

Abstract
[Purpose] Floating toe is a condition in which the toes make insufficient contact with the ground. Weak muscle strength is reportedly one cause of floating toe. However, little evidence exists regarding the relationship between foot muscle strength and floating toe. Here we examined the relationship between foot muscle strength and floating toe by investigating the children’ lower extremity muscle mass and floating toe conditions. [Participants and Methods] This cohort study enrolled 118 8-year-old children (62 females, 56 males) with recorded footprints and muscle mass evaluations using dual-energy X-ray absorptiometry. We calculated the floating toe score using the footprint. We measured the muscle weights and the muscle weights divided by the lengths of the lower limbs separately on the left and right sides using dual-energy X-ray absorptiometry. [Results] No significant correlations were observed between the floating toe score and muscle weights or muscle weights divided by lower-limb lengths for either gender or side. [Conclusion] In this study, no significant correlation was found between floating toe degree and lower limb muscle mass, suggesting that lower limb muscle strength is not the primary cause of floating toe, at least in children.
Keywords: Floating toe, Footprint, Dual-energy X-ray absorptiometry (DEXA)
INTRODUCTION
Floating toe (FT) is defined as a condition, in which the toes are in insufficient contact with the ground in the standing position, and the weight does not shift to the toe while walking1). FT has recently been considered one of the causes of toe dysfunction1, 2). Originally, FT was reported as a complication of surgery and is one of the most common complications of Weil osteotomy3, 4). Previous studies have reported that FT results from excessive dorsiflexion or a lack of plantarflexion of the metatarsophalangeal joints5,6,7). According to some Japanese studies, FT influences dynamic body balance, walking stride length, and walking speed1, 8).
While FT is reportedly very common among children, with an estimated incidence rate of approximately 40.3–98.7% in Japanese children2, 7, 9), its frequency decreases in adults. Increased muscle strength has been speculated as a reason for the decline in FT with aging. Tasaka et al. reported that a group of children with FT tended to have weak foot muscle strength and that FT improves as the foot muscle power increases with growth7). A few reports have suggested that muscle weakness in the lower extremities is the cause of FT; however, the evidence that weak muscle is the cause of FT in children is lacking, and the details remain unclear.
We have previously reported the lack of correlation between total body muscle weight measured by a body composition analyzer and the degree of FT10). However, the limitations of this previous report have been noted, where the total body muscle weight and foot morphology were compared, and the correlation between the muscle weight that is localized to the lower limb and foot condition was not examined.
We hypothesized that if weak lower limb muscle strength causes FT, then, there will be a correlation between lower limb muscle weight and the condition of FT. Accordingly, this study aimed to clarify the relationship between lower limb muscle weight and the FT condition in children.
PARTICIPANTS AND METHODS
The Japan Environment and Children’s Study (JECS) is a national project funded directly by the Ministry of the Environment in Japan; it is a birth cohort study undertaken to elucidate the influence of environmental factors during the fetal period and early childhood on children’s health, with follow-up examinations until the age of 13 years. Details of the protocol and baseline data of the JECS are available in a previous report11). In our institution, an additional survey was conducted for children aged 8 years among JECS participants living in Yamanashi prefecture. This additional survey included ophthalmologic or oral investigations, evaluation of foot posture using the foot pressure plate, or evaluation of bone mineral density and muscle mass using dual-energy X-ray absorptiometry (DEXA) in some of the participants of this cohort study. The Ethics Committee of our institution approved this additional survey (Approval No.: 2020). Written informed consent was obtained from the participants’ mothers or their partners in accordance with the Declaration of Helsinki.
Among the 960 children (age, 8 years) who participated in this additional survey conducted at our institution between July 2019 and March 2021, parents of 821 children were approached for consent after examining and evaluating foot posture. Parents of only 118 children (62 female and 56 male individuals) consented to the examination using DEXA and were included in the study.
The body height was measured and recorded in centimeters to the nearest millimeter; it was measured to the nearest 0.1 kg using an electronic weighing scale, with the participants wearing shorts and a T-shirt. FT was assessed using a foot pressure plate (Win-Pod, Medicapteurs, Balma, France). The method of measuring FT was the same as mentioned previously9). The following is a summary of the method. All participants were instructed to maintain an upright standing position on the plate, barefoot, with their arms hanging by their sides and their feet parallel to each other. They were tested twice with their eyes open, each test lasting 20 s. The inspection was performed using the postural mode that displayed the average foot pressure for 20 s. Based on a previous report1, 9, 10), the FT score was calculated using the image of the plantar footprint. If a toe appeared clearly in the image, 2 points were assigned; if the appearance was unclear, 1 point was assigned; and if it did not appear, 0 points were given for each toe. The total score of each toe was recorded as the FT score out of 20 points (Fig. 1). The FT score was evaluated with the footprint obtained from the two measurements, and the average of the two measurements was used.
Fig. 1.
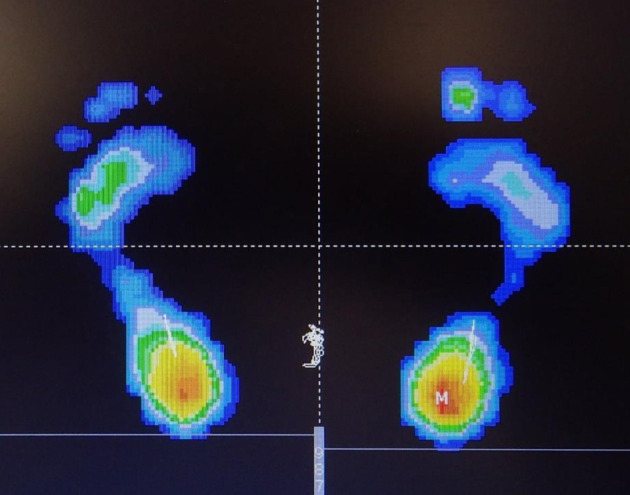
Example of plantar foot print and floating toe score.
One green and one blue toe on the right foot and four blue toes on the left foot resulted in a floating toe (FT) score of 7 points in this case.
The weights of the muscles (MW) of the lower limbs were measured separately on the left and right sides using DEXA (Horizon Wi, Hologic, Marlborough, MA, USA). The region of interest set for measuring lower extremity muscle mass was performed by a skilled radiologist (Fig. 2). Additionally, the weight of the muscles divided by the height (A-MW: muscle weight adjusted for height) was also evaluated.
Fig. 2.
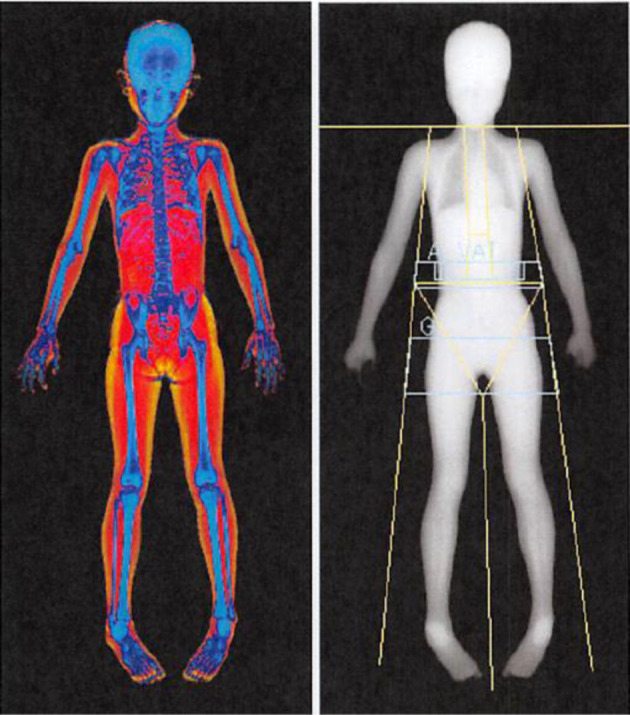
Measuring muscle weight with dual-energy X-ray absorptiometry (DEXA).
The measurement area was set up and measured by a skilled radiologist as shown in the figure.
To evaluate the intraobserver agreement for the FT score, the same reader (T. F.) repeated the measurements of 10 randomly selected plantar footprints during two sessions at least 1 month apart. A second reader (M.W.) repeated the measurements for the same 10 participants for interobserver agreement. Interobserver and intraobserver reliabilities for FT scores were assessed by estimating the intraclass correlation coefficients (ICCs) along with 95% confidence intervals (CIs) using an ICC (2,1) modeling scheme. The unpaired t-test was used to investigate the gender differences of each parameter. The paired t-test was used to examine the differences in FT score and muscle volume. Spearman’s correlation coefficient was used to investigate the correlations between the FT score and muscle weight. The level of statistical significance was set at p<0.05.
RESULTS
The interobserver and intraobserver reliabilities of the FT score of the 10 randomly selected participants were 0.970 (95% CI, 0.887–0.993) and 0.995 (95% CI, 0.981–0.999), respectively. These values indicated substantial agreement (ICC, >0.9). The height and weight of all participants are presented in Table 1. There were no significant gender-specific differences in height and weight; none of these participants had extreme body postures.
Table 1. Height and weight of all participants.
| Total (n=118) | Female (n=62) | Male (n=56) | |
| Height (cm) | 124.9 ± 4.5 | 124.1 ± 4.4 | 125.5 ± 4.5 |
| Weight (kg) | 25.3 ± 4.8 | 24.7 ± 4.4 | 25.8 ± 5.1 |
Mean ± SD.
The lower extremity muscle weight measured by DEXA was significantly higher in male participants and on the right side in both sexes (Table 2). The results of the FT score by side and gender are also presented in Table 2. There was no significant difference in FT scores between the left and right sides or between female and male individuals. Table 3 shows the correlations between the FT score and lower limb muscle weight and lower limb muscle weight/height. No significant correlations were observed between them for either gender or both sides.
Table 2. Lower extremity muscle weight in both genders.
| Female (n=62) | Male (n=56) | |||
| Right | Left | Right | Left | |
| MW (g) | 2,518.9 ± 414* | 2,466.2 ± 400.4 | 2,799.8 ± 460.9* | 2,739.9 ± 456.7 |
| A-MW | 102.6 ± 10.3* | 100.42 ± 9.8 | 109.8 ± 11.9* | 107.6 ± 12.8 |
| FT score | 1.86 ± 1.4 | 1.89 ± 1.3 | 1.84 ± 1.7 | 1.66 ± 1.8 |
Mean ± SD.
MW: muscle weight; A-MW: muscle weight adjusted for height (muscle weight/height); FT score: floating toe score.
*p<0.05 (paired t-test, between right and left).
Table 3. Spearman’s correlation coefficient between FT score and lower limb muscle weight and lower limb muscle weight/height.
| Female (n=62) | Male (n=56) | |||
| Right | Left | Right | Left | |
| MW | −0.102 | 0.110 | 0.006 | −0.076 |
| A-MW | −0.090 | 0.161 | 0.077 | −0.064 |
FT: floating toe; MW: muscle weight; A-MW: muscle weight adjusted for height (muscle weight/height).
DISCUSSION
The current study indicated that Japanese 8-year-old children had very small FT scores. Although the definition of FT varies across reports, Fukuyama et al. reported that a score of <10 points indicates FT1). Based on this definition, most of the participants in this study had FT. Furthermore, the current study indicated no significant correlation between lower limb muscle weight and the degree of FT. FT is an originally reported condition that occurs as a complication of Weil osteotomy3, 4), and FT has been highlighted as a possible cause of toe dysfunction in recent studies1, 2). Some previous reports have shown a high frequency of FT in children, ranging from 40.3–98.7%, although the definition of FT differs in each report. Araki et al. examined FT in children aged 3–5 years and reported that the frequency of cases with at least one FT was 87.7–98.7%2). Tasaka et al. examined FT in children aged 9–11 years and reported that the frequency of cases without the toe contacting the ground was 40.3%7). Fujimaki et al., in their study of 396 cases of 8-year-old children, reported that 97.7% of female and 95.6% of male individuals had FT9). FT in children is highly prevalent; however, the frequency varies widely. This may be because the definition of the FT has not been defined in each report. Using the definition reported by Fukuyama et al., 114 of the 118 cases (96.6%) in the current study were classified as FT, a very high percentage as in previous reports.
Although some reports have suggested that FT is caused by insufficient muscle strength in the foot, there is still little evidence explaining the relationship between lower limb muscle strength and FT, although reports in children are scarce. Tasaka et al. defined FT as feet in which all the toes are not grounded. They reported that toe flexion strength was significantly weaker in the FT group of children than in the non-FT group7). However, as aforementioned, the definition of FT has not yet been established; hence, comparing the groups with and without FT may be inappropriate. If the definitions of FT were to be changed slightly, the difference between the two groups would also change. To evaluate the relationship between FT and foot muscle strength, it would be more desirable to examine the correlation between the degree of FT and toe flexion strength. We believe that we have assessed the relationship between FT and muscle strength more accurately because we used scores to assess the correlation rather than comparing the two groups. The current study showed no significant correlation between FT and lower limb muscle weight. This suggests that the cause of FT is not caused by insufficient muscle strength in the foot, at least in children.
Our study had several limitations. First, we approximated muscle strength with muscle mass and did not measure the actual lower extremity strength. Lower extremity muscle weights are also not measured in a way that is limited to the muscles that move the toes. However, Lindemann et al. reported that the muscle volume, as assessed using magnetic resonance imaging, is correlated with lower limb muscle strength12); the findings of Sheth et al. in previously conducted animal studies corroborate this idea, suggesting that the muscle volume is correlated with muscle strength13). Therefore, we believe that the muscle weight measured in the present study is a good approximation of the muscle strength of the foot. We would like to conduct further research on the correlation between the toe flexion strength measured by the instrument and the lower limb muscle weight measured by DEXA. Second, as there was no standardized method for evaluating FT, we could not accurately compare it with previous similar reports on FT. Thus, the establishment of a simple evaluation system with less measurement error is expected.
Moreover, in the cohort where our additional study was conducted, in addition to footprint and body composition, we also interviewed the participants concerning their exercise habits and the results of sports tests conducted at school. In the future, we would like to investigate the relationship between these factors and FT and clarify the relationship between FT and the motor functions of the foot and the entire body.
Notably, this study was conducted as an Adjunct Study to the Ministry of the Environment’s JECS. The conclusions of this article are solely the responsibility of the authors and do not represent the official views of the above government body.
Based on the current findings, we report that FT was very frequent in 8-year-old children, with no significant correlation between the degree of FT and lower limb muscle mass. Hence, it can be suggested that lower limb muscle strength was not the primary cause of FT, at least among children.
Funding and Conflict of interest
None.
Acknowledgments
We are grateful to all the participants of the JECS-Y and all individuals involved in data collection. We also thank the following members of the JECS-Y as of 2020: Zentaro Yamagata (Principal investigator, e-mail: zenymgt@yamanashi.ac.jp), Ryoji Shinohara, Sanae Otawa, Anna Kobayashi, Sayaka Horiuchi, and Megumi Kushima (Center for Birth Cohort Studies, Interdisciplinary Graduate School of medicine, University of Yamanashi, Chuo, Japan); Takeshi Inukai and Emi Sawanobori (Department of Pediatrics, School of Medicine, University of Yamanashi, Chuo, Japan); Kyoichiro Tsuchiya (Third Department of Internal Medicine, University of Yamanashi, Chuo, Japan); Takahiko Mitsui (Department of Urology, Interdisciplinary Graduate School of Medicine, University of Yamanashi, Chuo, Japan); Kenji Kashiwagi (Department of Ophthalmology, University of Yamanashi, Chuo, Japan); Daijyu Sakurai and Hiroyuki Watanabe (Department of Otorhinolaryngology-Head and Neck Surgery, School of Medicine, University of Yamanashi, Chuo, Japan); Koichiro Ueki and Naana Baba (Department of Oral and Maxillofacial Surgery, Interdisciplinary Graduate School of Medicine, University of Yamanashi, Chuo, Japan); and Hiroshi Yokomichi, Kunio Miyake, Yuka Akiyama, Tadao Ooka, and Reiji Kojima (Department of Health Sciences, School of Medicine, University of Yamanashi, Chuo, Japan). We also would like to thank Editage (www.editage.com) for English language editing.
REFERENCES
- 1.Fukuyama K, Maruyama H: Occurrence of floating toe from the viewpoint of the structure of foot arch. J Phys Ther Sci, 2011, 23: 33–36. [Google Scholar]
- 2.Araki T, Masuda T, Jinno T, et al. : Incidence of floating toe and its association with the physique and foot morphology of Japanese children. J Phys Ther Sci, 2015, 27: 3159–3162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hofstaetter SG, Hofstaetter JG, Petroutsas JA, et al. : The Weil osteotomy: a seven-year follow-up. J Bone Joint Surg Br, 2005, 87: 1507–1511. [DOI] [PubMed] [Google Scholar]
- 4.Migues A, Slullitel G, Bilbao F, et al. : Floating-toe deformity as a complication of the Weil osteotomy. Foot Ankle Int, 2004, 25: 609–613. [DOI] [PubMed] [Google Scholar]
- 5.Trnka HJ, Nyska M, Parks BG, et al. : Dorsiflexion contracture after the Weil osteotomy: results of cadaver study and three-dimensional analysis. Foot Ankle Int, 2001, 22: 47–50. [DOI] [PubMed] [Google Scholar]
- 6.Perez HR, Reber LK, Christensen JC: The role of passive plantar flexion in floating toes following Weil osteotomy. J Foot Ankle Surg, 2008, 47: 520–526. [DOI] [PubMed] [Google Scholar]
- 7.Tasaka S, Matsubara K, Nishiguchi S, et al. : Association between floating toe and toe grip strength in school age children: a cross-sectional study. J Phys Ther Sci, 2016, 28: 2322–2325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Saito R, Okamoto S, Sakamoto M: Effect of toe contact condition during forward stepping on the ground reaction forces during turning movement. J Phys Ther Sci, 2019, 31: 344–348. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Fujimaki T, Wako M, Koyama K, et al. Yamanashi adjunct study of the Japan Environment and Children’s Study Group: Prevalence of floating toe and its relationship with static postural stability in children: the Yamanashi adjunct study of the Japan Environment and Children’s Study (JECS-Y). PLoS One, 2021, 16: e0246010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Wako M, Fujimaki T, Koyama K, et al. : A cross-sectional study on the correlations between floating toe, plantar arch posture, and body composition in 8-year-old children. Foot Ankle Surg, 2022, 28: 1035–1039. [DOI] [PubMed] [Google Scholar]
- 11.Kawamoto T, Nitta H, Murata K, et al. Working Group of the Epidemiological Research for Children’s Environmental Health: Rationale and study design of the Japan environment and children’s study (JECS). BMC Public Health, 2014, 14: 25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lindemann U, Mohr C, Machann J, et al. : Association between thigh muscle volume and leg muscle power in older women. PLoS One, 2016, 11: e0157885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Sheth KA, Iyer CC, Wier CG, et al. : Muscle strength and size are associated with motor unit connectivity in aged mice. Neurobiol Aging, 2018, 67: 128–136. [DOI] [PMC free article] [PubMed] [Google Scholar]