

Abstract
Mental health is an important component of public health, especially in times of crisis. However, monitoring public mental health is difficult, because data are often patchy and low-frequency. As a complement to established approaches, we turn to data from helplines. Helpline calls offer a real-time measure of ‘revealed’ distress and mental health concerns across a range of topics. We have collected data on 7 million calls from 19 countries, focusing on the COVID-19 crisis. We find that call volumes peaked six weeks after the initial outbreak, at 35% above pre-pandemic levels. The increase was mainly driven by fear (including fear of infection), loneliness, and, later in the pandemic, physical-health concerns. Relationship issues, economic problems, violence, and suicidal ideation, however, were less prevalent than before the pandemic. This pattern is apparent both during the first wave and during subsequent COVID-19 waves. Issues directly tied to the pandemic therefore seem to have substituted rather than exacerbated underlying anxieties. Conditional on infection rates, suicide-related calls increased when containment policies became more stringent and decreased when income support was extended. This implies that financial relief can allay the distress triggered by lockdown measures and illustrates the insights that can be gleaned from a statistical analysis of helpline data.
The state of population mental health is hard to measure. This could lead to policymakers neglecting mental health issues relative to aspects that can be measured more easily – especially during fast-moving crisis situations1–3.
We propose helpline data as a real-time information source on the state of public mental health. Helpline data have two main advantages. First, helpline calls can be considered as a manifestation of revealed distress and mental health concerns. Callers incur the mental and time cost of reaching out without having been prompted to do so. Therefore, helpline calls resemble clinical data by offering a measure of mental health that is unaffected by researchers’ study design and framing. Second, information about helpline calls is digitally recorded with daily frequency and covers a wide range of conversation topics.
Telephone helplines are well-established institutions for mental health protection and suicide prevention in many countries, and they offer support immediately, anonymously, cheaply, and accessibly4–6. Some helplines specialize on particular issues such as suicide, children, or violence against women. Suicide helplines, for example, have been shown to reduce suicide rates7, and calls to suicide helplines have been shown to relate to the incidence of actual suicides8.
In an application to the COVID-19 crisis, we document the growth and composition of helpline calls as well as their pandemic-related determinants. Helplines take on particular relevance in a pandemic, when face-to-face contacts carry infection risks and may even be impossible due stay-at-home orders9–14. We have collected data from 23 helplines in 14 European countries, the United States, China, Hong Kong, Israel, and Lebanon. The total dataset covers some 7 million individual calls made between 2019 and early 2021. Full details are provided in the Supplementary Information.
We find that call volumes peaked six weeks after the initial outbreak, at 35% above pre-pandemic levels. The increase was mainly driven by fear (including fear of infection), loneliness, and, later in the pandemic, physical-health concerns. Relationship issues, economic problems, violence, and suicidal ideation, however, were less prevalent than before the pandemic. This pattern is apparent both during the first wave and during subsequent COVID-19 waves. Issues directly tied to the pandemic therefore seem to have substituted rather than exacerbated underlying anxieties.
The panel structure of the data allows us to exploit differences in the timing of local infection waves and policy measures to isolate their separate effects on helpline calls. This is a first-order issue for policymakers, as interventions designed to contain infections might also affect mental health, by exacerbating unemployment, financial stress, loneliness, relationship problems, and pre-existing mental vulnerabilities. Those are in turn well-recognized risk factors for suicide15–22. We find that, conditional on infection rates, suicide-related calls increased when containment policies became more stringent and decreased when income support was extended.
We consider the analysis of helpline calls as a complement, not a substitute, to established approaches, such as survey evidence23–26 or suicide statistics27–29. Mental health surveys and suicide statistics are highly informative, but they tend to be low-frequency and available with a lag. Higher-frequency monitoring has been performed in the context of the COVID-19 pandemic based on online searches as recorded by Google Trends30–33, by tracking visits to emergency departments34,35, and by monitoring calls to the police for help with domestic disputes36–38. In line with our findings, the available evidence based on such indicators suggests that the COVID-19 pandemic has had significant deleterious effects on public mental health.
Results
Elevated call volumes across helplines.
When we pool and size-weight the data for our 21 sample helplines, we observe a peak call volume, reached six weeks after the outbreak of the pandemic, that exceeds the pre-pandemic level by 35% (95% CI: 22.6 to 48.3%; see Fig. 1). With the country-specific outbreak defined as the date when more than one SARS-CoV-2 infection per 100,000 inhabitants was recorded (Fig. 1a), we see a significant increase for the first time in week 3, peaking in week 6 at around 35%, gradually decreasing back towards pre-pandemic levels by around week 11. When we instead define the starting point of the pandemic as the entry into force of the first shelter-in-place (SIP) order (Fig. 1b), we observe a significant increase for the first time in week 2, reaching a steady peak level during weeks 3–8, and decreasing thereafter. The different time profiles are mainly explained by the fact that SIP orders on average were issued some 2 to 3 weeks after local outbreaks (see Extended Data Table 1 and Extended Data Fig. 1).
Fig. 1: Evolution of total helpline call numbers during the first wave.
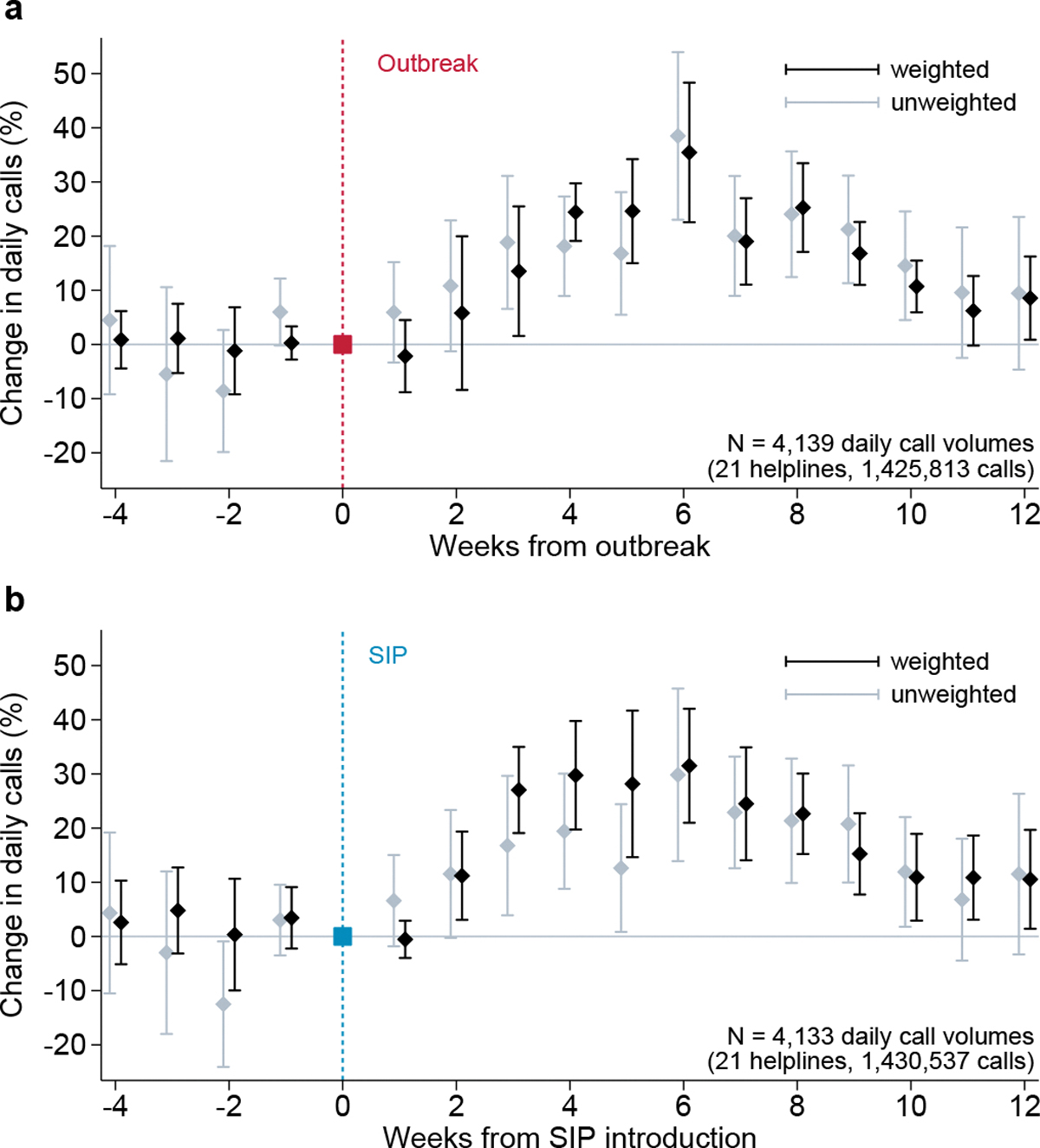
Estimated coefficients on week indicators with 95% confidence intervals. The dependent variable is ln(helpline calls+1). The sample includes daily data for 21 helplines during the period from 4 weeks before to 12 weeks after the event date in early 2020, and, for 17 of the 21 helplines, the corresponding days of 2019. Average percentage change in call volumes relative to reference week 0. Week 0 is when, a, the cumulative number of SARS-CoV-2 infections exceeded 1 per 100,000 population39, or, b, shelter-in-place orders were introduced40. Results on data weighted by total number of calls recorded for each helpline during the sample period (black); and unweighted models (gray); see Methods, equation (1).
The gradual nature of the increase in call volumes could to some extent be due to capacity constraints. Several helplines initially had to leave some of the additional calls unanswered and only gradually managed to adjust capacity to the new level of demand. Because of this capacity constraint, the evolution of recorded aggregate call numbers should be interpreted as a lower-bound estimate of the true increase in the number of people who sought to call a helpline in the first wave of the pandemic. However, unanswered calls are not pre-screened, and call answering is thus a random process unrelated to the motives of the caller. Hence, our data provide representative information on the reasons for calling even if some calls were left unanswered because of capacity constraints.
Caller issues and conversation topics.
We analyze the reasons for calling, using data on 12 helplines for which we have call-level information on conversation topics and caller characteristics.
Our main results relating to call topics are presented in Fig. 2. Fig. 2a shows that most pre-COVID-19 pandemic calls were made because of relationship issues (37%), loneliness (20%) or various fears and anxieties (13%). Women made 61% of total calls, and 63% of calls were made by people aged 30–60. The breakdown by topic is fairly similar across helplines, with relationship issues being the most prevalent topic in 8 of the 10 helplines for which this category is defined (see Extended Data Fig. 2). More than 90% of “calls” are voice calls, but for some helplines our data also includes text-based (online chat) conversations. Most calls are placed by first-time or sporadic callers, both before and after the onset of the pandemic (see Extended Data Table 2).
Fig. 2: Conversation topics during the first COVID-19 wave.
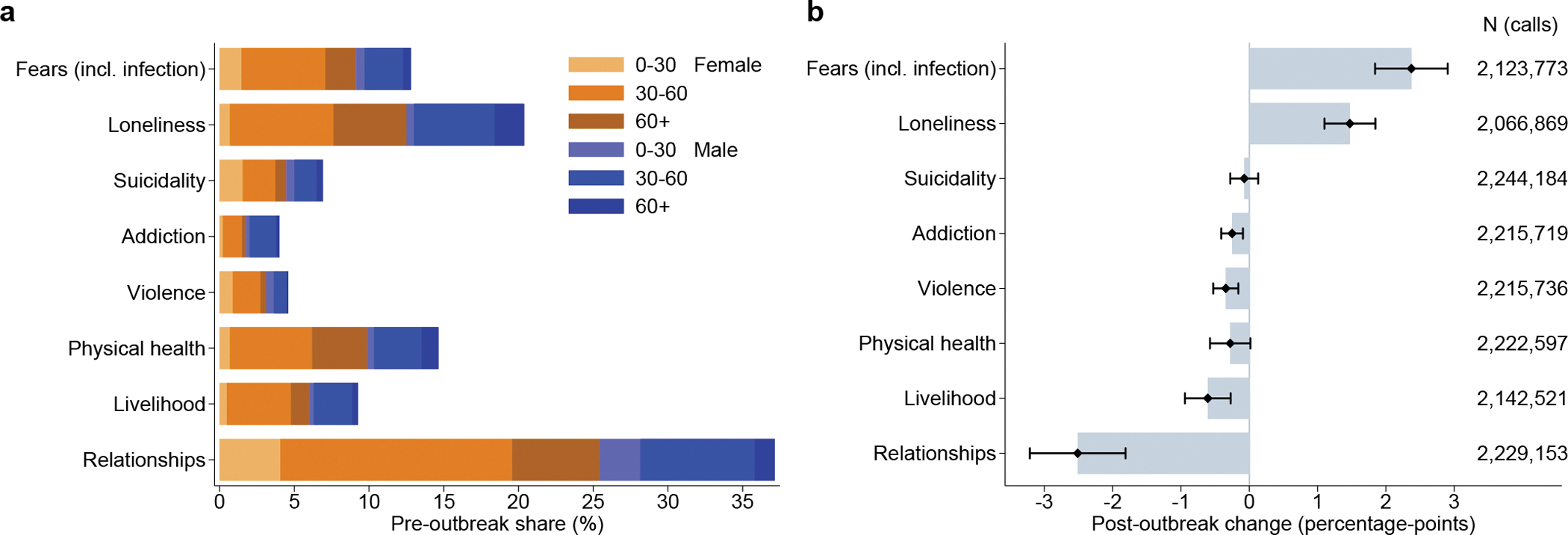
a, Pre-pandemic shares of main non-exclusive conversation topics by sex and age group, before 1/100,000 SARS-CoV-2 infections/population were recorded39. b, Estimated coefficients for binary post-outbreak indicator variable with 95% confidence intervals. Separate linear probability regression models with dependent variable set to one for calls related to the respective topic, see Methods, equation (2).
During the first wave of the pandemic, defined here as lasting until the end of June 2020, the composition of calls changed significantly (see Fig. 2b). The biggest increase in calls was recorded in the category ‘fear’ (+2.4 p.p.). This category includes calls made out of fear of infection with SARS-CoV-2. The other category of calls whose share increased during the first wave of the pandemic was ‘loneliness’ (+1.5 p.p.). The share of all other conversation topics decreased during the first wave. Statistically significant relative decreases were observed for the topics ‘relationships’ (−2.5 p.p.), ‘livelihood’ (i.e. economic worries, −0.6 p.p.), ‘violence’ (−0.3 p.p.), and addiction (−0.3 p.p.). We detect no statistically significant change in the share of calls made out of suicidal ideation. If we define a change of ≥ 5% in the volume of calls on a particular topic as a relevant change, then we can reject the hypothesis that the incidence of suicide-related calls has changed to a relevant extent during the first pandemic wave (see Extended Data Fig. 3). These results show that the first wave of the pandemic and associated lockdown measures led to a less than proportional increase in calls about domestic violence, addiction, and suicidal ideation relative to the overall increase in calls.
In Extended Data Fig. 4, we decompose post-pandemic changes in topic shares by gender and age group. Among the particularly noteworthy results, we observe that the strong increase in fear-related calls was entirely driven by the over-30s, both male and female. This is consistent with the fact that vulnerability to COVID-19 increases monotonically with age. The share of suicide-related calls fell particularly strongly for men under 30. That same category of young men stands out with an increase in the share of calls related to addiction and relationships. Conversely, an increased share of calls made by women under 30 was related to violence issues – despite the fact that it may well have been more difficult under stay-at-home orders to make helpline calls in situations of domestic violence.
For around a third of the calls underlying our analysis of Fig. 2, operators have recorded more than one conversation topic (see Extended Data Fig. 5a). The topics that most often feature jointly are ‘violence’ and ‘relationships’, and ‘livelihood’ and ‘relationships’, but combinations of all eight topics distinguished in our analyses are observed in the data (see Extended Data Fig. 5b). It turns out that that dropping multiple-topic calls from the analysis leaves results virtually unchanged (see Extended Data Fig. 5c).
Overall, our results suggest that the observed increase in helpline calls during the first wave of the COVID-19 pandemic was driven to a large extent by fears of the virus itself and by loneliness in the context of shelter-in-place orders, rather than domestic violence, addiction, or suicidal ideation.
The 2nd and 3rd COVID-19 waves.
For two of the largest helplines in our sample, Telefonseelsorge (Germany) and S.O.S. Amitié (France), we have received data up until 31 March 2021, allowing us to analyze helpline calls beyond the first wave of the pandemic. Fig. 3a and c show that call volumes increased again in the second half of 2020, in parallel with an increase in infections and a tightening of NPIs. While in Germany the volume of calls has increased continuously into early 2021, in France it fell again after a peak in December 2020. These diverging patterns correlate with stronger up- and downswings in both infections and the stringency of government measures in France compared to Germany.
Fig. 3: Helpline calls in Germany and France during the first and subsequent waves.
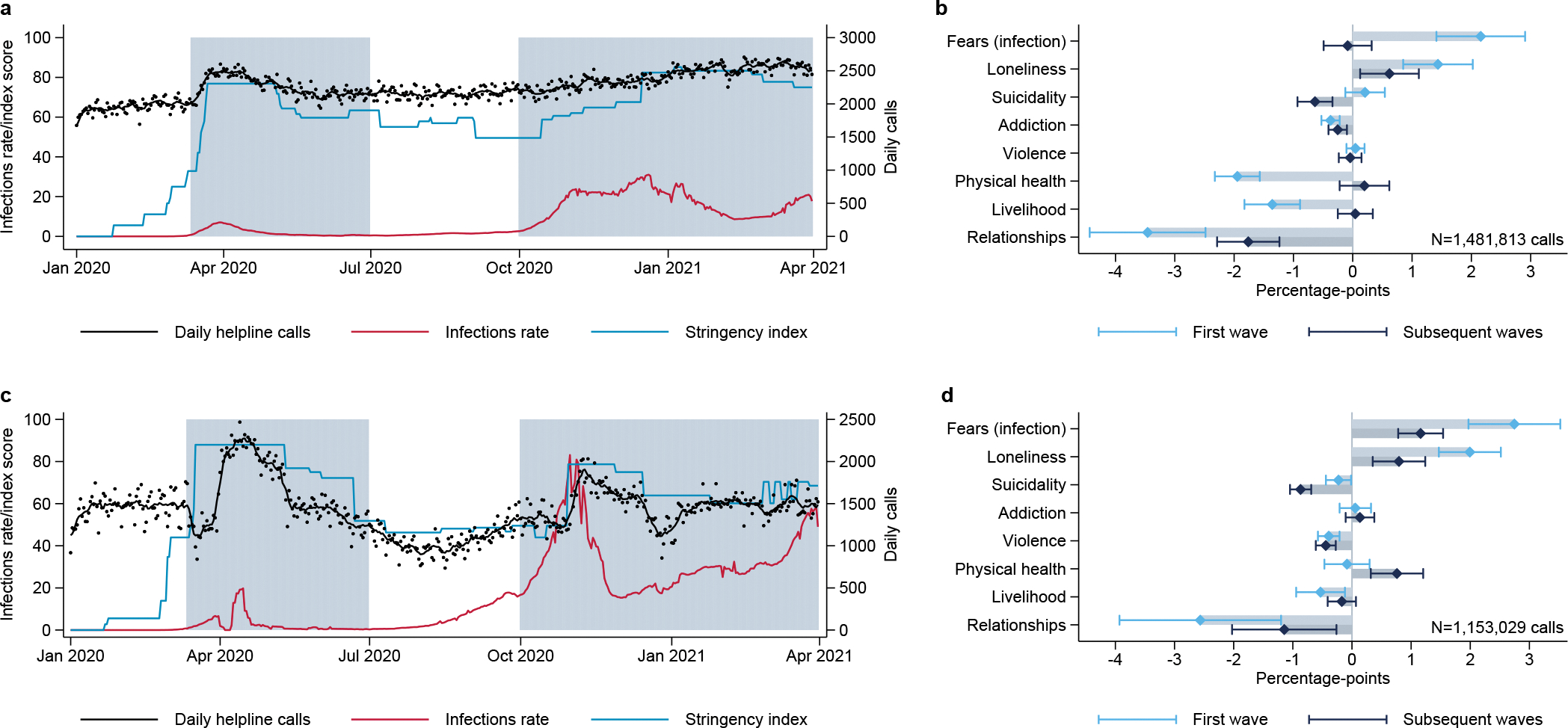
a, c, Sum of daily helpline calls with seven-day moving average in black (right axis), government response stringency index in blue40, and seven-day moving average of newly confirmed SARS-CoV-2 infections per million population and day in red (left axis)39, for a, Germany (Telefonseelsorge) and c, France (S.O.S. Amitié). Shaded areas indicate first- and subsequent-wave periods (11 March 2020–30 June 2020, and 1 October 2020–31 March 2021). b, d, Estimated coefficients for binary variables denoting the two periods, and their associated 95% confidence intervals, for b, Germany (Telefonseelsorge) and d, France (S.O.S. Amitié), based on separate linear probability regression models with dependent variable set to one for calls related to the respective topic; see Methods, equation (4).
Conversation topic patterns resemble each other both between the two countries and between the two distinguished periods of the pandemic (Fig. 3b and d). As in the first wave, fear (incl. of the fear infection) and loneliness were the conversation topics that saw their share of calls increase most, whereas the share of calls because of relationship issues decreased markedly. The share of calls related to suicide shrank further during subsequent waves. Conversely, the share of calls related to problems with physical health increased in the second/third waves. This could be related to a larger share of the population being infected with SARS-CoV-2, or to health worries because of restricted/postponed access to treatment facilities and reduced opportunities for physical activity. Similar to the first wave, additional calls focused predominantly on issues linked directly with the pandemic: fear of infection, loneliness, and – new in subsequent waves – physical health.
Infection rates and policy measures.
Helpline call data allow us to use panel data regression to isolate partial correlations between policy measures and indicators of mental health. A particularly informative empirical laboratory for this analysis are calls to the National Suicide Prevention Lifeline (Lifeline) in the United States. We have data for 2019, 2020, and early 2021, allowing us to exploit the considerable intra-national (state-level) variation of epidemiological situations and policy measures observed within the United States. Thanks to coordination across the network of crisis centers that constitute the Lifeline through a common set of general guidelines, institutional and measurement issues that complicate comparisons across diverse sets of helplines and nations are less of a concern in this dataset. As a helpline focused on suicide, however, the Lifeline does not allow us to track changes in the composition of mental health problems.
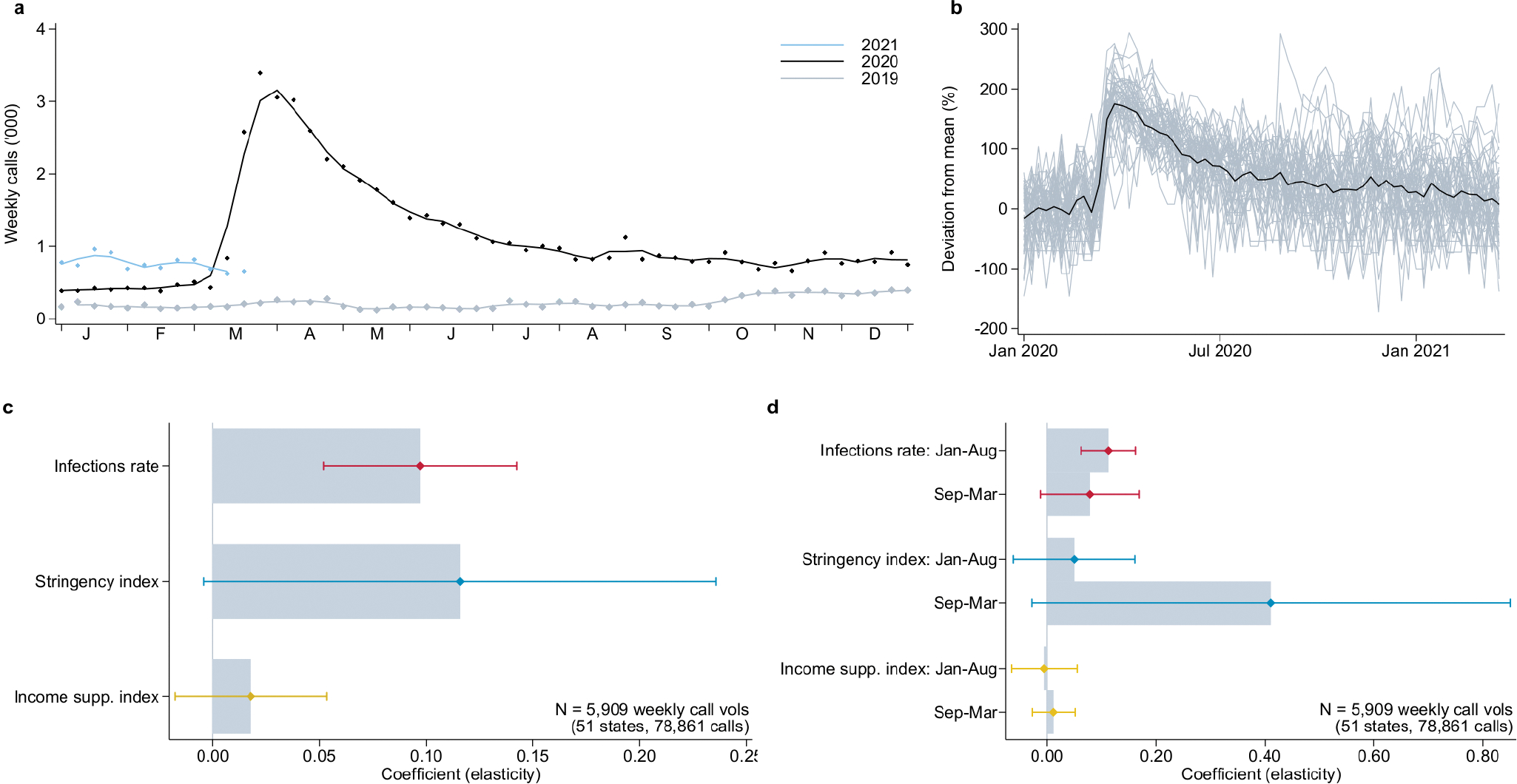
Fig. 4 presents our main findings. The averaged time trends shown in Fig. 4a reveal that calls to the Lifeline were no higher in 2020 than in 2019 during the first wave, but somewhat higher during subsequent waves of COVID-19. Fig. 4b illustrates the heterogeneity in the number and evolution of calls across states. It is this variation that we seek to ‘explain’ with state-week variation in infections and policies. In Figs. 4c to e, we show the variation of our three explanatory variables: SARS-CoV-2 infections39, NPIs as measured by the components ‘containment and closure policies’ summarized in the stringency index, and the generosity of public compensation payments to workers as measured by the component ‘income support’ of the Oxford COVID-19 Government Response Tracker40. These graphs illustrate the longitudinal variation of the independent variables in our regression analyses. In Fig. 4f, we summarize our regression results (see Methods for the precise model specification). The left-hand chart shows estimates from data that are pooled across the entire duration of the pandemic. We find that increases in SARS-CoV-2 infections, ceteris paribus, were associated with statistically significant decreases in the number of calls to the suicide helpline. The estimated coefficient implies that a 10% increase in SARS-CoV-2 infections leads to a drop in calls to the suicide helpline of some 0.1%.
Fig. 4: Lifeline calls, COVID-19, and policy measures in the United States.
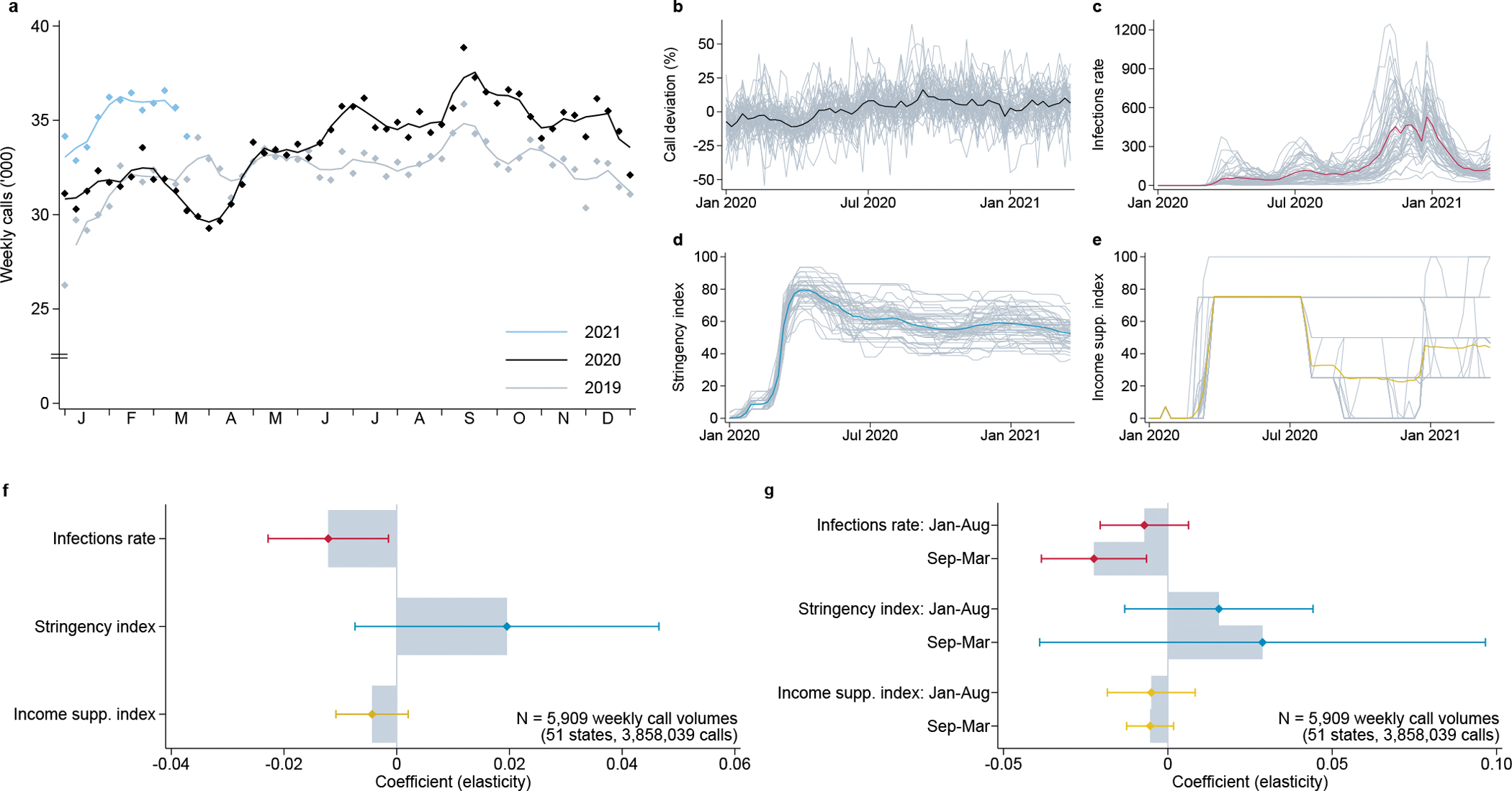
a, Overall sum of weekly calls routed to Lifeline centers by year, with 3-week moving average. b, Deviation of log calls from the state mean in gray, overall weekly average in black. Weekly average scores, with individual state values in gray, for c, newly confirmed SARS-CoV-2 infections per 100,000 population39, d, government response stringency index, and e, income support index40. f, Estimated coefficients and associated 95% confidence intervals. Sub-national panel model including state and week fixed effects. Dependent variable is ln(Lifeline calls+1), and independent variables are measured in logs as well; see Methods, equation (5). g, Coefficient estimates for interaction terms with indicators for the two periods from January–August 2020 and September 2020–March 2021, and associated 95% confidence intervals; see Methods, equation (6).
One interpretation of this result is that the pandemic itself attenuates suicidal anxieties, perhaps by shifting people’s focus on the distress of others, or on their own fear of the pandemic. This interpretation is consistent with the evolution of calls to the U.S. Disaster Distress Helpline, which is aimed at providing crisis counseling to people affected by COVID-19: calls to that helpline increased very strongly in the initial phase of the pandemic, suggesting some substitution away from pre-existing anxieties toward more proximate COVID-19-related sources of distress (see Extended Data Fig. 6).
Policy interventions in the shape of more stringent state-level NPIs or more generous state-level income support measures are not found to have statistically significant effects on Lifeline calls. Taking the somewhat imprecisely estimated coefficients at face value, however, suggests that stricter NPIs were followed by a slight increase in Lifeline calls, while income support policies had the opposite effect. The point estimate on the NPI stringency measure implies that tightening measures by 10% raised the volume of calls to the suicide helpline by some 0.2%.
Fig. 4g shows the estimated effects of the three explanatory variables separately for the first and the subsequent waves of the pandemic, with the cutoff date placed at September 1, 2020. We find that the dampening effect on Lifeline calls of the pandemic itself (measured through SARS-CoV-2 infections) increased across the two pandemic waves. The effects on Lifeline calls of more stringent NPIs or more generous income support, however, did not noticeably differ across waves of the pandemic. Taken together, these estimates confirm that the mental-health implications of the pandemic remained relatively stable across the first and subsequent waves. In the Supplementary Information, we show that these qualitative results are robust across a range of panel regression specifications.
The pattern observed in U.S. suicide helpline data is corroborated by a corresponding regression analysis based on the German and French helplines (Fig. 5): ceteris paribus, rising SARS-CoV-2 infections and more generous income support policies were followed by drops in the number of helpline calls due to suicidal ideation, whereas more stringent NPIs were followed by more suicide-related calls. These effects are estimated to be statistically significant, and consistent with those based on the U.S. Lifeline. Our findings suggest that public compensation payments for pandemic-induced losses not only reduce economic hardship but also have broader benefits: more generous income support is found to lead to fewer calls because of fear, loneliness, suicidal ideation, physical health concerns and, as expected, economic anxiety (‘livelihood’, see Fig. 5).
Fig. 5: Daily calls by conversation topic, COVID-19, and policy in Germany and France.
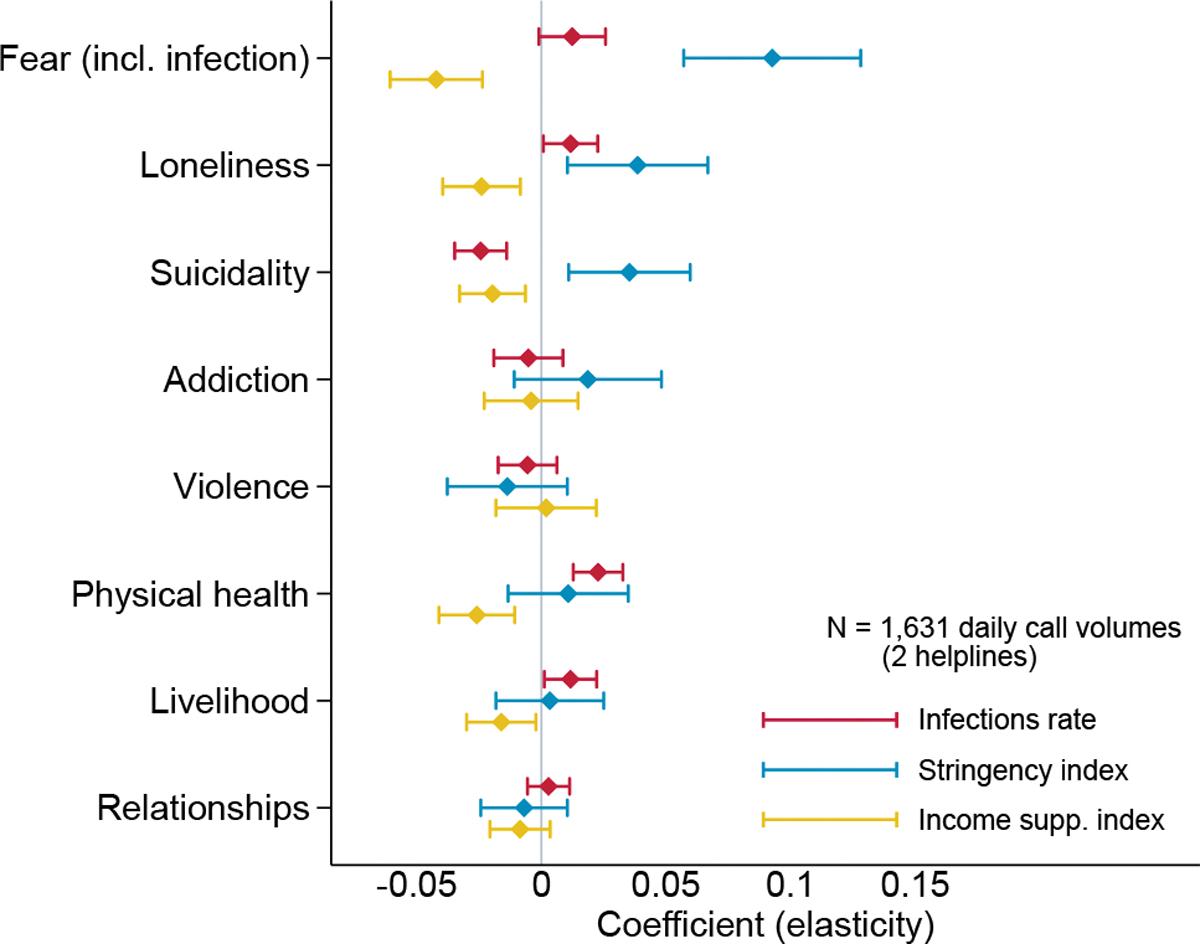
Coefficients from separate regression models by topic with 95% confidence intervals. Dependent variable is ln(calls+1), and independent variables are measured in logs as well39,40. The sample includes all calls to Telefonseelsorge (Germany) and S.O.S. Amitié (France) for which at least one conversation topic was recorded, aggregated to daily totals from January 1, 2019 to March 31, 2021; see Methods, equation (7).
Discussion
We draw on international helpline call data to shed light on something of a statistical blind spot of pandemic policy: mental health concerns and general distress of the population. We find that helpline calls increase during the pandemic, and that this increase is primarily driven by concerns linked to the pandemic itself (fear of infection, loneliness). Conversely, the share of calls due to other forms of distress, including suicidality, violence and addiction, has on averaged decreased. The non-increase in the share of suicide-related calls is consistent with observed decreases in actual suicides during the early stages of the pandemic across numerous countries28. Underlying these general patterns are helpline-specific evolutions that are documented in detail in the Supplementary Information.
The panel structure of the data allows us to estimate multivariate models to disentangle the separate effects of the pandemic itself (SARS-CoV-2 infections), of the stringency of containment policies, and of the generosity of income support policies. We find that, ceteris paribus, more stringent measures are associated with a greater number of calls out of fear, loneliness and suicidality, but that more generous income support has the opposite effect. This implies that compensation payments to workers and businesses affected economically by COVID-19, designed to preserve demand and productive capacity, have additional benefits by alleviating distress and mental health concerns.
Longitudinal helpline data offer an attractive complement to existing empirical approaches based on surveys, administrative and clinical data (suicide statistics, admissions to treatment centers, etc.) and internet search data. Naturally, helpline data also have their limitations. One issue is that call counts may be influenced not only by demand but also by supply, as capacity constraints can force operators to leave some calls unanswered. This may bias measures of increases in demand downwards. However, as calls are not pre-screened, capacity constraints are unlikely to affect analyses of the composition of calls in terms of topics or caller characteristics.
Another limitation lies in our agnosticism about the representativeness of callers to helplines. We are aware of no rigorous evidence on the composition of the helpline caller population in terms of socio-demographic status, health, occupation, nationality, etc. By focusing our analysis on changes in call volumes over time, we difference out time-invariant specificities of the helpline caller population, which should remove much of any potential sample selection bias. Moreover, anecdotal evidence from helpline workers confirms that the caller population typically includes the most vulnerable members of society, which is the population of greatest interest in a study of distress and mental health concerns.
Methods
Helpline call data
Our sample of helplines includes large, general crisis helplines, dedicated suicide prevention helplines, as well as some helplines that focus on specific groups such as children, parents, or immigrants. Observations within helplines are self-selected, as they consist of callers to helplines. The selection of sample helplines was based (a) on an internet search of well-documented helplines and (b) on receiving data from those helplines. Of 154 helplines contacted, we received data from 37 helplines. Where possible, we requested data from 1 January 2019 to the most recent available date, in order to allow a comparison of call patterns after the COVID19 outbreak to call patterns at the same time of year pre-pandemic. The information obtained from 23 helplines was of sufficiently detailed coverage and consistency to be included in our pooled analyses. Extended Data Table 1 lists the included helplines, grouped by the format in which the data were made available for this study.
The most detailed information was provided by the helplines in Extended Data Table 1a, where we have received individual conversation-level data, including information on caller’s sex and approximate age, as well as on the issues discussed during the conversation. From the three additional helplines in b, we received aggregate time series of daily call volumes, with separate series by gender, age category and topic. Moreover, for the two helplines in Extended Data Table 1c, we received sub-national weekly series of call volumes across US States. In contrast to the data in a and b, the number of calls in c does not refer to answered calls and actual conversations, but to the raw number of calls routed to local centers.
Data processing and analysis were conducted according to the guidelines of the Internal Review Board (IRB) of the Faculty of Business and Economics at the University of Lausanne. Two considerations were important. First, all helplines guarantee anonymity to their callers, both toward their operators and toward the outside world. Names and addresses are never asked, and caller numbers are hidden by the system. It is therefore impossible to identify callers even from the call-level data provided by a subset of helplines. Anonymous data is not covered by data protection considerations. Second, most helplines explicitly inform callers that anonymous call data are recorded and made available for reporting and statistical purposes. The analysis of those data conforms with the aim of the Ethics Charter of the International Federation of Telephone Emergency Services (IFOTES), which aims to “(c)ollect and disseminate data gathered by the Branches in connection with the challenges facing Mental Health and Prevention of Suicide”, and to “(a)ssist and encourage research carried out in these fields”6. The IRB exempted the study from a full review owing to the secondary nature of the data used.
Government response and epidemiological data
In order to measure the timing and intensity of government responses consistently across time, countries and sub-national regions, we rely on aggregate policy indices from the Oxford COVID-19 Government Response Tracker 40. In particular, we use two policy indices, the Government Response Stringency Index, and the Income Support Index. The stringency index shows the strictness of containment policies and restrictions of personal freedom, and is based on an unweighted average of 8 component scores for stay-at-home requirements, workplace and public transport closures, restrictions on public events, gatherings, domestic and international travel, and information campaigns. The income support index reflects the availability of financial support. To obtain a comparable measure, we construct the index score using the ordinal measure and the flag for sectoral targeting to arrive at a value between 0 and 100. For the sub-national information on policies in US states, it is important to note that we use the total index scores, where, whenever national policies were more restrictive than those of individual states, the higher score is imputed. Data on the daily number of newly confirmed SARS-CoV-2 infections are taken from the JHU CSSE COVID-19 Dataset 39.
Call volumes after the pandemic outbreak
For Fig. 1, we combine the time series data (Extended Data Table 1b) with aggregates based on the call-level data (Extended Data Table 1a) in a panel of daily call volumes for 21 helplines, covering the time up to June 30, 2020 if available. Note that for 4 of the helplines (MIELI, S.O.S. Détresse, SAHAR, Muslimisches Seelsorgetelefon) no data is available for 2019. We then look exclusively on the period from 4 weeks before to 12 weeks after the country-specific event date in 2020, as well as, if available, the corresponding days of the year 2019.
To summarize the overall dynamics, we estimate the following model:
| (1) |
The dependent variable is the natural logarithm of the number of calls to helpline h recorded on day t. We define the local outbreak as the date when (a) the cumulative number of SARS-CoV-2 infections per population exceeded 1/100,000 or (b) when SIP orders were first introduced. For both versions, we define indicator variables that are set to one for days in event week number τ ∈ [−4, 12] in 2020. The model includes helpline fixed effects ξh, interacted with year, week-of-year and day-of-week indicators, summarized in the vector Θt. The reference category is week 0 of the pandemic outbreak/SIP introduction, and the coefficients γτ allow us to track the percentage deviation in daily calls, controlling for seasonal effects and secular trends. See Extended Data Fig. 1 for details on event dates and call volumes for each of the 21 included helplines.
Helpline data, individual calls
To investigate changes in conversation topics in Fig. 2, we focus on the call-level data and combine information from 12 helplines (Extended Data Table 1a) for which we have information on converstation topics and inferred caller characteristics. This yields a sample of up to 2.2 million calls. For each helpline, we categorize calls based on the recorded information on the problems of callers and the topics discussed. Precise categorizations of call topics differ across helplines, but they are sufficiently similar to allow us to map them into to the following common, non-exclusive categories: loneliness (social isolation, entrapment), fear (general fear, anxiety disorder, fear of infection with SARS-Cov-2), suicidality (suicidal ideation, suicidal thoughts or plans, suicide attempts, suicidality of others), addiction (drugs, alcohol, other addictions), violence (physical violence and abuse, sexual harassment, rape), physical health (disease, long-term illness, disability), and two broad categories for livelihood (work situation, unemployment, financial problems, housing), and relationships (family life, parenting, marriage and intimate relationships, separation). As some topics are not recorded at all for some helplines, the sample size differs depending on which topic we look at: the largest sample includes data from 12 helplines, where we can distinguish calls related to suicide from calls concerning other issues (see Extended Data Fig. 2). Recorded conversation topics can be non-exclusive. We document the joint distribution of topics in Extended Data Fig. 5a.
Additionally, we have coded the sex and age category of each caller, and (where possible) further characteristics such as marital status, living situation and occupational status. In the Supplementary Information, we provide a more detailed description of each sample helpline. As helplines record age categories differently, our classification cannot be fully precise. Using the boundaries of available age groups, the group of callers below 30 includes only those that were recorded in an age group with an upper limit below 30. The same logic applies to the group of callers older than 60, and the middle category in some cases includes also individuals whose age is slightly below 30 years or above 60.
For Fig. 2 we restrict the sample to calls recorded for the time from 1 January 2019 through 30 June 2020, where information on sex and age group of callers is available. When estimating the relative importance of a topic, we define the dependent variable Ti,h,t as equal to one for call i to helpline h on day t if the conversation was related to topic T (Fear, Loneliness, Suicide, Addiction, Violence, Physical health, Livelihood, or Relationships), and zero for unrelated calls, where another topic was recorded. Calls without information on caller issues or conversation topics are not included. Based on the date when the cumulative number of SARS-CoV-2 infections per population exceeded 1/100,000 in the country of operation39, we define an indicator Post outbreakh,t and estimate a linear probability model as in equation 2:
| (2) |
The model includes helpline indicators ξh to account for time invariant differences among helplines. We further add year, week-of-year and day-of-week indicators, summarized in the vector Θt, interacted with the helpline fixed effects, to account for secular trends and for seasonal and day-of-week effects. Standard errors are clustered at the helpline-week level.
For the analysis of heterogeneous effects in Extended Data Fig. 4, we estimate an alternative specification including individual caller characteristics and interaction terms. To illustrate the change in topics for different groups, we classify callers into six non-overlapping groups, denoted in the vectors Sex (male, female) and Age group (below 30, 30–60, above 60). In the model illustrated in equation 3, we interact the post-outbreak variable with all six group indicators, so that the coefficients represent the group-specific changes in topic shares:
| (3) |
For the main effects of caller sex and age groups, indicators for the reference group of male callers in the 30–60 age category are omitted.
For the analysis of the longer time horizon and the second wave in Fig. 3, we focus on call level data from Germany and France, from January, 1 2019 through March, 31 2021. We estimate a specification similar to the previous approach, separately for the two helplines and each topic. To distinguish the changes around the outbreak from later adjustments during the subsequent wave, we define two indicator variables W1 and W2 denoting two periods. The first covers the time from 11 March 2020, when the World Health Organization declared the outbreak a pandemic, to 30 June 2020, when the number of infections decreased again and containment measures were relaxed both in Germany and in France. The second period indicator is equal to one for the time after 1 October 2020. equation 4 illustrates the estimated model:
| (4) |
As we analyze the two helplines separately, we do not include helpline fixed effects here, but capture secular trends and seasonal patterns through the inclusion of year, week-of-year, and day-of-week indicators. Standard errors are clustered at the week level.
Call volumes across U.S. states
The analysis of sub-national call volumes in Fig. 4 relies on data on weekly call volumes routed to the National Suicide Prevention Lifeline (Lifeline). The analysis is based on weekly call volumes for US States and Territories over 116 weeks, starting in the week to 6 January 2019, and up to the week ending on Sunday, 21 March 2020. Based on phone numbers, the state from which calls were placed can be inferred, even though internal migration means that this classification is subject to measurement error. While the Lifeline will serve any calls regardless of country of origin, its mission is to serve calls originating from the US and US territories. We focus on calls from 50 US states and the District of Columbia. Calls originating from Canadian provinces, US Territories, as well as those of other international or unknown origin are not considered, in order to maximize consistency and because of the limited availability of data on policy responses. The panel structure allows us to exploit the idiosyncratic variation within states j over time (weeks w) while controlling for overall trends. We estimate a two-way error component model as illustrated in equation 5:
| (5) |
The dependent variable is the natural logarithm of the number of calls plus one, Infections is defined as one plus the sum of newly confirmed SARS-CoV-2 infections in week w per 100,000 population, while Stringency and Income support are calculated as weekly averages of the respective daily index scores. State fixed effects ξj absorb all time-invariant factors, and our analysis is therefore based on the idiosyncratic within-state variation in call volumes over time. The inclusion of week indicators θw allows us to capture all nation-wide and global effects and to focus solely on the relative differences in pandemic exposure and policy response. Standard errors are clustered at the state-month level.
To investigate the extent to which the relationship changed over time, we re-estimate the model as in equation 6. Here, we include the three main explanatory variables interacted with two indicators variables that are set to 1 for the time period from January to August 2020, and for September 2020 to March 2021 respectively.
| (6) |
Call volumes in Germany and France
For the analysis in Fig. 5, we combine the previous approaches and estimate the relationship between call volumes and the three variables as illustrated in equation 7, based on topic-specific call volumes to Telefonseelsorge (Germany) and S.O.S. Amitié (France) during the time from January 1, 2019 to March 31, 2021.
| (7) |
In contrast to the sub-national panel of US states, here we do not include week fixed effects but capture secular trends and seasonal patterns through helpline fixed effects, interacted with year, week-of-year, and day-of-week indicators. Standard errors are clustered at the helpline-week level.
Extended Data
Extended Data Fig. 1: Evolution of daily helpline call volumes during the first wave.
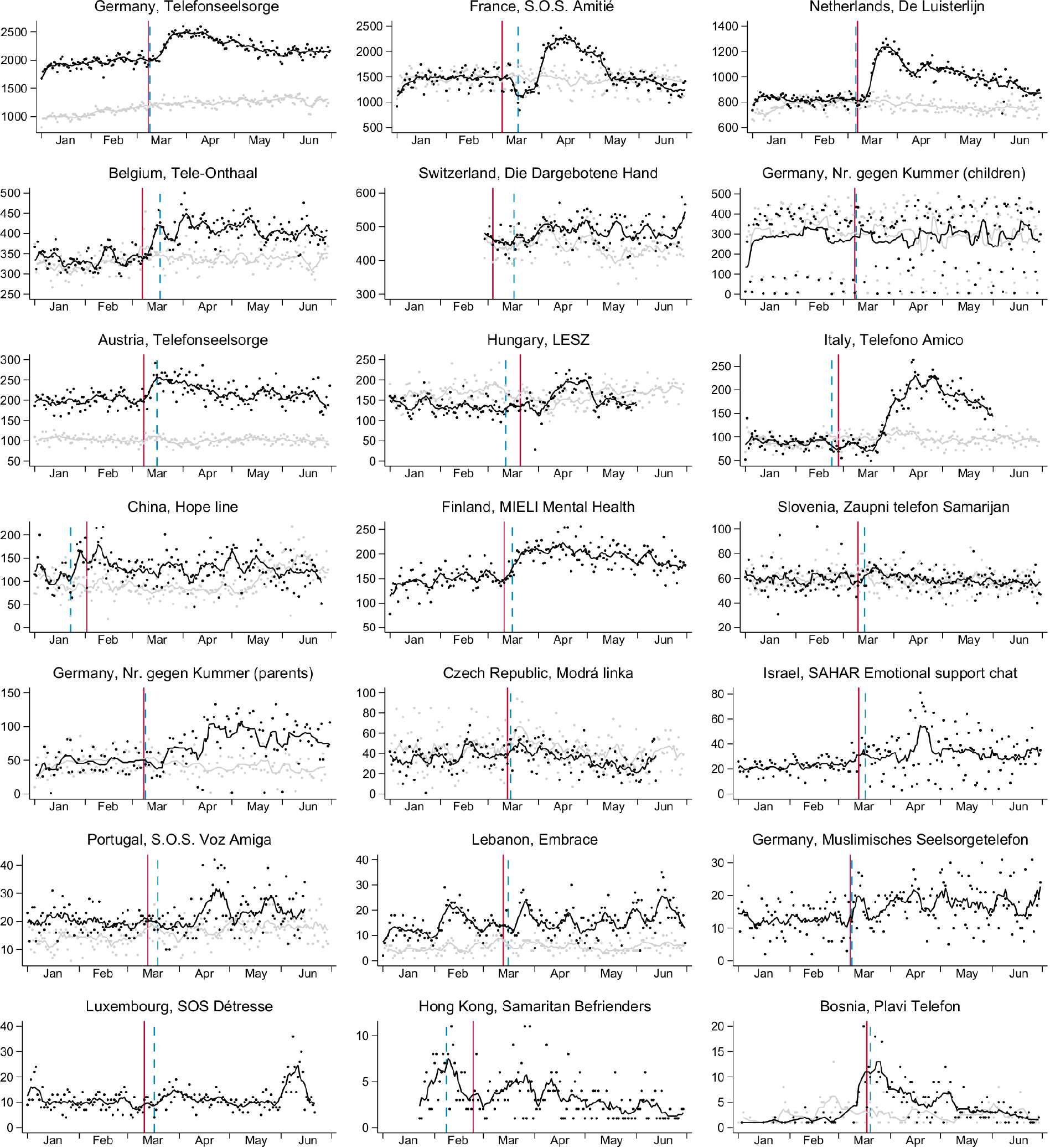
Sum of daily helpline contacts with seven-day moving average, January–June 2020 (black) and 2019 (light grey, not available for all helplines). The solid red line shows the date of the pandemic outbreak, when more than 100 SARS-CoV-2 infections per 100,000 population have been recorded, the dashed blue line shows the date when shelter-in-place requirements were first introduced in the country of operation.
Extended Data Fig. 2: Conversation topic shares by helpline.
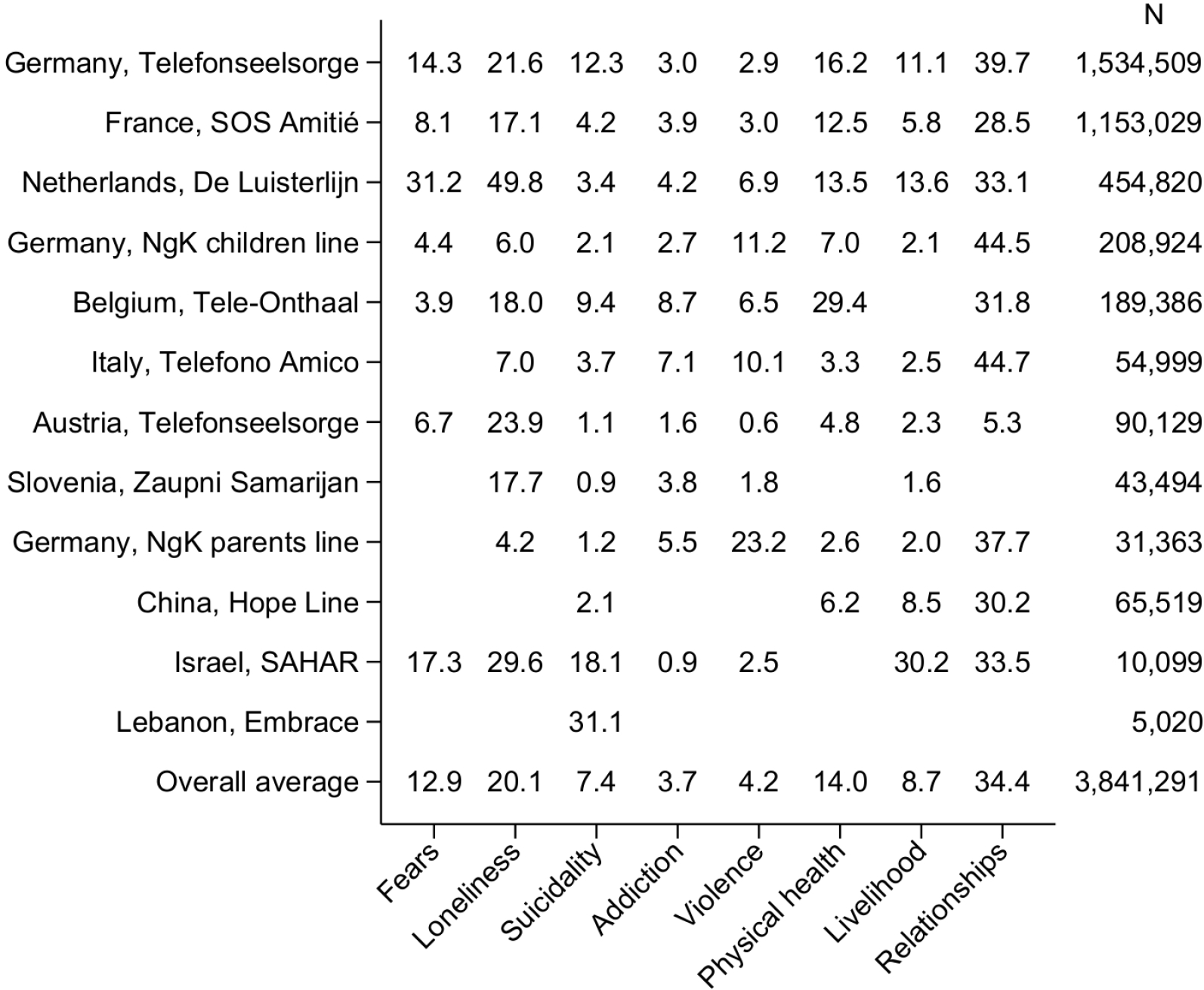
Each cell shows the share of calls related to the conversation topic on the horizontal axis, for calls with the helpline indicated on the vertical axis. Full dataset, covering all calls for which at least on topic was recorded, from 1 January 2019 to the respective end of available data, see Extended Data Table 1a.
Extended Data Fig. 3: Magnitude of post-outbreak change and equivalence tests.
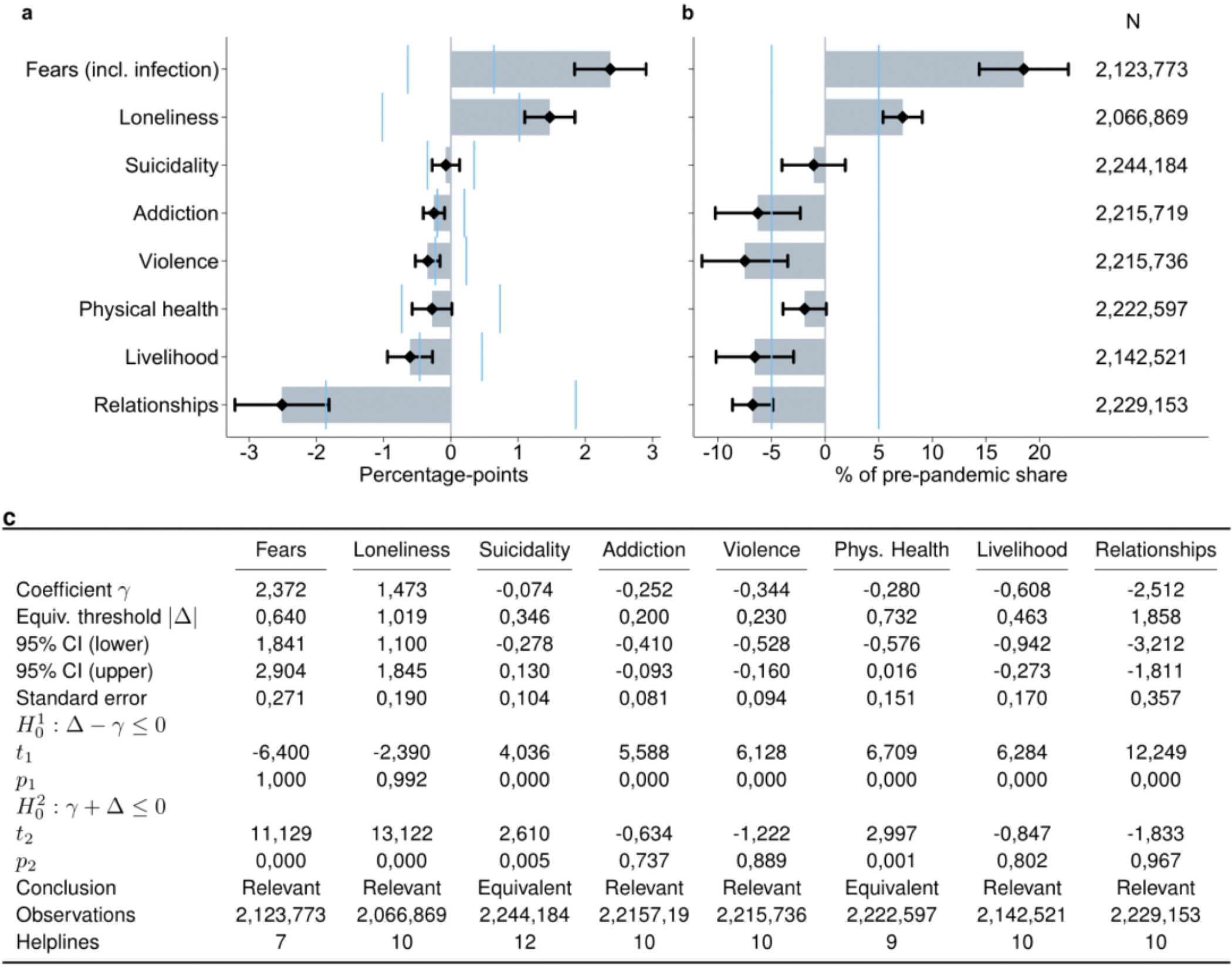
a, Coefficient estimates from linear probability models as in Fig.2b, with 95% confidence intervals and equivalence bounds, defined as 5% of the pre-pandemic share of the respective topic, indicated by light blue vertical bars. b, Results from a normalized across conversation topics, with coefficient estimates and associated 95% confidence intervals, and equivalence bounds divided by the pre-pandemic share of calls related to the respective topic. c, Relevance tests, numerical coefficient estimate with corresponding equivalence bounds, with test statistics and p-values from two one-sided tests for equivalence.
Extended Data Fig. 4: Change in conversation topics by caller sex and age group.
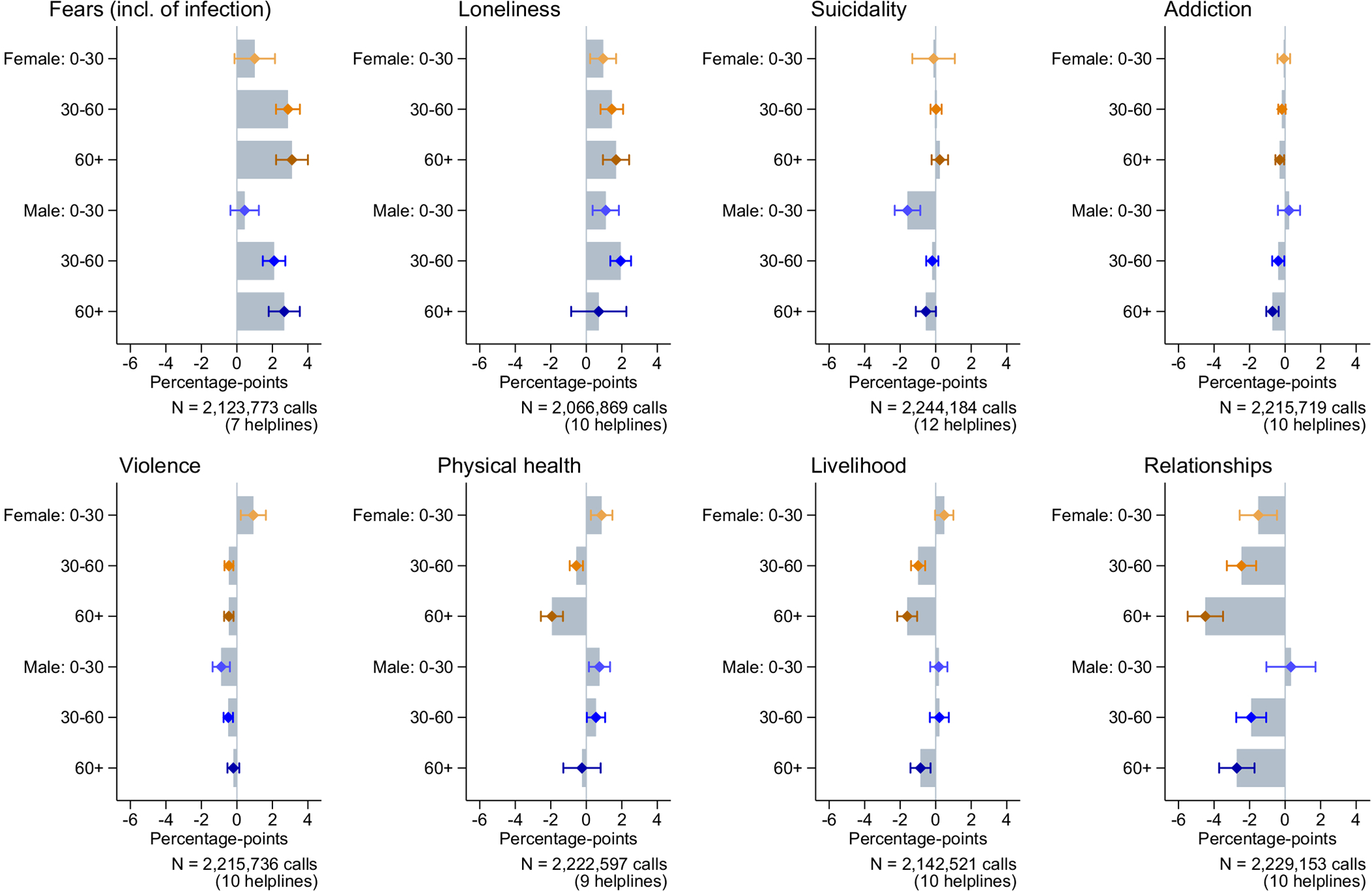
Estimated coefficients for interaction terms of group indicators with binary post-outbreak variable, and associated 95% confidence intervals. Separate linear probability regression models with dependent variable set to one for calls related to the respective topic, see Methods, equation (3).
Extended Data Fig. 5: Non-exclusive conversation topics.
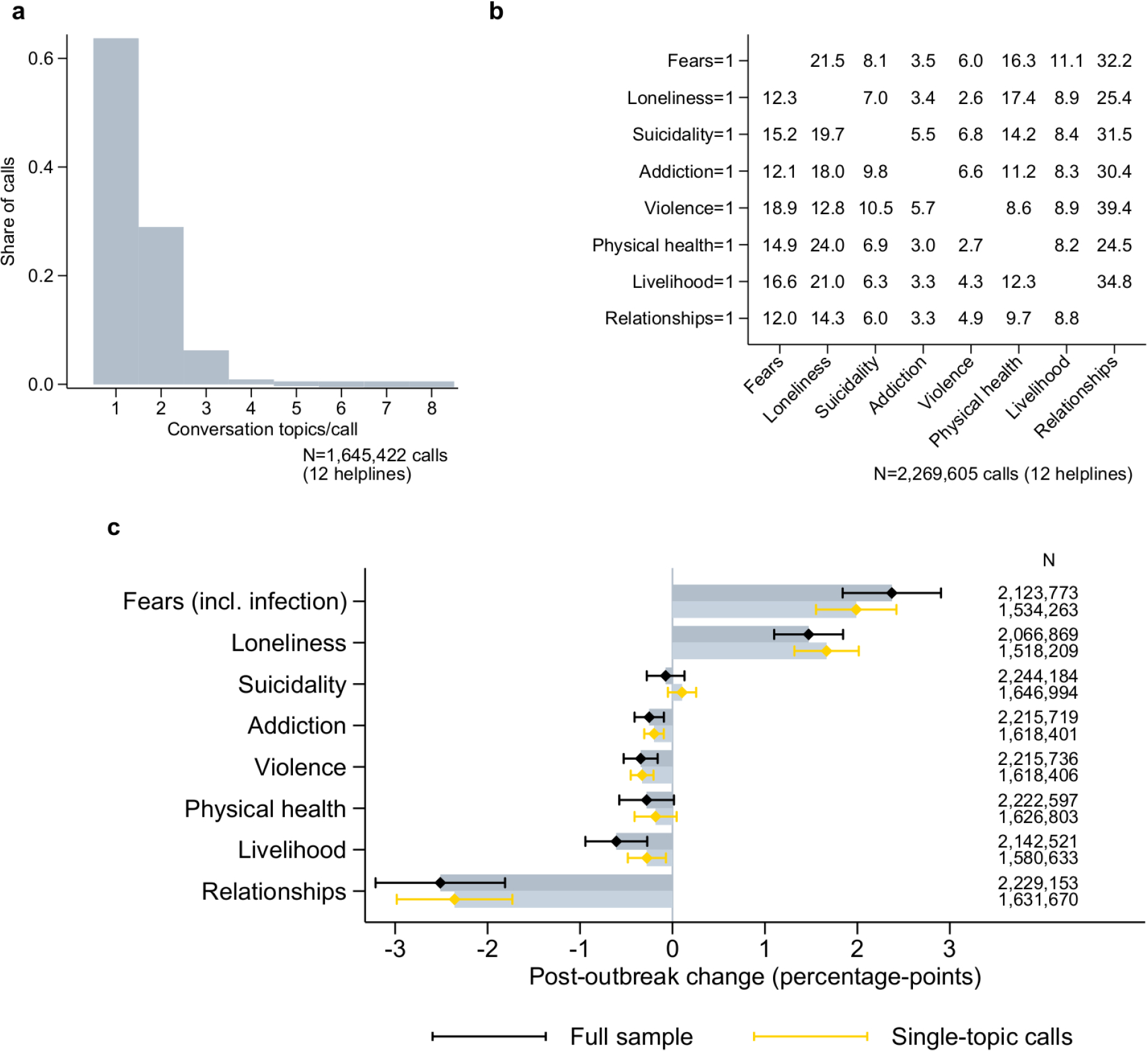
Relation among conversation topics for calls included in the estimation sample underlying Fig. 2, from 1 January 2019 to 30 June 2020, and where sex and age group of callers are observed. a, Distribution of recorded number of conversation topics per call, b, Overlap in conversation topics, where each row shows the distribution of second or further topics (horizontal axis), for calls related to one specific topic (vertical axis). c, Results from Fig. 2b, with alternative estimates based on a restricted sample of single-topic category calls.
Extended Data Fig. 6: Disaster Distress Helpline.
a, Sum of weekly calls routed to centers by year with 3-week moving average, b, deviation of log calls from state mean (gray), with overall weekly average (black). c, Estimated coefficients and associated 95% confidence intervals. Sub-national panel model including state and week fixed effects. Dependent variable is ln(Disaster Distress calls+1), and independent variables are measured in logs as well; see Methods, equation (5).d, Coefficient estimates for interaction terms with indicators for the two periods from January–August 2020 and September 2020–March 2021, and associated 95% confidence intervals; see Methods, equation (6).
Extended Data Table 1:
Overview over helpline data
| Country | Helpline | Total calls | Data start | Data end | |
|---|---|---|---|---|---|
|
| |||||
| a | Germany | Telefonseelsorge Deutschland | 1,500,938 | 01.01.2019 | 31.03.2021 |
| France | S.O.S. Amitié | 1,153,029 | 01.01.2019 | 31.03.2021 | |
| Netherlands | De Luisterlijn | 454,820 | 01.01.2019 | 30.06.2020 | |
| Germany | Nr. gegen Kummer (children) | 208,924 | 01.01.2019 | 18.02.2021 | |
| Belgium | Tele-Onthaal | 189,386 | 01.01.2019 | 28.06.2020 | |
| Austria | Telefonseelsorge Österreich | 89,619 | 01.01.2019 | 30.06.2020 | |
| China | Hope Line | 65,519 | 01.01.2019 | 25.06.2020 | |
| Italy | Telefono Amico | 54,999 | 01.01.2019 | 01.06.2020 | |
| Slovenia | Zaupni telefon Samarijan | 43,494 | 01.01.2019 | 14.01.2021 | |
| Germany | Nr. gegen Kummer (parents) | 31,363 | 01.01.2019 | 18.02.2021 | |
| Czech Republic | Modrá linka | 19,871 | 01.01.2019 | 12.06.2020 | |
| Israel | SAHAR Emotional support chat | 15,956 | 01.01.2020 | 24.12.2020 | |
| Portugal | S.O.S. Voz Amiga | 9,930 | 02.01.2019 | 15.06.2020 | |
| Germany | Muslimisches Seelsorgetelefon | 5,485 | 01.01.2020 | 08.12.2020 | |
| Lebanon | Embrace Lifeline | 5,020 | 02.01.2019 | 01.07.2020 | |
| Luxembourg | SOS Détresse | 1,928 | 01.01.2020 | 21.06.2020 | |
| Bosnia Herzeg. | Plavi Telefon | 1,034 | 01.01.2019 | 23.10.2020 | |
| Hong Kong | Samaritan Befrienders | 635 | 23.01.2020 | 06.10.2020 | |
|
| |||||
| b | Switzerland | Die Dargebotene Hand | 110,177 | 28.02.2019 | 30.06.2020 |
| Hungary | LESZ | 79,491 | 01.01.2019 | 31.05.2020 | |
| Finland | MIELI Mental Health | 32,148 | 01.01.2020 | 30.06.2020 | |
|
| |||||
| c | United States | National Suicide Prevention Lifeline | 3,858,039 | 01.01.2019 | 21.03.2021 |
| Disaster Distress Helpline | 78,861 | 01.01.2019 | 21.03.2021 | ||
a, Individual conversation-level data, including information on callers’ sex and approximate age (as inferred by helpline operators), as well as on the topics discussed during the conversation. b, Daily conversation volumes, by sex, age, and topic. c, Sub-national weekly call volumes across US States (raw number of calls routed to local centers).
Extended Data Table 2:
Caller characteristics before and after the pandemic outbreak
| Female |
Age < 30 |
Age > 60 |
Voice call |
Known caller |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Country | Helpline | pre | post | pre | post | pre | post | pre | post | pre | post | N (calls) |
|
| ||||||||||||
| Germany | Telefonseelsorge | 68.6 | 68.4 | 15.5 | 14.8 | 29.0 | 31.2 | 88.6 | 90.2 | . | . | 1,534,509 |
| France | S.O.S. Amitié | 54.0 | 55.8 | 4.3 | 5.2 | 17.9 | 18.0 | 95.8 | 95.7 | . | . | 1,153,029 |
| Netherlands | De Luisterlijn | 65.9 | 66.6 | 8.9 | 8.6 | 18.4 | 23.7 | 90.9 | 90.3 | . | . | 454,820 |
| Germany | NgK children line | 39.1 | 40.7 | 100 | 100 | 0 | 0 | 100 | 100 | 11.8 | 10.2 | 208,924 |
| Belgium | Tele-Onthaal | 66.5 | 67.3 | 13.3 | 15.6 | 28.6 | 30.2 | 87.0 | 86.0 | 42.9 | 41.3 | 189,386 |
| Austria | Telefonseelsorge | 67.3 | 62.7 | 9.1 | 8.1 | 31.8 | 36.3 | 100 | 100 | . | . | 90,129 |
| China | Hope Line | 49.2 | 54.7 | 61.6 | 66.1 | 0.4 | 0.3 | 100 | 100 | 29.6 | 31.4 | 65,519 |
| Italy | Telefono Amico | 43.3 | 34.5 | 5.5 | 7.2 | 9.7 | 6.3 | 98.1 | 92.4 | . | . | 54,999 |
| Slovenia | Zaupni Samarijan | 45.6 | 48.7 | 0.7 | 0.6 | 8.9 | 9.8 | 100 | 100 | . | . | 43,494 |
| Germany | NgK parent line | 74.8 | 73.4 | 11.4 | 10.7 | 8.4 | 7.5 | 100 | 100 | 10.3 | 9.0 | 31,363 |
| Israel | Sahar | 66.8 | 69.3 | 38.5 | 41.2 | 1.1 | 1.5 | 0 | 0 | 50.7 | 40.8 | 10,099 |
| Lebanon | Embrace | 56.5 | 50.6 | 74.1 | 56.2 | 4.6 | 9.7 | 100 | 100 | 11.5 | 17.6 | 5,020 |
Shares of callers belonging to the catergory indicated in the column header, pre and post March 1, 2020. Full dataset, covering calls from 1 January 2019 to the respective end of available data, see Extended Data Table 1a. Caller sex and age are not observed for all calls. Voice calls include phone and Voice-Over-IP calls, as opposed to text based conversations (online chats, messaging apps). Known callers are defined as individuals who repeatedly call the helpline and are therefore known to staff. Further details on individual helplines are available in the Supplementary Information.
Supplementary Material
Acknowledgments
We thank the following people and helplines for sharing their expertise and for granting us access to their data: Carola Hochhauser and Antonia Kesselring (Telefonseelsorge, Austria), Jennifer Pots (Tele-Onthaal, Belgium), Maja Kovacevic (Plavi Telefon, Bosnia and Herzegovina), Rujun Ma and Wenping Ni (Hope Line, China), Hana Regnerova (Modrá linka, Czech Republic), Hervé Dumont (S.O.S. Amitié, France), Susanna Winter (MIELI, Finland), Ludger Storch and Bernd Blömeke (Telefonseelsorge, Germany), M. Imran Sagir (Muslimisches Seelsorgetelefon, Germany), Heidi Schütz (Nummer gegen Kummer, Germany), Hsuan-Chia (Samaritan Befrienders, Hong Kong), Eva Brandisz (LESZ, Hungary), Yael Levy (Sahar, Israel), Monica Petra (Telefono Amico, Italy), Pia Zeinoun (Embrace Lifeline, Lebanon), Sébastien Hay (SOS Détresse, Luxembourg), Jaap Jakobs (De Luisterlijn, Netherlands), Francisco Paulino (SOS Voz Amiga, Portugal), Kristina Bogataj (Zaupni telefon Samarijan, Slovenia), Sabine Basler (Die Dargebotene Hand, Switzerland), Alena Goldstein, Johnathan Higgins, and Sean Murphy, Vibrant Emotional Health (National Suicide Prevention Lifeline and Disaster Distress Helpline, USA).
We thank Charles Efferson, Laurent Keller, Kairi Kõlves, and Judith Vornberger for comments and suggestions.
Funding
We are grateful to the Swiss National Science Foundation (NCCR LIVES –’Overcoming Vulnerability: Life Course Perspectives’) for financial support.
Footnotes
Competing interests The authors declare that they have no competing interests.
Additional Information Supplementary Information is available for this paper.
Code availability Files were collected in MS Excel 2016 and Notepad++ v7.9.5. Data preparation and analysis was carried out in Stata/SE 17.0, Do-files are available online at https://doi.org/10.5281/zenodo.5495830.
Data availability
Data were provided by helplines for the sole purpose of this research project, subject to confidentiality agreements. The full data underlying specific parts of the analysis is available from the authors upon reasonable request and conditional on permission of the respective helplines. Figure source data is provided with this paper. To obtain (updated) helpline data, researchers have to sign agreements with individual helplines, for further information, contact: presse@telefonseelsorge.de (Telefonseelsorge DE), contact@sosamitieparisidf.fr (S.O.S. Amitié), info@deluisterlijn.nl (De Luisterlijn), info@nummergegenkummer.de (Nr. gegen Kummer), federatie@tele-onthaal.be (Tele-Onthaal), telefonseelsorge@edw.or.at (Telefonseelsorge AT), lcicenter@163.com (Hope Line), telefonoamico@telefonoamico.it (Telefono Amico), samarijan@gmail.com (Zaupni Samarijan), hana.regnerova@modralinka.cz (Modrá linka), support@sahar.org.il (Sahar), direccaolphm@gmail.com (S.O.S. Voz Amiga), info@mutes.de (Muslim. Seels.), info@embracelebanon.org (Embrace), info@sosdetresse.lu (SOS Détresse), info@novageneracija.org (Plavi Telefon), sbhkinfo@sbhk.org.hk (Samaritan Befrienders), verband@143.ch (Die Dargebotene Hand), sos-keskus@mieli.fi (MIELI mental health), lesziroda@gmail.com (LESZ), info@vibrant.org, (Lifeline and Disaster Distress Helpline). Data on infection rates and policy measures is publicly available online from the JHU CSSE COVID-19 Dataset at https://github.com/CSSEGISandData, and the Oxford Covid-19 Government Response Tracker at https://github.com/OxCGRT.
References
- [1].United Nations (UN). COVID-19 and the need for action on mental health. UN Sustainable Development Group Policy Brief (2020). https://unsdg.un.org/resources/policy-brief-covid-19-and-need-action-mental-health. [Google Scholar]
- [2].OECD. Tackling the mental health impact of the COVID-19 crisis: An integrated, whole-of-society response. OECD Policy Responses to Coronavirus (COVID-19) (2021). 10.1787/0ccafa0b-en. [DOI] [Google Scholar]
- [3].Rehm J & Shield KD Global burden of disease and the impact of mental and addictive disorders. Current Psychiatry Reports 21 (2019). 10.1007/s11920-019-0997-0. [DOI] [PubMed] [Google Scholar]
- [4].Leach LS & Christensen H A systematic review of telephone-based interventions for mental disorders. Journal of Telemedicine and Telecare 12, 122–129 (2006). 10.1258/135763306776738558. [DOI] [PubMed] [Google Scholar]
- [5].Coveney CM, Pollock K, Armstrong S & Moore J Callers’ experiences of contacting a national suicide prevention helpline. Crisis 33, 313–324 (2012). 10.1027/0227-5910/a000151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].IFOTES. Ifotes ethical charter (1993). https://cms01.enbilab.com/admin/sites/11/media_library/download/3188e7e0-3ff1-0136-a986-2f94146ac224.
- [7].De Leo D, Buono MD & Dwyer J Suicide among the elderly: the long-term impact of a telephone support and assessment intervention in northern Italy. British Journal of Psychiatry 181, 226–229 (2002). 10.1192/bjp.181.3.226. [DOI] [PubMed] [Google Scholar]
- [8].Choi D et al. Development of a machine learning model using multiple, heterogeneous data sources to estimate weekly US suicide fatalities. JAMA Network Open 3, e2030932 (2020). 10.1001/jamanetworkopen.2020.30932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Batchelor S, Stoyanov S, Pirkis J & Kõlves K Use of kids helpline by children and young people in Australia during the COVID-19 pandemic. Journal of Adolescent Health 68, 1067–1074 (2021). 10.1016/j.jadohealth.2021.03.015. [DOI] [PubMed] [Google Scholar]
- [10].Zalsman G et al. Suicide-related calls to a national crisis chat hotline service during the COVID-19 pandemic and lockdown. Journal of Psychiatric Research (2021). 10.1016/j.jpsychires.2021.05.060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Turkington R et al. Behavior of callers to a crisis helpline before and during the COVID-19 pandemic: quantitative data analysis. JMIR Mental Health 7, e22984 (2020). 10.2196/22984. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Halford EA, Lake AM & Gould MS Google searches for suicide and suicide risk factors in the early stages of the COVID-19 pandemic. PLOS ONE 15, e0236777 (2020). 10.1371/journal.pone.0236777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Armbruster S & Klotzbücher V Lost in lockdown? COVID-19, social distancing, and mental health in Germany. Covid Economics: Vetted and real-time papers 22, 117–153 (2020). https://cepr.org/file/9096/download?token=RZ0VZVi5. [Google Scholar]
- [14].Brülhart M & Lalive R Daily suffering: Helpline calls during the COVID-19 crisis. Covid Economics: Vetted and Real-Time Papers 19, 143–158 (2020). https://cepr.org/file/9088/download?token=c6oU20eH. [Google Scholar]
- [15].Ridley M, Rao G, Schilbach F & Patel V Poverty, depression, and anxiety: Causal evidence and mechanisms. Science 370, eaay0214 (2020). 10.1126/science.aay0214. [DOI] [PubMed] [Google Scholar]
- [16].McInerney M, Mellor JM & Nicholas LH Recession depression: mental health effects of the 2008 stock market crash. Journal of Health Economics 32, 1090–1104 (2013). 10.1016/j.jhealeco.2013.09.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Parmar D, Stavropoulou C & Ioannidis JPA Health outcomes during the 2008 financial crisis in Europe: systematic literature review. BMJ 354, i4588 (2016). 10.1136/bmj.i4588. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Chang S-S, Stuckler D, Yip P & Gunnell D Impact of 2008 global economic crisis on suicide: time trend study in 54 countries. BMJ 347, f5239 (2013). 10.1136/bmj.f5239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Phillips JA & Nugent CN Suicide and the Great Recession of 2007–2009: the role of economic factors in the 50 US states. Social Science & Medicine 116, 22–31 (2014). 10.1016/j.socscimed.2014.06.015. [DOI] [PubMed] [Google Scholar]
- [20].Nordt C, Warnke I, Seifritz E & Kawohl W Modelling suicide and unemployment: a longitudinal analysis covering 63 countries, 2000–11. The Lancet Psychiatry 2, 239–245 (2015). 10.1016/S2215-0366(14)00118-7. [DOI] [PubMed] [Google Scholar]
- [21].Gunnell D et al. Suicide risk and prevention during the COVID-19 pandemic. The Lancet Psychiatry 7, 468–471 (2020). 10.1016/S2215-0366(20)30171-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Zortea TC et al. The impact of infectious disease-related public health emergencies on suicide, suicidal behavior, and suicidal thoughts. Crisis 0 (2020). 10.1027/0227-5910/a000753. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Richter D, Riedel-Heller S & Zürcher S Mental health problems in the general population during and after the first lockdown phase due to the SARS-Cov-2 pandemic: Rapid review of multi-wave studies. Epidemiology and Psychiatric Sciences 30, E27 (2021). 10.1017/s2045796021000160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Banks J, Xu X et al. The mental health effects of the first two months of lockdown during the COVID-19 pandemic in the UK. Fiscal Studies 41, 685–708 (2020). 10.1111/1475-5890.12239. [DOI] [Google Scholar]
- [25].Holman EA, Thompson RR, Garfin DR & Silver RC The unfolding COVID-19 pandemic: a probability-based, nationally representative study of mental health in the United States. Science Advances 6, eabd5390 (2020). 10.1126/sciadv.abd5390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Holingue C et al. Mental distress during the covid-19 pandemic among us adults without a pre-existing mental health condition: Findings from american trend panel survey. Preventive Medicine 139 (2020). 10.1016/j.ypmed.2020.106231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].John A, Pirkis J, Gunnell D, Appleby L & Morrissey J Trends in suicide during the COVID-19 pandemic. BMJ 371, m4352 (2020). 10.1136/bmj.m4352. [DOI] [PubMed] [Google Scholar]
- [28].Pirkis J et al. Suicide trends in the early months of the COVID-19 pandemic: Interrupted time series analysis of preliminary data from 21 countries. The Lancet Psychiatry (2021). 10.1016/S2215-0366(21)00091-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].Tanaka T & Okamoto S Increase in suicide following an initial decline during the COVID-19 pandemic in Japan. Nature Human Behaviour 5, 229–238 (2021). 10.1038/s41562-020-01042-z. [DOI] [PubMed] [Google Scholar]
- [30].Berger LM, Ferrari G, Leturcq M, Panico L & Solaz A COVID-19 lockdowns and demographically-relevant Google Trends: A cross-national analysis. PLOS ONE 16, e0248072 (2021). 10.1371/journal.pone.0248072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Brodeur A, Clark AE, Fleche S & Powdthavee N COVID-19, lockdowns and well-being: evidence from Google Trends. Journal of Public Economics 193, 104346 (2020). 10.1016/j.jpubeco.2020.104346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Silverio-Murillo A, Hoehn-Velasco L, Tirado AR & de la Miyar JRB COVID-19 blues: Lockdowns and mental health-related Google searches in Latin America. Social Science & Medicine 281, 114040 (2021). 10.1016/j.socscimed.2021.114040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Fetzer T, Hensel L, Hermle J & Roth C Coronavirus perceptions and economic anxiety. Review of Economics and Statistics 1–36 (2020). 10.1162/rest_a_00946. [DOI] [Google Scholar]
- [34].Faust JS et al. Suicide deaths during the COVID-19 stay-at-home advisory in Massachusetts, March to May 2020. JAMA Network Open 4, e2034273–e2034273 (2021). 10.1001/jamanetworkopen.2020.34273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Holland KM et al. Trends in US emergency department visits for mental health, overdose, and violence outcomes before and during the COVID-19 pandemic. JAMA Psychiatry 78, 372–379 (2021). 10.1001/jamapsychiatry.2020.4402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [36].Baron EJ, Goldstein EG & Wallace CT Suffering in silence: how COVID-19 school closures inhibit the reporting of child maltreatment. Journal of Public Economics 190, 1–13 (2020). 10.1016/j.jpubeco.2020.104258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [37].Bullinger LR, Carr JB & Packham A COVID-19 and crime: effects of stay-at-home orders on domestic violence. American Journal of Health Economics (2021). 10.1086/713787. [DOI] [Google Scholar]
- [38].Leslie E & Wilson R Sheltering in place and domestic violence: evidence from calls for service during COVID-19. Journal of Public Economics 189, 104241 (2020). 10.1016/j.jpubeco.2020.104241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [39].Dong E, Du H & Gardner L An interactive web-based dashboard to track COVID-19 in real time. The Lancet Infectious Diseases 20, 533–534 (2020). 10.1016/S1473-3099(20)30120-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [40].Hale T et al. A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nature Human Behaviour 5, 529–538 (2021). 10.1038/s41562-021-01079-8. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Data were provided by helplines for the sole purpose of this research project, subject to confidentiality agreements. The full data underlying specific parts of the analysis is available from the authors upon reasonable request and conditional on permission of the respective helplines. Figure source data is provided with this paper. To obtain (updated) helpline data, researchers have to sign agreements with individual helplines, for further information, contact: presse@telefonseelsorge.de (Telefonseelsorge DE), contact@sosamitieparisidf.fr (S.O.S. Amitié), info@deluisterlijn.nl (De Luisterlijn), info@nummergegenkummer.de (Nr. gegen Kummer), federatie@tele-onthaal.be (Tele-Onthaal), telefonseelsorge@edw.or.at (Telefonseelsorge AT), lcicenter@163.com (Hope Line), telefonoamico@telefonoamico.it (Telefono Amico), samarijan@gmail.com (Zaupni Samarijan), hana.regnerova@modralinka.cz (Modrá linka), support@sahar.org.il (Sahar), direccaolphm@gmail.com (S.O.S. Voz Amiga), info@mutes.de (Muslim. Seels.), info@embracelebanon.org (Embrace), info@sosdetresse.lu (SOS Détresse), info@novageneracija.org (Plavi Telefon), sbhkinfo@sbhk.org.hk (Samaritan Befrienders), verband@143.ch (Die Dargebotene Hand), sos-keskus@mieli.fi (MIELI mental health), lesziroda@gmail.com (LESZ), info@vibrant.org, (Lifeline and Disaster Distress Helpline). Data on infection rates and policy measures is publicly available online from the JHU CSSE COVID-19 Dataset at https://github.com/CSSEGISandData, and the Oxford Covid-19 Government Response Tracker at https://github.com/OxCGRT.