

We were impressed by the report by Chen and colleagues [1]. Although we had expected transpulmonary driving pressure (DPL) to be more prognostically relevant than airway driving pressure (DPaw), this large cohort study, to the best of our knowledge, showed for the first time that DPaw and DPL had equivalent predictive power for mortality in patients with acute respiratory distress syndrome (ARDS). However, we would like to point out three concerns regarding this study.
First, the authors suggest that chest wall driving pressure (DPcw) was associated with severity and outcome; however, this is controversial for the following reasons. There was no difference in DPcw between survivors and non-survivors (Table 1), and the correlation between DPcw and non-pulmonary sequential organ failure assessment (SOFA) (Pearson’s correlation coefficient = 0.150) is weak. In addition, the association between DPcw and 60-day mortality in Cox regression should be tested after adjusting for variables such as age, SOFA, and DPL. Since DPcw could have little effect on outcome, DPL and DPaw might have been equivalent predictors of outcome.
Second, there may be an error in the calculations for the elastance-derived plateau PL shown in the supplement. The formula is shown as “EL/Ers × Directly-measured end-inspiratory PL” however, we believe “EL/Ers × Pplat” is correct [2]. Since this may influence the prognostic value of elastance-derived plateau PL, we suggest modifying the values or the calculation if necessary.
Third, in the limitation, the section on airway closure and airway opening pressure (AOP) may be misleading. The authors mentioned “only 4 (8.8%) patients received a clinical positive end-expiratory pressure (PEEP) below AOP;” however, we believe the authors should express that “only 4 (8.8%) patients received a PEEPhigh (15 or 18 cmH2O) below AOP.” Table 1 of the authors’ previous study shows that 8.8% of their patients had AOP > PEEPhigh (15 or 18 cmH2O), not clinical PEEP [3]. Since this present study's median clinical PEEP was 12, there might be more patients with airway closure than predicted. The presence of airway closure requires the pressure needed to open the distal airway, which can be termed “wasting” driving pressure (Fig. 1). Therefore, this "wasting" drive pressure due to airway closure can cause misinterpretation of the compliance as low. Although the association between driving pressure and mortality was found for obese and non-obese ARDS patients combined, no association was found when limited to obese patients only [4]. We assumed that this may be due to the “wasting” driving pressure generated by airway closure, which is frequent in obese patients [5]. If possible, we suggest that the authors compare whether DPaw and DPL are predictors of mortality separately for obese and non-obese patients. In addition to driving pressure, airway closure should always be evaluated in patients with ARDS, especially if obese, and future studies should evaluate whether driving pressure considering AOP is a predictor of outcome.
Fig. 1.
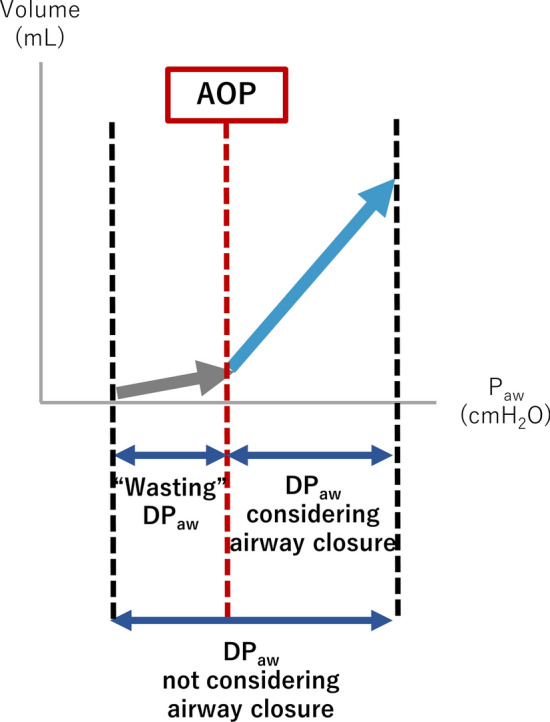
Conceptual diagram of driving pressure of the patient with airway closure. AOP airway opening pressure, Paw airway pressure, DPaw airway driving pressure
Author contributions
RN wrote this manuscript. NB, MT, and MN helped in writing this manuscript. All authors have read and approved the manuscript.
Funding
The authors received no specific funding for this work.
Data availability
The data are available from the corresponding author upon reasonable request.
Declarations
Conflicts of interest
The authors declare that they have no conflicts of interest.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Chen L, Grieco DL, Beloncle F, Chen GQ, Tiribelli N, Madotto F, Fredes S, Lu C, Antonelli M, Mercat A, Slutsky AS, Zhou JX, Brochard L. Partition of respiratory mechanics in patients with acute respiratory distress syndrome and association with outcome: a multicentre clinical study. Intensive Care Med. 2022;48:888–898. doi: 10.1007/s00134-022-06724-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gattinoni L, Carlesso E, Cadringher P, Valenza F, Vagginelli F, Chiumello D. Physical and biological triggers of ventilator-induced lung injury and its prevention. Eur Respir J Suppl. 2003;47:15s–25s. doi: 10.1183/09031936.03.00021303. [DOI] [PubMed] [Google Scholar]
- 3.Chen L, Del Sorbo L, Grieco DL, Junhasavasdikul D, Rittayamai N, Soliman I, Sklar MC, Rauseo M, Ferguson ND, Fan E, Richard JM, Brochard L. Potential for lung recruitment estimated by the recruitment-to-inflation ratio in acute respiratory distress syndrome. a clinical trial. Am J Respir Crit Care Med. 2020;201:178–187. doi: 10.1164/rccm.201902-0334OC. [DOI] [PubMed] [Google Scholar]
- 4.Coudroy R, Vimpere D, Aissaoui N, Younan R, Bailleul C, Couteau-Chardon A, Lancelot A, Guerot E, Chen L, Brochard L, Diehl JL. Prevalence of complete airway closure according to body mass index in acute respiratory distress syndrome. Anesthesiology. 2020;133:867–878. doi: 10.1097/ALN.0000000000003444. [DOI] [PubMed] [Google Scholar]
- 5.De Jong A, Cossic J, Verzilli D, Monet C, Carr J, Conseil M, Monnin M, Cisse M, Belafia F, Molinari N, Chanques G, Jaber S. Impact of the driving pressure on mortality in obese and non-obese ARDS patients: a retrospective study of 362 cases. Intensive Care Med. 2018;44:1106–1114. doi: 10.1007/s00134-018-5241-6. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data are available from the corresponding author upon reasonable request.