

Abstract
Aim
To assess the rate of self-reported concussion in midwestern skiers and snowboarders.
Patients
Recreational skiers and snowboarders between the ages of 14 and 69 years during a single winter ski season (2020–2021) at a ski area in Wisconsin, USA.
Methods
Survey study.
Results
Among this survey population (n = 161), 9.32 and 19.25% reported one or more diagnosed concussion and suspected concussion respectively as a result of a skiing- or snowboarding-related incident. Skiers and snowboarders that self-identified as advanced, those who utilized terrain park features, and those that participated in freestyle competition had significantly higher self-reported rates of concussion.
Conclusion
Self-reported concussion history indicates a concussion prevalence that is higher than expected based on previous studies. Participants reported significantly more suspected concussions than diagnosed concussions, indicating a possible issue with underreporting in this population.
Keywords: concussions, skiing, snow sports, snowboarding
Downhill skiing and snowboarding have a risk of injury comparable to other sports; however, the injuries sustained in alpine sports are typically more severe and often involve head trauma [1–6]. Previous studies evaluating the epidemiology of concussion in this population have been mainly limited to retrospective chart reviews of local and national trauma banks or emergency medicine records [4,7,8]. One such study, Gil et al. estimated an incidence of 16.9 and 17.4 concussions per 1 ,000 ,000 person-years for skiers and snowboarders, respectively [8]. However, only serious injuries that require medical transport or hospitalization are documented in this retrospective analysis, and this accounts for a small fraction of snow sports injuries. A recent study from Dickson and Terwiel that analyzed ski patrol injury reports from 29 Canadian ski resorts, found that fewer than 20% of those with head injures were transported to emergency department by ambulance or helicopter and only 20.9% of those with concussions were transported [3]. It is reasonable to assume that the previous epidemiological analysis of trauma banks and ER records severely underreport concussions among skiers and snowboarders, as they only include a fraction of those injured.
Furthermore, it is possible that some injuries remain undisclosed to ski patrol and lead to underreporting even in studies that analyze ski patrol injury reports. Falls, crashes and collisions are common among skiers and snowboarders. Incidents that result in significant or visible injury are generally reported to ski patrol and recorded; however, minor falls may not be reported. It is not uncommon to witness a skier or snowboarder fall on the ski slope only to get back up and continue descending downhill. It is conceivable some of these incidents may result in mild head trauma and possible unreported concussions. Therefore, we hypothesized that the prevalence of concussions in this population may be much higher than what has been previously reported.
Concussed individuals who are not evaluated and continue activity or return to activity prematurely have a high risk of severe subsequent injury and sequelae, as continued exposure to trauma, even subconcussive impacts, increases the risk of complications [9–11]. The population of skiers and snowboarders in North America has grown over the previous decades and now is in the tens of millions [12]. Concussions among this population present a serious health concern and require further investigation. According to Finch's Translating Research into Injury Prevention Practice, or TRIPP framework, a problem must first be fully understood before viable interventions can be implemented [13].
The aim of this preliminary study was to further characterize the issue of concussions associated with downhill skiing and snowboarding by assessing the self-reported concussion history of a population of midwestern skiers and snowboarders utilizing a ski area in northern Wisconsin, USA. A previous study utilized a similar survey model to evaluate risk taking and helmet use in the skiing and snowboarding community, demonstrating the utility of surveys in further profiling the alpine snow sports population [14]. This preliminary study in a local population does not purport to fully elucidate the problem of concussions in skiers and snowboarders, rather it demonstrates that self-reported concussion history may be a useful metric to consider when establishing the prevalence, incidence and etiology of concussion in alpine snow sports.
Methods
In order to assess the burden of concussions among skiers and snowboarders in the Midwestern USA, a survey tool was created to directly obtain self-reported concussion history and related information. This study was approved by the Medical College of Wisconsin Institutional Review Board. During the 2020–2021 winter season from December to March, participants were randomly selected for survey assessment across all areas of a Wisconsin ski resort. Researchers approached all skiers and snowboarders they came in contact with regardless of age, gender or other demographics. Participants were contacted in the area parking lot, lift ticket office, chalets, restaurants and on the chair-lifts.
Consenting individuals at least 14 years of age were given a QR code to the secure survey to complete on their own device or a sanitized device to complete the survey. Parental consent was obtained for participants under 18 years of age. 219 individuals took the survey, 173 completed the entire survey. Non-complete surveys were not included in analysis. 11 surveys were discarded due to discrepancies between questions, leaving 161 valid surveys. The survey consisted of 29 questions to determine demographics, experience (e.g., ability level, frequency, run preference), risk taking (e.g., helmet use, terrain and competition), and injury history (e.g., lifetime diagnosed concussions, lifetime suspected concussions) (Table 1). Data were recorded with secure survey software from Qualtrics (Qualtrics, UT, USA).
Table 1. . Survey demographics.
| Demographic category | Number | Percentage |
|---|---|---|
| Age (years): | ||
| 14–17 | 46 | 28.57% |
| 18–23 | 63 | 39.13% |
| 24–29 | 22 | 13.66% |
| 30–35 | 4 | 02.38% |
| 36–39 | 1 | 00.62% |
| 40–45 | 13 | 08.07% |
| 46–49 | 2 | 01.24% |
| 50–59 | 7 | 04.25% |
| 60–69 | 3 | 01.86% |
| Gender: | ||
| Female | 65 | 40.37% |
| Male | 96 | 59.63% |
| Style preference: | ||
| Ski | 112 | 69.56% |
| Snowboard | 41 | 25.47% |
| Both equally | 8 | 04.97% |
| Experience level: | ||
| Beginner | 26 | 16.15% |
| Intermediate | 71 | 44.10% |
| Advanced | 64 | 39.75% |
| Helmet use: | ||
| Yes | 138 | 85.71% |
| No | 23 | 14.29% |
| Terrain park frequency: | ||
| Often | 47 | 29.19% |
| Occasionally | 61 | 37.89% |
| No | 53 | 32.92% |
| Freestyle competition | ||
| Yes | 13 | 08.07% |
| No | 148 | 91.92% |
Concussion rates were quantified by dividing the number of participants in a subgroup that reported one or more concussion and dividing it by the group total. Comparisons between categorical variables (subgroups) were performed using a two-tailed Fisher's Exact Test, completed on GraphPad Prism version 8.0.0 for Windows (GraphPad Software, CA, USA). Fisher's exact test was used because it is optimal for small sample sizes and allows for comparison of more than two categorical variables.
Results
The survey revealed 9.32% of those surveyed, including both snowboarders and skiers across all ages, reported a history of at least one lifetime healthcare provider diagnosed concussion from a skiing- or snowboarding-related incident (Figure 1). Additionally, 19.25% reported they suspected at least one lifetime undiagnosed concussion from a skiing- or snowboarding-related incident (Figure 1). Our survey also evaluated self-reported concussion rates from the last 3 years. This allowed us to calculate a recent average as opposed to relying on a single annual data point. We used this average to estimate a rough annual cross sectional estimate of concussion incidence (2.9%) and identify what age groups may have the higher incidences. Only individuals under age 30 reported any diagnosed concussion in the past 3 years (Figure 2). The rate was 0.10 (14/137) among individuals under 30 years and 0.00 (0/35) in ages above 30 years. A similar trend was observed in undiagnosed suspected concussions.
Figure 1. . Self-reported concussion rates among alpine sports enthusiasts.

15 of 161 surveyed participants (9.32%) reported experiencing at least one lifetime concussion from skiing- or snowboarding-related incidents that was diagnosed by a healthcare provider. 31 of 161 (19.25%) reported a positive history of a suspected concussion as a result of skiing or snowboarding.
Figure 2. . Diagnosed concussion by age group within the last 3 years.
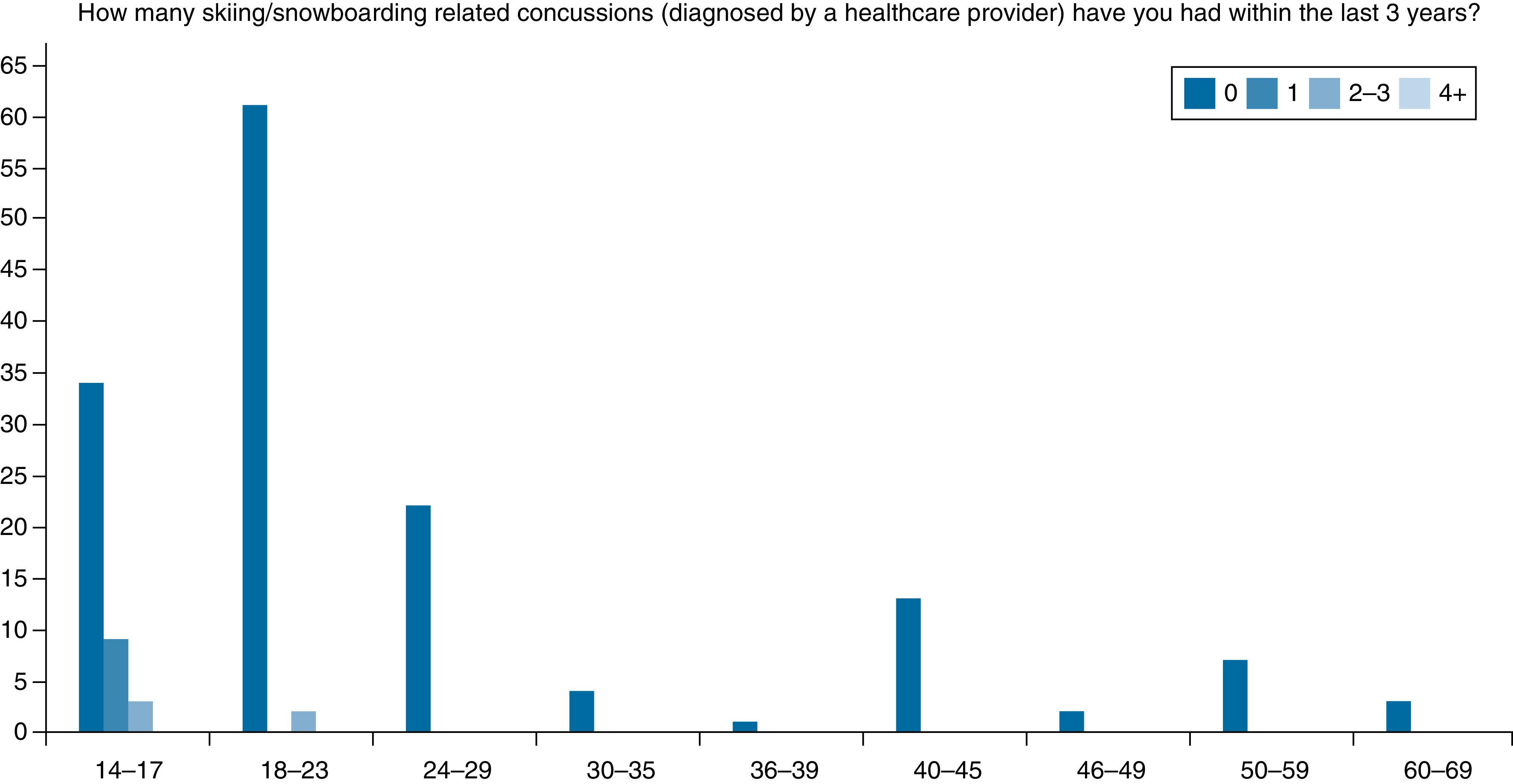
Overall incidence in the past 3 years was 8.7%, which equates to a 2.9% annual average. 12/46 (26.0%) of 14–17-year-olds report a diagnosed concussion as a result of skiing or snowboarding. 2/63 (3.2%) of 18–23-year-olds. No diagnosed concussions were reported in the last 3 years by anyone older than 30 years.
We found that the percentage of self-reported lifetime skiing- or snowboarding-related concussions was not statistically different between skiers and snowboarders, males and females, nor helmet users and non-users (Table 2). Skiers and snowboarders that self-identified as advanced had significantly higher rates of concussion than those who identified as beginner or intermediate. When respondents categorized themselves as “often, occasionally, or never using terrain park features,” there were higher rates of concussion for those who often use terrain features compared with others. Participants in freestyle competitions, such as Big Air, Slopestyle or Rail Jam events also had a significantly higher self-reported rate of diagnosed concussion compared with non-competitors. These findings were similar to undiagnosed and suspected concussion as well (Table 3). We explored other comparisons, but for sake of brevity we excluded these from this report.
Table 2. . Diagnosed skiing- or snowboarding-related concussion rate by category.
| Rate of diagnosed concussion | p-value | |
|---|---|---|
| Gender: | 0.286 | |
| Male | 11.46% | |
| Female | 6.15% | |
| Helmet use: | 0.698 | |
| Helmet | 10.14% | |
| No Helmet | 4.34% | |
| Style preference: | 0.187 | |
| Ski | 10.71% | |
| Snowboard | 2.44% | |
| Experience level: | ||
| Beginner | 3.85% | 0.005 |
| Intermediate | 2.82% | |
| Advanced | 18.75% | |
| Terrain park frequency: | 0.008 | |
| Often | 21.28% | |
| Occasionally | 5.00% | |
| Never | 3.77% | |
| Freestyle competition: | 0.0003 | |
| Yes | 46.15% | |
| No | 6.08% |
Table 3. . Suspected skiing- or snowboarding-related concussion rate by category.
| Rate of suspected concussion | p-value | |
|---|---|---|
| Gender: | 0.416 | |
| Male | 21.88% | |
| Female | 15.38% | |
| Helmet use: | 0.253 | |
| Helmet | 21.01% | |
| No helmet | 8.70 | |
| Style preference: | 0.768 | |
| Ski | 19.64% | |
| Snowboard | 17.07% | |
| Experience level: | 0.003 | |
| Beginner | 3.85% | |
| Intermediate | 14.08% | |
| Advanced | 31.25% | |
| Terrain park frequency: | 0.0013 | |
| Often | 36.17% | |
| Occasionally | 16.67% | |
| Never | 7.55% | |
| Freestyle competition: | 0.0038 | |
| Yes | 53.85% | |
| No | 16.22% |
Discussion
Although this study has its limitations, such as a small study population and geographic constraints, the data supports the hypothesis that previous studies have not elucidated the actual prevalence of head injury and concussion in downhill alpine sports. The percentage of self-reported diagnosed and suspected concussions of 9.32 and 19.25% respectively, far exceeds what would be expected based on previous literature. While we did not directly assess the annual rate in our survey, we found that 8.7% of our survey population reported a history of diagnosed concussion within the last 3 years. Dividing this percentage by three allows us to roughly estimate an annual incidence of 2.9%, which would suggest a nearly 170-fold increase to incidence estimated by Gil et al. [8]. We believe the true incidence may lie somewhere between our estimation and that of retrospective cross-sectional studies or trauma bank reviews. As evidenced by the data Dickson and Terwiel's studies of ski patrol reports, previous studies fail to include milder injuries that do not result in transfer to an emergency medical facility [2,3]. Patients that are seen in outpatient clinic would not be included in these studies, nor would those who do not seek diagnosis or treatment at all.
We recommend using a similar methodology to our study, using a survey tool, to assess self-reported concussions among a larger study population across multiple geographic areas in order to fully elucidate the epidemiology of concussions in North American skiers and snowboarders. While a power analysis indicated that our sample size was adequate for a preliminary report assessing our local population, a larger sample size would be preferred to increase the representativeness of the study. Furthermore, the authors understand that including skier days at the resort studied may allow for better assessment of generalizability of the data; however, we were unable to obtain this information as it was regarded proprietary information by the resort.
Our study also identified risk factors that are associated with higher rates of concussion. Skiers and snowboarders that self-identified as advanced, utilize terrain park features, and participate in freestyle competition appear more likely to suffer from skiing- or snowboarding-related concussion, findings which are consistent with similar studies [14–16]. Our data also mirrored previous findings that pediatric and young adult skiers and snowboarders have significantly higher incidences of concussion than adults, as none of the participants in our study over the age of 30 years reported a diagnosed concussion within the last 3 years [8]. While males in our study population did report more diagnosed and suspected concussions than females, the difference was not significant as other studies have found [4,8]. This is likely due to our smaller study population size when compared with previous studies. Additionally, it appeared that helmeted skiers and snowboarders reported higher percentages of both diagnosed and suspected concussions than non-helmeted peers. However, there were relatively few skiers and snowboarders in the non-helmeted category and this could contribute to the low number.
Furthermore, the large discrepancy between self-reported suspected and self-reported diagnosed concussions in our dataset is concerning. It implies that many skiers and snowboarders are not being evaluated by medical professionals after suspected head injury. This difference between suspected and diagnosed concussions was particularly disparate among snowboarders where 17.07% had a history of a suspected concussion, but only 2.44% reported a diagnosed concussion. There is potential for serious harm if snowboarders continue to ride and risk exposure to subsequent trauma [9–11]. However, data suggests that isolated well-managed concussions, where the brain is allowed to adequately recover, do not increase the risk of long term neurodegenerative disease [10,11]. Therefore, developing interventions to increase concussion symptom reporting and subsequently increase diagnosis and treatment are warranted in this population. Previous initiatives to increase helmet use have demonstrated considerable reduction in head injuries such as skull fractures, scalp lacerations, and other serious head injuries [3,17]. Our group is currently developing a peer education campaign to further encourage helmet use, increase concussion literacy, improve concussion reporting, and advocate for activity restriction following head injury.
Conclusion
This preliminary report suggests that concussions may be more prevalent among midwestern skiers and snowboarders than previously expected. Our study also identifies several risk factors that correlate with increased self-reported concussion and suspected concussion. These include higher perceived skill level, usage of terrain park features, participation in freestyle competition, and age below 30. Furthermore, the percentage of the study population who report one or more suspected concussion is more than double the percentage of those that report diagnosed concussion. This disparity between suspected and diagnosed concussions signals the possibility of a significant number of undiagnosed concussions in this population. A larger study of similar design would likely provide greater understanding of the epidemiology of concussion in downhill alpine snow-sports, and allow for greater statistical analysis to definitively determine risk factors.
Summary points.
Previous studies evaluating the epidemiology of concussion in this population have been mainly limited to retrospective chart reviews of local and national trauma banks or emergency medicine records.
Assessing for self-reported concussion history using a survey provides an alternative route to further characterize the epidemiology.
9.32% of those surveyed, including both snowboarders and skiers, reported a history of at least one lifetime healthcare provider diagnosed concussion from a skiing- or snowboarding-related incident.
19.25% of the survey population reported that they suspected suffering at least one lifetime undiagnosed concussion from a skiing- or snowboarding-related incident.
Using data collected from the survey study, annual concussion incidence was estimated to be 2.9%.
Only individuals under age 30 years reported suffering a diagnosed concussion in the past 3 years.
Skiers and snowboarders that self-identified as advanced appear more likely to suffer from skiing- or snowboarding-related concussion.
Skiers and snowboarders that reported utilizing terrain park features appear more likely to suffer from skiing- or snowboarding-related concussion.
Skiers and snowboarders that reported participation in freestyle competition appear more likely to suffer from skiing- or snowboarding-related concussion.
Acknowledgments
A Tischer (research assistant), C Hagen (research assistant), S Rifleman (other), R Calder (statistician).
Footnotes
Financial & competing interests disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
Ethical conduct of research
This study was approved by the Medical College of Wisconsin Institutional Review Board. The authors state that they have obtained appropriate institutional review board approval or have followed the principles outlined in the Declaration of Helsinki for all human or animal experimental investigations. In addition, for investigations involving human subjects, informed consent has been obtained from the participants involved.
Open access
This work is licensed under the Creative Commons Attribution 4.0 License. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
- 1.Davey A, Endres NK, Johnson RJ, Shealy JE. Alpine skiing injuries. Sports. Health 11(1), 18–26 (2019). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Dickson TJ, Terwiel FA. Injury trends in alpine skiing and a snowboarding over the decade 2008–09 to 2017–18. J. Sci. Med. Sport. 24(10), 1055–1060 (2021). [DOI] [PubMed] [Google Scholar]
- 3.Dickson TJ, Terwiel FA. Head injury and helmet usage trends for alpine skiers and snowboarders in western Canada during the decade 2008–9 to 2017–18. J. Sc.i Med. Sport. 24(10), 1004–1009 (2021). [DOI] [PubMed] [Google Scholar]
- 4.Levy AS, Hawkes AP, Hemminger LM, Knight S. An analysis of head injuries among skiers and snowboarders. J. Trauma 53(4), 695–704 (2002). [DOI] [PubMed] [Google Scholar]; •• Provides an in-depth analysis of ski patrol injury reports from western Canadian ski resorts and demonstrates that most injuries do not result in transport to hospital.
- 5.Owens BD, Nacca C, Harris AP, Feller RJ. Comprehensive review of skiing and snowboarding injuries. J. Am. Acad. Orthop. Surg. 26(1), e1–e10 (2018). [DOI] [PubMed] [Google Scholar]
- 6.Ackery A, Hagel BE, Provvidenza C, Tator CH. An international review of head and spinal cord injuries in alpine skiing and snowboarding. Inj. Prev. 13(6), 368–375 (2007). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bergmann KR, Flood A, Kreykes NS, Kharbanda AB. Concussion Among Youth Skiers and Snowboarders: A Review of the National Trauma Data Bank From 2009 to 2010. Pediatr. Emerg. Care 32(1), 9–13 (2016). [DOI] [PubMed] [Google Scholar]
- 8.Gil JA, DeFroda SF, Kriz P, Owens BD. Epidemiology of Snow Skiing- Versus Snowboarding-Related Concussions Presenting to the Emergency Department in the United States from 2010 to 2014. Clin. J. Sport Med. 27(5), 499–502 (2017). [DOI] [PubMed] [Google Scholar]
- 9.McKee AC, Alosco ML. Assessing Subconcussive Head Impacts in Athletes Playing Contact Sports-The Eyes Have It. JAMA. Ophthalmol. 137(3), 270–271 (2019). [DOI] [PubMed] [Google Scholar]
- 10.Wetjen NM, Pichelmann MA, Atkinson JL. Second impact syndrome: concussion and second injury brain complications. J. Am. Coll. Surg. 211(4), 553–557 (2010). [DOI] [PubMed] [Google Scholar]
- 11.Stein TD, Alvarez VE, McKee AC. Concussion in Chronic Traumatic Encephalopathy. Curr. Pain. Headache. Rep. 19(10), 47 (2015). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Vanat L. International report on snow & mountain tourism. Overview of the key industry figures for ski resorts (2014). www.vanat.ch/international-report-on-snow-mountain-tourism [Google Scholar]
- 13.Finch C. A new framework for research leading to sports injury prevention. J. Sci. Med. Sport. 9(1-2), 3–9 (2006). [DOI] [PubMed] [Google Scholar]
- 14.Willick SE, Wagner G, Ericson D, Josten G, Teramoto M, Davis J. Helmet Use and Risk-Taking Behavior Among Skiers and Snowboarders. Clin. J. Sport Med. 29(4), 329–335 (2019). [DOI] [PubMed] [Google Scholar]
- 15.Audet O, Hagel BE, Nettel-Aguirre A et al. What are the risk factors for injuries and injury prevention strategies for skiers and snowboarders in terrain parks and half-pipes? A systematic review. Br. J. Sports Med. 53(1), 19–24 (2019). [DOI] [PubMed] [Google Scholar]; • Demonstrates the need for studies identifying the risk factors for injuries to skiers and snowboarders. Our study identifies some key risk factors and supports the findings of this article.
- 16.Stenroos A, Handolin L. Head Injuries in Urban Environment Skiing and Snowboarding: A Retrospective Study on Injury Severity and Injury Mechanisms. Scand. J. Surg. 107(2), 166–17 (2018). [DOI] [PubMed] [Google Scholar]
- 17.Shealy J, Johnson R, Ettlinger C, Scher I. Role of helmets in mitigation of head injuries: epidemiologic study of head injuries to skiers. In: Skiing Trauma Safety - 20th Volume. ASTM International; (2015). [Google Scholar]