

Abstract
Objective
To evaluate the adoption and discontinuation of four broadly used non-pharmaceutical interventions on shifts in the covid-19 burden among US states.
Design
Retrospective, observational cohort study.
Setting
US state data on covid-19 between 19 January 2020 and 7 March 2021.
Participants
US population with a diagnosis of covid-19.
Main outcome measures
Empirically derived breakpoints in case and mortality velocities (ie, rate of change) were used to identify periods of stable, decreasing, or increasing covid-19 burden. Associations between adoption of non-pharmaceutical interventions and subsequent decreases in case or death rates were estimated by use of generalised linear models accounting for weekly variability across US states. State level case and mortality counts per day were obtained from the Covid-19 Tracking Project. State level policies on non-pharmaceutical interventions included stay-at-home orders, indoor public gathering bans (mild >10 or severe ≤10 people), indoor restaurant dining bans, and public mask mandates. National policies were not included in statistical models.
Results
28 602 830 cases and 511 899 deaths were recorded during the study. Odds of a reduction in covid-19 case velocity increased for stay-at-home orders (odds ratio 2.02, 95% confidence interval 1.63 to 2.52), indoor dining bans (1.62, 1.25 to 2.10), public mask mandates (2.18, 1.47 to 3.23), and severe indoor public gathering bans (1.68, 1.31 to 2.16) in univariate analysis. In mutually adjusted models, odds remained elevated for orders to stay at home (adjusted odds ratio 1.47, 95% confidence interval 1.04 to 2.07) and public mask mandates (2.27, 1.51 to 3.41). Stay-at-home orders (odds ratio 2.00, 95% confidence interval 1.53 to 2.62; adjusted odds ratio 1.89, 95% confidence interval 1.25 to 2.87) was also associated with a greater likelihood of decrease in death velocity in unadjusted and adjusted models.
Conclusions
State level non-pharmaceutical interventions used in the US during the covid-19 pandemic, in particular stay-at-home orders, were associated with a decreased covid-19 burden.
Keywords: COVID-19, Public health, Health policy, Infection control
What is already known on this topic
Non-pharmaceutical interventions are mitigation strategies used to reduce the spread of transmissible diseases
Research has shown effectiveness of these interventions in mitigating acute transmission of respiratory viruses such as influenza and covid-19 in retrospective observational data and simulated modelling
Quantified effect of different non-pharmaceutical interventions (individually and in combination) in respiratory viral pandemics has remained poorly defined
What this study adds
In a univariate analysis, increased odds of a reduced covid-19 burden was associated with the implementation of all four interventions studied (stay-at-home orders, severe indoor public gathering bans, indoor restaurant dining bans, and public mask mandates); these trends persisted in adjusted models
How this study might affect research, practice, or policy
These results should encourage additional analysis of non-pharmaceutical interventions in the US and international populations for covid-19 and future respiratory viral pandemics
These findings further support public policies using early and layered non-pharmaceutical interventions for mitigating the transmission of respiratory pathogens
Introduction
Non-pharmaceutical interventions are mitigation strategies that have been used to control the spread of transmissible diseases, epidemics, and pandemics for more than 100 years.1 2 During the covid-19 pandemic, a variety of these interventions were adopted and discontinued by state governments. Strategies in the US included travel bans, declarations of emergency situations, social distancing campaigns, self-quarantine on infection or known exposure, and universal facial masking recommendations.3 4 These strategies were adopted and discontinued with varying timing and relation to the severity of the pandemic across US states. Despite efforts to mitigate covid-19 spread, the US has reported more than 80 million cases and more than 1 million deaths related to covid-19.5 In 2020, covid-19 was the third leading cause of death in the US and was associated with a reduction in life expectancy of 1 year.6
Research on pandemic influenza has previously helped describe the use and effectiveness of non-pharmaceutical interventions in the US.7–14 Some of the highest quality research evaluating positive effect of these interventions was performed by Markel et al, who evaluated US cities and six relatively isolated communities during the 1918-19 influenza pandemic.13 14 Although these studies were important in demonstrating effect of non-pharmaceutical interventions on highly transmissible respiratory illnesses, such strategies in most US communities did not prevent the spread of the 1918 influenza virus. In subsequent influenza pandemics, fewer non-pharmaceutical interventions were implemented owing to milder observed case fatality ratios and suspected futility of intervention.2 15–18 Quantified effect of different strategies (individually and in combination) on case and mortality burden of pandemic influenzas of varying transmissibility has remained poorly defined.
Since the onset of the covid-19 pandemic, several researchers have commented on the effect of non-pharmaceutical interventions and covid-19 burden.19–22 Singh et al19 found that in the US from 1 January to 3 June 2020, introducing such interventions can reduce covid-19 cases, but did not offer additional benefit after 12 weeks. Yang et al20 found associations between reductions in the weekly effective reproductive numbers of covid-19 cases and multiple non-pharmaceutical interventions from 21 January to 5 July 2020. However, the heavy weighting on school closure in the study's modelling (association with covid-19 transmission was 2.5 times stronger with school closure than with a stay-at-home order) was concerning for considerable confounding. These studies and others highlight that most research has focused on non-pharmaceutical interventions individually or in broad groups, not accounting for multiple interventions over time or the relative effectiveness of each in an effective manner.19–21 23–26 Studies focused in Europe27 28 and worldwide27 29 30 have also reported effectiveness of these interventions in the context of covid-19, with similar limitations and concerns.
This study aimed to evaluate the adoption and discontinuation of four broadly used non-pharmaceutical interventions (stay-at-home order, indoor restaurant dining ban, public mask mandate, and indoor public gathering ban) on shifts in the covid-19 burden among US states.
Methods
Study design, setting, and population
We performed a retrospective, observational cohort study of the US population between 19 January 2020 (first covid-19 diagnosis in the US) and 7 March 2021. The primary analysis evaluated the dates of state specific adoption or discontinuation of non-pharmaceutical interventions on covid-19 case and mortality rates.
Data collection
State level case and mortality counts per day were obtained from the Covid-19 Tracking Project,31 which aggregate public reports of covid-19 diagnostic and death certification data for the US. The data reported are obtained from state public health authorities or official media accounts.24 32 The dominant covid-19 virus during the period of study was the original virus (SARS CoV-2), followed by the alpha variant (B.1.1.7) at the end of the observational period.33 34
We obtained dates for adoption and discontinuation of non-pharmaceutical interventions studied from publicly available reports (online supplemental table S1).24 35–40 Policies that were incorporated into the analysis included orders to stay at home, indoor public gathering bans (mild or severe), indoor restaurant dining bans, and public mask mandates. We recorded dates for each policy adoption or discontinuation from 21 February 2020 to 29 January 2021 for the time dependent modelling. When sources were not in agreement with the date of adoption or discontinuation, we reviewed executive orders and media outlet publications.
bmjmed-2021-000030supp001.pdf (1.1MB, pdf)
Definitions were set for each non-pharmaceutical intervention used. We defined indoor public gathering bans with a maximum of 10 or fewer people as severe, and indoor public gathering bans with more than 10 people as mild. Indoor restaurant dining bans were adopted when indoor dining was banned and were discontinued when indoor dining was reinstated, regardless of capacity specification or outdoor dining policies. Public mask mandates also applied to indoor mandates, regardless of outdoor policy. We defined stay-at-home orders as any statewide policy ordering discontinuation of all non-essential travel from home.
Statistical analysis
We used each state’s daily case and death counts to model the rate of change in the number of cases and deaths due to covid-19 per week (velocity). We obtained case and death velocity by taking the first derivative with respect to time of the log cumulative daily case (and death) counts reported at the state level.41 We defined establishment of community transmission (≥100 confirmed cases for each state) as time zero. Cubic splines were fit to the log cumulative counts to facilitate precise calculation of the first derivative with respect to time. We applied a log link to map the case (or death) velocities to the entire real line which allowed for modelling of velocities as a linear function.
We used a breakpoint analysis to evaluate changes in case velocity attributable to policy adoptions or discontinuations. This approach identifies time periods with deviations in the covid-19 case or death velocity rates. A change in covid-19 growth rate is determined if adding a new regression slope at a specific date decreases the residual sum of squares sufficiently to improve the bayesian information criterion. Breakpoints were empirically identified for each state using the strucchange R package for dating structural changes in regression models.42 A minimal segment length of 14 days was set by specifying a minimum number of observations per segment (14). As a result of the minimal segment size specification, each state had at most one breakpoint per 7 day week, which allowed for determination of whether a state experienced an increase, decrease, or no change in each week. We excluded breakpoints after 5 February 2021 for cases and 12 February 2021 for deaths to align with the data of adoption and discontinuation dates of non-pharmaceutical interventions, which extended up to 29 January 2021, plus anticipated lag time.
Assessments of the impact of policy adoption assumed prespecified lag times related to the natural course of transmission and disease. We estimated lags of 3-10 days from policy adoption to changes in transmission, 5-10 days from infection to covid-19 diagnosis, and 6-15 days from covid-19 diagnosis to death (online supplemental material). Based on these intervals, we considered policies adopted between 0 and 21 days (0-3 weeks; ie, lag time) before the start date in each week as potentially influential to case velocity. We considered policies adopted between seven and 35 days (1-5 weeks) before the start date of a given week as potentially significant to death velocity. We created generalised linear models from generalised estimating equations to evaluate policy changes in relation to shifts in covid-19 case and death velocities. We defined a three level outcome variable for case and death velocities (increase, no change, or decrease). Ordinal logistic regression with a cumulative logit link function modelled the probability of a state week corresponding to a decrease in case (or death) velocity versus no change, and no change versus an increase in case (or death) velocity.
We specified an independent working correlation structure to account for correlation within US states. We fit two sets of models that included a fixed effect for the given modelled policy (a separate unadjusted model for each policy), and a fixed effect for each policy (one adjusted model for all four policies). We subsequently describe this second set of models with the term mutually adjusted model in this article. Time variability shared across states was accounted for by including week number as a continuous fixed effect and using three change points to allow for piecewise trends during phases of the pandemic. We aligned four phases with the modelled calendar weeks (online supplemental material).
To account for uncertainty in our natural history estimations described, we performed a sensitivity analysis of shifting the lag time interval by 7 days before or 7 days after our base assumption of lag time (online supplemental material). The sensitivity analysis was a check to determine whether the lag times we chose up front (not biased by the data) were reasonable. We chose the lag times before analysis on the basis of what we thought was reasonable based on review of covid-19 transmission (online supplemental material). The analysis also explored, in a novel but limited fashion, how optimal lag times between adoption or discontinuation of non-pharmaceutical interventions and potential impacts in covid-19 case or death velocity might differ by intervention.
Policy models were fit to data consisting of one observation per state, per week, starting with the first week in which a breakpoint was observed. To summarise results from the cumulative logit model formulation, we use the phrase "decrease in case velocity" to imply either the probability of observing a decreasing breakpoint versus no change or observing no change versus an increasing breakpoint. Analyses were performed in R 4.0.3 (R Foundation for Statistical Computing, Vienna, Austria).43
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Results
During the period studied, we recorded 28 602 830 cases and 511 899 deaths, and a total of 409 adoptions and discontinuations of non-pharmaceutical interventions (online supplemental table S1). States were recorded and ranked by total cases per capita as of 7 March 2021 (online supplemental table S2). Timelines for the US states with the three highest and lowest case burdens of covid-19 are depicted as examples of variability in use of non-pharmaceutical intervention (figure 1).
Figure 1.

Timeline of non-pharmaceutical interventions for US states with the three lowest (top row) and three highest (bottom row) numbers of covid-19 cases per capita, as of 7 March 2021. For indoor public gathering bans, mild refers to gatherings of more than 10 people; severe refers to gatherings of 10 people or fewer. Numbers of covid-19 cases per capita per 100 000 people are Hawaii 2020, Vermont 2568, Maine 3422, Rhode Island 12 180, South Dakota 12 875, and North Dakota 13 208
Associations between non-pharmaceutical interventions and covid-19 case velocities
We identified 603 case breakpoints (table 1). A decrease in case velocity was observed in 433 (71.8%) breakpoints and an increase in case velocity was observed in 170 (28.2%). Across all 50 US states, the median number of case breakpoints was 12 (range 7-17). We graphed the number of breakpoints with an increase in case velocity and a decrease in case velocity chronologically (online supplemental figure S2), and plotted cumulative cases over time with their estimated breakpoints for the states with the three highest and lowest covid-19 burdens, according to cases per capita (figure 2). Plots of the derivative of the logarithm of cumulative cases (velocity) and the logarithm of the derivative of the logarithm (data implemented in modelling) for these states are available in online supplemental figures S4 and S5).
Table 1.
Status of non-pharmaceutical interventions relative to covid-19 case and death rates in US states, per state week. Data are number (%) of state weeks of each breakpoint type falling within observation period for adoption or discontinuation of a non-pharmaceutical intervention (7-21 days for cases, 14-35 days for deaths)
| Type and status of non-pharmaceutical intervention | Count of breakpoint types* | |||||
| Case velocity (2350 state weeks) |
Death velocity (2350 state weeks) |
|||||
| Decrease (433 breakpoints) |
No change (1747 breakpoints) |
Increase (170 breakpoints) | Decrease (330 breakpoints) | No change (1889 breakpoints) |
Increase (131 breakpoints) | |
| Stay-at-home order—on | 45 (10.4) | 72 (4.1) | 0 | 53 (16.1) | 103 (5.5) | 0 |
| Stay-at-home order—off | 22 (5.1) | 84 (4.8) | 9 (5.3) | 33 (10.0) | 116 (6.1) | 4 (3.1) |
| Indoor restaurant dining ban—on | 52 (12.0) | 109 (6.2) | 1 (0.6) | 57 (17.3) | 157 (8.3) | 2 (1.5) |
| Indoor restaurant dining ban—off | 32 (7.4) | 112 (6.4) | 12 (7.1) | 39 (11.8) | 161 (8.5) | 6 (4.6) |
| Public mask mandate—on | 29 (6.7) | 79 (4.5) | 3 (1.8) | 23 (7.0) | 121 (6.4) | 4 (3.1) |
| Indoor public gathering ban (mild)—on | 38 (8.8) | 154 (8.8) | 18 (10.6) | 59 (17.9) | 210 (11.1) | 10 (7.6) |
| Indoor public gathering ban (severe)—on | 62 (14.3) | 123 (7.0) | 1 (0.6) | 65 (19.7) | 177 (9.4) | 4 (3.1) |
| Indoor public gathering ban—off | 5 (1.2) | 35 (2.0) | 4 (2.4) | 8 (2.4) | 47 (2.5) | 2 (1.5) |
Velocity=rate of change in the number of cases and deaths due to covid-19 per week.
*Breakpoint segments were categorised as decreasing, no change, or increasing for the covid-19 case and death velocity analysis.
Figure 2.
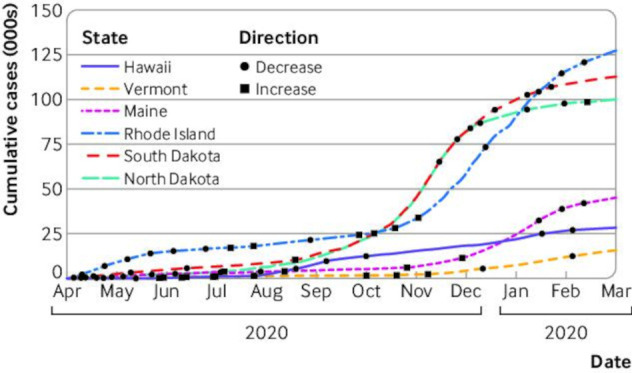
Cumulative covid-19 cases and the breakpoints identified for US states with three lowest and highest covid-19 cases per capita, as of 7 March 2021. Breakpoints, dates when linear segments of covid-19 case velocities showed substantial change in rate, were plotted over the linear plot of cases for each respective US state
Ordinal logistic regression models including a single policy adoption or discontinuation estimated increased odds of a decrease in case velocity after adoption of stay-at-home orders (odds ratio 2.02, 95% confidence interval 1.63 to 2.52), indoor restaurant dining bans (1.62, 1.25 to 2.10), public mask mandates (2.18, 1.47 to 3.23), and severe indoor public gathering bans (1.68, 1.31 to 2.16). Adoption of a mild indoor public gathering ban was associated with decreased odds of a reduction in case velocity (0.51, 0.39 to 0.68; table 2). In sensitivity analysis, discontinuation of indoor restaurant dining bans trended toward progressive association with decreasing odds of a reduction in case velocity as lag time was extended from baseline assumptions (ie, allowing additional time between policy discontinuation and measurement of effect; online supplemental eTable 1). The strongest association of decreased odds of a reduction in case velocity in sensitivity analysis was for a time lag time shifted 7 days more distal than our base assumption (odds ratio 0.39, 95% confidence interval 0.26 to 0.60; online supplemental eTable 1). Progressive strength of association with increased lag time was also noted for both adoption and discontinuation of stay-at-home orders, adoption of public mask mandates, and adoption of severe indoor public gathering bans (online supplemental eTable 1).
Table 2.
Association between non-pharmaceutical interventions and odds of decreasing covid-19 case and death burden in US state level data: one model per intervention
| Type and status of non-pharmaceutical intervention | Covid-19 cases | Covid-19 deaths | ||
| Odds ratio (95% CI) | P value | Odds ratio (95% CI) | P value | |
| Stay-at-home order—on | 2.02 (1.63 to 2.52) | <0.001 | 2.00 (1.53 to 2.62) | <0.001 |
| Stay-at-home order—off | 0.87 (0.53 to 1.42) | 0.57 | 1.21 (0.89 to 1.63) | 0.22 |
| Indoor restaurant dining ban—on | 1.62 (1.25 to 2.10) | <0.001 | 1.50 (1.15 to 1.95) | 0.002 |
| Indoor restaurant dining ban—off | 0.94 (0.60 to 1.45) | 0.77 | 1.04 (0.78 to 1.41) | 0.76 |
| Public mask mandate—on | 2.18 (1.47 to 3.23) | <0.001 | 1.39 (0.94 to 2.05) | 0.10 |
| Indoor public gathering ban (mild)—on | 0.51 (0.39 to 0.68) | <0.001 | 0.86 (0.62 to 1.18) | 0.34 |
| Indoor public gathering ban (severe)—on | 1.68 (1.31 to 2.16) | <0.001 | 1.45 (1.12 to 1.88) | 0.004 |
| Indoor public gathering ban—off | 0.64 (0.29 to 1.40) | 0.27 | 1.19 (0.65 to 2.19) | 0.57 |
CI=confidence interval. An odds ratio greater than 1 is associated with an increased probability that the covid-19 case or death velocities decreased. Each non-pharmaceutical intervention analysed in an individual model. For indoor public gathering bans, mild refers to gatherings of more than 10 people; severe refers to gatherings of 10 people or fewer. Indoor restaurant dining bans were adopted when indoor dining was banned and were discontinued when indoor dining was reinstated, regardless of capacity specification or outdoor dining policies.
In mutually adjusted models, adoption of a stay-at-home order was associated with decreasing case velocity (adjusted odds ratio 1.47, 95% confidence interval 1.04 to 2.07), as was adoption of a public masking mandate (2.27, 1.51 to 3.41). Adoption of a mild indoor public gathering ban was associated with a subsequent increase in case velocities (0.46, 0.34 to 0.61), yet adoption of a severe indoor indoor public gathering ban trended toward the opposite association (1.38, 0.97 to 1.95; table 3). In sensitivity analysis, adoption of indoor restaurant dining ban was associated with decreasing case velocity for a lag time shifted 7 days more distal than our base assumption (2.05, 1.22 to 3.45; online supplemental eTable 2). Associations to case velocity were also strongest at a lag time 7 days greater lthan our base assumption for the adoption of indoor restaurant dining bans, discontinuation of indoor restaurant dining bans, and adoption of public mask mandates (online supplemental eTable 2).
Table 3.
Association between non-pharmaceutical interventions and odds of decreasing covid-19 case and death burden in US state level data: one model including all interventions
| Type and status of non-pharmaceutical intervention | Cases | Deaths | ||
| Adjusted odds ratio (95% CI) | P value | Adjusted odds ratio (95% CI) | P value | |
| Stay-at-home order—on | 1.47 (1.04 to 2.07) | 0.03 | 1.89 (1.25 to 2.87) | 0.003 |
| Stay-at-home order—off | 0.93 (0.56 to 1.55) | 0.79 | 1.28 (0.89 to 1.85) | 0.19 |
| Indoor restaurant dining ban—on | 1.47 (0.96 to 2.26) | 0.07 | 1.15 (0.76 to 1.74) | 0.50 |
| Indoor restaurant dining ban—off | 1.25 (0.77 to 2.03) | 0.37 | 1.13 (0.81 to 1.59) | 0.48 |
| Public mask mandate—on | 2.27 (1.51 to 3.41) | <0.001 | 1.45 (0.97 to 2.17) | 0.07 |
| Indoor public gathering ban (mild)—on | 0.46 (0.34 to 0.61) | <0.001 | 0.78 (0.56 to 1.09) | 0.15 |
| Indoor public gathering ban (severe)—on | 1.38 (0.97 to 1.95) | 0.07 | 1.08 (0.72 to 1.64) | 0.69 |
| Indoor public gathering ban—off | 0.64 (0.30 to 1.39) | 0.26 | 1.16 (0.62 to 2.17) | 0.64 |
CI=confidence interval. An adjusted odds ratio greater than 1 is associated with an increased probability that the covid-19 case or death velocities decreased. All four non-pharmaceutical interventions were included as covariates in this model. For indoor public gathering bans, mild refers to gatherings of more than 10 people; severe refers to gatherings of 10 people or fewer. Indoor restaurant dining bans were adopted when indoor dining was banned and were discontinued when indoor dining was reinstated, regardless of capacity specification or outdoor dining policies.
Associations between non-pharmaceutical interventions and covid-19 death velocities
A total of 461 death breakpoints were identified (table 1). 330 (71.6%) of breakpoints corresponded to a decrease in death velocity and 131 (28.4%) corresponded to an increase in death velocity. Across all 50 US states, the median number of death breakpoints was 9 (range 4-17; online supplemental figure S3). We plotted cumulative deaths over time with their estimated breakpoints for the states with the three lowest or highest number of covid-19 cases per capita (online supplemental figure S6). Plots of the derivative of the logarithm of cumulative deaths (velocity) and the logarithm of the derivative of the logarithm (data implemented in modelling) for these states are available in the online supplemental figures S7 and S8.
Ordinal logistic regression models including a single policy estimated increased odds of a decrease in death velocity after adoption of stay-at-home orders (odds ratio 2.00, 95% confidence interval 1.53 to 2.62), indoor restaurant dining bans (1.50, 1.15 to 1.95), and severe indoor public gathering bans (1.45, 1.12 to 1.88; table 2). In sensitivity analysis, adoption of public mask mandate was associated with a decrease in death velocity for a lag time shifted 7 days more distal than our base assumption (1.84, 1.29 to 2.62; online supplemntal eTable 1). Associations to death velocity were also strongest at 7 days greater lag time than our base assumption for adoption of stay-at-home orders, adoption of indoor restaurant dining bans, and adoption of severe indoor public gathering bans (online supplemental eTable 1). In mutually adjusted models, institution of an order to stay at home was associated with decreasing death velocity (adjusted odds ratio 1.89, 95% confidence interval 1.25 to 2.87; table 3). Adoption of indoor restaurant dining bans (1.74, 1.15 to 2.63) and adoption of public mask mandates (1.95, 1.35 to 2.82) were associated with a decrease in death velocity for the more distally shifted lag time (online supplemental eTable 2).
Discussion
Principal findings
In our study, we found associations between the adoption of multiple non-pharmaceutical interventions and decreasing covid-19 case and mortality burdens in the US. With respect to cases, our adjusted time dependent models found that stay-at-home orders and public mask mandates were associated with decreases in the rate of new diagnoses of covid-19. Even after adjusting for three other concurrently adopted interventions, public mask mandates were associated with over twice the likelihood of reduced covid-19 transmission. Public mask mandates could encourage behavioural modifications as well as directly reduce the odds of transmission by using a physical barrier.44 45 Covid-19 is now understood to be transmitted primarily through aerosol spread in close contact.46 The US state level observations provide support for mask mandates in reducing the case burden of respiratory epidemics or pandemics.
US states that adopted mild indoor gathering bans had increases in covid-19 case burden relative to states that did not adopt a mild indoor public gathering ban. Results from the mutually adjusted policy model suggested indoor restaurant dining bans and severe indoor public gathering bans could be associated with decreased case velocity (both P<0.10). We found a stronger direction of association with a lag time 7 days more distal than our base assumption, suggesting that indoor dining bans and severe indoor public gathering bans might take longer to confer reductions in case burden.
Overall, we found that gathering bans with limits of more than 10 people were insufficient and were associated with exacerbation of covid-19 spread, possibly because US states often selected these bans as an alternative to the more effective severe ban. Furthermore, different non-pharmaceutical interventions could have been associated with increases or decreases in covid-19 burden owing to behavioural changes linked to the intervention but not specifically resolved by it. For example, indoor public gathering bans with maximums greater than 10 people might not inherently be ineffective in decreasing the burden of covid-19, but they could elicit a different generalised public response, especially relative to those severe bans limiting gatherings to 10 people or fewer. Brauner et al28 made a related finding of progressively stricter gathering bans inferring decreased covid-19 burden, including a median reduction greater than 35% in instantaneous reproduction number associated with the policy adoption of gatherings limited to 10 people or fewer. Overall, these observations are consistent with concerns regarding the indoor transmission of covid-19 among large groups of individuals in public settings. Policies of non-pharmaceutical interventions that discourage large gatherings are effective at reducing respiratory transmission.
With respect to mortality, stay-at-home orders were associated with decreasing covid-19 mortality in unadjusted and adjusted models, and in all sensitivity analyses considered. Additionally, adoption of indoor restaurant dining bans and adoption of public mask mandates were associated with decreasing covid-19 mortality in unadjusted and adjusted models incorporating a lag time 7 days more distal than our base assumption. One explanation of this finding is that the peak onset of effect of these four non-pharmaceutical interventions could differ. Adoption of indoor restaurant dining ban and public mask mandate might take longer to confer benefit, while stay-at-home orders could confer more immediate and sustained benefit. Despite some suggestion of benefit in some non-pharmaceutical interventions with respect to mortality, overall, the strengths of association were more profound for cases than for deaths. Sample size limitations, limited variation in timing of policies adopted, and temporal variation in the progression of covid-19 to death all limit our ability to attribute deviations in daily death counts to specific policy actions. Furthermore, interventions that are associated with case reductions but not mortality could reflect a shift towards infection among younger cohorts at lower risk for death. This observation might be particularly true for the public mask mandates, which appeared in later phases of the covid-19 pandemic.
Comparison with previous studies
Our modelling approach allowed us to evaluate the merits of various non-pharmaceutical interventions concomitantly in a time dependent fashion. Previous studies have generally focused on pandemic influenza and relied on expert opinion or modelling rather than real world data.7 9 13 26 47 In fact, the most recent pandemic influenza plan by the US Department of Health and Human Services described study of non-pharmaceutical interventions in the status of a data collection phase.26 Some retrospective data regarding these interventions and viral pandemics have been published. An analysis of US cities found an association between increased duration of non-pharmaceutical interventions and total mortality reduction.13 Auger et al24 found that school closures were associated with decreased covid-19 incidence and mortality but adjustment for other interventions was not included. Bendavid et al48 reported, in an international comparison of 10 countries including the US, no observable benefit of more restrictive non-pharmaceutical interventions (stay-at-home order, non-essential business closures) compared with less restrictive interventions (social distancing guidelines, discouraging travel, and ban on large gatherings). We find the limited sample size and lack of variation in this study makes an absence of evidence conclusion difficult. Brauner et al28 found an additional inferred decrease in instantaneous reproductive numbers with a stay-at-home order even when accounting for gathering bans, business closure mandates, and school closures.
Although our analysis used a different methodological approach and set of non-pharmaceutical interventions, we also found an additional association of benefit for the interventions—including when we accounted for other interventions adopted. Our analysis found that both the strength and the direction of benefit related to severity of a gathering ban is important when assessing transmission dynamics. We found associations between multiple non-pharmaceutical interventions and decreased case burden of covid-19 in adjusted models (stay-at-home order, public masking mandate, and severe gathering ban), which is supportive of previous expert opinions encouraging early, sustained, and layered application of these interventions to mitigate consequences of pandemic viral disease.
Limitations of the study
Our analyses included several limitations. US state government enforcement of recommendations and policies varied. The public adherence to stated policies might vary owing to regional differences in preferences and beliefs. We did not attempt to measure markers of behavioural change based on the adoption or discontinuation of policies, and focused primarily on outcomes such as known transmission and deaths. We used a breakpoint analysis of smoothed count data (7 day averages) to analyse time periods characterised by similar case velocities. This statistical approach allowed for aggregating time periods across the limited sample of states (n=50). Our model did not adjust for national recommendations and policies. The two most prominent of these announcements included the Centres for Disease Control and Prevention recommendation of wearing cloth face coverings in public from 3 April 20204 and "The President’s Coronavirus Guidelines for America" enacted 16 March 2020, which included avoiding non-essential travel and avoiding social gatherings in groups of more than 10 people.3
Additionally, this study did not account for county or municipal level variation in policies of non-pharmaceutical interventions. The early period of the covid-19 pandemic in the US probably had lower rates of case ascertainment and differences in testing capacity between states. Although we cannot explicitly control testing capacity and policy by state in the statistical models, the availability of diagnostic tests grew linearly during the period of analysis and therefore would be unlikely to explain shifts in either case or death velocities.
This analysis was unable to evaluate the impact of non-pharmaceutical interventions with substantial temporal overlap, such as school closures, and the impact of multiple interventions adopted during concomitant periods could contribute to instability of estimates. We believe that this limitation of temporal overlap should be noted in prior publications.19 20 24 To resolve this limitation, we selected a smaller subset of interventions for evaluation. However, collinearity of these interventions limits our ability to draw the strongest conclusions, but this limitation is inherent in the data and non-experimental design. Although one alternative would have been to present model estimates from univariate analysis only, we believe that the exploratory multiple regression analyses are informative. Evaluation of our models for high correlation (online supplemental material) was reassuring and within expectations for non-pharmaceutical interventions adopted and discontinued at similar dates.
We acknowledge that lower socioeconomic status could associate with a higher covid-19 burden49–51 and could even vary at the state level.19 20 We expect that socioeconomic factors were generally static during our study, especially in comparison with the exponential increases and decreases in covid-19 case or death velocities and the frequent adoption or discontinuation of the four non-pharmaceutical interventions observed. Although socioeconomic factors would influence the intercept of our models, we would not expect changes in case velocity on a week by week basis to be attributable. Importantly, the Coronavirus Aid, Relief, and Economic Security Act (CARES Act), passed by the US Congress and signed into US law on 27 March 2020, homogenised unemployment benefits in the US for most of the duration of our study in both length and amount of benefit.52
Our model also relied on several unverified assumptions, such as the length and placement of the policy adoption window relative to a given week, and the minimal segment specification of two weeks for breakpoint identification. Although these decisions were based on expert knowledge and review of the literature, the impact of these assumptions is unknown. Furthermore, any uncertainty in the establishment of the empirically estimated breakpoints was not reflected in the subsequent policy models, which suggests less precision in our final estimates. We believe that the breakpoint analysis is a more blinded approach to segmenting shifts in case and death counts, compared with arbitrary decisions to create time cutpoints for pandemic waves that have the potential to introduce bias. Finally, although all four of the non-pharmaceutical interventions studied were associated with a decrease in covid-19 cases over the period of study in univariate analysis, we acknowledge that the effect of these interventions on the total number of covid-19 cases and deaths during the ongoing covid-19 pandemic is not known.
Conclusion
Adoption of several non-pharmaceutical interventions used by US states during the covid-19 pandemic were associated with subsequent decreases in covid-19 case burden. When accounting for the adoption of all four interventions modelled, a stay-at-home order was the most strongly associated with decreases in covid-19 mortality. Both restaurant dining and severe indoor public gathering bans (limiting to <10 people) were more strongly associated with reductions in transmission compared with mild indoor public gathering bans (limiting to >10 people). These findings reinforce efforts to deploy non-pharmaceutical interventions early and encourage adherence to limit the spread of dangerous respiratory epidemics.
Footnotes
Twitter: @Mike_AhlersMD
Correction notice: This article has been corrected since it first published. Figure 1 has been replaced to clarify dates.
Contributors: MA primarily drafted the manuscript, as well as identified and cleaned primary data. HA and BZ developed the statistical models and analysis and contributed to manuscript writing. WT contributed to identification and cleaning of primary data, as well as literature review. BZ, HA, JBS, and GF contributed to manuscript writing. BZ was the senior author and supervised the analysis and all aspects of the manuscript. MA was study guarantor. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. Transparency: The lead author (the guarantor) affirms that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Funding: There was no specific funding given to this study. BZ’s research is supported by American Health Association scientist development grant 17SDG33630113 and the US National Institutes of Health (NIH)/National Center for Advancing Translational Science UCLA CTSI grant KL2TR001882. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Provenance and peer review: Not commissioned; externally peer reviewed.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Data availability statement
Data are available upon reasonable request.
Ethics approval
Not applicable.
References
- 1. Short KR, Kedzierska K, van de Sandt CE. Back to the future: lessons learned from the 1918 influenza pandemic. Front Cell Infect Microbiol 2018;8:343. 10.3389/fcimb.2018.00343 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Henderson DA, Courtney B, Inglesby TV, et al. Public health and medical responses to the 1957-58 influenza pandemic. Biosecur Bioterror 2009;7:265–73. 10.1089/bsp.2009.0729 [DOI] [PubMed] [Google Scholar]
- 3. The White House, Center for Disease Control . The President’s Coronavirus Guidelines for America, 2020. [Google Scholar]
- 4. Centers for Disease Control and Prevention (CDC) . Coronavirus disease: considerations for wearing masks, 2020. [Google Scholar]
- 5. Dong E, Du H, Gardner L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect Dis 2020;20:533–4. 10.1016/S1473-3099(20)30120-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Ahmad FB, Cisewski JA, Miniño A, et al. Provisional mortality data — United States, 2020. MMWR Morb Mortal Wkly Rep 2021;70:519–22. 10.15585/mmwr.mm7014e1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. World Health Organization Writing Group, Bell D, Nicoll A, et al. Non-pharmaceutical interventions for pandemic influenza, National and community measures. Emerg Infect Dis 2006;12:88–94. 10.3201/eid1201.051371 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Germann TC, Kadau K, Longini IM, et al. Mitigation strategies for pandemic influenza in the United States. Proc Natl Acad Sci U S A 2006;103:5935–40. 10.1073/pnas.0601266103 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Aledort JE, Lurie N, Wasserman J, et al. Non-pharmaceutical public health interventions for pandemic influenza: an evaluation of the evidence base. BMC Public Health 2007;7:1–9. 10.1186/1471-2458-7-208 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.et alQualls N, Levitt A, Kanade N. Community Mitigation Guidelines to Prevent Pandemic Influenza-United States, 2017 Centers for Disease Control and Prevention MMWR Editorial and Production Staff (Serials) MMWR Editorial Board [Internet], 2017. Available: http://www.cdc.gov/mmwr/cme/conted.html
- 11. Isfled-Kiely H, Moghadas S. Effectiveness of school closure for the control of influenza, 2014. [Google Scholar]
- 12. World Health Organization . WHO global influenza preparedness plan [Internet], 2005. Available: https://www.who.int/csr/resources/publications/influenza/WHO_CDS_CSR_GIP_2005_5.pdf
- 13. Markel H, Lipman HB, Navarro JA, et al. Nonpharmaceutical interventions implemented by US cities during the 1918-1919 influenza pandemic. JAMA 2007;298:644–54. 10.1001/jama.298.6.644 [DOI] [PubMed] [Google Scholar]
- 14. Markel H, Stern AM, Navarro JA, et al. Nonpharmaceutical influenza mitigation strategies, us communities, 1918-1920 pandemic. Emerg Infect Dis 2006;12:1961–4. 10.3201/eid1212.060506 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Association of State and Territorial Health Officers . Resolutions adopted by association of state and territorial health officers at special meeting on influenza. Washington, D.C, 1957. [Google Scholar]
- 16. Saunders-Hastings PR, Krewski D. Reviewing the history of pandemic influenza: understanding patterns of emergence and transmission. Pathogens 2016;5. doi: 10.3390/pathogens5040066. [Epub ahead of print: 06 12 2016]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Trotter Y, Dunn FL, Drachman RH, et al. Asian influenza in the United States, 1957–19581. Am J Epidemiol 1959;70:34–50. 10.1093/oxfordjournals.aje.a120063 [DOI] [PubMed] [Google Scholar]
- 18. Viboud C, Grais RF, Lafont BAP, et al. Multinational impact of the 1968 Hong Kong influenza pandemic: evidence for a smoldering pandemic. J Infect Dis 2005;192:233–48. 10.1086/431150 [DOI] [PubMed] [Google Scholar]
- 19. Singh S, Shaikh M, Hauck K, et al. Impacts of introducing and lifting nonpharmaceutical interventions on COVID-19 daily growth rate and compliance in the United States. Proc Natl Acad Sci U S A 2021;118:1–9. 10.1073/pnas.2021359118 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Yang B, Huang AT, Garcia-Carreras B, et al. Effect of specific non-pharmaceutical intervention policies on SARS-CoV-2 transmission in the counties of the United States. Nat Commun 2021;12:4–13. 10.1038/s41467-021-23865-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Dahlquist M, Kugelberg HD. Public justification and expert disagreement over non-pharmaceutical interventions for the COVID-19 pandemic. J Med Ethics 2021;10:medethics-2021-107671. 10.1136/medethics-2021-107671 [DOI] [PubMed] [Google Scholar]
- 22. Suh HH, Meehan J, Blaisdell L, et al. Non-pharmaceutical interventions and COVID-19 cases in US summer camps: results from an American cAMP association survey. J Epidemiol Community Health 2022;76:327–34. 10.1136/jech-2021-216711 [DOI] [PubMed] [Google Scholar]
- 23. Chan JF-W, Yuan S, Kok K-H, et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster. Lancet 2020;395:514–23. 10.1016/S0140-6736(20)30154-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Auger KA, Shah SS, Richardson T, et al. Association between statewide school closure and COVID-19 incidence and mortality in the US. JAMA 2020;324:859–70. 10.1001/jama.2020.14348 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Homeland Security Council . National strategy for pandemic influenza implementation plan, 2006: 233. [Google Scholar]
- 26. U.S. Department of Health and Human Services (HHS) . Pandemic Influenza Plan - 2017 Update. Off Assist Secr Prep HHS [Internet, 2017: 1–52. https://www.cdc.gov/flu/pandemic-resources/pdf/pan-flu-report-2017v2.pdf [Google Scholar]
- 27. Mendez-Brito A, El Bcheraoui C, Pozo-Martin F. Systematic review of empirical studies comparing the effectiveness of non-pharmaceutical interventions against COVID-19. J Infect 2021;83:281–93. 10.1016/j.jinf.2021.06.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Brauner JM, Mindermann S, Sharma M, et al. Inferring the effectiveness of government interventions against COVID-19. Science 2021;371. doi: 10.1126/science.abd9338. [Epub ahead of print: 19 02 2021]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Bo Y, Guo C, Lin C, et al. Effectiveness of non-pharmaceutical interventions on COVID-19 transmission in 190 countries from 23 January to 13 April 2020. Int J Infect Dis 2021;102:247–53. 10.1016/j.ijid.2020.10.066 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Islam N, Sharp SJ, Chowell G, et al. Physical distancing interventions and incidence of coronavirus disease 2019: natural experiment in 149 countries. BMJ 2020;370:1–10. 10.1136/bmj.m2743 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. The COVID Tracking Project [Internet]. Atl, 2020. Available: https://covidtracking.com/
- 32. Schneider EC. Failing the Test - The Tragic Data Gap Undermining the U.S. Pandemic Response. N Engl J Med 2020;383:299–302. 10.1056/NEJMp2014836 [DOI] [PubMed] [Google Scholar]
- 33. Galloway SE, Paul P, MacCannell DR, et al. Emergence of SARS-CoV-2 B.1.1.7 Lineage - United States, December 29, 2020-January 12, 2021. MMWR Morb Mortal Wkly Rep 2021;70:95–9. 10.15585/mmwr.mm7003e2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Centers for Disease Control and Prevention . COVID Data Tracker: Variant Proportions [Internet], 2022. Available: https://covid.cdc.gov/covid-data-tracker/#circulatingVariants
- 35. Raifamn J, Nocka K, Jones D, et al. COVID-19 US state policy database [Internet], 2020. Available: www.tinyurl/statepolicies
- 36. Treisman R. Which States Are Reopening? State-By-State Guide [Internet]. NPR, 2020. Available: https://www.npr.org/2020/03/12/815200313/what-governors-are-doing-to-tackle-spreading-coronavirus
- 37. Washington Post Staff . Where states reopened and cases spiked after the U.S. shutdown [Internet]. Washington Post, 2020. Available: https://www.washingtonpost.com/graphics/2020/national/states-reopening-coronavirus-map/
- 38. State Data and Policy Actions to Address Coronavirus [Internet]. KFF, 2020. Available: https://www.kff.org/coronavirus-covid-19/issue-brief/state-data-and-policy-actions-to-address-coronavirus/
- 39. The New York Times . See Coronavirus Restrictions and Mask Mandates for All 50 States [Internet]. New York Times, 2020. Available: https://www.nytimes.com/interactive/2020/us/states-reopen-map-coronavirus.html
- 40. Mervosh S, Lu D, Swales V. See Which States and Cities Have Told Residents to Stay at Home [Internet]. New York Times, 2020. Available: https://www.nytimes.com/interactive/2020/us/coronavirus-stay-at-home-order.html
- 41. Watson GL, Xiong D, Zhang L. Fusing a Bayesian case velocity model with random forest for predicting COVID-19 in the U.S. SSRN electron J 2020.
- 42. Zeileis A, Leisch F, Hornik K, et al. strucchange : An R Package for Testing for Structural Change in Linear Regression Models. J Stat Softw 2002;7:1–38. 10.18637/jss.v007.i02 [DOI] [Google Scholar]
- 43. R Core Team . A language and environment for statistical computing [Internet], 2020. Available: https://www.r-project.org/
- 44. Sommerstein R, Fux CA, Vuichard-Gysin D, et al. Risk of SARS-CoV-2 transmission by aerosols, the rational use of masks, and protection of healthcare workers from COVID-19. Antimicrob Resist Infect Control 2020;9:1–8. 10.1186/s13756-020-00763-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Science Brief: Community Use of Cloth Masks to Control the Spread of SARS-CoV-2 [Internet], 2020. Available: https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/masking-science-sars-cov2.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019-ncov%2Fmore%2Fmasking-science-sars-cov2.html [Accessed 8 Apr 2021]. [PubMed]
- 46. Wiersinga WJ, Rhodes A, Cheng AC, et al. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19). JAMA 2020;324:782–93. 10.1001/jama.2020.12839 [DOI] [PubMed] [Google Scholar]
- 47. Reiner RC, Barber RM, Collins JK. Modeling COVID-19 scenarios for the United States. Nat Med 2020;19. 10.1038/s41591-020-01181-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Bendavid E, Oh C, Bhattacharya J, et al. Assessing mandatory stay‐at‐home and business closure effects on the spread of COVID‐19. Eur J Clin Invest 2021;51. 10.1111/eci.13484 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Holuka C, Merz MP, Fernandes SB, et al. The COVID-19 pandemic: does our early life environment, life trajectory and socioeconomic status determine disease susceptibility and severity? Int J Mol Sci 2020;21:1–21. 10.3390/ijms21145094 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Egede LE, Walker RJ. Structural racism, social risk factors, and Covid-19 — a dangerous convergence for black Americans. N Engl J Med Overseas Ed 2020;383:e77–2. 10.1056/NEJMp2023616 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Price-Haywood EG, Burton J, Fort D, et al. Hospitalization and mortality among black patients and white patients with Covid-19. N Engl J Med 2020;382:2534–43. 10.1056/NEJMsa2011686 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. One Hundred Sixteenth Congress of the United States of America. Coronavirus Aid, Relief, and Economic Security Act [Internet], 2020. Available: http://www.copyright.gov/legislation/s505.pdf
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjmed-2021-000030supp001.pdf (1.1MB, pdf)
Data Availability Statement
Data are available upon reasonable request.