

Abstract
BACKGROUND
Little is known about the relationship between sleep disruption due to nocturnal bladder emptying and Quality of Life in patients with spinal cord injury
AIM
The aim of this study was to evaluate the possible influence of number of nocturnal bladder emptying, bladder emptying method and nocturnal incontinence on the Quality of Life of patients with spinal cord injury.
DESIGN
The design of this paper is a cross-sectional descriptive study.
SETTING
The setting is in- and outpatient.
POPULATION
Seventy-nine patients aged between 18 and 77 years with SCI in a first rehabilitation period or follow-up.
METHODS
Patients were asked to complete Short Form-36 and Incontinence Quality of Life questionnaires and a medical information form. Independent samples t-tests and ANOVA were used to compare scores between groups.
RESULTS
The response rate was 71 out of 79 (89%; 51 males and 20 females). 16 paraplegic and 4 tetraplegic patients were chronic, 29 paraplegic and 22 tetraplegic patients were in rehabilitation therapy or had finished this treatment recently. The paraplegic group had a significantly better Short Form-36 total score and emotional function score, while the tetraplegic group had a significantly better Incontinence Quality of Life total score and avoidance and limiting behavior score. The paraplegic patients with 0-1 nocturnal bladder emptying had better Short Form-36-derived Quality of Life than those with ≥2 emptying. Quality of Life score was not associated with gender, leg oedema, incontinence, or acute/chronic group. Incontinence Quality of Life score was significantly better for patients with incomplete spinal cord injury. Fully completed questionnaires were returned by 36 patients; at least 1 item was missing for 35 participants.
CONCLUSIONS
General Short Form-36-derived Quality of Life was better for the paraplegic population. Incontinence-related Quality of Life was better in tetraplegic patients, most of whom used suprapubic catheterization. Paraplegic patients had compromised sleep and Quality of Life when the patient had to wake up two or more times at night to empty the bladder by voiding or intermittent catheterization. The high number of incomplete responders indicates the shortcomings of Quality-of-Life questionnaires for wheelchair-bound patients with spinal cord injury.
CLINICAL REHABILITATION IMPACT
The use of suprapubic catheterization should be considered to improve Quality of Life for tetraplegic patients. For paraplegic patients, we must focus urological policy on aiming to reduce the number of nighttime bladder emptying to one or none.
Key words: Spinal cord injuries; Polyuria; Catheterization, Urinary bladder; Catheters
The impact of a spinal cord injury (SCI) on the Quality of Life (QoL) of the patient and his or her caregivers is significant because of the many physical, mental and social disturbances that are encountered in daily life due to the injury. Incontinence and nocturnal awakenings for bladder emptying are common problems in patients with SCI, influencing the night rest of both patients and their partners.1 Nightly intermittent self-catheterization (IC) is necessary because of the well-known problem of neurogenic overactive bladder (NOAB) and the high prevalence of nocturnal polyuria (NP).2 These urological problems, in combination with being wheelchair-bound, can make coping with incontinence and SCI even more difficult.3 Nocturnal polyuria, defined as an excessive production of urine during the individual’s main sleep period,4 is mainly caused by drainage of leg oedema during sleep in SCI patients.5-8 These oedemas are caused by sitting in a wheelchair during the day, becoming pronounced towards the evening and decreasing during the night as a result of the natural drainage system initiated by recumbency.7 The treatment options for NP in SCI are primarily conservative.7, 9 In a healthy adult population, nocturia with two or more voids during the night negatively influences sleep and QoL.10, 11 Sleep disorders have also been reported in patients with SCI.12-15 Although numerous articles describe disruption of sleep patterns, frequent nocturnal awakenings due to incontinence, voiding difficulties, bladder distention and bladder emptying by ISC, there are no studies evaluating the impact of sleep disorders and nocturia on QoL in SCI populations.12-15 Quality of Life, according to the definition of the World Health Organization, is “an individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns. It is an abroad ranging concept affected in a complex way by the person’s physical health, psychological state, personal beliefs, social relationships and their relationship to salient features and their environment.”16 Although life satisfaction for patients with SCI generally improves during the rehabilitation period and in the following years, it remains lower than in the general population. Life satisfaction seems to be related to the completeness of the injury. Contrary to expectations, however, those with a score of D on the American Spinal Injury Association (ASIA) Impairment scale have lower life satisfaction than those with a greater neurological impairment (scoring A-C on the scale).17 It is possible that this is related to secondary health conditions such as pain, fatigue related to walking, frustration and less visible deficits. Participants in other studies are reported to be dissatisfied with their sexual life, which can be related to incontinence and urological problems.17, 18 Older age, living alone and higher education are important factors related to a lower QoL. Having a partner, participating in activities and being vocationally active, on the other hand, increase QoL.17, 19, 20 One of the important limitations in choosing an instrument for the assessment of QoL is the languages in which the questionnaires are available. Some patient reported outcome measures such as the Short Form-36 (SF-36) and Incontinence Quality of Life I-QoL) questionnaire are available in different languages.21, 22 Higher scores on these measures indicate a better QoL or incontinence-related QoL, respectively. The SF-36 is a generic questionnaire that mainly assesses the underlying primary conditions, but can be used to measure the health-related Quality of Life of patients with SCI. However, it does not have the ability to differentiate between QoL before and after an intervention or therapy.3 The I-QoL was validated in a SCI population with neurogenic urinary incontinence by Schurch et al.3 However, neither the SF-36 nor the I-QoL questionnaire are specific for SCI patients or wheelchair-bound patients. These questionnaires therefore include questions which are not applicable for such patients. Not being able to stand up and walk, and being unable to take a few steps, make it difficult to answer some questions (e.g., about climbing stairs or walking more than a mile). The aim of this study was to evaluate the possible influence of the number of nocturnal bladder emptying, bladder emptying method and nocturnal incontinence on the QoL of SCI patients. In particular, sleep disruption caused by the number of nocturnal awakenings for bladder emptying by self-catheterization or spontaneous micturition and incontinence was investigated.
Materials and methods
This study was approved by the Ghent University Hospital review board (EC UZ Gent 2011/649, 4th November 2011, Belgian registration number: B670201112186). The Declaration of Helsinki was followed and written informed consent for study participation was obtained from all subjects. The present paper is a cross-sectional descriptive study.
Study population
SCI patients were included in the study if they were ≥18 years, inpatients or outpatients in a first rehabilitation period following their SCI, or patients who had finished the rehabilitation program and presented themselves for follow-up in the rehabilitation service. There were no limitations concerning age or time since SCI. Patients who were able to write filled in the questionnaires themselves. Patients who were not able to write because of insufficient hand function were helped by a neutral caregiver, who was instructed to read the questions without any comment and without asking questions of the patient in a way that could influence the answers of the participant. Exclusion criteria were not understanding the Dutch version of the questionnaires, not being able to answer the questionnaires because of communication problems, major complications which could influence QoL (e.g., decubitus problems at the time of inclusion) or urological treatment which could influence the perception of medical problems related to nocturnal polyuria (e.g., incontinent stoma).
Questionnaires
The Rand SF-36 Questionnaire is a self-reported generic questionnaire. The 35 items are grouped in 8 dimensions: physical function (10 items), role physical (4 items), bodily pain (2 items), general health (5 items), vitality (4 items), social function (2 items), emotional status (3 items) and mental health (5 items). The scores on each dimension range from 0 to 100, after recalibration for 10 reversed scores, where 0 corresponds to the worst health status and 100 to the best health status. The 36th item asks subjects about the change in their health status over the past year. The 8 dimensions can be combined to give a Physical Component Score and a Mental Component Score, and the total score for the 8 dimensions is also calculated.22-25 The I-QoL is a self-reported, condition-specific questionnaire for individuals with stress incontinence problems and overactive bladder. The I-QoL contains 22 negatively framed items, each with a five-point response scale (1 = extremely, 2 = quite a bit, 3 = moderately, 4 = a little, 5 = not at all). Besides the total score, three domain scores are calculated for avoidance and limiting behaviors (domain A; 8 items), psychosocial impact (domain B; 9 items) and social embarrassment (domain C: 5 items). The scores are transformed onto a 0-100 scale and a better Quality of Life is associated with a higher score.26, 27
Collection of the data
The participants were asked to participate in a QoL assessment by completing the SF-36 and I-QoL questionnaires and completing an information document with general health questions relevant to the topic of nocturnal polyuria. Between 2012 and 2016, 79 patients participated. Personal information on age, gender, date of SCI, level of SCI and American Spinal Injury Association (ASIA) Impairment Scale (AIS) type, bladder emptying method and number of nocturnal bladder emptying was noted (Table I). At least 1 item was missing on 35 questionnaires (49%; both scales), 36 patients returned the questionnaires fully completed. Patients were considered chronic if they were paraplegic, more than one-year postinjury and living at home, or if they were tetraplegic, more than 2 years postinjury and living at home at the time of informed consent.
Table I. —Characteristics of participants.
| Paraplegic (N.) | Tetraplegic (N.) | Total | |
|---|---|---|---|
| AIS group | |||
| A | 26 | 12 | 38 |
| B | 8 | 5 | 13 |
| C | 11 | 4 | 15 |
| D | 0 | 5 | 5 |
| Nocturnal bladder emptyings | |||
| 0 | 17 | 24 | 41 |
| 1 | 13 | 2 | 15 |
| ≥2 | 15 | 0 | 15 |
| Micturition mode for 41 patients without nocturnal bladder emptying | |||
| Suprapubic catheter | 3 | 20 | 23 |
| Intermittent catheterization | 11 | 2 | 13 |
| Spontaneous micturition | 3 | 2 | 5 |
Statistical analysis
Scores were described by their mean and standard deviation (SD). Categorical patient characteristics were described by their frequencies and percentages by patient group (paraplegic vs. tetraplegic). Age was described by mean and SD. Independent samples t-test and ANOVA were used to compare scores between groups. If Levene’s Test was significant, Welch’s t-test and ANOVA were applied. SPSS software (SPSS Inc., Chicago, IL, USA) was used as recommended in the RAND SF- 36 manual.
Results
Study sample characteristics
Between 2012 and 2016, 79 patients participated. The response rate was 71/79 (89%), with 51 males and 20 females aged between 18 and 77 years at the time of informed consent (IC) (Figure 1). At informed consent, 16 paraplegic patients and 4 tetraplegic patients were chronic, 29 paraplegic patients and 22 tetraplegic patients were in rehabilitation therapy or had finished this treatment recently.
Figure 1.
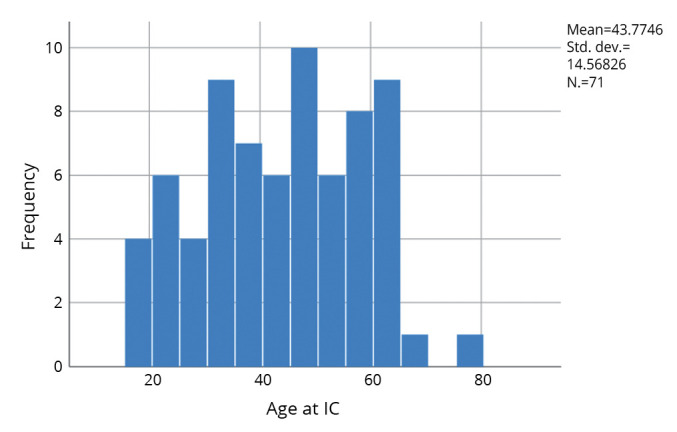
—Age at informed consent.
Quality of Life measurements
Table II describes the results of SF-36 and I-QoL for the total population (N.=71 patients), as well as the paraplegic and the tetraplegic patients separately. The paraplegic group had a significantly better score for SF-36 total score (P=0.032) and emotional function (P=0.019), while the tetraplegic group had a significantly better score in avoidance and limiting behavior (P=0.015) and total score for I-QoL (P=0.025). Overall, QoL was not significantly associated with the number of nocturnal awakenings in the group of 71 patients. There was a tendency toward better SF-36-determined QoL for the patients with one nocturnal awakening for bladder emptying compared with those with 0 or ≥ 2 awakenings. When the number of nocturnal awakenings were grouped as “0 and 1” versus “2 or more” nocturnal awakenings for bladder emptying in the paraplegic population, the SF-36 showed a significantly better QoL for the total and physical scores in the group with fewer awakenings. The same pattern was seen with I-QoL Scores, although this was not significant (Table III). Quality of Life Scores in relation to gender, leg edema and incontinence were not significantly different. There were no significant differences between the acute and chronic group of SCI patients. The I-QoL Score for social embarrassment was significantly better for the incomplete SCI patients (P=0.014; Table IV, Figure 2), and when the complete SCI patients (AIS A) were compared with the incomplete SCI patients (AIS BCD), the significance was much stronger, with a better QoL found in patients with incomplete lesions (P=0.002; Table IV). Those with incomplete lesions also had significantly better scores for total I-QoL (P=0.008) and avoidance and limiting behaviors (P=0.006) in this comparison (Table IV).
Table II. —SF-36 and I-QoL for the population of patients overall, and split by paraplegia and tetraplegia status.
| Overall | Paraplegic | Tetraplegic | P for paraplegic vs. tetraplegic | |
|---|---|---|---|---|
| N. | 71 | 45 | 26 | |
| SF-36 total, mean (SD) | 46 (17.38) | 49 (17.6) | 10 (15.7) | 0.032* |
| SF-36 physical function, mean (SD) | 35 (16.44) | 38 (17.0) | 32 (15.1) | 0.165 |
| SF-36 emotional function, mean (SD) | 57 (22.55) | 62 (22.8) | 49 (19.9) | 0.019* |
| I-QoL total | 72 (20) | 68 (21.5) | 78 (14.3) | 0.025* |
| I-QoL A | 75 (20) | 71 (20.9) | 83 (16.0) | 0.015* |
| I-QoL B | 71 (23) | 69 (25.5) | 76 (18.4) | 0.218 |
| I-QoL C | 72 (25) | 62 (25.1) | 74 (23.4) | 0.065 |
*P<0.05.
Table III. —SF 36 and I-QoL in relation to the number of nocturnal awakenings for the population of 71 patients and for the population of 45 patients with paraplegia.
| Nocturnal awakenings, total number = 71 patients | SF36 physical | SF36 emotional | SF36 total | I-QoL total | I-QoL A | I-QoL B | I-QoL C |
|---|---|---|---|---|---|---|---|
| 0 (N.=41) | 36 | 54 | 45 | 74 | 79 | 73 | 70 |
| 1 (N.=15) | 39 | 65 | 52 | 74 | 74 | 77 | 67 |
| ≥2 (N.=15) | 29 | 57 | 42 | 63 | 67 | 63 | 58 |
| P | 0.173 | 0.269 | 0.218 | 0.303 | 0.262 | 0.354 | 0.355 |
| Nocturnal awakenings 45 paraplegic patients | ANOVA | ANOVA WELCH | |||||
|---|---|---|---|---|---|---|---|
| 0-1 (N.=30) | 42 | 64 | 53 | 71 | 73 | 72 | 65 |
| ≥2 (N.=15) | 29 | 57 | 42 | 63 | 67 | 63 | 57 |
| P | 0.013* | 0.364 | 0.039* | 0.243 | 0.409 | 0.257 | 0.372 |
*P<0.05.
Table IV. —Quality of Life in relation to the completeness of the SCI according to AIS classification and complete versus incomplete SCI patients.
| AIS Scale | SF36 physical | SF36 emotional | SF36 total | I-QoL total | I-QoL A | I-QoL B | I-QoL C |
|---|---|---|---|---|---|---|---|
| A | 33 | 57 | 45 | 66 | 70 | 68 | 58 |
| B | 43 | 60 | 51 | 77 | 83 | 75 | 71 |
| C | 37 | 59 | 48 | 79 | 81 | 78 | 78 |
| D | 28 | 43 | 35 | 79 | 83 | 73 | 82 |
| P value | 0.22 | 0.545 | 0.331 | 0.078 | 0.092 | 0.451 | 0.014* |
| AIS in/complete | SF36 physical | SF36 Emotional | SF36 Total | I-QoL total | I-QoL A | I-QoL B | I-QoL C |
|---|---|---|---|---|---|---|---|
| A | 33 | 57 | 45 | 66 | 70 | 68 | 58 |
| BCD | 38 | 57 | 47 | 78 | 82 | 76 | 76 |
| P | 0.216 | 0.959 | 0.496 | 0.008** | 0.006** | 0.136 | 0.002** |
*P<0.05, **P<0.01.
Figure 2.
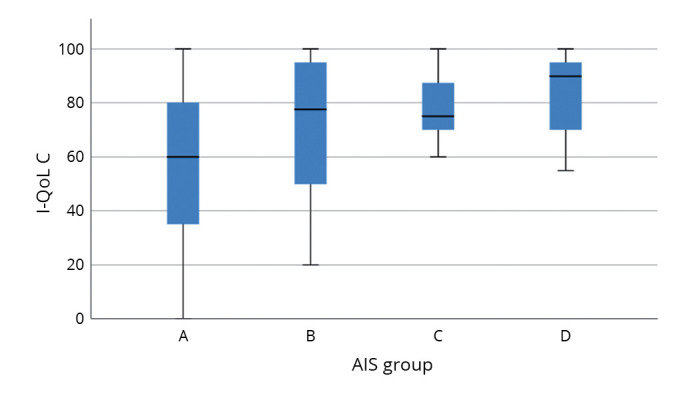
—I-QoL social embarrassment domain C for complete and incomplete SCI patients.
Questionnaires
At least one item response was missing in the questionnaires of 35 participants; frequently, they remarked that a question was “not relevant.” Fully completed questionnaires were returned by 36 patients. In the I-QoL, 15/22 questions (question 5–9, 11 and 13–21) had ≤3 missing answers. Question 1, 2, 10 and 12 had 4 missing answers, question 4 (I worry about where toilets are in new places) had 5 missing answers, question 22 (I worry about having sex because of my incontinence) had 8 missing answers and question 3 (I have to be careful standing up after I have been sitting down because of my incontinence) had 10 missing answers. In the SF-36, questions 1, 2, 6, 7 and 9A had no missing answers, question 3A-C, 3J, 4A-D,5A-C, 8, 9A-I, 10, 11A-D had ≤3 missing answers. Question 4A-D (role limitations due to physical health) and 5A–C (role limitations due to emotional problems) were missing for 2 participants (a female D4 AIS B and a male C5 AIS B, both with a suprapubic catheter). Questions 3A.J were the questions in the dimension “physical functioning;” 5 participants missed between 3 and 9 of these questions (Table V).
Table V. —Patients with 3-9 missing answers for the SF-36 physical functioning dimension.
| Male/female | Level | AIS | Number of bladder emptyings | Continent | Missing | |
|---|---|---|---|---|---|---|
| Day | Night | |||||
| F | D5 | A | 5 | 0 | Yes | D–I |
| F | D3 | A | 6 | 3 | No | DEGHI |
| M | C5 | C | 5 | 0 | Yes | DHI |
| M | D9 | A | 5 | 1 | No | D–I |
| M | D9 | A | 5 | 0 | No | A–I |
Discussion
Quality of Life
This study investigated the QoL of patients with a SCI by means of questionnaires. In SCI, QoL is dependent on the impact of the injury on physical, mental, social and financial disturbances.28, 29 Activity limitations are more important than the level of injury itself,30 although the level of injury is in many ways the determining factor for the functional level a patient can reach in daily life. When analyzing the tetraplegic group separately from the paraplegic group, it became clear that the tetraplegic group had a lower, general, SF-36-derived QoL. According to Parimbelli et al., Jörgensen et al., Adriaansen, et al., and Silviera et al., life satisfaction does not seem to be associated with the level of spinal cord injury,17, 20, 31, 32 which seems to be contradictory to the conclusion that participating in activities and being vocationally active, which is more evident for paraplegic patients than for tetraplegic patient, increases QoL.17, 19, 20 In the current study, only 20 patients in the study were living at home; 51 were still in rehabilitation or had just finished the program. During this period, the level of participation and being vocationally active is generally minimal. We found that SF-36 scores, representing general QoL, were higher in the paraplegic group; however, I-QoL Scores, representing incontinence-related QoL, were higher in the tetraplegic group. Our data demonstrate that SF-36 and I-QoL were not significantly associated with the number of nocturnal bladder emptyings in the entire study population. In the tetraplegic group, most of the patients had a suprapubic catheter or SPC, which likely influences the I-QoL of these patients. Indeed, 24 of 26 tetraplegics had no nocturnal bladder emptyings, and 20 of these 24 used SPC. In line with our findings, a study by Böthig et al. found a better Quality of Life and less urological complications in artificial ventilated tetraplegic patients and recommended the use of SPC in patients unable to perform IC themselves.33 In these patients, the burden of care increases. As a result, most of our tetraplegic patients prefer a SPC, especially when hand function is insufficient. One of the advantages of a SPC is that it helps to avoid sleep disturbances, because patients use a recipient bag connected with open flow to the SPC during the night. In the study population of Adriaansen et al., patients with tetraplegia were more likely to use a SPC, while paraplegic patients were more likely to use clean intermittent catheterization (CIC).34 Paraplegic patients who must wake up at least twice have a significantly lower SF-36-derived general QoL and a tendency towards lower I-QoL Score, compared with those who do not have to wake up or wake up only once during the night to empty the bladder. In this regard, it appears that the paraplegic population is similar to the normal population and their experience of the burden of nocturia, as defined by the International Continence Society.4, 11 That is, sleep and QoL are significantly affected when people have to wake up two or more times at night to empty the bladder, either by voiding10, 11 or by intermittent catheterization. This highlights the importance of reducing nocturnal polyuria and nocturia in paraplegic patients, where possible, to try to improve sleep and QoL. Life satisfaction is generally thought to be lower for patients with incomplete vs. complete SCI, possibly due to secondary health conditions such as pain, dissatisfaction with their sex life and urological problems, as well as less visible deficits that have an impact on daily living.17, 18 This is in contrast with our study population, however, where a significantly higher incontinence-related QoL was seen in the group with incomplete lesions, and SF-36 QoL was similar for both groups (except for the AIS D group specifically, whose SF-36 QoL scores tended to be lower). The complete AIS A group represented the majority of participants (38 patients, vs. 13 AIS B, 15 AIS C and 5 AIS D). The studied population is too small, therefore, to draw conclusions as to why the group with incomplete SCI had a better QoL for all items of the I-QoL. On the SF-36, results from the AIS D group were consistent with what we know in general, namely that they tend to have the poorest Quality of Life of the SCI groups.17, 18 Quality of Life is not influenced by age, or the number of years patients have lived with the SCI.17 In this study, there were only 20 patients in the chronic group, which means that the majority had lived with the SCI for less than 2 years for the tetraplegic group and less than 1 year for the paraplegic group. Furthermore, the imbalance between chronic and acute patients in our study population makes it difficult to detect why the general pattern of improvements in life satisfaction in the years following the rehabilitation period was not seen.
Questionnaires
Most of the study population was wheelchair bound (51 patients), while 15 were wheelchair dependent (able to stand or walk for transfers) and 5 were able to walk. Neither the SF-36 nor I-QoL questionnaires are specific for wheelchair patients, despite the validation of the I-QoL in a SCI population with neurogenic urinary incontinence.3 As a result, the major drawback of both questionnaires is that some questions cause the respondent to hesitate or be unable to answer and to complete the questionnaire. This is particularly true for those questions relating to the ability to stand up and walk. Half of the questionnaires were returned with at least 1 item missing, and 8 patients returned the questionnaires with only a few or no answers completed. Ten patients did not answer the question “I have to be careful standing up after I have been sitting down because of my incontinence” (I-QoL), because they found it “not relevant.” In the third series of questions in SF-36, the items about climbing stairs, bending, kneeling or stooping and walking one block, several blocks or a mile were frequently unanswered (up to 6 times), or marked as “not relevant.” This implies the urgent need for questionnaires on QoL, in different languages, which are adapted for use by wheelchair users. Besides the difficulties of asking patients to answer inappropriate questions which could be seen as not “patient friendly,” or could even cause offence, there is also a practical difficulty in how best to handle the missing data from a statistical point of view. Finkelstein opted for the method of multiple imputation to handle the missing answers, considering the possible bias, because excluding the questionnaires with the missing data completely would create a bias and lead to reduction of sample size.35
Conclusions
Quality of Life in this population of SCI patients is not influenced by age, or the period of time living with the SCI. General QoL (SF-36) is better for the paraplegic population, while incontinence-related QoL is better for tetraplegic patients. The latter is likely to be reflective of the fact that many tetraplegic patients are not able to perform self-catheterization, and therefore use SPC. This, in turn, may lead to fewer concerns relating to incontinence, as well as to improved sleep as a result of avoiding the need to wake for nocturnal bladder emptying. Paraplegic patients, on the other hand, are more likely to have compromised sleep and reduced general QoL when the patient has to wake up two or more times at night to empty the bladder (either by voiding or intermittent catheterization). In this regard, the paraplegic population is similar to the normal non-SCI population with nocturia. The high number of incomplete responders is indicative of the shortcomings of the QoL questionnaires that are currently available for the wheelchair-bound SCI patient population.
References
- 1.Everaert K, Anderson P, Wood R, Andersson FL, Holm-Larsen T. Nocturia is more bothersome than daytime LUTS: Results from an Observational, Real-life Practice Database including 8659 European and American LUTS patients. Int J Clin Pract 2018;72:e13091. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=29767479&dopt=Abstract 10.1111/ijcp.13091 [DOI] [PubMed] [Google Scholar]
- 2.Viaene A, Denys MA, Goessaert AS, Claeys J, Raes A, Roggeman S, et al. Evaluation of the occurrence and diagnose definitions for nocturnal polyuria in spinal cord injured patients during rehabilitation. Eur J Phys Rehabil Med 2019;55:40–6. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=29099160&dopt=Abstract 10.23736/S1973-9087.17.04851-1 [DOI] [PubMed] [Google Scholar]
- 3.Schurch B, Denys P, Kozma CM, Reese PR, Slaton T, Barron R. Reliability and validity of the Incontinence Quality of Life questionnaire in patients with neurogenic urinary incontinence. Arch Phys Med Rehabil 2007;88:646–52. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=17466735&dopt=Abstract 10.1016/j.apmr.2007.02.009 [DOI] [PubMed] [Google Scholar]
- 4.Hashim H, Blanker M, Drake M, Djurhuus JC, Meijlink J, Morris V, et al. The International Continence Society Standardisation of Terminology in Nocturia; 2018 [Internet]. Available from: https://www.ics.org/Documents/DocumentsDownload.aspx?DocumentID=3571 [cited 2018 Jun 29].
- 5.Barkin J. Nocturia: diagnosis and management for the primary care physicians. Can J Urol 2016;23:16–9. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=26924591&dopt=Abstract [PubMed] [Google Scholar]
- 6.Soda T, Masui K, Okuno H, Terai A, Ogawa O, Yoshimura K. Efficacy of nondrug lifestyle measures for the treatment of nocturia. J Urol 2010;184:1000–4. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=20643422&dopt=Abstract 10.1016/j.juro.2010.05.038 [DOI] [PubMed] [Google Scholar]
- 7.Viaene A, Roggeman S, Goessaert AS, Kessler TM, Mehnert U, Besien VV, et al. Conservative treatment for leg oedema and the effect on nocturnal polyuria in patients with spinal cord injury. BJU Int 2019;123:E43–50. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=30653810&dopt=Abstract 10.1111/bju.14672 [DOI] [PubMed] [Google Scholar]
- 8.Wein AJ. Re: The New England Research Institutes, Inc. (NERI) Nocturia Advisory Conference 2012: focus on outcomes of therapy. J Urol 2014;191:1053–4. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=24703130&dopt=Abstract 10.1016/j.juro.2014.01.082 [DOI] [PubMed] [Google Scholar]
- 9.Szollar S, North J, Chung J. Antidiuretic hormone levels and polyuria in spinal cord injury. A preliminary report. Paraplegia 1995;33:94–7. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7753575&dopt=Abstract [DOI] [PubMed] [Google Scholar]
- 10.Asplund R. The nocturnal polyuria syndrome (NPS). Gen Pharmacol 1995;26:1203–9. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=7590108&dopt=Abstract 10.1016/0306-3623(94)00310-J [DOI] [PubMed] [Google Scholar]
- 11.van Kerrebroeck P, Abrams P, Chaikin D, Donovan J, Fonda D, Jackson S, et al. Standardisation Sub-committee of the International Continence Society . The standardisation of terminology in nocturia: report from the Standardisation Sub-committee of the International Continence Society. Neurourol Urodyn 2002;21:179–83. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=11857672&dopt=Abstract 10.1002/nau.10053 [DOI] [PubMed] [Google Scholar]
- 12.Biering-Sørensen F, Biering-Sørensen M. Sleep disturbances in the spinal cord injured: an epidemiological questionnaire investigation, including a normal population. Spinal Cord 2001;39:505–13. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=11641793&dopt=Abstract 10.1038/sj.sc.3101197 [DOI] [PubMed] [Google Scholar]
- 13.Fogelberg DJ, Hughes AJ, Vitiello MV, Hoffman JM, Amtmann D. Comparison of Sleep Problems in Individuals with Spinal Cord Injury and Multiple Sclerosis. J Clin Sleep Med 2016;12:695–701. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=26857058&dopt=Abstract 10.5664/jcsm.5798 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Giannoccaro MP, Moghadam KK, Pizza F, Boriani S, Maraldi NM, Avoni P, et al. Sleep disorders in patients with spinal cord injury. Sleep Med Rev 2013;17:399–409. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=23618534&dopt=Abstract 10.1016/j.smrv.2012.12.005 [DOI] [PubMed] [Google Scholar]
- 15.Haddad R, Denys P, Arlandis S, Giannantoni A, Del Popolo G, Panicker JN, et al. Nocturia and Nocturnal Polyuria in Neurological Patients: From Epidemiology to Treatment. A Systematic Review of the Literature. Eur Urol Focus 2020;6:922–34. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=32192920&dopt=Abstract 10.1016/j.euf.2020.02.007 [DOI] [PubMed] [Google Scholar]
- 16.The World Health Organization Quality of Life assessment (WHOQOL): position paper from the World Health Organization. Soc Sci Med 1995;41:1403–9. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8560308&dopt=Abstract 10.1016/0277-9536(95)00112-K [DOI] [PubMed] [Google Scholar]
- 17.Jörgensen S, Hedgren L, Sundelin A, Lexell J. Global and domain-specific life satisfaction among older adults with long-term spinal cord injury. J Spinal Cord Med 2021;44:322–30. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=31099721&dopt=Abstract 10.1080/10790268.2019.1610618 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Post MW, van Leeuwen CM. Psychosocial issues in spinal cord injury: a review. Spinal Cord 2012;50:382–9. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=22270190&dopt=Abstract 10.1038/sc.2011.182 [DOI] [PubMed] [Google Scholar]
- 19.Brillhart B. Studying the quality of life and life satisfaction among persons with spinal cord injury undergoing urinary management. Rehabil Nurs 2004;29:122–6. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=15222093&dopt=Abstract 10.1002/j.2048-7940.2004.tb00328.x [DOI] [PubMed] [Google Scholar]
- 20.Parimbelli E, Pistarini C, Fizzotti G, Rognoni C, Olivieri G, Quaglini S. Computer-Assessed Preference-Based Quality of Life in Patients with Spinal Cord Injury. BioMed Res Int 2017;2017:4543610. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=28948166&dopt=Abstract 10.1155/2017/4543610 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Bushnell DM, Martin ML, Summers KH, Svihra J, Lionis C, Patrick DL. Quality of life of women with urinary incontinence: cross-cultural performance of 15 language versions of the I-QOL. Qual Life Res 2005;14:1901–13. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=16155777&dopt=Abstract 10.1007/s11136-005-5266-5 [DOI] [PubMed] [Google Scholar]
- 22.Ware JE. SF-36 Health Survey: Manual and Interpretation Guide. Boston, MA: Health Institute, New England Medical Center; 1993. p.344. [Google Scholar]
- 23.Van der Zee KI, Sanderman R. Measuring General Health with the RAND-36. Groningen: Noordelijk centrum voor gezondheidsvraagstukken; 1993. p.1–23. [Dutch]. [Google Scholar]
- 24.VanderZee KI, Sanderman R, Heyink JW, de Haes H. Psychometric qualities of the RAND 36-Item Health Survey 1.0: a multidimensional measure of general health status. Int J Behav Med 1996;3:104–22. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=16250758&dopt=Abstract 10.1207/s15327558ijbm0302_2 [DOI] [PubMed] [Google Scholar]
- 25.Stewart AL, Hays RD, Ware JE, Jr. The MOS short-form general health survey. Reliability and validity in a patient population. Med Care 1988;26:724–35. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=3393032&dopt=Abstract 10.1097/00005650-198807000-00007 [DOI] [PubMed] [Google Scholar]
- 26.Wagner TH, Patrick DL, Bavendam TG, Martin ML, Buesching DP. Quality of life of persons with urinary incontinence: development of a new measure. Urology 1996;47:67–71, discussion 71–2. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=8560665&dopt=Abstract 10.1016/S0090-4295(99)80384-7 [DOI] [PubMed] [Google Scholar]
- 27.Patrick DL, Martin ML, Bushnell DM, Yalcin I, Wagner TH, Buesching DP. Quality of life of women with urinary incontinence: further development of the incontinence quality of life instrument (I-QOL). Urology 1999;53:71–6. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=9886591&dopt=Abstract 10.1016/S0090-4295(98)00454-3 [DOI] [PubMed] [Google Scholar]
- 28.Blanes L, Carmagnani MI, Ferreira LM. Health-related quality of life of primary caregivers of persons with paraplegia. Spinal Cord 2007;45:399–403. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=17310256&dopt=Abstract 10.1038/sj.sc.3102038 [DOI] [PubMed] [Google Scholar]
- 29.Lynch J, Cahalan R. The impact of spinal cord injury on the quality of life of primary family caregivers: a literature review. Spinal Cord 2017;55:964–78. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=28653672&dopt=Abstract 10.1038/sc.2017.56 [DOI] [PubMed] [Google Scholar]
- 30.Jörgensen S, Iwarsson S, Lexell J. Secondary Health Conditions, Activity Limitations, and Life Satisfaction in Older Adults With Long-Term Spinal Cord Injury. PM R 2017;9:356–66. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=27647215&dopt=Abstract 10.1016/j.pmrj.2016.09.004 [DOI] [PubMed] [Google Scholar]
- 31.Adriaansen JJ, Ruijs LE, van Koppenhagen CF, van Asbeck FW, Snoek GJ, van Kuppevelt D, et al. Secondary health conditions and quality of life in persons living with spinal cord injury for at least ten years. J Rehabil Med 2016;48:853–60. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=27834436&dopt=Abstract 10.2340/16501977-2166 [DOI] [PubMed] [Google Scholar]
- 32.Silveira SL, Ledoux TA, Johnston CA, Kalpakjian C, O’Connor DP, Cottingham M, et al. Well on wheels intervention: satisfaction with life and health for adults with spinal cord injuries. J Spinal Cord Med 2020;43:60–8. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=30557093&dopt=Abstract 10.1080/10790268.2018.1554333 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Böthig R, Hirschfeld S, Thietje R. Quality of life and urological morbidity in tetraplegics with artificial ventilation managed with suprapubic or intermittent catheterisation. Spinal Cord 2012;50:247–51. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=21876550&dopt=Abstract 10.1038/sc.2011.94 [DOI] [PubMed] [Google Scholar]
- 34.Adriaansen JJ, van Asbeck FW, Tepper M, Faber WX, Visser-Meily JM, de Kort LM, et al. Bladder-emptying methods, neurogenic lower urinary tract dysfunction and impact on quality of life in people with long-term spinal cord injury. J Spinal Cord Med 2017;40:43–53. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=26446581&dopt=Abstract 10.1179/2045772315Y.0000000056 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Finkelstein MM, Skelly J, Kaczorowski J, Swanson G. Incontinence Quality of Life Instrument in a survey of primary care physicians. J Fam Pract 2002;51:952. https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=12485550&dopt=Abstract [PubMed] [Google Scholar]