

Key Points
Question
Lower exertional heart rate is associated with worse exercise capacity in patients with heart failure with preserved ejection fraction (HFpEF), but does increasing exercise heart rate with atrial pacing improve exercise tolerance?
Findings
Atrial pacing increased early and peak exercise heart rate, but there was no improvement in exercise performance or quality of life. Despite a higher exercise heart rate, there was no increase in exercise cardiac output, due to a decrease in stroke volume. Pacemaker implantation was associated with adverse events.
Meaning
In patients with HFpEF and inadequate response of heart rate to exertion (chronotropic incompetence), implantation of a pacemaker to enhance exercise heart rate did not improve exercise capacity, symptoms, or exercise cardiac output.
Abstract
Importance
Reduced heart rate during exercise is common and associated with impaired aerobic capacity in heart failure with preserved ejection fraction (HFpEF), but it remains unknown if restoring exertional heart rate through atrial pacing would be beneficial.
Objective
To determine if implanting and programming a pacemaker for rate-adaptive atrial pacing would improve exercise performance in patients with HFpEF and chronotropic incompetence.
Design, Setting, and Participants
Single-center, double-blind, randomized, crossover trial testing the effects of rate-adaptive atrial pacing in patients with symptomatic HFpEF and chronotropic incompetence at a tertiary referral center (Mayo Clinic) in Rochester, Minnesota. Patients were recruited between 2014 and 2022 with 16-week follow-up (last date of follow-up, May 9, 2022). Cardiac output during exercise was measured by the acetylene rebreathe technique.
Interventions
A total of 32 patients were recruited; of these, 29 underwent pacemaker implantation and were randomized to atrial rate responsive pacing or no pacing first for 4 weeks, followed by a 4-week washout period and then crossover for an additional 4 weeks.
Main Outcomes and Measures
The primary end point was oxygen consumption (V̇o2) at anaerobic threshold (V̇o2,AT); secondary end points were peak V̇o2, ventilatory efficiency (V̇e/V̇co2 slope), patient-reported health status by the Kansas City Cardiomyopathy Questionnaire Overall Summary Score (KCCQ-OSS), and N-terminal pro-brain natriuretic peptide (NT-proBNP) levels.
Results
Of the 29 patients randomized, the mean age was 66 years (SD, 9.7) and 13 (45%) were women. In the absence of pacing, peak V̇o2 and V̇o2 at anaerobic threshold (V̇o2,AT) were both correlated with peak exercise heart rate (r = 0.46-0.51, P < .02 for both). Pacing increased heart rate during low-level and peak exercise (16/min [95% CI, 10 to 23], P < .001; 14/min [95% CI, 7 to 21], P < .001), but there was no significant change in V̇o2,AT (pacing off, 10.4 [SD, 2.9] mL/kg/min; pacing on, 10.7 [SD, 2.6] mL/kg/min; absolute difference, 0.3 [95% CI, −0.5 to 1.0] mL/kg/min; P = .46), peak V̇o2, minute ventilation (V̇e)/carbon dioxide production (V̇co2) slope, KCCQ-OSS, or NT-proBNP level. Despite the increase in heart rate, atrial pacing had no significant effect on cardiac output with exercise, owing to a decrease in stroke volume (−24 mL [95% CI, −43 to −5 mL]; P = .02). Adverse events judged to be related to the pacemaker device were observed in 6 of 29 participants (21%).
Conclusions and Relevance
In patients with HFpEF and chronotropic incompetence, implantation of a pacemaker to enhance exercise heart rate did not result in an improvement in exercise capacity and was associated with increased adverse events.
Trial Registration
ClinicalTrials.gov Identifier: NCT02145351
This randomized crossover trial assessed if implanting and programming a pacemaker for rate-adaptive atrial pacing improved exercise performance in patients with heart failure with preserved ejection fraction and chronotropic incompetence at a single US tertiary referral center.
Introduction
Exercise intolerance is the cardinal symptomatic manifestation of heart failure with preserved ejection fraction (HFpEF). Increases in heart rate with exercise are characteristically reduced in patients with HFpEF,1,2,3,4,5,6,7,8,9,10,11 and frank chronotropic incompetence (the inability to reach expected peak heart rates) is present in more than 50% of patients.9,12 In cross-sectional studies, heart rate impairment in HFpEF is correlated with decreased cardiac output reserve and lower aerobic capacity (peak oxygen consumption [V̇o2]).1,2,5,6 Reducing exercise heart rate with negative chronotropic drugs decreased exercise capacity in patients with HFpEF in some studies,13 but not others,14 while β-blocker withdrawal was found to improve aerobic capacity,15 suggesting that heart rate enhancement might be beneficial in patients with HFpEF.
Based on this circumstantial evidence, expert consensus guidelines recommend consideration of pacing in this setting,16,17 but limitations in heart rate achieved with exercise in HFpEF may simply be a consequence of premature cessation because of dyspnea and leg fatigue, rather than a direct cause.10,11,18 There is also potential risk for harm from greater heart rate during exercise due to chamber underfilling reducing preload, exacerbated increases in filling pressures due to incomplete relaxation, inadequate rate-related enhancement in systolic performance, or induction of myocardial ischemia.19,20,21 No study has yet determined whether improving heart rate response to exertion with pacing can safely enhance exercise capacity or other measures of clinical status in patients with HFpEF.
The RAPID-HF (Rate-Adaptive Atrial Pacing in Diastolic Heart Failure) randomized, double-blind, crossover trial was therefore designed to prospectively test whether implanting pacemakers and increasing exertional heart rate through atrial pacing would improve exercise performance in patients with HFpEF and chronotropic incompetence.
Methods
Study Overview
The study protocol is available in Supplement 1; the statistical analysis plan is available in Supplement 2. This was an investigator-initiated, prospective, 2-period, 2-treatment randomized crossover clinical trial of rate-adaptive atrial pacing (AAI-R) for patients with HFpEF and chronotropic incompetence. The crossover trial was performed in a double-blind fashion so each participant was evaluated during both blinded pacing-on and pacing-off phases, each of which lasted 4 weeks and was separated by a 4-week washout period. Investigators, patients, clinicians, and outcome assessors were blinded to treatment assignment. Only the monitor was aware of treatment pacing assignment during each phase. The study was investigator initiated with complete access to the data and funded by Mayo Clinic, with secondary funding provided by Medtronic with a contract that provided no limitations on data to be considered for publication. The study was approved by the Mayo Clinic institutional review board, and all participants provided written informed consent. Data from the study will be available to other investigators on reasonable request by emailing the corresponding author.
Study Design
Participants were required to have left ventricular ejection fraction of 40% or greater, be in sinus rhythm, and have lifestyle-limiting symptoms of dyspnea and fatigue (New York Heart Association class II or greater) meeting objective criteria for heart failure and chronotropic incompetence as defined by low heart-rate reserve (eTable 1 in Supplement 3).22
Eligible participants were approached by the study coordinator. After providing written informed consent, patients were screened for eligibility and evaluated by an electrophysiologist to confirm that pacemaker implantation was clinically appropriate and to review potential risks and benefits (Figure 1). Participants then underwent dual-chamber pacemaker implantation (Azure XT DR MRI SureScan; Medtronic) to provide exertional rate-adaptive atrial pacing, with no planned pacing at rest. Patients taking β-blockers or other heart rate–slowing medicines continued with current dosages, with no down-titration or discontinuation. Following pacemaker implantation, patients were allowed to recover for 4 weeks, during which time the pacemaker was programmed to backup pacing at VVI 30/min only in case of unexpected bradyarrhythmia.
Figure 1. Study Design and Patient Flow in Trial of Rate-Adaptive Atrial Pacing for Heart Failure With Preserved Ejection Fraction.

CPET indicates cardiopulmonary exercise test; KCCQ-OSS, Kansas City Cardiomyopathy Questionnaire Overall Summary Score; NT-proBNP, N-terminal pro-brain natriuretic peptide.
After the 4-week recovery period, patients returned for their randomization visit (to start phase 1 with pacing on or pacing off) and underwent baseline patient-reported health status and assessment of N-terminal pro-brain natriuretic peptide (NT-proBNP) levels. The sequence of the pacing activation status was randomized using simple randomization, with no blocking or stratification imposed on the randomization schema. The list of sequences was generated prior to study initiation to allow for equal allocations of pacing on and pacing off during the first study period. The randomization schedule was secured via password protection so that only the monitor had access; this person was responsible for pacemaker programming as per the randomization sequence. All other investigators were blinded to the pacing allocation. At this randomization visit, patients were tested in AAI-R mode with increased programmed heart rate and slope at both the activity of daily living thresholds (goal heart rate of 100-110/min during brisk hall walk) and peak exercise thresholds (from historically observed peak exercise heart rate responses prior to study enrollment) to achieve greater heart rate during activities of daily living and peak exertion. Programming settings based on the hall walk and peak heart rate settings were saved to be used during the patient’s pacing-on phase. Programming was performed under the supervision of the monitor, with the assistance of an unblinded pacemaker nurse, to pacing-on mode (AAI-R with lower rate limit of 30/min and dual-slope rate response with activity) or pacing-off mode (VVI at 30/min to provide no pacing during activity and only backup pacing in the event of unexpected bradyarrhythmia) for the ensuing 4 weeks (phase 1).
Participants returned 4 weeks later (week 8), at which time they underwent end-point assessment with cardiopulmonary exercise test to maximal exertion, blood testing, and assessment of health status (Figure 1). Following this phase, participants were placed in VVI pacing mode at 30/min for the 4-week washout phase, after which they then returned for crossover programming to the pacing mode opposite of that from their initial randomization visit. Measurement of NT-proBNP level and health status was repeated at this time. Patients returned for their final study visit 4 weeks after the crossover programming was implemented, with repeat end-point assessments mirroring those at week 8. Following this visit, pacing was reprogrammed to standard AAI-R rate responsive settings per standard clinical practice and study procedures were complete.
End Points
Maximal effort cardiopulmonary exercise testing was performed on a treadmill after 4 weeks of pacing on and after 4 weeks of pacing off to measure volumes of oxygen consumed (V̇o2), carbon dioxide produced (V̇co2), breathing frequency, tidal volume, and minute ventilation (V̇e), using a low-resistance, open-circuit automated metabolic system (Medical Graphics) integrated with a mass spectrometer (Perkin Elmer, model 1100) as previously described.1,7,8 Investigators remained blinded to pacing intervention and were instructed to avoid scrutinizing the electrocardiogram for pacing artifacts where possible, other than to note for the presence of ischemia or arrhythmia. Exercise physiologists supervising the tests were blinded to heart rate during the tests to avoid coaching effects.
The primary end point was change in V̇o2 at anaerobic threshold (V̇o2,AT) determined by the V-slope method as the point of disproportionate rise in V̇co2 relative to V̇o2.23 During the early stages of exercise, there is a balanced increase in V̇o2 and V̇co2 as oxidative metabolism increases. At higher workload intensities, oxygen delivery from the heart to muscle is inadequate to meet metabolic demands, resulting in an increase in anaerobic glycolysis, where lactic acid is generated, which is buffered through the action of carbonic anhydrase, such that CO2 is increased out of proportion to O2 consumption (ie, V̇o2), and the V̇o2 at this inflection point defines the V̇o2,AT. V̇o2,AT is known to be impaired in HFpEF1,24 and provides a measure of submaximal exercise performance more representative of activities of daily living in HFpEF as compared with peak exertion. V̇o2,AT can be interpreted even when participants do not achieve their true maximum possible effort.23,25 We hypothesized that higher heart rate with pacing would improve cardiac output and therefore O2 delivery to skeletal muscles during these earlier stages of exercise, which would then lead to a later onset of this shift to anaerobic metabolism and therefore an increase in V̇o2,AT. Secondary end points included peak aerobic capacity (peak V̇o2), determined as the mean of values obtained over the final 30 seconds of exercise, ventilatory efficiency (V̇e/V̇co2) determined as the nadir of V̇e/V̇co2 ratio during exercise, patient-reported health status assessed by the Kansas City Cardiomyopathy Questionnaire Overall Summary Score (KCCQ-OSS),26,27 and change in plasma NT-proBNP levels.
Cardiac output during rest and exercise was measured using an open-circuit acetylene technique that has been previously validated in our laboratory (eMethods in Supplement 3).28 Stroke volume was calculated as cardiac output divided by heart rate. Arterial-venous O2 content difference was calculated by dividing peak V̇o2 by cardiac output. O2 pulse was calculated as the ratio of V̇o2 to heart rate during exercise.
Statistical Analysis
Based on previous work, we have observed that the standard deviation of the change in Vo2,AT between 2 cardiopulmonary exercise tests in participants receiving placebo in the RELAX trial was 1.14 mL/kg/min.29 Assuming this degree of variability will be present for the change between study periods, a sample size of 30 participants provided 90% power to detect a change in V̇o2,AT of 0.70 mL/kg/min or greater with pacing using a paired t test, assuming a 2-sided significance level of .05 in a crossover study design with no statistically significant period or carryover effects. This detectable difference corresponds to approximately 10% of the baseline mean V̇o2,AT observed in the RELAX trial. Peak heart rate in that trial was 109/min (SD, 24/min), on average 39/min below expected peak heart rate based on the average age of the population. Our pacing algorithm was designed to augment the achieved heart rate during early exercise by at least half of the heart rate deficit, and we were therefore adequately powered to test our hypothesis that an increase in heart rate would augment V̇o2,AT by the proposed effect size.
The primary outcome to quantify the effect of pacing-on compared with pacing-off phases was V̇o2,AT in mL/kg/min. For the KCCQ-OSS and NT-proBNP secondary end points, a baseline and postperiod assessment was available under both pacing periods. To simplify the model-based comparisons and better guard against the hypothetical potential for carryover effects, the dependent variables for these end points were taken as the changes in values within the study period. The analysis of the crossover design for all end points considered 2 models: one that allowed for period and carryover effects and a simplified model that assumed the period and carryover effects to be zero. To empirically test if the simplified model was supported by the data, likelihood ratio tests using maximum likelihood estimation to compare the 2 mixed models were used. For all primary and secondary end points, there were no significant carryover or period effects observed. Thus, the final results reported here are based on the restricted maximum likelihood estimates of a mixed model with a main effect of treatment (pacing on or off) and a random participant effect using all available data. Estimated marginal means and 95% CIs were used to summarize the effect of atrial pacing relative to the no pacing condition.
All P values are 2-sided. P < .05 was taken as statistically significant, and no corrections for multiple testing have been added to any reported P values. Analyses were performed using JMP version 14.1.0 (JMP Statistical Discovery) and R version 4.1.2 (R Foundation). Additional model specification details are available in the statistical analysis plan in Supplement 2.
Results
Study Participants
A total of 32 patients met all eligibility criteria and agreed to participate after providing written informed consent between 2014-2022. Three patients did not return for follow-up visits after pacemaker implantation (1 new diagnosis of malignancy, 1 foot fracture, 1 unknown/lost to follow-up), leaving a total of 29 patients who completed the study (Figure 1; eFigure in Supplement 3). One of these patients did not agree to complete the final exercise test but completed all other assessments. Patients were older, obese, with high comorbidity burden and elevated NT-proBNP levels, in keeping with typical HFpEF characteristics observed in the community (Table 1). All participants had HFpEF defined by ejection fraction 50% or greater.
Table 1. Baseline Characteristics.
| No. (%) | ||
|---|---|---|
| Pacing off (n = 15) | Pacing on (n = 14) | |
| Age, mean (SD), y | 66.5 (12.2) | 65.4 (6.4) |
| Age >65 y | 9 (60) | 7 (50) |
| Women | 8 (53) | 5 (36) |
| Men | 7 (47) | 9 (64) |
| BMI, mean (SD) | 32.8 (5.3) | 34.7 (5.7) |
| Heart rate reserve, mean (SD), %a | 0.49 (0.16) | 0.43 (0.13) |
| β-Blockers | 6 (40) | 10 (71) |
| Diuretics | 8 (53) | 13 (93) |
| HFpEF (EF ≥50%) | 15 (100) | 14 (100) |
| Comorbidities | ||
| Hypertension | 13 (87) | 14 (100) |
| Diabetes | 4 (27) | 5 (36) |
| Paroxysmal atrial fibrillation | 5 (33) | 2 (14) |
| Laboratory testing | ||
| NT-proBNP, median (IQR), pg/mL | 197 (141-388) | 159 (81-683) |
| Hemoglobin, mean (SD), g/dL | 13.2 (1.6) | 13.3 (1.7) |
| <12 g/dL | 3 (20) | 4 (29) |
| Creatinine, mean (SD), mg/dL | 1.2 (0.3) | 1.4 (0.3) |
| >1.5 mg/dL | 2 (13) | 5 (36) |
| Echocardiography, mean (SD) | ||
| Left ventricular end diastolic dimension, mm | 47 (12) | 51 (7) |
| Left ventricular mass index, g/m2 | 88 (20) | 83 (25) |
| Left ventricular ejection fraction, % | 63 (6) | 61 (6) |
| Left atrial volume index, mL/m2 | 35 (12) | 39 (8) |
| Septal E/e’ ratiob | 12.7 (5.0) | 14.0 (11.3) |
| Estimated pulmonary artery systolic pressure, mm Hg | 36 (16) | 36 (15) |
Abbreviations: BMI, body mass index; EF, ejection fraction; HFpEF, heart failure with preserved ejection fraction; NT-proBNP, N-terminal pro-brain natriuretic peptide.
SI conversion factor: To convert creatinine values to μmol/L, multiply by 88.4.
Heart rate reserve was calculated as [observed peak heart rate – observed rest heart rate]/[predicted peak heart rate – observed rest heart rate] with predicted peak heart rate = 220 – age. Normal values are greater than 80% or greater than 62% for patients taking β-blockers.
E/e’ is calculated by Doppler echocardiography across the mitral valve and provides a noninvasive estimate of left ventricular filling pressures. It is calculated as the ratio of early diastolic mitral inflow velocity (E) to septal mitral annulus tissue relaxation velocity (e’). Normal values of E/e’ are less than 8.
Consistent with prior cross-sectional studies in patients with HFpEF, there was a significant correlation observed between peak heart rate and V̇o2,AT (r = 0.46, P = .02), as well as peak V̇o2 during the exercise test performed in the pacing-off phase (r = 0.51, P = .006) (Figure 2A).
Figure 2. Heart Rate Dynamics.
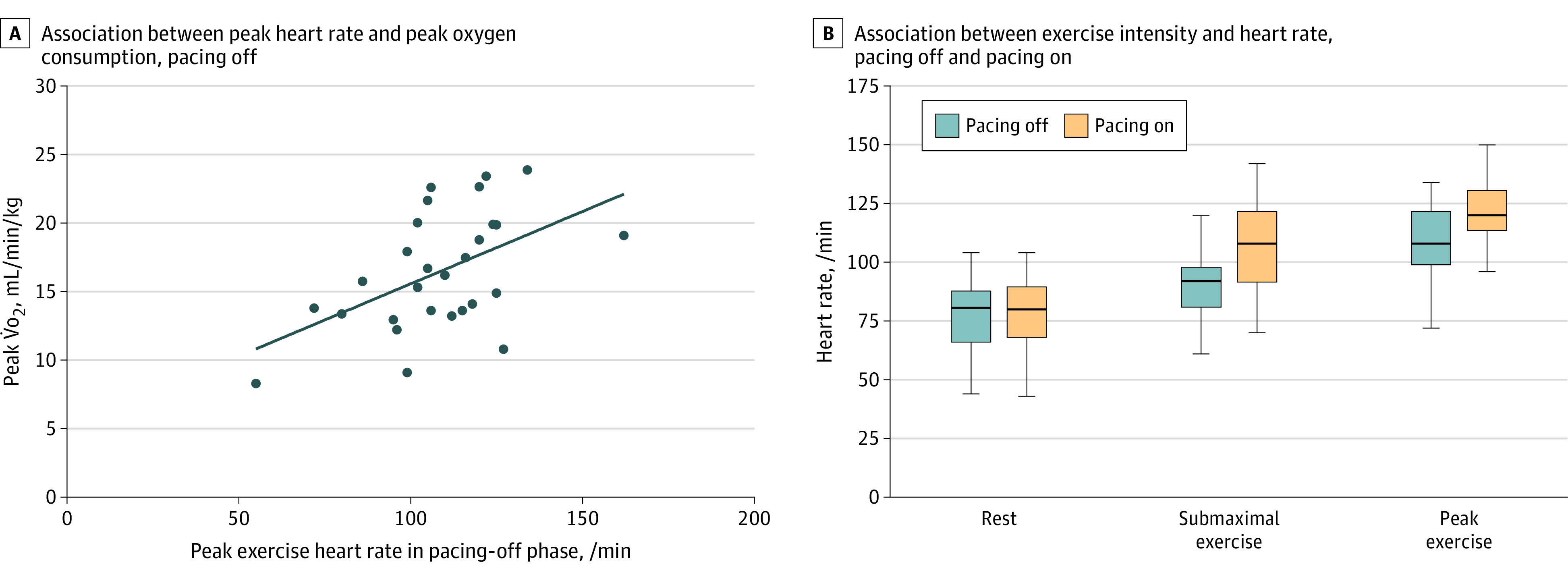
A, Peak exercise heart rate during pacing-off phase was positively associated with peak oxygen consumption (V̇o2) (r = .51, P = .006). B, Tukey box plots represent median and interquartile range, with whiskers extending to the minimum and maximum values. Pacing-on phase was associated with a higher heart rate during submaximal (stage 1 of treadmill) and peak exercise, P < .001 for both comparisons (n = 28 for all 3 pacing-off phases and n = 29 for all 3 pacing-on phases, because 1 patient did not complete the pacing-off–phase exercise test).
Effect of Pacing on Heart Rate Dynamics
Pacemaker device interrogations revealed significantly more atrial pacing averaged throughout the pacing phase (median, 23.87% [95% CI, 13.3%-42.87%]) compared with the placebo phase (median, 0% [95% CI, 0%-0%]) (P < .001), confirming the absence of pacemaker therapy during the control period. There was no clinically significant right ventricular pacing during both the pacing (median, 0.005% [95% CI, 0%-0.168%]) and control (median, 0% [95% CI, 0%-0.01%]) phases, indicating no risk for iatrogenic dyssynchrony effects.
During the exercise testing there was a significant increase in heart rate during submaximal and peak exercise in the pacing-on period as compared with the pacing-off period (Figure 2B). Specifically, during low-level exercise (first stage of treadmill), mean heart rate increased by 16/min (95% CI, 10 to 23; P < .001) with pacing on, and at peak exercise mean heart rate increased by 14/min (95% CI, 7 to 21; P < .001) with pacing on compared with pacing off.
Primary and Secondary End Points
There was no significant effect of pacing on the primary end point of V̇o2,AT from pacing-off to pacing-on phases (mean difference, 0.3 mL/kg/min; [95% CI, −0.5 to 1.0 mL/kg/min]; P = .46) (Table 2, Figure 3). There was also no significant difference in the secondary end points of peak V̇o2 (mean difference, 0.4 mL/kg/min [95% CI, −0.4 to 1.2 mL/kg/min]; P = .27) or V̇e/V̇co2 (mean difference, 0.5 [95% CI, −0.6 to 1.6]; P = .34). There was no significant difference in effort level between tests as determined by the respiratory exchange ratio (1.20 [SD, 0.13] vs 1.23 [SD, 0.13]; mean difference, −0.03 [95% CI, −0.08 to 0.03]; P = .38).
Table 2. Primary and Secondary End Points and Adverse Events.
| Mean (SD) | Absolute difference (95% CI)a | P valueb | ||
|---|---|---|---|---|
| Pacing off | Pacing on | |||
| Primary end point | ||||
| V̇o2 at anaerobic threshold, mL/kg/min | 10.4 (2.9) | 10.7 (2.6) | 0.3 (−0.5 to 1.0) | .46 |
| Secondary end points | ||||
| Peak V̇o2, mL/kg/min | 16.5 (4.3) | 16.8 (4.1) | 0.4 (−0.4 to 1.2) | .27 |
| V̇e/Vco2 slope | 34.2 (6.6) | 34.9 (6.3) | 0.5 (−0.6 to 1.6) | .34 |
| Change in NT-proBNPc | −88 (390) | −36 (255) | 53 (−117 to 221) | .53 |
| Change in KCCQ-OSSc | 4.7 (16.4) | 3.8 (20.2) | −0.9 (−11.0 to 9.3) | .86 |
| Hemodynamic effects | ||||
| Peak heart rate, /min | 109 (21) | 123 (15) | 14 (7 to 21) | <.001 |
| Early exercise heart rate, /min | 90 (16) | 106 (18) | 16 (10 to 23) | <.001 |
| Peak exercise cardiac output, L/min | 11.5 (3.5) | 10.8 (3.0) | −0.7 (−1.7 to 0.3) | .14 |
| Peak exercise stroke volume, mL | 112 (47) | 88 (23) | −24 (−43 to −5) | .02 |
| Adverse events, No. (%) | ||||
| Any adverse event | 8 (27.6) | 7 (24.1) | ||
| Chest discomfort/palpitations | 1 (3.4) | 5 (17) | ||
| Pacemaker implantation–related adverse events, No. (%) | ||||
| Pericardial effusion requiring drainage | 1 (3.4) | |||
| Pacing lead–induced tricuspid regurgitation | 1 (3.4) | |||
| Upper extremity deep venous thrombosis | 1 (3.4) | |||
| Incision site reaction | 3 (10.3) | |||
Abbreviations: KCCQ-OSS, Kansas City Cardiomyopathy Questionnaire Overall Summary Score; NT-proBNP, N-terminal pro-brain natriuretic peptide; V̇e/V̇co2, minute ventilation/carbon dioxide production; V̇o2, oxygen consumption.
Reflects change after 4 weeks of pacing on compared with pacing off.
The 2-period, 2-treatment crossover design was analyzed using a linear mixed model for each of the end points, including measures of hemodynamic effects. The final models consisted of a main (fixed) effect for pacing status only (ie, no period or carryover effects) and a random-participant effect with a compound symmetry covariance structure on the repeated outcomes. The models were used to estimate the absolute differences, confidence intervals, and P values. Separate models were used for each end point.
Reflects change from the beginning of the pacing-off/pacing-on phase to the end of that 4-week phase. KCCQ-OSS range, 0 to 100; higher scores are better.
Figure 3. Parallel Line Plots of Primary and Select Secondary End Points.

Each vertical line represents an individual patient, with patients ordered by baseline value with pacing off, with the vertical line extending up (improvement) or down (deterioration) in the pacing-on phase. For panel A, P = .46; panel B, P = .27; and panel C, P = .86. KCCQ-OSS indicates Kansas City Cardiomyopathy Questionnaire Overall Summary Score; V̇o2, oxygen consumption; V̇o2,AT, oxygen consumption at anaerobic threshold.
There was no significant difference in the change in NT-proBNP level during pacing-off compared with pacing-on phases (mean difference, 53 pg/mL [95% CI, −117 to 221 pg/mL]; P = .53). There was no significant difference in the change in KCCQ-OSS during pacing-off compared with pacing-on phases (mean difference, −0.9 [95% CI, −11.0 to 9.3]; P = .86) (Figure 3).
Exploratory Mechanistic Analyses
Exploratory analyses using O2 pulse (V̇o2/heart rate, a surrogate for stroke volume) demonstrated a significant decrease in O2 pulse during pacing compared with control phase (mean difference, −0.015 mL/kg/min/beat [95% CI, −0.024 to −0.006 mL/kg/min/beat]; P = .002). Adequate-quality data for acetylene cardiac output from both phases was available for 22 patients. Despite the increase in heart rate, there was no significant effect of pacing on exercise cardiac output (mean difference, −0.7 L/min [95% CI, −1.7 to 0.3 L/min]; P = .14). This was related to a significant decrease in stroke volume at peak exercise during the pacing phase compared with the control phase (mean difference, −24 mL [95% CI, −43 to −5 mL]; P = .02). There was no significant difference in arterial-venous O2 content difference with pacing (mean difference, 1.0 mL/dL [95% CI, −0.3 to 2.2 mL/dL]; P = .13).
Safety
A total of 6 adverse events were observed and judged related to the pacemaker implantation procedure, including 1 upper extremity deep vein thrombosis, 1 pericardial effusion requiring drainage, 1 potential case of pacemaker lead–induced tricuspid regurgitation, and 3 local skin reactions at the pacemaker pocket site. There was 1 serious adverse event that was judged related to pacemaker implantation (pericardial effusion). Minor adverse events during the pacing-on phase occurred in 8 patients during the control phase and 7 during pacing (Table 2). Chest discomfort or palpitations occurred in 5 patients during the pacing-on phase compared with 1 during the pacing-off phase (details available in eTable 2 in Supplement 3).
Discussion
This randomized, double-blind crossover trial was conducted to determine whether increasing heart rate during exercise would improve exercise performance in patients with HFpEF. All patients were required to fulfill the current criteria for chronotropic incompetence as an indication for rate adaptive atrial pacing and received a dual-chamber pacemaker, with exercise capacity compared after 4 weeks of treatment with pacing on and pacing off, separated by a washout period. There was a direct relationship between exercise heart rate and exercise capacity during the pacing-off phase, and heart rate during exercise was increased with pacing. However, there was no beneficial effect of pacing on patient-perceived health status or on exercise performance using objectively measured cardiopulmonary exercise metrics independent of baseline activity levels (peak V̇o2, V̇o2,AT). The absence of benefit may relate to a decrease in stroke volume during exercise, which prevented gains in cardiac output from a higher exercise heart rate during pacing. There were also adverse events clearly related to pacemaker implantation, as well as an increased incidence of chest pain during pacing phases, which mechanistically could be related to pacing-related discomfort, angina from myocardial supply-demand mismatch, or both. These data do not support use of rate-adaptive atrial pacing to treat patients with HFpEF and chronotropic incompetence.
Exercise capacity in patients with HFpEF is limited by impairments in cardiac output, peripheral limitations in oxygen transport and utilization, and elevation in filling pressures that promote lung congestion.5,6,8,30 With a cardiac-centered intervention (pacing), there was predictably no change in O2 uptake and utilization in the periphery (as assessed by the arterial-venous O2 content difference), which is an important modifiable factor for exercise tolerance in HFpEF.6,31 However, there was also no improvement in cardiac output despite the increase in exercise heart rate with pacing, which is the most likely explanation for the lack of benefit in exercise performance. This may have been related to a reduction in stroke volume with pacing. Prior studies at rest in HFpEF have suggested that atrial pacing decreases resting stroke volume.32,33,34 The current study suggests that faster atrial pacing during exercise also results in a decrease in exercise stroke volume that prevents further increases in exercise cardiac output. The mechanisms for stroke volume reduction with pacing cannot be determined but may relate to increased intramyocellular calcium with higher heart rate, impairing diastolic function,35 as well as inadequate time for relaxation with shorter diastolic periods as heart rate increases,19,20 which may result in left ventricular underfilling (lower preload or left ventricular end diastolic volume). Patients with HFpEF also display blunted increases in contractile function with exercise,7,36 including impaired force-frequency responses (ie, less augmentation in contractility with higher heart rate, or Treppe phenomenon),21 which may have limited the ability to augment ejection. Right atrial pacing may also result in interatrial dyssynchrony37 with a more delayed left atrial activation than the typical sinus node activation sequence, which may have deleterious effects on left atrial booster function.38 Increases in heart rate also augment arterial afterload, which could worsen ventricular-vascular coupling reserve during exertion, contributing to blunted stroke volume responses.
In addition to lack of efficacy, pacemaker implantation was associated with increased risk of significant, clinically important adverse events, even when implanted by highly experienced operators (Table 2; eTable 2 in Supplement 3). Current guideline recommendations for pacing for chronotropic incompetence are largely based on expert opinion, including consideration of pacing in patients with HFpEF and a phenotype with chronotropic incompetence.16,17 The present data do not support this recommendation.
Limitations
This study had limitations. First, the study was single center owing to the sophisticated expired gas assessments performed and cost considerations, which may limit generalizability. Second, the cohort studied was relatively small, but sample size was selected to provide adequate power to test the study hypothesis while balancing cost, risk, and participant burden considerations, which were significant, including invasive pacemaker implantation, repeated exercise tests, and multiple follow-up visits. These factors, along with a lack of equipoise from many primary cardiologists, were associated with a long enrollment period. Indeed, these barriers were responsible for premature discontinuation of a prior multicenter trial of pacing in HFpEF that was abandoned due to poor enrollment.34 Third, activity levels were not directly measured in this study. Patients with HFpEF are typically sedentary, and this lack of activity may have affected the response to pacing. Fourth, cardiac filling pressures were not directly assessed at rest or during exercise, so the effect on central hemodynamics of higher heart rate during the pacing-on phase could not be determined. Fifth, paired cardiac output assessments with exercise were not available in 6 of 28 patients, but despite the smaller sample size reducing power, statistically significant reductions in stroke volume were still apparent, and the results were consistent with the reduction in O2 pulse from cardiopulmonary testing.
Conclusions
In patients with HFpEF and chronotropic incompetence, implantation of a pacemaker to enhance exercise heart rate did not result in an improvement in exercise capacity and was associated with increased adverse events.
Study Protocol
Statistical Analysis Plan
eMethods
eTable 1. Inclusion and Exclusion Criteria
eTable 2. Adverse Events During Pacing-Off And Pacing-On Phase
eFigure. Number of Patients Enrolled Per Year
Data Sharing Statement
References
- 1.Borlaug BA, Melenovsky V, Russell SD, et al. Impaired chronotropic and vasodilator reserves limit exercise capacity in patients with heart failure and a preserved ejection fraction. Circulation. 2006;114(20):2138-2147. doi: 10.1161/CIRCULATIONAHA.106.632745 [DOI] [PubMed] [Google Scholar]
- 2.Brubaker PH, Joo KC, Stewart KP, Fray B, Moore B, Kitzman DW. Chronotropic incompetence and its contribution to exercise intolerance in older heart failure patients. J Cardiopulm Rehabil. 2006;26(2):86-89. doi: 10.1097/00008483-200603000-00007 [DOI] [PubMed] [Google Scholar]
- 3.Phan TT, Shivu GN, Abozguia K, et al. Impaired heart rate recovery and chronotropic incompetence in patients with heart failure with preserved ejection fraction. Circ Heart Fail. 2010;3(1):29-34. doi: 10.1161/CIRCHEARTFAILURE.109.877720 [DOI] [PubMed] [Google Scholar]
- 4.Kosmala W, Rojek A, Przewlocka-Kosmala M, Mysiak A, Karolko B, Marwick TH. Contributions of nondiastolic factors to exercise intolerance in heart failure with preserved ejection fraction. J Am Coll Cardiol. 2016;67(6):659-670. doi: 10.1016/j.jacc.2015.10.096 [DOI] [PubMed] [Google Scholar]
- 5.Reddy YNV, Olson TP, Obokata M, Melenovsky V, Borlaug BA. Hemodynamic correlates and diagnostic role of cardiopulmonary exercise testing in heart failure with preserved ejection fraction. JACC Heart Fail. 2018;6(8):665-675. doi: 10.1016/j.jchf.2018.03.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Haykowsky MJ, Brubaker PH, John JM, Stewart KP, Morgan TM, Kitzman DW. Determinants of exercise intolerance in elderly heart failure patients with preserved ejection fraction. J Am Coll Cardiol. 2011;58(3):265-274. doi: 10.1016/j.jacc.2011.02.055 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Borlaug BA, Olson TP, Lam CS, et al. Global cardiovascular reserve dysfunction in heart failure with preserved ejection fraction. J Am Coll Cardiol. 2010;56(11):845-854. doi: 10.1016/j.jacc.2010.03.077 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Abudiab MM, Redfield MM, Melenovsky V, et al. Cardiac output response to exercise in relation to metabolic demand in heart failure with preserved ejection fraction. Eur J Heart Fail. 2013;15(7):776-785. doi: 10.1093/eurjhf/hft026 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Brubaker PH, Kitzman DW. Chronotropic incompetence: causes, consequences, and management. Circulation. 2011;123(9):1010-1020. doi: 10.1161/CIRCULATIONAHA.110.940577 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Sarma S, Howden E, Lawley J, Samels M, Levine BD. Central command and the regulation of exercise heart rate response in heart failure with preserved ejection fraction. Circulation. 2021;143(8):783-789. doi: 10.1161/CIRCULATIONAHA.120.048338 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Sarma S, Stoller D, Hendrix J, et al. Mechanisms of chronotropic incompetence in heart failure with preserved ejection fraction. Circ Heart Fail. 2020;13(3):e006331. doi: 10.1161/CIRCHEARTFAILURE.119.006331 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Wolsk E, Kaye DM, Komtebedde J, et al. Determinants and consequences of heart rate and stroke volume response to exercise in patients with heart failure and preserved ejection fraction. Eur J Heart Fail. 2021;23(5):754-764. doi: 10.1002/ejhf.2146 [DOI] [PubMed] [Google Scholar]
- 13.Pal N, Sivaswamy N, Mahmod M, et al. Effect of selective heart rate slowing in heart failure with preserved ejection fraction. Circulation. 2015;132(18):1719-1725. doi: 10.1161/CIRCULATIONAHA.115.017119 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kosmala W, Holland DJ, Rojek A, Wright L, Przewlocka-Kosmala M, Marwick TH. Effect of If-channel inhibition on hemodynamic status and exercise tolerance in heart failure with preserved ejection fraction: a randomized trial. J Am Coll Cardiol. 2013;62(15):1330-1338. doi: 10.1016/j.jacc.2013.06.043 [DOI] [PubMed] [Google Scholar]
- 15.Palau P, Seller J, Domínguez E, et al. Effect of β-blocker withdrawal on functional capacity in heart failure and preserved ejection fraction. J Am Coll Cardiol. 2021;78(21):2042-2056. doi: 10.1016/j.jacc.2021.08.073 [DOI] [PubMed] [Google Scholar]
- 16.Kusumoto FM, Schoenfeld MH, Barrett C, et al. 2018 ACC/AHA/HRS guideline on the evaluation and management of patients with bradycardia and cardiac conduction delay: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2019;74(7):e51-e156. doi: 10.1016/j.jacc.2018.10.044 [DOI] [PubMed] [Google Scholar]
- 17.Shah SJ, Kitzman DW, Borlaug BA, et al. Phenotype-specific treatment of heart failure with preserved ejection fraction: a multiorgan roadmap. Circulation. 2016;134(1):73-90. doi: 10.1161/CIRCULATIONAHA.116.021884 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Mesquita T, Zhang R, Cho JH, et al. Mechanisms of sinoatrial node dysfunction in heart failure with preserved ejection fraction. Circulation. 2022;145(1):45-60. doi: 10.1161/CIRCULATIONAHA.121.054976 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Hay I, Rich J, Ferber P, Burkhoff D, Maurer MS. Role of impaired myocardial relaxation in the production of elevated left ventricular filling pressure. Am J Physiol Heart Circ Physiol. 2005;288(3):H1203-H1208. doi: 10.1152/ajpheart.00681.2004 [DOI] [PubMed] [Google Scholar]
- 20.Borlaug BA, Jaber WA, Ommen SR, Lam CS, Redfield MM, Nishimura RA. Diastolic relaxation and compliance reserve during dynamic exercise in heart failure with preserved ejection fraction. Heart. 2011;97(12):964-969. doi: 10.1136/hrt.2010.212787 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Liu CP, Ting CT, Lawrence W, Maughan WL, Chang MS, Kass DA. Diminished contractile response to increased heart rate in intact human left ventricular hypertrophy: systolic versus diastolic determinants. Circulation. 1993;88(4, pt 1):1893-1906. doi: 10.1161/01.CIR.88.4.1893 [DOI] [PubMed] [Google Scholar]
- 22.Kligfield P, Lauer MS. Exercise electrocardiogram testing: beyond the ST segment. Circulation. 2006;114(19):2070-2082. doi: 10.1161/CIRCULATIONAHA.105.561944 [DOI] [PubMed] [Google Scholar]
- 23.Wasserman K, Beaver WL, Whipp BJ. Gas exchange theory and the lactic acidosis (anaerobic) threshold. Circulation. 1990;81(1)(suppl):II14-II30. [PubMed] [Google Scholar]
- 24.Kitzman DW, Little WC, Brubaker PH, et al. Pathophysiological characterization of isolated diastolic heart failure in comparison to systolic heart failure. JAMA. 2002;288(17):2144-2150. doi: 10.1001/jama.288.17.2144 [DOI] [PubMed] [Google Scholar]
- 25.Malhotra R, Bakken K, D’Elia E, Lewis GD. Cardiopulmonary exercise testing in heart failure. JACC Heart Fail. 2016;4(8):607-616. doi: 10.1016/j.jchf.2016.03.022 [DOI] [PubMed] [Google Scholar]
- 26.Joseph SM, Novak E, Arnold SV, et al. Comparable performance of the Kansas City Cardiomyopathy Questionnaire in patients with heart failure with preserved and reduced ejection fraction. Circ Heart Fail. 2013;6(6):1139-1146. doi: 10.1161/CIRCHEARTFAILURE.113.000359 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Green CP, Porter CB, Bresnahan DR, Spertus JA. Development and evaluation of the Kansas City Cardiomyopathy Questionnaire: a new health status measure for heart failure. J Am Coll Cardiol. 2000;35(5):1245-1255. doi: 10.1016/S0735-1097(00)00531-3 [DOI] [PubMed] [Google Scholar]
- 28.Johnson BD, Beck KC, Proctor DN, Miller J, Dietz NM, Joyner MJ. Cardiac output during exercise by the open circuit acetylene washin method: comparison with direct Fick. J Appl Physiol (1985). 2000;88(5):1650-1658. doi: 10.1152/jappl.2000.88.5.1650 [DOI] [PubMed] [Google Scholar]
- 29.Redfield MM, Chen HH, Borlaug BA, et al. ; RELAX Trial . Effect of phosphodiesterase-5 inhibition on exercise capacity and clinical status in heart failure with preserved ejection fraction: a randomized clinical trial. JAMA. 2013;309(12):1268-1277. doi: 10.1001/jama.2013.2024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Reddy YNV, Obokata M, Wiley B, et al. The haemodynamic basis of lung congestion during exercise in heart failure with preserved ejection fraction. Eur Heart J. 2019;40(45):3721-3730. doi: 10.1093/eurheartj/ehz713 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Pandey A, Shah SJ, Butler J, et al. Exercise intolerance in older adults with heart failure with preserved ejection fraction. J Am Coll Cardiol. 2021;78(11):1166-1187. doi: 10.1016/j.jacc.2021.07.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Westermann D, Kasner M, Steendijk P, et al. Role of left ventricular stiffness in heart failure with normal ejection fraction. Circulation. 2008;117(16):2051-2060. doi: 10.1161/CIRCULATIONAHA.107.716886 [DOI] [PubMed] [Google Scholar]
- 33.Kitzman DW. Diastolic dysfunction: one piece of the heart failure with normal ejection fraction puzzle. Circulation. 2008;117(16):2044-2046. doi: 10.1161/CIRCULATIONAHA.108.770602 [DOI] [PubMed] [Google Scholar]
- 34.Kass DA, Kitzman DW, Alvarez GE. The Restoration of chronotropic compEtence in heart failure patientS with normal Ejection fracTion (RESET) study: rationale and design. J Card Fail. 2010;16(1):17-24. doi: 10.1016/j.cardfail.2009.08.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Selby DE, Palmer BM, LeWinter MM, Meyer M. Tachycardia-induced diastolic dysfunction and resting tone in myocardium from patients with a normal ejection fraction. J Am Coll Cardiol. 2011;58(2):147-154. doi: 10.1016/j.jacc.2010.10.069 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Borlaug BA, Kane GC, Melenovsky V, Olson TP. Abnormal right ventricular-pulmonary artery coupling with exercise in heart failure with preserved ejection fraction. Eur Heart J. 2016;37(43):3293-3302. doi: 10.1093/eurheartj/ehw241 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Laurent G, Eicher JC, Mathe A, et al. Permanent left atrial pacing therapy may improve symptoms in heart failure patients with preserved ejection fraction and atrial dyssynchrony: a pilot study prior to a national clinical research programme. Eur J Heart Fail. 2013;15(1):85-93. doi: 10.1093/eurjhf/hfs150 [DOI] [PubMed] [Google Scholar]
- 38.Martens P, Deferm S, Bertrand PB, et al. The detrimental effect of RA pacing on LA function and clinical outcome in cardiac resynchronization therapy. JACC Cardiovasc Imaging. 2020;13(4):895-906. doi: 10.1016/j.jcmg.2019.04.022 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Study Protocol
Statistical Analysis Plan
eMethods
eTable 1. Inclusion and Exclusion Criteria
eTable 2. Adverse Events During Pacing-Off And Pacing-On Phase
eFigure. Number of Patients Enrolled Per Year
Data Sharing Statement