

Abstract
Introduction:
Although magnetic resonance imaging (MRI) is the preferred imaging modality for diagnosing cauda equina syndrome (CES), computerized tomography (CT) myelogram may be used in patients who are unable to undergo MRI. When inserting the needle for CT myelogram, there is a risk of cerebrospinal fluid (CSF) leak, which theoretically could lead to CES. To the best of our knowledge, there are no reports of CT myelogram resulting in cauda equina compression.
Case Report:
We report the case of a 38-year-old man who underwent surgical decompression for CES and developed an iatrogenic CSF leak from a pre-operative CT myelogram causing recurrent thecal sac compression requiring repeat surgery and dural repair.
Conclusion:
Although CT myelogram may be used to aid in the diagnosis of CES, consideration should be given to the potential risk for causing a CSF leak and resultant thecal sac compression.
Keywords: Spine, cauda equina, cauda equina syndrome, computerized tomography myelogram, magnetic resonance imaging, lumbar puncture, cerebrospinal fluid leak, dura, puncture, complications, saddle anesthesia
Learning Point of the Article:
Although computerized tomography myelogram may be used to aid in the diagnosis of Cauda Equina Syndrome, consideration should be given to the potential risk for causing a cerebrospinal fluid leak and resultant thecal sac compression.
Introduction
Cauda equina syndrome (CES) can result in severe neurological deficits if misdiagnosed or left untreated [1]. Magnetic resonance imaging (MRI) is the preferred imaging modality for diagnosing CES, but computerized tomography (CT) myelogram may be used in patients who are unable to undergo MRI due to large body habitus or incompatible devices [1, 2, 3, 4].
CES is most commonly caused by an acute disc herniation, however, iatrogenic cerebrospinal fluid (CSF) leak has also been a reported cause [3]. There is a risk of a CSF leak with CT myelogram, which theoretically could accumulate and compress the thecal sac. However, to the best of our knowledge, there are no reports of CT myelography resulting in cauda equina compression. We present a case of a patient who underwent surgical decompression for CES secondary to epidural lipomatosis and later developed residual thecal sac compression due to complications from a pre-operative CT myelogram.
The patient was informed that data concerning the case would be submitted for publication, and he provided consent.
Case Presentation
A 38-year-old obese (body mass index 40.3) man was presented to the emergency department (ED) with atraumatic progressive bilateral lower extremity weakness and numbness resulting in the inability to ambulate. Physical examination was notable for the loss of motor and sensation from L3-S1, weak rectal tone, and saddle anesthesia. A CT of the lumbar spine without contrast was initially obtained and revealed facet arthropathy and hypertrophy with a mild disk bulge at L4-L5 (Fig. 1).
Figure 1.
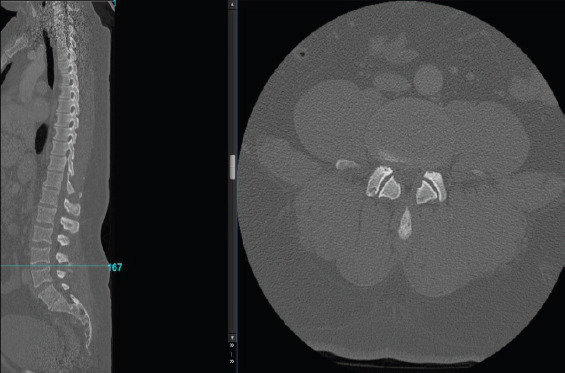
Initial pre-operative computed tomography of lumbar spine revealing facet arthropathy and hypertrophy with a mild disk bulge at L4-L5.
MRI was unable to be obtained due to the patient’s large body habitus. Four hours after arrival, a CT myelogram was then attempted with a 20 gauge (G) needle resulting in intermittent CSF return, but myelogram was not performed due to lack of free flow of CSF (Fig. 2).
Figure 2.
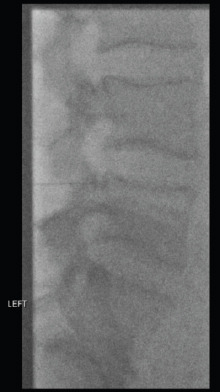
Aborted computed tomography myelogram.
Despite lack of radiologic confirmation in the setting of high clinical suspicion for CES, the patient underwent an emergent L2-S1 laminectomy 6 h after arrival to the ED. Significant epidural lipomatosis and ligamentum flavum hypertrophy were identified as the compressive source. Two small punctures in the dura were noted to be minimally draining CSF at the level of L4-5 and were addressed with DuraSeal® (Integra Life Sciences). No further drainage was seen and the integrity of the dura was confirmed with the Valsalva maneuver. The patient tolerated the procedure well and was made head of bed flat for 24 h.
On post-operative day 2, the patient failed to demonstrate improvement in sensory or motor function. His surgical dressing was noted to be saturated with clear serous fluid. Notably, the patient denied headaches and other traditional symptoms related to a CSF leak. He was transferred to an outpatient imaging center for an open MRI which demonstrated a large homogeneous fluid collection measuring 9.7 × 4.1 × 3.6 cm causing significant thecal sac and cauda equina compression (Fig. 3). The patient returned to the operating room due to failure of clinical improvement and the two small dural defects were identified as the source of the compressive collection of CSF. The defects were repaired using 5-0 nylon (Ethicon) followed by DuraSeal® (Integra Life Sciences). Postoperatively, motor and sensory function improved and bladder function returned before being discharged on post-operative day 7.
Figure 3.
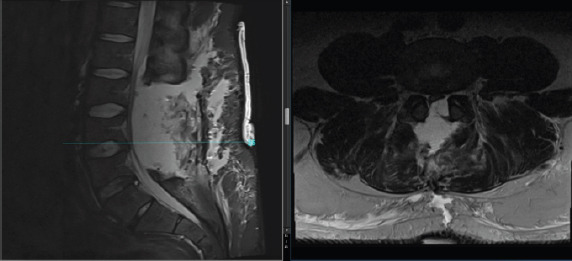
Post-operative magnetic resonance imaging of lumbar spine. Sagittal (STIR) and axial (T2 weighted) images demonstrating a large epidural fluid collection causing significant mass effect on the thecal sac and cauda equina concerning for epidural hematoma versus cerebrospinal fluid leak.
At follow-up 4 months postoperatively, the patient regained bowel and bladder function with only occasional need for self-catheterization. He regained motor strength and sensory distribution from L2-S1 while using an ankle foot orthosis on the right lower extremity due to tibialis anterior weakness.
Discussion
Although CT myelogram may be indicated in select cases to aid in diagnosis of CES, there are significant risks including neurologic injuries, hematoma formation, and CSF leak [4, 5]. The negative effects of CSF leaks are generally limited to transient intracranial hypotension without clinically significant neurologic deficits. To the best of our knowledge, no cases of a CT myelogram causing an accumulation of CSF with subsequent neurologic deficits have been reported. Amini et al. reported a case of a CSF leak causing cauda equina impingement following a lumbar puncture (LP), however, the patient clinically improved without surgical intervention [6]. CES has also been linked to epidural steroid injections [7]. In theory, when a CSF leak occurs, intrathecal and extrathecal CSF pressure should equalize and should not cause compression. However, in this case, the CSF leak resulted in external compression of the thecal sac. One possible explanation is that the hole created by the needle may have acted as a one-way valve, allowing CSF to flow out of the thecal sac but not back in, resulting in external compression of the thecal sac and recompression of the cauda equina. Despite this injury, it is possible that if the CSF leak was not treated, it may have normalized and resulted in no clinically apparent difference.
The most common clinical symptom of a CSF leak is a post-dural puncture headache (PDPH) and occurs in up to one-third of patients undergoing an LP [8, 9, 10]. The risk is lower with fluoroscopically guided LP, occurring at a rate of 2.2% [11]. Approximately 16% of all CSF leaks are due to iatrogenic causes [12]. Careful consideration is necessary performing these procedures for diagnostic purposes. Typically, 22–25G needles are recommended for CT myelography, however, in our case, a 20G needle was used [13]. Use of needles with a smaller diameter and atraumatic needles such as the Sprotte needle may decrease the incidence of PDPH and the risk of a propagating dural injury [12, 13, 14, 15].
Conclusion
Although CT myelogram is historically an alternative imaging modality when MRI is unable to be obtained, it carries significant potential risks including the development of a CSF leak. Clinicians with a reasonably high clinical suspicion for CES may consider forgoing such procedures when diagnosing and treating CES.
Clinical Message.
CT myelogram has the potential to cause CSF leak, which may cause or exacerbate CES. The risks of CT myelogram should be carefully evaluated when considering its use in aiding diagnosis of CES and other spinal pathologies.
Biography


Footnotes
Conflict of Interest: Nil
Source of Support: Nil
Consent: The authors confirm that informed consent was obtained from the patient for publication of this case report
References
- 1.Spector LR, Madigan L, Rhyne A, Darden B, Kim D. Cauda equina syndrome. J Am Acad Orthop Surg. 2008;16:471–9. doi: 10.5435/00124635-200808000-00006. [DOI] [PubMed] [Google Scholar]
- 2.Coscia M, Leipzig T, Cooper D. Acute cauda equina syndrome. Diagnostic advantage of MRI. Spine (Phila Pa 1976) 1994;19:475–8. doi: 10.1097/00007632-199402001-00020. [DOI] [PubMed] [Google Scholar]
- 3.Kebaish KM, Awad JN. Spinal epidural hematoma causing acute cauda equina syndrome. Neurosurg Focus. 2004;16:e1. [PubMed] [Google Scholar]
- 4.Patel DM, Weinberg BD, Hoch MJ. CT myelography:Clinical indications and imaging findings. Radiographics. 2020;40:470–84. doi: 10.1148/rg.2020190135. [DOI] [PubMed] [Google Scholar]
- 5.Sather MD, Gibson MD, Treves JS. Spinal subarachnoid hematoma resulting from lumbar myelography. AJNR Am J Neuroradiol. 2007;28:220–1. [PMC free article] [PubMed] [Google Scholar]
- 6.Amini A, Liu JK, Kan P, Brockmeyer DL. Cerebrospinal fluid dissecting into spinal epidural space after lumbar puncture causing cauda equina syndrome:Review of literature and illustrative case. Childs Nerv Syst. 2006;22:1639–41. doi: 10.1007/s00381-006-0204-6. [DOI] [PubMed] [Google Scholar]
- 7.Slimp KL, Martinez LN, Nielson JA, Johnson RL. Acute cauda equina syndrome caused by epidural steroid injection in the setting of a spinal dural arteriovenous fistula. Cureus. 2022;14:e21752. doi: 10.7759/cureus.21752. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bezov D, Lipton RB, Ashina S. Post-dural puncture headache:Part I diagnosis, epidemiology, etiology, and pathophysiology. Headache. 2010;50:1144–52. doi: 10.1111/j.1526-4610.2010.01699.x. [DOI] [PubMed] [Google Scholar]
- 9.Van Oosterhout WP, van der Plas AA, van Zwet EW, Zielman R, Ferrari MD, Terwindt GM. Postdural puncture headache in migraineurs and nonheadache subjects. Neurology. 2013;80:941–8. doi: 10.1212/WNL.0b013e3182840bf6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Wang YF, Fuh JL, Lirng JF, Chen SP, Hseu SS, Wu JC, et al. Cerebrospinal fluid leakage and headache after lumbar puncture:A prospective non-invasive imaging study. Brain. 2015;138:1492–8. doi: 10.1093/brain/awv016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Rodriguez D, Branstetter BF, Agarwal V, Palfey S, Ching KC, Bump GM, et al. JOURNAL CLUB:Incidence of complications following fluoroscopically guided lumbar punctures and myelograms. Am J Roentgenol. 2016;206:20–5. doi: 10.2214/AJR.15.14664. [DOI] [PubMed] [Google Scholar]
- 12.Le C, Strong EB, Luu Q. Management of anterior skull base cerebrospinal fluid leaks. J Neurol Surg B Skull Base. 2016;77:404–11. doi: 10.1055/s-0036-1584229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.American College of Radiology Website. ACRASNR-SPR Practice Guideline for the Performance of Myelography and Cisternography. United States: American College of Radiology; 2014. Available from: https://www.acr.org/˜/media/ACR/documents/PGTS/guidelines/myelography.pdf . [Google Scholar]
- 14.Arevalo-Rodriguez I, Muñoz L, Godoy-Casasbuenas N, Ciapponi A, Arevalo JJ, Boogaard S, et al. Needle gauge and tip designs for preventing post-dural puncture headache (PDPH) Cochrane Database Syst Rev. 2017;4:CD010807. doi: 10.1002/14651858.CD010807.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Nath S, Koziarz A, Badhiwala JH, Alhazzani W, Jaeschke R, Sharma S, et al. Atraumatic versus conventional lumbar puncture needles:A systematic review and meta-analysis. Lancet. 2018;391:1197–204. doi: 10.1016/S0140-6736(17)32451-0. [DOI] [PubMed] [Google Scholar]