

Abstract
Increased global demand for touch screens, photovoltaics, and optoelectronics has resulted in an increase in the production of indium–tin oxide (ITO). Occupational exposure to indium compounds is associated with the development of indium lung disease. Although many previous epidemiologic investigations highlight an excess of lung abnormalities in workplaces where ITO is produced, few assessments of occupational exposure to respirable and inhalable indium are reported to date. The objective of this study was to identify the determinants of respirable and inhalable indium at an ITO production facility to target exposure interventions. In 2012 and 2014, we conducted exposure assessments at an ITO production facility and collected full-shift personal respirable (n = 159) and inhalable (n = 57) indium samples. We also observed workers and recorded information on task duration and location, materials used, and use of personal protective equipment (PPE). Tasks (n = 121) recorded in task diaries were categorized into 40 similar task groups using the Advanced REACH Tool and process-related information. Mixed-effects models were fit separately for log-transformed respirable and inhalable indium, with random effect of subject and fixed effects of task groups. Overall, respirable and inhalable indium measurements ranged from 0.1 to 796.6 μg m−3 and 1.6 to 10 585.7 μg m−3, respectively, and were highly correlated with Spearman correlation coefficient of 0.90. The final model for respirable indium explained 36.3% of total variance and identified sanding, powder transfer tasks in reclaim, powder transfer tasks in refinery, handling indium materials, and liquid transfer tasks in ITO production as tasks associated with increased respirable indium exposure. The final model for inhalable indium explained 24.6% of total variance and included powder transfer tasks in ITO production, cleaning cylinder or tile, and handling indium material tasks. Tasks identified as strong predictors of full-shift exposure to respirable and inhalable indium can guide the use of engineering, administrative, and PPE controls designed to mitigate occupational exposure to indium. Moreover, since the tasks were aligned with REACH activities, results from this study can also be used to inform REACH activity scenarios.
Keywords: determinants of exposure, exposure assessment, indium, indium–tin oxide, inhalable, metals, respirable work task
Introduction
Increased global demand for indium–tin oxide (ITO) in flat-panel displays, touch screens, photovoltaics, and optoelectronics in the last 20 years has resulted in increases in the production, use, and reclamation of ITO (Omae et al., 2011; Hines et al., 2013). Occupational exposure to indium is associated with indium lung disease which is characterized as pulmonary alveolar proteinosis that can progress to pulmonary fibrosis with or without emphysema (Cummings et al., 2012). Indium lung disease was previously reported in workers involved in the production, use, or reclamation of indium (Omae et al., 2011) and symptoms have been observed as early as 1 year after first exposure to indium (Cummings et al., 2013). Disease can initially present as cough and dyspnea without a work-related pattern and can progress to disability and death (Cummings et al., 2013). Indium concentration in serum or plasma of exposed workers is used as an exposure metric in epidemiological studies. However, little is known about the relationship between serum or plasma indium measurements and occupational exposure to respirable and inhalable indium because few published studies have included both a medical evaluation and exposure assessment of the workplace (Cummings et al., 2016).
Previous epidemiological studies that included an exposure assessment focused on respirable indium exposure because indium lung disease manifests in the alveolar region of the lung and respirable indium is the logical choice for this health endpoint (Cummings et al., 2010, 2012). However, correlations between measurements of indium in blood matrices and current respirable indium exposure are inconsistent (Hoet et al., 2012; Cummings et al., 2016). Differences between these measurements might be due to different chemical forms of indium and their relative solubilities as well as not accounting for larger, inhalable particles containing indium that deposit in the upper and conducting airways and contribute to plasma or serum indium levels (Hawley Blackley et al., 2019). Additionally, measurements of indium in plasma or serum reflect both current exposure and historical exposure that could have occurred in different working conditions (Cummings et al., 2016; Hawley Blackley et al., 2019). Although many previous epidemiologic investigations highlight an excess of lung abnormalities in workplaces where indium lung disease occurred, few exposure assessments of occupational exposure to respirable and inhalable indium have been reported to date (Chen, 2007; Miyauchi et al., 2012; Cummings et al., 2013).
Two previous occupational exposure assessments at facilities where ITO was used or produced reported highly variable exposures, with partial- to full-shift time-weighted average (TWA) exposures ranging from 0.0004 to 0.11 milligrams per meter cubed (mg m−3) respirable indium, 0.41 to 3.3 mg m−3 inhalable indium, and less than 0.0048 to 9.8 mg m−3 total indium (NIOSH, 2012; Hines et al., 2013). The ACGIH® recently adopted a Threshold Limit Value (TLV®) TWA of 0.0001 mg m−3 for respirable particulate matter as indium to protect against adverse lung effects including effects on pulmonary function, inflammation, alveolar proteinosis, and lung fibrosis (ACGIH, 2019). Full-shift sampling can be used to identify jobs with the highest TWA exposures, but requires additional information to unravel the causes of variation. Specific tasks and processes that contribute to high full-shift TWAs can be overlooked without (i) task-based sampling or (ii) task diaries and modeling of tasks as predictors of full-shift exposures (Goldberg et al., 1997; Seixas et al., 2003; Thilsing et al., 2015). Task-based sampling can be utilized when assessing occupational exposures sufficiently high to capture detectable quantities of an analyte, despite shorter sampling durations. However, task-based sampling is expensive in terms of time, equipment, and sample analyses. A cost-effective alternative approach to task-based sampling is to use task diaries in combination with full-shift samples to identify determinants of full-shift exposures. The objective of this study was to identify the determinants of exposure to respirable and inhalable indium at an ITO manufacturing facility to target exposure interventions. Tasks identified as strong predictors of full-shift exposure to respirable and inhalable indium can help inform control strategies designed to mitigate occupational exposure to indium.
Methods
Process description
The ITO manufacturing facility processes indium oxide and tin oxide into ITO ceramic tiles used by customers for sputtering applications and the manufacturing processes have been described previously. (Medvedovski et al., 2008; Cummings et al., 2013; Hines et al., 2013; Badding et al., 2014; Hawley Blackley et al., 2019) The major steps in the production of ITO ceramic tiles and reclamation of indium starts in the refinery, where indium oxide is produced from solid indium metal. In the ITO area, indium oxide and tin oxide are mixed together. The resulting mixture is formed into planar or cylindrical tiles in the casting areas or spray dried followed by cold isostatic pressing. These tiles undergo limited cutting and sanding, and are then fired to sinter the ITO. After firing, the sintered tiles are ground and cut to customers’ specifications in the grinding areas. Once cut, a backing material is applied to the tiles in the bonding area, after which the tiles are packaged and shipped. In the reclaim area, spent tiles and waste materials from all production areas are converted to indium metal. Molten metal is then cast into ingots and finally into shot to be used in the refinery. Other production-related processes include quality control (QC) and research and development (R&D).
Respirable and inhalable indium exposure assessment
We performed exposure assessments at the ITO production and reclamation facility in June and September 2012 and in July 2014. Full-shift and composite personal samples were collected to assess personal exposure to respirable and inhalable indium. Composite samples were collected in administrative areas, and included sampling over multiple shifts/days on the same media to collect adequate mass to reach the detection limit. Additionally, NIOSH staff observed workers as they performed their regular job duties and periodically recorded task duration, task location, materials, and use of personal protective equipment (PPE) in task diaries. The use of an N95, full-face, or powered air purifying (PAPR) respirator was recorded and used to calculate the percent time of a full-shift sample that was spent in respiratory protection.
GK2.69 cyclones (BGI, Inc., Waltham, MA) operated at 4.2 liters per minutes (Lpm) flow rate and equipped with a two-piece, 37-millimeter (mm) cassette sampler were used to collect personal respirable samples on 49 workers during the 2012 exposure assessment. The 37-mm cassette samplers were loaded with 5-micrometer (μm) pore size polyvinyl chloride (PVC) filters and samples were collected for 6–22 h duration. A total of 110 samples were collected using respirable cyclones. IOM personal samplers (SKC, Inc., Eighty Four, PA) operated at 2 Lpm and equipped with a multidisc foam insert and a PVC filter were used to collect both respirable and inhalable personal samples on 39 workers during the 2014 exposure assessment. A total of 59 respirable and inhalable samples were collected in 2014. Sample duration ranged from 4 to 9 h. Ten respirable and two inhalable samples were excluded from analyses due to equipment malfunction or incomplete task diaries.
All air samples were analyzed for indium content using inductively coupled plasma atomic emission spectrometry in accordance with NIOSH Method 7303, using methods described previously (Hawley Blackley et al., 2019). Limits of detection (LOD) were 0.375 μg respirable indium per sample collected using the respirable cyclone, 0.4 μg per IOM filter sample, and 0.3 μg per IOM foam sample.
Respirable sampler correction equation
Side-by-side area air samples using IOMs and respirable cyclones were collected throughout the ITO production and reclamation facility. Pairs of IOMs and respirable cyclones were placed in seventeen fixed locations in production areas, to include the planar and rotary bond shops, ITO areas, planar and rotary grinding areas, reclaim, refinery, and R&D. Orthogonal regression models were fit using log-transformed respirable indium from the respirable cyclone as the outcome variable, and the IOM as the predictor variable, with the assumption that the error in variance was equal for the pairs of samplers, as described previously (Hawley Blackley et al., 2019). Respirable indium measurements from the IOM samplers were adjusted to account for differences with the respirable cyclones, using equation (1),
| (1) |
where Resp Cyclone and IOM represent respirable indium sampling results in μg m−3.
Statistical analyses
Statistical analyses were conducted using SAS software version 9.4 (SAS Institute, Inc., Cary, NC). Because plots of the full-shift TWA exposure data indicated the distributions were not normal, respirable and inhalable indium TWA measurements were log-transformed for all analyses. Exposure data were summarized using the geometric mean (GM), geometric standard deviation (GSD), and estimated 95th percentile including correlation analysis and orthogonal regression for respirable and inhalable indium.
Tasks recorded in task diaries were categorized into task groups using the Advanced REACH Tool and process-related information (see Supplementary Table S1, available at Annals of Work Exposures and Health online edition). Multiple mixed-effects regression models were developed to identify the determinants of exposure, with log-transformed respirable and inhalable indium as dependent variables, subject ID as random effect, and task groups as independent fixed-effects predictor variables. The default covariance structure (variance components—VCs) was assumed and estimates of VCs were based on the restricted maximum-likelihood method. Univariate analysis was used to evaluate significance of individual tasks, task groups, and tasks by department as predictors of full-shift respirable and inhalable indium. Task groups were split by department when respirable or inhalable indium exposure was different (P < 0.05) by department. Forward selection procedure was used to construct the final multiple regression models. Single covariates with a P-value of less than 0.2 significance level were added to the model using forward stepwise selection and only task groups with a significance level of less than 0.1 were retained in the model. Variables were added until no improvement to the model was made. Task groups were included in the model as continuous variables representing total minutes spent performing the task during full-shift exposure monitoring. A null model was constructed for each outcome variable with no fixed effects and the random effects of subject ID to obtain the total, within-worker, and between-worker VCs. The percent variance explained by the fixed effects were estimated by calculating the difference in the total, between-worker and within-worker variance estimates between the null and the full models.
Results
Respirable and inhalable indium exposure assessment
A total of 159 respirable and 57 inhalable indium measurements were collected on 65 and 39 workers, respectively, among all fourteen departments at the facility (Table 1). Less than 1% of all measurements for respirable indium were below the LOD (n = 1). For respirable indium, 31% of workers had a single measurement, while 69% had repeated measurements (28% with two measurements, 21% with three measurements and 20% workers four or more measurements). For inhalable indium, 54 of workers had a single measurement, while 46% had two measurements. Some workers (35%) participated in both exposure surveys, while 39% participated only in 2012 and 26% participated only in 2014 surveys. All samples for inhalable indium were above the LOD. Logged values of respirable and inhalable indium measurements were strongly correlated with a Spearman correlation coefficient of ρ = 0.90 (Fig. 1). With the exception of the rotary bond shop machinist, all TWA respirable exposures exceeded the TLV®. The highest respirable and inhalable indium concentrations were observed on ITO operators, reclaim operators, and R&D project technicians (Table 1). Respirable indium exposures measured on ITO operators, reclaim operators, and R&D project technicians ranged from 1.1 to 518.3 μg m−3, 4.8 to 796.6 μg m−3, and 2.2 to 694.3 μg m−3, respectively. Inhalable indium exposures measured on ITO operators, reclaim operators, and R&D project technicians ranged from 68.0 to 1716.3 μg m−3, 150.7 to 2562.9 μg m−3, and 95.9 to 10 585.7 μg m−3, respectively. ITO operators, reclaim operators, and R&D project technicians wore full-face respirator or PAPR 9.1%, 17.6%, and 5.8% of the time.
Table 1.
Personal full-shift TWA exposure levels for respirable indium and inhalable indium by department and job group.
| Work group | Department | Job group | Respirable indium (μg m−3) |
Inhalable indium (μg m−3) |
||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | GM | GSD | 95th % tile | N | GM | GSD | 95th %tile | |||
|
| ||||||||||
| Administrative | Administrative | Administrative | 4 | 1.5 | 1.1 | 1.8 | 4 | 12.4 | 1.5 | 23.8 |
| Production | Bond Shop-Planar | Planar Bond Technician | 8 | 8.8 | 4.0 | 85.2 | 4 | 111.8 | 6.5 | 2437.5 |
| Bond Shop-Rotary | Rotary Bond Operator | 6 | 3.4 | 2.9 | 19.4 | 6 | 42.6 | 2.6 | 205.1 | |
| Rotary Bond Technician | 9 | 3.0 | 2.0 | 9.6 | – | – | – | – | ||
| Machinist | 1 | <0.1 | – | – | 1 | <1.6 | – | – | ||
| ITO | ITO Lead Operator | 3 | 11.6 | 1.2 | 14.7 | – | – | – | – | |
| ITO Operator | 27 | 38.0 | 3.7 | 320.7 | 8 | 282.9 | 2.8 | 1540.6 | ||
| Planar Grinding | ITO Grinder | 6 | 14.6 | 4.6 | 181.0 | 2 | 90.5 | 1.9 | 258.7 | |
| PTC Saw Operator | 6 | 10.7 | 2.4 | 43.9 | 2 | 74.2 | 2.1 | 251.7 | ||
| Reclaim | Reclaim Operator | 16 | 41.5 | 4.5 | 499.0 | 3 | 581.0 | 4.1 | 6021.1 | |
| Refinery | Refinery Operator | 9 | 17.1 | 2.0 | 51.7 | 3 | 125.7 | 1.7 | 289.5 | |
| Rotary Grinding | ITO Grinder | 1 | 21.5 | 2.3 | 81.6 | 2 | 156.2 | 2.3 | 610.2 | |
| Machinist | 4 | 36.4 | 1.6 | 78.2 | – | – | – | – | ||
| Maintenance | Maintenance | 8 | 6.5 | 2.3 | 26.1 | 4 | 68.1 | 1.9 | 190.0 | |
| Janitor | 2 | 3.4 | 1.1 | 4.2 | – | – | – | – | ||
| Production Support | Engineering | Engineer | 10 | 2.5 | 1.9 | 7.2 | 2 | 43.7 | 11.4 | 2405.6 |
| QC Lab | QA/QC Technician | 6 | 2.8 | 2.3 | 10.9 | 3 | 28.3 | 4.9 | 387.3 | |
| QA/QC Inspector | 6 | 2.3 | 2.2 | 8.7 | 4 | 20.5 | 1.3 | 31.5 | ||
| R&D | R&D Project Technician | 10 | 21.4 | 5.9 | 398.2 | 4 | 428.2 | 8.8 | 15 303.4 | |
| Process Chemist | 2 | 2.1 | 1.0 | 2.1 | – | – | – | – | ||
| Shipping and Receiving | Shipper | 4 | 1.5 | 1.3 | 2.4 | 2 | 19.2 | 1.7 | 46.8 | |
| Forming | Master Mold Maker | 3 | 1.5 | 3.5 | 11.8 | 2 | 13.2 | 1.9 | 37.4 | |
| Mold Maker | 7 | 3.3 | 3.0 | 19.9 | 1 | 5.7 | – | – | ||
| Total Samples | 159 | 57 | ||||||||
GM, geometric mean; GSD, geometric standard deviation; 95th %tile, estimates of the 95th percentile; < indicates a sample that was below the LOD.
Figure 1.
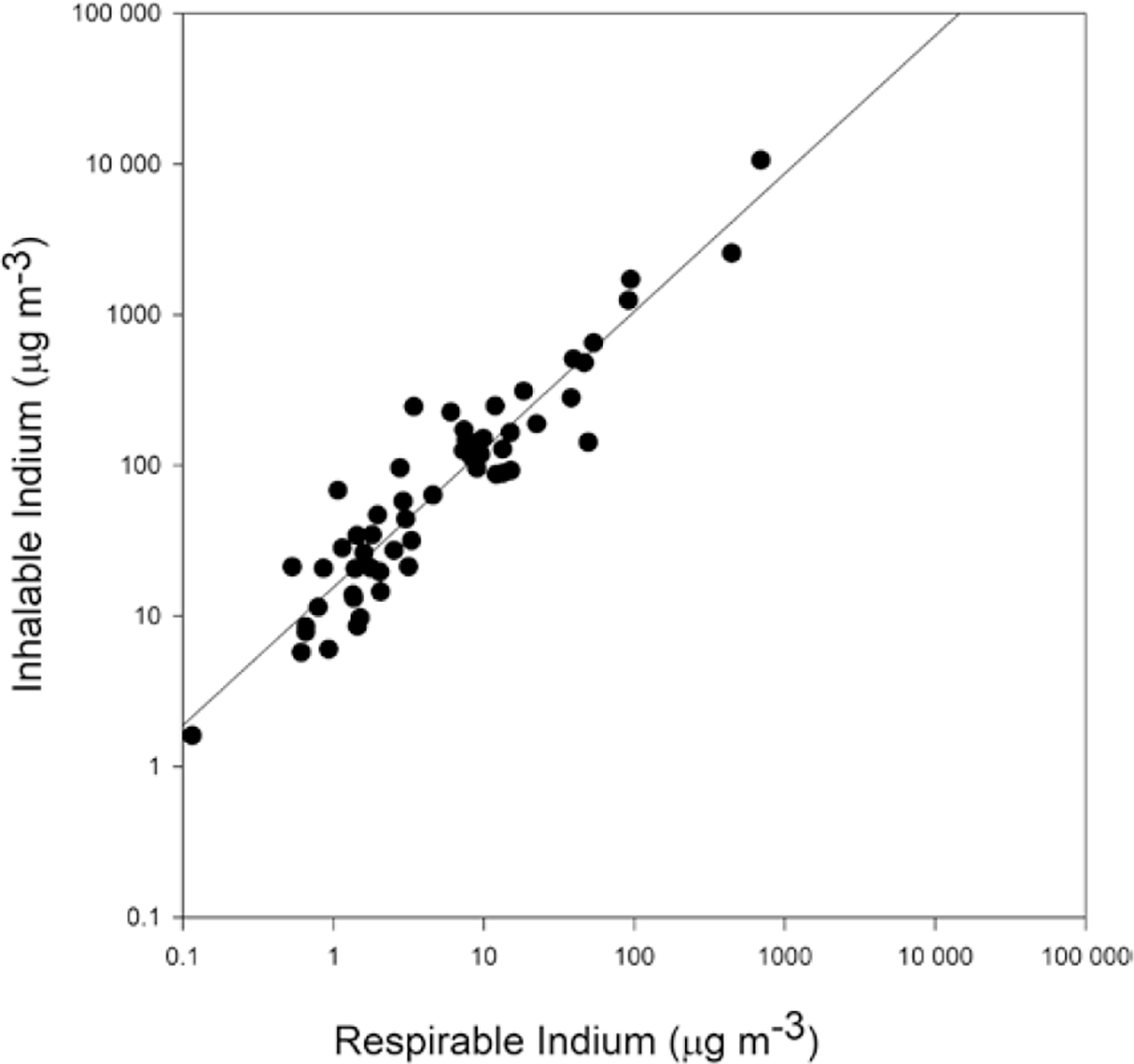
Scatterplot of respirable and inhalable indium measurements.
Task groups
Tasks recorded in task diaries (n = 121 tasks) were categorized into 40 task groups (see Supplementary Table S1, available at Annals of Work Exposures and Health online edition). Task group by department as a predictor of respirable or inhalable indium was significant for powder transfer and powder fraction task groups and these were divided into: powder transfer, reclaim; powder transfer, refinery; powder transfer, ITO; powder transfer, all other departments (R&D, forming); powder fraction, reclaim; and powder fraction, all other departments (ITO, refinery, R&D, and QC Lab) (see Supplementary Table S1, available at Annals of Work Exposures and Health online edition).
Tasks as determinants of respirable indium exposure
Results from the linear mixed-effects model for respirable indium can be seen in Table 2. The frequency of task occurrence, the average time spent performing the task, and the use of PPE is also displayed in Table 2. The model for respirable indium included six task groups that explained 30.0% of the within-worker variability and 43.9% of the between-worker variability. The total variance was 36.3% lower than the null model. Tasks that increased exposure to respirable indium included sanding, powder transfer tasks in reclaim, powder transfer tasks in refinery, handling indium materials, and liquid transfer tasks in ITO. Correlations among the predictor variable were mostly negative and the Pearson correlation coefficient ranged from ρ = −0.054 to 0.17. Packaging tasks were associated with lower exposure to respirable indium. Sanding was the strongest positive determinant of respirable indium (Table 2). Performing sanding for the average duration 87 min is estimated to increase respirable indium exposure by 10-fold (exp(0.027 × 87 min)). Estimates of respirable indium exposure during sanding tasks ranged from 11.4 to 604.3 μg m−3 for sanding times ranging from 25 to 172 min (Fig. 2). PPE in the form of a full-face respirator or PAPR was observed being used 55.8% of the time and N95 respirators were observed being used 10% of the time that sanding was performed (Table 2). Powder transfer tasks in reclaim also significantly increased exposure. Performing powder transfer tasks in reclaim for the average duration of 116 min is estimated to increase respirable indium exposure by 6.4-fold. Estimates of exposure during powder transfer tasks in reclaim ranged from 9.4 to 209.4 μg m−3 (Fig. 2). The highest frequency of use of a full-face respirator or PAPR was observed during powder transfer tasks in reclaim (84.3%). Powder transfer tasks in the refinery also significantly increased exposure to respirable indium. Estimates of exposure during powder transfer tasks in the refinery ranged from 6.8 to 40.9 μg m−3 (Fig. 2).
Table 2.
Effect of tasks on personal level of exposure to respirable indium (μg m−3)
| Model with tasks | N | Average time spent performing task, per shiftb (min–max) | β a | e | P | %time observed in N95 | %time observed in full-face or PAPR |
|---|---|---|---|---|---|---|---|
|
| |||||||
| Intercept | 159 | – | 1.76 | 0.15 | <0.0001 | – | – |
| Sanding | 9 | 87 (25–172) | 0.027 | 0.004 | < 0.0001 | 10.0 | 55.8 |
| Powder transfer, reclaim | 9 | 116 (30–224) | 0.016 | 0.003 | < 0.0001 | 0 | 84.3 |
| Package | 8 | 80 (15–319) | −0.006 | 0.003 | 0.09 | 17.2 | 0 |
| Powder transfer, refinery | 6 | 58 (10–122) | 0.016 | 0.008 | 0.05 | 24.8 | 5.5 |
| Handling indium materials | 10 | 43 (5–95) | 0.014 | 0.008 | 0.07 | 0 | 7.0 |
| Liquid transfer, ITO | 17 | 56 (5–135) | 0.014 | 0.005 | 0.02 | 0 | 15.6 |
| Random effects model | Mixed model | % variance explained | |||||
| σ 2 ww | 1.38 | 0.98 | 30.0 | ||||
| σ 2 bw | 1.32 | 0.74 | 43.9 | ||||
| σ 2 total | 2.70 | 1.72 | 36.3 | ||||
N, number of observations; β, regression coefficient for ln-transformed exposure data; e, standard, error; P, P value; %time, percent time.
Per 1 min of task performance.
Average time in minutes.
Figure 2.
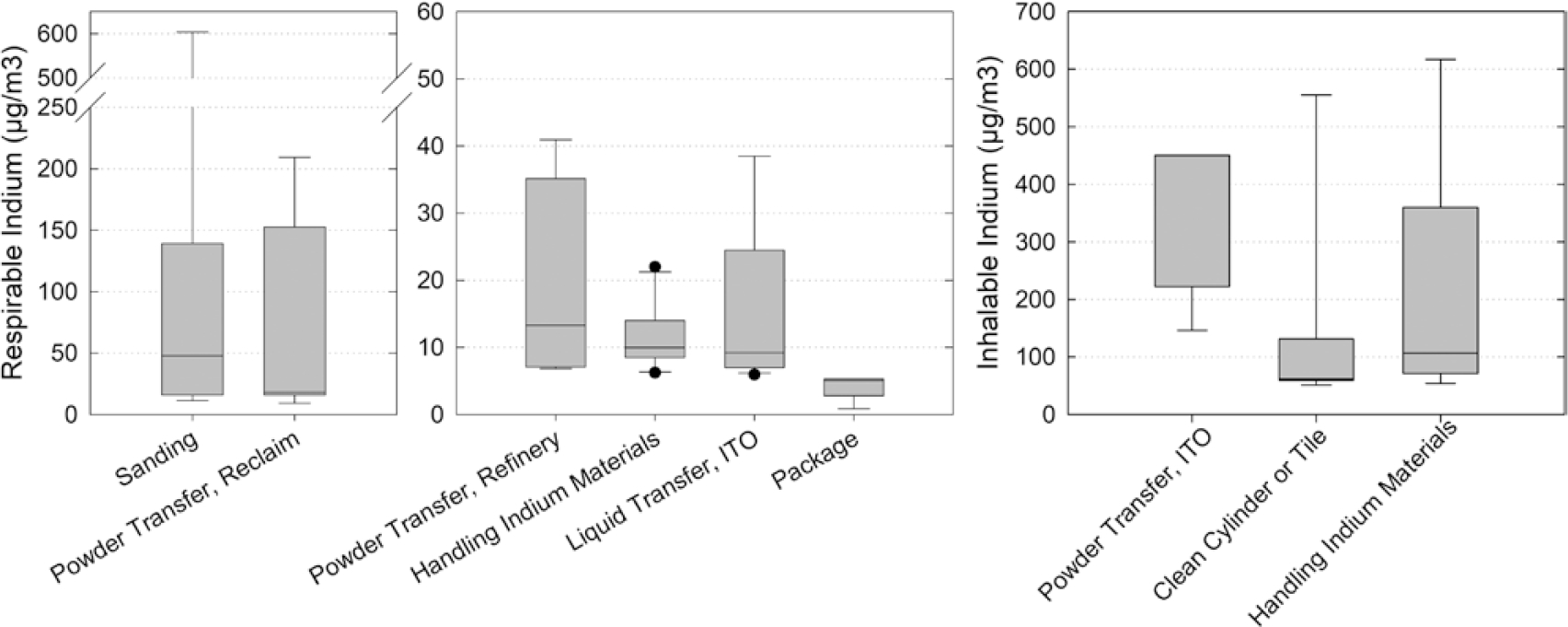
Model estimates of respirable and inhalable indium exposure during specific tasks.
Tasks as determinants of inhalable indium exposure
Results from the linear mixed-effects model for inhalable indium can be seen in Table 3. The frequency of task occurrence, the average time spent performing the task, and the use of PPE is also seen in Table 3. The model for inhalable indium included three task groups that explained 24.6% of the total variance. Tasks that increased exposure to inhalable indium included powder transfer tasks in ITO, cleaning a cylinder or tile, and handling indium materials. Correlations among the predictor variable were all negative and the Pearson correlation coefficient ranged from ρ = −0.045 to −0.025. Powder transfer task in ITO was the strongest positive determinant of exposure to inhalable indium (Table 3). Performing powder transfer tasks in ITO for the average duration 26 min is estimated to increase inhalable indium exposure by 7-fold (exp(0.075 × 26 min)). Estimates of inhalable indium exposure during powder transfer tasks in ITO ranged from 146.2 to 450.3 μg m−3 for the task duration of 15–30 min (Fig. 2). PPE in the form of a full-face respirator or PAPR was observed being used 14.3% of the time and N95 respirators were observed being used 28.6% of the time that powder transfer tasks in ITO were performed (Table 3). Handling indium material also significantly increased exposure. Handling indium materials for the average duration of 41 min is estimated to increase respirable indium exposure by 3-fold (exp(0.027 × 41 min)). Estimates of inhalable indium exposure during handling indium materials tasks ranged from 54.3 to 617.1 μg m−3 (Fig. 2). PPE in the form of a PAPR was used 12.3% of the time that handling indium materials tasks were performed.
Table 3.
Effect of tasks on personal level of exposure to inhalable indium (μg m−3)
| Model with tasks | N | Average timeb spent performing task, per shift (min–max) | β a | e | P | %time observed in N95 | %time observed in full-face or PAPR |
|---|---|---|---|---|---|---|---|
|
| |||||||
| Intercept | 57 | – | 3.86 | 0.23 | <0.0001 | – | – |
| Powder transfer, ITO | 4 | 26 (15–30) | 0.075 | 0.027 | 0.013 | 28.6 | 14.3 |
| Clean cylinder or tile | 8 | 44 (5–164) | 0.015 | 0.008 | 0.08 | 50.7 | 0 |
| Handling indium materials | 6 | 41 (5–95) | 0.027 | 0.012 | 0.03 | 0 | 12.3 |
| Random effects model | Mixed model | % variance explained | |||||
| σ 2 total | 2.85 | 2.15 | 24.6 | ||||
N, number of observations; β, regression coefficient for ln-transformed exposure data; e, standard, error; P, P value; %time, percent time.
Per 1 min of task performance.
Average time in minutes.
Discussion
We performed an exposure assessment of respirable and inhalable indium at an ITO production facility in 2012 and 2014. Few exposure assessments of occupational exposure to respirable and inhalable indium have been reported to date despite previous epidemiologic investigations observing an excess of lung abnormalities in workplaces where indium lung disease occurred (Chen, 2007; Miyauchi et al., 2012; Cummings et al., 2013). In 2002, the company introduced periodic air sampling designed to identify areas of high indium exposure that could be targeted with exposure mitigation controls. The company’s air sampling data from partial to full-shift samples collected in 2005 measured respirable indium concentrations ranging from 4 to 111 μg m−3 in the reclaim area, grinding area, and ITO areas. Inhalable indium measurements collected by the company in 2005 and 2006 ranged from 410 to 3300 μg m−3 in the reclaim and grinding areas (NIOSH, 2012; Hines et al., 2013). The highest measurements of respirable and inhalable indium were observed in the reclaim area (NIOSH, 2012). Subsequently, the company introduced engineering, administrative, and PPE controls to mitigate exposure to indium. Exposure controls included installing ventilation filtration devices; installing upgraded reclaim milling and mixing equipment; isolating and enclosing grinding processes; installing a downdraft table in the ITO inspection room of ITO; placing tacky mats outside of the doors of production and non-production areas; and implementing a respiratory protection program (NIOSH, 2012). Despite exposure mitigation strategies implemented prior to assessments in 2012 and 2014, we observed that reclaim operators continued to have the highest exposures to respirable and inhalable indium. Personal full-shift samples collected on reclaim operators ranged from 4.8 to 796.6 μg m−3 respirable and 150.7 to 2562.9 μg m−3 inhalable indium. Overall, we observed that reclaim operators, ITO operators, and R&D project technicians had the highest full-shift TWA exposures to respirable and inhalable indium.
We observed inconsistent PPE use during many tasks associated with increased exposure to respirable and inhalable indium, indicating a need for better PPE training and compliance among workers who perform high exposure tasks. However, even if respiratory protection with an assigned protection factor of 1000 was used 100% of the time by all job groups, with the exception of machinists in the rotary bond shop, workers in all job groups could be exposed to concentrations of respirable indium above the ACGIH TLV-TWA of 0.1 μg m−3 (ACGIH, 2019). Further, PPE in the form of respiratory protection is considered the least effective means for controlling respiratory exposures because breakdowns in implementation can result in insufficient protection. Alternatively, engineering controls are preferred to PPE controls because engineering controls can remove the hazard at its source, before it comes into contact with the worker (NIOSH, 2015). Results from our exposure assessment indicated that additional engineering and administrative controls are necessary to mitigate exposures throughout the facility.
Previous studies observed that when full-shift area sampling is used to guide engineering, administrative, and PPE controls designed to mitigate occupational exposure, specific tasks and processes that contribute to high full-shift TWA exposures can be overlooked (Goldberg et al., 1997; Seixas et al., 2003; Thilsing et al., 2015). Additionally, as we observed at this facility, considerable heterogeneity in mean exposure levels can exist among workers with the same job title, due to different tasks, different types of equipment used, and different levels of training and experience (Rappaport and Kupper, 2008). Task-based sampling provides information about tasks and procedures that generate intermittent, high exposures, but is expensive and may result in non-detectable measurements. Real-time particulate sampling may also identify high dust exposure tasks however, these tasks may not correspond to high indium exposure tasks because real-time samplers are not specific for any chemical, the indium content of the dust was variable at this facility. We used task diaries in combination with full-shift samples and identified six groups of tasks that contributed respirable indium exposure and three groups of tasks that contributed inhalable indium exposure.
Results from our linear mixed-effects model identified specific tasks associated with increases in respirable and inhalable indium and explained 36.3% and 24.6% of the variation in exposures, respectively. The total variances explained in our linear mixed-effects models for respirable and inhalable indium are similar to what other researchers using mixed modeling have published for other industries. Previous studies using mixed models to identify determinants of exposure in (i) woodworking explained 31% of the total variance in inhalable dust exposures (Mikkelsen et al., 2002); (ii) flour production explained 37% of the total variance in inhalable flour dust exposures (Meijster et al., 2007); (iii) the cement industry explained 9–42% of the total variance in thoracic aerosol exposures (Noto et al., 2017); (iv) pig farming explained 35% of the total variance in inhalable dust exposures (Basinas et al., 2013); and (v) greenhouses explained 28–51% of the total variance in dust, endotoxin, fungi, and bacteria exposures (Thilsing et al., 2015). Mixed modeling can be used to successfully identify determinants of exposure across a wide variety of occupational settings, including its use in this study, to identify tasks associated with increased respirable and inhalable indium exposure at an ITO production and reclamation facility.
Sanding tasks, powder transfer tasks in reclaim, powder transfer tasks in refinery, handling indium materials, and liquid transfer tasks in ITO were all associated with increases in respirable indium. Tasks associated with increases in inhalable indium included powder transfer tasks in ITO, handling of indium materials tasks, and cleaning cylinder or tile tasks. Of the jobs identified with the highest TWA exposure to respirable indium and inhalable indium, ITO operators performed many tasks that were associated with increases in exposure to respirable indium, including sanding and liquid transfer tasks in ITO. ITO operators also performed tasks associated with increased exposure to inhalable indium, including powder transfer tasks in ITO and handling indium material tasks. Reclaim operators also had high exposures to respirable and inhalable indium and performed powder transfer tasks in reclaim as well as handling of indium materials tasks that were associated with increased exposure to respirable. Similarly, R&D project technicians also had high exposures to respirable and inhalable indium and performed cleaning cylinder or tile tasks associated with increased exposure to respirable indium, as well as handling indium materials tasks that were associated with increased exposure to respirable indium and inhalable indium. Planar bond technicians as well as ITO grinders in rotary grinding had high measurements for inhalable indium and performed cleaning cylinder or tile tasks.
Our mixed modeling indicated that additional engineering and administrative controls to supplement existing controls are needed to mitigate respirable and inhalable indium exposures during identified tasks. Exposure interventions that target tasks associated with increased respirable or inhalable exposure are especially important in metal-related lung disease such as indium lung disease where indium exposure is associated with a steep concentration–response curve in human studies (Nakano et al., 2009; Cummings et al., 2012, 2016). Additional indium dust control measures during sanding as well as powder transfer tasks in reclaim and ITO could reduce exposures to respirable and inhalable indium observed for two of the highest exposure jobs: ITO and reclaim operators. Additional indium dust control measures during cleaning cylinder or tile tasks could also serve to mitigate the highest exposures measured on R&D project technicians as well as ITO grinders in rotary grinding, respectively. A previous study by Nakano et al. observed that dissemination of health risk information to indium production workers resulted in increased use of dust-protective masks among indium production workers, with a subsequent reduction of measured serum indium and lung interstitial effects (Nakano et al., 2009). Awareness of health risks associated with indium exposure combined with an awareness of high exposure tasks can inform the design of engineering and administrative controls as well as enhance proper training and compliance with PPE use.
A limitation of using mixed modeling to identify and quantify the effects of determinants of exposure is that positive or negative bias can exist due to measurement errors when measuring time at task. Measurement errors in observed duration of tasks can be either positive or negative and can influence estimates of determinants of TWA exposures (Burstyn, 2009). Barrero et al. observed that self-reported time at task can underestimate task duration by −22% and overestimate task duration by 38% (Barrero et al., 2009). To minimize uncertainty in observed duration of task, we did not rely on worker self-reports of time at task; rather, trained NIOSH staff observed workers for the duration of their shift and recorded time spent at task, task location, materials, and use of PPE in task diaries.
Conclusions
Tasks identified as strong predictors of full-shift exposure to respirable and inhalable indium can guide the use of engineering, administrative, and PPE controls designed to mitigate occupational exposure to indium. Moreover, since the tasks were aligned with REACH activities, results from this study can also be used to inform REACH activity scenarios. Finally, a modeling approach can be useful when assessing occupational exposure for which short-duration, task-based sampling may not be feasible due to analytical or cost limitations.
Supplementary Material
Acknowledgements
We would like to thank the following NIOSH staff for their help in data collection and analysis: David Blackley, Randy Boylstein, Matt Duling, Nicole Edwards, Deborah Hirst, Robert B. Lawrence, and Ju-Hyeong Park.
Funding
This work was supported by intramural funding from the National Institute for Occupational Safety and Health.
Footnotes
Disclaimer
The authors declare no conflicts of interest relating to the material presented in this Article. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention. Mention of product names does not imply endorsement by NIOSH/CDC.
Supplementary Data
Supplementary data are available at Annals of Work Exposures and Health online.
References
- ACGIH. (2019) 2019 TLVs(R) and BEIs(R): threshold limit values for chemical substances and physical agents and biological exposure indices. C. Cincinnati, OH: American Conference of Governmental Industrial Hygienists. [Google Scholar]
- Badding MA, Stefaniak AB, Fix NR et al. (2014) Cytotoxicity and characterization of particles collected from an indium-tin oxide production facility. J Toxicol Environ Health A; 77: 1193–209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barrero LH, Katz JN, Perry MJ et al. (2009) Work pattern causes bias in self-reported activity duration: a randomised study of mechanisms and implications for exposure assessment and epidemiology. Occup Environ Med; 66: 38–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Basinas I, Schlünssen V, Takai H et al. (2013) Exposure to inhalable dust and endotoxin among Danish pig farmers affected by work tasks and stable characteristics. Ann Occup Hyg; 57: 1005–19. [DOI] [PubMed] [Google Scholar]
- Burstyn I (2009) Measurement error and model specification in determining how duration of tasks affects level of occupational exposure. Ann Occup Hyg; 53: 265–70. [DOI] [PubMed] [Google Scholar]
- Chen HW. (2007) Exposure and health risk of gallium, indium, and arsenic from semiconductor manufacturing industry workers. Bull Environ Contam Toxicol; 78: 123–7. [DOI] [PubMed] [Google Scholar]
- Cummings KJ, Donat WE, Ettensohn DB et al. (2010) Pulmonary alveolar proteinosis in workers at an indium processing facility. Am J Respir Crit Care Med; 181: 458–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cummings KJ, Nakano M, Omae K et al. (2012) Indium lung disease. Chest; 141: 1512–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cummings KJ, Suarthana E, Edwards N et al. (2013) Serial evaluations at an indium-tin oxide production facility. Am J Ind Med; 56: 300–7. [DOI] [PubMed] [Google Scholar]
- Cummings KJ, Virji MA, Park JY et al. (2016) Respirable indium exposures, plasma indium, and respiratory health among indium-tin oxide (ITO) workers. Am J Ind Med; 59: 522–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldberg M, Levin SM, Doucette JT et al. (1997) A task-based approach to assessing lead exposure among iron workers engaged in bridge rehabilitation. Am J Ind Med; 31: 310–8. [DOI] [PubMed] [Google Scholar]
- Hawley Blackley B, Gibbs JL, Cummings KJ et al. (2019) A field evaluation of a single sampler for respirable and inhalable indium and dust measurements at an indium-tin oxide manufacturing facility. J Occup Environ Hyg; 16: 66–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hines CJ, Roberts JL, Andrews RN et al. (2013) Use of and occupational exposure to indium in the United States. J Occup Environ Hyg; 10: 723–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hoet P, De Graef E, Swennen B et al. (2012) Occupational exposure to indium: what does biomonitoring tell us? Toxicol Lett; 213: 122–8. [DOI] [PubMed] [Google Scholar]
- Medvedovski E, Alvarez N, Yankov O, et al. (2008) Advanced indium-tin oxide ceramics for sputtering targets. Ceram Int; 34: 1173–82. [Google Scholar]
- Meijster T, Tielemans E, de Pater N et al. (2007) Modelling exposure in flour processing sectors in the Netherlands: a baseline measurement in the context of an intervention program. Ann Occup Hyg; 51: 293–304. [DOI] [PubMed] [Google Scholar]
- Mikkelsen AB, Schlunssen V, Sigsgaard T et al. (2002) Determinants of wood dust exposure in the Danish furniture industry. Ann Occup Hyg; 46: 673–85. [DOI] [PubMed] [Google Scholar]
- Miyauchi H, Minozoe A, Tanaka S et al. (2012) Assessment of workplace air concentrations of indium dust in an indium-recycling plant. J Occup Health; 54: 103–11. [DOI] [PubMed] [Google Scholar]
- Nakano M, Omae K, Tanaka A et al. (2009) Causal relationship between indium compound inhalation and effects on the lungs. J Occup Health; 51: 513–21. [DOI] [PubMed] [Google Scholar]
- NIOSH. (2012). HETA No. 2009–0214-3153. Health Hazard Evaluation Report: an evaluation of preventive measures at an indium-tin oxide production facility, Rhode Island. Morgantown, WV: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health. [Google Scholar]
- NIOSH. (2015) Hierarchy of controls. National Institute for Occupational Safety and Health. Morgantown, WV: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health. Available at https://www.cdc.gov/niosh/topics/hierarchy/default.html [Google Scholar]
- Notø H, Nordby KC, Skare Ø et al. (2017) Job tasks as determinants of thoracic aerosol exposure in the cement production industry. Ann Work Expo Health; 62: 88–100. [DOI] [PubMed] [Google Scholar]
- Omae K, Nakano M, Tanaka A et al. (2011) Indium lung—case reports and epidemiology. Int Arch Occup Environ Health; 84: 471–7. [DOI] [PubMed] [Google Scholar]
- Rappaport S, Kupper L. (2008) Quantitative exposure assessment. El Cerrito, CA, U.S.A.: Stephen M. Rappaport. [Google Scholar]
- Seixas NS, Sheppard L, Neitzel R. (2003) Comparison of task-based estimates with full-shift measurements of noise exposure. AIHA J (Fairfax, VA); 64: 823–9. [DOI] [PubMed] [Google Scholar]
- Thilsing T, Madsen AM, Basinas I et al. (2015) Dust, endotoxin, fungi, and bacteria exposure as determined by work task, season, and type of plant in a flower greenhouse. Ann Occup Hyg; 59: 142–57. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.