

1. PATIENT PRESENTATION
A 19‐year‐old man presented to the emergency department with weakness, loss of appetite, and a weight loss of at least 13 kg in 5 months. He also complained of exertional dyspnea, dry cough, day and night sweats, and abdominal plus lower back pain. The physical examination revealed a temperature of 39.3°C but nothing else abnormal. The chest x‐ray (Figure 1) revealed a mass that appeared to be located in the posterior mediastinum.
FIGURE 1.
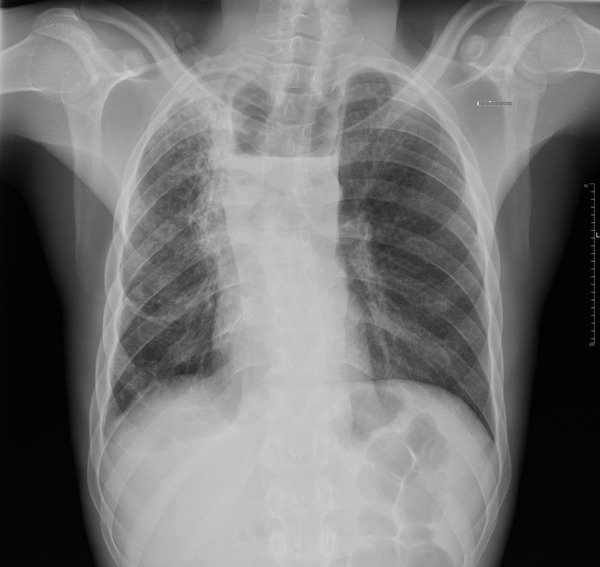
Chest X‐ray revealing a posterior mediastinum mass.
2. DIAGNOSIS: POTT'S DISEASE WITH EXTENDED DOUBLE PERISPINAL COLLECTION
A computed tomography (CT) scan (Figure 2) was performed in the emergency department to assess the extent of the disease, which showed pulmonary tuberculosis and spinal osteomyelitis associated with a perispinal collection from T1 to T12 and from L5 to S2, suggesting Pott's disease. 1 The diagnosis of disseminated tuberculosis was confirmed by the presence of Mycobacterium tuberculosis in culture. 2 A quadri‐therapy for tuberculosis was initiated with isoniazid, rifampicin, pyrazinamide, and ethambutol, then downgraded to a tri‐therapy because of the absence of resistance at the antibiogram. 3 Magnetic resonance imaging (Figure 3) performed later during the hospitalization revealed a staged spondylodiscitis associated with collections from the beginning of the extension to the central nervous system. Echocardiography confirmed the presence of associated chronic pericarditis. Finally, the indication for radio‐controlled drainage of the posterior mediastinal collection was decided owing to the important risk of fistulization. 4
FIGURE 2.
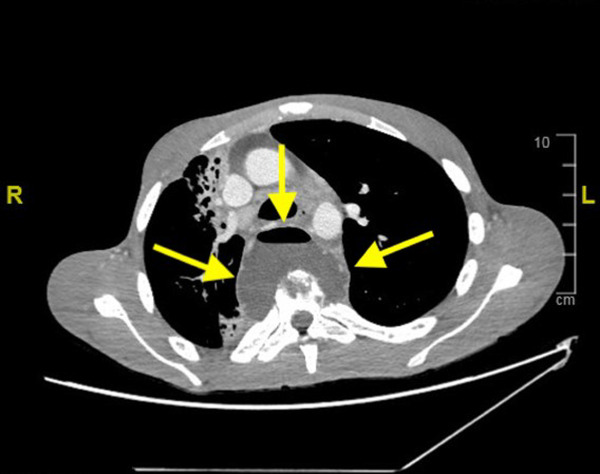
Computed tomography scan showing a perispinal collection from T1 to T12.
FIGURE 3.
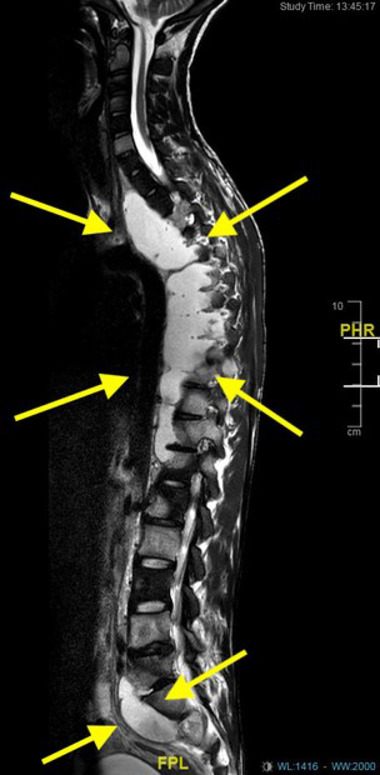
Magnetic resonance imaging exploring collections from T1 to T12 and from L5 to S2.
Tuberculosis is caused by slow growing aerobic bacilli, Mycobacterium tuberculosis complex. This disease, affecting mainly the lungs, also takes osteoarticular forms, the most frequent of which is spondylodiscitis. Spinal involvement is always secondary to hematogenous dissemination of bacilli from the primary site. 5 Pott's disease results from an infection of the vertebrae (spondylitis) and intervertebral discs (discitis) with M. tuberculosis. The intervertebral disc is a relatively avascular structure and is spared until late stage of the disease. Bone destruction in spinal tuberculosis can be fragmentary, osteolytic, subperiosteal, or localized destruction with sclerosed margins. Cold abscesses are pus collections that lack surrounding inflammatory response and are seen in nearly 70% of patients with spinal tuberculosis. This is a severe form of the disease, located near nerve structures, which may be significantly and permanently affected, and may be life threatening.
Fremery A, Zappa M, Pujo J, Epelboin L. Air‐fluid level in the mediastinum. JACEP Open. 2023;4:e12916. 10.1002/emp2.12916
REFERENCES
- 1. Rajasekaran S, Soundararajan DCR, Shetty AP, Kanna RM. Spinal tuberculosis: current concepts. Glob Spine J. 2018;8(4):96S‐108S. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Akkerman OW, van der Werf TS, de Boer M, et al. Comparison of 14 molecular assays for detection of Mycobacterium tuberculosis complex in bronchoalveolar lavage fluid. J Clin Microbiol. 2013;51(11):3505‐3511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Yong LN, Ahmedy F, Yin KN, Engkasan JP. Functional outcomes in spinal tuberculosis: a review of the literature. Asian Spine J. 2021;15(3):381‑391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Garg D, Goyal V. Spinal tuberculosis treatment: an enduring bone of contention. Ann Indian Acad Neurol. 2020;23(4):441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Kubihal V, Sharma R, Krishna Kumar RG, et al. Imaging update in spinal tuberculosis. J Clin Orthop Trauma. 2021;25:101742. [DOI] [PMC free article] [PubMed] [Google Scholar]