

SWITCH-1 was a phase 2b study assessing the efficacy, safety, and dose-response relationship of elinzanetant, a selective neurokinin-1,3 receptor antagonist, for the treatment of vasomotor symptoms. Elinzanetant resulted in significant and clinically meaningful improvements in vasomotor symptoms, sleep and quality of life and was well tolerated across all doses.
Key Words: KNDy neuron; Menopause; Neurokinin B; Neurokinin-1,3 receptor antagonist; Substance P; Vasomotor symptoms
Abstract
Objective
Neurokinin (NK)-3 and NK-1 receptors have been implicated in the etiology of vasomotor symptoms (VMS) and sleep disturbances associated with menopause. This phase 2b, adaptive, dose-range finding study aimed to assess the efficacy and safety of multiple doses of elinzanetant (NT-814), a selective NK-1,3 receptor antagonist, in women experiencing VMS associated with menopause, and investigate the impact of elinzanetant on sleep and quality of life.
Methods
Postmenopausal women aged 40 to 65 years who experienced seven or more moderate-to-severe VMS per day were randomized to receive elinzanetant 40, 80, 120, or 160 mg or placebo once daily using an adaptive design algorithm. Coprimary endpoints were reduction in mean frequency and severity of moderate-to-severe VMS at weeks 4 and 12. Secondary endpoints included patient-reported assessments of sleep and quality of life.
Results
Elinzanetant 120 mg and 160 mg achieved reductions in VMS frequency versus placebo from week 1 throughout 12 weeks of treatment. Least square mean reductions were statistically significant versus placebo at both primary endpoint time points for elinzanetant 120 mg (week 4: −3.93 [SE, 1.02], P < 0.001; week 12: −2.95 [1.15], P = 0.01) and at week 4 for elinzanetant 160 mg (−2.63 [1.03]; P = 0.01). Both doses also led to clinically meaningful improvements in measures of sleep and quality of life. All doses of elinzanetant were well tolerated.
Conclusions
Elinzanetant is an effective and well-tolerated nonhormone treatment option for postmenopausal women with VMS and associated sleep disturbance. Elinzanetant also improves quality of life in women with VMS.
Vasomotor symptoms (VMS) and sleep disturbances are some of the most frequent and bothersome symptoms associated with menopause.1-4 VMS are experienced by up to 80% of women during the menopausal transition, lasting on average 7 to 10 years after the last menstrual period,5-7 with a third of women reporting very frequent or severe symptoms.8,9 Around 40% to 60% of women experience sleep disturbances during the menopausal transition.
Hormone therapy is currently the most effective treatment option approved for the management of VMS.10 However, many women are not candidates for hormone therapy because of medical contraindications or choose not to use it because of personal preferences.11-13 There is therefore an unmet need for safe and effective nonhormone options to treat VMS associated with menopause.
Evolving evidence supports a central role of hypothalamic, estrogen-sensitive kisspeptin, neurokinin (NK)-B, and dynorphin (KNDy) neurons in thermoregulation and the etiology of VMS.14-19 KNDy neurons express substance P and NK-B (NK-1 receptor [NK-1R] and NK-3R endogenous ligands, respectively), which may be involved in the modulation of VMS related to menopause.14,20-23 Substance P and NK-1R may also modulate sleep effects related to menopause and contribute to peripheral vasodilatation.24-27 Therefore, targeting NK-1R/substance P and NK-3R/NKB signaling may offer a nonhormone way to treat directly the cause of VMS and sleep disturbances associated with menopause.
Elinzanetant (NT-814) is a novel, selective NK-1,3R antagonist in development for the treatment of moderate-to-severe VMS associated with menopause. It is the first dual antagonist targeting both NK-1 and NK-3 receptors. NK-1R–specific antagonism has previously shown efficacy in primary insomnia and mood disorders not related to menopause.28-32 However, the mechanism behind sleep disturbances associated with menopause is not fully understood, and there are no data on the impact of NK-1R antagonism on sleep disorders associated with menopause. Elinzanetant has previously been evaluated in a phase 2a randomized, placebo-controlled, multiple ascending dose trial (RELENT-1), where it demonstrated rapid and marked reductions in the frequency and severity of VMS.23 The objectives of this phase 2b trial (SWITCH-1) were to assess further the efficacy and safety of elinzanetant in women experiencing bothersome VMS, evaluate dose-response, and, secondarily, to investigate the impact of elinzanetant on sleep disturbances and quality of life associated with menopause.
METHODS
Study design
SWITCH-1 was a multicenter, multicountry, double-blind, placebo-controlled, dose-range finding study with an adaptive randomization design evaluating elinzanetant in postmenopausal women aged 40 to 65 years. Menopause was defined as either (1) at least 12 months of spontaneous amenorrhea, (2) at least 6 months of spontaneous amenorrhea with serum follicle-stimulating hormone levels of more than 40 mIU/mL and serum estradiol less than 30 pg/mL, or (3) at least 6 weeks of postsurgical bilateral oophorectomy with or without hysterectomy. The study protocol and statistical analysis plan are available in Supplemental Digital Content (Supplemental Data 1, http://links.lww.com/MENO/B68).
Institutional review board and ethics committee approval was obtained for all study sites, and all participants provided written informed consent. A 3-week initial screening period was used to assess eligibility. This 3-week period included a single-blind placebo run-in in the last 2 weeks in which participants received placebo once daily. To be eligible for the study, participants needed to meet the inclusion criteria (Supplemental Table 1, http://links.lww.com/MENO/B69), including recording on average at least seven moderate or severe VMS per day (see definition hereinafter) over the past 7 days of the screening period.
Eligible participants were initially randomized 1:1:1:1:1 and stratified by region (North America [United States and Canada] versus United Kingdom) to receive either once-daily elinzanetant (40, 80, 120, or 160 mg, soft gel capsules) or matching placebo for 12 weeks followed by a 4-week off-treatment follow-up (Supplemental Fig. 1, http://links.lww.com/MENO/B69). Participants were to take their assigned treatment orally at the same time each day.
The trial used an adaptive design algorithm based on Bayesian Emax dose-response modeling33 and T statistic adaptive dose-finding design,34 which provided dose assignment recommendations. An unblinded data review committee reviewed these recommendations, the model outputs for VMS frequency and severity, and emerging safety data and determined changes to the randomization ratio, if appropriate, to optimize sample size to improve the probability of finding effective doses.
Data collection
Participants recorded the frequency and severity of VMS and the number of nighttime awakenings secondary to VMS twice daily in electronic diaries (eDiaries). Severity was scored on a scale of 0 to 3, with 0 representing none; 1, mild (sensation of heat without sweating); 2, moderate (sensation of heat with sweating but able to continue activity); and 3, severe (sensation of heat with sweating, causing cessation of activity). Any VMS causing a nighttime awakening by definition was considered severe.
The Insomnia Severity Index (ISI) questionnaire and Pittsburgh Sleep Quality Index (PSQI) were used to assess participants' sleep, whereas the Menopause-specific Quality-of-Life questionnaire intervention version (MenQoL-I) assessed quality of life (Supplemental Table 2, http://links.lww.com/MENO/B69). A decrease in score in each instrument corresponds to an improvement in symptoms. Participants completed the questionnaires during clinic visits at baseline and weeks 4, 8, 12, and 16.
Safety was assessed through adverse event monitoring. Other routine assessments included medical history, physical examinations, 12-lead electrocardiograms, suicide severity rating, clinical laboratory assessments, vital signs, and bone turnover markers. For changes in liver enzymes, only increases three or more times the upper limit of normal (ULN) were considered relevant, as per US Food and Drug Administration guidance.35
Endpoints
The coprimary efficacy endpoints were mean change in the frequency and severity of moderate-to-severe VMS compared with placebo from baseline to weeks 4 and 12. Secondary endpoints included the mean change from baseline compared with placebo of moderate-to-severe VMS frequency and severity at weeks 1, 2, 8, and 16; number of nighttime awakenings secondary to VMS at weeks 1, 2, 4, 8, 12, and 16; and ISI, PSQI, and MenQoL-I scores at weeks 4, 8, 12, and 16.
Statistical analysis
Assuming a common standard deviation of 4.4, n = 27 per treatment group would give approximately 95% power via trend test across all doses including placebo if the true underlying dose-response was nondecreasing from a reduction of four VMS on placebo up to eight on the highest dose of elinzanetant. Thus, the initial sample size was planned to be 33 participants per treatment group (165 in total) to allow for participants dropping out.
Descriptive statistical analyses were performed on all endpoint time points using Statistical Analysis System, version 9.4. Formal statistical hypothesis testing was performed at the two-sided, 0.05 level of significance for VMS frequency, severity, and nighttime awakenings secondary to VMS at all time points up to week 12 and ISI, PSQI, and MenQoL-I scores at weeks 4 and 12. Efficacy analyses were performed on the full analysis set, which included all randomized participants who received at least one dose of the study drug and had VMS data for at least 7 days of posttreatment assessments. Endpoints were analyzed using a mixed-effect model repeated measures approach incorporating postrandomization data up to week 12. Pairwise statistical comparisons were performed for each elinzanetant dose group versus placebo and least square (LS) means, SE, and 95% CI for the treatment difference were reported. Safety endpoints were summarized in all participants who received at least one dose of study drug.
RESULTS
SWITCH-1 was conducted at 25 sites across the United States, United Kingdom, and Canada. In total, 760 participants were screened, 199 were randomized, and 180 completed treatment (Fig. 1). Based on emerging efficacy data, the data review committee chose to discontinue randomization to the 80 mg and 40 mg doses after 17 and 31 participants were enrolled in these groups, respectively. All randomized participants were included in both the full analysis set and safety analysis set. Baseline demographics, VMS, sleep, quality of life, and menopause characteristics were well balanced between treatment groups and indicated a high symptom burden (Table 1; Supplemental Tables 3 and 6-9, http://links.lww.com/MENO/B69).
FIG. 1.
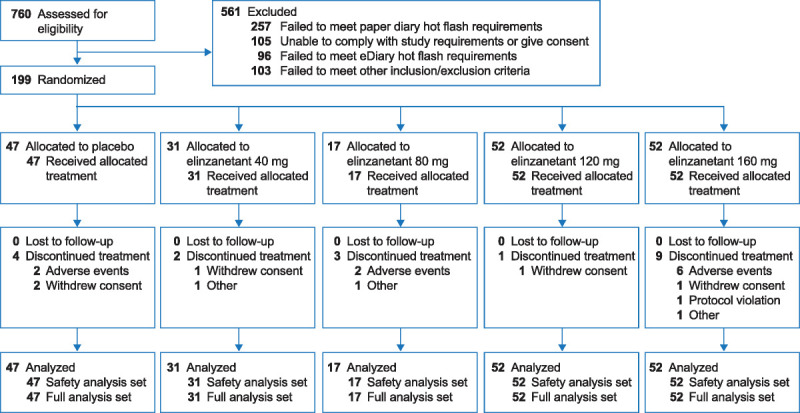
Disposition of study participants.
Table 1.
Baseline demographics and characteristics
| Parameter/category | Elinzanetant group | |||||
|---|---|---|---|---|---|---|
| Placebo group (N = 47) | 40 mg (n = 31) | 80 mg (n = 17) | 120 mg (n = 52) | 160 mg (n = 52) | Total elinzanetant (N = 152) | |
| Demographics (safety analysis set) | ||||||
| Age, mean (SD) (y) | 55.6 (4.1) | 55.4 (4.0) | 55.9 (4.2) | 54.8 (4.4) | 55.0 (3.8) | 55.1 (4.1) |
| Race, n (%) | ||||||
| Asian | 2 (4) | 0 | 0 | 1 (2) | 1 (2) | 2 (1.3) |
| Black or African American | 6 (13) | 5 (16) | 3 (18) | 13 (25) | 11 (21) | 32 (21.1) |
| White | 38 (81) | 24 (77) | 13 (77) | 37 (71) | 40 (77) | 114 (75.0) |
| Othera | 1 (2) | 2 (7) | 1 (6) | 1 (2) | 0 | 4 (2.6) |
| BMI, mean (SD) (kg/m2) | 28.56 (3.83) | 27.72 (4.88) | 29.56 (5.02) | 27.24 (4.64) | 27.72 (4.87) | 27.76 (4.81) |
| Moderate and severe VMS characteristics (full analysis set), mean (SD) | ||||||
| Frequency, daily | 11.82 (4.42) | 12.13 (8.81) | 14.55 (5.87) | 13.54 (7.17) | 12.92 (6.90) | 13.16 (7.28) |
| Severity, weekly | 2.54 (0.20) | 2.51 (0.26) | 2.63 (0.24) | 2.54 (0.24) | 2.54 (0.26) | 2.55 (0.25) |
BMI, body mass index; VMS, vasomotor symptoms.
aNo additional detail was collected for participants in this category.
Vasomotor symptoms
Compared with placebo, there were statistically significant and clinically relevant reductions (improvements) in the mean daily frequency of moderate-to-severe VMS with elinzanetant 120 mg at week 4 (difference in LS means [SE], −3.93 [1.02]; P < 0.001) and week 12 (−2.95 [1.15]; P = 0.01) (Fig. 2). The improvements with elinzanetant 160 mg were significant at week 4 (−2.63 [1.03]; P = 0.01) but not week 12 (−1.78 [1.19]; P = 0.13). Improvements with elinzanetant 40 mg and 80 mg were observed but not statistically significant compared with placebo at either of the primary endpoint time points.
FIG. 2.
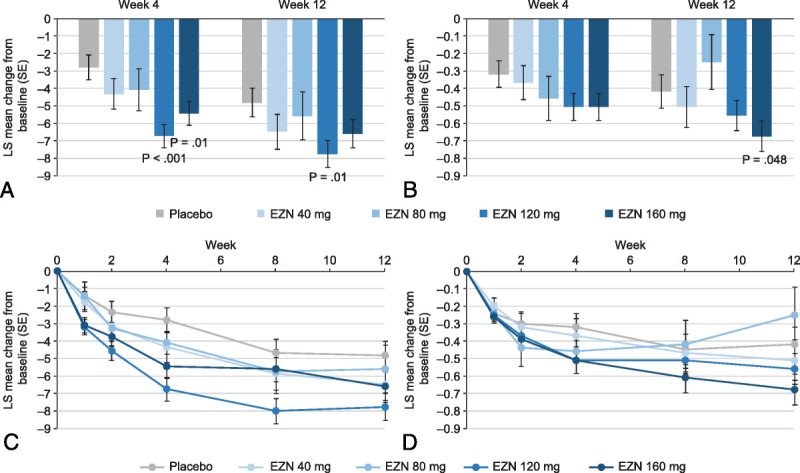
Change from baseline in mean daily frequency (A, C) and weekly severity (B, D) of moderate and severe VMS by treatment group. EZN, elinzanetant; LS, least square; VMS, vasomotor symptoms.
Statistically significant improvements compared with placebo in the mean daily frequency of moderate-to-severe VMS were achieved by week 1 for both elinzanetant 120 mg (difference in LS means [SE], −1.80 [0.67]; P = 0.008) and 160 mg (−1.69 [0.67]; P = 0.01) (Fig. 2). Improvements tended to increase throughout treatment and returned toward baseline 4 weeks after treatment discontinuation (Supplemental Table 4, http://links.lww.com/MENO/B69).
Reductions in mean weekly severity of moderate-to-severe VMS followed a similar trend; however, reductions were only significant compared with placebo for elinzanetant 160 mg at week 12 (0.27 [0.13]; P = 0.048) (Fig. 2; Supplemental Table 5, http://links.lww.com/MENO/B69).
Sleep and quality of life
Reductions (improvements) in the frequency of nighttime awakenings secondary to VMS were significantly larger compared with placebo for elinzanetant 120 mg at weeks 1, 2, 4, and 8 (P = 0.006 to P = 0.049) but not at week 12 (Supplemental Table 6, http://links.lww.com/MENO/B69). Improvements were not significant compared with placebo for other doses.
Compared with placebo, there were statistically significant improvements in ISI score at weeks 4 and 12 for elinzanetant 120 mg (differences in LS means [SE], −3.41 [0.92]; P < 0.001 and −4.27 [1.01]; P < 0.001, respectively) and 160 mg (−3.28 [0.95]; P < 0.001 and −4.85 [1.05]; P < 0.001, respectively) (Fig. 3A). Clinically meaningful improvements of at least a 6-point reduction were achieved at weeks 8 and 12 for elinzanetant 120 mg and week 12 for elinzanetant 160 mg (Supplemental Table 7, http://links.lww.com/MENO/B69).36 Improvements in ISI score were not significant compared with placebo for lower doses except for at week 12 for elinzanetant 80 mg (P = 0.008).
FIG. 3.
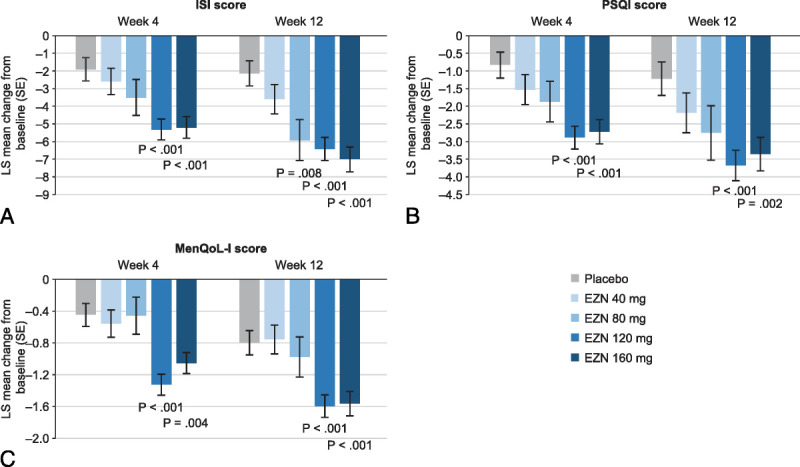
Change from baseline in ISI (A), PSQI (B), and MenQoL-I (C) score by treatment group at weeks 4 and 12. EZN, elinzanetant; ISI, Insomnia Severity Index questionnaire; LS, least square; MenQoL-I, Menopause-specific Quality-of-Life questionnaire intervention version; PSQI, Pittsburgh Sleep Quality Index.
Compared with placebo, there were statistically significant improvements in PSQI total score at weeks 4 and 12 for elinzanetant 120 mg (difference in LS means [SE], −2.05 [0.51]; P < 0.001 and −2.46 [0.67]; P < 0.001, respectively) and 160 mg (−1.90 [0.52]; P < 0.001 and −2.14 [0.69]; P = 0.002, respectively) (Fig. 3B; Supplemental Table 7, http://links.lww.com/MENO/B69). Improvements in PSQI score were not significant compared with placebo for lower doses at any time points.
Improvements in overall MenQoL-I score were statistically significant compared with placebo at weeks 4 and 12 for elinzanetant 120 mg (difference in LS means [SE], −0.87 [0.20]; P < 0.001 and −0.80 [0.22]; P < 0.001, respectively) and 160 mg (−0.61 [0.21]; P = 0.004 and −0.77 [0.23]; P < 0.001, respectively) (Fig. 3C). Clinically meaningful improvements of at least a 1-point reduction were seen for elinzanetant 120 mg and 160 mg at weeks 4, 8, 12 and 16 (Supplemental Table 9, http://links.lww.com/MENO/B69).37 Significant improvements compared with placebo were not seen for lower doses.
Improvements in sleep and quality of life returned toward baseline 4 weeks after treatment discontinuation (Supplemental Tables 6-9, http://links.lww.com/MENO/B69).
Safety
Overall, 235 treatment-emergent adverse events (TEAEs) were reported in 67.8% (103 of 152) of participants in the elinzanetant groups, and 80 TEAEs were reported in 60% (28 of 47) of participants in the placebo group (Table 2). Most TEAEs were mild or moderate. The most frequently reported TEAEs across all treatment groups were headache, somnolence, and diarrhea. Seven of 152 elinzanetant-treated participants (4.6%) (2 of 17 [12%] for elinzanetant 40 mg and 5 of 52 [10%] for elinzanetant 160 mg) and 1 of 47 (2%) placebo-treated participants discontinued treatment because of adverse events; there were no discontinuations in the 120-mg dose group. Reasons for treatment discontinuation were prolonged QT and bradycardia; increased liver function test; headache; somnolence, abdominal distension, and dyspepsia; fatigue; depression and anxiety; and erythema multiforme in the elinzanetant groups and headache in the placebo group. The apparent prolonged QT leading to withdrawal of a participant was found to be erroneous (QTc was within normal limits) on expert review. There was no obvious relationship between elinzanetant dose and the number of TEAEs. Somnolence was reported more frequently in the 160-mg dose and 40-mg dose groups compared with other doses, at a similar incidence in each group. Dizziness was only reported at higher doses of elinzanetant (120 and 160 mg); however, all incidences of dizziness were considered unrelated to treatment by the investigators.
Table 2.
Treatment-emergent adverse events by treatment group
| AE category (preferred term)a | Elinzanetant group, n (%) | |||||
|---|---|---|---|---|---|---|
| Placebo group, n (%) (N = 47) | 40 mg (n = 31) | 80 mg (n = 17) | 120 mg (n = 52) | 160 mg (n = 52) | Total (N = 152) | |
| Any TEAEs | 28 (60) | 17 (55) | 14 (82) | 34 (65) | 38 (73) | 103 (67.8) |
| Serious TEAEs | 2 (4) | 0 | 1 (6) | 1 (2) | 1 (2) | 3 (2) |
| TEAEs leading to discontinuation of study treatment | 1 (2) | 0 | 2 (12) | 0 | 5 (10) | 7 (4.6) |
| Most common TEAEs (occurring in ≥3 participants in any treatment group) | ||||||
| Headache | 6 (13) | 3 (10) | 2 (12) | 6 (12) | 4 (8) | 15 (9.9) |
| Somnolence | 1 (2) | 3 (10) | 1 (6) | 2 (4) | 6 (12) | 12 (7.9) |
| Dizziness | 0 | 0 | 0 | 3 (6) | 3 (6) | 6 (3.9) |
| Nasopharyngitis | 4 (9) | 1 (3) | 0 | 3 (6) | 0 | 4 (2.6) |
| Diarrhea | 3 (6) | 2 (6) | 2 (12) | 3 (6) | 3 (6) | 10 (6.6) |
| Blood creatine phosphatase increased | 1 (2) | 1 (3) | 1 (6) | 3 (6) | 1 (2) | 6 (3.9) |
| Fatigue | 0 | 3 (10) | 1 (6) | 1 (2) | 4 (8) | 9 (5.9) |
AE, adverse event; TEAEs, treatment-emergent adverse events.
aCoded using MedDRA version 21.1.
There were sporadic increases in transaminases during treatment of no more than three times the ULN, but these were of equal frequency and magnitude in placebo- and elinzanetant-treated participants (11% and 8.8%, respectively) and were not considered clinically relevant. Two participants randomized to elinzanetant (both 80 mg) showed increases in transaminases three or more times the ULN; however, these participants had no detectable elinzanetant in plasma samples drawn at the same time as the enzyme increases and were considered to be noncompliant with study medication. In one of the two, there was also a marked increase in creatine kinase, suggesting that the transaminase increase in this participant was likely to have been of muscle origin. There was no evidence of drug-related liver toxicity. No safety concerns were seen in any other routine safety assessments.
DISCUSSION
SWITCH-1 is the first phase 2b study to demonstrate significant improvements in menopause-related symptoms, such as VMS and sleep disturbance, and improved quality of life with a selective NK-1,3R antagonist in postmenopausal women. Although improvements were observed in placebo-treated participants, consistent with other studies of VMS treatments,38-41 greater improvements were seen across elinzanetant doses over the treatment period. In particular, improvements with elinzanetant 120 mg and 160 mg were statistically significant compared with placebo for VMS frequency (except for elinzanetant 160 mg at week 12), ISI score, PSQI score, and MenQoL-I score. Reductions in VMS frequency compared with placebo at the 120-mg dose were similar to those seen with hormone therapy and NK-3R antagonists and met the threshold for clinical relevance of a reduction of two or more per day beyond that achieved by placebo.38-42
The findings of this study further support the potential of NK signaling for the rapid treatment of VMS. Elinzanetant 120 mg and 160 mg led to meaningful reductions in VMS frequency after only 1 week of treatment. This is consistent with results from RELENT-1, in which similarly rapid reductions in VMS frequency were shown with a 150-mg dose of elinzanetant, and studies of NK-3R antagonists that demonstrate maximum efficacy within weeks.38,39,43 The effect on VMS seen with elinzanetant may be mediated by suppression of KNDy neuron hyperactivation and an effect on peripheral vasodilatation through NK-1R antagonism in peripheral blood vessels.
In some of our analyses, elinzanetant 120 mg seems to have a greater benefit than elinzanetant 160 mg, particularly for VMS frequency. However, findings for elinzanetant 160 mg were skewed by a single participant in this group whose VMS frequency increased by more than 200% from baseline at times during the study. In a prespecified nonparametric analysis (data not shown) and an exploratory analysis excluding high outliers (ie, the one participant in the 160-mg group), reductions in mean VMS frequency were similar to that of the 120-mg dose and statistically significant compared with placebo.
Although VMS severity showed marked reductions across the higher elinzanetant doses, reductions were only significant compared with placebo at week 12 for elinzanetant 160 mg. Despite VMS severity being used to assess efficacy of VMS treatments by some regulatory authorities, it is recognized as a problematic endpoint because average severity takes no account of the number of VMS episodes overall.44
VMS that occur at night can be particularly distressing for women and disrupt sleep. This study did not require sleep disturbance for eligibility and participants recorded a low baseline number of nighttime awakenings. Reductions in nighttime awakenings secondary to VMS therefore were small and generally did not reach statistical significance. However, many women with little VMS interference report experiencing sleep disturbance during the menopause.45 In this study, despite a low number of self-reported awakenings due to VMS, at baseline, participants reported a high degree of sleep disturbance with average ISI scores indicative of moderate insomnia (8-14) and PSQI scores in the range associated with fatigue (>8).46 After treatment with elinzanetant 120 mg and 160 mg, mean ISI scores fell to the subthreshold insomnia range (5-7) and PSQI scores fell below the level associated with fatigue. The present results support that antagonism of both NK-1R and NK-3R confers a benefit on sleep disturbance associated with menopause, and a reduction in sleep disturbance because of fewer awakenings secondary to VMS.
In a recent survey, sleep disturbances were rated as more bothersome than VMS as measured by the MenQoL questionnaire and had a greater impact on work productivity and day-to-day activities.1 Treatment with elinzanetant 120 mg and 160 mg in this study resulted in statistically significant and clinically meaningful improvements in overall MenQoL-I scores, indicating improved menopause-specific quality of life.37 These improvements in quality of life may have arisen because of participants experiencing fewer VMS and sleeping better or from the combination of these effects contributing to a greater sense of well-being, although it is not possible to determine the exact cause from our study.
Elinzanetant was well tolerated with no TEAEs of concern at any doses tested. There were no clear differences in the incidences of TEAEs between the treatment groups, although a slightly higher incidence of somnolence was reported for elinzanetant 160 mg (Table 2). Owing to previous reports of increases in liver enzymes with some single-mechanism NK-3R antagonists,38,39 liver enzymes were monitored closely in SWITCH-1. There were significant transaminase increases in two elinzanetant-treated participants, but elinzanetant was undetectable in the plasma of these participants, suggesting that both were noncompliant with study medication.
The strengths of the study include its randomized, placebo-controlled adaptive design and the standardization of procedures across all study sites. The 2-week single-blind placebo run-in before the 12-week treatment period allowed 1 week for participants to familiarize themselves with the eDiaries and 1 week of baseline efficacy assessments. The inclusion of the placebo run-in, which has been used in similar studies previously, allowed for recording of baseline assessments under similar conditions to the treatment period and may provide the additional benefit of screening out participants with a high placebo response who would not have benefitted further from treatment.47 eDiaries included time lockouts to ensure that only contemporaneous data could be entered, improving the robustness of data. A key limitation is the high entry criteria for VMS frequency and severity; these criteria are used to support regulatory approval of VMS treatments but represent a barrier to study participation, resulting in many participants being ineligible at screening. Accordingly, the efficacy in patients with a lower VMS burden could not be investigated in this study. In addition, the use of an adaptive randomization schema aimed to improve the efficiency of the trial by reducing allocation to doses that appeared suboptimal. This resulted in smaller treatment groups for elinzanetant 40 mg and 80 mg, and consequently, the statistical analyses of these two doses have less power than the two higher dose groups. However, the reduced power at lower doses was offset by increased power for the effective doses. Finally, there were no minimum eligibility criteria for nighttime awakenings secondary to VMS, and the average baseline frequency of these awakenings was low. Absolute reductions over the treatment period were small, and the study was not sufficiently powered to show statistical significance with these small differences.
CONCLUSIONS
Taken together, findings from our study suggest that, relative to other elinzanetant doses tested, the 120-mg dose offers clinically important efficacy across a range of menopause-related symptoms with the most favorable benefit/risk profile. Elinzanetant demonstrated a generally dose-ordered response across all efficacy outcomes with no additional benefit observed with the 160-mg dose, suggesting a plateau of effect at 120 mg. The efficacy and safety of elinzanetant 120 mg will be further evaluated in a phase 3 program (NCT05042362, NCT05099159, NCT05030584).
Acknowledgments: The study was sponsored by NeRRe Therapeutics. Medical writing support was provided by Highfield with sponsorship from Bayer.
Data sharing statement: see Supplemental Digital Content, Supplemental Data 2, http://links.lww.com/MENO/B70.
Supplementary Material
Footnotes
E.B. was employed at NeRRe Therapeutics, Stevenage, United Kingdom at the time the research was done.
This study was presented at The North American Menopause Society 2020 Meeting, Denver, CO, on September 30 to October 3 and the 13th European Congress on Menopause and Andropause, virtual meeting, September 8-10, 2021.
Funding/support: The study was sponsored by NeRRe Therapeutics.
Clinical Trial Registration: ClinicalTrials.gov identifier, NCT03596762 (https://clinicaltrials.gov/ct2/show/NCT03596762).
Financial disclosure/conflicts of interest: C.C. and L.Z. are employees of Bayer CC AG. C.S. is an employee of Bayer AG. M.K., S.P., E.B., S.S., and M.T. are employees of NeRRe Therapeutics. J.B., as an employee of Cytel Inc, was a paid statistical consultant on this trial. R.A.A. has undertaken consultancy work for NeRRe Therapeutics and Sojournix Inc. J.A.S. has grant/research support from AbbVie, Inc, Bayer Healthcare LLC, Daré Bioscience, Ipsen, Mylan/Viatris Inc, Myovant Sciences, ObsEva SA, Sebela Pharmaceuticals Inc, and Viveve Medical; has been a consultant/advisory boards of Bayer HealthCare Pharmaceuticals Inc, Besins Healthcare, California Institute of Integral Studies, Camargo Pharmaceutical Services, LLC, Covance Inc, Daré Bioscience, DEKA M.E.L.A. S.r.l., Femasys Inc, KaNDy/NeRRe Therapeutics Ltd, Khyria, Madorra Pty Ltd, Mitsubishi Tanabe Pharma Development America, Inc, QUE Oncology Pty, Limited, Scynexis Inc, Sebela Pharmaceuticals, Inc, Sprout Pharmaceuticals, Inc, and Vella Bioscience Inc; has served on the Speaker's bureaus of Mayne Pharma, Inc, Myovant Sciences, Inc, Pfizer Inc, Pharmavite LLC, Scynexis Inc, and TherapeuticsMD; and is a stockholder (direct purchase) in Sermonix Pharmaceuticals. N.P. has undertaken consultancy and speaker's bureau work for a number of pharmaceutical companies including Bayer AG. H.J. has received grant funding from National Institutes of Health, Merck, Pfizer, and Hello Therapeutics; has undertaken consultancy work for Bayer, Jazz, and Eisai; and her spouse is an employee at Arsenal Biosciences and has equity at Merck.
Supplemental digital content is available for this article. Direct URL citations are provided in the HTML and PDF versions of this article on the journal’s Website (www.menopause.org).
Contributor Information
Richard A. Anderson, Email: Richard.Anderson@ed.ac.uk.
Elizabeth Ballantyne, Email: lizmason@ymail.com.
James Bolognese, Email: Bolognese@cytel.com.
Cecilia Caetano, Email: cecilia.caetano@bayer.com.
Hadine Joffe, Email: joffe.hadine@gmail.com.
Mary Kerr, Email: mary.kerr@nerretherapeutics.com.
Nick Panay, Email: nickpanay@msn.com.
Christian Seitz, Email: christian.seitz@bayer.com.
Susan Seymore, Email: susan.seymore@nerretherapeutics.com.
Mike Trower, Email: mike.trower@nerretherapeutics.com.
Lineke Zuurman, Email: lineke.zuurman@bayer.com.
Steve Pawsey, Email: steve.pawsey@nerretherapeutics.com.
REFERENCES
- 1.Nappi RE Kroll R Siddiqui E, et al. Global cross-sectional survey of women with vasomotor symptoms associated with menopause: prevalence and quality of life burden. Menopause 2021;28:875–882. doi: 10.1097/GME.0000000000001793 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Thurston RC. Vasomotor symptoms: natural history, physiology, and links with cardiovascular health. Climacteric 2018;21:96–100. doi: 10.1080/13697137.2018.1430131 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Thurston RC, Chang Y, Buysse DJ, Hall MH, Matthews KA. Hot flashes and awakenings among midlife women. Sleep 2019;42:zsz131. doi: 10.1093/sleep/zsz131 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Thurston RC, Joffe H. Vasomotor symptoms and menopause: findings from the Study of Women's Health across the Nation. Obstet Gynecol Clin North Am 2011;38:489–501. doi: 10.1016/j.ogc.2011.05.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Avis NE Crawford SL Greendale G, et al. Duration of menopausal vasomotor symptoms over the menopause transition. JAMA Intern Med 2015;175:531–539. doi: 10.1001/jamainternmed.2014.8063 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Freeman EW, Sammel MD, Lin H, Liu Z, Gracia CR. Duration of menopausal hot flushes and associated risk factors. Obstet Gynecol 2011;117:1095–1104. doi: 10.1097/AOG.0b013e318214f0de [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Freeman EW, Sammel MD, Sanders RJ. Risk of long-term hot flashes after natural menopause: evidence from the Penn Ovarian Aging Study cohort. Menopause 2014;21:924–932. doi: 10.1097/GME.0000000000000196 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gold EB Colvin A Avis N, et al. Longitudinal analysis of the association between vasomotor symptoms and race/ethnicity across the menopausal transition: study of women's health across the nation. Am J Public Health 2006;96:1226–1235. doi: 10.2105/AJPH.2005.066936 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Williams RE Kalilani L DiBenedetti DB, et al. Frequency and severity of vasomotor symptoms among peri- and postmenopausal women in the United States. Climacteric 2008;11:32–43. doi: 10.1080/13697130701744696 [DOI] [PubMed] [Google Scholar]
- 10.de Villiers TJ Gass ML Haines CJ, et al. Global consensus statement on menopausal hormone therapy. Climacteric 2013;16:203–204. doi: 10.3109/13697137.2013.771520 [DOI] [PubMed] [Google Scholar]
- 11.Biglia N, Bounous VE, De Seta F, Lello S, Nappi RE, Paoletti AM. Non-hormonal strategies for managing menopausal symptoms in cancer survivors: an update. Ecancermedicalscience 2019;13:909. doi: 10.3332/ecancer.2019.909 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Constantine GD Graham S Clerinx C, et al. Behaviours and attitudes influencing treatment decisions for menopausal symptoms in five European countries. Post Reprod Health 2016;22:112–122. doi: 10.1177/2053369116632439 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Neves-E-Castro M Birkhauser M Samsioe G, et al. EMAS position statement: the ten point guide to the integral management of menopausal health. Maturitas 2015;81:88–92. doi: 10.1016/j.maturitas.2015.02.003 [DOI] [PubMed] [Google Scholar]
- 14.Rance NE, Dacks PA, Mittelman-Smith MA, Romanovsky AA, Krajewski-Hall SJ. Modulation of body temperature and LH secretion by hypothalamic KNDy (kisspeptin, neurokinin B and dynorphin) neurons: a novel hypothesis on the mechanism of hot flushes. Front Neuroendocrinol 2013;34:211–227. doi: 10.1016/j.yfrne.2013.07.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lehman MN, Coolen LM, Goodman RL. Minireview: kisspeptin/neurokinin B/dynorphin (KNDy) cells of the arcuate nucleus: a central node in the control of gonadotropin-releasing hormone secretion. Endocrinology 2010;151:3479–3489. doi: 10.1210/en.2010-0022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Rance NE, McMullen NT, Smialek JE, Price DL, Young WS, 3rd. Postmenopausal hypertrophy of neurons expressing the estrogen receptor gene in the human hypothalamus. J Clin Endocrinol Metab 1990;71:79–85. doi: 10.1210/jcem-71-1-79 [DOI] [PubMed] [Google Scholar]
- 17.Rance NE, Young WS, 3rd. Hypertrophy and increased gene expression of neurons containing neurokinin-B and substance-P messenger ribonucleic acids in the hypothalami of postmenopausal women. Endocrinology 1991;128:2239–2247. doi: 10.1210/endo-128-5-2239 [DOI] [PubMed] [Google Scholar]
- 18.Rometo AM, Krajewski SJ, Voytko ML, Rance NE. Hypertrophy and increased kisspeptin gene expression in the hypothalamic infundibular nucleus of postmenopausal women and ovariectomized monkeys. J Clin Endocrinol Metab 2007;92:2744–2750. doi: 10.1210/jc.2007-0553 [DOI] [PubMed] [Google Scholar]
- 19.Padilla SL, Johnson CW, Barker FD, Patterson MA, Palmiter RD. A neural circuit underlying the generation of hot flushes. Cell Rep 2018;24:271–277. doi: 10.1016/j.celrep.2018.06.037 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Borsay BA Skrapits K Herczeg L, et al. Hypophysiotropic gonadotropin-releasing hormone projections are exposed to dense plexuses of kisspeptin, neurokinin B and substance p immunoreactive fibers in the human: a study on tissues from postmenopausal women. Neuroendocrinology 2014;100(2-3):141–152. doi: 10.1159/000368362 [DOI] [PubMed] [Google Scholar]
- 21.Hrabovszky E Borsay BA Racz K, et al. Substance P immunoreactivity exhibits frequent colocalization with kisspeptin and neurokinin B in the human infundibular region. PLoS One 2013;8:e72369. doi: 10.1371/journal.pone.0072369 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Navarro VM Bosch MA Leon S, et al. The integrated hypothalamic tachykinin-kisspeptin system as a central coordinator for reproduction. Endocrinology 2015;156:627–637. doi: 10.1210/en.2014-1651 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Trower M, Anderson RA, Ballantyne E, Joffe H, Kerr M, Pawsey S. Effects of NT-814, a dual neurokinin 1 and 3 receptor antagonist, on vasomotor symptoms in postmenopausal women: a placebo-controlled, randomized trial. Menopause 2020;27:498–505. doi: 10.1097/GME.0000000000001500 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Andersen ML, Nascimento DC, Machado RB, Roizenblatt S, Moldofsky H, Tufik S. Sleep disturbance induced by substance P in mice. Behav Brain Res 2006;167:212–218. doi: 10.1016/j.bbr.2005.09.008 [DOI] [PubMed] [Google Scholar]
- 25.Lieb K Ahlvers K Dancker K, et al. Effects of the neuropeptide substance P on sleep, mood, and neuroendocrine measures in healthy young men. Neuropsychopharmacology 2002;27:1041–1049. doi: 10.1016/S0893-133X(02)00369-X [DOI] [PubMed] [Google Scholar]
- 26.Schaffalitzky De Muckadell OB, Aggestrup S, Stentoft P. Flushing and plasma substance P concentration during infusion of synthetic substance P in normal man. Scand J Gastroenterol 1986;21:498–502. doi: 10.3109/00365528609015169 [DOI] [PubMed] [Google Scholar]
- 27.Wong BJ, Minson CT. Neurokinin-1 receptor desensitization attenuates cutaneous active vasodilatation in humans. J Physiol 2006;577(Pt 3):1043–1051. doi: 10.1113/jphysiol.2006.112508 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kramer MS Winokur A Kelsey J, et al. Demonstration of the efficacy and safety of a novel substance P (NK1) receptor antagonist in major depression. Neuropsychopharmacology 2004;29:385–392. doi: 10.1038/sj.npp.1300260 [DOI] [PubMed] [Google Scholar]
- 29.Ratti E Bellew K Bettica P, et al. Results from 2 randomized, double-blind, placebo-controlled studies of the novel NK1 receptor antagonist casopitant in patients with major depressive disorder. J Clin Psychopharmacol 2011;31:727–733. doi: 10.1097/JCP.0b013e31823608ca [DOI] [PubMed] [Google Scholar]
- 30.Ratti E Bettica P Alexander R, et al. Full central neurokinin-1 receptor blockade is required for efficacy in depression: evidence from orvepitant clinical studies. J Psychopharmacol 2013;27:424–434. doi: 10.1177/0269881113480990 [DOI] [PubMed] [Google Scholar]
- 31.Kramer MS Cutler N Feighner J, et al. Distinct mechanism for antidepressant activity by blockade of central substance P receptors. Science 1998;281:1640–1645. doi: 10.1126/science.281.5383.1640 [DOI] [PubMed] [Google Scholar]
- 32.Ratti E Carpenter DJ Zamuner S, et al. Efficacy of vestipitant, a neurokinin-1 receptor antagonist, in primary insomnia. Sleep 2013;36:1823–1830. doi: 10.5665/sleep.3208 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Cytel . Compass User Manual. Cambridge, MA: Cytel Inc; 2012. [Google Scholar]
- 34.Ivanova A, Bolognese JA, Perevozskaya I. Adaptive dose finding based on t-statistic for dose-response trials. Stat Med 2008;27:1581–1592. doi: 10.1002/sim.3209 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.US Food and Drug Administration . Guidance for Industry. Drug-Induced Liver Injury: Premarketing Clinical Evaluation. Washington DC: US Department of Health and Human Services; 2009. [Google Scholar]
- 36.Yang M, Morin CM, Schaefer K, Wallenstein GV. Interpreting score differences in the Insomnia Severity Index: using health-related outcomes to define the minimally important difference. Curr Med Res Opin 2009;25:2487–2494. doi: 10.1185/03007990903167415 [DOI] [PubMed] [Google Scholar]
- 37.Lewis JE, Hilditch JR, Wong CJ. Further psychometric property development of the Menopause-Specific Quality of Life questionnaire and development of a modified version, MENQOL-Intervention questionnaire. Maturitas 2005;50:209–221. doi: 10.1016/j.maturitas.2004.06.015 [DOI] [PubMed] [Google Scholar]
- 38.Fraser GL Lederman S Waldbaum A, et al. A phase 2b, randomized, placebo-controlled, double-blind, dose-ranging study of the neurokinin 3 receptor antagonist fezolinetant for vasomotor symptoms associated with menopause. Menopause 2020;27:382–392. doi: 10.1097/GME.0000000000001510 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Prague JK Roberts RE Comninos AN, et al. Neurokinin 3 receptor antagonism as a novel treatment for menopausal hot flushes: a phase 2, randomised, double-blind, placebo-controlled trial. Lancet 2017;389:1809–1820. doi: 10.1016/s0140-6736(17)30823-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Lobo RA Archer DF Kagan R, et al. A 17β-estradiol-progesterone oral capsule for vasomotor symptoms in postmenopausal women: a randomized controlled trial. Obstet Gynecol 2018;132:161–170. doi: 10.1097/AOG.0000000000002645 [DOI] [PubMed] [Google Scholar]
- 41.Pinkerton JV, Utian WH, Constantine GD, Olivier S, Pickar JH. Relief of vasomotor symptoms with the tissue-selective estrogen complex containing bazedoxifene/conjugated estrogens: a randomized, controlled trial. Menopause 2009;16:1116–1124. doi: 10.1097/gme.0b013e3181a7df0d [DOI] [PubMed] [Google Scholar]
- 42.US Food and Drug Administration . Brisdelle Cross Discipline Team Leader Review. Silver Spring, MD: Center for Drug Evaluation and Research; 2013. [Google Scholar]
- 43.Prague JK Roberts RE Comninos AN, et al. Neurokinin 3 receptor antagonism rapidly improves vasomotor symptoms with sustained duration of action. Menopause 2018;25:862–869. doi: 10.1097/GME.0000000000001090 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.US Food and Drug Administration . Clinical review of Brisdelle for the treatment of moderate to severe vasomotor symptoms associated with the menopause. Silver Spring, MD: Center for Drug Evaluation and Research; 2013. [Google Scholar]
- 45.Woods NF Hohensee C Carpenter JS, et al. Symptom clusters among MsFLASH clinical trial participants. Menopause 2016;23:158–165. doi: 10.1097/GME.0000000000000516 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Carpenter JS, Andrykowski MA. Psychometric evaluation of the Pittsburgh Sleep Quality Index. J Psychosom Res 1998;45:5–13. doi: 10.1016/s0022-3999(97)00298-5 [DOI] [PubMed] [Google Scholar]
- 47.Simon JA Portman DJ Kaunitz AM, et al. Low-dose paroxetine 7.5 mg for menopausal vasomotor symptoms: two randomized controlled trials. Menopause 2013;20:1027–1035. doi: 10.1097/GME.0b013e3182a66aa7 [DOI] [PubMed] [Google Scholar]