

Abstract
Upper gastrointestinal bleeding is a common emergency presentation requiring prompt resuscitation and management. Peptic ulcers are the most common cause of the condition. Thorough initial management with a structured approach is vital with appropriate intravenous fluid resuscitation and use of a restrictive transfusion threshold of 7-8 g/dL. Pre-endoscopic scoring tools enable identification of patients at high risk and at very low risk who might benefit from specific management. Endoscopy should be carried out within 24 h of presentation for patients admitted to hospital, although optimal timing for patients at a higher risk within this period is less clear. Endoscopic treatment of high risk lesions and use of subsequent high dose proton pump inhibitors is a cornerstone of non-variceal bleeding management. Variceal haemorrhage results in higher mortality than non-variceal haemorrhage and, if suspected, antibiotics and vasopressors should be administered urgently, before endoscopy. Oesophageal variceal bleeding requires endoscopic band ligation, whereas bleeding from gastric varices requires thrombin or tissue glue injection. Recurrent bleeding is managed by repeat endoscopic treatment. If uncontrolled bleeding occurs, interventional radiological embolisation or surgery is required for non-variceal bleeding or transjugular intrahepatic portosystemic shunt placement for variceal bleeding.
Keywords: Gastroenterology, Gastrointestinal diseases
Questions for future research.
Is fresh frozen plasma of value in the correction of coagulation in patients with cirrhosis and upper gastrointestinal bleeding?
What is the optimal timing of urgent endoscopy in patients at higher risk?
Will explainable machine learning models allow meaningful treatment changes that improve patient outcomes?
Introduction
Upper gastrointestinal bleeding (UGIB) is a common and potentially life threatening condition. Defined as bleeding originating proximal to the ligament of Trietz; bleeding from the oesophagus, stomach, or duodenum can present as haematemesis, melaena; or, in the context of severe bleeding and rapid intestinal transit, haematochezia. Coffee ground vomiting can be due to non-bleeding pathology, including obstruction, but might indicate UGIB. In addition to externalisation of blood, patients can present with symptoms of blood loss such as syncope, fatigue, and shortness of breath. The cause of bleeding can be classified as variceal or non-variceal, with non-variceal including peptic ulcer bleeding. Peptic ulcer bleeding is the most common cause for UGIB despite Helicobacter pylori (H Pylori) eradication treatment and proton pump inhibitor use.1 While incidence of UGIB has been reported to be declining owing to a combination of drug and endotherapeutic interventions,2 3 emergency presentation is common with mortality between 2% and 10%.4–6
Management of UGIB can be considered in three stages: pre-endoscopic management, endoscopic assessment and treatment, and post-endoscopic management. In this article, we review these stages with particular focus on initial management, including risk stratification, resuscitation, and drug treatment.
Incidence
The incidence of UGIB varies both globally and regionally. Based on population studies from 10 hospitals in Spain, the incidence of admission to hospital from UGIB was 47-87 per 100 000 people between 1996 and 2005,7 with more recent data from nationwide administrative databases in the US showing hospital admission rates of 67-81 per 100 000 from 2002 to 2012.3 Within the UK, differences also exist. A large systematic linkage of hospital in-patients in Wales showed an incidence of 134 per 100 000, whereas data from Scotland reported a figure of 172 per 100 000. Factors proposed for these differences include social deprivation and prevalence of H Pylori.7–9
Improved management, including resuscitation, proton pump inhibitor use, and endoscopic treatments have been associated with the reported reduction in mortality from UGIB over the past two decades.10 However, patients presenting with UGIB are increasingly of an older age with substantial comorbidities including cardiac, vascular, and renal disease, and use of antiplatelet or anticoagulant drug is common. This demographic could account for the static mortality reported by some studies.11
Sources and selection criteria
We searched PubMed, Cochrane Central Register of Controlled Trials, and Embase using the terms "upper gastrointestinal bleeding," "non-variceal bleeding," and "variceal bleeding" for articles published between 1 January 2010 and 31st December 2021. We also reviewed reference lists from articles that we deemed to be high quality. Preference was given to randomised controlled trials, meta-analyses, and systematic reviews that have informed guidelines. We included smaller studies if they were of particular note or if other evidence was unavailable, for example, a large case series in the absence of data from randomised controlled trial. In general, case reports and case series were excluded.
Initial management
A thorough history and clinical examination of the patient can provide an indication as to the cause of bleeding, but this indication is not certain until direct visualisation at endoscopy. Regardless of cause, any patient with haemodynamic instability should be appropriately resuscitated by use of a systematic approach.
Airway and breathing
Prophylactic intubation for airway protection in UGIB has not been investigated in a large randomised controlled trial. A few meta-analyses have shown that prophylactic intubation does not reduce incidence of pneumonia, length of stay in hospital, or risk of mortality, and in some studies, the risk is increased.12–14 One of these meta-analyses of 10 observational studies and 6068 patients showed no effect on mortality (odds ratio 1.92, 95% confidence interval 0.71 to 5.23; P=0.20), but did show a significant increase in aspiration (3.85, 1.46 to 10.25; P=0.01) and pneumonia (4.17, 1.82 to 9.57; P<0.001).13 These observational studies are likely to have involved selection bias, therefore, results should be interpreted with caution.
The European non-variceal UGIB guidelines recommend that prophylactic intubation should be performed only in the context of severe haematemesis, agitation, or inability to protect the airway.15 The Baveno VII guidance for variceal bleeding suggests use of intubation in patients with altered consciousness and actively vomiting blood, with extubation as soon as possible after endoscopy.16 In these situations, early anaesthetic input should be provided. Patients unable to tolerate endoscopy under conscious sedation might also require intubation.
Supplemental oxygen should be administered to achieve target saturations and maintain end organ oxygenation. Close observation is required of patients using face masks given the risk of aspiration.17
Circulation
Fluid resuscitation aims to maintain adequate tissue perfusion. Intravenous access should be secured usually with two ≤18 G cannula in each antecubital fossa. Short, wide bore cannulas are preferable to central access given the higher flow rates achievable.18 However, in some situations, such as difficult peripheral access or high osmolarity drug infusion, central access might be required.
A small, non-randomised study of 72 patients with UGIB showed a reduction in mortality (P=0.04) and myocardial infarction (P=0.04) in people who were managed with intensive early fluid resuscitation.19 A targeted systolic blood pressure of 90-100 mg Hg has been suggested by several guidelines.20 21 Whether intravenous crystalloid or colloid is superior in resuscitation in hypovolaemic shock is debatable; however, a multicentre randomised controlled trial showed no significant difference in 28 day mortality between people treated with the fluids.22 The British Society of Gastroenterology UGIB Care Bundle advises giving 500 mL crystalloid in less than 15 minutes to patients who are haemodynamically unstable, with regular review to determine ongoing requirement.23 In patients with persisting hypotension, despite fluid resuscitation, high dependency or intensive care is appropriate.24
Blood product transfusion
Packed red cells
Restrictive transfusion of packed red cells in the context of non-life-threatening UGIB has become the standard of care and is recommended by all major guidelines.15 25–28 A meta-analysis involving 12 587 patients, across 31 randomised controlled trials, who required a transfusion due to a range of causes, including acute blood loss, compared outcomes based on restrictive or liberal transfusion. A restrictive transfusion threshold, most commonly a haemoglobin concentration of 7-8 g/dL, did not alter mortality at 30 days (risk ratio 0.97, 95% confidence interval 0.81 to 1.16).29 Restrictive transfusion was not associated with increased adverse events in people with cardiovascular disease, but data were insufficient to be able to comment on those presenting with acute coronary syndrome. Owing to the heterogenous reasons for transfusion, the populations in this study might not be directly comparable to those with UGIB.
Within the setting of UGIB, a single centre randomised controlled trial from Spain assigned 921 patients to a restrictive (haemoglobin concentrations of <70 g/L) versus a liberal (<90 g/L) transfusion strategy. People receiving a restrictive strategy had a significantly lower risk of death at six weeks (hazard ratio 0.55, 95% confidence interval 0.33 to 0.92) after adjusting for baseline risk factors.30 A subsequent, large, UK, cluster randomised controlled trial reported no difference in clinical outcomes when comparing transfusions thresholds of less than 8 g/dL with less than 10 g/dL in patients presenting with UGIB.31 A meta-analysis of restrictive versus liberal packed red cells transfusion in UGIB including 1965 patients from five randomised controlled trials showed that restrictive transfusion was associated with lower mortality (relative risk 0.65, 95% confidence interval 0.44 to 0.97; P=0.03) and reduced rebleeding (0.58, 0.40 to 0.84; P=0.004).32
Importantly, patients with exsanguinating bleeding were excluded from most transfusion trials. Owing to intravascular volume depletion, haemoglobin concentrations can be artificially high in this group. Although not advising target orientated resuscitation, the British Society of Gastroenterology variceal guidelines suggest that a venous saturation of more than 70% is an easily measurable level within the resuscitation setting and a useful guide for clinicians.21
Platelets and clotting factors
Limited evidence exists regarding the need, or threshold, for platelet transfusion in UGIB.33 The British Society of Gastroenterology consensus bundle advises a threshold of transfusion at 50×109 platelets/L or less based on major haemorrhage protocols with the acknowledgment that this advice is based primarily on expert opinion.24 34 Within the context of variceal bleeding, no evidence suggests that platelet count correlates with inability to control bleeding or rebleeding. However, in the event of these outcomes, the Baveno VII consensus advises correction can be considered on an individual basis,16 whereas the National Institute for Health and Care Excellence and British Society of Gastroenterology variceal guidelines advise transfusion at the threshold of 50×109/L or less.21 35
Clotting abnormalities and their management in patients with cirrhosis and UGIB is a complex area. Prothrombin time is often prolonged leading to the use of fresh frozen plasma; however, prothrombin is not an accurate indicator of the clotting risk in cirrhosis.36 37 Studies have not shown a clear benefit from fresh frozen plasma and the most recent iteration of US variceal guidelines did not advocate its use in patients with cirrhosis and UGIB.38
Risk assessment
Numerous risk assessment scores can be used for prognostication of patients with UGIB. These include post-endoscopic scoring tools (eg, full Rockall score, Cedars Sinai, and Progretto Nazionale Emorragia Digestiva) and pre-endoscopic scoring tools (eg, pre-endoscopy Rockall, AIMS65, and Glasgow Blatchford scores). Pre-endoscopic scores enable early identification of patients at high or low risk who might benefit from specific clinical management within an appropriate level of care.20 25 The Rockall (full and pre-endoscopic), AIMS65, and Glasgow Blatchford scores are best studied.39–41 An international, multicentre, prospective study of 3012 patients compared these scores and two other post endoscopy scores. Results suggested that the Glasgow Blatchford scores had the highest discriminative ability at predicting need for a hospital based intervention or death at 30 days (Glasgow Blatchford scores of area under the receiver operating characteristic of 0.86, admission Rockall of 0.66, AIMS65 of 0.6842; figure 1). No score was particularly good at predicting rebleeding or death. The more recently developed pre-endoscopic ABC score has shown better prediction of 30 day mortality;43 however, this tool has not yet been widely adopted and requires further validation.
Figure 1.
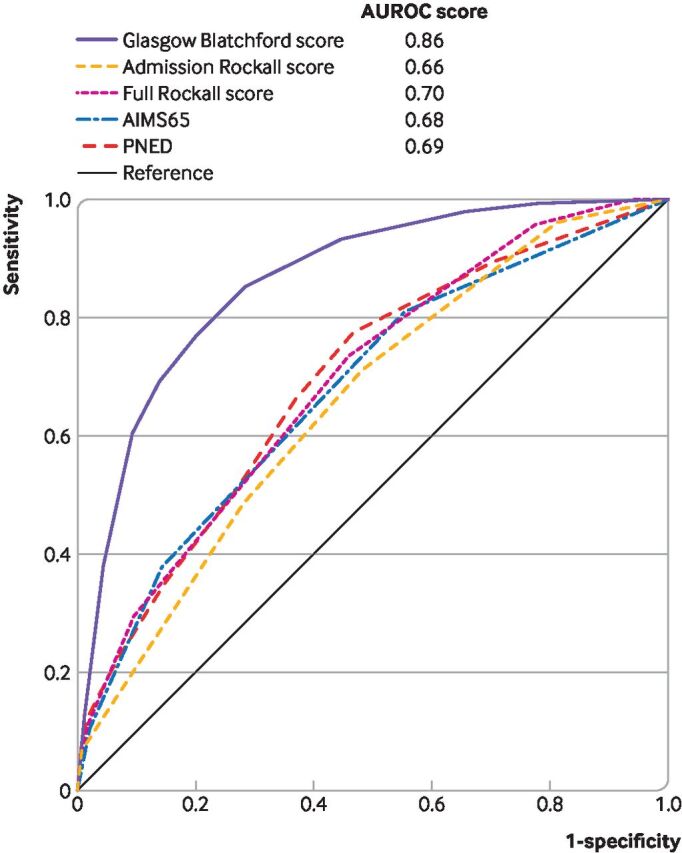
Comparisons of prediction scores related to the need for any intervention (transfusion, endoscopic treatment, interventional radiology, or surgery) or 30 day mortality (n=1704). All figures compared patients with complete data for all compared scores. AUROC=area under the receiver operating characteristic curve42; PNED=Progretto Nazionale Emorragia Digestiva
Pre-endoscopy risk scoring also enables patients who are at very low risk to avoid admission to hospital (or be discharged earlier). A systematic review of 16 studies assessing the predictive value of scores for adverse events (a composite of mortality, recurrent bleeding, and need for intervention) within 30 days identified the Glasgow Blatchford scores as having the greatest sensitivity (0.98) compared with pre-endoscopic Rockall (0.93) and AIMS65 (0.79).44 Specificity was quite low for all scores (0.16, 0.24, and 0.61, respectively); however, for patient safety reasons, high sensitivity is much more important than specificity.
A Glasgow Blatchford score of 0 or 1 has been shown by multiple studies to be the optimum threshold for identification of patients at low risk suitable for outpatient management42 44–46 and has been recommended in the most recent Asian-Pacific, European, American, and international guidelines.15 26–28
Time to endoscopy
Data from studies over the past two decades have suggested that early endoscopy (within 24 h) is preferable to later endoscopy in patient groups at high and low risk,47–49 reflected in recent guidelines.15 27 28 In two randomised controlled trials of patients at low risk,50 51 early endoscopy versus delayed endoscopy (defined in one trial as 6 h v 48 h, and <2 h v 1-2 days in the other) resulted in no difference in mortality or rebleeding. However, length of hospital stay varied. One study reported no difference in duration of admission (odds ratio 3.98 days (95% confidence interval 2.84 to 5.11) for early endoscopy v 3.26 days (2.32 to 4.21) for delayed endoscopy).50 In the second randomised controlled trial, 26 (46%) of 56 patients assigned to early endoscopy were discharged immediately (median stay of one day v two days).51 Facilitating endoscopy within 24 h should enable early discharge in many patients with substantial reduction in healthcare costs.
Whether urgent endoscopy, defined in various studies as between 2 h and 12 h, confers benefit compared with early endoscopy is unclear. A Danish cohort study involving 12 601 patients reported lower in-hospital mortality in patients who are haemodynamically stable who underwent endoscopy 12-36 h after admission (odds ratio 0.48, 95% confidence interval 0.34 to 0.67). For patients who are haemodynamically unstable, hospital mortality was lower in patients undergoing endoscopy 6-24 h after admission to hospital than in patients undergoing endoscopy outside of this time (0.73, 0.54 to 0.98).52 An important randomised controlled trial of 516 patients at high risk (defined by Glasgow Blatchford scores ≥12) reported no difference in 30 day mortality or rebleeding in those undergoing urgent endoscopy within less than 6 h versus early endoscopy within 6-24 h (hazard ratio 1.35, 95% confidence interval 0.72 to 2.54; P=0.34;53 figure 2).
Figure 2.
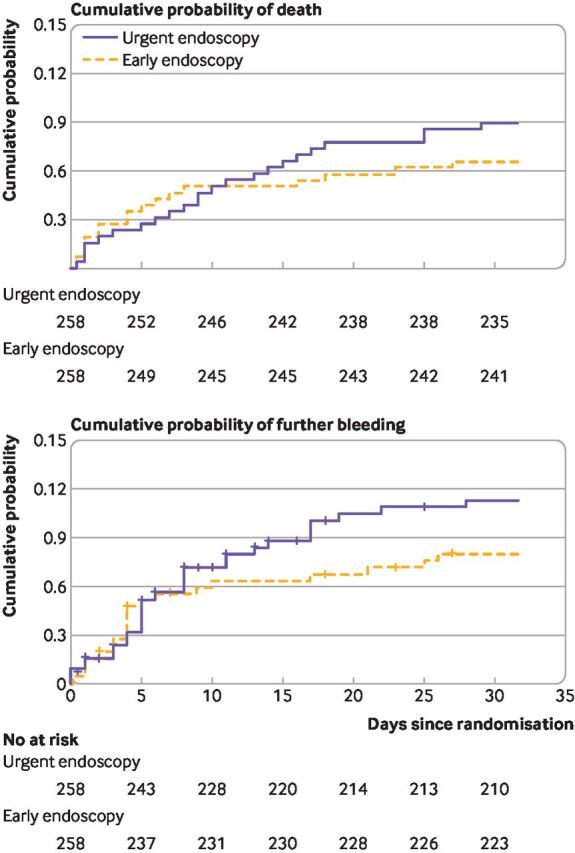
Comparison of mortality and further bleeding between urgent (<6 h) versus early (6-24 h) endoscopy in patients with high risk gastrointestinal bleeding (Glasgow Blatchford Score ≥12)53
Although current evidence does not appear to support urgent endoscopy at less than 6 h, some variceal bleeding guidelines advise that endoscopy should be performed at between 12 h and 24 h.21 38 54 Exact timing of endoscopy can be challenging and should be decided on the basis of thorough clinical assessment, including haemodynamics and underlying comorbidities. Appropriate resuscitation and optimisation of comorbidities is essential before endoscopy.20
Management of antithrombotic agents
Use is increasing for antiplatelet and anticoagulant drugs for cardiovascular or cerebrovascular disease; one international study reported that 253 (45%) of 568 patients presenting with UGIB were taking these drugs.55 This poses a major dilemma in the treatment of UGIB because clinicians must balance the risk of bleeding with the risk of thrombotic events and decide if, and for how long, these drugs should be withheld or their effects corrected.56 57
Antiplatelet treatment
Combined guidelines from the European Society of Gastrointestinal Endoscopy and British Society of Gastroenterology advise that in patients presenting with a proven UGIB, aspirin should be stopped (potentially indefinitely) when used for primary cardiovascular prevention but continued in secondary prevention.58 A meta-analysis of 50 279 patients showed that aspirin discontinuation in the context of secondary prevention was associated with a three times increase in the risk of major cardiac events (odds ratio 3.14, 95% confidence interval 1.75 to 5.61).59 This risk increased 89-fold in patients with stents (89.78, 29.90 to 269.60). A placebo controlled, single centre randomised controlled trial of 156 patients reported that although patients continuing aspirin monotherapy for secondary prevention had an increased risk of recurrent bleeding versus controls (10.3% (95% confidence interval 3.4% to 17.2%) v 5.4% (0.3% to 10.5%)), patients who stopped aspirin had a significantly higher 30 day mortality verus those who were continuing aspirin use (9% (2.7% to 15.3%) v 1.3% (0.1% to 3.8%) in the aspirin group).60 If aspirin is temporarily withheld in patients who have a life threating bleed, the recommended time to resumption varies across guidelines from time of haemostasis to five days.58 61
A meta-analysis of aspirin in primary prevention trials of 95 000 patients showed only a 0.07% annual reduced risk of serious adverse vascular events; therefore, the risk of bleeding by continuing aspirin probably outweighs the benefit, except in patients who have a calculated cardiovascular risk that is high.62
Limited evidence exists for the management of patients on dual antiplatelet treatment. In patients with stents, the risk of occlusion is high and must be balanced against the risk of bleeding.61 European guidelines recommend that treatment is continued in this group, if possible, and a consultation with cardiology is sought.58 In cases of severe bleeding, aspirin use should be continued and a P2Y12 antagonist withheld, but recommenced within five days.63
Anticoagulant treatment
Patients on anticoagulants have an inherent underlying thrombotic risk that must be balanced against the bleeding risk in UGIB. In cases of severe UGIB, both European and US guidelines suggest that patients on warfarin have the drug withheld, together with anticoagulant reversal. Vitamin K should be given in addition to the faster acting four factor prothrombin complex. This method is preferred over fresh frozen plasma because of the lower volume required.58 63 In less severe UGIB, the risk versus benefit balance of continuing anticoagulation must be assessed. Rebleeding after endotherapy does not appear to be affected by a moderately elevated International Normalised Ratio, based on a case series of 233 patients, where anticoagulation was defined as an International Normalised Ratio greater than or equal to 1.3.64 Ninety seven (95%) of 102 patients who were anticoagulated had an International Normalised Ratio of between 1.3 and 2.7, with a rebleeding rate (after initial haemostasis) of 23% (23/102) noted in patients who had anticoagulation, and 21% (28/131) in those with International Normalised Ratio less than 1.3. In the absence of large randomised controlled trials, the US guidelines suggest that endotherapy is appropriate in patients with an International Normalised Ratio of less than 2.5.63
Data are limited to guide timing of reintroduction of warfarin. A retrospective cohort study of 442 patients suggested that early reintroduction lowers the risk of thromboembolic events (hazard ratio 0.05, 95% confidence interval 0.01 to 0.58) and death (0.31, 0.15 to 0.62).65 Current European guidance advises reintroduction of warfarin after haemostasis is achieved and within seven days, taking patient factors into consideration.15 Unlike warfarin, the direct oral anticoagulants have a rapid onset of action and short half-life of 12-24 h. Various reversal agents have been identified, including andexanet alfa and idarucizumab. Although effective, these drugs are expensive and concerns exist regarding a possible procoagulant effect. European and British Society of Gastroenterology guidelines suggest that given their short half-life, apart from life threatening bleeds, simply withholding the direct oral anticoagulant is an appropriate course of action.58
Drug intervention pre-endoscopy
Prokinetic agents
Use of intravenous erythromycin at 250 mg for 30-120 minutes before endoscopy has been shown to improve gastric mucosa visualisation in several randomised controlled trials.66 67 A subsequent meta-analysis reported that this might reduce transfusion requirements, need for second endoscopy and length of stay.68 A more recent meta-analysis of 598 patients also reported that intravenous erythromycin led to a reduced requirement for repeat endoscopy (odds ratio 0.51, 95% confidence interval 0.34 to 0.77) and shorter length of stay (mean difference −1.75 days, 95% confidence interval −2.43 to −1.06), although no difference in transfusion requirement was identified.69 Despite these findings, erythromycin has not been widely adopted within the UK. The British Society of Gastroenterology consensus bundle advises use of erythromycin in selected patients at the discretion of the endoscopist.23
Tranexamic acid
This antifibrinolytic agent inhibits the interaction of plasminogen with plasmin and fibrin, and is widely used in the management of major bleeding in trauma, obstetrics, and surgery.70 Results from relatively small studies and meta-analyses are conflicting about the effectiveness of its use in UGIB.71–73 The HALT-IT study, an international, placebo controlled randomised controlled trial of 12 009 patients74 showed no improvement in five day mortality with tranexamic acid compared with placebo (risk ratio 0.99, 95% confidence interval 0.82 to 1.18; figure 3). Additionally, risk of venous thromboembolism was increased with tranexamic acid (1.85, 1.15 to 2.98). As a result, guidelines recommend that tranexamic acid is not used in UGIB outside of clinical trials.15 16
Figure 3.

Effect of tranexamic acid versus placebo on death due to bleeding within 5 days of an upper gastrointestinal bleed 74
Proton pump inhibitors
Use of proton pump inhibitors before endoscopy might reduce the need for endoscopic treatment at index endoscopy, but does not improve more clinically relevant endpoints, therefore, use in this situation is not advocated by National Institute for Health and Care Excellence.35 This advice is based on a meta-analysis of six studies comprising 2223 patients, which showed no significant reduction in mortality (odds ratio 1.12, 95% confidence interval 0.72 to 1.73), rebleeding (0.81, 0.61 to 1.09), or need for surgery (0.96, 0.68 to 1.35).75 Despite this guidance, the 2015 UK National Confidential Enquiry into Patient Outcome and Death report found that 150 (73%) of 206 patients had acid suppression started before definitive diagnosis, which was thought likely owing to clinicians' desires to start a specific treatment when managing a haemorrhage.76 European, Asian-Pacific, International, and US guidelines are not consistent on the use of proton pump inhibitors, with some suggesting that these compounds could have a role in the context of delayed endoscopy in consideration of relative costs of proton pump inhibitors and endotherapy.15 26–28
Drug treatment pre-endoscopy in suspected variceal bleeding
Antibiotic prophylaxis
Bacterial infections are identified in 35-66% of patients with cirrhosis and variceal bleeding77 and patients with cirrhosis and UGIB are at increased risk of rebleeding and mortality.78 Empirical antibiotic treatment reduces this risk, with a meta-analysis of 12 trials and 1241 patients reporting reduced mortality (risk ratio 0.79, 95% confidence interval 0.63 to 0.98), rebleeding (0.53, 0.38 to 0.74), and length of hospital stay.79 The choice of antibiotic should be determined by local resistance patterns and continued for up to seven days.80 81
Vasoactive drugs
Vasopressors, including somatostatin, its analogue octreotide, and terlipressin, reduce portal pressures via splanchnic vasoconstriction. Two randomised controlled trials of 205 and 76 patients, have shown that these drugs improve bleeding control at the time of endoscopy (P=0.012 and P=0.034, respectively), reduce mortality and the need for rescue treatment in the first randomised controlled trial (P=0.05), and reduce mortality at 15 days in the second randomised controlled trial (P=0.035).82 83 No difference in control of bleeding has been identified between the different drugs.84 Current guidelines recommend commencing a vasoactive drug at presentation in suspected variceal bleeding with a suggested course of two to five days.16 21 Contraindications include cardiac or severe vascular disease.
Endoscopic management
Non-variceal bleeding
Most research in endotherapy for non-variceal bleeding has focused on patients with peptic ulcers. Options available for haemostasis in ulcer bleeding include injection (1:10 000 epinephrine, sclerosant, or thrombin), thermal (contact or non-contact), or mechanical treatment with clips.85 The widely adopted Forrest classification allows for categorisation of ulcer morphology at endoscopy86 and helps to identify high-risk lesions that require treatment. Spurting and oozing vessels (Forrest Ia and Ib) are independent risk factors for persistent or recurrent bleeding87 and require intervention, as do lesions with visible vessels (Forrest IIa). A meta-analysis of studies comparing endotherapy with no endotherapy showed significantly decreased rates of further bleeding when endotherapy is applied in patients with spurting or oozing lesions (risk ratio 0.29, 95% confidence interval 0.20 to 0.43) and patients with visible vessels (0.49, 0.40 to 0.5988; figure 4). These groups also showed a reduced need for surgery. The need for endotherapy in lesions with adherent clot (Forrest IIb) is under debate, with current guidelines advocating either endoscopic or medical management alone. Low risk lesions that do not require endoscopic intervention include those with a pigmented or clean base (Forrest IIC and III).15 20
Figure 4.

Peptic ulcer with persistent oozing of blood (left image), treated endoscopically with epinephrine injection and clips, and then haemostatic powder (right image)
Multiple studies have shown each single endotherapy modality to be comparable in achieving haemostasis, with the exception of epinephrine, which appears to have a temporary action only and therefore should not be used as a monotherapy.85 Epinephrine can be used to temporarily reduce bleeding and aid visualisation20 before use of another endoscopic modality, but is inferior as a monotherapy compared with as a component of dual treatment (risk ratio 0.53, 95% confidence interval 0.35 to 0.81).89
Variceal bleeding
Bleeding from gastro-oesophageal varices is a life threatening consequence of portal hypertension. Despite both drug and endotherapeutic advances, six week mortality following a variceal bleed is approximately 20%.90 First described in 1988, variceal band ligation has long replaced sclerotherapy as the optimal endoscopic management for oesophageal variceal bleeding due to a superior reduction in both rebleeding and mortality.91
Gastric variceal bleeding is less common, but associated with poorer outcomes than oesophageal variceal bleeding.92 The recommended treatment modality advocated by guidelines is dependent on the anatomical location and relationship with any oesophageal varices. The Sarin classification is a useful tool to assess gastric varices and guide endoscopic treatment.93 Bleeding gastric varices continuous with oesophageal varices extending 2-5 cm along the lesser curve of the stomach can be managed with band ligation, with other types of gastric varices managed with injection of tissue glue or thrombin.21 94
Post-endoscopic management
Non-variceal bleeding
For patients at high risk who require endoscopic treatment after non-variceal UGIB, use of high dose proton pump inhibitors after endoscopy has been shown to decrease the risk of rebleeding.62 These agents are commonly administered as a single intravenous bolus of 80 mg omeprazole (or equivalent) followed by 8 mg/h of continuous infusion for 72 h, based on an randomised controlled trial in Hong Kong of 240 patients.95 This trial showed a significant reduction in rebleeding within three days in the infusion group (P<0.001). A subsequent meta-analysis comparing proton pump inhibitor infusion and placebo also showed a significant reduction in rebleeding (risk ratio 0.40, 95% confidence interval 0.28 to 0.59), in addition to a reduced need for surgery (0.43, 0.24 to 0.76), and reduced risk of mortality (0.41, 0.20 to 0.84).88
A meta-analysis of 13 studies has addressed whether intermittent intravenous bolus or oral proton pump inhibitors at high dose (potentially lowering cost) are equivalent to continuous intravenous infusion.96 The results showed non-inferiority of intermittent proton pump inhibitor (relative risk of rebleed within 7 days 0.72, upper boundary of one sided 95% confidence interval 0.97). A subgroup analysis comparing results of intermittent IV proton pump inhibitor to intermittent oral use did not show heterogeneity, although the 95% confidence interval between intermittent oral and continuous intravenous proton pump inhibitor was wide (risk ratio 0.96, 95% upper bound confidence interval 2.02). These findings are consistent with earlier studies that showed that an oral proton pump inhibitor was equally effectively in lowering gastric pH and non-inferior to intravenous proton pump inhibitor in UGIB.97 98 Updated European and American guidelines advise that intermittent intravenous or oral proton pump inhibitors given at a high dosecould be considered as alternatives to continuous infusion.15 27
After high dose intravenous (or oral) proton pump inhibitor treatment for patients with high risk lesions that require endotherapy, American and International guidelines advise commencing a two week course of twice daily, high dose, oral proton pump inhibitor.27 28 This treatment is based on an randomised controlled trial that showed that twice daily high dose proton pump inhibitors (40 mg esomeprazole) in patients with high risk lesions had significantly reduced rebleeding compared with patients given a standard dose (40 mg esomeprazole once daily) (fourth to 28th day: 10.8% v 28.7%, P=0.002).99 Patients with low risk lesions can receive standard dose oral proton pump inhibitor after endoscopy.15
In bleeding secondary to peptic ulceration, H pylori status should be assessed by rapid urease testing or histology for H pylori at index endoscopy. However, a meta-analysis of 23 studies showed these tests to have low sensitivity (pooled sensitivity 0.67, 95% confidence interval 0.64 to 0.70 for rapid urease testing and 0.7, 0.66 to 0.74 for histology).100 In the event of a negative result, European guidelines advised retesting within four weeks and eradication of H pylori if positive.15
Variceal bleeding
In cases of proven variceal bleeding, vasoactive drugs should be continued for two to five days as noted above. A meta-analysis of eight studies concluded that the combination of vasoactive drugs with endotherapy resulted in better initial control of bleeding and five day haemostasis than endotherapy alone, although this result did not translate to a survival benefit.101 In people with cirrhosis and UGIB, antibiotics should be administered for up to seven days, even if the cause of bleeding is non-variceal, owing to the risk of sepsis.78
A transjugular intrahepatic portosystemic shunt decreases portal pressure and can also decrease the risk of variceal rebleeding. A multicentre, European randomised controlled trial of 63 patients Child-Pugh class C<14 or class B with active bleeding reported reduced risk of rebleeding (3% v 50%, P<0.001) and improved one year survival (86% v 61%, P<0.001) in patients undergoing an early (<72 h) so-called pre-emptive transjugular intrahepatic portosystemic shunt.102 An European guideline and the Baveno VII consensus now advocates the use of early pre-emptive transjugular intrahepatic portosystemic shunt (<72 h) to be considered in patients bleeding from oesophageal varices, or gastro-oesophageal varices type I or II who have bleeding controlled by endotherapy but are at high risk of rebleeding.16 54 A Scottish, open label, randomised controlled trial done in two centres of 58 patients also reported a reduced risk of rebleeding (0% v 27.6%, P=0.04) but no effect on survival (76.9% v 75.9%, P=0.9).103 This study reported difficulty in delivering this so-called elective transjugular intrahepatic portosystemic shunt procedure within 72 h, which could be challenging for many centres globally. In patients with gastric varices and a clinical or anatomical contraindication to transjugular intrahepatic portosystemic shunt, balloon occluded retrograde transvenous obliteration can be considered with outcomes appearing similar to transjugular intrahepatic portosystemic shunt in a small retrospective study.104
Ongoing or recurrent bleeding
Non-variceal bleeding
The term "further bleeding" encompasses both no haemostasis at index endoscopy and also early rebleeding. If acute bleeding persists despite standard endotherapy, European guidelines suggest the use of the larger over the scope clip or haemostatic powder; however, owing to reported high rates of rebleeding, haemostatic powder should probably be used as a temporising measure before definitive management by other means, such as interventional radiology.15
Rebleeding is indicated by externalisation of blood, more than 20 g/L reduction after stabilisation of haemoglobin concentration, or tachycardia and hypotension. All major guidelines recommend repeat endoscopy in this event.15 25–28 A randomised controlled trial of 100 patients comparing repeat endoscopy with surgery in rebleeding after index endoscopy showed 35 (73%) of 48 patients having repeat endoscopy had long term control of bleeding with significantly reduced complications, no increase in risk of mortality, and reduced resource costs.105 If bleeding cannot be controlled endoscopically, interventional radiology (for transarterial embolisation) or surgical input should be sought; a meta-analysis reported no difference in mortality or need for further intervention between these groups.106 For patients with substantial comorbidities, interventional radiology is generally a safer option than surgery.
Variceal bleeding
If variceal bleeding is uncontrolled by standard endoscopic band ligation or injection techniques, a balloon tamponade might be required. A 1978 trial of 97 patients showed that balloon tamponade was highly effective at meeting primary haemostasis in oesophageal varices (86%) but rebleeding was common (52%).107 Safety concerns remain because of potential complications such as aspiration pneumonia and oesophageal rupture.21 Balloon tamponade is, therefore, only recommended as a temporising measure before repeat endoscopy or so-called rescue transjugular intrahepatic portosystemic shunt is undertaken.54 The self expanding Danis stent has emerged as a possible alternative to the balloon tamponade, with National Institute for Health and Care Excellence guidance and Baveno VII consensus advocating this stent as an alternative in managing uncontrolled bleeding from oesophageal varices.16 108 A Spanish, multicentre randomised controlled trial involving 28 patients compared balloon tamponade with stent insertion and reported improved bleeding control in the stent group (85% v 47%, P=0.037), with a reduced need for transfusion but no significant difference in mortality.109
Emerging treatments
Machine learning modelling
Existing risk stratification scoring systems for UGIB allow predictions and inform decisions in patient care. However, these scores are not dynamic and do not subsequently assist clinicians during hospital admission. Machine learning might improve patient management in cohorts at high or low risk. A study in more than 2000 patients with UGIB reported that a machine learning model outperformed existing risk scores at predicting an adverse event (composite of hospital intervention or death within 30 days) with 100% sensitivity and a higher specificity, thereby potentially increasing identification of patients at low risk and suitable for discharge.110 Separately, an explainable machine learning model, trained using data from 5691 patients in intensive care who were admitted to hospital with UGIB, performed better than the APACHE IVa score in the identification of patients at high risk who died.111 Ability to explain allows physicians insight into why a specific score is reached, which can then aid clinical decision making on an individual basis. These models could be embedded into electronic health records as a dynamic aid to clinicians who manage patients with UGIB.
Doppler probes
The use of doppler probes as adjunct in endoscopic management of UGIB have been investigated. Although not currently recommended by guidelines,15 a randomised controlled trial of 86 patients showed potential benefit in patients undergoing doppler guided haemostasis who had significantly lower rates of rebleeding at 30 days than visually guided endoscopic haemostasis (11.1% v 26.3%, P=0.02).112 Further work is required to establish if this approach improves outcomes and is practical and cost-effective for widespread use.
Novel haemostatic techniques
Several new developments have been made in endoscopic haemostasis, mostly in the form of novel haemostatic powders or gels. These advancements include Endoclot, Purastat, and Nexpowder.113–115 Studies are required to clarify their role in the endoscopic management of UGIB.
Guidelines
Multiple comprehensive international guidelines exist for the management of UGIB. The most recently updated of which include guidance from the American College of Gastroenterology and the European Society of Gastrointestinal Endoscopy.15 27 The seventh iteration of the Baveno consensus was published in 2022 and provided updated evidence based recommendations on management of variceal bleeding.16 These guidelines are referenced throughout the paper and where differences do exist, usually in areas with less evidence, relevance and applicability were considered.
Conclusions
Advances in management of UGIB over recent years include improved resuscitation and a relatively restrictive red cell transfusion strategy that has improved patient outcomes. A more accurate risk assessment has enabled early decision making, particularly in facilitating safe outpatient management of patients at very low risk.
The management of comorbidities is critical, given that mortality after UGIB is most commonly due to underlying comorbidities. Increased use of antithrombotic agents has increased the complexity of management decisions in UGIB, with the need to balance risks of both bleeding and thrombotic events. Further data are required to guide optimal management in this situation, including the timing of reintroduction of antithrombotic drugs.
Endotherapy has rapidly evolved with multiple haemostatic techniques now available to the endoscopists. Endoscopic treatment that does not work in non-variceal UGIB should prompt interventional radiological emoblisation, with surgery now rarely required. Endoscopic band ligation is effective in controlling oesophageal variceal bleeding with injection of tissue glue or thrombin used for gastric variceal bleeding. Transjugular intrahepatic portosystemic shunt might be used as rescue treatment for variceal bleeding uncontrolled by endoscopic treatment, but further research is required to determine the role of pre-emptive transjugular intrahepatic portosystemic shunt in in patients at higher risk after initial bleeding control.
In the future, the development of machine learning techniques embedded in the electronic patient record could lead to dynamic patient assessment, which should help to direct clinical care. Improved endoscopic and medical treatments will continue to evolve; however, owing to the increasingly older population with substantial comorbidities and often on treatment with an antithrombotic drug, UGIB will probably remain a common medical emergency.
Patient involvement.
The charity Guts UK was contacted and three patients identified who kindly volunteered to review an initial draft. After their comments, changes were made to the sections on timing of endoscopy and regarding patient comorbidities.
Footnotes
Contributors: JO-P wrote the initial draft and the subsequent editing. AS planned the article and edited/adapted the drafts. Both were involved in reviewing the literature. AS is guarantor.
Funding: No funding declared.
Competing interests: We have read and understood the BMJ policy on declaration of interests and declare the following interests: none.
Provenance and peer review: Commissioned; externally peer reviewed.
Data availability statement
No data are available.
References
- 1. Oakland K. Changing epidemiology and etiology of upper and lower gastrointestinal bleeding. Best Pract Res Clin Gastroenterol 2019;42-43:101610–43. 10.1016/j.bpg.2019.04.003 [DOI] [PubMed] [Google Scholar]
- 2. Abougergi MS. Epidemiology of upper gastrointestinal hemorrhage in the USA: is the bleeding slowing down? Dig Dis Sci 2018;63:1091–3. 10.1007/s10620-018-4951-5 [DOI] [PubMed] [Google Scholar]
- 3. Wuerth BA, Rockey DC. Changing epidemiology of upper gastrointestinal hemorrhage in the last decade: a nationwide analysis. Dig Dis Sci 2018;63:1286–93. 10.1007/s10620-017-4882-6 [DOI] [PubMed] [Google Scholar]
- 4. Abougergi MS, Travis AC, Saltzman JR. The in-hospital mortality rate for upper Gi hemorrhage has decreased over 2 decades in the United States: a nationwide analysis. Gastrointest Endosc 2015;81:882–8. 10.1016/j.gie.2014.09.027 [DOI] [PubMed] [Google Scholar]
- 5. Nahon S, Hagège H, Latrive JP, et al. Epidemiological and prognostic factors involved in upper gastrointestinal bleeding: results of a French prospective multicenter study. Endoscopy 2012;44:998–1006. 10.1055/s-0032-1310006 [DOI] [PubMed] [Google Scholar]
- 6. Hearnshaw SA, Logan RFA, Lowe D, et al. Acute upper gastrointestinal bleeding in the UK: patient characteristics, diagnoses and outcomes in the 2007 UK audit. Gut 2011;60:1327–35. 10.1136/gut.2010.228437 [DOI] [PubMed] [Google Scholar]
- 7. Lanas A, García-Rodríguez LA, Polo-Tomás M, et al. Time trends and impact of upper and lower gastrointestinal bleeding and perforation in clinical practice. Am J Gastroenterol 2009;104:1633–41. 10.1038/ajg.2009.164 [DOI] [PubMed] [Google Scholar]
- 8. Blatchford O, Davidson LA, Murray WR, et al. Acute upper gastrointestinal haemorrhage in West of Scotland: case ascertainment study. BMJ 1997;315:510–4. 10.1136/bmj.315.7107.510 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Button LA, Roberts SE, Evans PA, et al. Hospitalized incidence and case fatality for upper gastrointestinal bleeding from 1999 to 2007: a record linkage study. Aliment Pharmacol Ther 2011;33:64–76. 10.1111/j.1365-2036.2010.04495.x [DOI] [PubMed] [Google Scholar]
- 10. Chaudhary S, Mackay D, Pell JP, et al. Upper gastrointestinal bleeding in Scotland 2000-2015: trends in demographics, aetiology and outcomes. Aliment Pharmacol Ther 2021;53:383–9. 10.1111/apt.16170 [DOI] [PubMed] [Google Scholar]
- 11. Rosenstock SJ, Møller MH, Larsson H, et al. Improving quality of care in peptic ulcer bleeding: nationwide cohort study of 13,498 consecutive patients in the Danish clinical register of emergency surgery. Am J Gastroenterol 2013;108:1449–57. 10.1038/ajg.2013.162 [DOI] [PubMed] [Google Scholar]
- 12. Almashhrawi AA, Rahman R, Jersak ST, et al. Prophylactic tracheal intubation for upper Gi bleeding: a meta-analysis. World J Metaanal 2015;3:4. 10.13105/wjma.v3.i1.4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Alshamsi F, Jaeschke R, Baw B, et al. Prophylactic endotracheal intubation in patients with upper gastrointestinal bleeding undergoing endoscopy: a systematic review and meta-analysis. Saudi J Med Med Sci 2017;5:201. 10.4103/sjmms.sjmms_95_17 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Chaudhuri D, Bishay K, Tandon P, et al. Prophylactic endotracheal intubation in critically ill patients with upper gastrointestinal bleed: a systematic review and meta-analysis. JGH Open 2020;4:22–8. 10.1002/jgh3.12195 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Gralnek IM, Stanley AJ, Morris AJ, et al. Endoscopic diagnosis and management of nonvariceal upper gastrointestinal hemorrhage (NVUGIH): European Society of Gastrointestinal Endoscopy (ESGE) Guideline - Update 2021. Endoscopy 2021;53:300–32. 10.1055/a-1369-5274 [DOI] [PubMed] [Google Scholar]
- 16. de Franchis R, Bosch J, Garcia-Tsao G, et al. Baveno VII - Renewing consensus in portal hypertension. J Hepatol 2022;76:959–74. 10.1016/j.jhep.2021.12.022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Ghosh S, Watts D, Kinnear M. Management of gastrointestinal haemorrhage. Postgrad Med J 2002;78:4–14. 10.1136/pmj.78.915.4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Reddick AD, Ronald J, Morrison WG. Intravenous fluid resuscitation: was Poiseuille right? Emerg Med J 2011;28:201–2. 10.1136/emj.2009.083485 [DOI] [PubMed] [Google Scholar]
- 19. Baradarian R, Ramdhaney S, Chapalamadugu R, et al. Early intensive resuscitation of patients with upper gastrointestinal bleeding decreases mortality. Gastroenterology 2003;124:A508. 10.1016/S0016-5085(03)82571-4 [DOI] [PubMed] [Google Scholar]
- 20. Stanley AJ, Laine L. Management of acute upper gastrointestinal bleeding. BMJ 2019;364:l536. 10.1136/bmj.l536 [DOI] [PubMed] [Google Scholar]
- 21. Tripathi D, Stanley AJ, Hayes PC, et al. U.K. guidelines on the management of variceal haemorrhage in cirrhotic patients. Gut 2015;64:1680–704. 10.1136/gutjnl-2015-309262 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Annane D, Siami S, Jaber S, et al. Effects of fluid resuscitation with colloids vs crystalloids on mortality in critically ill patients presenting with hypovolemic shock: the CRISTAL randomized trial. JAMA 2013;310:1809–17. 10.1001/jama.2013.280502 [DOI] [PubMed] [Google Scholar]
- 23. Siau K, Hearnshaw S, Stanley AJ, et al. British Society of Gastroenterology (BSG)-led multisociety consensus care bundle for the early clinical management of acute upper gastrointestinal bleeding. Frontline Gastroenterol 2020;11:1–13. 10.1136/flgastro-2019-101395 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Hunt BJ, Allard S, Keeling D, et al. A practical guideline for the haematological management of major haemorrhage. Br J Haematol 2015;170:788–803. 10.1111/bjh.13580 [DOI] [PubMed] [Google Scholar]
- 25. Hwang JH, Fisher DA, Ben-Menachem T, et al. The role of endoscopy in the management of acute non-variceal upper Gi bleeding. Gastrointest Endosc 2012;75:1132–8. 10.1016/j.gie.2012.02.033 [DOI] [PubMed] [Google Scholar]
- 26. Sung JJ, Chiu PW, Chan FKL, et al. Asia-Pacific Working group consensus on non-variceal upper gastrointestinal bleeding: an update 2018. Gut 2018;67:1757–68. 10.1136/gutjnl-2018-316276 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Laine L, Barkun AN, Saltzman JR, et al. Acg clinical guideline: upper gastrointestinal and ulcer bleeding. Am J Gastroenterol 2021;116:899–917. 10.14309/ajg.0000000000001245 [DOI] [PubMed] [Google Scholar]
- 28. Barkun AN, Almadi M, Kuipers EJ, et al. Management of nonvariceal upper gastrointestinal bleeding: guideline recommendations from the International consensus group. Ann Intern Med 2019;171:805–22. 10.7326/M19-1795 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Carson JL, Stanworth SJ, Roubinian N, et al. Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst Rev 2016;10:CD002042. 10.1002/14651858.CD002042.pub4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Villanueva C, Colomo A, Bosch A, et al. Transfusion strategies for acute upper gastrointestinal bleeding. N Engl J Med 2013;368:11–21. 10.1056/NEJMoa1211801 [DOI] [PubMed] [Google Scholar]
- 31. Jairath V, Kahan BC, Gray A, et al. Restrictive versus liberal blood transfusion for acute upper gastrointestinal bleeding (trigger): a pragmatic, open-label, cluster randomised feasibility trial. Lancet 2015;386:137–44. 10.1016/S0140-6736(14)61999-1 [DOI] [PubMed] [Google Scholar]
- 32. Odutayo A, Desborough MJR, Trivella M, et al. Restrictive versus liberal blood transfusion for gastrointestinal bleeding: a systematic review and meta-analysis of randomised controlled trials. Lancet Gastroenterol Hepatol 2017;2:354–60. 10.1016/S2468-1253(17)30054-7 [DOI] [PubMed] [Google Scholar]
- 33. Razzaghi A, Barkun AN. Platelet transfusion threshold in patients with upper gastrointestinal bleeding: a systematic review. J Clin Gastroenterol 2012;46:482–6. 10.1097/MCG.0b013e31823d33e3 [DOI] [PubMed] [Google Scholar]
- 34. Estcourt LJ, Birchall J, Allard S, et al. Guidelines for the use of platelet transfusions. Br J Haematol 2017;176:365–94. 10.1111/bjh.14423 [DOI] [PubMed] [Google Scholar]
- 35. Overview | acute upper gastrointestinal bleeding in over 16S: management | guidance | NICE. [PubMed]
- 36. Harrison MF. The misunderstood coagulopathy of liver disease: a review for the acute setting. West J Emerg Med 2018;19:863–71. 10.5811/westjem.2018.7.37893 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Northup PG, Sundaram V, Fallon MB, et al. Hypercoagulation and thrombophilia in liver disease. J Thromb Haemost 2008;6:2–9. 10.1111/j.1538-7836.2007.02772.x [DOI] [PubMed] [Google Scholar]
- 38. Garcia-Tsao G, Abraldes JG, Berzigotti A. Portal hypertensive bleeding in cirrhosis: risk stratification, diagnosis, and management: 2016 practice guidance by the American association for the study of liver diseases 2016. 10.1002/hep.28906 [DOI] [PubMed]
- 39. Rockall TA, Logan RF, Devlin HB, et al. Risk assessment after acute upper gastrointestinal haemorrhage. Gut 1996;38:316–21. 10.1136/gut.38.3.316 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Blatchford O, Murray WR, Blatchford M. A risk score to predict need for treatment for upper-gastrointestinal haemorrhage. Lancet 2000;356:1318–21. 10.1016/S0140-6736(00)02816-6 [DOI] [PubMed] [Google Scholar]
- 41. Saltzman JR, Tabak YP, Hyett BH, et al. A simple risk score accurately predicts in-hospital mortality, length of stay, and cost in acute upper Gi bleeding. Gastrointest Endosc 2011;74:1215–24. 10.1016/j.gie.2011.06.024 [DOI] [PubMed] [Google Scholar]
- 42. Stanley AJ, Laine L, Dalton HR, et al. Comparison of risk scoring systems for patients presenting with upper gastrointestinal bleeding: international multicentre prospective study. BMJ 2017;356:i6432. 10.1136/bmj.i6432 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Laursen SB, Oakland K, Laine L, et al. Abc score: a new risk score that accurately predicts mortality in acute upper and lower gastrointestinal bleeding: an international multicentre study. Gut 2021;70:707–16. 10.1136/gutjnl-2019-320002 [DOI] [PubMed] [Google Scholar]
- 44. Ramaekers R, Mukarram M, Smith CAM, et al. The predictive value of Preendoscopic risk scores to predict adverse outcomes in emergency department patients with upper gastrointestinal bleeding: a systematic review. Acad Emerg Med 2016;23:1218–27. 10.1111/acem.13101 [DOI] [PubMed] [Google Scholar]
- 45. Laursen SB, Dalton HR, Murray IA, et al. Performance of new thresholds of the Glasgow Blatchford score in managing patients with upper gastrointestinal bleeding. Clin Gastroenterol Hepatol 2015;13:115–21. 10.1016/j.cgh.2014.07.023 [DOI] [PubMed] [Google Scholar]
- 46. Stanley AJ, Ashley D, Dalton HR, et al. Outpatient management of patients with low-risk upper-gastrointestinal haemorrhage: multicentre validation and prospective evaluation. Lancet 2009;373:42–7. 10.1016/S0140-6736(08)61769-9 [DOI] [PubMed] [Google Scholar]
- 47. Ananthakrishnan AN, McGinley EL, Saeian K. Outcomes of weekend admissions for upper gastrointestinal hemorrhage: a nationwide analysis. Clin Gastroenterol Hepatol 2009;7:296–302. 10.1016/j.cgh.2008.08.013 [DOI] [PubMed] [Google Scholar]
- 48. Barkun AN, Bardou M, Kuipers EJ, et al. International consensus recommendations on the management of patients with nonvariceal upper gastrointestinal bleeding. Ann Intern Med 2010;152:101–13. 10.7326/0003-4819-152-2-201001190-00009 [DOI] [PubMed] [Google Scholar]
- 49. Cipolletta L, Bianco MA, Rotondano G, et al. Outpatient management for low-risk nonvariceal upper Gi bleeding: a randomized controlled trial. Gastrointest Endosc 2002;55:1–5. 10.1067/mge.2002.119219 [DOI] [PubMed] [Google Scholar]
- 50. Bjorkman DJ, Zaman A, Fennerty MB, et al. Urgent vs. elective endoscopy for acute non-variceal upper-GI bleeding: an effectiveness study. Gastrointest Endosc 2004;60:1–8. 10.1016/s0016-5107(04)01287-8 [DOI] [PubMed] [Google Scholar]
- 51. Lee JG, Turnipseed S, Romano PS, et al. Endoscopy-based triage significantly reduces hospitalization rates and costs of treating upper Gi bleeding: a randomized controlled trial. Gastrointest Endosc 1999;50:755–61. 10.1016/s0016-5107(99)70154-9 [DOI] [PubMed] [Google Scholar]
- 52. Laursen SB, Leontiadis GI, Stanley AJ, et al. Relationship between timing of endoscopy and mortality in patients with peptic ulcer bleeding: a nationwide cohort study. Gastrointest Endosc 2017;85:936–44. 10.1016/j.gie.2016.08.049 [DOI] [PubMed] [Google Scholar]
- 53. Lau JYW, Yu Y, Tang RSY, et al. Timing of endoscopy for acute upper gastrointestinal bleeding. N Engl J Med 2020;382:1299–308. 10.1056/NEJMoa1912484 [DOI] [PubMed] [Google Scholar]
- 54. Karstensen JG, Ebigbo A, Bhat P, et al. Endoscopic treatment of variceal upper gastrointestinal bleeding: European Society of gastrointestinal endoscopy (ESGE) cascade guideline. Endosc Int Open 2020;8:E990–7. 10.1055/a-1187-1154 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Dunne PDJ, Laursen SB, Laine L, et al. Previous use of antithrombotic agents reduces mortality and length of hospital stay in patients with high-risk upper gastrointestinal bleeding. Clinical Gastroenterology and Hepatology 2019;17:440–7. 10.1016/j.cgh.2018.04.046 [DOI] [PubMed] [Google Scholar]
- 56. Chang H-Y, Zhou M, Tang W, et al. Risk of gastrointestinal bleeding associated with oral anticoagulants: population based retrospective cohort study. BMJ 2015;350:h1585. 10.1136/bmj.h1585 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Holster IL, Valkhoff VE, Kuipers EJ, et al. New oral anticoagulants increase risk for gastrointestinal bleeding: a systematic review and meta-analysis. Gastroenterology 2013;145:105–12. 10.1053/j.gastro.2013.02.041 [DOI] [PubMed] [Google Scholar]
- 58. Veitch AM, Radaelli F, Alikhan R, et al. Endoscopy in patients on antiplatelet or anticoagulant therapy: British Society of gastroenterology (Bsg) and European Society of gastrointestinal endoscopy (ESGE) guideline update. Gut 2021;70:1611–28. 10.1136/gutjnl-2021-325184 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Biondi-Zoccai GGL, Lotrionte M, Agostoni P, et al. A systematic review and meta-analysis on the hazards of discontinuing or not adhering to aspirin among 50,279 patients at risk for coronary artery disease. Eur Heart J 2006;27:2667–74. 10.1093/eurheartj/ehl334 [DOI] [PubMed] [Google Scholar]
- 60. Sung JJY, Lau JYW, Ching JYL, et al. Continuation of low-dose aspirin therapy in peptic ulcer bleeding: a randomized trial. Ann Intern Med 2010;152:1–9. 10.7326/0003-4819-152-1-201001050-00179 [DOI] [PubMed] [Google Scholar]
- 61. Chan FKL, Goh K-L, Reddy N, et al. Management of patients on antithrombotic agents undergoing emergency and elective endoscopy: joint Asian Pacific association of gastroenterology (APAGE) and Asian Pacific Society for digestive endoscopy (APSDE) practice guidelines. Gut 2018;67:405. 10.1136/gutjnl-2017-315131 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Laine L, Jensen DM. Management of patients with ulcer bleeding. Am J Gastroenterol 2012;107:345–60. 10.1038/ajg.2011.480 [DOI] [PubMed] [Google Scholar]
- 63. ASGE Standards of Practice Committee, Acosta RD, Abraham NS, et al. The management of antithrombotic agents for patients undergoing Gi endoscopy. Gastrointest Endosc 2016;83:3–16. 10.1016/j.gie.2015.09.035 [DOI] [PubMed] [Google Scholar]
- 64. Wolf AT, Wasan SK, Saltzman JR. Impact of anticoagulation on rebleeding following endoscopic therapy for nonvariceal upper gastrointestinal hemorrhage. Am J Gastroenterol 2007;102:290–6. 10.1111/j.1572-0241.2006.00969.x [DOI] [PubMed] [Google Scholar]
- 65. Witt DM, Delate T, Garcia DA, et al. Risk of thromboembolism, recurrent hemorrhage, and death after warfarin therapy interruption for gastrointestinal tract bleeding. Arch Intern Med 2012;172:1484–91. 10.1001/archinternmed.2012.4261 [DOI] [PubMed] [Google Scholar]
- 66. Carbonell N, Pauwels A, Serfaty L, et al. Erythromycin infusion prior to endoscopy for acute upper gastrointestinal bleeding: a randomized, controlled, double-blind trial. Am J Gastroenterol 2006;101:1211–5. 10.1111/j.1572-0241.2006.00582.x [DOI] [PubMed] [Google Scholar]
- 67. Coffin B, Pocard M, Panis Y, et al. Erythromycin improves the quality of EGD in patients with acute upper Gi bleeding: a randomized controlled study. Gastrointest Endosc 2002;56:174–9. 10.1016/s0016-5107(02)70174-0 [DOI] [PubMed] [Google Scholar]
- 68. Bai Y, Guo J-F, Li Z-S,. Meta-Analysis: erythromycin before endoscopy for acute upper gastrointestinal bleeding. Aliment Pharmacol Ther 2011;34:166–71. 10.1111/j.1365-2036.2011.04708.x [DOI] [PubMed] [Google Scholar]
- 69. Rahman R, Nguyen DL, Sohail U, et al. Pre-endoscopic erythromycin administration in upper gastrointestinal bleeding: an updated meta-analysis and systematic review. Ann Gastroenterol 2016;29:312–7. 10.20524/aog.2016.0045 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70. Cai J, Ribkoff J, Olson S, et al. The many roles of tranexamic acid: an overview of the clinical indications for TXA in medical and surgical patients. Eur J Haematol 2020;104:79. 10.1111/ejh.13348 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71. Bennett C, Klingenberg SL, Langholz E, et al. Tranexamic acid for upper gastrointestinal bleeding. Cochrane Database Syst Rev 2014;4. 10.1002/14651858.CD006640.pub3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72. Gayet-Ageron A, Prieto-Merino D, Ker K, et al. Effect of treatment delay on the effectiveness and safety of antifibrinolytics in acute severe haemorrhage: a meta-analysis of individual patient-level data from 40 138 bleeding patients. Lancet 2018;391:125–32. 10.1016/S0140-6736(17)32455-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73. Gluud LL, Klingenberg SL, Langholz E. Tranexamic acid for upper gastrointestinal bleeding. Cochrane Database Syst Rev;1. 10.1002/14651858.CD006640.PUB3 [DOI] [PubMed] [Google Scholar]
- 74. HALT-IT Trial Collaborators . Effects of a high-dose 24-h infusion of tranexamic acid on death and thromboembolic events in patients with acute gastrointestinal bleeding (HALT-IT): an international randomised, double-blind, placebo-controlled trial. Lancet 2020;395:1927–36. 10.1016/S0140-6736(20)30848-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75. Sreedharan A, Martin J, Leontiadis GI, et al. Proton pump inhibitor treatment initiated prior to endoscopic diagnosis in upper gastrointestinal bleeding. Cochrane Database Syst Rev 2010:CD005415. 10.1002/14651858.CD005415.pub3 [DOI] [PubMed] [Google Scholar]
- 76. Alleway R, Butt A, Freeth H. Improving the quality of healthcare time to get control? time to get control?.
- 77. Goulis J, Patch D, Burroughs AK. Bacterial infection in the pathogenesis of variceal bleeding. Lancet 1999;353:139–42. 10.1016/S0140-6736(98)06020-6 [DOI] [PubMed] [Google Scholar]
- 78. Bernard B, Cadranel JF, Valla D, et al. Prognostic significance of bacterial infection in bleeding cirrhotic patients: a prospective study. Gastroenterology 1995;108:1828–34. 10.1016/0016-5085(95)90146-9 [DOI] [PubMed] [Google Scholar]
- 79. Chavez-Tapia NC, Barrientos-Gutierrez T, Tellez-Avila FI, et al. Antibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleeding. Cochrane Database Syst Rev;20. 10.1002/14651858.CD002907.pub2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80. Hwang JH, Shergill AK, Acosta RD, et al. The role of endoscopy in the management of variceal hemorrhage. Gastrointest Endosc 2014;80:221–7. 10.1016/j.gie.2013.07.023 [DOI] [PubMed] [Google Scholar]
- 81. Sarin SK, Kumar A, Angus PW, et al. Diagnosis and management of acute variceal bleeding: Asian Pacific association for study of the liver recommendations. Hepatol Int 2011;5:607–24. 10.1007/s12072-010-9236-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82. Avgerinos A, Nevens F, Raptis S, et al. Early administration of somatostatin and efficacy of sclerotherapy in acute oesophageal variceal bleeds: the European acute bleeding oesophageal variceal episodes (above) randomised trial. Lancet 1997;350:1495–9. 10.1016/s0140-6736(97)05099-x [DOI] [PubMed] [Google Scholar]
- 83. Levacher S, Letoumelin P, Pateron D, Blaise M, Pourriat JL, et al. Early administration of terlipressin plus glyceryl trinitrate to control active upper gastrointestinal bleeding in cirrhotic patients. Lancet 1995;346:865–8. 10.1016/s0140-6736(95)92708-5 [DOI] [PubMed] [Google Scholar]
- 84. Seo YS, Park SY, Kim MY, et al. Lack of difference among terlipressin, somatostatin, and octreotide in the control of acute gastroesophageal variceal hemorrhage. Hepatology 2014;60:954–63. 10.1002/hep.27006 [DOI] [PubMed] [Google Scholar]
- 85. Alzoubaidi D, Lovat LB, Haidry R. Management of non-variceal upper gastrointestinal bleeding: where are we in 2018? Frontline Gastroenterol 2019;10:35. 10.1136/flgastro-2017-100901 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86. Forrest JA, Finlayson ND, Shearman DJ. Endoscopy in gastrointestinal bleeding. Lancet 1974;2:394–7. 10.1016/s0140-6736(74)91770-x [DOI] [PubMed] [Google Scholar]
- 87. Elmunzer BJ, Young SD, Inadomi JM, et al. Systematic review of the predictors of recurrent hemorrhage after endoscopic hemostatic therapy for bleeding peptic ulcers. Am J Gastroenterol 2008;103:2625–32. 10.1111/j.1572-0241.2008.02070.x [DOI] [PubMed] [Google Scholar]
- 88. Laine L, McQuaid KR. Endoscopic therapy for bleeding ulcers: an evidence-based approach based on meta-analyses of randomized controlled trials. Clin Gastroenterol Hepatol 2009;7:33–47. 10.1016/j.cgh.2008.08.016 [DOI] [PubMed] [Google Scholar]
- 89. Vergara M, Bennett C, Calvet X, et al. Epinephrine injection versus epinephrine injection and a second endoscopic method in high-risk bleeding ulcers. Cochrane Database Syst Rev 2014:CD005584. 10.1002/14651858.CD005584.pub3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90. El-Serag HB, Everhart JE. Improved survival after variceal hemorrhage over an 11-year period in the Department of Veterans Affairs. Am J Gastroenterol 2000;95:3566–73. 10.1111/j.1572-0241.2000.03376.x [DOI] [PubMed] [Google Scholar]
- 91. Laine L, Cook D, Deborah Cook MD. Endoscopic ligation compared with sclerotherapy for treatment of esophageal variceal bleeding. A meta-analysis. Ann Intern Med 1995;123:280–7. 10.7326/0003-4819-123-4-199508150-00007 [DOI] [PubMed] [Google Scholar]
- 92. Sarin SK, Lahoti D, Saxena SP, et al. Prevalence, classification and natural history of gastric varices: a long-term follow-up study in 568 portal hypertension patients. Hepatology 1992;16:1343–9. 10.1002/hep.1840160607 [DOI] [PubMed] [Google Scholar]
- 93. Sarin SK, Kumar A,. Gastric varices: profile, classification, and management. Am J Gastroenterol 1989;84:1244–9. [PubMed] [Google Scholar]
- 94. Lo GH, Lai KH, Cheng JS, et al. A prospective, randomized trial of butyl cyanoacrylate injection versus band ligation in the management of bleeding gastric varices. Hepatology 2001;33:1060–4. 10.1053/jhep.2001.24116 [DOI] [PubMed] [Google Scholar]
- 95. Lau JY, Sung JJ, Lee KK, et al. Effect of intravenous omeprazole on recurrent bleeding after endoscopic treatment of bleeding peptic ulcers. N Engl J Med 2000;343:310–6. 10.1056/NEJM200008033430501 [DOI] [PubMed] [Google Scholar]
- 96. Sachar H, Vaidya K, Laine L. Intermittent vs continuous proton pump inhibitor therapy for high-risk bleeding ulcers: a systematic review and meta-analysis. JAMA Intern Med 2014;174:1755–62. 10.1001/jamainternmed.2014.4056 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97. Freston JW, Pilmer BL, Chiu Y-L, et al. Evaluation of the pharmacokinetics and pharmacodynamics of intravenous lansoprazole. Aliment Pharmacol Ther 2004;19:1111–22. 10.1111/j.1365-2036.2004.01942.x [DOI] [PubMed] [Google Scholar]
- 98. Laine L, Shah A, Bemanian S. Intragastric pH with oral vs intravenous bolus plus infusion proton-pump inhibitor therapy in patients with bleeding ulcers. Gastroenterology 2008;134:1836–41. 10.1053/j.gastro.2008.03.006 [DOI] [PubMed] [Google Scholar]
- 99. Cheng H-C, Wu C-T, Chang W-L, et al. Double oral esomeprazole after a 3-day intravenous esomeprazole infusion reduces recurrent peptic ulcer bleeding in high-risk patients: a randomised controlled study. Gut 2014;63:1864–72. 10.1136/gutjnl-2013-306531 [DOI] [PubMed] [Google Scholar]
- 100. Gisbert JP, Abraira V. Accuracy of Helicobacter pylori diagnostic tests in patients with bleeding peptic ulcer: a systematic review and meta-analysis. Am J Gastroenterol 2006;101:848–63. 10.1111/j.1572-0241.2006.00528.x [DOI] [PubMed] [Google Scholar]
- 101. Bañares R, Albillos A, Rincón D, et al. Endoscopic treatment versus endoscopic plus pharmacologic treatment for acute variceal bleeding: a meta-analysis. Hepatology 2002;35:609–15. 10.1053/jhep.2002.31354 [DOI] [PubMed] [Google Scholar]
- 102. García-Pagán JC, Caca K, Bureau C, et al. Early use of tips in patients with cirrhosis and variceal bleeding. N Engl J Med 2010;362:2370–9. 10.1056/NEJMoa0910102 [DOI] [PubMed] [Google Scholar]
- 103. Dunne PDJ, Sinha R, Stanley AJ, et al. Randomised clinical trial: standard of care versus early-transjugular intrahepatic porto-systemic shunt (TIPSS) in patients with cirrhosis and oesophageal variceal bleeding. Aliment Pharmacol Ther 2020;52:98–106. 10.1111/apt.15797 [DOI] [PubMed] [Google Scholar]
- 104. Sabri SS, Abi-Jaoudeh N, Swee W, et al. Short-Term rebleeding rates for isolated gastric varices managed by transjugular intrahepatic portosystemic shunt versus balloon-occluded retrograde transvenous obliteration. J Vasc Interv Radiol 2014;25:355–61. 10.1016/j.jvir.2013.12.001 [DOI] [PubMed] [Google Scholar]
- 105. JYW L, Sung JJY, Lam YH. Endoscopic retreatment compared with surgery in patients with recurrent bleeding after initial endoscopic control of bleeding ulcers. N Engl J Med 1999;340:765–7. 10.1056/NEJM199903113401002 [DOI] [PubMed] [Google Scholar]
- 106. Kyaw M, Tse Y, Ang D, et al. Embolization versus surgery for peptic ulcer bleeding after failed endoscopic hemostasis: a meta-analysis. Endosc Int Open 2014;2:E6–14. 10.1055/s-0034-1365235 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107. Terés J, Cecilia A, Bordas JM, et al. Esophageal tamponade for bleeding varices. controlled trial between the Sengstaken-Blakemore tube and the Linton-Nachlas tube. Gastroenterology 1978;75:566–9. [PubMed] [Google Scholar]
- 108. Danis stent for acute oesophageal variceal bleeding medical technologies guidance, 2021. Available: www.nice.org.uk/guidance/mtg57 [Accessed 14 Jan 2022].
- 109. Escorsell Àngels, Pavel O, Cárdenas A, et al. Esophageal balloon tamponade versus esophageal stent in controlling acute refractory variceal bleeding: a multicenter randomized, controlled trial. Hepatology 2016;63:1957–67. 10.1002/hep.28360 [DOI] [PubMed] [Google Scholar]
- 110. Shung DL, Au B, Taylor RA, et al. Validation of a machine learning model that outperforms clinical risk scoring systems for upper gastrointestinal bleeding. Gastroenterology 2020;158:160–7. 10.1053/j.gastro.2019.09.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111. Deshmukh F, Merchant SS. Explainable machine learning model for predicting Gi bleed mortality in the intensive care unit. Am J Gastroenterol 2020;115:1657–68. 10.14309/ajg.0000000000000632 [DOI] [PubMed] [Google Scholar]
- 112. Jensen DM, Kovacs TOG, Ohning GV, v OG, et al. Doppler endoscopic probe monitoring of blood flow improves risk stratification and outcomes of patients with severe Nonvariceal upper gastrointestinal hemorrhage. Gastroenterology 2017;152:1310–8. 10.1053/j.gastro.2017.01.042 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113. Park J-S, Bang BW, Hong SJ, et al. Efficacy of a novel hemostatic adhesive powder in patients with refractory upper gastrointestinal bleeding: a pilot study. Endoscopy 2019;51:458–62. 10.1055/a-0809-5276 [DOI] [PubMed] [Google Scholar]
- 114. Branchi F, Klingenberg-Noftz R, Friedrich K, et al. PuraStat in gastrointestinal bleeding: results of a prospective multicentre observational pilot study. Surg Endosc 2022;36:2954–61. 10.1007/s00464-021-08589-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115. Beg S, Al-Bakir I, Bhuva M, et al. Early clinical experience of the safety and efficacy of EndoClot in the management of non-variceal upper gastrointestinal bleeding. Endosc Int Open 2015;3:E605–9. 10.1055/s-0034-1393087 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
No data are available.