

Abstract
Introduction:
Babies born large-for-gestational age (LGA) have an increased risk of adverse health outcomes, including birth injuries, childhood obesity, and cardiometabolic disorders. However, little work has been done to characterize patterns of fetal growth among LGA births, which may further elucidate high- and low-risk subgroups.
Objectives:
Identify subgroups of LGA births based on trajectories of fetal growth derived from prenatal ultrasound measurements, and explore differences in sociodemographic, pregnancy, and birth outcome characteristics across subgroups.
Study Design:
We identified and described trajectories of fetal growth among LGA births (n = 235) in the LIFECODES Fetal Growth Study. Ultrasound measurements of fetal growth in mid- to late pregnancy were abstracted from health records. We applied group-based multi-trajectory modeling to measurements of head circumference (HC), abdominal circumference (AC), and femur length (FL) z-scores to identify multivariate trajectories of fetal growth. We then summarized sociodemographic variables, pregnancy characteristics, and birth outcomes based on trajectory membership.
Results:
We identified four multivariate trajectories of fetal growth among LGA births: Catch-up Growth (n = 28), Proportional AC:FL Growth (n = 67), Disproportional AC:FL Growth (n = 96), and Consistently Large (n = 44). Fetuses in the “Catch-up Growth” group exhibited small relative size in mid-pregnancy (i.e., below average HC, AC, and FL z-scores) and large relative size in late-pregnancy. Growth among these births was driven by increases in relative AC and HC size. Participants who delivered births assigned to this group were less likely to have normal glucose control (40% vs. 65 – 75%) and more likely to have pre-gestational diabetes (36% vs. 10 – 17%) compared to other LGA subgroups. The babies in this trajectory group were also more likely to have macrosomia (86% vs. 67 – 73%) and to be admitted to the NICU (32% vs. 14 – 21%) compared to other LGA subgroups. On the other hand, babies in the “Consistently Large” group had the largest relative size for all growth parameters throughout gestation and experienced lower risk of adverse birth outcomes than other LGA subgroups.
Conclusions:
We characterized several trajectories of fetal growth among LGA births, which were related to different pregnancy characteristics and distribution of adverse birth outcomes. While the numbers of individuals within some trajectories was small, we identified a subgroup that exhibited a catch-up growth phenotype during gestation, which may be uniquely associated with exposure to pre-gestational diabetes and a higher risk of admission to the NICU. These results highlight that the risk of adverse outcomes may not be evenly distributed across all LGA births.
Keywords: Large-for-gestational age, group-based trajectory models, latent class trajectory analysis, fetal growth trajectories
INTRODUCTION
Abnormal fetal size is linked to adverse health outcomes, such as neurodevelopmental, cardiovascular, and metabolic disorders.1–4 Past work has highlighted the difficulties in identifying babies that are born abnormally small (i.e., growth restricted),5–7 including that reliance on percentile cut-offs, such as small-for-gestational age (SGA; < 10 percentile-for-gestational age), does not reliably distinguish between babies with pathological versus constitutional growth profiles.7–9 The identification of abnormally large babies, or large-for-gestational age (LGA; > 90th percentile weight-for-gestational age), likely suffers from the same shortfalls, but to our knowledge, has received less attention in the peer-reviewed literature.
The incorporation of ultrasound measurements of fetal growth to characterize the overall growth trajectory of a fetus has been suggested as a mechanism to better distinguish pathological deviations in growth from normal variability. Specifically, growth mixture models have been used to characterize fetal growth trajectories, with a particular focus on characterizing small fetuses or isolating subgroups consistent with fetal growth restriction.10–13 To our knowledge, these same methods have not been used to characterize growth trajectories among large babies (e.g., LGA) for whom health risks may also differ depending on the trajectory of prenatal growth. These methods assume that identified growth trajectories represent subgroups of individuals with shared risk factors or etiologies14 and may be more informative in future studies than a single definition of LGA when examining how either exposures or outcomes relate to fetal growth.
In this analysis, we characterized growth trajectories among LGA births using ultrasound measurements of fetal growth collected from mid- to late pregnancy in the LIFECODES Fetal Growth Study. Specifically, we applied group-based multi-trajectory modeling to identify subgroups of individuals with shared profiles of multiple growth indicators, namely, head circumference (HC), abdominal circumference (AC) and femur length (FL) z-scores. We described the distribution of demographic and pregnancy characteristics across trajectory groups and examined how these fetal growth trajectories relate to birth outcomes.
METHODS
Study population
The LIFECODES cohort is an ongoing, prospective pregnancy cohort that began in 2006 at Brigham and Women’s Hospital in Boston, MA.15 The study has few eligibility criteria: participants must be at least 18 years of age, initiate prenatal care prior to 15 weeks gestation, and plan on delivering at Brigham and Women’s Hospital. As a part of the study, participants attend a total of three study visits occurring at approximately 10-, 26-, and 35-weeks gestation. At the first study visit, participants provide written and informed consent. The LIFECODES study was approved by the Institutional Review Board of Brigham and Women’s Hospital and the present analyses were deemed exempt by the National Institute of Environmental Health Sciences.
This analysis utilizes the LIFECODES Fetal Growth Study, which is nested within the LIFECODES cohort and has been described elsewhere.12 Briefly, this case-cohort study included pregnancies in the LIFECODES cohort that resulted in singleton deliveries between 2008 – 2018 and that had birthweight recorded at delivery. Prior to selection, we determined the birthweight z-score using a standard from the underlying Brigham and Women’s Hospital clinic population, which provides a mean and standard deviations of birthweight according to nearest completed weeks gestation.16,17 Using the calculated z-scores, we identified all SGA (i.e., < 10th percentile-for-gestational age), appropriate-for-gestational age (AGA; i.e., 10th – 90th percentile-for-gestational age), and LGA (i.e., > 90th percentile-for-gestational age) births in the underlying LIFECODES cohort. Selection subsequently occurred in two stages. First, a subcohort of 504 participants was randomly selected from within this time frame. Second, enrichment sets of SGA (N = 199) and LGA (N = 198) births were randomly selected from identified cases in LIFECODES. This selection mechanism resulted in 249 SGA, 411 AGA, and 241 LGA births. For the purposes of this analysis, we focus on LGA cases and present AGA controls for initial comparisons only.
Ultrasound measurements of fetal growth
We abstracted standard measurements of fetal growth, namely HC, AC, and FL, from ultrasound records. All measurements collected after 15 weeks gestation were converted to gestational age-specific z-scores using an internal growth standard.16,17 As described above, the internal growth standard used in this study provided mean and standard deviations for each ultrasound measurement according to nearest completed gestational week. For a subset of participants, no HC measure was available (n = 47). Instead, we abstracted biparietal diameter (BPD) and substituted their BPD z-score for the HC z-score. As a summary measure of growth, we also calculated estimated fetal weight (EFW) using Hadlock’s Formula #3 based on HC, AC, and FL. For participants missing HC measurements, EFW was calculated using Hadlock’s Formula #2, which uses BPD as a measure of head size instead of HC.18
Participant characteristics and birth outcomes
At the first study visit, participants completed detailed questionnaires to assess demographics (e.g., self-reported race and ethnicity, educational attainment), behavioral characteristics (e.g., smoking and alcohol consumption), and medical history (e.g., previous pregnancies and pregnancy complications). Clinical measurements (e.g., weight and blood pressure) were collected during all study visits. Medical diagnoses occurring during pregnancy were validated by two Maternal-Fetal Medicine specialists. We examined glucose homeostasis on a spectrum with a categorical variable derived from information on glucose test results and information related to gestational, Type-1 or Type-2 diabetes mellitus in the medical record. The categories were as follows: (1) normal glucose metabolism, including participants without gestational or pre-gestational diabetes and normal results (<140 mg/dL) on the standard 1-hour glucose loading test (GLT); (2) mild carbohydrate intolerance, including participants who met or exceeded 140 mg/dL glucose on the GLT, but who did not meet criteria for gestational diabetes on a subsequent 3-hour oral glucose tolerance test and/or did not receive a diagnosis of gestational diabetes in the medical record; (3) gestational diabetes diagnosis in the medical record; and (4) pre-gestational diabetes in the medical record.
Birth outcomes were abstracted from medical records after delivery. The outcomes considered in this analysis included: birthweight z-scores calculated from an internal growth standard16, birthweight, birthweight-length ratio,19 gestational age at delivery, delivery via C-section (including scheduled vs. unscheduled), admission to the neonatal intensive care unit (NICU), and length of NICU stay.
Statistical analysis
We summarized demographics, pregnancy characteristics, and birth outcomes of parent-child pairs with either an LGA or AGA birth by calculating the median (interquartile range [IQR]) or n (%). Demographics, pregnancy characteristics, and birth outcomes observed among parent-child pairs selected into the LIFECODES Fetal Growth Study were also compared to those in the underlying LIFECODES cohort from which they were sampled. We displayed the distributions of ultrasound measurements of fetal growth using scatter plots.
We identified the number and shape of growth trajectories among LGA births using group-based multi-trajectory modeling, as described in Appendix A. Briefly, we optimized the number of multivariate trajectories of HC, AC, and FL z-scores using criteria described by Nagen and colleagues.20 After optimizing the number of trajectories, individual participants were assigned to the trajectory group that corresponded to their highest posterior inclusion probability. We visualized growth trajectories by displaying the predicted mean z-scores (95% CI) for each parameter within each of the identified groups and provided descriptive names to each trajectory group based on visual inspection of these trajectories rather than the calculation or examination of any additional characteristics.
We summarized the median (IQR) and n (%) of demographics, pregnancy characteristics, and birth outcomes among multivariate trajectory groups. In addition, we examined how the identified trajectory groupings compared to another method of identifying pathologically large fetuses, namely macrosomia (defined as birthweight > 4000 g24).
One limitation of latent class trajectory modeling is that the assignment of group membership contains uncertainty. While individuals were assigned to the group corresponding to their highest posterior inclusion probability, there is some probability of belonging to any of the groups identified. Not accounting for this uncertainty may result in misclassification of the group assignments. To address this, we replicated our descriptive statistics using a case-weight approach, where all results were produced using the posterior inclusion probabilities of group membership as inverse probability weights, rather than assigning fixed trajectory group membership.25
Several previous analyses applying trajectory modeling to longitudinal measurements of fetal growth have analyzed EFW as a summary measure of growth.10–12 In order to compare our results to this literature, we applied univariate group-based trajectory modeling14 to identify the shape and number of EFW trajectories, and we present these results supplementally. The shape and number of univariate growth trajectories was optimized using the criteria defined above.21–23 Demographics, pregnancy characteristics, and birth outcomes were summarized across univariate groups as described previously. In addition, we compared the group assignments for participants between the multivariate and univariate trajectory modeling approaches.
We present this analysis as descriptive in nature and have not included p-values or statistical testing in presentation of our results. Instead, in accordance with recommendations from the American Statistical Association26 and the guidelines for Strengthening Reporting of Observational Studies in Epidemiology (STROBE)27, we focus primarily on the direction and magnitude of differences observed between groups under investigation in this work.
RESULTS
Study characteristics
This study comprises 241 parent-child pairs with an LGA birth and 411 with an AGA birth (Table 1). Compared to those with an AGA birth, participants who gave birth to an LGA baby were more likely to have a bachelor’s degree or higher education level, to self-identify as non-Hispanic white, have a higher pre-pregnancy BMI, have pre-gestational diabetes, and to give birth to a baby identified as male at birth. They were also less likely to report consuming alcohol or smoking during pregnancy compared to those with an AGA birth. There were similar rates of preeclampsia and gestational diabetes in these two groups. With respect to birth outcomes, LGA babies had similar gestational ages at delivery but were more likely to be delivered via C-section and to be admitted to the NICU at delivery compared to AGA babies. In addition, characteristics observed within our sample of AGA and LGA births were consistent with those observed among all AGA and LGA births in the underlying LIFECODES cohort (Supplemental Tables 1 and 2).
Table 1.
Demographics, pregnancy characteristics, and birth outcomes among parent-child pairs with an LGA or AGA birth in the LIFECODES Fetal Growth Study
| Median (25th, 75th percentile) or n (%) | ||
|---|---|---|
| AGA births (N = 411) | LGA births (N = 241) | |
| Age, years | 32.4 (28.8, 36.2) | 33.7 (29.6, 37.3) |
| Education | ||
| High school or less | 49 (12) | 30 (13) |
| Some college or associate degree | 89 (22) | 36 (15) |
| Bachelor’s degree or greater | 268 (66) | 171 (72) |
| Race and ethnicity | ||
| Non-Hispanic white | 243 (59) | 161 (67) |
| Non-Hispanic Black | 55 (13) | 29 (12) |
| Hispanic | 63 (15) | 38 (16) |
| Other | 50 (12) | 13 (5) |
| Health insurance | ||
| Private | 298 (74) | 177 (74) |
| Public | 107 (26) | 62 (26) |
| Pre-pregnancy BMI, kg/m2 | 24.8 (21.5, 29.28) | 27.0 (23.4, 32.5) |
| Height, inches | 64 (63, 66) | 65 (63, 67) |
| Alcohol consumption in pregnancy | ||
| No | 377 (93) | 234 (98) |
| Yes | 29 (7) | 6 (3) |
| Smoking in pregnancy | ||
| No | 379 (92) | 236 (98) |
| Yes | 32 (8) | 5 (2) |
| Primiparous | ||
| No | 254 (62) | 171 (71) |
| Yes | 157 (38) | 70 (29) |
| ART | ||
| No | 364 (89) | 208 (86) |
| Yes | 47 (11) | 33 (14) |
| Preeclampsia | ||
| No | 397 (97) | 228 (95) |
| Yes | 14 (3) | 13 (5) |
| Glucose control | ||
| Normal glucose metabolism | 323 (83) | 141 (64) |
| Mild carbohydrate intolerance | 28 (7) | 24 (11) |
| Gestational diabetes | 28 (7) | 18 (8) |
| Pre-gestational diabetes | 11 (3) | 36 (16) |
| Type of pre-gestational diabetes | ||
| Type 1 | 4 (36) | 23 (64) |
| Type 2 | 7 (64) | 13 (36) |
| Infant sex | ||
| Female | 199 (48) | 82 (34) |
| Male | 212 (52) | 159 (66) |
| Gestational age at delivery, weeks | 39.0 (37.9, 39.7) | 38.9 (38.0, 39.6) |
| Birthweight z-score | −0.15 (−0.64, 0.33) | 1.73 (1.49, 2.04) |
| Birthweight, kg | 3245 (2965, 3532) | 4140 (3941, 4300) |
| Birthweight - length ratio, gm/cm | 66.4 (62.0, 70.0) | 79.4 (76.3, 82.7) |
| Delivery via C-section | ||
| No | 249 (61) | 107 (45) |
| Yes | 158 (39) | 133 (55) |
| Delivery via unscheduled C-section | 92 (59) | 78 (61) |
| No | ||
| Yes | 65 (41) | 50 (39) |
| NICU Admission | ||
| No | 363 (89) | 189 (80) |
| Yes | 45 (11) | 47 (20) |
| Length of NICU Stay, days | 5 (3, 17) | 5 (3, 13) |
Abbreviations: AGA = appropriate-for-gestational age, ART = assisted reproductive technologies, BMI = body mass index, LGA = large-for-gestational age, NICU = neonatal intensive care unit
Notes: n = 9 missing education, n = 8 missing health insurance, n = 9 missing pre-pregnancy BMI, n = 6 missing alcohol consumption, n = 43 missing measures of glucose control, n = 36 missing birthweight-length ratio, n = 5 missing delivery via C-section, n = 6 missing unscheduled C-section; n = 8 missing NICU admission. Other race and ethnicity includes Asian (n = 31), More than one race (n = 20) and Other (n = 12). Public insurance category includes those using Medicaid/Mass Health/SSI (n = 162), Self pay (n = 12) and no health insurance (n = 1). Type of pre-gestational diabetes only displayed for individuals diagnosed with pre-gestational diabetes (n = 47). Unscheduled C-section only displayed among individuals with a C-section delivery (n = 291). Length of NICU stay only calculated among individuals with a known NICU admission (n = 92).
Fetal growth characteristics
Distributions of ultrasound measurements of fetal growth are shown in Figure 1. In general, babies that were identified as LGA at birth had fetal growth measurements that were larger than those reported for AGA babies. Nevertheless, there was still overlap between measurements in the two groups, especially for FL and HC. There was an average of 4.3 and 4.1 ultrasounds per parent-child pair with an LGA and AGA birth, respectively. A total of 235 parent-child pairs with an LGA birth had at least one HC, AC, and FL z-score and were used in subsequent trajectory modeling.
Figure 1.
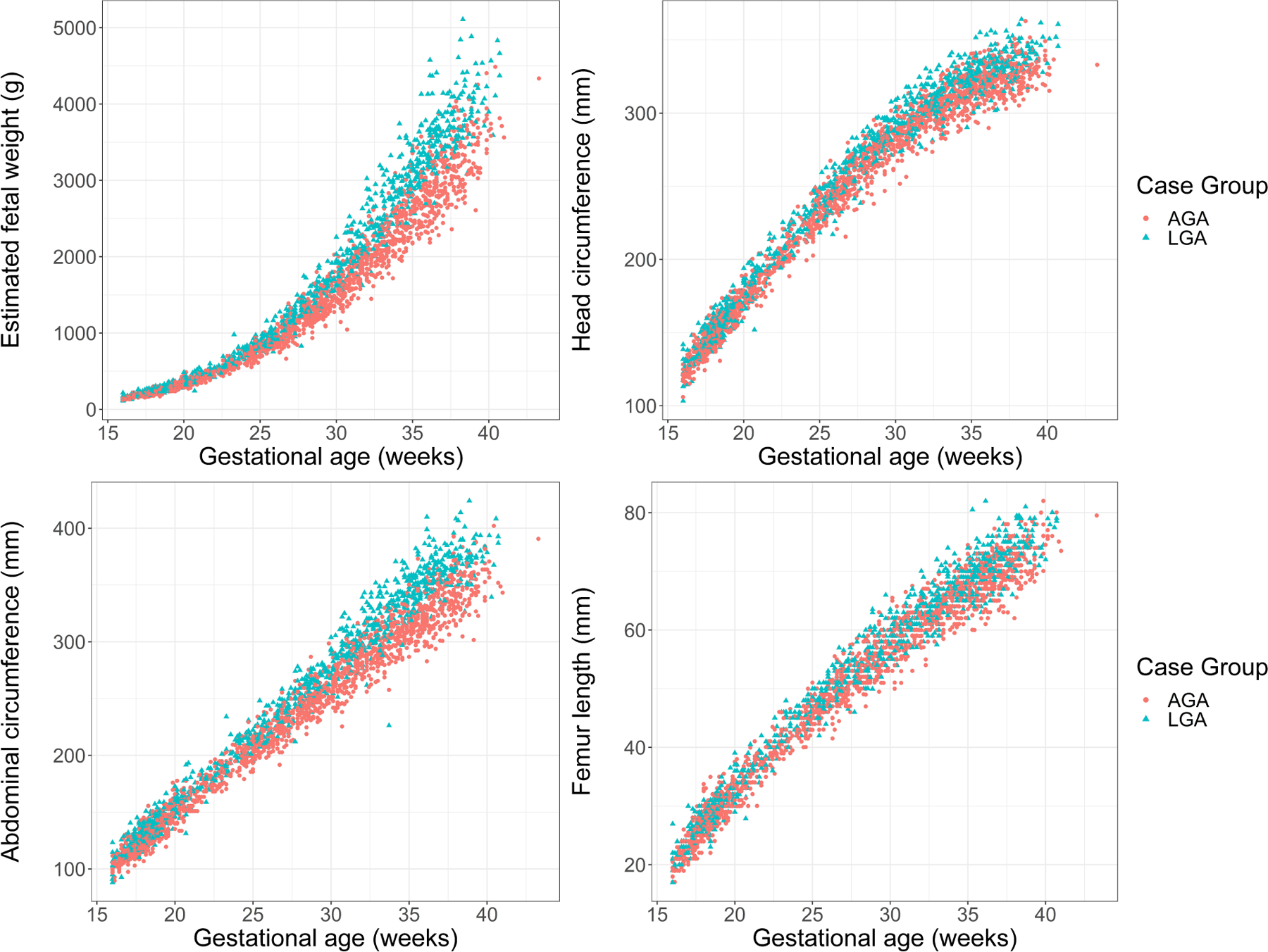
Distribution of ultrasound measures of fetal growth by case status in the LIFECODES Fetal Growth Study. Measures of fetal growth abstracted from ultrasounds (i.e., estimated fetal weight, head circumference, abdominal circumference, and femur length) are shown according to case status. AGA = appropriate-for-gestational age, SGA = small-for-gestational age.
Growth trajectories among LGA births
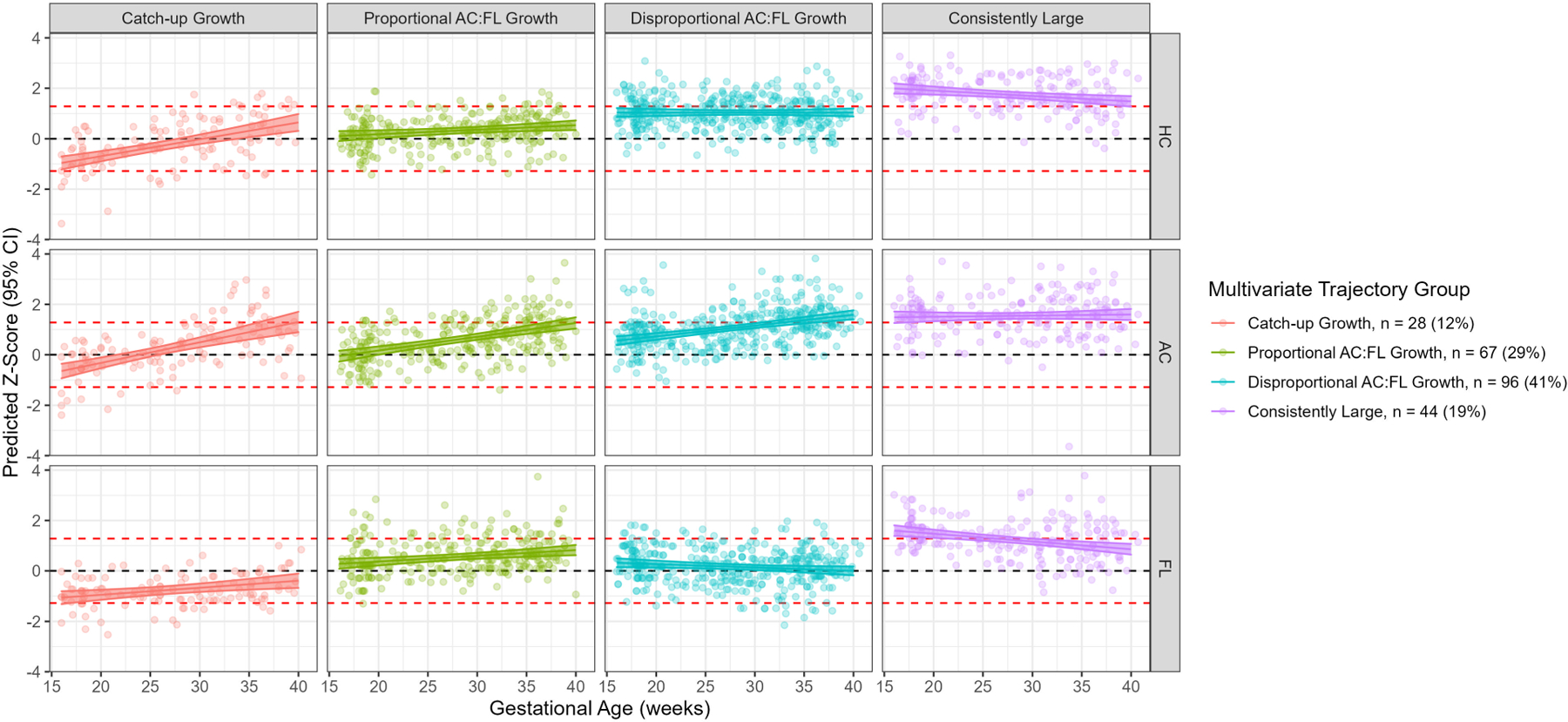
Using a multivariate trajectory modeling approach, a 4-group solution was deemed optimal to describe trajectories of fetal growth (Figure 2; Table 2; Supplemental Table 3). The “Catch-up Growth” group (n = 28 [12%]) had the smallest relative size in mid-pregnancy with growth driven primarily by increases in relative HC and AC into late pregnancy. There were two groups, termed “Proportional AC:FL Growth” (n = 67 [29%]) and “Disproportional AC:FL Growth” (n = 96 [41%]), where fetuses were average in size in mid-pregnancy but large in late pregnancy. These groups also had increasing relative AC across gestation, though they differed with respect to the other growth parameters, particularly FL. Relative FL in the “Proportional AC:FL” group increased steadily across pregnancy, as with AC, but FL in the “Disproportional AC:FL” group remained average across gestation. Last, we identified a “Consistently Large” group (n = 44 [19%]) with the largest z-scores for all growth measurements throughout gestation.
Figure 2.
Predicted mean HC, AC, and FL z-scores (95% CI) of multivariate trajectory groups identified among babies born LGA in the LIFECODES fetal growth case-cohort. Red dashed lines indicate lines representing LGA (z-score = 1.28) and SGA (z-score = −1.28) cut points. Black dashed line indicates average growth (z-score = 0).
Table 2.
Descriptions of fetal growth phenotypes identified by univariate and multivariate latent class trajectory models in the LIFECODES Fetal Growth Study.
|
Univariate trajectory groups
| ||
|---|---|---|
| Group | Name | Description |
| 1 | Catch-up Growth | Smallest relative size in mid-pregnancy. Steep growth rate for all HC and AC, through late pregnancy. |
| 2 | Proportional AC:FL Growth | Average relative size in mid-pregnancy. Increasing growth rate for all growth parameters, especially AC, through late pregnancy. |
| 3 | Disproportional AC:FL Growth | Average relative size in mid-pregnancy. Increasing growth rate for AC through late pregnancy, stable or slowing growth rate for HC and FL. |
| 4 | Consistently Large | Largest relative size on all parameters in mid-pregnancy. Growth rate slows for HC and FL through late pregnancy. |
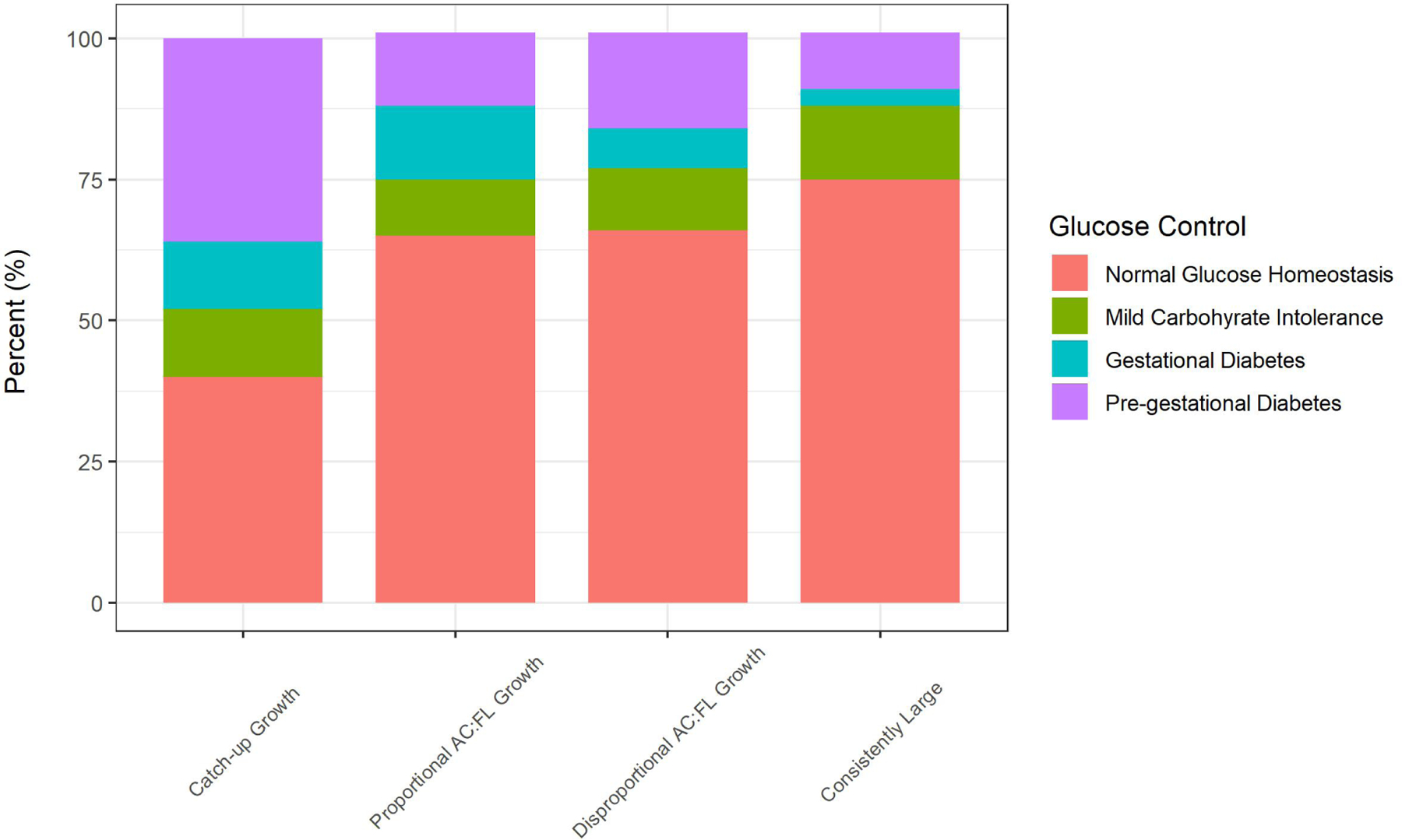
We observed that participants assigned to the “Catch-up Growth” group were least likely to have normal glucose metabolism and most likely to have pre-gestational diabetes compared to other LGA groups (Table 3; Figure 3). The “Disproportional AC:FL Growth” group was characterized by older participants, the highest proportion of participants with a bachelor’s degree or greater, and were more likely to self-identifiy as non-Hispanic white, have private health insurance, and to have used assisted reproductive technologies to conceive relative to the other LGA groups. The “Proportional AC:FL Growth” group had higher pre-pregnancy BMI relative to participants in the other LGA groupings. The “Consistently Large” group were most likely to have normal glucose metabolism relative to the other LGA groups.
Table 3.
Demographics, pregnancy characteristics, and birth outcomes for multivariate fetal growth trajectory groups among parent-child pairs with an LGA birth in the LIFECODES Fetal Growth Study
| Median (25th, 75th percentile) or n (%) |
|||||
|---|---|---|---|---|---|
| Catch-up Growth (N = 28) |
Proportional AC:FL Growth (N = 67) | Disproportional AC:FL Growth (N = 96) | Consistently Large (N = 44) | ||
| Age, years | 32.4 (27.3, 37.3) | 31.8 (27.6, 37.0) | 34.6 (30.4, 37.6) | 33.6 (31.6, 37.3) | |
| Education | |||||
| High school or less | 5 (18) | 12 (18) | 9 (10) | 4 (9) | |
| Some college or associate degree | 7 (25) | 14 (21) | 8 (9) | 7 (16) | |
| Bachelor’s degree or greater | 16 (57) | 40 (61) | 77 (82) | 32 (74) | |
| Race and ethnicity | |||||
| Non-Hispanic white | 15 (54) | 36 (54) | 77 (80) | 28 (64) | |
| Non-Hispanic Black | 5 (18) | 14 (21) | 2 (2) | 8 (18) | |
| Hispanic | 5 (18) | 14 (21) | 14 (15) | 5 (11) | |
| Other | 3 (11) | 3 (4) | 3 (3) | 3 (7) | |
| Health insurance | |||||
| Private | 20 (71) | 42 (63) | 79 (82) | 30 (71) | |
| Public | 8 (29) | 25 (37) | 17 (18) | 12 (29) | |
| Pre-pregnancy BMI, kg/m2 | 27.1 (22. 7, 31.9) | 29.4 (25.1, 35.4) | 25.8 (22.6, 31.2) | 27.4 (22.7, 31.5) | |
| Height, inches | 66 (63, 67) | 65 (63, 68) | 65 (63, 67) | 66 (65, 68) | |
| Alcohol consumption in pregnancy | |||||
| No | 28 (100) | 66 (99) | 91 (95) | 43 (100) | |
| Yes | 0 (0) | 1 (1) | 5 (5) | 0 (0) | |
| Smoking in pregnancy | |||||
| No | 28 (100) | 66 (99) | 94 (98) | 42 (95) | |
| Yes | 0 (0) | 1 (1) | 2 (2) | 2 (5) | |
| Primiparous | |||||
| No | 21 (75) | 50 (75) | 63 (66) | 33 (75) | |
| Yes | 7 (25) | 17 (25) | 33 (34) | 11 (25) | |
| ART | |||||
| No | 25 (89) | 61 (91) | 77 (80) | 40 (91) | |
| Yes | 3 (11) | 6 (9) | 19 (20) | 4 (9) | |
| Preeclampsia | |||||
| No | 25 (89) | 64 (96) | 91 (95) | 42 (95) | |
| Yes | 3 (11) | 3 (4) | 5 (5) | 2 (5) | |
| Glucose control | |||||
| Normal glucose metabolism | 10 (40) | 41 (65) | 59 (66) | 30 (75) | |
| Mild carbohydrate intolerance | 3 (12) | 6 (10) | 10 (11) | 5 (13) | |
| Gestational diabetes | 3 (12) | 8 (13) | 6 (7) | 1 (3) | |
| Pre-gestational diabetes | 9 (36) | 8 (13) | 15 (17) | 4 (10) | |
| Type of pre-gestational diabetes | |||||
| Type 1 | 7 (78) | 4 (50) | 9 (60) | 3 (75) | |
| Type 2 | 2 (22) | 4 (50) | 6 (40) | 1 (25) | |
| Infant sex | |||||
| Female | 10 (36) | 30 (45) | 29 (30) | 12 (27) | |
| Male | 18 (64) | 37 (55) | 67 (70) | 32 (73) | |
| Gestational age at delivery, weeks | 39.4 (37.9, 40.4) | 39.0 (38.4, 39.7) | 38.8 (37.9, 39.5) | 38.9 (38.3, 39.6) | |
| Birthweight z-score | 1.72 (1.42, 2.03) | 1.64 (1.47, 1.94) | 1.77 (1.52, 2.09) | 1.73 (1.52, 2.29) | |
| Birthweight, kg | 4188 (4052, 4312) | 4105 (3995, 4250) | 4173 (3905, 4313) | 4139 (3945, 4407) | |
| Birthweight - length ratio, gm/cm | 80.8 (78.8, 83.9) | 78.6 (77.0, 81.6) | 79.4 (75.6, 82.1) | 79.0 (75.8, 82.9) | |
| Delivery via C-section | |||||
| No | 14 (50) | 32 (48) | 34 (36) | 23 (52) | |
| Yes | 14 (50) | 35 (52) | 61 (64) | 21 (48) | |
| Delivery via unscheduled C-section | |||||
| No | 8 (57) | 22 (67) | 35 (59) | 11 (55) | |
| Yes | 6 (43) | 11 (33) | 24 (41) | 9 (45) | |
| NICU Admission | |||||
| No | 19 (68) | 55 (83) | 74 (79) | 36 (86) | |
| Yes | 9 (32) | 11 (17) | 20 (21) | 6 (14) | |
Abbreviations: AGA = appropriate-for-gestational age, ART = assisted reproductive technologies, BMI = body mass index, LGA = large-for-gestational age, NICU = neonatal intensive care unit
Note: n = 4 missing education, n = 2 missing health insurance, n = 2 missing pre-pregnancy BMI, n = 1 missing alcohol consumption during pregnancy, n = 14 missing measures of glucose control, n = 8 missing birthweight-length ratio, n = 1 missing delivery via C-section, n = 5 missing delivery via unscheduled C-section, n = 5 missing NICU admission. Other race and ethnicity includes Asian (n = 5), More than one race (n = 5) and Other (n = 2). Public insurance category includes those using Medicaid/Mass Health/SSI (n = 61) and Self pay (n = 1). Type of pregestational diabetes only displayed for individuals diagnosed with pregestational diabetes (n = 36). Unscheduled C-section only displayed among individuals with a C-section delivery (n = 131). Length of NICU stay only calculated among individuals with a known NICU admission (n = 46).
Figure 3.
Categories of glucose control for multivariate fetal growth trajectory groups among parent-child pairs with an LGA birth in the LIFECODES Fetal Growth Study. Data underlying this figure can be found in Table 3.
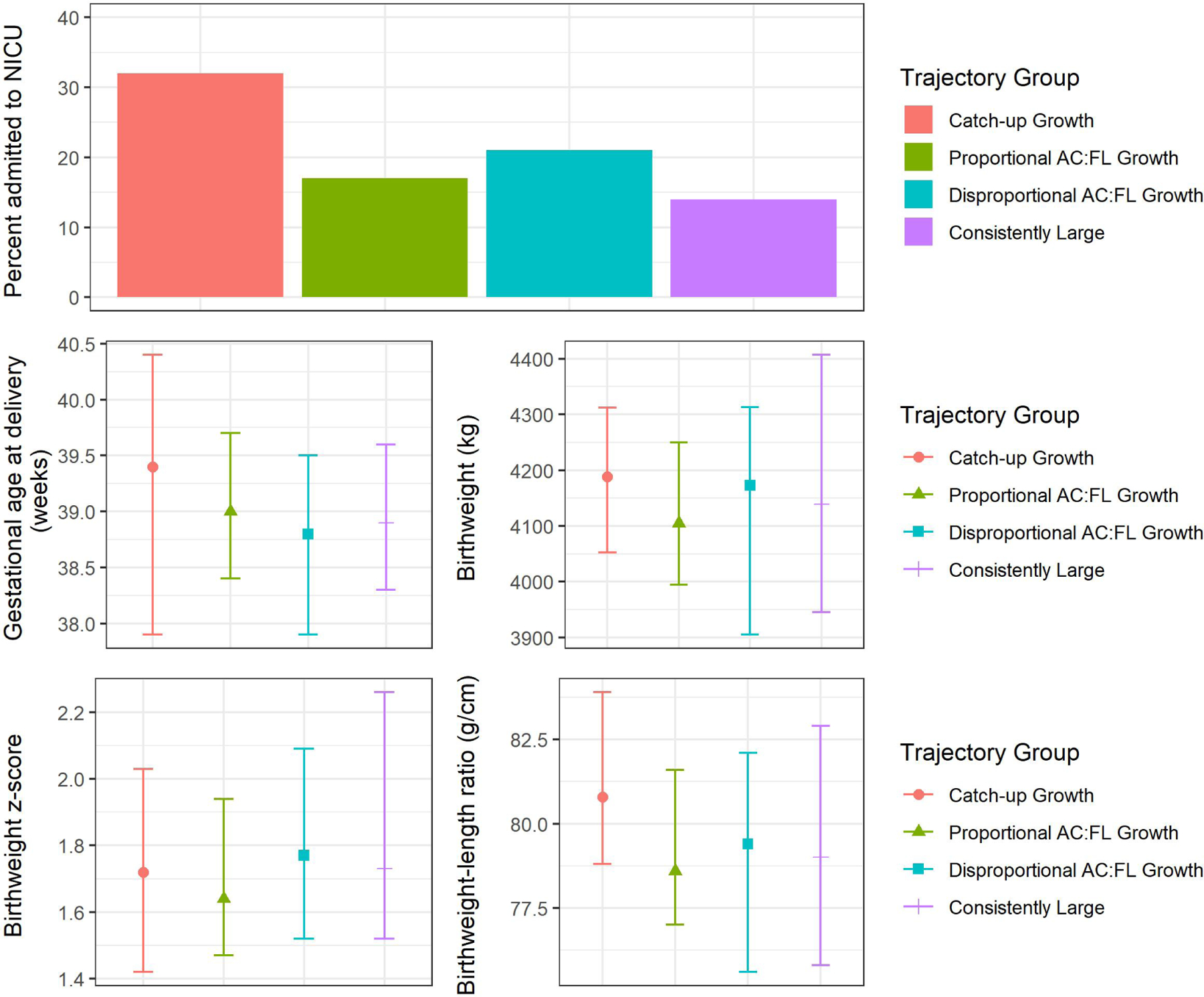
With respect to birth outcomes, the “Catch-up Growth” group had the highest proportion of babies admitted to the NICU relative to other LGA groups (Figure 4; Table 3). However, the distributions of other birth outcome measurements overlapped substantially with those observed among the other groups. Conclusions were consistent using a case-weight approach rather than assigning fixed trajectory group membership (Supplemental Table 4).
Figure 4.
Proportion or median (IQR) of select birth outcomes in univariate trajectory groups among LGA births in the LIFECODES Fetal Growth Study. NICU = neonatal intensive care unit. Data underlying this figure can be found in Table 3.
Some differences in the distribution of macrosomia diagnoses by multivariate trajectory group membership were observed (Supplemental Table 5). Notably, the “Catch-up Growth” group had the highest proportion of infants with macrosomia (86%) compared to the other LGA groups (67–73%).
In sensitivity analyses, we identified three univariate EFW trajectory groups among babies born LGA (Supplemental Figure 1). There were some similarities between the univariate and multivariate trajectories. For example, we identified a group of “Consistently Large” babies, with the largest EFW z-scores throughout gestation, and a “Catch-up Growth” group where EFW was relatively small (i.e., below the 10th percentile) in mid-pregnancy and large during late pregnancy. There were also similarities with respect to trends in sociodemographic variables and birth outcomes observed in the identified trajectory groups (Supplemental Table 6). For example, participants in the “Catch-up Growth” group had the highest proportion of NICU admissions relative to other trajectory groups. There was concordance between parent-child pairs assigned to the “Consistently Large” group in both the univariate and multivariate approach (Supplemental Table 7). Similarly, the univariate “Catch-up Growth” group was inclusive of nearly all individuals in the multivariate “Catch-up Growth” group.
COMMENT
Principal findings
In this study, we identified and described phenotypes of fetal growth among LGA births in the LIFECODES Fetal Growth Study. Using repeated ultrasound measurements collected from mid- to late pregnancy, we identified four multivariate trajectories based on shared profiles of HC, AC, and FL z-scores. These trajectory groups differed in their associations with birth outcomes, including NICU admission. Specifically, fetuses exhibiting the largest relative increase in AC and HC across pregnancy, which we defined as a prenatal “Catch-up Growth” group, had the highest proportion of births admitted to the NICU.
Results in the context of what is known
To our knowledge, no other studies have characterized growth phenotypes among LGA births using repeated ultrasound measurements of growth across gestation. However, we have previously conducted similar analyses among SGA infants. In these studies, we reported 3 univariate trajectories based on EFW and 4 multivariate growth trajectories based on measurements of HC, AC, and FL z-scores.10,12 In this context, we observed that babies with the smallest size across gestation had higher risk of adverse birth or childhood neurodevelopmental outcomes relative to those with transient growth profiles. This is contrary to our current findings among LGA births, where we have found that fetuses with transient growth (e.g., “Catch-up Growth”) had the highest proportion of infants admitted to the NICU compared to other groups. Specifically, the “Catch-up Growth” trajectory group was characterized by smaller relative size during mid-pregnancy and large increases in relative HC and AC. A key characteristic of the “Catch-up Growth” group was that it contained the highest proportion of individuals with pre-gestational diabetes (primarily Type 1 diabetes) and the lowest proportion of individuals with normal glucose control. Previous studies examining growth profiles among pregnant persons with diabetes that have described fetal growth trajectories featuring both mid-pregnancy growth delays and rapid increases in AC from mid- to late-pregnancy.28–32 Others have hypothesized that mid-pregnancy growth delay among pregnant persons with diabetes could be due to the influence of poor glycemic control on placentation in early pregnancy.33 On the other hand, increased growth rate in late pregnancy may be due to fetal hyperinsulinemia triggered by maternal hyperglycemia, which may result in greater adipose development.33,34 Together, these findings suggest that this growth phenotype could be a characteristic of prenatal exposure to diabetes.
Clinical implications
Latent class methods have shown promise in their ability to identify hidden subgroups of diseased individuals with shared clinical profiles or etiologies, including in the analysis of fetal growth.8,35 While these methods have been primarily applied to growth at the small end of the birthweight spectrum, we have demonstrated that it may also distinguish between clinically meaningful subgroups of LGA babies. Further research is warranted to continue interrogation of fetal growth trajectories among LGA babies.
Research implications
Latent class trajectory modeling is used to derive relatively homogenous subgroups of individuals hypothesized to share etiology or mechanisms of disordered growth.14 From this perspective, these subgroups may be more meaningful in the context of future epidemiologic studies seeking to examine how risk factors or outcomes relate to fetal growth. Thus, this characterization of LGA phenotypes may contribute to further understanding the determinants and consequences of abnormally large babies.
Strengths and limitations
This analysis was not without limitations. First, this study population was recruited from a high-risk tertiary care facility. While the number of ultrasounds collected on these participants was relatively large, their measurements may not reflect “normal” growth among LGA births within the general population, representing possible selection bias. Thus, the shape and distribution of growth phenotypes may not generalize to other populations. However, the enrichment for high-risk pregnancies may improve our ability to characterize pathological growth phenotypes, such as those characterized by individuals with diabetes. Second, although we standardized our growth measures for gestational age using an internal standard, it only provided information to characterize growth according to the nearest completed week and did not consider individual gestational days.16,17 This may result in some misclassification, particularly for measures occurring at either the beginning or the end of a gestational week. Third, we limited our analysis to participants with LGA births. One consequence of this approach is that we were not able to capture fetuses that may still have exceeded their true growth potential, but who were not classified as LGA at the time of delivery. Yet, we expect that a large proportion of babies experiencing pathological overgrowth would be captured among LGA births. Fourth, we had a limited number of birth and childhood follow-up outcomes that could be included in this analysis. Last, while this study population had a large number of LGA births, we observed small sizes within subgroups. Thus, further research is needed to replicate our findings with larger sample sizes.
Nevertheless, this study had several strengths. To our knowledge, this is the first analysis to characterize phenotypes of fetal growth among LGA births using longitudinal ultrasound measurements. Given the large number of ultrasounds in this population (on average > 4 per participant), we were able to identify multiple trajectory groupings in our approach. In addition, we were able to apply group-based multi-trajectory modeling to examine profiles of growth according to HC, AC, and FL measurements. Relying solely on EFW as a summary measure of growth has been shown to have several issues36–38 and we expect the ability to consider fetal body composition to provide a more comprehensive analysis of growth.
Conclusions
We identified phenotypes of fetal growth among LGA births in the LIFECODES Fetal Growth Study, which differed in their profiles of demographics, pregnancy characteristics, and adverse health outcomes. Specifically, we observed that a small subgroup of babies following a prenatal “Catch-up Growth” phenotype during gestation were characterized by potentially higher risk of adverse birth outcomes, namely NICU admission, than other babies born LGA. These findings suggest that considering the overall trajectory of fetal growth may provide important information about health risks compared to relying on birthweight alone. Given the exploratory nature of this study, further work is needed to replicate these findings.
Supplementary Material
AJOG AT A GLANCE:
Why was this study conducted?
This exploratory study sought to characterize fetal growth profiles of babies born large-for-gestational age using latent class multi-trajectory modeling applied to ultrasound measurements of fetal growth from mid- to late pregnancy
What are the key findings?
We observed that the subgroup of fetuses with small relative size in mid-pregnancy and rapid growth into late pregnancy had the highest risk of admission to the neonatal intensive care unit at the time of delivery relative to other subgroups of large-for-gestational age births. In addition, this subgroup was characterized by the greatest exposure to pre-gestational diabetes relative to others.
What does this add to what is known?
To our knowledge, this is the first study to characterize multivariate fetal growth trajectories among large-for-gestational age births using latent class trajectory modeling approaches.
CONDENSATION:
This study identifies subgroups of fetal growth using biometry measurements abstracted from repeated ultrasounds taken from mid- to late pregnancy among large-for-gestational age births.
ACKNOWLEDGEMENTS
The authors would like to acknowledge the LIFECODES study participants and the many BWH faculty involved in collecting and validating medical record information for making this work possible.
FUNDING:
This research was funded by the Intramural Research Program of the National Institute of Environmental Health Sciences, National Institutes of Health (ZIA E103321). The funder had no role in the conduct of this research or preparation of this article.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
CONFLICTS OF INTEREST:
The authors report no conflict of interest.
REFERENCES
- 1.Mullis PE, Tonella P. Regulation of fetal growth: consequences and impact of being born small. Best Pract Res Clin Endocrinol Metab 2008;22(1):173–190. [DOI] [PubMed] [Google Scholar]
- 2.van Wassenaer A Neurodevelopmental consequences of being born SGA. Pediatr Endocrinol Rev 2005;2(3):372–377. [PubMed] [Google Scholar]
- 3.Zhang Y, Li H, Liu SJ, et al. The associations of high birth weight with blood pressure and hypertension in later life: a systematic review and meta-analysis. Hypertens Res 2013;36(8):725–735. [DOI] [PubMed] [Google Scholar]
- 4.Derraik JGB, Maessen SE, Gibbins JD, Cutfield WS, Lundgren M, Ahlsson F. Large-for-gestational-age phenotypes and obesity risk in adulthood: a study of 195,936 women. Scientific Reports 2020;10(1):2157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wilcox AJ. On the importance—and the unimportance— of birthweight. International Journal of Epidemiology 2001;30(6):1233–1241. [DOI] [PubMed] [Google Scholar]
- 6.Hutcheon JA, Platt RW. The missing data problem in birth weight percentiles and thresholds for “small-for-gestational-age”. Am J Epidemiol 2008;167(7):786–792. [DOI] [PubMed] [Google Scholar]
- 7.Ananth CV, Vintzileos AM. Distinguishing pathological from constitutional small for gestational age births in population-based studies. Early Hum Dev 2009;85(10):653–658. [DOI] [PubMed] [Google Scholar]
- 8.Hutcheon JA, Riddell CA, Himes KP. A New Approach for Classifying Fetal Growth Restriction. Epidemiology 2021;32(6):860–867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wilcox AJ, Cortese M, McConnaughey DR, Moster D, Basso O. The limits of small-for-gestational-age as a high-risk category. European Journal of Epidemiology 2021;36(10):985–991. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ferguson KK, Sammallahti S, Rosen E, et al. Fetal Growth Trajectories Among Small for Gestational Age Babies and Child Neurodevelopment. Epidemiology 2021;32(5):664–671. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Barker ED, McAuliffe FM, Alderdice F, et al. The Role of Growth Trajectories in Classifying Fetal Growth Restriction. Obstetrics & Gynecology 2013;122(2 PART 1):248–254. [DOI] [PubMed] [Google Scholar]
- 12.Bommarito PA, Cantonwine DE, Stevens DR, et al. An application of group-based trajectory modeling to define fetal growth phenotypes among small-for-gestational age births in the LIFECODES Fetal Growth Study. Am J Obstet Gynecol 2022. [DOI] [PMC free article] [PubMed]
- 13.Slaughter JC, Herring AH, Thorp JM. A Bayesian latent variable mixture model for longitudinal fetal growth. Biometrics 2009;65(4):1233–1242. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Nagin D Group-based modeling of development Harvard University Press; 2009. [Google Scholar]
- 15.McElrath TF, Lim K-H, Pare E, et al. Longitudinal evaluation of predictive value for preeclampsia of circulating angiogenic factors through pregnancy. American journal of obstetrics and gynecology 2012;207(5):407. e401–407. e407. [DOI] [PubMed] [Google Scholar]
- 16.Cantonwine DE, Ferguson KK, Mukherjee B, et al. Utilizing Longitudinal Measures of Fetal Growth to Create a Standard Method to Assess the Impacts of Maternal Disease and Environmental Exposure. PLOS ONE 2016;11(1):e0146532. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Cantonwine DE, Ferguson KK, Mukherjee B, et al. Utilizing Longitudinal Measures of Fetal Growth to Create a Standard Method to Assess the Impacts of Maternal Disease and Environmental Exposure. Supporting Information. Means and standard deviations (SD) or ultrasound parameters outside the clinically proscribed window of gestation.. PLOS ONE 2016;11:e0146532. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hadlock FP, Harrist RB, Sharman RS, Deter RL, Park SK. Estimation of fetal weight with the use of head, body, and femur measurements—A prospective study. American Journal of Obstetrics and Gynecology 1985;151(3):333–337. [DOI] [PubMed] [Google Scholar]
- 19.Villar J, Puglia FA, Fenton TR, et al. Body composition at birth and its relationship with neonatal anthropometric ratios: the newborn body composition study of the INTERGROWTH-21(st) project. Pediatr Res 2017;82(2):305–316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Nagin DS, Jones BL, Passos VL, Tremblay RE. Group-based multi-trajectory modeling. Stat Methods Med Res 2018;27(7):2015–2023. [DOI] [PubMed] [Google Scholar]
- 21.Andruff H, Carraro N, Thompson A, Gaudreau P, Louvet B. Latent class growth modelling: a tutorial. Tutorials in Quantitative Methods for Psychology 2009;5(1):11–24. [Google Scholar]
- 22.Jones BL, Nagin DS, Roeder K. A SAS procedure based on mixture models for estimating developmental trajectories. Sociological methods & research 2001;29(3):374–393. [Google Scholar]
- 23.Klijn SL, Weijenberg MP, Lemmens P, van den Brandt PA, Lima Passos V. Introducing the fit-criteria assessment plot - A visualisation tool to assist class enumeration in group-based trajectory modelling. Stat Methods Med Res 2017;26(5):2424–2436. [DOI] [PubMed] [Google Scholar]
- 24.Macrosomia: ACOG Practice Bulletin, Number 216. Obstetrics & Gynecology 2020;135(1). [DOI] [PubMed] [Google Scholar]
- 25.Kamata A, Kara Y, Patarapichayatham C, Lan P. Evaluation of Analysis Approaches for Latent Class Analysis with Auxiliary Linear Growth Model. Frontiers in Psychology 2018;9(130). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Wasserstein RL, Lazar NA. The ASA Statement on p-Values: Context, Process, and Purpose. The American Statistician 2016;70(2):129–133. [Google Scholar]
- 27.Vandenbroucke JP, von Elm E, Altman DG, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and Elaboration. Annals of Internal Medicine 2007;147(8):W-163–W-194. [DOI] [PubMed] [Google Scholar]
- 28.Mulder EJ, Koopman CM, Vermunt JK, de Valk HW, Visser GH. Fetal growth trajectories in Type-1 diabetic pregnancy. Ultrasound Obstet Gynecol 2010;36(6):735–742. [DOI] [PubMed] [Google Scholar]
- 29.Hammoud NM, Visser GH, Peters SA, Graatsma EM, Pistorius L, de Valk HW. Fetal growth profiles of macrosomic and non-macrosomic infants of women with pregestational or gestational diabetes. Ultrasound Obstet Gynecol 2013;41(4):390–397. [DOI] [PubMed] [Google Scholar]
- 30.Sovio U, Murphy HR, Smith GC. Accelerated Fetal Growth Prior to Diagnosis of Gestational Diabetes Mellitus: A Prospective Cohort Study of Nulliparous Women. Diabetes Care 2016;39(6):982–987. [DOI] [PubMed] [Google Scholar]
- 31.Brand JS, West J, Tuffnell D, et al. Gestational diabetes and ultrasound-assessed fetal growth in South Asian and White European women: findings from a prospective pregnancy cohort. BMC Medicine 2018;16(1):203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Li M, Hinkle SN, Grantz KL, et al. Glycaemic status during pregnancy and longitudinal measures of fetal growth in a multi-racial US population: a prospective cohort study. Lancet Diabetes Endocrinol 2020;8(4):292–300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Desoye G The Human Placenta in Diabetes and Obesity: Friend or Foe? The 2017 Norbert Freinkel Award Lecture. Diabetes Care 2018;41(7):1362–1369. [DOI] [PubMed] [Google Scholar]
- 34.Desoye G, Nolan CJ. The fetal glucose steal: an underappreciated phenomenon in diabetic pregnancy. Diabetologia 2016;59(6):1089–1094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Mori M, Krumholz HM, Allore HG. Using Latent Class Analysis to Identify Hidden Clinical Phenotypes. JAMA 2020;324(7):700–701. [DOI] [PubMed] [Google Scholar]
- 36.Papageorghiou AT, Kennedy SH, Salomon LJ, et al. The INTERGROWTH-21st fetal growth standards: toward the global integration of pregnancy and pediatric care. American Journal of Obstetrics & Gynecology 2018;218(2):S630–S640. [DOI] [PubMed] [Google Scholar]
- 37.Dudley NJ. A systematic review of the ultrasound estimation of fetal weight. Ultrasound Obstet Gynecol 2005;25(1):80–89. [DOI] [PubMed] [Google Scholar]
- 38.Nesbitt-Hawes EM, Tetstall E, Gee K, Welsh AW. Ultrasound (in)accuracy: it’s in the formulae not in the technique - assessment of accuracy of abdominal circumference measurement in term pregnancies. Australas J Ultrasound Med 2014;17(1):38–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.