

Abstract
PURPOSE
The Teaming and Integrating for Smiles and Health (TISH) Learning Collaborative was developed to help health care organizations accelerate progress in integrating delivery of oral and primary care. By providing expert support and a structure for testing change, the project aimed to improve the early detection of hypertension in the dental setting and of gingivitis in the primary care setting, and to increase the rate of bidirectional referrals between oral and primary care partners. We report its outcomes.
METHODS
A total of 17 primary and oral health care teams were recruited to participate in biweekly virtual calls over 3 months. Participants tested changes to their models of care through Plan-Do-Study-Act cycles between calls. Sites tracked the percentages of patients screened and referred, completed the TeamSTEPPS (Team Strategies and Tools to Enhance Performance and Patient Safety) and Interprofessional Assessment questionnaires, and provided qualitative feedback and updates in storyboard presentations.
RESULTS
On average, with implementation of the TISH Learning Collaborative, sites displayed a nonrandom improvement in the percentages of patients screened for hypertension, referred for hypertension, referred to primary care, and referred for gingivitis. Gingivitis screening and referral to oral health care were not markedly improved. Qualitative responses indicated that teams made progress in screening and referral workflows, improved communication between medical and dental partners, and furthered understanding of the connection between primary care and oral care among staff and patients.
CONCLUSIONS
The TISH project is evidence that a virtual Learning Collaborative is an accessible and productive avenue to improve interprofessional education, further primary care and oral partnerships, and achieve practical progress in integrated care.
Key words: oral health, primary care, integrated care, virtual learning collaborative, multidisciplinary research, hypertension screening, gingivitis screening, interprofessional education, interprofessional relations, referral and consultation, organizational change
INTRODUCTION
Primary and oral health care professionals nationally perceive a need to expand the capacity of the health care workforce through the integration of services. Chronic illness and poor oral health are increasingly prevalent, and patients are more often living with undiagnosed conditions or poorly managed symptoms because of barriers to patient-centered, integrated care.1 Each year, more than 100 million people in the United States receive care from a physician but not a dentist, and 27 million people visit a dentist but not a physician.2 In this context, it is logical to use both clinical settings as opportunities for screening, counseling, and referral.3
Most physicians and dentists believe screening for oral and systemic conditions in both the medical and dental settings is critical and are willing to accept and offer a referral to or from their medical or dental counterparts.4,5 Inadequate time and training, limited interoperability of information systems, and poor care coordination between these teams pose challenges to integration in practice, however.6,7 At this stage, testing innovative solutions is critical to driving progress to improve access and health outcomes.
A Learning Collaborative offers the structure for teams motivated toward a common goal to learn from experts, test real-world change, and document progress for quality improvement. The Institute for Healthcare Improvement’s Breakthrough Series model for collaborative learning produces accelerated progress in a range of health care applications, and work by CoImagine Health has shown the benefit of a quality improvement framework in guiding oral health integration into primary care.8,9 These experiences support the creation of a Breakthrough Series collaborative targeted at bidirectional oral and primary care integration. The Center for Integration of Primary Care and Oral Health (CIPCOH), with help from the Harvard School of Dental Medicine’s Initiative to Integrate Oral Health and Medicine, developed and implemented the Teaming and Integrating for Smiles and Health (TISH) virtual Learning Collaborative. The project had 2 overall goals: (1) to increase the early detection of hypertension in the oral care setting and gingivitis in the primary care setting and (2) to improve referral rates between primary care and oral health partners. Both are attainable objectives of clinical importance.
Hypertension and gingivitis were selected as targets for improved detection based on their high prevalence, ease of screening, and potential for identifying patients needing preventive primary or oral health care. Gingivitis is a common condition of the oral cavity that presents as inflammation of the gingiva, which can be reversed with appropriate treatment. Without intervention, gingivitis can sometimes progress to more severe forms of periodontal disease, such as periodontitis. Although periodontitis is acknowledged for its risks to systemic health, the project targeted gingivitis for the ease of screening by visual oral examination and because the higher prevalence can identify more patients in need of preventive dental care.10-12
Similarly, hypertension, defined by the Seventh Report of the Joint National Committee as a systolic blood pressure greater than 140 mm Hg or a diastolic blood pressure greater than 90 mm Hg,13 is highly prevalent among adults in the United States. Furthermore, many patients have uncontrolled disease or are unaware of their hypertensive status.14,15 In this context, the dental setting is an opportunity to identify undiagnosed or poorly managed hypertension and to make a referral for proper care. Screening for hypertension is also relevant in the immediate dental appointment, as nonemergent dental procedures are recommended to be postponed for patients with blood pressures greater than 180/110 mm Hg.16
The TISH Learning Collaborative describes medical and dental teams working together to implement screening and referral processes in tandem and thereby improve the detection and management of gingivitis and hypertension. The Learning Collaborative framework and finalized driver diagram, described below, serve as a model and a tool for primary and oral care integration for broad dissemination.
METHODS
The TISH Learning Collaborative was developed by CIPCOH and funded by the Health Resources and Services Administration (HRSA). Project development began in November 2020 with the assembly of a core team responsible for site recruitment, curriculum development, and ultimate implementation of the virtual project. Project methods were approved by the Harvard Longwood Campus Institutional Review Board.
The initial goal was to recruit 20 teams, 2 from each HRSA region. Many teams, however, lacked the bandwidth to participate while negotiating the COVID-19 vaccine rollout. On the basis of this feedback, the project start date was postponed until April 2021. Ultimately, 17 sites from 7 of the 10 HRSA regions, and 1 site from Somaliland, Africa, joined the project. The inclusion of a site outside the United States was not part of the initial recruitment plan but contributed to the diverse assortment of teams.
Driver Diagram
From the current understanding of primary care and oral health integration, the core team constructed a driver diagram to illustrate the steps necessary to achieve the project aim (Figure 1). Primary drivers directly contributed to the project aim, while secondary drivers represented the norms, processes, and structures that promoted the primary drivers. The driver diagram was used to create a curriculum presenting the knowledge and evidence-based strategies needed to achieve the primary and secondary drivers (Table 1). At project closure, teams had the opportunity to refine the driver diagram based on lessons learned and to contribute their actionable change ideas to the logic map.
Figure 1.
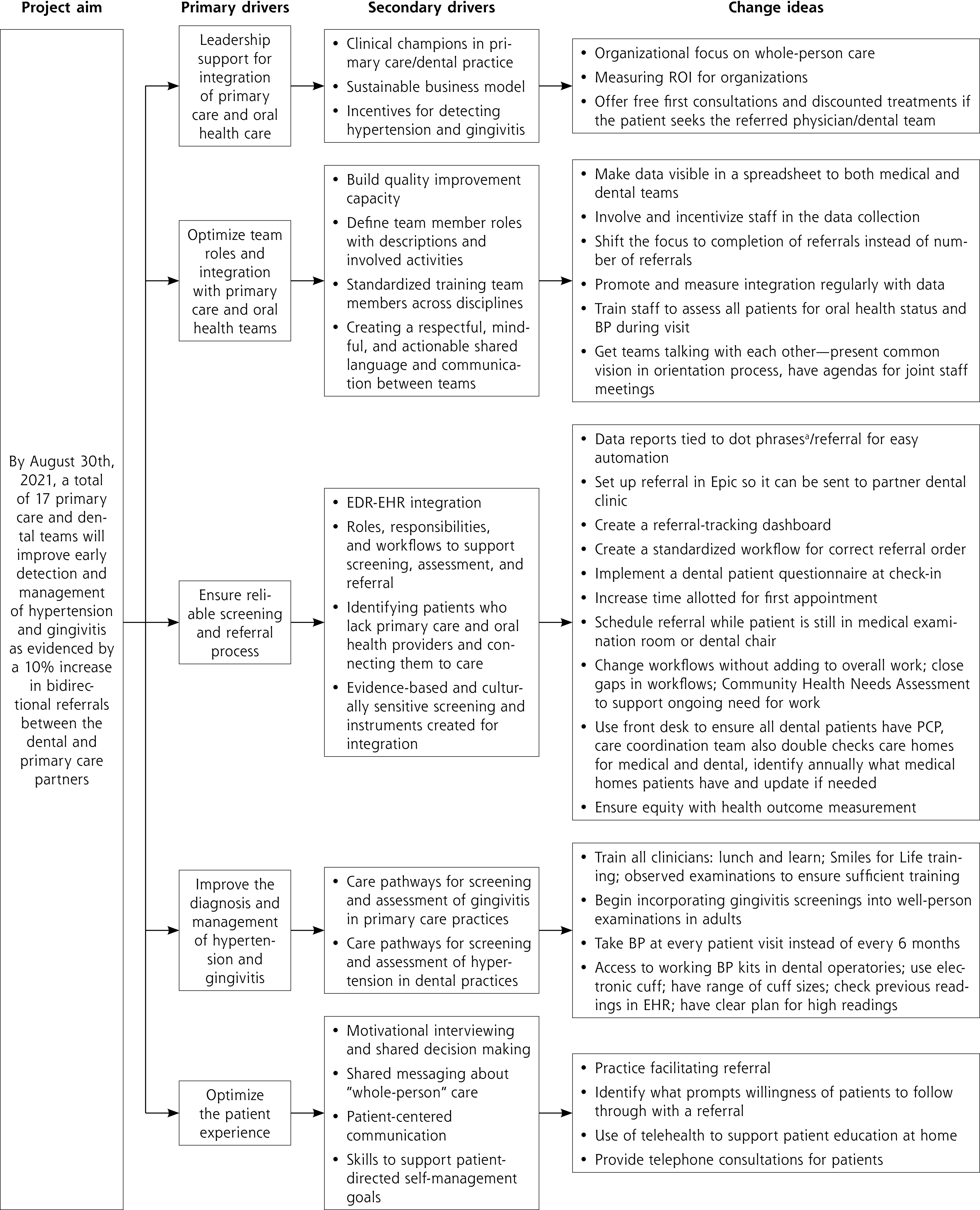
Driver diagram for the TISH Learning Collaborative.
BP = blood pressure; EDR = electronic dental record; EHR = electronic health record; PCP = primary care professional; ROI = return on investment; TISH = Teaming and Integrating for Smiles and Health.
a Blocks of text that can be inserted by typing a period (dot) followed by a short phrase.25
Table 1.
TISH Learning Collaborative Curriculum
| Component | Topics and Activities |
|---|---|
| Learning Session I | Teams draft aims statements Review quality improvement methodology, process mapping, goals for data collection, and IRB process |
| Webinar: Oral Health Integration Care Pathways I | Review the Integration Spectrum Share examples of screening workflows Teams use process mapping to plan unique workflows Highlight anticipated challenges and corresponding solutions |
| Webinar: Oral Health Integration Care Pathways II | Review oral pathology and indications for dental referrals Present ADA and ACEP guidelines for hypertension and consider creating team guidelines for referral Review how to build referral networks and ensure communication between health care teams |
| Learning Session II | Share evidence-based strategies to improve patient engagement and teamwork |
| Webinar: Team Progress | Teams present storyboards with progress updates on PDSA cycles, requests for assistance, and goals for future learning |
| Webinar: Optimizing Workflows | Review the benefits of visual workflows for quality improvement Share tips for introducing workflows to staff, communicating roles, and recognizing missteps or redundancies |
| Webinar: Sustain and Spread | Prepare teams to sustain improvements Consider ways to communicate knowledge learned |
| Learning Session III | Teams share final storyboards that include reflections, lessons learned, and sustainability plans |
ACEP = American College of Emergency Physicians; ADA = American Dental Association; IRB = institutional review board; PDSA = Plan-Do-Study-Act; TISH = Teaming and Integrating for Smiles and Health.
Project Implementation
The TISH project operated using a virtual structure adapted from the Institute for Healthcare Improvement’s Breakthrough Series model. At project onset, each site created a team of 3 to 5 primary and oral health care professionals motivated to drive change in their organizations. Teams completed a Readiness Assessment questionnaire to measure their understanding of quality improvement methodology and current efforts in integration. Teams also drafted aim statements to clarify site-specific goals for the project.
Over 3 months, participants engaged in biweekly educational webinars or virtual learning sessions facilitated by experts in integrating primary and oral health care (Table 1). From knowledge learned, teams theorized changes to their existing workflows that would achieve the project goals. Ideas were tested through Plan-Do-Study-Act (PDSA) cycles during the “action periods” between virtual meetings, and progress updates were presented as “storyboards” in Learning Sessions II and III.17 Storyboards were created as presentations in PowerPoint (Microsoft). These sessions offered teams the space to voice setbacks, ask questions, and collaborate with one another as they worked through similar challenges. To equip teams to maintain and improve on progress made, we provided a sustainability planning worksheet 2 weeks before the final learning session.
Data Collection and Analysis
At project start and end, participants completed the Agency for Healthcare Research and Quality’s TeamSTEPPS (Team Strategies and Tools to Enhance Performance and Patient Safety) questionnaire and an Interprofessional Assessment questionnaire created by the core team.18 TeamSTEPPS measured improvement in team functioning, identity, and leadership, and the Interprofessional Assessment tracked changes in self-reported confidence in cross-disciplinary care. Questions for the latter were tailored to medical or dental perspectives, depending on the respondent’s role.
Sites were asked to track the number of medical and dental screenings completed, the number of patients presenting with hypertension or gingivitis, the number of referrals made to primary and dental care partners in general and for hypertension or gingivitis specifically, and the number of referrals that successfully resulted in a patient appointment. Eligible patients were defined as individuals aged 18 years and older presenting for an annual physical examination or biannual dental cleaning and examination. Data were reported in 2-week collection intervals, and run charts were created to show the progress of individual teams over time. Additional run charts displayed the average among sites and the corresponding median (Supplemental Figure 1). Charts were evaluated according to the quality improvement rule that fewer than 3 crossings of the median suggest a nonrandom change.18 Qualitative responses in storyboards were examined through conceptual analysis based on frequency to identify common themes among participating sites and to draw connections to existing literature.19
We analyzed TeamSTEPPS responses by the accepted method of summing individual subscores.18 Interprofessional Assessment responses were converted to a numerical scale (strongly disagree/ lowest = 1; strongly agree/highest = 5) and separated into medical and dental cohorts. Because our sample was small, formal statistical testing of the underlying hypothesis is likely not supported; therefore, we propose a future study with adequate power in the Supplemental Appendix.
RESULTS
All 17 recruited sites completed the Readiness Assessment questionnaire. Of those, 10 completed the initial Team-STEPPS and Interprofessional Assessment questionnaires, and 8 sustained active participation through biweekly calls and data collection. The participating sites were preferentially from HRSA regions 2, 8, and 9.
The Readiness Assessment results (Table 2) and qualitative feedback indicated that sites were at varying stages of integration at the start of the TISH project. The Interprofessional Assessment results showed moderate levels of confidence in cross-disciplinary care at that time (Table 3).
Table 2.
Team Responses on Readiness Assessment Questionnaire (N = 17)
| Readiness Statement | Teams Endorsing Statement, % |
|---|---|
| Quality improvement | |
| A dental measure is part of the primary care team’s quality improvement plan | 70.6 |
| A hypertension measure is part of the dental team’s quality improvement plan | 76.5 |
| The primary medical care team utilizes telehealth services | 88.2 |
| The dental care team utilizes teledentistry services | 52.9 |
| Referrals | |
| Team has a formal referral process/system | 25.0 |
| Team has an informal referral process/system | 56.3 |
| Team has no referral process/system | 18.8 |
| Communication between teams | |
| Team has an engrained line of communication | 33.3 |
| Team has an informal or loose line of communication | 53.3 |
| Team has no communication | 13.3 |
| EHR connection between dental and medical teams | |
| Teams’ EHRs are connected | 37.5 |
| Teams’ EHRs are not connected | 62.5 |
EHR = electronic health record.
Table 3.
Team Responses on Interprofessional Assessment Questionnaire
| Group and Question | Pre-TISH Score | Post-TISH Score |
|---|---|---|
| Primary care teams | (n = 3) | (n =7) |
| How much do you perceive that dental colleagues are interested in the overall health of patients? | 4.67 | 4.00 |
| How important do you feel good oral health is for the overall health of your patients? | 4.67 | 4.29 |
| How do you rate your skill to counsel patients on oral health? | 3.00 | 3.14 |
| How would you rate your skill level to examine and assess a patient’s mouth? | 2.67 | 2.86 |
| How would you rate your awareness of local dentists and the details of making referrals to/from them? | 4.00 | 3.29 |
| How would you rate your current ability to communicate with local dentists? | 3.67 | 3.14 |
| How confident are you that your patients will get timely referrals to dental colleagues? | 3.67 | 3.43 |
| Dental teams | (n = 8) | (n = 5) |
| How much do you perceive that medical colleagues are interested in the overall health of patients? | 3.63 | 3.60 |
| How important do you feel that your medical colleagues believe good oral health contributes to the overall health of their patients? | 4.13 | 5.00 |
| How would you rate your skill level to counsel patients on blood pressure? | 3.50 | 4.40 |
| How would you rate your skill level to examine and assess a patient’s blood pressure? | 3.63 | 4.20 |
| How would you rate your awareness of local primary care/medical providers and the details of making referrals to/from them? | 3.86 | 4.75 |
| How would you rate your current ability to communicate with local primary care/medical providers? | 4.14 | 4.75 |
| How confident are you that your patients will get timely referrals to primary care/medical colleagues? | 3.43 | 4.25 |
TISH = Teaming and Integrating for Smiles and Health.
Note: Scores are means. Possible range of scores is 1 (strongly disagree/lowest) to 5 (strongly agree/highest).
Table 4 summarizes characteristics of the participating sites and their respective TISH-related workflow changes, screening and referral data, and reflections on the experience. Given the mix in readiness levels and the diversity of practice styles, teams naturally prioritized different objectives and tested unique change ideas.
Table 4.
Summary of Teams’ TISH Experiences and Results
| Team | Site Description | Change Ideas | Results | Reflection |
|---|---|---|---|---|
| The National Health Professions Commission (NHPC) Somaliland | A statutory body that mandates the regulation, accreditation, and licensing of health care professionals, health care facilities, and health training institutions in Somaliland, Africa | Longer first visits/consultations with patients to implement screenings More thorough oral health assessment in primary care setting Physician and dentist have telephone consultation over BP measurements, blood sugar levels, gingivitis Regular biweekly meetings to update the team and discuss weaknesses and strengths |
Screened 100 patients (16.1%) for hypertension Referred 57 patients (9.9%) to primary care Screened 339 patients (89.9%) for gingivitis Referred 176 patients (46.7%) to dental care |
“When patients come from their … physician and finally understand the importance of oral health, and they seek dental professionals for check-ups/treatment, it is truly a milestone!” |
| St Barnabas Hospital (SBH) Health System | A teaching hospital with medical and dental residency programs | Education of residents and assistants Medical team evaluates patient initially using the questionnaire and the examination follows Reinforced team cooperativity by presenting a virtual meeting to residents and attendings about progress Developed the spreadsheets on teams so data can be seen by everyone |
Screened 861 patients (100%) for hypertension Referred 83 patients (9.6%) to primary care |
“Created an awareness of the impact of dental health on overall health” |
| St Mary’s Medical Center Family Medicine Residency Program | A patient-centered medical home with a focus on training physicians for rural practice; the team partnered with a nearby health center to provide dental services | Begin incorporating gingivitis screen into well-person examinations in adults; results are recorded in the chart Set up referrals to dental partners in Epic to streamline referral process |
Screened 409 patients (92.1%) for hypertension Referred 59 patients (13.3%) to primary care Screened 58 patients (63.0%) for gingivitis Referred 11 patients (11.9%) to dental care |
“Watching our dental examination numbers and referral numbers improve from zero, showing that we’re starting to take oral health more seriously in our clinic, and that we now have dental partners to help us do better in this goal” |
| Tiburcio Vasquez Health Center (TVHC) | A Federally Qualified Health Center providing comprehensive medical and dental services | Access to working BP kits in dental operatories; staff are educated on hypertension guidelines Warm hand-off to medical team if BP >160/110 mm Hg Education and training for medical team Trackable and streamlined referral process between dental and medical teams |
Referred 557 patients (14.7%) to primary care | “Medical-to-dental process is now so much swifter for adult patients who need to be seen, increased Epic connectivity between the 2 disciplines.” |
| Pacific Dental Services | A dental support organization with a focus on raising awareness of the link between oral health and overall health on a national scale | Dental front office has patient complete questionnaire at check-in Front office, medical assistants, and dental assistant coordinate to schedule referral appointments while patient still in dental chair or medical examination room Improved EHR referral and launched referral-tracking dashboard Altered marketing material in the medical and dental settings |
Referred 114 patients (6.0%) to primary care Referred 287 patients (17.5%) to dental care |
“We have had some big wins in getting dental to engage in the referral process with minimal added lift to improve bidirectional flow and the level of care being provided to patients.” |
| The Partners in Integrated Care (PIC) Place | A nonprofit organization offering medical, dental, vision, and behavioral health services | Train dental staff to take manual BP measurements “Summer Smackdown” to incentivize staff to make cross-discipline referrals; involve staff in the data collection process Implemented checklists for medical team to remember oral screening |
Referred 43 patients (2.8%) to primary care Referred 89 patients (7.6%) to dental care |
“Summer Smackdown winners really put forth effort in creating referrals and thrived under the positive incentives and recognition.” |
| Harvard Dental Center | An academic dental clinic with faculty professionals | BP measured at every patient visit Dental assistant takes and records BP at the start of every visit in AxiUm and Excel sheet |
Screened 83% of patients for hypertension | “The workflow between a dentist and dental assistant is like doing a dance. This team started working together just 1 month before TISH. TISH helped establish the footwork for at least one part of the clinic workflow. We’re proud to say that we’re now dancing!” |
| Cambridge Health Alliance (CHA) | A safety net hospital system with a dental center | Studied criteria and process for dental-to-medical referral by tracking hypertension screenings and the action taken by provider Train dental users on Epic |
Screened 158 patients for hypertension Counseled 23% of patients with stage 2 hypertension |
“Learning what upstream resources our organization has to address structural determinants to health and how they can be applied in the dental setting” |
BP = blood pressure; EHR = electronic health record; TISH = Teaming and Integrating for Smiles and Health.
Aggregate team data showed a nonrandom improvement from baseline to the end of the 3-month TISH project in the percentage of patients screened for hypertension, the percentage referred to primary care, the percentage referred for hypertension, and the percentage referred for gingivitis (Supplemental Figure 1). Data for the percentage of patients assessed for oral health status and the percentage of patients referred to a dental partner crossed the median 3 times and, therefore, are not considered a nonrandom improvement.
Qualitative responses from the teams in their final storyboards supported the TISH project’s success. Teams expressed improvement in their referral process and in their communication within and between medical and dental teams, and attained a greater understanding of the connection between oral and systemic health among patients and staff. Highlights of team reflections are shown in Table 4.
In presenting their lessons learned, many sites noted the continuous effort required to maintain momentum. Consistent coaching in team meetings, identifying areas for retraining, and creating incentives for staff were some strategies teams used to promote enthusiasm toward integrated care. Participants also noted strategies that increased their referral success, such as an initial patient questionnaire to prime patients for future conversations about cross-disciplinary care. In such conversations, some teams worked to communicate the oral-systemic link and, when possible, drew connections between a patient’s oral and primary care concerns. Teams also suggested warm hand-offs to medical and dental partners or leveraging assistants and front office staff to schedule the referral while the patient was still in the office. Sites planned to use various strategies to sustain and build on these lessons learned (Table 5).
Table 5.
Team Sustainability Planning
| Sustainability Question | Team Plans |
|---|---|
| What type of training will we use? | Introductory and ongoing training to share TISH material and demonstrate data collection Data scorecard automatically delivered to dental and medical champions monthly to help target training and retraining Literature/journal sharing Team huddles, leading by example, setting daily goals, creating excitement |
| How will we make it hard to do the wrong thing and easy to do the right thing? | Draft new guidelines for each workflow Documentation and constant coaching to the same message and workflow Checklists and reminders in EMR to prompt screening Questionnaires and brochures at every computer Automating referrals and data tracking in EMR Ensuring more than 1 person is assigned for critical/important steps |
| Are our changes increasing the overall workload to the system? If so, how can we decrease the workload? If not, how will we communicate about what is? | Slightly yes—but hopefully it becomes the workflow and not an addition to the old workflow Simple system is most sustainable Using standard documentation (dot phrasesa) and referral processes will decrease burden Some day interface between 2 EHRs Continue collecting subjective data from huddle |
EHR = electronic health record; EMR = electronic medical record; TISH = Teaming and Integrating for Smiles and Health.
Blocks of text that can be inserted by typing a period (dot) followed by a short phrase.25
Results from the Interprofessional Assessment questionnaire showed that by the end of TISH, dental respondents had markedly improved their self-reported ability to counsel patients on blood pressure (Table 3). Although other responses did not change appreciably, dental respondents unanimously believed that their medical colleagues regarded oral health as strongly important to patients’ overall health at the project’s closure. TeamSTEPPS scores did not show a statistically significant change (results not shown)
DISCUSSION
The TISH project demonstrates that the Breakthrough Series model can be modified to a shortened, virtual format to accelerate progress in integrating primary and oral health care. With the insight of experts in the field, we synthesized knowledge about facilitators of integration into a driver diagram and provided the structure for teams to work toward these elements and address barriers to progress.6,7 Team revisions to the diagram provide practical suggestions for other organizations to implement this work (Figure 1).
Our results show that cross-disciplinary screening is a means for dental professionals to identify undiagnosed or poorly managed hypertension and for medical professionals to improve access to oral health monitoring and care. The financial sustainability of these efforts is a primary concern in the existing literature, however. An analysis by Nasseh et al20 finds that collaboration among team members maximizes cost-effectiveness and suggests training dental assistants to conduct the screenings. Our work aligns with their proposal by presenting a model for interprofessional training and showing teams leveraging assistants and front office personnel in their workflows.
To our knowledge, TISH is the first Learning Collaborative focused on bidirectional referrals between dental and medical teams. This is particularly relevant as the analysis of Nasseh et al20 asserts the importance of successful referral for financial sustainability, but building referral processes is an acknowledged challenge in other studies. Among the pilot projects described by Linabarger et al,7 clinical sites faced difficulty gaining clinician buy-in and adjusting workflows. The support TISH offered for the creation of screening and referral processes simultaneously and the ability of teams to accomplish this goal are a notable success. It is possible that the groundwork required for participation—including designating a leadership team and choosing a dental or medical partner to receive referrals—mitigated some of these challenges. Harnagea et al6 found through a scoping review that integrating oral health into primary care faces specific resistance because of the perception that oral care is less valuable given that oral conditions are usually non–life-threatening. Concerns over the scope of practice and shared responsibility can also impede progress. Potentially, the TISH project alleviated some of this resistance because medical and dental teams convened with a common motivation to integrate care. Additionally, teams mentioned that they attained better understanding of the importance of oral health among staff and patients throughout the project.
Past research highlights the need to address inadequate training and confidence in achieving cross-disciplinary care. A survey by Vernon et al21 found that 87.7% of physicians regard their medical training as inadequate to evaluate oral conditions, and work by dela Cruz et al22 determined that physicians with high confidence in their screening ability are more likely to initiate referrals for pediatric patients. Although the TISH curriculum presented the clinical information relevant for screening, only dental professionals showed quantitative improvement in self-reported screening confidence; thus, a Learning Collaborative is a potential way to address these concerns but may benefit from revision. Past work on improving interprofessional education demonstrates the success of hands-on instruction for physicians learning to conduct fluoride varnish and oral cancer screenings.23,24 Although the virtual format had numerous benefits—especially in the context of the COVID-19 pandemic—a future collaborative could incorporate in-person meetings between local teams to supplement virtual education.
The characteristics of our recruited sites align with the observation by Atchinson et al3 that health care organizations caring for Medicaid-enrolled populations tend to be leaders in promoting integration. We chose to recruit practice sites with an overall goal of integrating primary and oral health care, even if they did not aim to improve both screening and bidirectional referrals. The option for teams to individualize their work was a benefit of the collaborative structure but also posed a challenge to data collection because many sites tailored collection to their specific goals. The lack of financial incentives likely also contributed to inconsistent participation and the lower site retention rate. Altogether, these factors limited the amount of data available as evidence of the project. This shortcoming is particularly relevant when examining the TeamSTEPPS and Interprofessional Assessment results. For these measures, the identity of respondents and the sample size of respondent cohorts changed between the start and end questionnaires; therefore, responses may not represent individual changes in attitude or may inaccurately show improvement or lack thereof.
Although the data collection and participation challenges are limitations of this work, we also note that teams were negotiating the demands of COVID-19 during the project’s timespan. The diligent work of 8 sites without financial support therefore suggests the level of motivation present to integrate care and the potential interest to build on this model. A future collaborative could focus on optimizing electronic health record systems because participating teams noted this as both a challenge to overcome and a means to streamline their referral and data-tracking processes.
In conclusion, the TISH project demonstrates that a Learning Collaborative adapted from the Breakthrough Series model is a viable strategy to disseminate knowledge of and ignite progress in the integration of oral and primary care. The virtual format was accessible to health care organizations across the country and internationally, and the tools and strategies presented were relevant to a diverse network of health care sites. The progress made through the TISH project suggests the multitude of ways in which integration can be achieved and shows that progress is feasible with proper support and innovation.
Supplementary Material
Acknowledgments
We would like to thank all oral health and primary care professionals who worked toward the TISH project goals in their clinical sites. Their diligent efforts and feedback contributed to the production of this article.
Footnotes
Conflicts of interest: Dr Phillips is an advisor for Bicycle Health, a for-profit company providing telemedicine services to patients with opioid use disorder. He is also an advisor for Grow Therapy, a for-profit company that assists social workers and psychiatric nurse practitioners with insurance credentialing, record keeping, billing, and marketing. The other authors report no conflicts.
Funding support: This work was funded by the US Department of Health and Human Services (HHS), Health Resources and Services Administration (HRSA) under cooperative agreement UH1HP29962.
Disclaimer: The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by HRSA, HHS or the US Government.
References
- 1.Raghupathi W, Raghupathi V. An empirical study of chronic diseases in the United States: a visual analytics approach. Int J Environ Res Public Health. 2018;15(3):431. 10.3390/ijerph15030431 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Molayem S. Dentists and doctors need to play on the same team. Nature. 2021;Oct 27. 10.1038/d41586-021-02919-3 [DOI] [PubMed]
- 3.Atchison KA, Weintraub JA, Rozier RG. Bridging the dental-medical divide: case studies integrating oral health care and primary health care. J Am Dent Assoc. 2018;149(10):850-858. 10.1016/j.adaj.2018.05.030 [DOI] [PubMed] [Google Scholar]
- 4.Greenberg BL, Glick M, Frantsve-Hawley J, Kantor ML. Dentists’ attitudes toward chairside screening for medical conditions. J Am Dent Assoc. 2010;141(1):52-62. 10.14219/jada.archive.2010.0021 [DOI] [PubMed] [Google Scholar]
- 5.Harnagea H, Lamothe L, Couturier Y, Emami E. How primary health care teams perceive the integration of oral health care into their practice: A qualitative study. PLoS ONE. 2018;13(10):e0205465. 10.1371/journal.pone.0205465 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Harnagea H, Couturier Y, Shrivastava R, et al. Barriers and facilitators in the integration of oral health into primary care: a scoping review. BMJ Open. 2017;7(9):e016078. 10.1136/bmjopen-2017-016078 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Linabarger M, Brown M, Patel N. A pilot study of integration of medical and dental care in 6 states. Prev Chronic Dis. 2021;18:E72. 10.5888/pcd18.210027 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Institute for Healthcare Improvement (IHI) . The Breakthrough Series. IHI’s collaborative model for achieving breakthrough improvement. Published 2003. Accessed Sep 5, 2022. https://www.ihi.org:443/resources/Pages/IHIWhitePapers/TheBreakthroughSeriesIHIsCollaborativeModelforAchievingBreakthroughImprovement.aspx
- 9.Hummel J, Phillips KE, Holt B, Hayes C. Oral Health: An Essential Component of Primary Care. White Paper. Qualis Health; 2015. [Google Scholar]
- 10.Hegde R, Awan KH. Effects of periodontal disease on systemic health. Dis Mon. 2019;65(6):185-192. 10.1016/j.disamonth.2018.09.011 [DOI] [PubMed] [Google Scholar]
- 11.Tonetti MS, Jepsen S, Jin L, Otomo-Corgel J. Impact of the global burden of periodontal diseases on health, nutrition and wellbeing of mankind: a call for global action. J Clin Periodontol. 2017;44(5):456-462. 10.1111/jcpe.12732 [DOI] [PubMed] [Google Scholar]
- 12.Stamm JW. Epidemiology of gingivitis. J Clin Periodontol. 1986;13(5):360-366. 10.1111/j.1600-051X.1986.tb01473.x [DOI] [PubMed] [Google Scholar]
- 13.Textor SC, Schwartz GL, Frye RL. The new hypertension guidelines from JNC 7: is the devil in the details? Mayo Clin Proc. 2003;78(9):1078-1081. 10.4065/78.9.1078 [DOI] [PubMed] [Google Scholar]
- 14.Vasan RS, Larson MG, Leip EP, et al. Impact of high-normal blood pressure on the risk of cardiovascular disease. N Engl J Med. 2001;345(18):1291-1297. 10.1056/NEJMoa003417 [DOI] [PubMed] [Google Scholar]
- 15.Park S, Gillespie C, Baumgardner J, et al. Modeled state-level estimates of hypertension prevalence and undiagnosed hypertension among US adults during 2013-2015. J Clin Hypertens (Greenwich). 2018;20(10):1395-1410. 10.1111/jch.13388 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Department of Scientific Information, Evidence Synthesis & Translation Research, ADA Science & Research Institute, LLC . Hypertension (high blood pressure). Accessed Sep 5, 2022. https://www.ada.org/resources/research/science-and-research-institute/oral-health-topics/hypertension
- 17.Health Literacy Universal Precautions Toolkit, 2nd ed . Plan-Do-Study-Act (PDSA) directions and examples. Last reviewed Sep 2020. Accessed Sep 5, 2022. https://www.ahrq.gov/health-literacy/improve/precautions/tool2b.html
- 18.American Institutes for Research . TeamSTEPPS® Teamwork Perceptions Questionnaire Manual. Agency for Healthcare Research and Quality; 2010. [Google Scholar]
- 19.Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277-1288. 10.1177/1049732305276687 [DOI] [PubMed] [Google Scholar]
- 20.Nasseh K, Greenberg B, Vujicic M, Glick M. The effect of chairside chronic disease screenings by oral health professionals on health care costs. Am J Public Health. 2014;104(4):744-750. 10.2105/AJPH.2013.301644 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Vernon LT, Teng KA, Kaelber DC, Heintschel GP, Nelson S. Time to integrate oral health screening into medicine? A survey of primary care providers of older adults and an evidence-based rationale for integration. Gerodontology. 2022;39(3):231-240. 10.1111/ger.12561 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.dela Cruz GG, Rozier RG, Slade G. Dental screening and referral of young children by pediatric primary care providers. Pediatrics. 2004;114(5):e642-e652. 10.1542/peds.2004-1269 [DOI] [PubMed] [Google Scholar]
- 23.Slade GD, Rozier RG, Zeldin LP, Margolis PA. Training pediatric health care providers in prevention of dental decay: results from a randomized controlled trial. BMC Health Serv Res. 2007;7:176. 10.1186/1472-6963-7-176 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Epstein JB, Gorsky M, Cabay RJ, Day T, Gonsalves W. Screening for and diagnosis of oral premalignant lesions and oropharyngeal squamous cell carcinoma: role of primary care physicians. Can Fam Physician. 2008;54(6):870-875. [PMC free article] [PubMed] [Google Scholar]
- 25.American College of Emergency Physicians . Things you can do on your own - Epic. Published Jan 4, 2021. Accessed Dec 28, 2022. https://www.acep.org/administration/quality/health-information-technology/epic-articles/things-you-can-do-on-your-own-epic/
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.