

Practice Gaps
Although most pediatricians are regularly confronted with patients with unusual movements or spells, it can be difficult to distinguish seizures, movement disorders, and variations of normal behavior.
Although statistics are not readily available, other movement disorders, such as tic disorders, may be confused with chorea.
Acute cerebellar ataxia is not universally benign, and treatment should be considered for children with this diagnosis.
Objectives
After completing this article, readers should be able to:
Recognize common and/or important movement disorders relevant to contemporary pediatric practice.
Provide appropriate management of common childhood movement disorders and recognize when subspecialist referral may be necessary.
Case Study
A previously healthy 7-year-old boy is admitted to the pediatrics ward for evaluation and management of abnormal movements that have progressed during the last few days. The child was transferred from a rural area of the state after being seen in a local emergency department. Antistreptolysin O titers are greater than 420 U/mL. The boy’s parents became concerned after he began displaying frequent shoulder shrugging, rapid elbow extension, facial grimacing, and snorting behavior. On examination, the child is lucid but anxious and readily exhibits the movements of concern. Your resident asks if she should order intravenous immunoglobulin for treatment of Sydenham chorea.
Introduction
Pediatricians are often confronted by parents puzzled or concerned about “weird things” their children are doing. Patients with movement disorders typically present first to primary care clinics. Childhood movement disorders are surprisingly common, and pediatric movement disorders clinics are now a fixture in many major medical centers. Although subspecialist referral is certainly appropriate in many cases, in others, the pediatrician may play a key role in diagnosing and managing the child’s abnormal involuntary movements.
In managing movement problems in children, arriving at the correct diagnosis is crucial to perform an appropriate workup and develop a proper management plan. In some cases, movement disorders merely need to be recognized as benign and distinguished from events such as seizures. In other cases, movement disorders can severely impair the affected child’s quality of life (ie, in the case of tic disorders or chorea) or can themselves be directly life-threatening (as in status dystonicus).
In diagnosing movement disorders, phenomenology (how the disorder appears to the observer) is crucial. Paroxysmal movement disorders, where the child’s abnormal movements characteristically come and go, can be particularly challenging to diagnose. In such cases, the physician is often not able to directly observe the abnormal movement that has alarmed the child’s parents. Although a detailed description (along with a demonstration by the parent, if possible) of the entire episode can be useful in such circumstances, in many cases diagnosis may be difficult without video documentation. Fortunately, parents are often able to capture footage of their child’s movements if requested to do so, and this can be reviewed by the pediatrician and/or shared with a consulting pediatric neurologist.
Movement disorders in childhood are distinct from those seen in adults in terms of pathogenesis and even treatment. However, childhood movement disorders can still be classified in terms of whether the disorders are distinguished by a paucity of movement (hypokinetic) or characterized by excessive or exaggerated movement (hyperkinetic). In general, hyperkinetic movement disorders predominate in children. In addition to the causes listed below, drugs of abuse, particularly stimulants in the adolescent patient, should be considered as potential causes of hyperkinetic movement disorders.
Hypokinetic Movement Disorders
Parkinsonism (Slowness)
Parkinsonism, the cardinal hypokinetic movement disorder, is rare in children. Parkinsonism is characterized by slowed movements (bradykinesia) and a paucity of movement (akinesia) in addition to cogwheel rigidity on examination of muscle tone. A resting tremor due to parkinsonism is often not seen in childhood, even if other features of parkinsonism are present.
Primary parkinsonism (juvenile Parkinson disease, with onset before age 21 years) is typically caused by single-gene mutations. When juvenile parkinsonism is encountered, it is often part of a mixed movement disorder (eg, dystonia-parkinsonism) manifesting as a feature of neurodegenerative disease (ie, lysosomal storage disease, Wilson disease, mitochondrial encephalopathy, and juvenile Huntington disease). Drug-induced parkinsonism is more common and is most often encountered as an adverse effect of neuroleptic (antipsychotic) medications, such as phenothiazines, clozapine, quetiapine, olanzapine, and risperidone. Parkinsonism can also be seen in infectious and autoimmune forms of encephalitis.
Hyperkinetic Movement Disorders
Ataxia (Drunkenness)
Ataxia (lack of muscle control during voluntary movements) is one of the most common movement disorders in the pediatric population and is an important entity for the pediatrician to be familiar with. Ataxia is most commonly caused by dysfunction of the cerebellum but also occurs as a manifestation of proprioceptive sensory loss (typically related to diseases of the peripheral nerves or posterior columns of the spinal cord). Sensory ataxia can be distinguished from cerebellar ataxia by concurrent findings of sensory impairment; such patients often look to their feet when ambulating given their uncertainty regarding their own position in space. Ataxia leads to imprecise movements, and affected patients will classically have past-pointing (dysmetria), difficulty with controlling the tempo and amplitude of arm, finger, or leg movements, and an impaired ability to generate rapid, alternating movements. Video 1 depicts a patient with ataxia.
Video 1.
Click here to view the video. An 8-year-old girl with acute cerebellar ataxia performing rapid alternating pronation-supination, attempting to generate rotating movements of the wrists (resulting in irregular amplitude and erratic control), and walking down the hallway (illustrating a stumbling, lurching gait).
Examination of the Child With Cerebellar Ataxia
Ataxia may be elicited in young children by engaging them in play with blocks or observing their spontaneous reach for toys. Children with cerebellar ataxia may exhibit an intention tremor that gets worse when nearing a target. Having a child drink from an open cup can be helpful in evaluating ataxia, and evaluating gait is paramount even in the hospitalized patient. An ataxic patient may perform slightly better on finger-to-nose testing if a pulse oximeter is in place on the affected hand.
Truncal ataxia and/or head nodding (titubation) may be observed even when a child is sitting. When walking, ataxic children tend to adopt a wider station to compensate for their instability. When going down a hallway, children with ataxia will often appear drunk or lurching and bounce from wall to wall. Cerebellar lesions may affect speech production (leading to diminished expressive speech or scanning speech), prompting parents to state their child’s speech is slurred.
Mimics of Ataxia
Myoclonus (rapid jerks that occur singly or in clusters) can resemble ataxia, particularly if exacerbated by activity, and these conditions can be difficult to distinguish. Fortunately, myoclonus is relatively rare. More commonly, acute-onset weakness can mimic ataxia, and important differential considerations include Guillain-Barré syndrome and transverse myelitis. These conditions can be distinguished by the presence of dropped reflexes (seen in Guillain-Barré syndrome or acute transverse myelitis) or hyperreflexia or bowel and/or bladder dysfunction (seen in transverse myelitis).
Differential Diagnosis
An important distinguishing factor among causes of ataxia is whether the movement disorder is acute or chronic. In the case of acute ataxia, signs of altered mental status and/or elevated intracranial pressure are important indicators of occult trauma or hemorrhage. Acute ataxia is a frequent finding in toxic ingestions; common culprits include anticonvulsants including benzodiazepines, alcohols, essential oils (tea tree or eucalyptus), cough syrups (dextromethorphan), and drugs of abuse. Opsoclonus-myoclonus syndrome (OMS) often features ataxia, and in some cases, this may be the only movement disorder present. Encephalitis may cause ataxia, particularly in the case of varicella zoster. Autoimmune encephalitis may also lead to ataxia. Posterior fossa tumors, including medulloblastomas and gliomas, often present with ataxia. In such cases, the ataxia may be acute (ie, if there is an associated hemorrhage) but more often present indolently.
Acute Cerebellar Ataxia
Acute cerebellar ataxia is a relatively common postinfectious and autoimmune form of ataxia that predominantly occurs in preschool and school-aged children. Acute cerebellar ataxia is a diagnosis of exclusion because currently there is no clinically available confirmatory test. There is often a history of antecedent infection. Neuroimaging results are generally normal, and cerebrospinal fluid study findings are typically unremarkable, although oligoclonal bands (indicating active antibody synthesis within the central nervous system), if present, offer a helpful clue. The natural history of this condition is often benign and self-limited, with most children recovering within weeks to months without intervention. However, for 10% to 20% of children, their recovery may be incomplete, and these children may have lasting neurologic deficits that affect balance and coordination. (1) For this reason, treatment with high-dose intravenous corticosteroids and/or intravenous immunoglobulin should be considered once a diagnosis of acute cerebellar ataxia is made because it is not currently possible to determine which children will have a benign course from those who will have permanent sequelae. Miller Fisher syndrome, a form of Guillain-Barré syndrome that leads to prominent sensory ataxia, may mimic acute cerebellar ataxia and can also be treated with intravenous immunoglobulin.
Chronic Ataxias
Chronic ataxia may result from a number of inherited disorders, including a variety of neurometabolic disorders, the spinocerebellar ataxias, Friedreich ataxia, and ataxia telangiectasia. Nutritional deficiencies, including inadequate vitamin E, zinc, vitamin B12, and folate, may lead to ataxia. Gluten encephalopathy is a controversial entity associated with autoantibodies against gliadin or transglutaminase in some patients (2) and diverse neurologic symptoms, which may include ataxia. Some of these patients may respond to a gluten-free diet.
Treatment
Treatment for symptoms of ataxia is largely supportive, although identifying the cause of ataxia may facilitate treatment directed at the underlying cause. This is particularly true in cases wherein a restriction diet (eg, gluten encephalopathy) or a specific treatment (eg, vitamin E) may be available.
Dystonia (Twisting or Posturing)
Dystonia is characterized by concurrent activation of agonist and antagonist muscles, resulting in abnormal twisting and posturing movements. Dystonia can be focal (the best known example of this is cervical dystonia or torticollis) or generalized. Dystonia may occur at rest but is often provoked by action, and asking patients to perform simple activities, such as holding the hands outstretched with fingers spread apart, may be informative. In some patients, the dystonia is remarkably task specific, as in the case of musician’s dystonia (dystonia that affects the hand and is caused by performing repeated hand movements). Patients with dystonia may develop a sensory trick (such as placing their palm on the side of the head) that profoundly alleviates their dystonia. Dystonia can severely interfere with function, affecting a patient’s ability to eat, speak, or ambulate, and can be painful, particularly if prolonged. In extremis, uncontrolled dystonia (status dystonicus) can lead to rhabdomyolysis and renal failure. A patient with generalized dystonia is featured in Video 2 .
Video 2.
Click here to view the video. A 15-year-old boy with generalized dystonia due to mutation in DYT6. Note the irregular posturing of the hands and fingers. After deep brain stimulation surgery and programming, this patient regained the ability to walk.
Acute Dystonic Reactions
Acute dystonic reactions are sometimes seen in the context of metoclopramide or neuroleptic use (including agents such as prochlorperazine commonly used for nausea or vertigo) and can cause alarming symptoms, such as blepharospasm, opisthotonus (a form of dystonia with involuntary hyperextension of the arms, legs, and spine), spasms of the tongue and jaw, trunk, extremities, and laryngospasm. Fortunately, these medication reactions typically respond to anticholinergics and antihistamines, such as diphenhydramine. Benzodiazepines may be administered in refractory cases. An acute dystonic reaction should typically prompt a change to an alternate medication.
Chronic Dystonia
Chronic dystonia will most frequently be encountered in the context of children with extrapyramidal forms of cerebral palsy and can sometimes overlap with spasticity in such patients. Both hypoxic-ischemic injury and kernicterus can lead to dystonic forms of cerebral palsy. These children often have demonstrable injury to the basal ganglia on neuroimaging (Figure 1).
Figure 1.
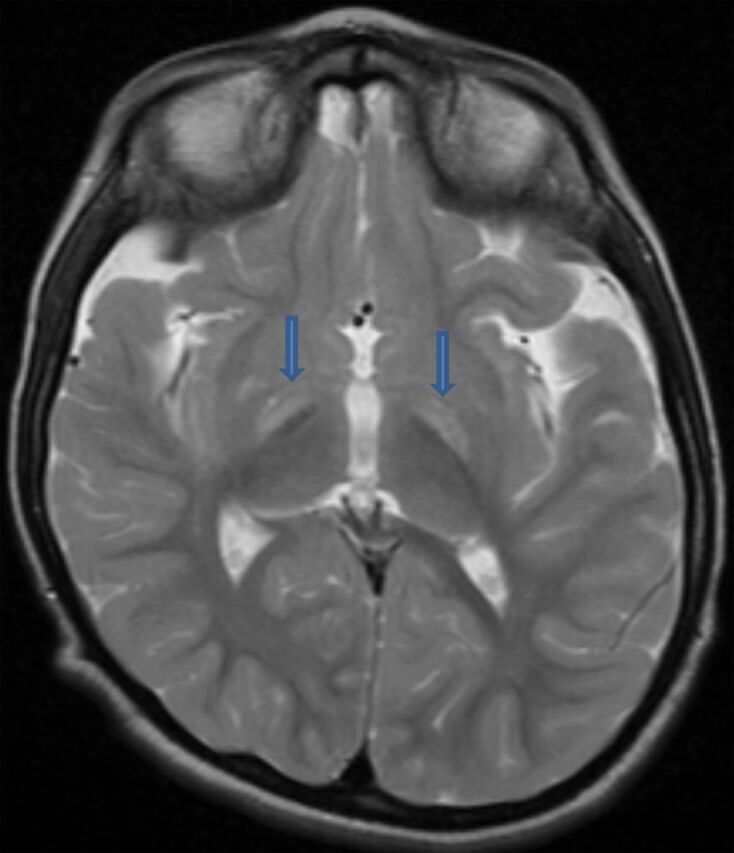
Basal ganglia deposition of bilirubin (arrows) as revealed by brain magnetic resonance imaging.
Other children with dystonia may be divided into 1 of 2 categories. The first category encompasses the increasing number of mendelian forms of primary dystonia. Although clinical features vary, most patients with primary dystonia have symptom onset in the teens, and their dystonia gradually generalizes, often severely limiting function. Affected patients typically have normal intellect, although their ability to communicate may be impaired, leading their peers to make inaccurate assumptions as to their abilities.
The secondary dystonias include forms of dystonia related to cerebral palsy, neurodegenerative disease, brain injury, or cortical maldevelopment. Such children often have seizures or other neurodevelopmental disabilities.
Treatment
Oral treatment options are focused on ameliorating dystonia and include trihexyphenidyl and baclofen. Botulinum toxin therapy is the mainstay of treatment for focal dystonias but is not often a good option for more generalized symptoms. For generalized dystonia, surgical options include intrathecal or intraventricular baclofen pump implantation. Deep brain stimulation may substantially improve an affected child’s quality of life in carefully selected patients and is being performed in more and more centers.
Dopamine-Responsive Dystonia
Dopamine-responsive dystonia is a rare genetic disorder that is nevertheless important to consider because this is one of the few disorders for which appropriate recognition and treatment with levodopa can help affected children “get up out of their wheelchairs and walk.”
Chorea-Athetosis (Writhing)
Chorea describes near-continuous irregular movements with a writhing or dancelike quality, whereas athetosis refers to similar movements of larger amplitude. Current consensus definitions consider chorea and athetosis as points on a spectrum. True chorea is uncommon in children, although stereotypies, frequent tics, myoclonus, and psychogenic disorders may resemble chorea. A patient with chorea is depicted in Videos 3A and 3B.
Video 3A.
A 6-year-old girl with intermittent chorea of uncertain etiology, presented before treatment (3A, click here) and after (3B, click here) treatment with tetrabenazine.
Video 3B.
A 6-year-old girl with intermittent chorea of uncertain etiology, presented before treatment (3A, click here) and after (3B, click here) treatment with tetrabenazine.
Chorea is most often encountered in children with a history of hypoxic-ischemic injury, resulting in cerebral palsy with injury to the basal ganglia. In such children, chorea may coexist with other movement disorders, such as dystonia. The most frequent cause of new-onset chorea in children is probably Sydenham chorea, which is defined as chorea occurring in the context of active streptococcal infection. Sydenham chorea is believed to result from molecular mimicry, wherein antistreptococcal antibodies have cross-reactivity to basal ganglia antigens. Currently, Sydenham chorea is rare in developed countries. Chorea usually develops 1 to 2 months after infection. It is typically bilateral, but unilateral cases may occur. Associated symptoms may include hypotonia, facial dystonia, dysarthria, and motor impersistence (wherein the child will fail to maintain a grip on the physician’s hand or unable to keep their tongue out when asked to do so). Concurrent neuropsychiatric symptoms are often seen. Rheumatic carditis and arthritis often co-occur, although chorea may be the only presenting sign of rheumatic fever in approximately 20% of patients. Chorea typically improves spontaneously, although many patients have incomplete resolution of their symptoms, sometimes with disabling, persistent chorea. Chorea may respond to high-dose intravenous methylprednisolone (30 mg/kg daily for 5 days), plasma exchange, and/or intravenous immunoglobulin (2 g/kg divided during 2–5 days). The American Academy of Pediatrics Red Book criteria for the diagnosis and treatment (including prophylaxis) of rheumatic fever can be found in Table 1 and Table 2.
Table 1.
Jones Criteria for Diagnosis of Acute Rheumatic Fever

Table 2.
Duration of Prophylaxis for People Who Have Had Acute Rheumatic Fever (ARF): Recommendations of the American Heart Associationa

Healthy infants have physiologic chorea at approximately age 6 months. Metabolic causes of chorea can include hypoglycemia or hyperglycemia, hyponatremia or hypernatremia, hypocalcemia, and hyperthyroidism. Postpump chorea is an important entity to consider in children presenting with consistent movements after cardiopulmonary bypass. Pediatric autoimmune neuropsychiatric disorder associated with streptococcus (PANDAS) and the recently proposed entity pediatric acute-onset neuropsychiatric syndrome (PANS) remain a controversial topic without likely resolution in the near future given the lack of definitive diagnostic tools and the extremely high colonization rate of group A Streptococcus in pediatric patients. Children with attention-deficit/hyperactivity disorder (ADHD), learning disabilities, and/or dyspraxia (developmental coordination disorder) will often exhibit choreiform movements with hands outstretched during physical examination as a neurologic soft sign. This condition must be distinguished from true chorea by the magnitude of movements and the degree of functional impairment that occurs with true chorea. Chorea often responds best to treatment with tetrabenazine, although this is an off-label use outside the context of Huntington chorea.
Stereotypy (Behaviors)
Stereotypies are consistent, rhythmic, repetitive movements without clear purpose and include finger rubbing, hand flapping, head shaking, mouth posturing, vocalizing, and rocking behavior. They can appear very early in development (within the first year of life). Stereotypies have been conceptualized as a means to redirect a state of arousal, but evidence also suggests that stereotypies are heritable to some degree. Video 4 depicts a patient with complex stereotypies.
Video 4.
Click here to view the video. A 2-year-old boy with hand-flapping and mouth-opening stereotypies.
Stereotypies are more frequent in children with primary sensory deprivation (visual or hearing-impaired children) or in those subjected to severe neglect. Children with stereotypies are more prone to exhibit learning disabilities, ADHD, dyspraxia, and depression or anxiety, (3) but stereotypies can occur in neurodevelopmentally normal children as an isolated finding. Hand-flapping behaviors in a child with autism or midline hand-wringing in a child with Rett syndrome are examples of stereotypies. Stereotypies often occur when a child is excited or may occur during downtimes, such as when a child is quietly reading or playing. Stereotypies are generally benign and tend to recede as a child reaches school age, possibly as the child becomes more aware of social implications of his or her stereotypies. Those children whose stereotypies persists are prone to be teased and bullied by others, particularly if the stereotypy is more dramatic, such as jumping and hand flapping. Although most stereotypies do not require treatment, the movements may respond to neuroleptics, and emerging evidence suggests that cognitive-behavioral approaches that emphasize habit reversal training may also be effective for stereotypies. (4) Stereotypies can be distinguished from tics by their lack of a premonitory sensation and their relatively consistent nature over time (vs the waxing and waning typical of tics). Stereotypies can be differentiated from paroxysmal dystonias and choreoathetosis by their phenomenology. Complex partial seizures can be challenging mimics of stereotypy. Important distinguishing features include the fact that children can typically be distracted from their stereotypies and redirected to other activities and the recognition that stereotypies do not lead to postictal symptoms.
Tics
Tics represent repetitive stereotyped vocalizations or movements that occur in up to 1 of 5 children at some point in their life. Tics are thus quite common and often do not come to medical attention (although they may persist into adulthood as nervous habits or mannerisms). Tics can be frequent enough to mimic chorea and can have a twisting or posturing quality to them (so-called dystonic tics). The velocity of a tic is slower than myoclonus. Tics commonly manifest during school age and may worsen during adolescence. They are uncommon in the preschool age, and an alternative cause should be sought for an unusual movement within the first 2 years of life. A variety of tics are presented in Videos 5, 6, and 7.
Video 5.
Click here to view the video. A 10-year-old girl with simple phonic (sniffing) and motor (grimacing) tics.
Video 6.
Click here to view the video. A 9-year-old boy with a blocking tic when reading aloud. After reading much of a paragraph containing age-appropriate material, the word that stalls the patient is “the.”
Video 7.
Click here to view the video. A 7-year-old boy illustrating a more complex motor tic, consisting of elbow extension and wrist flinging.
Tics may occur in bouts during a day, and for some, precipitants, such as stress or anxiety, can be identified. For other affected children, the tics are sometimes worse after school, when they are relaxing and watching television or having a snack. This may be because the child has been suppressing the tics as much as possible during the school day (see below) only to “let them out” in a safe environment, such as the home. Tics may persist during sleep.
Tourette Syndrome
Tics are divided into phonic and motor manifestations, and it is common for a child to have both phonic and motor tics, although many times parents do not recognize phonic tics as such. If both phonic and motor tics are present for more than 1 year, a diagnosis of Tourette syndrome may be made. It is important to recognize that the severity of the tic disorder is not weighted in making a diagnosis of Tourette syndrome, and for many children with Tourette syndrome, their tics may be relatively mild. This diagnosis must be made with sensitivity because it may upset parents, who often carry preconceptions about Tourette syndrome.
Related Disorders
Tics form part of a larger neurobehavioral phenotype that includes ADHD, mood disorders, learning disabilities, and obsessive-compulsive disorder. Tics are also often seen in patients with autism spectrum disorders. Tics have a male-female sex bias of 4:1. Tourette syndrome and related comorbidities are highly heritable and may run in families in an autosomal dominant manner, but with markedly variable penetrance. In this regard, the family history can be a helpful clue as to the cause of the child’s abnormal movements. In taking the history, one may learn of a grandfather with a need to flush every toilet before leaving the house (obsessive-compulsive disorder), a father with poor school performance (related to ADHD and dyslexia), and a son with tics and anxiety. Despite the high incidence of these disorders in the population, the responsible genes have not been identified.
Phonic Tics
Common phonic tics may include repetitive sniffing (often misdiagnosed as allergy related), throat-clearing, snorting, or coughing. Other common phonic tics include humming or brief vocalizations, such as high-pitched shrieks. Coprolalia (uttering obscenities) is a feared but fortunately rare complex phonic tic. Other complex phonic tics include stereotyped changes in pitch or volume, palilalia (repeating one’s own words), or echolalia (repeating others’ words). Blocking tics are examples of tics that manifest as negative phenomena, in this case interrupting an otherwise fluent train of speech. Blocking tics can be challenging to differentiate from stuttering, although the vocal cadence in the 2 disorders is distinct. Phonic tics as a group are often misinterpreted in schools, and it is not uncommon for children to see their physician only after multiple trips to the principal’s office.
Motor Tics
Motor tics commonly include forced eye blinking, facial grimacing, widening the eyes, shoulder shrugging or rolling, and neck extension. Complex motor tics are composed of more elaborate but nevertheless stereotyped, repetitive, purposeless movements, such as foot tapping while walking, truncal posturing, or punching oneself. The recognition of complex motor tics may be facilitated by the company they keep, namely, more common tics, such as sniffing and forced blinking. Examples of phonic and motor tics are summarized in Table 3.
Table 3.
Tic Subtypes
| Motor Tics | Complex Motor Tics | Vocal Tics | Complex Vocal Tics |
| Forced blinking | Jumping | Sniffing | Shrieking |
| Eyebrow raising | Teeth baring | Throat-clearing | Coprolalia |
| Facial grimacing | Lip chewing | Coughing | Blocking tics |
| Exaggerated eye opening | Punching oneself | Whistling | Repeating oneself or others |
| Neck jerking | Foot shaking, stomping or tapping | Humming | Abrupt changes in volume or prosody |
| Broadening nostrils | Tensing the abdomen | Spitting | |
| Shoulder jerking | Tapping or touching of self or objects | ||
| Shoulder shrugging |
Natural History
Tics may be transient in some children and not recur. For others, their tics intrinsically wax and wane in severity without treatment on a time scale of weeks to months, and it is not uncommon for one tic to fade only to be replaced by another or even for a child’s tics to abate spontaneously for a time only to return later. Stimulants may worsen a child’s tics or even provoke new tics to manifest; however, there is little evidence that stimulants cause tics in those who do not have an underlying susceptibility. The natural history of tics is generally reassuring, with the rule of thirds dictating that approximately one-third of children will have cessation of their tics by the time they graduate high school, one-third of children will have stable and improved tics, and only one-third will have persistent tics that adversely affect their quality of life. (5)
Tic Phenomenology
Tics are classically preceded by a premonitory sensation, which the affected child may variably describe as a twinge, tickle, tingle, or tight feeling or as a vague sense of discomfort. Children younger than 10 years are often unaware of this premonitory sensation and/or may struggle to describe it unless specifically asked to report what they feel before their movements. In addition, although older children may feel validated by their description of their struggles with tics, younger kids may lack the self-awareness needed to explain why they exhibit these unusual movements.
As a rule, tics are briefly suppressible, and this feature may be very helpful in clinching the diagnosis. Although most older children will acknowledge that their tics may be suppressed for a short while, they are also quick to point out that after a short period their premonitory sensation grows more and more intolerable, with a building sense of internal tension “like an itch that you try not to scratch.” Indulging the tic temporarily relieves that sense of tension, but the relief is short-lived as the premonitory sensation inevitably recurs. A vicious cycle ensues.
Diagnosis
Parents may be counseled that tics are common, and although neurologic in nature, they are only rarely associated with an underlying endocrine (ie, hyperthyroidism) or neurologic origin (ie, neurodegenerative disorder, such as juvenile Huntington disease).
Treatment
In determining when and how to treat tics, it is important to discuss with the family that tics are seldom a sign of a more serious neurologic disorder, and they are only rarely inherently dangerous (exceptions exist because whiplash neck jerking tics may occur and eye blinking may be so severe that it interferes with the child’s ability to ride his or her bike or drive a car safely). In younger children, tics do not typically lead to much social distress. However, by the time a child reaches third grade, teasing or bullying related to tics can affect a child’s self-esteem and contribute to feelings of depression or social anxiety. Children dealing with these social implications of their tics, even if inherently shy, may be quite vocal in telling their pediatrician whether their tics need to be treated.
Comprehensive Behavioral Intervention for Tics
If treatment is undertaken, comprehensive behavioral intervention for tics is a structured cognitive-behavioral therapy–based training program for tics that develops a child’s self-awareness so the child can recognize premonitory sensations. The child then works with a therapist (often a child psychologist or occupational therapist) to develop a competing response that will replace the tic with a tic-incompatible behavior. This therapy is quite successful for children with the insight and motivation required to complete the program, and ongoing training programs for practitioners are being conducted on a regular basis with strong support from the Tourette Syndrome Association.
Several good medication options also exist. α2-Adrenergic agonists, such as clonidine and guanfacine, are often helpful in reducing tic frequency and severity. They have the added benefit of treating concurrent ADHD, if present. However, for children with more severe tics, low-dose topiramate (50 mg nightly) may lead to more sustained benefit, often with few adverse effects. Typical (fluphenazine and pimozide) and atypical neuroleptics (risperidone and aripiprazole) may also be effective in treating tics. Realistic treatment expectations are important to communicate because tics seldom completely disappear. Nevertheless, families are often satisfied if their child’s most troublesome tics are ameliorated by treatment.
Myoclonus (Jerking)
Myoclonus is characterized by rapid jerks, which can occur singly or in clusters. Most everyone has experienced hypnic jerks, which occurs when one is just drifting off to sleep, only to be jolted awake. This form of myoclonus is physiologic, but myoclonus that occurs during wakefulness is pathologic and may be either epileptic or nonepileptic in origin. Epileptic myoclonus may occur as a manifestation of generalized epilepsy. Nonepileptic myoclonus can be challenging to localize because myoclonus can occur as a result of lesions anywhere in the neuraxis. Video 8 illustrates myoclonus.
Video 8.
Click here to view the video. A 3-year-old girl with myoclonus related to a frontal lobe brain tumor that was successfully resected, leading to cessation of her movements.
Opsoclonus-Myoclonus Syndrome
Myoclonus is rare in childhood, but a notable cause of myoclonus is OMS (sometimes called opsoclonus-myoclonus-ataxia syndrome given the ataxia that many affected patients exhibit). This disorder typically arises as a paraneoplastic autoimmune phenomenon in association with a neuroblastoma. As the immune system mounts a response to the neoplastic cells, normal central nervous system tissue comes under “friendly fire,” leading to the characteristic erratic eye movements (opsoclonus) and multifocal myoclonic jerks typical of the disorder. The new onset of opsoclonus, myoclonus, and/or ataxia should prompt consideration of this diagnosis. The underlying neuroblastoma (which sometimes is not directly symptomatic itself) can usually be detected by analysis of serum or urine catecholamines. In the child with opsoclonus or myoclonus and a negative metabolite screening result, subspecialist referral is warranted, and in some cases, morphologic (computed tomography or magnetic resonance imaging) or nuclear ([18F]-fluorodeoxyglucose [18F-FDG] or [123I]-metaiodobenzylguanidine [123I MIBG]) imaging may be appropriate. In the child presenting with solely ataxia, other causes should be considered. If both a neuroblastoma and OMS are present, each requires specific treatment, with immunotherapy benefiting OMS. In addition, both genetic and autoimmune mimics of OMS have recently been described.
Tremor (Oscillations)
Tremor is characterized by a sinusoidal oscillation about a central point. Multifocal myoclonus can mimic tremor. Resting tremor, commonly seen in parkinsonism in adults, is rare in children. A kinetic tremor is a tremor that is more prominent with volitional movement. Ataxia is associated with an intention tremor, a specific form of kinetic tremor that gets worse as the target is neared. Kinetic tremor can be seen in children with neurodevelopmental disabilities and may be persistent and interfere with normal functioning. A child with tremor is presented in Video 9 .
Video 9.
Click here to view the video. An 11-year-old boy with mild kinetic tremor. The phenomenology and family history were consistent with essential tremor.
Essential Tremor
Essential tremor, the most common movement disorder worldwide, can occur at any age in the pediatric population but presents most frequently in adolescents. Essential tremor classically leads to a kinetic tremor of the hands, although the head and neck, legs, and voice can be involved. Essential tremor is autosomal dominant with incomplete penetrance, and so a family history can help confirm the diagnosis. β-Blockers or topiramate can be helpful treatments.
Special Cases
Paroxysmal Movement Disorders
Paroxysmal movement disorders describe conditions that lead to episodic movement abnormalities. Affected patients are largely asymptomatic between attacks. This group of disorders includes paroxysmal torticollis, the episodic ataxias, and paroxysmal dyskinesias (which largely lead to dystonia or choreoathetosis). Some forms of paroxysmal movement disorders have previously been classified as migraine variants; however, advances in genetics have indicated that mutations in genes that control neuronal excitability may variably lead to either migraine with or without hemiplegia or episodic movement disorders. (6) The diagnosis of these disorders can be challenging; video documentation or direct observation of spells is often required. The paroxysmal movement disorders can respond to migraine prophylaxis, acetazolamide, or sodium channel blocking anticonvulsants (eg, oxcarbazepine). A boy with paroxysmal dyskinesia is depicted in Video 10 .
Video 10.
Click here to view the video. A 16-year-old boy who developed the dystonic movements featured after prolonged standing or abruptly rising from a seated position.
Movement Disorders in Infants and Toddlers
Several special cases affecting young children bear mentioning. These are disorders that can be distressing to parents yet remarkably benign or conversely can escape parents’ radar yet carry an ominous prognosis. For example, infantile spasms are often not recognized by parents yet these seizures require a high index of suspicion to ensure that an appropriate workup is conducted and treatment plan initiated.
Benign Neonatal Sleep Myoclonus
Infants may exhibit myoclonic movements during sleep (not just at sleep-wake transitions) very early in life. If the myoclonus does not occur during wakefulness and occurs in the context of an otherwise healthy and neurodevelopmentally normal child, the parents can be reassured. Electroencephalograms capturing these spells are characteristically normal, and the long-term outcome for children with this condition is generally quite good. Video 11 shows an infant with this condition.
Video 11.
Click here to view the video. An infant with benign neonatal sleep myoclonus was identified in the newborn nursery, where astute nurses captured video.
Sandifer Syndrome
The movements and posturing (arching of the back and rigid opisthotonic posturing) that infants with gastroesophageal reflux can sometimes exhibit may mimic seizures or dystonia. When the child’s movements are found to correlate with episodes of reflux, a diagnosis of Sandifer syndrome is appropriate. Treatment of the underlying reflux leads to resolution of the movement disorder.
Autostimulation
Many children, not confined by social conventions, will exhibit odd posturing and writhing behavior against a carpet or bed that represents childhood masturbation. Although this diagnosis requires tactful discussion with parents, it is actually fairly common and likely to be brought to the primary care pediatrician’s attention. It can be treated as a behavior rather than a true movement disorder.
Tardive Syndromes
From 2005 to 2009, nearly 4% of all outpatient office visits for adolescents were associated with treatment with an antipsychotic medication. (7) Although effective in many children with autism spectrum disorder, behavior disorders, and tics, prolonged antipsychotic medication use carries the risk of provoking a tardive (late-onset) movement disorder. Tardive forms of tics, dystonia, and parkinsonism can occur, as well as other unusual hyperkinetic syndromes (eg, akathisia, which is characterized by an overwhelming sense of internal restlessness that leads to near-constant movement). The mechanisms that lead to tardive syndromes are poorly understood. Risks are higher with traditional than with newer neuroleptics, but the risk of developing a tardive syndrome in childhood (or in adulthood as a result of childhood neuroleptic use) is not well studied. The usual treatment for tardive syndromes involves cessation of the offending medication, which may improve symptoms, but unfortunately, tardive symptoms may be permanent. In such cases, benzodiazepines or off-label treatment with tetrabenazine may be helpful.
Functional Movement Disorders
Functional (or psychogenic) movement disorders represent a diagnosis of exclusion, and affected patients can be among the most difficult to properly diagnose and treat. Functional movement disorders may take a variety of forms, including flailing, arm waving, unusual speaking patterns, or abnormal gaits. They are distinguished from typical movement disorders by their atypical and sometimes elaborate phenomenology and by associated findings (ie, affected patients may exhibit la belle indifference, a surprising degree of unflappability despite, for example, severe symptoms that have led to cessation of normal activities and hospitalization). Other common findings include inconsistent or fluctuating phenomenology and distractibility of the movements.
Some patients initially diagnosed as having functional movement disorders are later found to have an organic cause, so periodic reevaluation is important. Many others improve with appropriate treatment for functional conditions (see below). Patients with functional movement disorders often have mood disorders, but some do not. It is not uncommon to find a history of abuse, either physical or sexual, in such patients. It is also not uncommon for friends or other family members of the patient to have either a severe neurologic disease or unexplained symptoms of some kind.
The best manner in which to share this diagnosis with the patient and family is controversial. It is often important to emphasize that functional does not equate to factitious or malingering and that the patient’s symptoms are very real but simply not referable to a severe organic brain disease (such as a brain tumor). Many patients with functional movement disorders will have relapses and typically benefit from longitudinal psychotherapy. Many will also benefit from antidepressant medications, even in the absence of a formal mood disorder. (8) An example of a functional movement disorder is shown in Video 12.
Video 12.
Click here to view the video. A 12-year-old girl with psychogenic movement disorder. The phenomenology of these movements was not consistent with a recognizable movement disorders.
Summary.
On the basis of some research evidence and consensus, identification of acute opsoclonus, ataxia, or myoclonus should prompt consideration of an underlying neuroblastoma. (9)
On the basis of some research evidence and consensus, surgical treatment options should be considered for children with dystonia, including secondary dystonias, such as those related to cerebral palsy, and include intrathecal baclofen pumps and deep brain stimulation. (10)
On the basis of some research evidence and clinical experience, tetrabenazine may be effective in treating chorea. (11)
On the basis of strong research evidence, although seldom inherently dangerous, tics may be uncomfortable for affected children and interfere with academic achievement and social development. (12)
On the basis of some research evidence and clinical experience, topiramate may be an effective treatment for tic disorders. (13)
References
- 1. Connolly AM , Dodson WE , Prensky AL , Rust RS . Course and outcome of acute cerebellar ataxia. Ann Neurol. 1994;35(6):673–679 [DOI] [PubMed] [Google Scholar]
- 2. Lionetti E , Francavilla R , Pavone P , et al. The neurology of coeliac disease in childhood: what is the evidence? a systematic review and meta-analysis. Dev Med Child Neurol. 2010;52(8):700–707 [DOI] [PubMed] [Google Scholar]
- 3. Barry S , Baird G , Lascelles K , Bunton P , Hedderly T . Neurodevelopmental movement disorders: an update on childhood motor stereotypies. Dev Med Child Neurol. 2011;53(11):979–985 [DOI] [PubMed] [Google Scholar]
- 4. Freeman KA , Duke DC . Power of magic hands: parent-driven application of habit reversal to treat complex stereotypy in a 3-year-old. Health Psychol. 2013 Aug;32(8):915–20. [DOI] [PubMed] [Google Scholar]
- 5. Erenberg G , Cruse RP , Rothner AD . The natural history of Tourette syndrome: a follow-up study. Ann Neurol. 1987;22(3):383–385 [DOI] [PubMed] [Google Scholar]
- 6. Silveira-Moriyama L , Gardiner AR , Meyer E , et al. Clinical features of childhood-onset paroxysmal kinesigenic dyskinesia with PRRT2 gene mutations. Dev Med Child Neurol. 2013;55(4):327–334 [DOI] [PubMed] [Google Scholar]
- 7. Olfson M , Blanco C , Liu SM , Wang S , Correll CU . National trends in the office-based treatment of children, adolescents, and adults with antipsychotics. Arch Gen Psychiatry. 2012;69(12):1247–1256 [DOI] [PubMed] [Google Scholar]
- 8. LaFrance WC Jr , Reuber M , Goldstein LH . Management of psychogenic nonepileptic seizures. Epilepsia. 2013;54(suppl 1):53–67 [DOI] [PubMed] [Google Scholar]
- 9. Gorman MP . Update on diagnosis, treatment, and prognosis in opsoclonus-myoclonus-ataxia syndrome. Curr Opin Pediatr. 2010;22(6):745–750 [DOI] [PubMed] [Google Scholar]
- 10. Olaya JE , Christian E , Ferman D , et al. Deep brain stimulation in children and young adults with secondary dystonia: the Children’s Hospital Los Angeles experience. Neurosurg Focus. 2013;35(5):E7 [DOI] [PubMed] [Google Scholar]
- 11. Chatterjee A , Frucht SJ . Tetrabenazine in the treatment of severe pediatric chorea. Mov Disord. 2003;18(6):703–706 [DOI] [PubMed] [Google Scholar]
- 12. Conelea CA , Woods DW , Zinner SH , et al. Exploring the impact of chronic tic disorders on youth: results from the Tourette Syndrome Impact Survey. Child Psychiatry Hum Dev. 2011;42(2):219–242 [DOI] [PubMed] [Google Scholar]
- 13. Jankovic J , Jimenez-Shahed J , Brown LW . A randomised, double-blind, placebo-controlled study of topiramate in the treatment of Tourette syndrome. J Neurol Neurosurg Psychiatry. 2010;81(1):70–73 [DOI] [PubMed] [Google Scholar]
Suggested Reading/Viewing
- DVD Educational Programming, Home Box Office Inc, and the Tourette Syndrome Association. I have Tourette’s but Tourette’s doesn’t have me [4-minute clip]. Bayside, NY: Tourette Syndrome Association; 2005. http://tsa-usa.org/ZHBO/VideoPlayer.html . [Google Scholar]
- Singer HS , Mink JW , Gilbert JL , Jankovic J . Movement Disorders in Childhood. Philadelphia, PA: Elsevier; 2010. [Google Scholar]
Internet Resources
- Tourette Syndrome Association. Parents Med Guide. http://ParentsMedGuide.org.