mammillary bodies (bottom).
Funding Statement
Financial support and sponsorship
Nil.
Footnotes
How to cite this article: Arulprakash N, Shah V. Cerebellar restricted diffusion in Wernicke’s encephalopathy. J Neurosci Rural Pract 2023;14:182-3.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.