

Abstract
Introduction:
Women of reproductive age are less prone to cardiovascular disease (CVD) than men. However, diabetes (DM) negates this female advantage. The prevalence change of pre-diabetes (pre-DM) and DM, and DM-associated cardiovascular risk factors have not been clearly described in women before menopause.
Methods:
Using NHANES data (1999–2018), this study estimated the age-adjusted prevalence of pre-DM (2005–2018), diagnosed DM, and undiagnosed DM in premenopausal women. Logistic regression was used to examine cardiovascular risk factors including obesity, central obesity, hypercholesterolemia, hypertension, and hypertriglyceridemia associated with pre-DM, diagnosed DM, or undiagnosed DM in premenopausal women. The magnitude of the association with age-matched men and postmenopausal women was compared. The analysis was conducted in 2022.
Results:
Premenopausal women experienced an increased prevalence of pre-DM and undiagnosed DM, contrasting with steady trends in all U.S. adults over the last 2 decades. Premenopausal women with pre-DM or DM (vs normoglycemia) have significant obesity risk, and the risk is equivalent to age-matched men and higher than postmenopausal women. The association between pre-DM and hypercholesterolemia or hypertriglyceridemia was significant in premenopausal women only. Hypercholesterolemia or hypertension associated with undiagnosed DM was significant in premenopausal women and men of the same age, respectively. Diagnosed and Undiagnosed DM was associated with hypertriglyceridemia in men and postmenopausal women, respectively.
Conclusions:
Premenopausal women had increased pre-DM and undiagnosed DM in the past 2 decades. They face a considerable cardiovascular risk burden associated with pre-DM and DM. Cardiometabolic risk screening and patient education should be improved in young and early middle-aged adults, particularly in women.
INTRODUCTION
Women of reproductive age are less prone to cardiovascular disease (CVD) than men, partly due to the cardio-protection of estrogens. However, diabetes (DM) negates this female advantage.1 Of note, women can develop CVD with a lower glucose level than men and may be at a higher risk of CVD associated with pre-diabetes (pre-DM).2,3 Compared to men, women are more likely to have undiagnosed DM due to inequitable healthcare access and screening and lower disease risk awareness.4 Untreated DM is associated with a higher mortality risk and CVD hospitalization than diagnosed/controlled DM.5 Among individuals with pre-DM or undiagnosed DM, the raised cardiometabolic risk factors are likely to go undetected and untreated, contributing to future risk of CVD, particularly in women. Understanding of cardiovascular complications in DM and the sex difference in diabetic CVD are primarily based on late middle-aged and elderly cohorts.6–9 Premenopausal women with pre-DM or DM may already have accumulated more pronounced cardiometabolic risks than men of the same age, which is yet to be verified. Further, the prevalence change of pre-DM and DM among premenopausal women has not been clearly described. This study examined the 20-year trends of pre-DM, diagnosed and undiagnosed DM, and associated cardiometabolic risk factors in premenopausal women compared with age-matched men and postmenopausal women.
METHODS
Data were drawn from the National Health and Nutrition Examination Survey (NHANES) (1999–2000 to 2017–2018).10 The study included men and non-pregnant women 20–84 years with information on DM measurements, menopause status (women), and other key covariates. For regression analysis, we excluded those with a previous history of CVD (Appendix Figure 1).
Premenopausal status was defined by having regular periods over the last 12 months, without regular periods not due to menopause (i.e., pregnancy, breastfeeding, medical conditions/treatments, including contraceptive use), or being younger than 41 years.11 A lower limit of 41 years was chosen for premenopause because the average age of menopause in the U.S. is 51-years-old, and perimenopause may last up to 10 years.12,13 Postmenopausal women in this study were those without regular periods over the last 12 months due to menopause.
Diagnosed DM was self-reported. For those without a diagnosis, fasting glucose (FG) ≥126 mg/dL, HbA1c≥6.5% (FG and HbA1c were available all cycles), or oral glucose tolerance test (OGTT) ≥200 mg/dL (available from cycle 2005–2006 to 2017–2018) were classified as undiagnosed DM. Pre-DM was defined by FG 100–126 mg/dL, HbA1c 5.7%–6.5%, or OGTT 140–200 mg/dL.14
Outcomes included obesity (BMI≥30 kg/m2), central obesity (waist circumference≥102 cm in men and ≥88 cm in women), hypercholesterolemia (total cholesterol ≥240 mg/dL), hypertension (systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg), and hypertriglyceridemia (triglycerides ≥200mg/dL).
The study calculated the age-adjusted prevalence of pre-DM, diagnosed and undiagnosed DM by the direct methods of the 2000 U.S. Census standard population. Multivariable logistic regressions were performed for the association between cardiometabolic risk factors and pre-DM, diagnosed and undiagnosed DM in premenopausal women, age-matched men (1:1 match Appendix Text 1), and postmenopausal women adjusted for age, race/ethnicity, education, income, insurance, smoking, BMI, total calorie intake, physical activity, and use of any anti-hypertensive or lipid-lowering medications. The study employed survey-related commands to adjust for the complex survey design effect. The primary sampling unit and stratum for each observation were considered in the analyses. SAS version 9.4 (SAS Institute Cary, NC) was used for analysis.
RESULTS
In women of reproductive age, nearly 1 in 4 had pre-DM, 5.2% had diagnosed DM, and 2.5% had undiagnosed DM (Appendix Tables 1 and 2). The result showed an increased prevalence of pre-DM in premenopausal women, rising from 20% in years 2005–2008 to 28% in the years 2015–2018, contrasting with the high but steady trend of pre-DM in all adults (~34.5%). The prevalence of undiagnosed DM in premenopausal women doubled from the years 1999–2002 (1.7%) to the years 2015–2018 (3.5%) as opposed to a slight decline in all adults (3.1% to 2.9%). Diagnosed DM steadily increased in premenopausal women (Figure 1).
Figure 1.
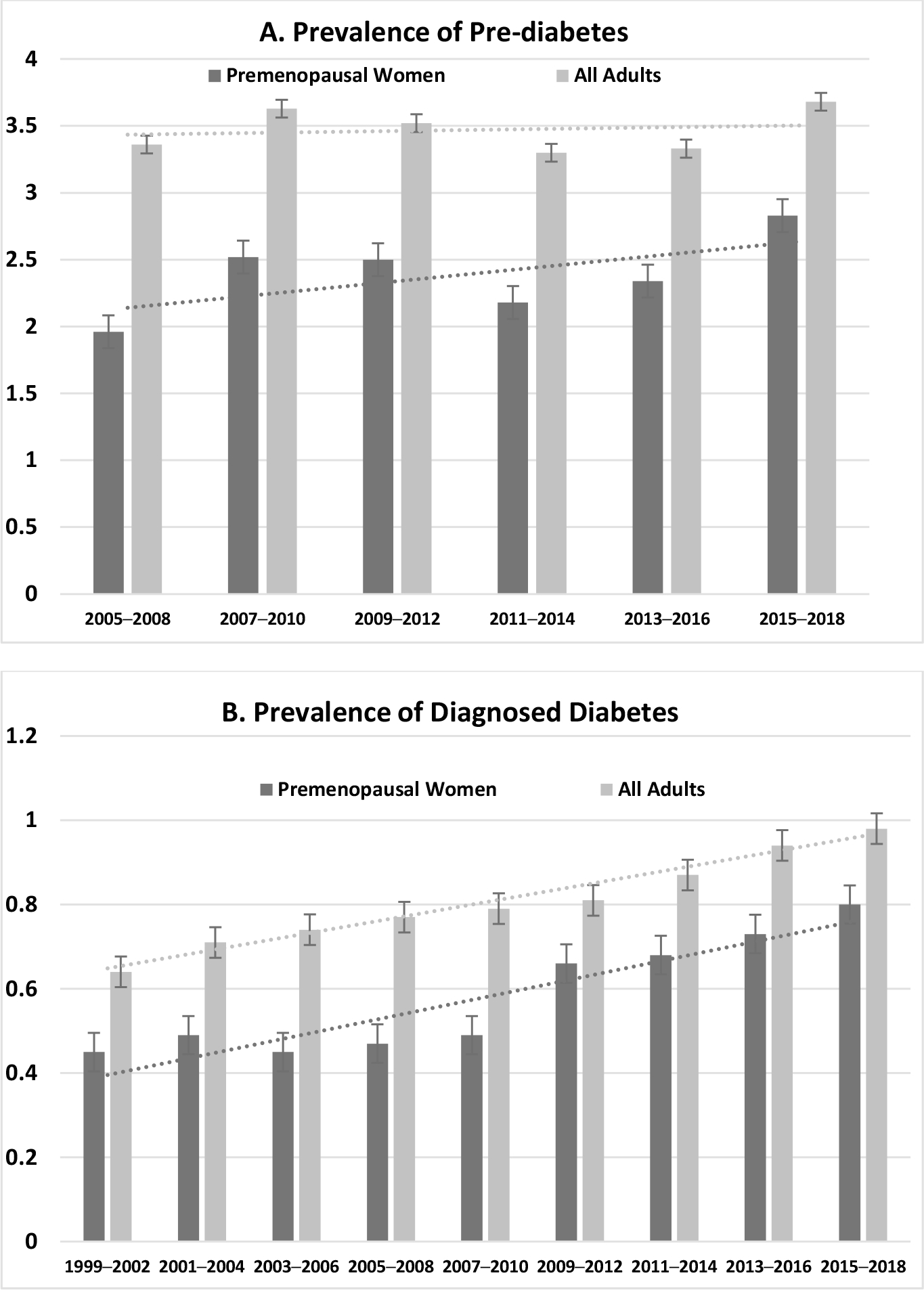
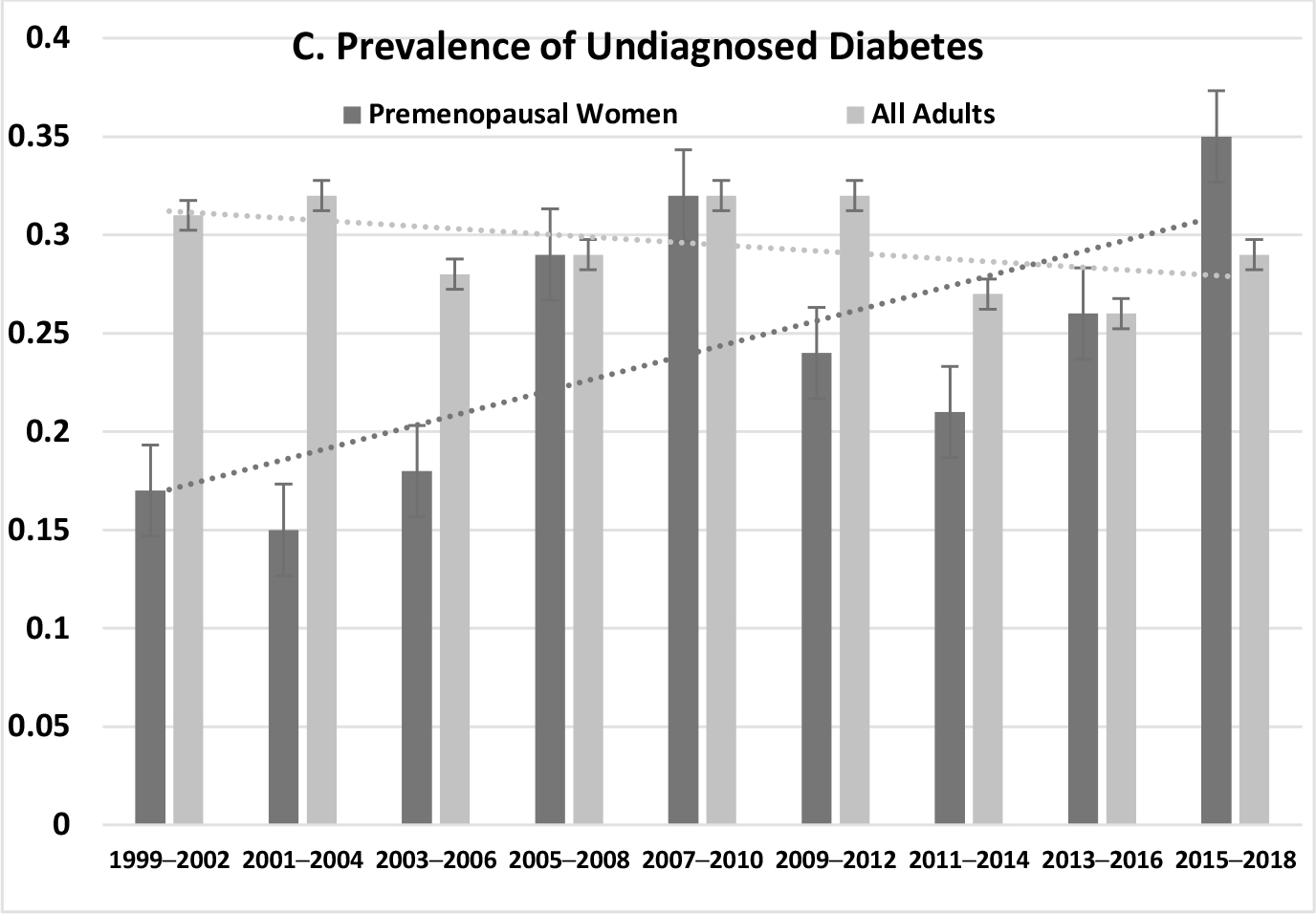
Age-adjusted prevalence of pre-diabetes (A), diagnosed (B), undiagnosed diabetes (C) in premenopausal women (W) and all adults, NHANES 1999–2000 to 2017–2018.
NHANES, National Health and Nutrition Examination Survey.
In adjusted analysis, premenopausal women with pre-DM were associated with an almost 3-fold risk of obesity (OR=2.8, 95% CI=2.1, 3.7) and central obesity (OR=2.8, 95% CI=2, 3.9) than those with normoglycemia; the magnitude of the association was less pronounced in age-matched men or postmenopausal women. Undiagnosed DM was associated with over 4-fold obesity risk in premenopausal women (obesity OR=5.4, 95% CI=2.6, 11.4, central obesity OR=4, 95% CI=1.2, 12.9) and men (obesity OR=4.8, 95% CI=1.8, 12.6, central obesity OR=4.6, 95% CI=2, 10.2), and 2-fold obesity risk in postmenopausal women (obesity OR=2, 95% CI=1.3, 3.2, central obesity OR=2.6, 95% CI=1.3, 4.7). The magnitude of the association between diagnosed DM and obesity/central obesity was greater in premenopausal women than in age-matched men or postmenopausal women (Figure 2).
Figure 2.
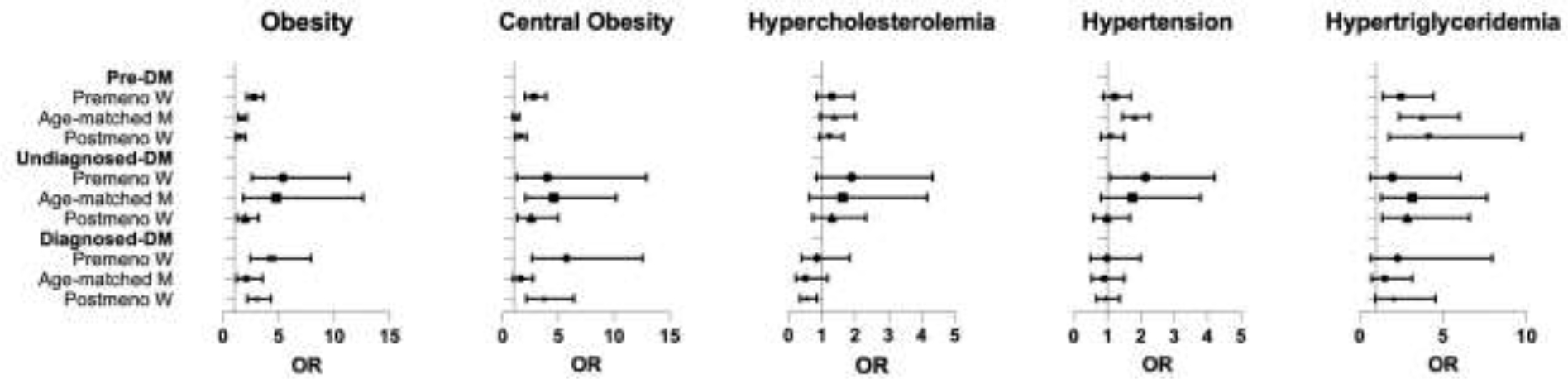
AORa of pre-diabetes, diagnosed and undiagnosed diabetes, and cardiometabolic risk factors in premenopausal women, age-matched men, and postmenopausal women, NHANES 1999–2000 to 2017–2018.
aAdjusted for age, race/ethnicity, education, income, insurance, smoking, BMI, total calorie intake, physical activity, and use of any anti-hypertensive or lipid-lowering medications. The reference group in each logistic regression was individuals with normoglycemia (i.e., premenopausal women with normoglycemia, age-matched men with normoglycemia, and postmenopausal women with normoglycemia).
NHANES, National Health and Nutrition Examination Survey.
The association between undiagnosed DM and hypertension was significant in premenopausal women only (OR=2.1, 95% CI=1.1, 4.2), whereas the association between pre-DM and hypertension was significant in age-matched men only. Pre-DM was associated with hypertriglyceridemia risk in premenopausal women (OR=2.5, 95% CI=1.4, 4.4), age-matched men (OR=3.8, 95% CI=2.4, 6), and postmenopausal women (OR=4.1, 95% CI=1.7, 9.7). Undiagnosed DM was associated with hypertriglyceridemia risk in age-matched men (OR=3.1, 95% CI=1.3, 7.6) and postmenopausal women (OR=2.8, 95% CI=1.3, 6.6) but not in premenopausal women (Figure 2).
DISCUSSION
The study found upward trends of undiagnosed DM and pre-DM among premenopausal women. In all adults, a declining trend of undiagnosed DM is related to changes in diabetes diagnostic and screening practices.15 The increasing prevalence of undiagnosed DM and pre-DM in premenopausal women signals a lack of screening and low awareness of DM risk in this group relative to men of the same age and older women. Additionally, the upward trends of pre-DM and DM in premenopausal women run parallel to the rising obesity in young and middle-aged adults,16 suggesting the need for a more robust effort to improve nutrition and physical activity in women of reproductive age.
Premenopausal women with pre-DM or DM face more cardiometabolic risk factors than those with normoglycemia. Notably, their risk profiles were equivalent to or even worse than men of the same age and postmenopausal women. Previous research suggests that obesity, hypertension, and dyslipidemia are concomitant risk factors in DM, and aggregation of these risk factors synergistically increases the risk of CVD.6–9 However, these findings were mainly derived from middle-aged or elderly cohorts.6–9 This study quantifies the extent to which pre-DM, diagnosed, and undiagnosed DM correlates with cardiometabolic risk factors in women of reproductive age and highlights the concerning cardiovascular consequences if risk factors are left uncontrolled. These findings, in part, explains women’s disadvantage in diabetic CVD in middle and late adulthood and suggest the decline of cardiometabolic health in women starts as early as young adulthood. Limitations of this study included self-reported menopausal status. Also, the cross-sectional design of NHANES precludes quantifying future CVD risk in premenopausal women.
CONCLUSIONS
Though premenopausal women have a lower prevalence of Pre-DM, DM, and undiagnosed DM, all 3 conditions have been increasing at a greater rate among women of reproductive age relative to the overall adult population. Premenopausal women face a significant cardiovascular risk burden associated with pre-DM and DM. This study indicates the need to increase cardiometabolic risk screening and improve patient education around the risks and consequences of pre-DM and DM in women of reproductive age.
Supplementary Material
Footnotes
No conflicts of interest or financial disclosures were reported by the authors of this paper.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
REFERENCES
- 1.Mauvais-Jarvis F Gender differences in glucose homeostasis and diabetes. Physiol Behav. 2018;187:20–23. 10.1016/j.physbeh.2017.08.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Koro CE, Bowlin SJ, Rabatin V, Fedder DO. Cardiovascular disease risk among subjects with impaired fasting glucose in the United States: Results from NHANES 1999 2004. Diabetes Metab Syndr. 2008;2:239–244. 10.1016/j.dsx.2008.07.003. [DOI] [Google Scholar]
- 3.Levitzky YS, Pencina MJ, D’Agostino RB, et al. Impact of impaired fasting glucose on cardiovascular disease: the Framingham Heart Study. J Am Coll Cardiol. 2008;51(3):264–270. 10.1016/j.jacc.2007.09.038. [DOI] [PubMed] [Google Scholar]
- 4.Danaei G, Friedman AB, Oza S, Murray CJL, Ezzati M. Diabetes prevalence and diagnosis in US states: analysis of health surveys. Popul Health Metr. 2009;7(1):16. 10.1186/1478-7954-7-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Navarro-Pérez J, Orozco-Beltran D, Gil-Guillen V, et al. Mortality and cardiovascular disease burden of uncontrolled diabetes in a registry-based cohort: the ESCARVAL-risk study. BMC Cardiovasc Disord. 2018;18(1):180. 10.1186/s12872-018-0914-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hubbard D, Colantonio LD, Tanner RM, et al. Prediabetes and Risk for Cardiovascular Disease by Hypertension Status in Black Adults: The Jackson Heart Study. Diabetes Care. 2019;42(12):2322–2329. 10.2337/dc19-1074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Abdelbagi O, Musa IR, Musa SM, Altigani SA, Adam I. Prevalence and associated factors of hypertension among adults with diabetes mellitus in northern Sudan: a cross-sectional study. BMC Cardiovasc Disord. 2021;21(1):168. 10.1186/s12872-021-01983-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ballantyne CM, Hoogeveen RC, McNeill AM, et al. Metabolic syndrome risk for cardiovascular disease and diabetes in the ARIC study. Int J Obes (Lond). 2008;32(Suppl 2):S21–24. 10.1038/ijo.2008.31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wong ND, Zhao Y, Patel R, et al. Cardiovascular Risk Factor Targets and Cardiovascular Disease Event Risk in Diabetes: A Pooling Project of the Atherosclerosis Risk in Communities Study, Multi-Ethnic Study of Atherosclerosis, and Jackson Heart Study. Diabetes Care. 2016;39(5):668–676. 10.2337/dc15-2439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.About National Health and Nutrition Examination Survey. https://www.cdc.gov/nchs/nhanes/about_nhanes.htm. Accessed October 2019.
- 11.Shirazi TN, Hastings WJ, Rosinger AY, Ryan CP. Parity predicts biological age acceleration in postmenopausal, but not premenopausal, women. Sci Rep. 2020;10(1):20522. 10.1038/s41598-020-77082-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lobo RA. Chapter 15 - Menopause and Aging. In: Strauss JF, Barbieri RL, eds. Yen & Jaffe’s Reproductive Endocrinology (Seventh Edition). Philadelphia: W.B. Saunders; 2014:308–-339.e308.. 10.1016/B978-1-4557-2758-2.00015-9. [DOI] [Google Scholar]
- 13.El Khoudary SR, Aggarwal B, Beckie TM, et al. Menopause Transition and Cardiovascular Disease Risk: Implications for Timing of Early Prevention: A Scientific Statement From the American Heart Association. Circulation. 2020;142(25):e506–e532. 10.1161/CIR.0000000000000912. [DOI] [PubMed] [Google Scholar]
- 14.Association AD. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2021. Diabetes Care. 2020;44(Supplement_1):S15–S33. 10.2337/dc21-S002. [DOI] [PubMed] [Google Scholar]
- 15.Selvin E, Ali MK. Declines in the Incidence of Diabetes in the U.S.-Real Progress or Artifact? Diabetes Care. 2017;40(9):1139–1143. 10.2337/dc16-2442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.National Health and Nutrition Examination Survey 2017-March 2020 Prepandemic Data Files Development of Files and Prevalence Estimates for Selected Health Outcomes, National Health Statistics Reports; (2021). [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.