

Introduction
Basal cell carcinoma (BCC) is the most common type of skin cancer. However, it rarely metastasizes. Herein, we present a case of metastatic BCC treated with chemotherapy following vismodegib treatment failure.
Case Presentation
An 82-year-old man visited our clinic for regular follow up due to a personal history of cutaneous BCC which was located on the face. The primary tumor was excised with clear margins 16 months ago and the histopathology report indicated a nodular BCC. Physical examination revealed a swollen lymph node in the right anterior neck. The Fine Needle Aspiration of the lymph node demonstrated the presence of basosquamous BCC (BSC). Due to the presence of headaches, lacrimation and tinnitus, a head MRI and later a PET-CT scan were performed. The latter revealed bones involvement (Figure 1A). Following these findings, vismodegib treatment was initiated. A new PET-CT was performed 3 months later that indicated disease progression (Figure 1B, Figure 2A). Therefore, switch to carboplatin and paclitaxel-based chemotherapy was decided. One month after treatment initiation, the patient did not longer suffer from the symptoms mentioned above. Accordingly, three months later, a new PET-CT was performed, which revealed complete response of the BCC (Figure 2B).
Figure 1.
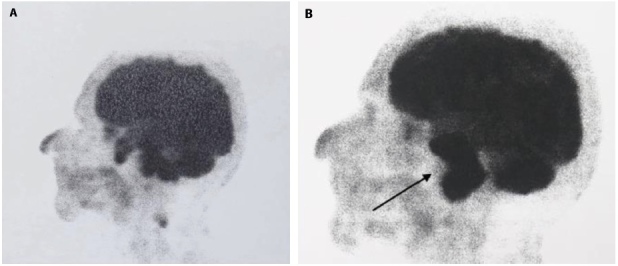
Metastatic BCC. (A) PET-CT at baseline displaying bone involvement and a mass of soft tissue in the skull base invading the clivus, both petrosal bones and the right sphenoid bone. An additional mass of soft tissue is seen to protrude back of the right sphenoid bone to the right sinus. (B) 3 months after vismodegib administration indicating progression of the disease (black arrow).
Figure 2.
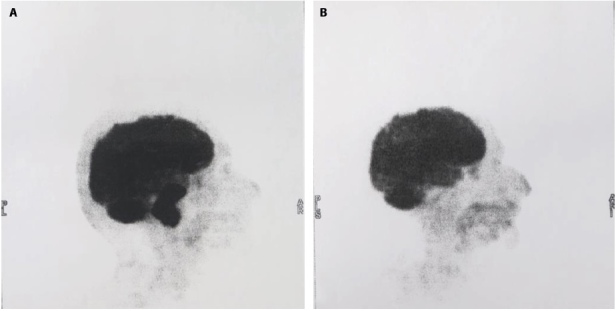
Comparative PET-CTs (A) before and (B) after 3 months treatment with carboplatin combined with paclitaxel (150 mg and 120 mg were administered per week, respectively) revealing complete response and disappearance of the tumor brain metastases.
Conclusions
Although BCCs are very common neoplasms, it is by nature extremely rare to metastasize.
In our patient, the primary tumor was histologically diagnosed as a nodular BCC, whilst histology of the lymph node mass indicated a BSC, which is considered a more aggressive form of BCC. This discrepancy may be attributed to sectioning limitations, not always allowing examination of all the areas of the tumor, in conjunction with the possible coexistence of different areas of differentiation within the tumor mass. Mixed histology is a common scenario, especially in large BCCs. Recent introduction of line-field confocal optical coherence tomography for the in-vivo diagnosis of keratinocyte tumors has improved BCC subtype recognition and its aggressive variants like basosquamous carcinoma. Thus, it could serve as a very helpful tool for clinicians even in such cases to overcome this discrepancy [1,2].
Surgical excision with clear margins is the gold standard of treatment of all BCCs. In contrast, in locally advanced and metastatic BCCs the therapeutic management seems to be limited to the so-called sonic hedgehog pathway inhibitors (HHI), namely vismodegib and sonidegib. However, their use remains controversial in the case of BSCs. Specifically, several studies in the past demonstrated squamatization of BCC in the setting of acquired drug resistance during HHI therapy [3,4]. On the other hand, recent studies have reported complete responses of locally advanced BSCs with vismodegib [5]. In our patient, vismodegib treatment was not beneficial. However, 3-month treatment with carboplatin and paclitaxel led to radiologically confirmed, complete response of the tumor. This is in line with previous evidence suggesting that cisplatin-based chemotherapy may be associated with rapid symptomatic responses [6]. However, despite the brilliant response to the systemic therapy, long term follow-up will be of crucial importance to evaluate the real efficacy of the therapy.
This case report illustrates the clinical challenge of managing patients with metastatic BCC with squamous differentiation and, subsequently, highlights the need of a multidisciplinary approach among the clinicians involved for the patient benefit.
Footnotes
Funding: None.
Competing Interests: None.
Authorship: All authors have contributed significantly to this publication.
References
- 1.Cappilli S, Dejonckheere G, Hajjar N, et al. Line-field confocal optical coherence tomography: a case on the importance of full-lesion examination for basal cell carcinoma. Int J Dermatol. 2022;61(7):e248–e250. doi: 10.1111/ijd.15930. [DOI] [PubMed] [Google Scholar]
- 2.Cappilli S, Cinotti E, Lenoir C, et al. Line-field confocal optical coherence tomography of basosquamous carcinoma: a case series with histopathological correlation. J Eur Acad Dermatol Venereol. 2022;36(8):1214–1218. doi: 10.1111/jdv.18038. [DOI] [PubMed] [Google Scholar]
- 3.Iarrobino A, Messina JL, Kudchadkar R, Sondak VK. Emergence of a squamous cell carcinoma phenotype following treatment of metastatic basal cell carcinoma with vismodegib. J Am Acad Dermatol. 2013;69(1):e33–e34. doi: 10.1016/j.jaad.2013.01.023. [DOI] [PubMed] [Google Scholar]
- 4.Bancalari B, Llombart B, Serra-Guillén C, et al. Histologic Changes During Treatment With Vismodegib in Locally Advanced Basal Cell Carcinoma: A Series of 19 Cases. Am J Dermatopathol. 2019;41(10):711–717. doi: 10.1097/DAD.0000000000001384. [DOI] [PubMed] [Google Scholar]
- 5.Apalla Z, Giakouvis V, Gavros Z, et al. Complete response of locally advanced basosquamous carcinoma to vismodegib in two patients. Eur J Dermatol. 2019;29(1):102–104. doi: 10.1684/ejd.2018.3482. [DOI] [PubMed] [Google Scholar]
- 6.Jefford M, Kiffer JD, Somers G, Daniel FJ, Davis ID. Metastatic basal cell carcinoma: rapid symptomatic response to cisplatin and paclitaxel. ANZ J Surg. 2004;74(8):704–705. doi: 10.1111/j.1445-1433.2004.03130.x. [DOI] [PubMed] [Google Scholar]