

Abstract
Aims and objectives
To determine the differences between type 1 diabetic children and healthy children regarding oral hygiene, gingival and periodontal health, and permanent teeth eruption.
Materials and methods: A case-control study was conducted on 80 children (40 type 1 diabetic children and 40 healthy children) aged 6–12-year-old. The groups were further divided into subgroups (early and late mixed dentition). All study aspects were examined clinically using the simplified oral hygiene index, Löe and Silness gingival index, clinical attachment loss (CAL), and Logan and Kronfeld stages for tooth eruption. The data were analyzed using Fisher's exact test, chi-squared test, and logistic regression models. A p-value of ≤0.05 was the threshold for statistical significance.
Results
No significant difference was found between diabetic and healthy children regarding oral hygiene and gingival health. Most children had poor oral hygiene (52.5% in the case group and 60% in the control group), with fair gingival health (70% in the case group and 55% in the control group). Diabetic children had significantly (p = 0.05) more periodontitis than healthy children. Teeth in the advanced stage of the eruption were significantly higher in diabetic than control subjects (p = 0.048 in stage V and p = 0.003 in stage VI). Older diabetic children in late mixed dentition exhibited accelerated eruption.
Conclusion
Periodontitis was significantly more common in diabetic than in healthy children. The advanced stage of the eruption was significantly higher in diabetic than in control subjects.
Clinical significance
Type 1 diabetic children had more periodontal disease and advanced stage of permanent teeth eruption compared to healthy children. Therefore, periodic dental evaluation and a strong preventive plan for diabetic children is crucial.
How to cite this article
Mandura RA, El Meligy OA, Attar MH, et al. Assessment of Oral Hygiene, Gingival, and Periodontal Health, and Teeth Eruption among Type 1 Diabetic Saudi Children. Int J Clin Pediatr Dent 2022;15(6):711-716.
Keywords: Case-control study, Children, Dental health, Diabetes mellitus, Periodontal health, Tooth eruption
Introduction
Juvenile diabetes or insulin-dependent diabetes, now called type 1 diabetes mellitus, is defined as a chronic autoimmune disorder. It is highly dependent on insulin secretion that results from improper and dysfunctional pancreatic ß cells that are responsible for insulin hormone production.1 Previously, type 1 diabetes was considered the disease of young children and teens strictly, but many studies have shown that it is a disease that can occur later in life. Polydipsia, polyphagia, polyuria, and the use of external insulin lifelong are now considered strong indicators of type 1 diabetes mellitus.2
Type 1 diabetes incidence is increasing worldwide, and the World Health Organization (WHO) estimates that the number of diabetic individuals will be doubled by the year 2030.3 Furthermore, type 1 diabetes mellitus is a very popular disease in Arab regions, especially in Gulf countries, particularly in Kuwait and Saudi Arabia.4,5 International Diabetes Federation documented that Saudi Arabia is considered as one of the top ten countries that have the highest incidence and prevalence of type 1 diabetes.
Diabetes has a negative effect on organs and tissues that are rich in blood vessels, such as kidneys, eyes, and nerves.6 The oral cavity is no exception since it is covered with epithelial tissues which are affluent with small blood vessels. Multiple studies reported that there are different oral signs and symptoms that might correlate with diabetes mellitus, such as dental caries, gingival and periodontal diseases, decrease in salivary flow rate, and alteration in teeth eruption. In addition, other conditions, including oral lesions such as candidiasis, oral lichen planus, burning mouth sensation, taste alteration, geographic and fissured tongue, and impaired wound healing, were also reported.7,8 On the other hand, other articles contradict this fact.9–11
The purpose of the study was to determine the differences between type 1 diabetic children and healthy children regarding oral hygiene, gingival health, periodontal health, and permanent teeth eruption.
Materials and Methods
Study Design
This is a nonexperimental case-control study that took place at King Abdul Aziz University Faculty of Dentistry (KAUFD), University Dental Hospital, Jeddah, Saudi Arabia.
Ethical Approval
Ethical approval was obtained from the Research Ethics Committee of the Faculty of Dentistry (approval no. 115-07-19) and the Unit of Biomedical Committee of the Faculty of Medicine (registration no. HA-02-J-008) at KAU, Jeddah, Saudi Arabia. All the study aspects were explained to the patients and parents. A written consent form was obtained from the parents and an assent form was obtained from the children.
Sample Size Calculation
Sample size calculation was done using G*Power version 3.1. A sample size of 37 patients and 37 controls were the total numbers of patients required to achieve a statistical power of 85%. The estimated sample size was rounded to 40 patients and 40 controls.
Study Population
A total of 80 children were enrolled in the study in the age range from 6 to 12 years. A total of 40 diabetic children were randomly collected from the Department of Endocrinology at KAU (case group), and 40 healthy control children were randomly recruited from dental clinics at KAUFD (control group), which were matched with the case group in age, gender, and nationality. Thereafter, subgrouping for both groups was done according to the dentition, that is, early and late mixed dentition, to examine teeth shedding and eruption. Accordingly, early and late mixed dentition were in the age ranges from 6 to 9 years and from 10 to 12 years, respectively. Dental examinations for both groups took place at KAU dental clinics. Children in both groups were excluded when they were non-Saudi, who were taking any medication that affected oral flora or inflammatory response in the previous 3 months, and who underwent orthodontic treatment. Adding to that, diabetic children were excluded when they were diagnosed with type 1 diabetes mellitus in <3 years and when they had any other medical conditions in addition to diabetes mellitus.
Clinical Examination
All patients and their parents responded to the questions regarding medical and dental history. After that, an oral examination was done by one postgraduate pediatric dentistry resident.
Soft Tissue Health
Oral soft tissues (labial and buccal mucosa, gingiva, hard and soft palate, tongue, and floor of the mouth) clinical examination was done to detect any disease or abnormal condition.
Oral Hygiene Examination
Oral hygiene index-Simplified12 was used to assess the amount of plaque and calculus accumulation for all children. The tooth was excluded if it was covered with a crown or if the surface to be examined was lost. Children who had plaque only were categorized into three groups which are good when the score was between 0.0 and 0.6, fair when the score was between 0.7 and 1.2, or poor when the score was between 1.3 and 6.0. On the contrary, children who had plaque and calculus also had three categories (good, fair, and poor) but with different scores, which are 0.0–1.2, 1.3–3.0, and 3.1–6.0, respectively.13 For young children who did not have permanent teeth, primary teeth were examined instead.14
Gingivitis and Periodontitis Detection
Löe and Silness gingival index15,16 was used to investigate the presence and severity of the gingival health using the WHO periodontal probe. Gingival health index was divided into four categories (excellent, <0.1; good, 0.1–1.0; fair, 1.1–2.0; and poor, 2.1–3).13 For young children who did not have permanent teeth, primary teeth were examined instead.17
Periodontal health was evaluated by the presence or absence of CAL. The child was considered to have periodontitis when two nonadjacent teeth had at least one site with CAL >1.5 mm.18
Teeth Eruption
Permanent teeth eruption of diabetic children to healthy children was compared according to Logan and Kronfeld19 as shown in Table 1.
Table 1.
Stages of teeth eruption
| Stage I | Unerupted successor tooth and presence of predecessor's tooth |
| Stage II | Unerupted successor tooth and predecessor's tooth are about to exfoliate (mobile) |
| Stage III | Unerupted successor tooth and predecessor's tooth had exfoliated |
| Stage IV | Only the cusp tip of the successor's tooth is present in the oral cavity |
| Stage V | More than the cusp tip of the successor's tooth is present in the oral cavity, but it still does not reach the occlusal plane |
| Stage VI | Successor's tooth fully erupts |
Statistical Analysis
Univariate analysis was performed using Fisher's exact and chi-squared tests for categorical variables. The statistical analysis was performed using (GraphPad Prism version. 9.0.0.0 for Mac operating system X; GraphPad Software, California, United States of America). The tooth eruption stage was classified from stages I to VI. The dichotomization of the eruption stages into five versions was done. Logistic regression models were used for each version to compare case patients and control subjects using Stata version 23 (Stata Corp LP, College Station, Texas, United States of America). A generalized estimating equation method was used to accommodate for correlations between teeth for the same participant. The analysis was adjusted for age, gender, and nationality. For all the tests, a p-value of ≤0.05 was the threshold for statistical significance.
Results
Age and Gender Distribution
The final sample size was 80 children (40 type 1 diabetic children and 40 healthy children) in the age range from 6 to 12 years. The mean age for the diabetic group was 9.8 ± 1.9 years, while the mean age for the healthy control group was 9.6 ± 1.7 years.
Soft Tissue Health
Based on our sample, there was no significant difference between diabetic and healthy children and youths in oral soft tissue findings. Only one child with type 1 diabetes had gingival hyperplasia (2.5%).
Oral Hygiene
The present study showed that most of the sample population had poor oral hygiene, with 52.5% in the case group and 60% in the control group, but the difference was not statistically significant (p = 0.6). On the contrary, there was a borderline significant difference between diabetic and healthy children in the category of good oral hygiene (p = 0.05). Around 12.5% of healthy individuals had good oral hygiene, while good oral hygiene was found in 0% of the diabetic group.
Moreover, A significant association was found between gender and oral hygiene among diabetic patients (p = 0.03). Most of the diabetic male patients had poor oral hygiene (72.2%), while most of the diabetic female patients had fair oral hygiene (63.6%).
Gingival and Periodontal Health
According to Löe and Silness gingival index, this study showed that fair gingival health was the most common category in diabetic and healthy groups, without a significant difference between them (Fig. 1).
Fig. 1.
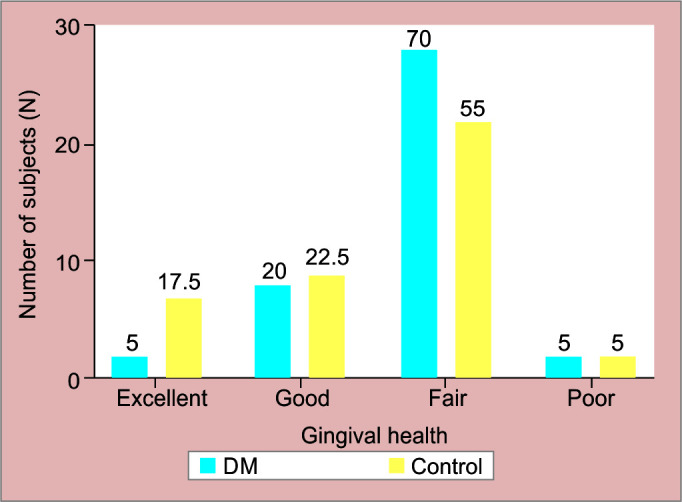
Bar graph for gingival health among the study group
Periodontal health was assessed based on CAL. The present study showed a borderline significant difference in the presence of periodontitis between diabetic and healthy groups (p = 0.05). The presence of periodontitis was noticed more among diabetic children than healthy children (Fig. 2). Around 75% of diabetic patients who were enrolled in this study were classified as having uncontrolled diabetes disease (hemoglobin A1c ≥ 8%). According to that, we could not test the difference in the presence of periodontitis between controlled and uncontrolled diabetic patients.
Fig. 2.
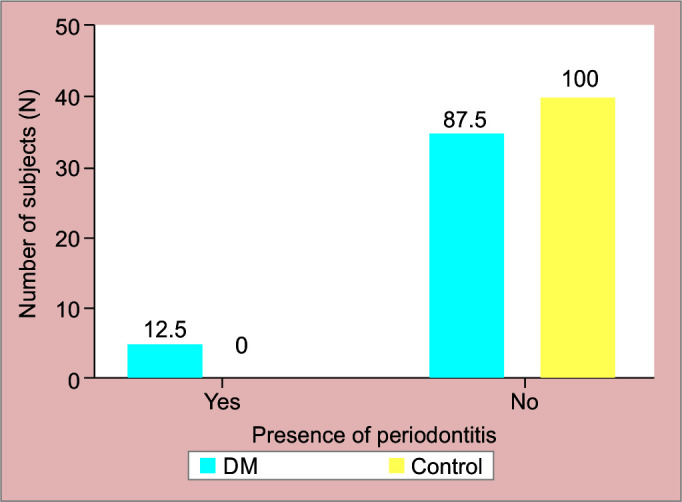
Presence of periodontitis among study groups
Furthermore, no significant gender difference was found in gingival or periodontal health among the diabetic group.
Teeth Eruption
Logistic regression showed that the odds of a tooth being in the advanced stage of the eruption was significantly higher in diabetic patients than in control subjects, suggesting that accelerated tooth eruption occurs among diabetic patients. The difference is statistically significant in stages V and VI (Fig. 3).
Fig. 3.
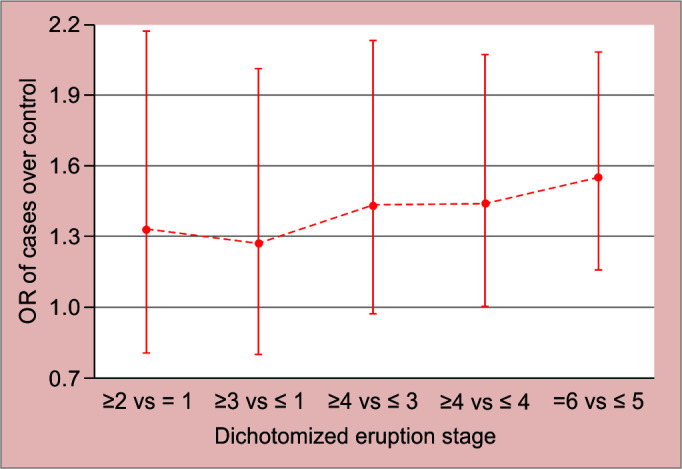
Odds ratio of cases over controls for different versions of dichotomized eruption status
A separate analysis was done for the two subgroups; early mixed dentition (6–9-year-old) and late mixed dentition (10–12-year-old); results showed older diabetic children in the late mixed dentition exhibited accelerated eruption but not the younger diabetic children in the early mixed dentition group when compared to healthy subjects of same age group (Table 2).
Table 2.
Odds ratio of case patients over control subjects’ versions of dichotomized eruption status according to dentition stage
| Dichotomized eruption status | Dentition period | OR (95% CI) * | p-value |
|---|---|---|---|
| Stage ≥ II vs I | Early | 1.05 (0.623–1.78) | 0.84 |
| Late | 1.86 (0.78–4.40) | 0.15 | |
| Stage ≥ III vs II | Early | 0.95 (0.60–1.51) | 0.84 |
| Late | 1.88 (0.84–4.18) | 0.11 | |
| Stage ≥ IV vs III | Early | 0.96 (1.87–3.23) | 0.88 |
| Late | 2.25 (1.21–4.18) | 0.01 | |
| Stage ≥ V vs IV | Early | 0.97 (0.63–1.51) | 0.91 |
| Late | 2.11 (1.22–3.61) | 0.007 | |
| Stage ≥ VI vs V | Early | 0.97 (0.635–1.50) | 0.91 |
| Late | 2.19 (1.53–3.14) | 0.001 |
*From generalized equation logistic regression model fit, controlled for age, gender, and nationality; CI: confidence interval; OR: odds ratio
Furthermore, in the early mixed dentition group, the odds of a tooth being in the advanced eruptive stage were significantly lower in female diabetic patients than in male diabetic patients (odds ratio = 0.73 and p = 0.03). However, in the late mixed dentition group, the odds of a tooth being in an advanced eruptive stage were significantly higher in female diabetic patients compared to male diabetic subjects (odds ratio = 1.34 and p = 0.014).
There was an association between gingivitis and accelerated tooth eruption in both early and late mixed dentition groups in diabetic patients (odds ratio = 1.11, p = 0.001, odds ratio = 1.09, and p = 0.014), respectively.
Discussion
Insulin is a polypeptide hormone consisting of two amino acid chains attached with disulfide linkage.20 Normally, in response to increased glucose concentration in the blood, ß cells secrete insulin hormone, which targets insulin receptors present on specific cells for signal transduction. This will lead to a cascade of events, which will stimulate the cells to bind glucose transport proteins into its membrane, which results in decreasing the glucose level in the blood. As the blood glucose level normalizes, ß cells inhibit themselves from secreting more insulin or decrease cells’ sensitivity to insulin.21
Type 1 diabetes mellitus is considered one of the most common diseases in the region. Many studies predict that the incidence of the disease will continue to increase in the future. Although the disease has a long history and a tremendous amount of research, there is a lack of knowledge regarding the effect of type 1 diabetes mellitus on oral health in children specifically.
According to our knowledge, there is a lack of studies clinically examining the presence of oral candidiasis and other oral mucosal lesions in type 1 diabetic children. Most of the previous studies have been done on adult individuals who have diabetes (type 1 or 2). Many studies reported that fungal infections are considered common conditions that can be observed and detected in diabetic adult individuals compared to nondiabetic people.22 On the contrary, other studies contradict these results.23–25 According to our study, we did not observe any child from both groups suffering from oral candidiasis or any other oral soft tissue diseases. Only 1 diabetic subject had oral soft tissue changes, which were generalized gingival inflammation and hyperplasia. This result might be influenced by our small sample size. Subsequently, conducting further studies to explore the effect of type 1 diabetes on oral health among children is crucial.
Regarding oral hygiene and gingival health, our results align with Wyne et al. results which showed that there was no significant difference between healthy and diabetic children in terms of gingival health status.11 In contrast, Ferizi et al. study showed the opposite result.26 This can be attributed to prolonged disease periods which can increase the severity of gingivitis due to the high amount of glucose present in the composition of saliva and gingival crevicular fluid, which can facilitate plaque growth and accumulation.27 In addition, Aren et al. stated that there is a strong relationship between the level of glucose in the blood and gingival health.28
Furthermore, periodontal disease is not confined to adult patients, it can present in young and adolescent diabetic patients, as reported in the current study, but it increases with age and during puberty due to changes in metabolic control.29 Many studies reported that periodontitis could more commonly occur in patients who have a long duration of hyperglycemia as well as with patients who have uncontrolled diabetes.30–32 Presence of gingival inflammation in diabetic patients is more serious than if it presented in healthy individuals. Gingival inflammation among diabetic subjects is more prone to progress into periodontitis.33 Accordingly, periodic dental follow-up and early treatment of gingivitis or periodontitis in diabetic subjects are considered a crucial part of their dental care schedules.
Alteration in teeth eruption sequence, as well as acceleration or delay in teeth eruption, can cause disturbance in occlusion. Diabetes mellitus is one of the metabolic diseases that might affect teeth eruption among children. Generally, the reason for accelerated or delayed teeth eruption is not clear. However, it has been shown that several factors might have an influence on teeth eruption, which are: molecular signaling to osteoclastic activity, development of the root, diet, and hormonal effect.34,35 In the present study, we found that diabetic patients had accelerated teeth eruption in comparison to the healthy group. This finding goes parallel with the study done in 2008.36 Lal et al. found that children who were in late mixed dentition had accelerated teeth eruption, while this acceleration was not noticed in early mixed dentition,36 which also goes in line with our results. On the contrary, other studies illustrated dissimilar results.37,38 Orbak et al. concluded that diabetic patients in an age range from 5 to 9 years had accelerated dental development, while retarded teeth development was noticed in an age range from 10 to 14 years. We observed that the methodology used in our study varies from Orbak et al. methodology.37 Other studies concluded that diabetic children and youths younger than 11 years and 6 months had teeth eruption acceleration in comparison to healthy children and adolescents, while the contradictory result was found in diabetic patients who were older than 11 years and 6 months. The explanation of this result is that diabetes can accelerate teeth eruption at young age and delay eruption at the prepubertal and pubertal stages, which could be due to the effect of the pituitary gland. At the early stages of the disease, the pituitary gland spur causes acceleration. Afterward, with the long duration of the disease, the pituitary gland reaches a stage of exhaustion, causing the delay.38
Furthermore, in the present study, there was an association between gingivitis and accelerated teeth eruption in diabetic children. The reason for this relationship could be due to the high inflammatory response that causes a local change in the bone surrounding the tooth, leading to a decrease in the amount and quality of the surrounding bone.36
One of the main limitations of this study is the small sample size. Accordingly, we could not test the association between periodontitis and increased age. Adding to that, only one child with diabetes had oral soft tissue lesions, which also could be affected by the small sample size. Most diabetic patients who were enrolled in this study were classified as having uncontrolled diabetes disease. Accordingly, we could not test the difference in the presence of periodontitis between controlled and uncontrolled diabetic patients.
To have a better understanding of the oral health status of type 1 diabetic children which can help to formulate an adequate preventive program, there is a demand to conduct prospective studies (cohort studies) on a larger sample size with different geographic locations to reach into the cause-and-effect relationship between type 1 diabetes and oral findings.
Conclusion
Based on this study's results, the following conclusions can be made:
No significant difference between type 1 diabetic children and healthy children regarding oral hygiene and gingival health.
A borderline significant difference was found between the two groups in the presence of periodontitis. Diabetic children had more periodontal inflammation than healthy children.
The advanced stage of the eruption was significantly higher in diabetic patients than in control subjects. Older diabetic children in the late mixed dentition exhibited accelerated eruption but not the younger diabetic children in the early mixed dentition group when compared to healthy subjects of the same age group.
Further prospective studies (cohort studies) on a larger sample size with different geographic locations are encouraged.
Clinical Significance
Most type 1 diabetic children, youths, and their parents are unaware of the effect and complications of diabetes mellitus on the oral soft tissues and dental health. Dental health practitioners have the responsibility to educate those patients and their parents about the relationship between diabetes disease and oral health. Diabetic patients need to have a strong dental preventive plan, as well as a comprehensive treatment plan and follow-up in order to reduce oral complications.
Acknowledgment
The authors wish to thank Dr Hanaa Khalil Allaf for her valuable contribution to the data collection part.
Footnotes
Source of support: Nil
Conflict of interest: None
References
- 1.American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014;37(Suppl 1):S81–S90. doi: 10.2337/dc14-S081. [DOI] [PubMed] [Google Scholar]
- 2.Atkinson MA, Eisenbarth GS, Michels AW. Type 1 diabetes. Lancet. 2014;383(9911):69–82. doi: 10.1016/S0140-6736(13)60591-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Canadian Diabetes Association Clinical Practice Guidelines Expert Committee, Goldenberg R, Punthakee Z. Definition, classification and diagnosis of diabetes, prediabetes and metabolic syndrome. Can J Diabetes. 2013;37(Suppl 1):S8–S11. doi: 10.1016/j.jcjd.2013.01.011. [DOI] [PubMed] [Google Scholar]
- 4.Cherian MP, Al-Kanani KA, Al Qahtani SS, et al. The rising incidence of type 1 diabetes mellitus and the role of environmental factors–three decade experience in a primary care health center in Saudi Arabia. J Pediatr Endocrinol Metab. 2010;23(7):685–695. doi: 10.1515/jpem.2010.23.7.685. [DOI] [PubMed] [Google Scholar]
- 5.LaPorte RE, Tuomilehto J, King H. WHO multinational project for childhood diabetes. Diabetes Care. 1990;13(10):1062–1068. doi: 10.2337/diacare.13.10.1062. [DOI] [PubMed] [Google Scholar]
- 6.Rask-Madsen C, King GL. Vascular complications of diabetes: mechanisms of injury and protective factors. Cell Metab. 2013;17(1):20–33. doi: 10.1016/j.cmet.2012.11.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ship JA. Diabetes and oral health: an overview. J Am Dent Assoc. 2003;134(Spec No):4S–10S. doi: 10.14219/jada.archive.2003.0367. [DOI] [PubMed] [Google Scholar]
- 8.Adler P, Wegner H, Bohatka L. Influence of age and duration of diabetes on dental development in diabetic children. J Dent Res. 1973;52(3):535–537. doi: 10.1177/00220345730520032601. [DOI] [PubMed] [Google Scholar]
- 9.Bremenkamp RM, Caris AR, Jorge AO, et al. Prevalence and antifungal resistance profile of Candida spp. oral isolates from patients with type 1 and 2 diabetes mellitus. Arch Oral Biol. 2011;56(6):549–555. doi: 10.1016/j.archoralbio.2010.11.018. [DOI] [PubMed] [Google Scholar]
- 10.Edblad E, Lundin SA, Sjödin B, et al. Caries and salivary status in young adults with type 1 diabetes. Swed Dent J. 2001;25(2):53–60. [PubMed] [Google Scholar]
- 11.Wyne AH, Chohan AN, Al-sharari R. Caries, oral hygiene and gingival health status in type I diabetic Saudi children. Pakistan Oral Dent J. 2016;36(3):421–426. [Google Scholar]
- 12.Greene JG, VermilIion JR. The simplified oral hygiene index. J Am Dent Assoc. 1964;68(1):7–13. doi: 10.14219/jada.archive.1964.0034. [DOI] [PubMed] [Google Scholar]
- 13.Marwah Nikhil. Textbook of pediatric dentistry. 3rd ed. Vol. 53. New Delhi: Jaypee Brothers Medical Pub; 2013. pp. 1689–1699. p. [Google Scholar]
- 14.Rodrigues CR, Ando T, Guimarães LO. Simplified oral hygiene index for ages 4 to 6 and 7 to 10 (deciduous and mixed dentition). Rev Odontol Univ Sao Paulo. 1990;4(1):20–24. [PubMed] [Google Scholar]
- 15.Löe H. The gingival index, the plaque index and the retention index systems. J Periodontol. 1967;38(6):610–616. doi: 10.1902/jop.1967.38.6.610. [DOI] [PubMed] [Google Scholar]
- 16.Poulsen S. Epidemiology and indices of gingival and periodontal disease. Pediatr Dent. 1981;3(Special issue):82–88. [Google Scholar]
- 17.Rodrigues CR, Ando T, Guimarães LO. Simplified gingival index for ages 4 to 6 and 7 to 10. (Deciduous and mixed dentition). Rev Odontol Univ Sao Paulo. 1989;3(3):414–419. [PubMed] [Google Scholar]
- 18.Genco RJ, Grossi SG, Ho A, et al. A proposed model linking inflammation to obesity, diabetes, and periodontal infections. J Periodontol. 2005;76(11 Suppl):2075–2084. doi: 10.1902/jop.2005.76.11-S.2075. [DOI] [PubMed] [Google Scholar]
- 19.Loganc WHG, Kronfeld R. Development of the human jaws and surrounding structures from birth to the age of fifteen years. J Am Dent Assoc. 1933;20(3):379–427. doi: 10.14219/jada.archive.1933.0080. [DOI] [Google Scholar]
- 20.Steiner DF, Chan SJ, Welsh JM, et al. Structure and evolution of the insulin gene. Annu Rev Genet. 1985;19(1):463–484. doi: 10.1146/annurev.ge.19.120185.002335. [DOI] [PubMed] [Google Scholar]
- 21.Qaid MM, Abdelrahman MM. Role of insulin and other related hormones in energy metabolism—a review. Cogent Food Agric. 2016;2(1):1267691. [Google Scholar]
- 22.Obradović RR, Kesić GL, Pejčić AN, et al. Diabetes mellitus and oral candidiasis. Acta Stomatol Naissi. 2011;27(63):1025–1034. doi: 10.5937/asn1163025O. [DOI] [Google Scholar]
- 23.Gupta S, Koirala J, Khardori R, et al. Infections in diabetes mellitus and hyperglycemia. Infect Dis Clin North Am. 2007;21(3):617–638. doi: 10.1016/j.idc.2007.07.003. [DOI] [PubMed] [Google Scholar]
- 24.Khovidhunkit SO, Suwantuntula T, Thaweboon S, et al. Xerostomia, hyposalivation, and oral microbiota in type 2 diabetic patients: a preliminary study. J Med Assoc Thai. 2009;92(9):1220–1228. [PubMed] [Google Scholar]
- 25.Muzyka BC, Glick M. A review of oral fungal infections and appropriate therapy. J Am Dent Assoc. 1995;126(1):63–72. doi: 10.14219/jada.archive.1995.0025. [DOI] [PubMed] [Google Scholar]
- 26.Ferizi L, Dragidella F, Spahiu L, et al. Oral health and salivary status in children with type 1 diabetes mellitus. J Int Dent Med Res. 2018;11(3):931–937. [Google Scholar]
- 27.Hugoson A, Thorstensson H, Falk H, et al. Periodontal conditions in insulin-dependent diabetics. J Clin Periodontol. 1989;16(4):215–223. doi: 10.1111/j.1600-051x.1989.tb01644.x. [DOI] [PubMed] [Google Scholar]
- 28.Aren G, Sepet E, Ozdemir D, et al. Periodontal health, salivary status, and metabolic control in children with type 1 diabetes mellitus. J Periodontol. 2003;74(12):1789–1795. doi: 10.1902/jop.2003.74.12.1789. [DOI] [PubMed] [Google Scholar]
- 29.Lalla E, Cheng B, Lal S, et al. Periodontal changes in children and adolescents with diabetes: a case-control study. Diabetes Care. 2006;29(2):295–299. doi: 10.2337/diacare.29.02.06.dc05-1355. [DOI] [PubMed] [Google Scholar]
- 30.Oliver RC, Tervonen T. Diabetes-a risk factor for periodontitis in adults? J Periodontol. 1994;65(Suppl 5S):530–538. doi: 10.1902/jop.1994.65.5s.530. [DOI] [PubMed] [Google Scholar]
- 31.Seppälä B, Seppälä M, Ainamo J. A longitudinal study on insulin-dependent diabetes mellitus and periodontal disease. J Clin Periodontol. 1993;20(3):161–165. doi: 10.1111/j.1600-051x.1993.tb00338.x. [DOI] [PubMed] [Google Scholar]
- 32.Tervonen T, Oliver RC. Long-term control of diabetes mellitus and periodontitis. J Clin Periodontol. 1993;20(6):431–435. doi: 10.1111/j.1600-051x.1993.tb00384.x. [DOI] [PubMed] [Google Scholar]
- 33.Dakovic D, Pavlovic MD. Periodontal disease in children and adolescents with type 1 diabetes in Serbia. J Periodontol. 2008;79(6):987–992. doi: 10.1902/jop.2008.070549. [DOI] [PubMed] [Google Scholar]
- 34.Shroff B, Kashner JE, Keyser JD, et al. Epidermal growth factor and epidermal growth factor-receptor expression in the mouse dental follicle during tooth eruption. Arch Oral Biol. 1996;41(6):613–617. doi: 10.1016/0003-9969(96)00147-1. [DOI] [PubMed] [Google Scholar]
- 35.Shroff B, Siegel SM. Molecular basis for tooth eruption and its clinical implications in orthodontic tooth movement. Semin Orthod. 2000;6(3):155–172. doi: 10.1053/sodo.2000.8082. [DOI] [Google Scholar]
- 36.Lal S, Cheng B, Kaplan S, et al. Accelerated tooth eruption in children with diabetes mellitus. Pediatrics. 2008;121(5):e1139–1143. doi: 10.1542/peds.2007-1486. [DOI] [PubMed] [Google Scholar]
- 37.Orbak R, Simsek S, Orbak Z, et al. The influence of type-1 diabetes mellitus on dentition and oral health in children and adolescents. Yonsei Med J. 2008;49(3):357–365. doi: 10.3349/ymj.2008.49.3.357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Bohátka L, Wegner H, Adler P. Parameters of the mixed dentition in diabetic children. J Dent Res. 1973;52(1):131–135. doi: 10.1177/00220345730520010601. [DOI] [PubMed] [Google Scholar]