

Abstract
Fertility problems are known to exert a negative impact on psychological health. Meanwhile, individuals with fertility challenges often view adoption as a positive healing experience. Yet, a dearth of work has examined the long-term impact that fertility problems have on adoptive parents and their childrearing stress. Here, we investigated how fertility problems related to parenting daily hassle (PDH) trajectories among adoptive mothers and fathers in the Early Growth and Development Study (N = 333). When adopted children were 9 months old, adoptive parents reported whether they had fertility problems prior to their decision to adopt and rated their PDH frequency and intensity on six occasions over the next 7 years. Multilevel models revealed inverse U-shaped curves for PDH among both fertile and infertile parents, such that PDH increased from child age 9 months until about 5 to 6 years and decreased thereafter. Mothers with fertility problems exhibited a steeper PDH incline from 9 months to the peak at child age 5 to 6, but also incurred a swifter subsequent decline. There were no significant differences in fathers’ PDH trajectories based on fertility problems. We discuss why fertility problems appear to impact PDH trajectories for mothers rather than fathers.
Keywords: fertility problems, parenting daily hassles, adoption, childhood, trajectories
There are nearly 1.8 million adopted children in the United States, which accounts for over 2% of the nation’s children (Children’s Bureau, 2016). While there is research on adopted children’s psychological outcomes, the experiences of adoptive parents have been largely neglected both in the scientific literature and practice (Hendry & Netherwood, 2010). In particular, little research has explored the parenthood experience of adoptive parents with consideration of their preadoption experiences. The literature on community-based samples of parents shows that the transition to parenthood is physically taxing and emotionally stressful while simultaneously joyful and fulfilling (Belsky, 1986; Epifanio et al., 2015; Perren et al., 2005). For many adoptive parents, this transition may include additional stress originating from preadoption experiences, including fertility problems (Hendry & Netherwood, 2010; Payne, Fields, Meuchel, Jaffe, & Jha, 2010). In this study, we aim to examine the role of fertility problems on adoptive parents’ decision to adopt and specific experiences related to the perception of parenting stress during the first 7 years of parenthood. Ultimately, our results shed light on the significance of pre-parenthood factors on adoptive parents’ perceptions of parenting stress during early and middle childhood.
Previous studies have defined infertility inconsistently, but a persistent component of its definition is the absence of a live birth for long-term couples (Mascarenhas, Cheung, Mathers, & Stevens, 2012). Although infertility is a medical condition that prevents couples from conceiving or having a child naturally, the ramifications of this diagnosis go beyond biology. Research has shown that fertility problems evoke psychological distress (McQuillan, Greil, White, & Jacob, 2003; Seibel & Taymor, 1982) and relationship conflicts with the partner (McGrath, Samra, Zukowsky, & Baker, 2010). In most societies, married heterosexual couples are expected to reproduce and such expectations can lead to psychological complications when fertility is elusive for couples, as they pose challenges for both social and personal expectations (McGrath et al., 2010). For infertile couples who continue to want to parent a child, one option is adoption.
Qualitative studies have identified that fertility problems are a primary reason for why couples decide to pursue adoption (Goldberg, Downing, & Richardson, 2009). However, knowledge about the prevalence of fertility problems in adoptive parents and its role in adoption motivations are limited, with many studies relying solely on anecdotes from clinical settings (Kupecky & Anderson, 1998). Ivaldi (2000) estimated that 81% of the couples who choose adoption have not had birth children of their own. However, one cannot assume that all or even most of adoptive parents without a biological child are infertile or that infertility is the only reason for the adoption. For instance, a small body of qualitative adoption research reveals that couples cite diverse reasons for their decision to pursue adoption, including providing a positive family environment for a child that has a history of adversity (Zhang & Lee, 2011), familiarity with adoption such as having family or friends who went through the same process (Jennings, Mellish, Tasker, Lamb, & Golombok, 2014), and religious or spiritual beliefs about providing for children (Tyebjee, 2003). Malm and Welti (2010) investigated adoptive parent motivations among adoptive families who used three different types of adoption: foster care, international adoption, and private domestic adoption. The most frequently cited motivations for adoption across the three categories were providing a home for a child (81%), expanding the family (69%), and fertility problems (52%). Among the three types of adoption, fertility problems are most frequently reported in private domestic adoption (89%). The Malm and Welti (2010) study uses the National Survey of Adoptive Parents (NSAF; Bramlett et al., 2010), which includes children who were adopted by grandparents and other relatives. The current study seeks to replicate this investigation using a nonrelative domestic infant adoption sample in the United States. The first goal of this study is, therefore, to provide a systematic description of the prevalence of fertility problems in parents who pursued infant domestic adoption (private and public) and their motivations for pursuing adoption.
How Do Fertility Problems Influence Parenting Stress?
Parenting is a challenging process; one concept that captures such a challenge associated with parenthood is parenting stress (Crnic & Booth, 1991). Parenting stress includes subjective experiences of distress generated from parenting and being a parent (Deater-Deckard, 2008). Previous research has identified that parenting daily hassles (PDH), defined by mundane, everyday hassles related to childrearing, such as difficulties with bedtime or managing the child’s public behavior, are major contributors to distress in parents (Creasey & Reese, 1996), the child (Myers et al., 1992; Coplan, Bowker, & Cooper, 2003), and parent-child relationships (Patterson, 1983; Golombok, MacCallum, & Goodman, 2001). The effect of PDH on parental psychological well-being is robust; it is known to be a better predictor of psychological distress in parents than major stressful life events such as divorce or death of a family member (Dohrenwend & Shrout, 1985). PDH is traditionally measured via its frequency (the number of occurred stressful events) and intensity (the appraisal of its impact), both of which are highly correlated but conceptually distinct (Creasey & Reese, 1996).
According to an emerging line of research, pre-parenthood fertility problems may impact how parents perceive daily parenting tasks (e.g., Daniluk & Hurtig‐Mitchell, 2003; Hamilton, Cheng, & Powell, 2007; McGrath et al., 2010). Two hypotheses have emerged from the literature (i.e., “the distress hypothesis” and “the gratitude hypothesis”), which will be explained in the following two sections.
The Distress Hypothesis
The distress hypothesis posits that adoptive couples’ fertility problems before becoming parents have a negative influence on their psychological well-being, which adversely impacts their behaviors and perceptions about parenting (Groza & Rosenberg, 1998; Wallach & Mahlstedt, 1985). Under this framework, a central challenge associated with fertility problems is a fundamental feeling of loss and inadequacy. These feelings may include the perceived loss of biological children, the acute awareness of discontinuation of one’s genetic lineage, and/or lamentations about the lost opportunity to experience pregnancy (Groza & Rosenberg, 1998), which translates to diminished self-esteem, self-confidence, and security (Wallach & Mahlstedt, 1985). When coupled with stress and uncertainties involving the adoption process (Foli, Hebdon, Lim, & South, 2017; South, Lim, Jarnecke, and Foli, 2019), reaction and negative feelings toward infertility may lead to a perceived decrease in relationship closeness and life satisfaction, which in turn could translate into increased parenting stress after the arrival of an adopted child.
Previous studies identified fertility problems as a risk factor for family conflicts, including parenting and marital problems. For example, Burns (1990) found that parents who underwent fertility treatment were more likely to rate their parenting as overprotective and abusive/neglectful than a comparison group of fertile parents. Moreover, recognizing the infertility experience as a negative event increased marital conflict and the incidence of psychosocial problems (Burns, 1990). Cook, Bradley, and Golombok (1998) compared the parenting quality and stress between families with twins conceived by in vitro fertilization (IVF) and families who had naturally conceived twins. While no differences were found in parenting behavior, IVF parents reported greater stress associated with parenting than their counterparts. Similarly, evidence shows that primiparous IVF mothers tend to report lower self-esteem and less parenting competence than primiparous fertile mothers (Gibson, Ungerer, Tennant, & Saunders, 2000). Therefore, it appears that couples who have had fertility problems experience more stressors and challenges once they become parents (Holditch-Davis, Sandelowski, & Harris, 1998), supporting the distress hypothesis.
There are two issues that are noteworthy about the aforementioned findings. First, the majority of prior studies are based on parents with infants or younger children, failing to identify potential disparities in parenting stress between parents with and without fertility problems later in childhood. Two follow-up studies found no significant differences between infertile (i.e., IVF) and fertile parents’ reports of parenting stress and parental behavior of raising children who are 9 to 10 years (Colpin & Soenen, 2002) and 15–16 years of age (Colpin & Bossaert, 2008). It is speculated that stress related to infertility could dissipate over time as the child grows and as the culture shifts toward the normalization of this conceptualization mode (Colpin & Bossaert, 2008). These studies of older children propose the possibility of a gradual convergence between infertile and fertile parents’ PDH over time, but no longitudinal study has been conducted that follows the trajectories of PDH separately by pre-parenthood fertility status, especially within adoptive samples. Though speculative, the potential reason for the attenuation of differences in parenting stress over time between parents with and without fertility problems is that with time, families constructed through medical (e.g., IVF) and social interventions (e.g., adoption) build a stronger emotional bond and connection among the members, which overrides the negative effects due to pre-parenthood fertility problems. Second, evidence in support of the distress hypothesis has primarily been generated from IVF studies. While IVF studies are informative in examining the role of fertility problems in parenting, IVF has unique characteristics that adoption does not carry. For example, IVF, especially homologous IVF, can make it possible for infertile couples to conceive a child who is genetically related to the mother and/or father, but nonrelative adoption, as used in this study, cannot. Additionally, IVF also brings unique stress to parents such as high financial and physical burden. Therefore, it is currently unknown whether the findings supporting the distress hypothesis can be generalized to adoptive parents.
The Gratitude Hypothesis
The gratitude hypothesis suggests that infertile parents who obtain a child through nonbiological means (including adoption and fertility treatment) are grateful for the arrival of the child and well-prepared for parenthood, which translates into greater parental investment: they are less likely to perceive parenting stressful and more likely to demonstrate a positive attitude toward parenthood (Daniluk & Hurtig‐Mitchell, 2003; Foli et al., 2017; Hamilton, Cheng, & Powell, 2007).
Qualitative studies suggest that couples use their infertility experience as an opportunity for growth in personal and relational domains, such as improved communication (Leiblum, Kemmann, & Lane, 1987) and establishing a closer relationship with the partner who shares this experience (Greil, Leitko, & Porter, 1988). By extending the findings on the potential positive outcomes among those with fertility problems, the main tenet of the gratitude hypothesis is that adoption helps attenuate the stress associated with fertility problems. According to Daniluk and Hurtig‐Mitchell (2003), parents who experience fertility challenges yet manage to have a child – including infertile adoptive parents and patients who seek fertility treatment – often perceive parenthood as a very positive force in their lives. They appear to experience high levels of gratitude and positivity associated with the arrival of the adopted child, which contribute to their greater global well-being (Abbey, Halman, & Andrews, 1992). Compared to parents who conceived naturally, those who underwent fertility treatment exhibit more positive parental investment and attitudes toward parenthood, presumably because the parenting experience is more planned, voluntary, and coordinated (for reviews, see Nelson, Kushlev, & Lyubomirsky, 2014; Natsuaki & Dimler, 2018). As Brodzinsky and Pinderhughes (2005) suggest, in response to the frustration and emotional challenges associated with fertility problems, infertile adoptive parents might feel exceptionally fulfilled after the adopted child joins the family, which might provide a buffer from daily stressors in the early phase of adoptive family life. Accordingly, the gratitude hypothesis posits that infertile adoptive parents would perceive less frequent and less intense PDH than fertile adoptive parents at the arrival of the child, but no prior research has investigated the long-term endurance of such positivity.
Although the gratitude and distress hypotheses may seem contradictive, they may not be mutually exclusive. Presumably, parenthood experience is likely nuanced and multifaceted for all parents and they experience both joy and distress. For those who have faced the challenge of not being able to have a biological child, the distress and gratitude may both be more intense.
A Missing Piece: A Developmental Approach to Fertility Problems and Parenting Stress
A critical omission in the literature is a developmental approach to understanding PDH. According to Crnic and Booth (1991), PDH increases when the child undergoes developmental transitions. During the transition from infancy to the toddler period, children quickly develop greater physical mobility without concomitant increases in cognitive appreciation for basic principles, perspective taking and reasoning, language and self-regulatory skills, as well as awareness of inflicting harm to self or others, including pets and valuable objects (Shaw & Bell, 1993). This disconnection between advances in physical mobility and limited language and cognitive skills often results in increased challenges for parents to manage (Fagot & Kavanaugh, 1993; Shaw & Bell, 1993). Hence, toddlerhood is often referred to by parents as the “terrible twos”. According to Ames (2012), two-and-a-half-year-olds often become more rigid, explosive, and tense, especially when parents need to enforce limits on their behavior because of danger to self and others. The increased use of the command “no” often results in children reacting with heightened emotionality (Ames, 2012). Consistent with the developmental transitions that occur during the toddler period, cross-sectional research examining the differences in parenting stress among couples with infants and toddlers reveals that PDH frequency tends to increase from the age of 9–12 months to 18–24 months and then decrease from 18–24 months to 30–36 months. However, PDH intensity exhibits a consistent increase (Crnic & Booth, 1991), which reaffirms the importance of examining PDH frequency and intensity independently with special attention to the age and developmental needs of children. This pattern of finding implies that it is not only the frequency of stressful events, but also parents’ perceptions of how irritating the situations are change during these transitional periods (Crnic & Booth, 1991). A longitudinal study with slightly older children found that PDH frequency remains highly stable across 6-month periods from ages 3 to 5 years (Crnic, Gaze, & Hoffman, 2005). However, lacking are long-term longitudinal studies that track parents’ perceptions of PDH from infancy through middle childhood.
The absence of a developmental approach is further exacerbated in the literature linking fertility problems and parenting stress. Prior research investigating the impact of fertility problems on PDH among adoptive couples has focused predominantly on the transitional period from experiencing fertility problems to adoption (e.g., Daly, 1999, 2009), rather than its influence over time. However, the effects of stress might accumulate progressively, making some parents even more vulnerable in the long run, especially during transitional periods (Deater‐Deckard, 2005; Crnic et al., 2005). Therefore, the second goal of this study is to track the trajectories of PDH by the preadoption fertility status of adoptive parents.
Parenting Stress by Gender
Although the parenting stress literature often emphasizes mothers’ experiences, there is an increased attention towards fathers due to improved recognition of fathers’ involvement (Davis & Carter, 2008; Deater, Deckard, & Searr, 1996). One study found that fathers of children with disabilities had lower parenting stress when compared to mothers (Esdaile & Greenwood, 2003), while others have found comparable levels of parenting stress across gender (Deater-Deckard & Scarr, 1996; Krauss, 1993). Additionally, past work notes a negative relation between fathers’ parenting stress and life satisfaction during infancy and toddlerhood that was not present among mothers (Crnic & Booth, 1991). However, we are aware of no prior research that has investigated adoptive fathers’ PDH in relation to infertility. As a result, we examined adoptive mothers’ and fathers’ PDH experiences separately.
Potential Covariates: First-time Parenthood and Child Temperament
To isolate the effect of infertility on PDH, we examined two covariates relevant to parents’ perceived stress: (1) first-time parent status and (2) child temperament. We expected first-time parents to perceive higher parenting stress than those with more childrearing experience due to past work finding that parenting style differs based on the child’s birth order (Shebloski et al., 2005). For example, parents often supply greater parental attention, involvement, and, also, discipline to first-born children (Furman & Lanthier, 2002; Hotz & Pantano, 2015; Lutz et al., 2012; Scher & Sharabany, 2005). Controlling for first-time parent status allowed us to confine any effect this may have had on PDH. The literature also indicates that child temperament affects parenting daily stress (Deater-Deckard, Smitha, Ivya, & Petrilb, 2005). For example, Deater-Deckard et al. (2005) found that negative emotionality in children corresponded with increased parenting distress. Nevertheless, parenting hassles uniquely predict child externalizing problems over and above child temperament. For these reasons, we treated first-time parent status and child temperament as covariates.
Present Study
The current study seeks to fill several important gaps in the literature on fertility problems and parenting stress among adoptive parents. First, there is no quantitative description involving a large sample of adoptive parents that evaluates the prevalence of fertility problems and its role in the decision to pursue adoption. Second, it is unclear whether and to what extent fertility problems are associated with perceptions of parenting stress in the years following adoption. Finally, most of the prior research on fertility issues and parenthood are based on female participants/mothers, while fathers’ experience is understudied.
The following hypotheses were formulated. First, we hypothesized that fertility problems would emerge as a prevalent issue in adoptive parents and a common reason for pursuing adoption. Second, we predicted that PDH frequency and intensity would gradually increase from infancy to toddlerhood (at approximately the age of 2 to 3 years) and then remain stable thereafter for adoptive parents. Third, we explored an integrative view concerning the impact of fertility problems on the perceptions of trajectories of PDH. Combining the distress and gratitude hypotheses, we expected that parents with fertility problems might experience more frequent and intense PDH in infancy and toddlerhood, but less frequent and intense PDH subsequently. Although we do not have any specific hypothesis that differentiate mothers’ and fathers’ PDH experiences, we explored the aforementioned hypotheses for adoptive mothers and fathers separately.
Method
Participants
The analytical sample consisted of 333 adoptive mother-father dyads who participated in Cohort I of the Early Growth and Development Study (EGDS; Leve et al., 2019). The EGDS is a prospective, longitudinal adoption study that follows birth and adoptive families linked through nonrelative infant adoption. The families included in this study are all adoptive families, but 15% of these families also have biological children at home (n = 53). Participants were recruited from 33 adoption agencies in the United States at three sites: the Mid-Atlantic, the West/Southwest, and the Pacific Northwest, between 2003 and 2010 (Leve et al., 2019).
The EGDS adopted children (57.3% males) were placed in adoptive homes at a median age of 2.0 days old (SD = 14.7). Fifty-eight percent of the adopted children were Caucasian, 21% were mixed-race, 11% were Black or African American, 9% were Hispanic or Latino, and 2% were unknown. The mean ages of adoptive mothers and fathers at the first wave of data collection (i.e., child’s age of 9 months) were 38.6 years (SD = 5.5) and 39.3 years (SD = 5.8), respectively. More than 90% of adoptive parents were Caucasian, college educated and middle class (see Leve et al., 2019 for study details).
The current investigation is based on the first six waves of EGDS when adoptive children were 9 months, 18 months, 27 months, 4.5 years, 6 years, and 7 years old. Data were collected through both home visit assessments and online questionnaires. Out of the EGDS Cohort I sample of 361 adoptive parents, same-sex parents (n = 20) and single parents (n = 5) were asked to skip the infertility question and were therefore not included in the analysis. This exclusion led to a final sample size of 333 adoptive mother-father dyads.
Measures
Adoptive parents’ fertility problems.
At the first in-person adoptive family interview (i.e., child’s age of 9 months), adoptive parents reported whether they had difficulty conceiving or carrying a baby to term using a dichotomous scale (1 = yes, 0 = no). Mothers and fathers were asked to complete the questionnaire independently using computers. The correlation of fertility problems between adoptive mothers and fathers is 0.24 (p < .001). Self-reported fertility problems have been used in previous fertility problems literature (Chandra et al., 2005; McQuillan et al., 2003) and is considered to be more inclusive than formal diagnoses of fertility problems (e.g., Daly, 1988), as not all couples who face fertility challenges seek treatment.
Reasons for pursuing adoption.
At the 9-month in-person interview, we asked adoptive mothers and fathers to provide their reasons for adopting a child, with fertility problems being one response option. Using a four-point Likert scale (1 = not at all, 2 = a little bit, 3 = pretty much, 4 = a lot), each parent rated his/her agreement with a list of statements, such as “I was or my partner was adopted” and “My partner or I was not able to have a child biologically” (see Table 1 for the full list of items). Higher values indicated that the statement represented a more relevant reason for adoption.
Table 1.
Adoptive Mothers’ and Fathers’ Motivations for Adoption (in percentages)
| How much does this statement reflect your reason for pursuing an adoption plan? | Not at all | A little bit | Pretty much | A lot | ||||
|---|---|---|---|---|---|---|---|---|
| M | F | M | F | M | F | M | F | |
| I wanted to be a parent. | 2.5 | 6.6 | 3.1 | 5.0 | 7.1 | 18.9 | 86.2 | 68.6 |
| My partner and I were unable to have a child biologically. | 8.6 | 9.5 | 10.2 | 9.8 | 11.1 | 15.2 | 68.8 | 64.2 |
| I wanted to provide a home for a child who needs it. | 14.8 | 11.7 | 33.2 | 35.0 | 20.3 | 23.3 | 30.5 | 29.0 |
| I always planned to adopt a child. | 44.0 | 60.6 | 28.9 | 22.1 | 9.8 | 8.5 | 15.7 | 6.9 |
| I have parents, friends or other family members who have adopted. | 41.8 | 44.2 | 34.5 | 34.7 | 8.9 | 8.8 | 13.5 | 11.4 |
| I am or my partner was adopted. | 90.2 | 91.1 | 2.5 | 3.2 | 0.6 | 1.6 | 4.9 | 3.2 |
| I am concerned about overpopulation. | 74.8 | 73.5 | 18.2 | 18.6 | 2.5 | 5.0 | 3.4 | 1.9 |
| I (my spouse/romantic partner) did not want to be pregnant. | 85.8 | 81.0 | 8.0 | 6.6 | 1.8 | 2.8 | 2.8 | 1.9 |
| My partner and I were recruited to become adoptive parents. | 94.8 | 93.4 | 2.5 | 2.8 | 0.9 | 1.9 | 0.6 | 0.6 |
Note. M = mother; F = father.
Parenting daily hassles (PDH).
Across all six waves, adoptive mothers and fathers independently responded to a 20-item measure of potentially stressful everyday events that involve children or parenting (Crnic & Greenberg, 1990). Measures were mailed out for the first three waves and collected online for the last three waves. Mothers and fathers rated how often a given daily hassle occurred on a five-point scale (the frequency scale; 1 = rarely, 2 = sometimes, 3 = a lot, 4 = constantly, 5 = does not apply) and how hassled they felt each event was (the intensity scale; 1= no hassle to 5 = big hassle). Sample survey items included “the baby/child/kid(s) resist or struggle over bedtime with you,” “the baby/child/kid(s)’ schedules interfere with meeting your own or household needs,” and “the baby/child/kid(s) are hard to manage in public (grocery store, shopping center, restaurant)”. Two summary scales were constructed from the measure: PDH frequency, which reflects the existence of stressors, and PDH intensity, which is indicative of perceived stressfulness (Crnic et al., 2005). Higher scores indicated greater frequency and intensity of perceived PDH. The reliability of the frequency scale across waves ranged from α = .72 – .85 for adoptive mothers and α = .69 – .88 for adoptive fathers. The reliability of the intensity scale across waves ranged from α = .84 – .91 for adoptive mothers and α = .87 – .92 for adoptive fathers.
Covariates.
In addition to the basic demographic characteristics, we considered two covariates that might affect parenting stress: first-time parenthood status and the adopted child’s difficult temperament. In this study, adoptive mothers provided a list of family members living in the household when the child joins the family. Using the family roster, we created a dichotomous variable representing whether there are other children in the family before the adoptee joins the family (0 = no, 1 = yes). Accordingly, the reference group (0) indicates first-time parents. To control for a child’s difficult temperament, adoptive mothers and fathers independently reported on the Difficultness factor (e.g., “how easy or difficult is it for you to calm or soothe your baby when s/he is upset”) of the Infant Characteristics Questionnaire (ICQ: Bates, Freeland, & Lounsbury, 1979) at the child’s age of 9 months. The reliability of this 6-item subscale was α = .82 for adoptive mothers and α = .81 for adoptive fathers. We included a mother-report of ICQ when analyzing maternal PDH and a father-report of ICQ when analyzing paternal PDH.
The results from bivariate correlations revealed that the first-time parenthood status and child fussiness were correlated with PDH frequency across six waves (for mothers, rs range from .15 to .58 and from .14 to .31, respectively; for fathers, rs range from .17 to .56 and from .12 to .26, respectively) and intensity (for mothers, rs range from .13 to .61 and from .12 to .30, respectively; for fathers, rs range from .11 to .56 and from .17 to .28, respectively). Thus, these two variables were included as covariates in subsequent analyses.
Data Analysis
Missing data analysis.
The retention rates of adoptive parents across six waves were high, with 99%, 98%, 94%, 86%, 86%, and 83%, respectively. The percentage of missingness on any study variable ranges from 6% to 36%. Little’s Missing Completely at Random (MCAR) test revealed that all the variables were missing completely at random, χ2(27, N = 333) = 2084.86, p = .09. We also conducted a series of t-tests comparing those who had no missing data with those who had at least one missing data point across waves. The results did not show any significant differences, except that at child age 7 years, adoptive fathers who had at least one missing study variable (M = 34.69, SD = 9.22) showed lower levels of PDH frequency than those who had no missing data (M = 37.79, SD = 8.04), t(335) = 2.62, p = .01.
Descriptive Statistics.
First, to examine the prevalence of infertility issues among adoptive parents, we evaluated the descriptive information regarding reasons behind adoptive parents’ decision to adopt a child and adoptive mothers’ and fathers’ self-reported infertility problems. Second, to explore how PDH change over time, we evaluated the descriptive statistics on PDH over six waves for mothers and fathers, separately.
Multilevel modeling.
To estimate the age trajectories of PDH across time, we performed a sequence of multilevel modeling using SAS PROC MIXED (Singer, 1998; Singer, Willett, & Willett, 2003). The estimated parameters of main effects are parallel to unstandardized coefficients in multiple regression analyses, which indicate the increase or decrease in PDH as a function of a child’s age (in years). We first tested an unconditional means model with intercept and linear slope, then added a quadratic age term, and estimated with the maximum likelihood (ML) estimation procedure with an unstructured covariance matrix. We identified the shape of PDH trajectories from 9 months to 7 years, separately for mothers and fathers. To avoid multicollinearity between the intercept and the slope for the polynomial models (McElreath, 2020), we centered PDH at the age of 18 months, and consequently, the intercept was interpreted as the average PDH when the adopted child was 18 months old. Once the shape of the PDH trajectories was determined, we added fertility problems as a level-2 predictor. To choose between models, a chi-square test was conducted to compare the indexes of −2 residual log likelihood.
Results
Reasons to Adopt a Child and Prevalence of Fertility Problems
Reasons for adoption.
Table 1 presents the reported reasons for adoption among mothers and fathers. The majority of adoptive parents (80% of mothers and 79% of fathers) reported not being able to have a child biologically reflects “pretty much” or “a lot” of their reason for adoption. Additional prominent reasons for adoption were the desire to be a parent (93% of mothers and 88% of fathers) and the desire to provide a home for a child in need (51% of mothers and 52% of fathers).
Prevalence of fertility problems.
Among 333 adoptive couples, 302 (90%) adoptive mothers and 286 (83%) fathers reported having experienced fertility challenges. Among these individuals, a majority (83%) considered fertility problems to be a primary reason for adoption.
Trajectories of Parenting Daily Hassles by Fertility Status
Descriptive statistics.
The means and standard deviations of PDH frequency and intensity are presented in Table 2 for adoptive mothers and fathers, separated by fertility status. As a result of the high prevalence of fertility problems in adoptive families, we have unequal sample sizes for fertile (n = 31) and infertile (n = 302) mothers, as well as fertile (n = 47) and infertile (n = 286) fathers. For both groups of parents with and without fertility problems, the trajectories of adoptive mothers’ PDH frequency and intensity appeared to follow a curvilinear trend, which was at the lowest when the adopted child was 9 months old, peaked around age 4.5 years, and then gradually declined thereafter (Figure 1). The longitudinal change of adoptive fathers’ PDH frequency and intensity by fertility problems experience mirrored this pattern (Figure 2).
Table 2.
Means and Standard Deviations Parenting Daily Hassles among Adoptive Parents
| 9 months | 18 months | 27 months | 4.5 years | 6 years | 7 years | |||
|---|---|---|---|---|---|---|---|---|
| Adoptive Mothers N=333 |
Frequency | Infertile | 32.13a | 37.80 | 39.85 | 41.05b | 38.85 | 38.57 |
| (9.46) | (6.95) | (6.55) | (6.86) | (7.06) | (7.09) | |||
| Fertile | 35.97a | 39.29 | 38.76 | 38.33b | 39.60 | 38.38 | ||
| (11.89) | (8.48) | (9.81) | (5.78) | (6.47) | (7.06) | |||
| Intensity | Infertile | 30.67c | 36.97 | 39.15 | 42.19 | 39.72 | 39.68 | |
| (12.98) | (10.61) | (10.24) | (10.29) | (10.70) | (11.22) | |||
| Fertile | 36.31c | 39.11 | 40.47 | 41.68 | 41.40 | 41.11 | ||
| (14.82) | (12.25) | (12.66) | (8.48) | (10.23) | (10.64) | |||
| Adoptive Fathers N=333 |
Frequency | Infertile | 30.68 | 35.94 | 38.57 | 39.30 | 37.79 | 38.02 |
| (10.48) | (7.27) | (7.33) | (7.30) | (7.35) | (8.23) | |||
| Fertile | 30.71 | 35.62 | 37.46 | 37.70 | 35.11 | 37.54 | ||
| (11.35) | (10.32) | (7.91) | (7.28) | (7.40) | (7.98) | |||
| Intensity | Infertile | 29.12 | 34.84 | 37.32 | 38.68 | 38.14 | 38.07 | |
| (12.96) | (8.94) | (10.49) | (10.67) | (10.71) | (11.49) | |||
| Fertile | 29.68 | 35.34 | 37.10 | 38.07 | 35.18 | 37.14 | ||
| (12.87) | (11.82) | (11.13) | (9.15) | (10.64) | (10.23) |
Note. Shared subscripts represent statistically significant difference at p < .05.
Infertile adoptive mothers n = 302; Infertile adoptive fathers n = 286.
Figure 1.
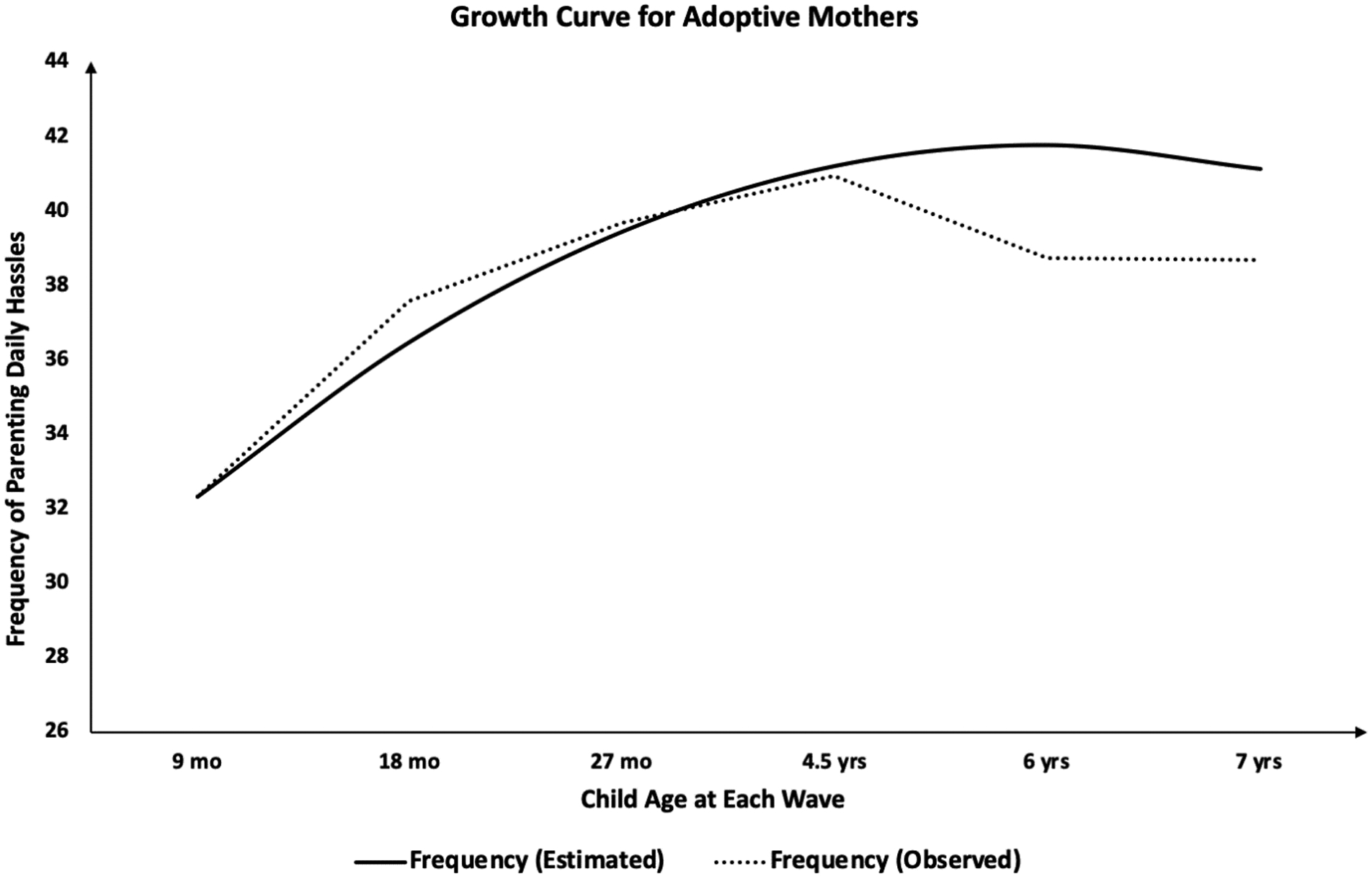
Growth Curve of Parenting Daily Hassle Frequency among Adoptive Mothers (Model 0b).
Figure 2.
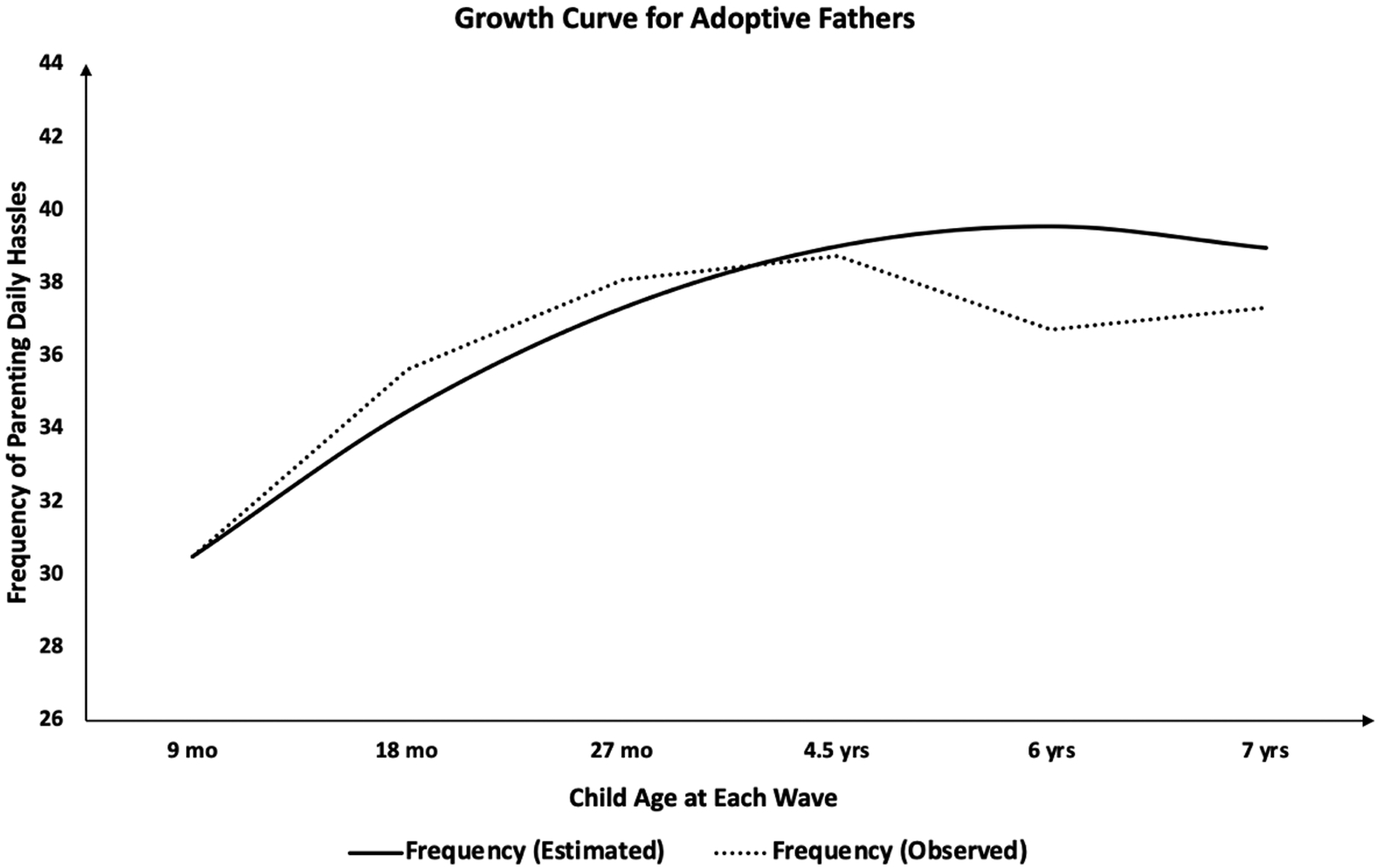
Growth Curve of Parenting Daily Hassle Frequency among Adoptive Fathers (Model 0b).
A two-way repeated measures ANOVA was then conducted to examine the impact of fertility problems on PDH at the six times of assessment. While only the main effect of age was significant for adoptive fathers, F(5, 730) = 110.14, p < .001, the results for adoptive mothers indicated both a significant main effect of age, F(5, 804) = 51.76, p < .001, and a significant fertility problems × age interaction effect, F(5, 804) = 9.82, p < .001. We then conducted pairwise comparisons using Tukey’s HSD test to examine the differences between mothers with or without fertility problems at each wave (Table 2). The results showed that at child age 9 months and 4.5 years, adoptive mothers’ PDH were different by fertility status: mothers with fertility problems (M = 32.13, SD = 9.46) had significantly less frequent PDH than fertile mothers (M = 35.97, SD = 11.89) at 9 months, t(1, 284) = −2.04, p = .04, while at 4.5 years, mothers with fertility issues (M = 41.22, SD = 7.07) had more frequent PDH than fertile mothers (M = 38.33, SD = 5.78), t(1, 220) = 1.84, p = .05. Regarding PDH intensity, mothers with fertility challenges (M = 30.47, SD = 12.98) had less intense PDH than fertile mothers (M = 36.31, SD = 14.82), t(1, 284) = −2.22, p = .03, only when children were 9 months old.
Age trajectories of PDH.
To estimate the PDH trajectories over time, we performed multilevel modeling. Results are shown in Table 3 for mothers and Table 4 for fathers. As shown in Model 0a in Table 3, the linear age term for mothers’ PDH was positive and significant (γs = .80, 1.21, both p < .001 for frequency and intensity, respectively), indicating that PDH increased over the course of childhood. Similar results were found among fathers (Table 4, Model 0a; γs = .83, 1.11, both p < .001 for frequency and intensity, respectively). Both the estimated between- and within-person variances were significant among mothers (, , , all p < .001 for frequency; , , , all p < .001 for intensity) and fathers (, , , all p < .001 for frequency; , , , all p < .001 for intensity).
Table 3.
Fixed and Random Coefficients for Trajectories of parenting daily hassles among Adoptive Mothers
| Model 0a | Model 0b | |||||||
|---|---|---|---|---|---|---|---|---|
| Frequency | Intensity | Frequency | Intensity | |||||
| Coefficients | SE | Coefficients | SE | Coefficients | SE | Coefficients | SE | |
| Intercept | 36.36** | 0.39 | 35.32** | 0.56 | 36.48** | 0.39 | 35.45** | 0.56 |
| Fertility problemsa | — | — | — | — | — | — | — | — |
| Age | 0.80** | 0.09 | 1.21** | 0.11 | 3.56** | 0.22 | 4.17** | 0.28 |
| Fertility problems × Age | — | — | — | — | — | — | — | — |
| Age2 | — | — | — | — | −0.60** | 0.04 | −0.65** | 0.05 |
| Fertility problems × Age2 | — | — | — | — | — | — | — | — |
| Variance Components | ||||||||
| Level 1 | ||||||||
| Within-person | 1.15** | 0.36 | 2.07** | 0.61 | 6.02** | 2.15 | 9.82** | 2.15 |
| Level 2 | ||||||||
| In intercept | 40.55** | 5.51 | 87.98** | 10.68 | 42.61** | 8.06 | 89.63** | 8.06 |
| In linear slope | −3.59** | 1.20 | −5.83** | 2.14 | −9.80** | 3.04 | −15.56** | 3.04 |
| Goodness-of-fit | ||||||||
| −2 Residual log likelihood | 10994.1 | 11930.0 | 10694.4 | 11730.5 | ||||
Note. Covariates (child fussiness and first-time parenthood status) are not included in the table.
Fertility problems= 0 for fertile adoptive mothers, 1 for infertile adoptive mothers.
p < .05;
p < .01.
Table 4.
Fixed and Random Coefficients for Trajectories of Parenting Daily Hassles among Adoptive Fathers
| Model 0a | Model 0b | |||||||
|---|---|---|---|---|---|---|---|---|
| Frequency | Intensity | Frequency | Intensity | |||||
| Coefficients | SE | Coefficients | SE | Coefficients | SE | Coefficients | SE | |
| Intercept | 34.30** | 0.42 | 33.06** | 0.54 | 34.47** | 0.41 | 33.22** | 0.54 |
| Fertility problemsa | — | — | — | — | — | — | — | — |
| Age | 0.83** | 0.09 | 1.11** | 0.12 | 3.40** | 0.23 | 3.60** | 0.32 |
| Fertility problems × Age | — | — | — | — | — | — | — | — |
| Age2 | — | — | — | — | −0.57** | 0.04 | −0.55** | 0.06 |
| Fertility problems × Age2 | — | — | — | — | — | — | — | — |
| Variance Components | ||||||||
| Level 1 | ||||||||
| Within-person | 1.25** | 0.42 | 2.36** | 0.79 | 7.32** | 1.49 | 12.72** | 2.83 |
| Level 2 | ||||||||
| In intercept | 47.06** | 6.28 | 77.37** | 10.16 | 47.71** | 4.40 | 78.54** | 7.41 |
| In linear slope | −4.05** | 1.40 | −5.28** | 2.37 | −11.89** | 1.89 | −12.54** | 2.83 |
| Goodness-of-fit | ||||||||
| −2 Residual log likelihood | 10533.4 | 11365.1 | 10306.1 | 11238.6 | ||||
Note. Covariates (child fussiness and first-time parenthood status) are not included in the table.
Fertility problems = 0 for fertile adoptive fathers, 1 for infertile adoptive fathers.
p < .05;
p < .01.
Then, in Model 0b, we added a quadratic age term to capture the curvilinear nature of the change, which was observed in the descriptive statistics described earlier (Table 2). For mothers, both the positive coefficients of the linear age term (γs= 5.12, 5.68, both p < .001, for frequency and intensity, respectively) and the negative coefficients of the quadratic age term (γs = −0.60, −0.65, both p < .001 for frequency and intensity, respectively) were significant, indicating inverse U-shaped curves for PDH in childhood, peaking at age 5.9 years for frequency and at age 6.2 years for intensity (Table 3; Figure 1). The PDH of fathers mirrored this result (Table 4, Model 0b; γs = 3.40, 3.60, both p < .001 for linear coefficients of frequency and intensity, respectively; γs = −0.57, −0.55, both p < .001 for quadratic coefficients of frequency and intensity, respectively), with the frequency peaking at age 5.9 years and the intensity peaking at age 6.3 years (Figure 2). Both the estimated between- and within-person variances were significant among mothers (, , , all p < .001 for frequency; , , , all p < .001 for intensity) and fathers (, , , all p < .001 for frequency; , , , all p < .001 for intensity).
To assist our choice between Models 0a and 0b, we compared their −2 residual log likelihood for mothers and fathers independently. The chi-square difference test suggested that Model 0b displayed significantly lower indexes of −2 residual log likelihood (p <.05), indicating that Model 0b had a better fit than Model 0a for mothers. Similarly, Model 0b revealed superiority for fathers (p <.05). Given the support for the curvilinear age trend, we applied Model 0b as our base unconditional growth model.
Effect of fertility problems on the PDH trajectories.
Model 1 was then employed to include fertility problems as a predictor of PDH trajectories and child fussiness and first-time parenthood status as covariates (Table 5). The results indicated that adoptive mothers’ PDH frequency was significantly higher at 18 months when the adopted child was perceived to have higher fussiness (γ = .34, p < .001) or adoptive mothers were not first-time parents (γ = 5.36, p < .001). The results for maternal PDH intensity mirrored these patterns (γs = .50 and 8.88, respectively, both p < .001) for fussiness and first-time parenthood status.
Table 5.
Fixed and Random Coefficients for Trajectories of Parenting Daily Hassles among Adoptive Parents
| Adoptive Mother (Model 1) | Adoptive Father (Model 1) | |||||||
|---|---|---|---|---|---|---|---|---|
| Frequency | Intensity | Frequency | Intensity | |||||
| Coefficients | SE | Coefficients | SE | Coefficients | SE | Coefficients | SE | |
| Intercept | 29.10** | 1.53 | 24.83** | 2.42 | 28.07** | 1.48 | 23.17** | 1.91 |
| Fertility problemsa | 0.18 | 1.12 | −0.48 | 1.62 | 0.69 | 1.07 | 0.03 | 1.35 |
| Age | 1.17* | 0.72 | 1.91* | 0.96 | 3.12** | 0.63 | 3.56** | 0.87 |
| Fertility problems × Age | 2.60** | 0.76 | 2.49** | 1.01 | 0.33 | 0.69 | 0.07 | 0.95 |
| Age2 | −0.19* | 0.13 | −0.27* | 0.17 | −0.51** | 0.12 | −0.58** | 0.16 |
| Fertility problems × Age2 | −0.45** | 0.13 | −0.43 | 0.18 | −0.06 | 0.13 | 0.04 | 0.17 |
| Variance Components | ||||||||
| Level 1 | ||||||||
| Within-person | 5.81** | 0.37 | 9.93** | 0.65 | 7.15** | 0.44 | 14.35** | 0.85 |
| Level 2 | ||||||||
| In intercept | 26.13** | 4.13 | 55.94** | 7.87 | 32.78** | 5.21 | 50.68** | 7.96 |
| In linear slope | −3.31** | 1.04 | −3.57** | 1.90 | −6.53** | 1.32 | −1.38** | 2.21 |
| Goodness-of-fit | ||||||||
| −2 Residual log likelihood | 9418.0 | 10358.0 | 8687.8 | 9439.4 | ||||
Note. Covariates (child fussiness and first-time parenthood status) are not included in the table.
Fertility problems = 0 for fertile adoptive mothers, 1 for infertile adoptive mothers.
p < .05;
p < .01.
For mothers, the main effect of fertility problems was not significant for neither PDH frequency (γ = .18, p = .88) nor intensity (γ = −.48, p = .77). The interactions between fertility problems and linear age terms were positive and statistically significant for both PDH frequency (γ = 2.60, p < .001) and intensity (γ = 2.49, p = .01), and the interactions between maternal fertility problems and quadratic age terms were negative and statistically significant for both PDH frequency (γ = −.45, p < .001) and intensity (γ = −.43, p = .02), suggesting that mothers with fertility problems established significantly faster growth before reaching the peak and a faster decline afterward. Figure 3 depicts this trend.
Figure 3.
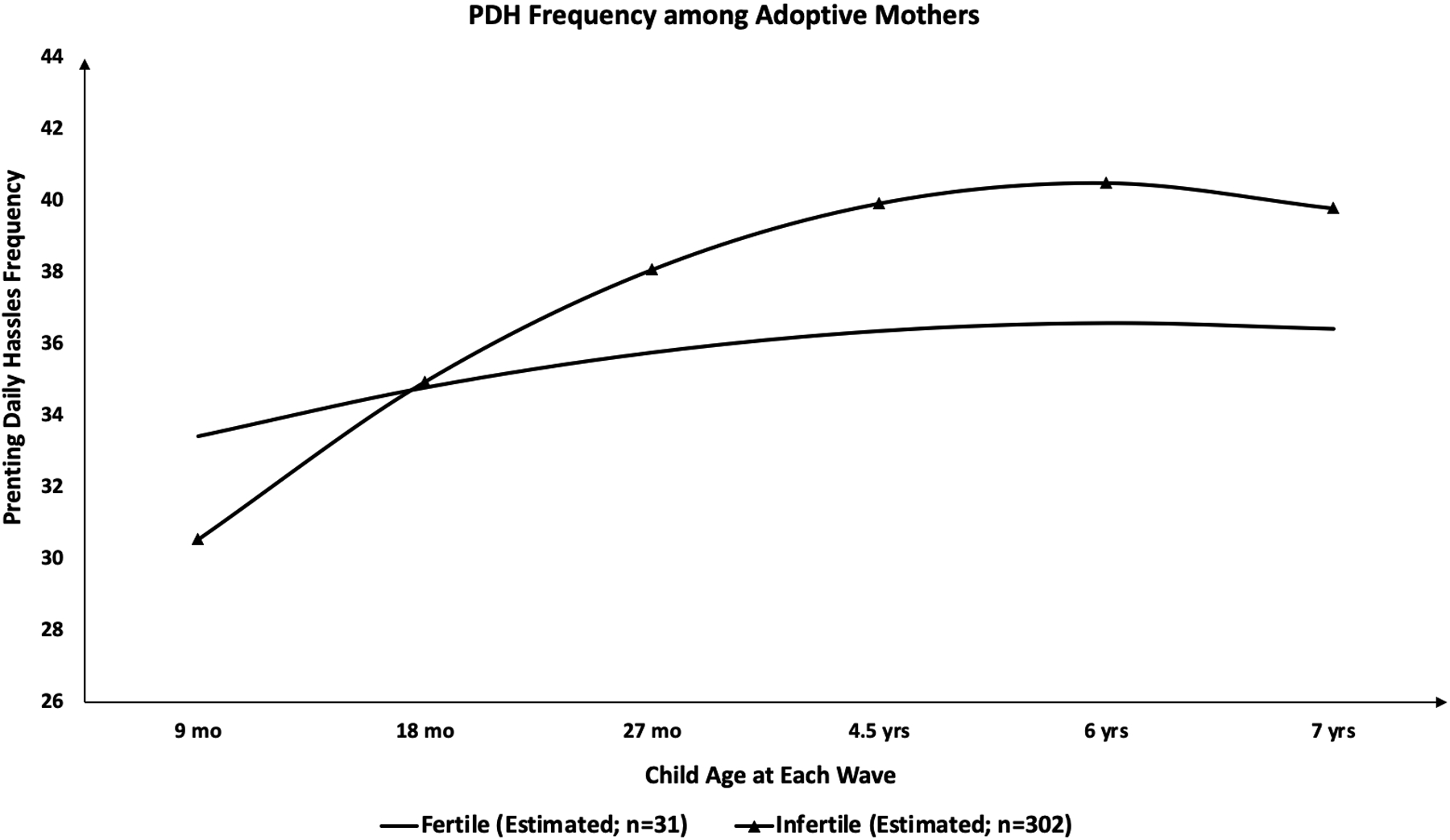
Frequency of Parenting Daily Hassles among Adoptive Mothers (Model 1).
However, the effects of fertility problems were not reflected among adoptive fathers (Figure 4). They established the same patterns as mothers concerning covariates: both PDH frequency and intensity at 18 months were higher if the child was fussier (γ = .23, p = .002 for frequency and γ = .42, p < .001 for intensity) or if adoptive fathers are not first-time parents (γs = 6.06, 8.86, both p < .001 for frequency and intensity, respectively). However, fertility problems was not predictive of the fathers’ PDH trajectories, as none of the main effects of fertility problems (γ = .69, p = .52 for frequency; γ = .03, p = .98 for intensity), the interactions between fertility problems and linear age terms (γ = .33, p = .64 for frequency; γ = .07, p = .94, for intensity), or the interactions between fertility problems and quadratic age terms (γ = −.06, p = .64 for frequency; γ = 0.04, p = .84 for intensity) was statistically significant (Table 5).
Figure 4.
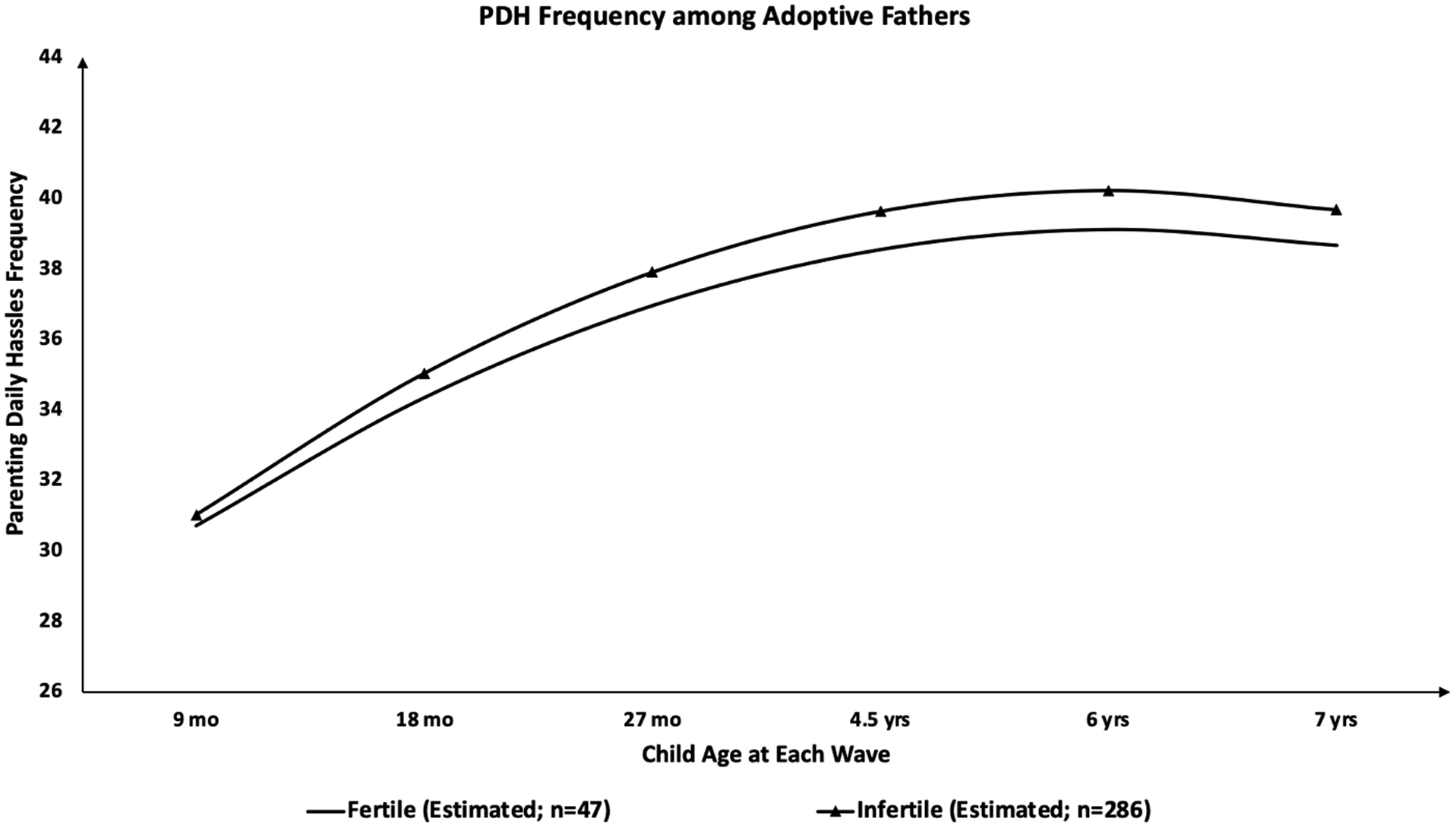
Frequency of Parenting Daily Hassles among Adoptive Fathers (Model 1).
Discussion
Parenting daily hassles is a meaningful construct for evaluating some components of stress in the context of rearing children (Crnic & Greenburg, 1990). Despite a growing body of research pertaining to parenting stress in adoptive families, little attention has been devoted to investigating its trajectories from infancy to childhood with consideration of pre-parenthood fertility problems. The current study examined associations between fertility problems and levels of adoptive mothers’ and fathers’ PDH over the first 7 years of parenthood.
Trajectories of PDH over the First 7 Years of a Child’s Life
The results indicate inverse U-shaped PDH trajectories for both adoptive mothers and fathers, with PDH frequency and intensity increasing from 9 months to child age 5.9 years to 6.3 years and declining subtly thereafter. The peaks seem to correspond to the children’s entry into kindergarten (around age 5) and elementary school (around age 6). Perhaps this is a challenging transitional time for both children and parents that requires adjustment to new family arrangements and life roles (Turnbull & Turnbull, 2001). The entry of the child into school may be especially challenging for adoptive families because through school activities (e.g., family trees) and peer interaction, children become more conscious of their adoption history where the psychological effects of the biological differences might pose additional hassles for adoptive parents (Hoopes, 1990).
Our findings extend previous cross-sectional studies (Crnic & Booth, 1991) and a shorter-term longitudinal study (Crnic et al., 2005). Existing longitudinal evidence has shown the stability of PDH from ages 3 to 5 years (Crnic et al., 2005), but we observed that PDH continues to increase until approximately the age of 6 years in both frequency and intensity. This inconsistency between previous studies and our study may result from various methodological reasons, including samples and measures. Our study is exclusively on adoptive parents’ experiences, which may slightly differ from the experiences of biological parents. Therefore, we conducted a follow-up analysis (a t-test between adoptive parents and biological parents) to compare parenting stress between these two groups. Results (not shown) suggested that our adoptive parents reported less PDH than biological parents (Crnic & Booth, 1991) at infancy and toddlerhood; thus, the PDH trajectories in our sample may have had more ‘room’ to increase. This difference between adoptive and biological parents might be explained by the gratitude hypothesis: adoptive parents are less likely to perceive parenting stressful because they are especially grateful for the arrival of the child and are more prepared for parenthood.
The Effect of Fertility Problems on Parenting Stress
Another major aim of this investigation is to evaluate the impact of pre-parenthood fertility problems on how parents perceive and experience PDH. Our results indicate that fertility problems are differentially associated with PDH for adoptive mothers and fathers. For mothers, the ANOVA results suggest that infertile mothers exhibit less frequent and less intense PDH compared to the fertile group at 9 months. This finding is consistent with the gratitude hypothesis, which posits that there is a heightened ‘honeymoon’ period for infertile parents after the adopted child joins the family (Brodzinsky & Pinderhughes, 2005).
Findings from the multilevel modeling analysis, however, illustrate that from the age of 9 months to the age of 5.9–6.2 years, mothers with fertility issues seem to experience a greater increase in parenting hassles than fertile mothers. This accelerated change in PDH may reflect that mothers who had fertility problems experience continued struggles after the adoptees join the family (Daly, 1988; Holditch-Davis et al., 1998). Such a pattern is consistent with previous research demonstrating that fertility problems have a long-term emotional impact that may reappear over time, creating further challenges for adoptive parents (Hendry & Netherwood, 2010), such as depression (Wallach & Mahlstedt, 1985), constant worry that the biological parents might take the child back, and a feeling of loss and anger from being deprived of the chance of becoming a biological parent (Daly, 1988).
Altogether, our findings provide support for the hybrid of distress and gratitude hypotheses for adoptive mothers who experienced fertility problems. Their PDH is lower than fertile mothers in infancy, but shows a faster increase in early childhood. However, this heightened distress eventually dissipates. After the peak around age 6, both PDH frequency and intensity among mothers with fertility problems decrease faster and drop to a similar level as the fertile mothers at age 7. This finding expands previous literature in examining the long-term effects of fertility problems, revealing that its impact diminishes in the long run for adoptive mothers.
For adoptive fathers, however, fertility problems were unrelated to their PDH trajectories, neither for the initial level nor for the pace of change. Previous research demonstrated that compared to mothers, fathers are more resistant to stress generated from family-related issues, including parenting stress and fertility problems. For instance, an examination of changes in PDH in families of young children with intellectual disabilities suggests that mothers’ parenting stress increases significantly from the child’s age of 30 to 60 months, while fathers’ stress level remains more constant (Gerstein, Crnic, Blacher, & Baker, 2009). Furthermore, multiple studies illustrated that women usually experience more psychological distress from fertility problems compared to men, including higher levels of anxiety, depression, hostility, cognitive disturbances, and stress (Ulbrich, Coyle, & Llabre, 1990; Wright et al., 1991). The emotional toll of fertility problems that women carry may be rooted in concerns such as the physical and psychological cost and invasiveness of women’s infertility treatment (Whiteford & Gonzalez, 1995), a societal emphasis on motherhood as a primary role for women (Greil, 1991), and an implicit but pervasive assumption that infertility treatment involves only women (Abbey, Halman, & Andrews, 1992). However, it is noteworthy that the discrepancy between mothers and fathers as a result of fertility problems may be confounded with reporter bias: research has shown that fathers tend to feel less comfortable discussing fertility problems compared to mothers (Jordan & Revenson, 1999).
Limitations
The results should be interpreted with the following caveats. First, we used parents’ self-reports to identify infertile versus fertile adoptive parents. Given the highly personal and sensitive nature of the question, fertility problems are typically measured via self-report in nonclinical research (e.g., McQuillan et al., 2003; Steuber & Solomon, 2008). However, there is a wide variation in the experiences of fertility problems, from receiving formal diagnoses to unsuccessful conception after years of trying to conceive without seeking medical treatment. Those referred to as infertile parents in the current study self-claimed to have had fertility problems but did not necessarily receive formal diagnoses. In our sample, 35% of self-identified infertile mothers and 40% of self-identified infertile fathers received formal diagnoses. There are also various reasons for infertility, some eliminate the possibility of reproduction (e.g., chemotherapy), while others can be treated by IVF or surrogacy (e.g., low egg or sperm count and quality). Though we were not able to explore personal reasons for infertility, future work should examine how these experiences impact PDH. In addition, our fertility measure was based on a single item that defined infertility as including both difficulties conceiving a child and obstetric issues (e.g., miscarriages). Future studies should include various items representing different aspects of infertility, as this may influence participants’ responses (Larsen, 2005). We also relied solely on self-reports to assess PDH. Therefore, the parenting stress captured in this study is parents’ own perceptions rather than a more objective frequency and intensity of parenting stress. Finally, most adoptive parents in our study reported fertility problems, which led to a smaller fertile parent sample. Future research should endeavor to collect more proportionate fertile and infertile parent groups.
A final remark is that our finding by no means suggests any deficiency in parenting among infertile adoptive parents. While parenting stress differs depending on fertility experiences, parenting behavior may not, the latter of which was not included in the current report. According to prior work, no evidence supports the negative impact of fertility problems on parenting behavior (Holditch-Davis et al., 1998). As Allen et al. (1996) suggest, while mothers’ experience of fertility problems can be challenging for their transition to parenthood, it is not necessarily detrimental to the child’s development. Similarly, for fathers, those with a history of fertility problems – especially those who chose to adopt a child – are known to be more involved in interacting with their infants and share in the responsibility of taking care of the child with their parenting partner(s) (Holditch-Davis et al., 1999).
Conclusions
The current research expands the existing literature on the trajectories of parenting stress by tracking adoptive parents from the child’s age of 9 months to 7 years, depicting an inverse U-shaped curve. Our results illustrate the importance of pre-parenthood factors, such as fertility problems and the couples’ decision on how to form a family, in predicting motherhood experience. Future research should investigate parenting experience with consideration of the predictive role of pre-parenthood factors and family dynamics.
References
- Abbey A, Halman LJ, & Andrews FM (1992). Psychosocial, treatment, and demographic predictors of the stress associated with infertility. Fertility and Sterility, 57(1), 122–128. [DOI] [PubMed] [Google Scholar]
- Allen KD, Maguire KD, Williams GE, & Sanger WG (1996). The effects of fertility problems on parent-child relationships and adjustment. Children’s Health Care, 25(2), 93–105. [Google Scholar]
- Ames LB (2012). Your two-year-old: Terrible or Tender. Dell. [Google Scholar]
- Bates JE, Freeland CAB, & Lounsbury ML (1979). Measurement of infant difficultness. Child Development, 794–803. [PubMed] [Google Scholar]
- Belsky J (1986). Transition to parenthood. Medical Aspects of Human Sexuality. [Google Scholar]
- Bramlett MD, Foster EB, Frasier AM, Satorius J, Skalland BJ, Nysse-Carris KL, et al. (2010). Design and Operation of the National Survey of Adoptive Parents, 2007. National Center for Health Statistics. Vital Health Statistics, 1(50), 1–154. [PubMed] [Google Scholar]
- Brodzinsky DM, & Pinderhughes E (2005). Parenting and child development in adoptive families. Handbook of Parenting, 1, 279–311. [Google Scholar]
- Burns LH (1990). An exploratory study of perceptions of parenting after fertility problems. Family Systems Medicine, 8(2), 177. [Google Scholar]
- Chandra A, Martinez GM, Mosher WD, Abma JC, & Jones J (2005). Fertility, family planning, and reproductive health of U.S. women: data from the 2002 national survey of family growth. DHHS Publication, 23(25). [PubMed] [Google Scholar]
- Child Welfare Information Gateway. (2016). Trends in U.S. adoptions: 2008–2012. Washington, DC: U.S. Department of Health and Human Services, Children’s Bureau. [Google Scholar]
- Colpin H, & Bossaert G (2008). Adolescents conceived by IVF: parenting and psychosocial adjustment. Human Reproduction, 23(12), 2724–2730. [DOI] [PubMed] [Google Scholar]
- Colpin H, & Soenen S (2002). Parenting and psychosocial development of IVF children: a follow-up study. Human Reproduction, 17(4), 1116–1123. [DOI] [PubMed] [Google Scholar]
- Cook R, Bradley S, & Golombok S (1998). A preliminary study of parental stress and child behaviour in families with twins conceived by in-vitro fertilization. Human Reproduction (Oxford, England), 13(11), 3244–3246. [DOI] [PubMed] [Google Scholar]
- Coplan RJ, Bowker A, & Cooper SM (2003). PDH, child temperament, and social adjustment in preschool. Early Childhood Research Quarterly, 18(3), 376–395. [Google Scholar]
- Creasey G, & Reese M (1996). Mothers’ and fathers’ perceptions of parenting hassles: Associations with psychological symptoms, nonparenting hassles, and child behavior problems. Journal of Applied Developmental Psychology, 17(3), 393–406. [Google Scholar]
- Crnic KA, & Booth CL (1991). Mothers’ and fathers’ perceptions of daily hassles of parenting across early childhood. Journal of Marriage and the Family, 53(4), 1042–1050. [Google Scholar]
- Crnic KA, Gaze C, & Hoffman C (2005). Cumulative parenting stress across the preschool period: Relations to maternal parenting and child behaviour at age 5. Infant and Child Development: An International Journal of Research and Practice, 14(2), 117–132. [Google Scholar]
- Crnic KA, & Greenberg MT (1990). Minor parenting stresses with young children. Child Development, 61(5), 1628–1637. [DOI] [PubMed] [Google Scholar]
- Daly K (1988). Reshaped parenthood identity: The transition to adoptive parenthood. Journal of Contemporary Ethnography, 17(1), 40–66. [Google Scholar]
- Daly KJ (1999). Crisis of genealogy: Facing the challenges of fertility problems. In McCubbin HI, Thompson EA, Thompson AI, & Futrell J (Eds.), The Dynamics of Resilient Families (pp. 1–40). Sage. [Google Scholar]
- Daly K (2009). Preparation needs of infertile couples who seek to adopt. Canadian Journal of Community Mental Health, 8(1), 111–121. [Google Scholar]
- Daniluk JC, & Hurtig‐Mitchell J (2003). Themes of hope and healing: Infertile couples’ experiences of adoption. Journal of Counseling and Development, 81(4), 389–399. [Google Scholar]
- Davis NO, & Carter AS (2008). Parenting stress in mothers and fathers of toddlers with autism spectrum disorders: Associations with child characteristics. Journal of Autism and Developmental Disorders, 38(7), 1278. [DOI] [PubMed] [Google Scholar]
- Deater-Deckard K (2008). Parenting stress. Yale University Press. [Google Scholar]
- Deater‐Deckard K (2005). Parenting stress and children’s development: Introduction to the special issue. Infant and Child Development: An International Journal of Research and Practice, 14(2), 111–115. [Google Scholar]
- Deater-Deckard K, & Scarr S (1996). Parenting stress among dual-earner mothers and fathers: Are there gender differences?. Journal of Family Psychology, 10(1), 45. [Google Scholar]
- Deater‐Deckard K, Smith J, Ivy L, & Petril SA (2005). Differential perceptions of and feelings about sibling children: Implications for research on parenting stress. Infant and Child Development: An International Journal of Research and Practice, 14(2), 211–225. [Google Scholar]
- Dohrenwend BP, & Shrout PE (1985). “ Hassles” in the conceptualization and measurement of life stress variables. American Psychologist, 40(7), 780–785. [Google Scholar]
- Epifanio MS, Genna V, De Luca C, Roccella M, & La Grutta S (2015). Paternal and Maternal Transition to Parenthood: The Risk of Postpartum Depression and Parenting Stress. Pediatric Reports, 7(2). 10.4081/pr.2015.5872 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Esdaile SA, & Greenwood KM (2003). A comparison of mothers’ and fathers’ experience of parenting stress and attributions for parent–child interaction outcomes. Occupational Therapy International, 10(2), 115–126. [DOI] [PubMed] [Google Scholar]
- Fagot BI, & Kavanagh K (1993). Parenting during the Second Year: Effects of Children’s Age, Sex, and Attachment Classification. Child Development, 64(1), 258–271. [DOI] [PubMed] [Google Scholar]
- Foli KJ, Hebdon M, Lim E, & South SC (2017). Transitions of adoptive parents: A longitudinal mixed methods analysis. Archives of Psychiatric Nursing, 31(5), 483–492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Furman W, & Lanthier R (2002). Parenting siblings. In Bornstein MH (Ed), Handbook of Parenting: Vol.1: Children and Parenting (2nd ed.) (pp. 165–188). Mahwah, NJ: Lawrence Erlbaum Associates, Publishers. (xxxviii, 418 pp). [Google Scholar]
- Gerstein ED, Crnic K, Blacher J, & Baker BL (2009). Resilience and the course of daily parenting stress in families of young children with intellectual disabilities. Journal of Intellectual Disability Research, 53(12), 981–997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gibson FL, Ungerer JA, Tennant CC, & Saunders DM (2000). Parental adjustment and attitudes to parenting after in vitro fertilization. Fertility and Sterility, 73(3), 565–574. [DOI] [PubMed] [Google Scholar]
- Goldberg AE, Downing JB, & Richardson HB (2009). The transition from fertility problems to adoption: Perceptions of lesbian and heterosexual couples. Journal of Social and Personal Relationships, 26(6–7), 938–963. [Google Scholar]
- Golombok S, MacCallum F, & Goodman E (2001). The “Test‐Tube” Generation: Parent–Child Relationships and the Psychological Well‐Being of In Vitro Fertilization Children at Adolescence. Child Development, 72(2), 599–608. [DOI] [PubMed] [Google Scholar]
- Greil AL (1991). Not yet pregnant: Infertile couples in contemporary America. Rutgers University Press. [Google Scholar]
- Greil AL, Leitko TA, & Porter KL (1988). Fertility problems: His and hers. Gender and Society, 2(2), 172–199. [Google Scholar]
- Groza V, & Rosenberg KF (Eds.). (1998). Clinical and practice issues in adoption: bridging the Gap between adoptees placed as infants and as older children. Praeger Publishers. [Google Scholar]
- Hamilton L, Cheng S, & Powell B (2007). Adoptive parents, adaptive parents: Evaluating the importance of biological ties for parental investment. American Sociological Review, 72(1), 95–116. [Google Scholar]
- Hendry A, & Netherwood P (2010). A child at last: Adoption after fertility problems. In Crawshaw M & Balen R (Eds.), Adopting after fertility problems: Messages from practice, research, and personal experience (pp. 151–163). Jessica Kingsley Publishers. [Google Scholar]
- Holditch-Davis D, Sandelowski M, & Harris BG (1999). Effect of infertility on mothers’ and fathers’ interactions with young infants. Journal of Reproductive and Infant Psychology, 17(2), 159–173. [Google Scholar]
- Holditch-Davis D, Sandelowski M, & Harris BG (1998). Fertility problems and early parent–infant interactions. Journal of Advanced Nursing, 27(5), 992–1001. [DOI] [PubMed] [Google Scholar]
- Hoopes JL (1990). Adoption and identity formation. The Psychology of Adoption, 144–166. [Google Scholar]
- Hotz VJ, & Pantano J (2015). Strategic parenting, birth order, and school performance. Journal of Population Economics, 28(4), 911–936. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ivaldi G (2000). Surveying Adoption: A comprehensive analysis of local authority adoptions 1998–1999 (England). London: British Agencies for Adoption and Fostering. [Google Scholar]
- Jennings S, Mellish L, Tasker F, Lamb M, & Golombok S (2014). Why adoption? Gay, lesbian, and heterosexual adoptive parents’ reproductive experiences and reasons for adoption. Adoption Quarterly, 17(3), 205–226. [Google Scholar]
- Jordan C, & Revenson TA (1999). Gender differences in coping with fertility problems: a meta-analysis. Journal of Behavioral Medicine, 22(4), 341–358. [DOI] [PubMed] [Google Scholar]
- Krauss MW (1993). Child-related and parenting stress: Similarities and differences between mothers and fathers of children with disabilities. American Journal on Mental Retardation, 97, 393–404. [PubMed] [Google Scholar]
- Kupecky R, & Anderson KJ (1998). Fertility problems and adoption. In Groza V & Rosenberg KF (Eds.), Clinical and practice issues in adoption: Bridging the gap between adoptees placed as infants and as older children (pp. 21–36). Greenwood Publishing Group, Inc. [Google Scholar]
- Larsen U (2005). Research on infertility: which definition should we use?. Fertility and Sterility, 83(4), 846–852. [DOI] [PubMed] [Google Scholar]
- Leiblum SR, Kemmann E, & Lane MK (1987). The psychological concomitants of in vitro fertilization. Journal of Psychosomatic Obstetrics and Gynecology, 6(3), 165–178. [Google Scholar]
- Leve LD, Neiderhiser JM, Ganiban JM, Natsuaki MN, Shaw DS, & Reiss D (2019). The early growth and development study: A dual-family adoption study from birth through adolescence. Twin Research and Human Genetics, 1–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lutz KF, Burnson C, Hane A, Samuelson A, Maleck S, & Poehlmann J (2012). Parenting Stress, Social Support, and Mother-Child Interactions in Families of Multiple and Singleton Preterm Toddlers. Family Relations, 61(4), 642–656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Malm K, & Welti K (2010). Exploring motivations to adopt. Adoption Quarterly, 13(3–4), 185–208. [Google Scholar]
- Mascarenhas MN, Cheung H, Mathers CD, & Stevens GA (2012). Measuring infertility in populations: constructing a standard definition for use with demographic and reproductive health surveys. Population Health Metrics, 10(1), 17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McBride BA, Schoppe SJ, & Rane TR (2002). Child characteristics, parenting stress, and parental involvement: Fathers versus mothers. Journal of Marriage and Family, 64(4), 998–1011. [Google Scholar]
- McElreath R (2020). Statistical rethinking: A Bayesian course with examples in R and Stan. CRC press. [Google Scholar]
- McGrath JM, Samra HA, Zukowsky K, & Baker B (2010). Parenting after fertility problems: issues for families and infants. MCN: The American Journal of Maternal/Child Nursing, 35(3), 156–164. [DOI] [PubMed] [Google Scholar]
- McQuillan J, Greil AL, White L, & Jacob MC (2003). Frustrated fertility: Fertility problems and psychological distress among women. Journal of Marriage and Family, 65(4), 1007–1018. [Google Scholar]
- Myers HF, Taylor S, Alvy KT, Arrington A, & Richardson MA (1992). Parental and family predictors of behavior problems in inner-city black children. American Journal of Community Psychology, 20(5), 557–576. [DOI] [PubMed] [Google Scholar]
- Natsuaki MN, & Dimler LM (2018). Pregnancy and child developmental outcomes after preimplantation genetic screening: a meta-analytic and systematic review. World Journal of Pediatrics, 14(6), 555–569. [DOI] [PubMed] [Google Scholar]
- Nelson SK, Kushlev K, & Lyubomirsky S (2014). The pains and pleasures of parenting: When, why, and how is parenthood associated with more or less well-being?. Psychological Bulletin, 140(3), 846–895. [DOI] [PubMed] [Google Scholar]
- Patterson GR (1983). Stress: A change agent for family process. In Garmezy N & Rutter M (Eds.), Stress, coping and development in children (pp. 235–264). Johns Hopkins University Press. [Google Scholar]
- Payne JL, Fields ES, Meuchel JM, Jaffe CJ, & Jha M (2010). Post adoption depression. Archives of Women’s Mental Health, 13(2), 147–151. [DOI] [PubMed] [Google Scholar]
- Perren S, Wyl A. von, Bürgin D, Simoni H, & Klitzing K. von. (2005). Depressive symptoms and psychosocial stress across the transition to parenthood: Associations with parental psychopathology and child difficulty. Journal of Psychosomatic Obstetrics & Gynecology, 26(3), 173–183. [DOI] [PubMed] [Google Scholar]
- Scher A, & Sharabany R (2005). Parenting Anxiety and Stress: Does Gender Play a Part at 3 Months of Age? The Journal of Genetic Psychology, 166(2), 203–214. [DOI] [PubMed] [Google Scholar]
- Seibel MM, & Taymor ML (1982). Emotional aspects of fertility problems. Fertility and Sterility, 37(2), 137. [DOI] [PubMed] [Google Scholar]
- Shaw DS, & Bell RQ (1993). Developmental theories of parental contributors to antisocial behavior. Journal of Abnormal Child Psychology, 21, 493–518. [DOI] [PubMed] [Google Scholar]
- Shebloski B, Conger KJ, & Widaman KF (2005). Reciprocal links among differential parenting, perceived partiality, and self-worth: A three-wave longitudinal study. Journal of Family Psychology, 19(4), 633–642. [DOI] [PubMed] [Google Scholar]
- Singer JD (1998). Using SAS PROC MIXED to fit multilevel models, hierarchical models, and individual growth models. Journal of Educational and Behavioral Statistics, 23(4), 323–355. [Google Scholar]
- Singer JD, Willett JB, & Willett JB (2003). Applied longitudinal data analysis: Modeling change and event occurrence. Oxford university press. [Google Scholar]
- South SC, Lim E, Jarnecke AM, & Foli KJ (2019). Relationship quality from pre-to postplacement in adoptive couples. Journal of Family Psychology, 33(1), 64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steuber KR, & Haunani Solomon D (2008). Relational uncertainty, partner interference, and fertility problems: A qualitative study of discourse within online forums. Journal of Social and Personal Relationships, 25(5), 831–855. [Google Scholar]
- Tyebjee T (2003). Attitude, interest, and motivation for adoption and foster care. Child Welfare, 82(6), 685–706. [PubMed] [Google Scholar]
- Ulbrich PM, Coyle AT, & Llabre MM (1990). Involuntary childlessness and marital adjustment: His and hers. Journal of Sex and Marital Therapy, 16(3), 147–158. [DOI] [PubMed] [Google Scholar]
- Wallach EE, & Mahlstedt PP (1985). The psychological component of fertility problems. Fertility and Sterility, 43(3), 335–346. [DOI] [PubMed] [Google Scholar]
- Whiteford LM, & Gonzalez L (1995). Stigma: the hidden burden of fertility problems. Social Science & Medicine, 40(1), 27–36. [DOI] [PubMed] [Google Scholar]
- Wright J, Duchesne C, Sabourin S, Bissonnette F, Benoit J, & Girard Y (1991). Psychosocial distress and fertility problems: men and women respond differently. Fertility and Sterility, 55(1), 100–108. [PubMed] [Google Scholar]
- Zhang Y, & Lee GR (2011). Intercountry versus transracial adoption: Analysis of adoptive parents’ motivations and preferences in adoption. Journal of Family Issues, 32(1), 75–98. [Google Scholar]