

Abstract
The severity of septic arthritis of the hand and the prospects for restoration of joint function are determined by a complex of factors. Among them, the leading role belongs to local changes in tissue structures. This includes the destruction of articular cartilage and bone tissue with the development of osteomyelitis, the involvement of paraarticular soft tissues in the purulent process, and the destruction of the flexor/extensor tendons of the fingers. The currently missing specialized classification of septic arthritis could help in systematizing the diseases, determining treatment tactics, and predicting the results of treatment. The classification of septic arthritis of the hand proposed for discussion is based on the following principle: Joint−Wound−Tendon (JxWxTx); Jx characterizes damage to the osteochondral structures of the joint, Wx is the presence of paraarticular purulent wounds or fistulas, and Tx is destruction of the flexor/extensor tendons of the finger. The classification of the diagnosis makes it possible to assess the nature and severity of damage to the structures of the joint and may also be useful when comparing the results of treatment of septic arthritis of the hand.
Keywords: Hand, Septic arthritis, Classification, Osteomyelitis, Paraarticular wounds
Core Tip: The absence to date of a specialized classification of septic arthritis of the hand determines the relevance of its development. The proposed classification is based on the principle JOINT-WOUND-TENDON and reflects in aggregate the lesion of the osteo-cartilaginous structures of the joint, paraarticular soft tissues, and tendons of the flexor/extensor of the finger.
TO THE EDITOR
Septic arthritis of the hand is a common infectious pathology of the joints and ranks second in frequency after inflammation of the knee joint[1]. Given the high functional significance of the small joints of the hand, their inflammation often leads to serious consequences, sometimes ending in limitation or even disability. The most common cause of septic arthritis of the hand is various penetrating wounds. The pathogenic microflora that has entered the joint cavity causes the development of an infectious process, which, if surgical care is not provided in time, leads to the destruction of the articular cartilage and the development of osteomyelitis. In septic arthritis of the hand, a purulent process often occurs in paraarticular tissues with the formation of wounds and fistulas, which has a significant impact on the extent of surgical intervention and the results of treatment in general. The inflammatory process in the small joints of the hand, proceeding with purulent-necrotic lesions of the surrounding soft tissues, may be accompanied by destructive changes in the area of the flexor/extensor tendons of the finger, which negatively affects the prospects for restoring movements in the joint. This fact distinguishes the course of septic arthritis of the hand from purulent arthritis of large joints, in which tendon damage is uncharacteristic[2].
Thus, the course of septic arthritis of the hand and the features of treatment and its results are determined by a complex of pathological changes in the osteochondral apparatus, paraarticular soft tissues, and flexor/extensor tendons of the finger. While analyzing the literature on septic arthritis of the hand (published in the World Journal of Orthopedics 2022; 13: 622-630)[3], we faced problems comparing the results of surgical treatment presented by different authors.
To obtain reliable results, it is necessary to understand the nature and extent of tissue damage in the observations that we compare.
Evaluating the response to treatment of isolated septic arthritis, septic arthritis with osteomyelitis, purulent process in the paraarticular soft tissues, and tendon destruction can hardly be justified. However, in most cases, the authors use the term "septic arthritis of the hand" when formulating the diagnosis, only occasionally highlighting cases with osteomyelitis[4].
As a consequence, comparison of the results of treatment presented by different experts may be incorrect since the severity of the disease was initially different. In this regard, the use in clinical practice and in the course of scientific analysis of the classification of the pathological process is of great importance. However, to date, there has been no specialized classification of septic arthritis of the hand. According to the most common classification of hand infection given by Brown[5], only two forms can be attributed to the characteristics of purulent arthritis: Osteomyelitis and septic arthritis. However, this is clearly not enough in view of the above arguments[5]. This can be partially compensated for by using the classification of Tan et al[6] for infection of the joints of the hand, which was developed to characterize the inflammatory process in large joints[6]. It presents information about the damage to the osteochondral structures of the joint and paraarticular soft tissues (isolated septic arthritis; septic arthritis with soft-tissue extension, but no osteomyelitis; septic arthritis with contiguous osteomyelitis). At the same time, this classification does not reflect the presence/absence of destruction of the tendon apparatus, which is rare in arthritis of large joints but is extremely important in septic arthritis of the hand. In addition, the classification of Tan et al[6] is quite voluminous, which makes it difficult to use it in wide clinical practice.
We have significant experience in the treatment of patients with septic arthritis of the hand and would like to propose our classification of septic arthritis of the hand.
The classification is based on the principle of Joint−Wound−Tendon (JxWxTx) and takes into account the presence of damage to the osteochondral structures of the joint, paraarticular soft tissues, and tendon apparatus.
The symbol Jx characterizes the lesion of the osteochondral structures of the joint, where the index "x" determines the presence or absence of a sign: J0–without osteomyelitis; J1–with osteomyelitis.
The symbol Wx characterizes the presence of purulent wounds or fistulas in the paraarticular region: W0–without wounds or fistulas; W1–with a fistula; W2–with a purulent wound.
The symbol Tx characterizes the destruction of the flexor/extensor tendons: Т0–without tendon destruction; Т1–extensor tendon destruction; Т2–flexor tendon destruction; Т3–destruction of both tendons.
Schematically, this classification can be represented below (Figure 1).
Figure 1.

New classification for septic arthritis of the hand. JxWxTx: Joint−Wound−Tendon.
Examples of the application of this classification in the formulation of a diagnosis are shown below (Figures 2-4).
Figure 2.

Septic arthritis of the proximal interphalangeal joint of the index finger (J1W0T0). A: Hand after repeated treatment; B: X-ray.
Figure 4.
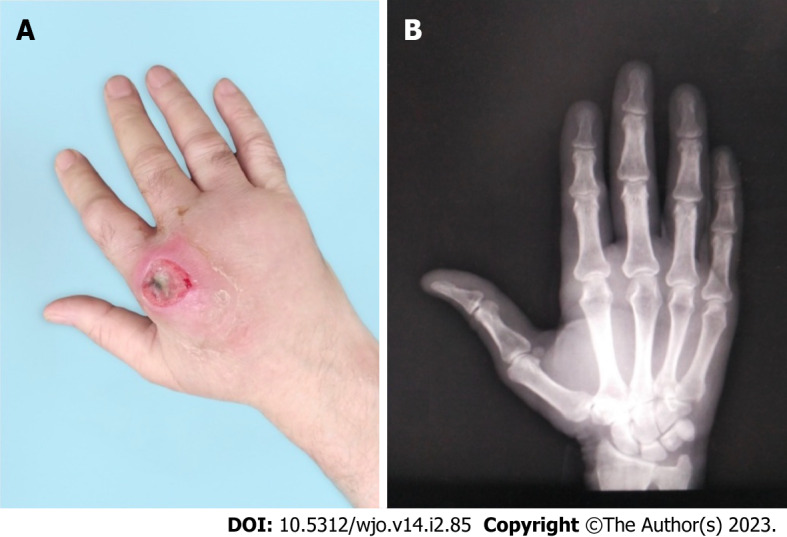
Septic arthritis of the 2nd metacarpophalangeal joint of the right hand (J0W2T1). A: During hospitalization; B: X-ray.
A 58-year-old woman pricked the index finger of her right hand with a needle while doing embroidery 3 wk ago. A day later, she noticed swelling of the finger and aching pain, aggravated by bending the finger. She was examined by a polyclinic surgeon and received a course of antibacterial drugs with some positive effect. Despite this, finger edema and pain on flexion persisted, which served as the basis for a second visit to the doctor. Upon further diagnostic testing, X-ray showed osteomyelitis in the proximal interphalangeal joint. On magnetic resonance imaging, there was purulent inflammation in the joint without destruction of the capsule and tendon apparatus (Figure 2).
A 54-year-old woman pricked the index finger of her left hand with a plant thorn while gardening a month ago. The next day, she noted swelling of the nail phalanx and reddening of the skin. She was self-treated using topical antiseptics and oral antibiotics (amoxicillin). The inflammation subsided, but a week ago, swelling and redness of the skin and pain reappeared in the same area. After using ointment dressings, a purulent fistula opened. X-ray showed signs of osteomyelitis in the area of the distal interphalangeal joint (DIP). On examination, there was a purulent fistula in the DIP projection. Intraoperative finding included the destruction of the joint capsule and extensor tendon (Figure 3).
Figure 3.
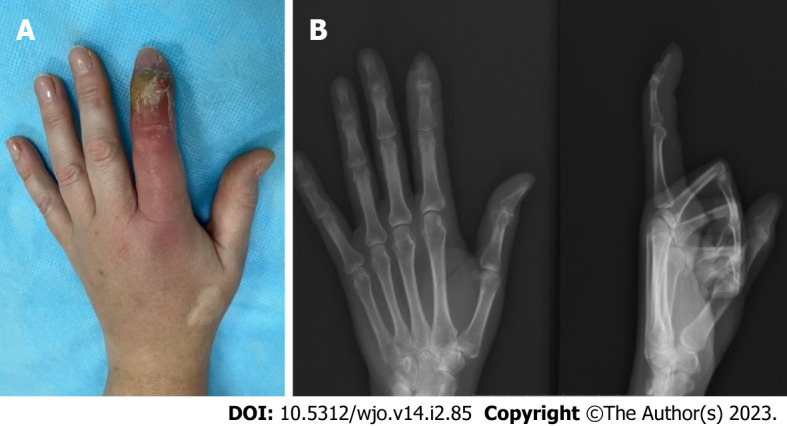
Septic arthritis of the distal interphalangeal joint of the index finger (J1W1T1). A: During hospitalization; B: X-ray.
A 30-year-old man injured his right hand as a result of a blow with a fist in a fight 10 d ago. The patient did not consult a doctor. He treated himself independently with topical antiseptics. During the last few days, the pain increased, the swelling of the hand increased, and the discharge from the wound became purulent. Wound revision revealed damage to the extensor tendon of the finger and a violation of the integrity of the capsule of the metacarpophalangeal joint and purulent exudate in the joint cavity. Upon further diagnostic testing, X-ray showed no evidence of osteomyelitis (Figure 4).
Thus, a specialized classification of septic arthritis of the hand takes into account the main pathological changes that occur in this disease: Destruction of bone and cartilage structures, paraarticular soft tissues, and tendon apparatus. Its use can help in predicting the course of the inflammatory process, determining treatment tactics, and determining the nature and timing of the start of rehabilitation measures. The use of the classification will make it possible to objectify the comparison of the results of treatment of septic arthritis of the hand presented by various authors.
Footnotes
Conflict-of-interest statement: All the authors report no relevant conflicts of interest for this article.
Provenance and peer review: Unsolicited article; Externally peer reviewed.
Peer-review model: Single blind
Peer-review started: November 16, 2022
First decision: November 25, 2022
Article in press: February 7, 2023
Specialty type: Orthopedics
Country/Territory of origin: Russia
Peer-review report’s scientific quality classification
Grade A (Excellent): 0
Grade B (Very good): B, B
Grade C (Good): 0
Grade D (Fair): 0
Grade E (Poor): 0
P-Reviewer: Doski JO, Iraq; Mehta V, India S-Editor: Fan JR L-Editor: Wang TQ P-Editor: Fan JR
Contributor Information
Konstantin V Lipatov, Department of General Surgery, Institute of Clinical Medicine Named After N.V. Sklifosovsky, Sechenov First Moscow State Medical University (Sechenov University), Moscow 119021, Russia. lipatov_k_v@staff.sechenov.ru.
Arthur Asatryan, Department of Wound and Wound Infection Surgery, State Budgetary Institution “City Clinical Hospital named after S.S. Yudin of Moscow Healthcare Department”, Moscow 115446, Russia.
George Melkonyan, Department of General Surgery, Hospital for War Veterans №3, Moscow 129336, Russia.
Aleksandr D Kazantcev, Department of General Surgery, Institute of Clinical Medicine Named After N.V. Sklifosovsky, Sechenov First Moscow State Medical University (Sechenov University), Moscow 119021, Russia.
Ekaterina I Solov’eva, Department of General Surgery, I.M. Sechenov First Moscow State Medical University, Moscow 119048, Russia.
Irina V Gorbacheva, Department of General Surgery, I.M. Sechenov First Moscow State Medical University, Moscow 119048, Russia.
Alexander S Vorotyntsev, Department of General Surgery, I.M. Sechenov First Moscow State Medical University, Moscow 119048, Russia.
Andrey Y Emelyanov, Department of General Surgery, I.M. Sechenov First Moscow State Medical University, Moscow 119048, Russia.
References
- 1.Sendi P, Kaempfen A, Uçkay I, Meier R. Bone and joint infections of the hand. Clin Microbiol Infect. 2020;26:848–856. doi: 10.1016/j.cmi.2019.12.007. [DOI] [PubMed] [Google Scholar]
- 2.McBride S, Mowbray J, Caughey W, Wong E, Luey C, Siddiqui A, Alexander Z, Playle V, Askelund T, Hopkins C, Quek N, Ross K, Orec R, Mistry D, Coomarasamy C, Holland D. Epidemiology, Management, and Outcomes of Large and Small Native Joint Septic Arthritis in Adults. Clin Infect Dis. 2020;70:271–279. doi: 10.1093/cid/ciz265. [DOI] [PubMed] [Google Scholar]
- 3.Lipatov KV, Asatryan A, Melkonyan G, Kazantcev AD, Solov'eva EI, Cherkasov UE. Septic arthritis of the hand: Current issues of etiology, pathogenesis, diagnosis, treatment. World J Orthop. 2022;13:622–630. doi: 10.5312/wjo.v13.i7.622. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Wang J, Wang L. Novel therapeutic interventions towards improved management of septic arthritis. BMC Musculoskelet Disord. 2021;22:530. doi: 10.1186/s12891-021-04383-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Brown H. Hand infections. Am Fam Physician. 1978;18:79–85. [PubMed] [Google Scholar]
- 6.Tan V, Pepe MD, Esterhai JL. Sepsis of the shoulder girdle. In: Disoders of the shoulder: diagnosis and management. Edited by J. Iannotti, G.R. Williams. Philadelphia, Baltimore, New York, London, Buenos Aires, Hong Kong, Sydney, Tokyo. Lippincott Williams and Wilkins, 1998.-P.951-976. In: Habermeyer P, Magosch P, Lichtenberg S editors. Classifications and Scores of the Shoulder. Springer 2006: 179-181. [Google Scholar]