

Abstract
Rationale
The coronavirus disease (COVID-19) pandemic has negatively affected women more than men and may influence the publication of non–COVID-19 research.
Objectives
To evaluate whether the COVID-19 pandemic is associated with changes in manuscript acceptance rates among pulmonary/critical care journals and sex-based disparities in these rates.
Methods
We analyzed first, senior, and corresponding author sex (female vs. male, identified by matching first names in a validated Genderize database) of manuscripts submitted to four pulmonary/critical care journals between January 1, 2018 and December 31, 2020. We constructed interrupted time series regression models to evaluate whether the proportion of female first and senior authors of non–COVID-19 original research manuscripts changed with the pandemic. Next, we performed multivariable logistic regressions to evaluate the association of author sex with acceptance of original research manuscripts.
Results
Among 8,332 original research submissions, women represented 39.9% and 28.3% of first and senior authors, respectively. We found no change in the proportion of female first or senior authors of non–COVID-19 or COVID-19 submitted research manuscripts during the COVID-19 era. Non–COVID-19 manuscripts submitted during the COVID-19 era had reduced odds of acceptance, regardless of author sex (first author adjusted OR [aOR], 0.46 [95% confidence interval (CI), 0.36–0.59]; senior author aOR, 0.46 [95% CI, 0.37–0.57]). Female senior authorship was associated with decreased acceptance of non–COVID-19 research manuscripts (crude rates, 14.4% [male] vs. 13.2% [female]; aOR, 0.84 [95% CI, 0.71–0.99]).
Conclusions
Although female author submissions were not disproportionately influenced by COVID-19, we found evidence suggesting sex disparities in manuscript acceptance rates. Journals may need to consider strategies to reduce this disparity, and academic institutions may need to factor our findings, including lower acceptance rates for non–COVID-19 manuscripts, into promotion decisions.
Keywords: sex bias, publications, COVID-19 pandemic, scholarly publishing
The coronavirus disease (COVID-19) pandemic has profoundly disrupted academic endeavors worldwide, with a disproportionately negative impact on female physicians and scientists compared with their male colleagues (1, 2). In a survey of more than 5,000 faculty, staff, and trainees at a large academic medical institution, nearly half of participants were moderately or seriously worried that the COVID-19 pandemic negatively affected their career development. In particular, women with children were more likely to consider reducing their hours or leaving the workforce altogether (3). Similarly, in a study of scientists based in the United States and Europe, women (particularly those with young dependents) reported larger declines in their research-dedicated time during the pandemic compared with their male colleagues (4).
Not surprisingly, women’s scholarly output has disproportionately suffered during the pandemic (5, 6). One study estimated that female first authors published COVID-19–related manuscripts at a 19% lower than expected rate than manuscripts published in similar journals before the pandemic began, suggesting that women may have less flexibility to pivot their focus toward timely research topics (7). Because manuscript publication in high-impact journals is a crucial measure of scientific productivity and necessary for career advancement, these findings highlight how the COVID-19 pandemic may amplify existing sex-based disparities in academic medicine (8–20).
Furthermore, the torrent of articles published on COVID-19 since early 2020 also may have negatively impacted research unrelated to COVID-19 (21, 22). COVID-19–related studies were published at much faster rates during 2020 than are typical for most journals (21), whereas the number of non–COVID-19 research manuscripts published in leading medical journals decreased during the same time period (23). The quality of published studies, of which manuscript acceptance rate is an indirect indicator, may also have been influenced by the urgency to publish COVID-19–related research.
Rapid review and publication of research related to COVID-19 is crucial to inform clinicians, administrators, and policy makers as part of efforts to save lives during a public health emergency. However, it is also imperative that high-quality research on non–COVID-19 topics continue to be disseminated despite and throughout the pandemic. For this reason, we sought to describe submission changes after the COVID-19 pandemic started and to evaluate whether the pandemic was associated with changes in manuscript acceptance rates among four journals focused on pulmonary and critical care medicine, a field with a clinical and research workforce on the front line combating the pandemic. Because the COVID-19 pandemic has disproportionately affected female physicians and scientists, we also aimed to evaluate if the pandemic was associated with potential sex-based disparities in these rates. We hypothesized that 1) the pandemic would be associated with reduced acceptance rates among non–COVID-19 original research articles, 2) a minority of submitted manuscripts before and during the COVID-19 pandemic would be from female first or senior authors, and 3) acceptance rates (as a proxy measure of manuscript quality) would not differ by sex.
Methods
We obtained data on all manuscripts submitted to three journals published by the American Thoracic Society (ATS) (American Journal of Respiratory and Critical Care Medicine [AJRCCM], American Journal of Respiratory Cell and Molecular Biology [AJRCMB], and Annals of the American Thoracic Society [AnnalsATS]) and the journal published by the American College of Chest Physicians (CHEST) between January 1, 2018, and December 31, 2020. We did not include manuscripts submitted to ATS Scholar, because this journal was first published in February 2020. Only first names of authors were provided by the journals. This study was approved by the Veterans Affairs Institutional Review Board (5027).
Cohort
Our primary cohort consisted of original research manuscripts and/or original contributions (as defined by ATS journals [24–26]) submitted via the online submission systems. We excluded manuscripts submitted to CHEST from the primary cohort because they did not include information regarding first and senior author sex. We divided the primary cohort into two mutually exclusive subgroups: COVID-19 and non–COVID-19 manuscripts. COVID-19 manuscripts were defined as those submitted on or after March 11, 2020 (the date COVID-19 was declared a pandemic by the World Health Organization, defined as the COVID-19 era) (27), and that included “COVID,” “coronavirus,” or “SARS-CoV-2” in their titles. We defined non–COVID-19 manuscripts as those submitted at any point over the 3-year study period that did not have “COVID,” “coronavirus,” or SARS-CoV-2” in their manuscript titles. Any manuscript not meeting either criterion was excluded.
We considered two sensitivity cohorts. First, we expanded our cohort to include all manuscript types (e.g., including editorials, commentaries, letters). Second, we included original research submitted to ATS journals and CHEST (when examining corresponding author sex).
Exposures and Outcomes
We performed two distinct primary analyses. In the first analysis, the primary exposure was first author sex (female vs. male). In the second analysis, the primary exposure was senior author sex (female vs. male), defined as the last author listed for a given manuscript. Corresponding author sex was our primary exposure in sensitivity analyses. We identified author sex by matching first names to entries in a validated Genderize database containing 216,286 names across 79 countries and 89 languages (28) and that previously has been found to have a misclassification rate of 1.7% (29). We merged these data with a gender package in R that relies on historical data from the U.S. Census Bureau and Social Security registrations to determine whether a name was associated with a particular sex during our specified time frame (30). If we were unable to identify an author’s sex, we excluded that manuscript from its corresponding analyses. (For example, if we identified senior author but not first author sex, the paper was only included in the senior author analysis.) For manuscripts with one author only, that author was considered both first and senior author. Our primary outcome was manuscript acceptance, classified as either acceptance (i.e., outright or after “revise/resubmit”) or rejection (either before or after review).
Other Data Elements
Data obtained from all journals included the first names and countries of corresponding authors, manuscript title, date of submission, study type (e.g., original research manuscript, systematic review, editorial), and final decision (e.g., accepted for publication, rejected after review). In addition, ATS journals’ data included the number of authors, first names and countries of all authors, whether the manuscript was received as a transfer from AJRCCM (to AJRCMB or AnnalsATS), and subject categories (31). Countries were grouped into United Nations world regions (32).
Analysis
We used descriptive statistics as appropriate to examine the proportion of women in first and senior author positions among all manuscripts. We used Wilcoxon rank-sum testing to evaluate differences in the number of submissions and acceptance rates over time, and we used chi-square testing to compare author sex in COVID-19 and non–COVID-19 manuscripts by calendar month and world region. Next, we constructed interrupted time series regression models to assess whether the proportion of female first and senior authors of non–COVID-19 manuscripts changed coincident with the COVID-19 pandemic. For these analyses, first and senior author sex were modeled separately. We included three independent variables: month of submission since January 2018 (modeled as linear), submission during the COVID-19 pandemic (modeled as binary), and month of submission since the beginning of the COVID-19 pandemic (modeled as linear with value of 0 before March 11, 2020) (33).
Finally, we performed a series of multivariable logistic regressions to separately evaluate 1) whether the pandemic is associated with changes in manuscript acceptance rates for non–COVID-19 research, 2) whether first author sex is associated with acceptance rates of original research for both non–COVID-19 and COVID-19 manuscripts, and3) whether senior author sex is associated with acceptance rates of original research for both non–COVID-19 and COVID-19 manuscripts. Non–COVID-19 and COVID-19 manuscripts were considered separately. Each model was adjusted for author world region and journal; non–COVID-19 manuscript models were also adjusted for subject category. These covariates were selected a priori on the basis of concerns that they may be associated both with our exposures (first and, separately, senior author sex) and our outcome (manuscript acceptance). In addition, among the non–COVID-19 cohort, we evaluated whether the COVID-19 era is an effect modifier for the association of author sex with manuscript acceptance. For this analysis, we included an interaction term between the submission during the COVID-19 era (on or after March 11, 2020) with author sex. Margins for each author sex were calculated from each model assuming all covariables (all independent variables other than author sex) were at population mean values.
Sensitivity Analyses
We performed several sensitivity analyses. First, across ATS journals, we evaluated the association of author sex with acceptance rates among all manuscript types and then excluding papers transferred to AJRCMB or AnnalsATS from AJRCCM. Next, among all original research submissions to ATS journals and CHEST, we evaluated the association of corresponding author sex with acceptance rates. Last, we evaluated all submissions (not limited to original research manuscripts) to ATS journals and CHEST. Given low rates of missingness (∼5%), complete cases were used for all analyses.
Statistical significance was determined on the basis of a P < 0.05 threshold. No adjustments were made for multiple comparisons, because each primary analysis (for first and, separately, senior author sex) was distinct. All nonprimary analyses (e.g., sensitivity analyses) should be considered supportive and hypothesis generating.
Results
Manuscript Submissions
We identified 8,373 original research manuscripts that were submitted to all ATS journals during the study period, 880 of which related to COVID-19 (Figure 1). The total number of submitted research manuscripts increased during the COVID-19 era (median [interquartile range], 189.5 [183–209] before COVID-19 to 335 [306–366] during the COVID-19 era; P < 0.001) (see Figure E1 in the data supplement). Of the 7,493 non–COVID-19 manuscripts, we identified the sex of 95.0% of first authors and 94.8% of senior authors. After excluding 41 COVID-19–related manuscripts submitted before March 11, 2020, our cohort consisted of 839 COVID-19 manuscripts; we identified the sex of 95.4% of first authors and 92.6% of senior authors. In addition, among 15,870 original research manuscripts with corresponding authors across both CHEST and ATS journals, we identified the sex of the corresponding author in 86.8% of COVID-19 manuscripts and 89.9% of non–COVID-19 manuscripts that were published on or after March 11, 2020 (Figure E2).
Figure 1.

Flow diagram. AJRCCM = American Journal of Respiratory and Critical Care Medicine; AJRCMB = American Journal of Respiratory Cell and Molecular Biology; AnnalsATS = Annals of the American Thoracic Society; ATS = American Thoracic Society.
Table 1 shows the characteristics of the original research submissions to the ATS journals. Among all research manuscripts with nonmissing sex submitted during the study period, women represented 39.9% and 28.3% of first and senior authors, respectively. In unadjusted analyses, 41.6% of submitted manuscripts had female first authors before the pandemic, compared with 37.0% submitted during the pandemic.
Table 1.
Cohort characteristics*
| Full Cohort (n) | Female First Author† [n (%)] | Female Senior Author† [n (%)] | |
|---|---|---|---|
| No. of manuscripts (%) | 8,332 | 3,157 (39.9) | 2,227 (28.3) |
| Journal | |||
| AJRCCM | 5,316 | 1,969 (39.0) | 1,379 (27.5) |
| AJRCMB | 1,029 | 413 (42.9) | 293 (30.1) |
| AnnalsATS | 1,987 | 775 (40.6) | 555 (29.4) |
| Transfer from AJRCCM | 698 | 265 (40.1) | 226 (33.8) |
| No. of authors, median (IQR) | 9 (6, 13) | 9 (7, 13) | 9 (6, 13) |
| Subject category‡ | |||
| Asthma | 256 | 102 (42.0) | 78 (31.8) |
| Behavioral science | 104 | 56 (55.4) | 25 (25.8) |
| Cell & mol biology | 116 | 51 (44.7) | 23 (20.9) |
| Critical care | 721 | 215 (31.8) | 156 (22.7) |
| Environmental hlth | 144 | 57 (41.0) | 48 (35.3) |
| Lung disease | 849 | 318 (39.0) | 209 (26.2) |
| Microbio & infn | 391 | 121 (32.8) | 90 (24.1) |
| Mycobacteria | 224 | 97 (45.8) | 74 (34.1) |
| Other | 235 | 90 (40.5) | 54 (25.0) |
| Pediatrics | 92 | 40 (46.0) | 39 (45.3) |
| Sleep | 218 | 89 (43.0) | 62 (29.4) |
| Vascular biology | 83 | 25 (32.1) | 25 (33.3) |
| More than one category | 4,717 | 1,830 (40.8) | 1,299 (29.1) |
| World region of first author§ | |||
| N America | 3,550 | 1,362 (39.9) | 998 (29.0) |
| Europe | 2,097 | 876 (43.2) | 575 (28.3) |
| Aust/NZ/Oceania | 263 | 117 (45.7) | 80 (31.6) |
| Cent/S Am, Carib | 156 | 53 (35.8) | 42 (28.4) |
| Asia | 1,936 | 639 (36.6) | 441 (26.2) |
| Africa | 53 | 28 (52.8) | 22 (45.8) |
| World region of senior author¶ | |||
| N America | 3,639 | 1,368 (39.1) | 1,026 (28.9) |
| Europe | 2,081 | 857 (42.6) | 575 (28.6) |
| Aust/NZ/Oceania | 242 | 113 (48.5) | 79 (33.2) |
| Cent/S Am, Carib | 141 | 53 (39.8) | 40 (29.4) |
| Asia | 1,803 | 605 (37.0) | 429 (27.0) |
| Africa | 49 | 26 (54.2) | 23 (46.9) |
| COVID-19–related‖ | 839 | 259 (32.4) | 212 (27.3) |
| Timing of submission** | |||
| Pre-COVID-19 era (1/1/18–3/10/20) | 5,168 | 2,041 (41.6) | 1,371 (28.0) |
| COVID-19 era (3/11/20–12/31/20) | 3,164 | 1,116 (37.0) | 856 (28.8) |
| Final decision†† | |||
| Provisional accept | 1,009 | 385 (39.6) | 262 (26.5) |
| Reject after review | 2,650 | 1,071 (42.5) | 706 (27.9) |
| Reject no review | 4,402 | 1,591 (38.2) | 1,172 (28.6) |
Definition of abbreviations: AJRCCM = American Journal of Respiratory and Critical Care Medicine; AJRCMB = American Journal of Respiratory Cell and Molecular Biology; AnnalsATS = Annals of the American Thoracic Society; Aust/NZ/Oceania = Australia/New Zealand/Oceania; Cent/S Am, Carib = Central America/South America/Caribbean; COVID-19 = coronavirus disease; hlth = health; infn = infection; IQR = interquartile range; Microbio = microbiology; mol = molecular; N America = North America.
Chi-square testing for categorial and Mann-Whitney U testing for continuous variables.
Unable to determine author sex of 412 (4.9%) of first authors and 456 (5.5%) of senior authors.
Missing data for subject category in 182 (2.2%) of cohort; P < 0.001 for subject category by first and senior author sex.
Missing data for first author world region in 227 (2.7%) of cohort; P < 0.001 for first author world region by first author sex and P = 0.023 by senior author sex.
Missing data for senior author world region in 377 (4.5%) of cohort; P < 0.001 for senior author world region by first author sex and P = 0.027 by senior author sex.
P < 0.001 for COVID-19–related by first author sex.
P < 0.001 for timing of submission by first author sex.
Missing data for final decision in 271 (3.3%) of cohort; P = 0.002 for final decision by first author sex.
Using an interrupted time series approach, we found no step up or down in the proportion of female first or senior authors of submitted non–COVID-19 research manuscripts during the COVID-19 era (regression coefficient [95% confidence interval (CI)] for submission during COVID-19 era, first author, −0.03 [−0.10, 0.03]; P = 0.35; senior author, 0.00 [−0.06, 0.06]; P = 0.89) (Figure 2). Similarly, during the pandemic, the proportion of female first and senior authors of submitted COVID-19 research manuscripts did not vary significantly over time or by world region (Figure 3). However, there were significant geographic differences in authorship sex for non–COVID-19 research manuscripts (Figure E3). Specifically, Africa had the highest proportion of female first and senior authors (first, 54%; P < 0.001; senior, 47%; P = 0.014). South America (35%) and Asia (37%) had the fewest female first authors; South America, Asia, Europe, and North America (26–29%) had the fewest female senior authors.
Figure 2.
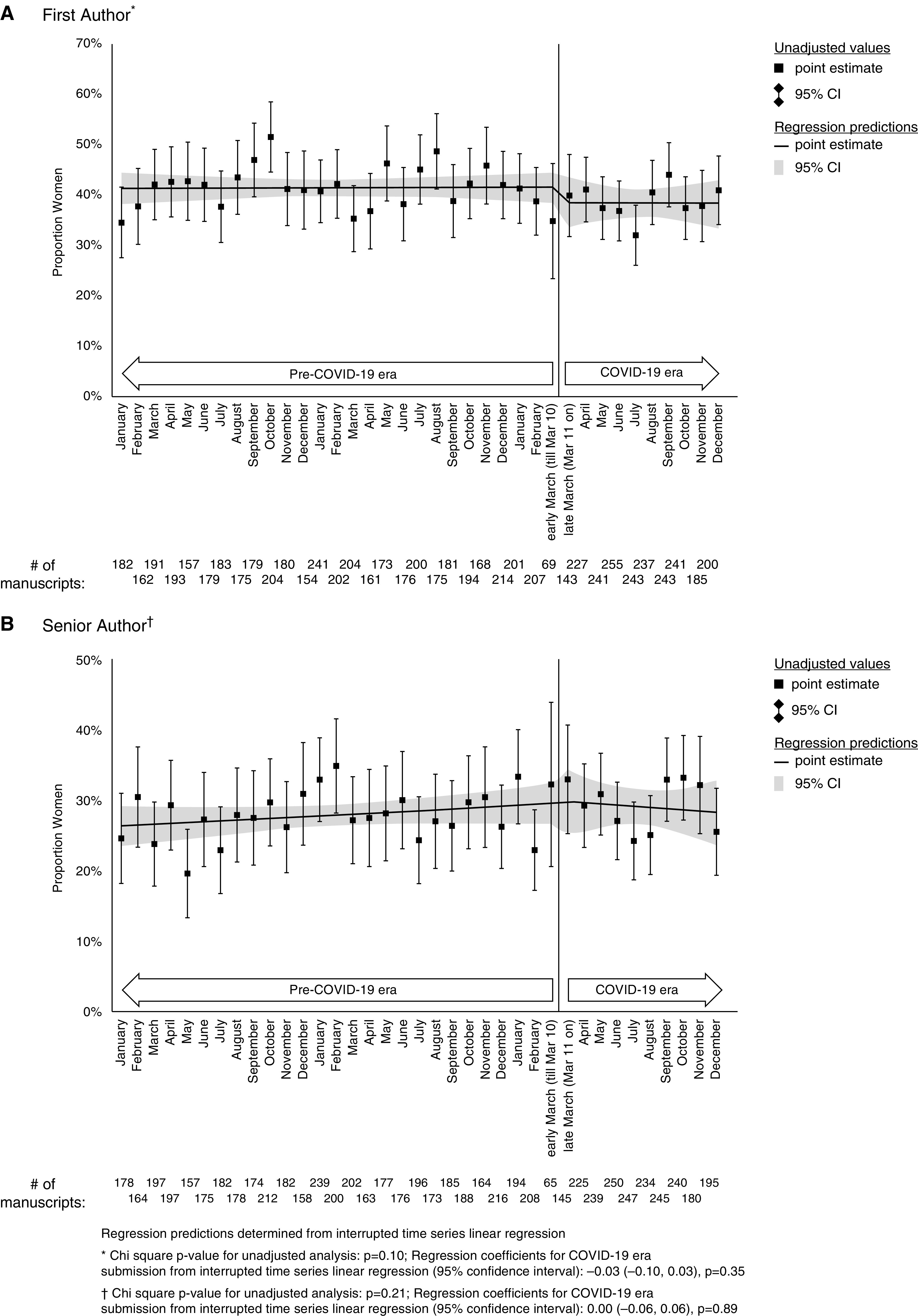
The proportion of women authors of non–COVID-19 manuscripts, stratified by submission month. (A) First author. (B) Senior author. Regression predictions determined from interrupted time series linear regression. *Chi-square P value for unadjusted analysis: P = 0.10. Regression coefficients for COVID-19 era submission from interrupted time series linear regression (95% confidence interval): −0.03 (−0.10, 0.03); P = 0.35. †Chi-square P value for unadjusted analysis: P = 0.21; regression coefficients for COVID-19 era submission from interrupted time series linear regression (95% confidence interval): 0.00 (−0.06, 0.06), P = 0.89. CI = confidence interval; COVID-19 = coronavirus disease.
Figure 3.
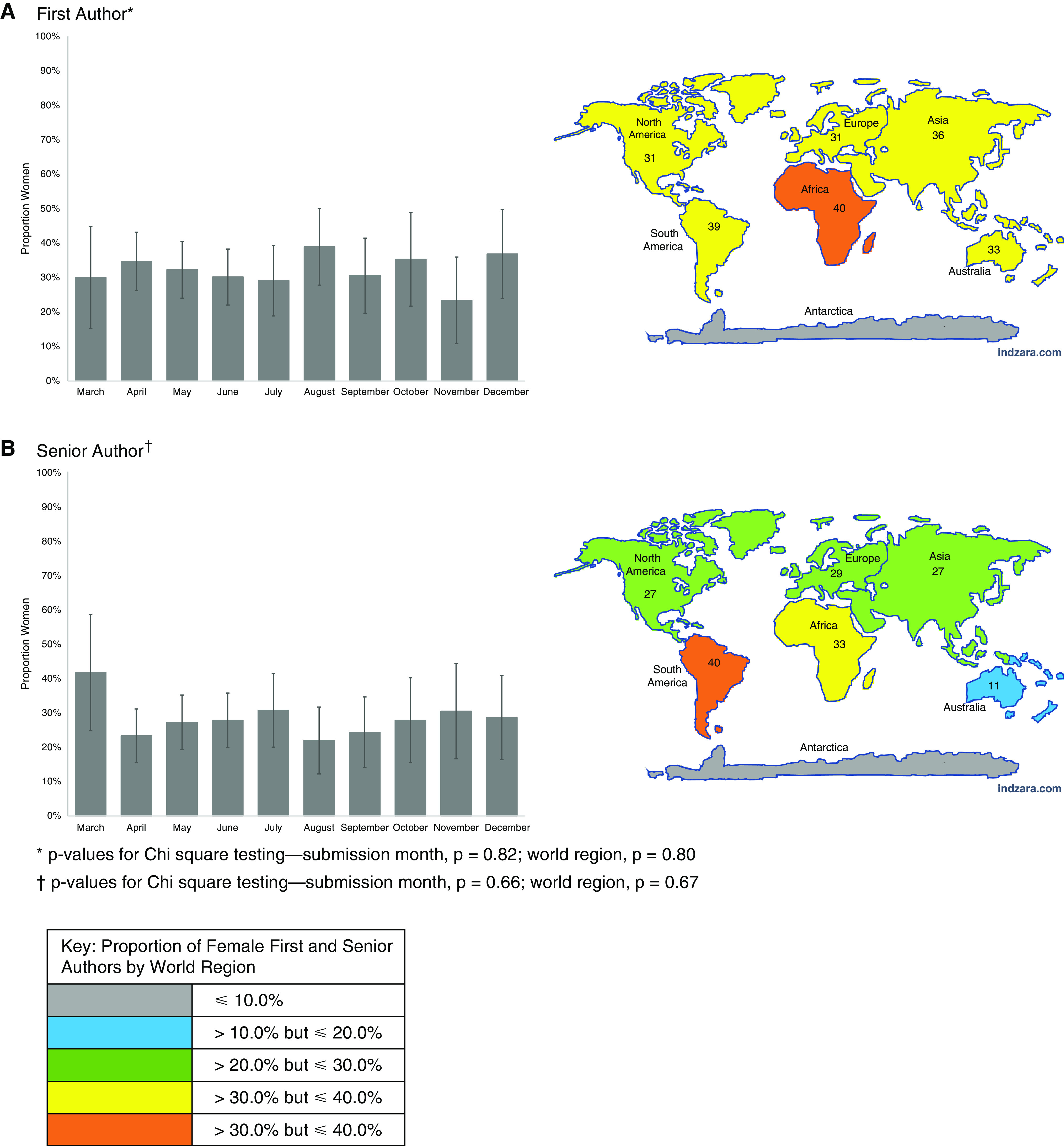
Proportion of women authors of COVID-19 manuscripts, stratified by submission month and author world region. *P values for chi-square testing—submission month, P = 0.82; world region, P = 0.80. †P values for chi-square testing—submission month, P = 0.66; world region, P = 0.67. COVID-19 = coronavirus disease.
Non–COVID-19 Manuscript Acceptance Rates
Despite the increase in submission rates of all research manuscripts during the COVID-19 era, the number of accepted manuscripts per month (both COVID-19 and non–COVID-19) decreased (median [interquartile range], 28 [25–36] before COVID-19 to 25 [4–29] during the COVID-19 era; P < 0.001). Among non–COVID-19 manuscripts, we found that 14.0% with male first authors and 13.5% with female first authors were accepted for publication. Similarly, 14.4% of non–COVID-19 manuscripts with male senior authors were accepted for publication compared with 13.2% of non–COVID-19 manuscripts with female senior authors (Table E1). In multivariable analyses adjusted for author world region and journal as well as subject category, we found that the pandemic was associated with reduced odds of acceptance of non–COVID-19 manuscripts, regardless of first or senior author sex (first author analysis, 0.46 [0.36, 0.59]; P < 0.001; senior author analysis, 0.46 [0.37, 0.57]; P < 0.001) (Table 2). There was no association between first author sex and the odds of acceptance for non–COVID-19 research manuscripts. However, female senior authorship was associated with lower odds of acceptance than male senior authorship (adjusted odds ratio [95% CI], 0.84 [0.71, 0.99]; P = 0.039), with an absolute difference in acceptance rate of 1.7% (P = 0.034). In addition, the interaction term for authorship sex and COVID-19 era submission for non–COVID-19 manuscripts was not significant (Table E2).
Table 2.
Association of author sex and COVID-19 era with provisional acceptance
| Cohort | Date Range | Exposure Variables* | First Author Sex Analysis |
Senior Author Sex Analysis |
||
|---|---|---|---|---|---|---|
| OR (95% CI) | P Value | OR (95% CI) | P Value | |||
| Non–COVID-19 manuscripts† | 1/1/18–12/31/20 | Author female | 0.91 (0.78–1.06) | 0.23 | 0.84 (0.71–0.99) | 0.039 |
| Non–COVID-19 manuscripts‡ | Pre-COVID-19 era (1/1/18–3/10/20) vs. COVID-19 era (3/11/20–12/31/20) | Author female | 0.90 (0.76–1.07) | 0.24 | 0.84 (0.70–1.01) | 0.07 |
| COVID-19 era | 0.46 (0.36–0.59) | <0.001 | 0.46 (0.37–0.57) | <0.001 | ||
| Author female × COVID-19 era | 0.93 (0.63–1.38) | 0.73 | 0.97 (0.63–1.49) | 0.89 | ||
| COVID-19 manuscripts§ | 3/11/20–12/31/20 | Author female | 0.91 (0.36–2.33) | 0.85 | 1.39 (0.53–3.61) | 0.50 |
Definition of abbreviations: CI = confidence interval; COVID-19 = coronavirus disease; OR = odds ratio.
Models also adjusted for world region of author and journal.
For first author sex analysis, Hosmer-Lemeshow testing for goodness of fit P = 0.23 and area under receiver operating characteristic curve = 0.71; for senior author sex analysis, Hosmer-Lemeshow testing for goodness of fit P = 0.09 and area under receiver operating characteristic curve = 0.71.
For first author sex analysis, Hosmer-Lemeshow testing for goodness of fit P = 0.044 and area under receiver operating characteristic curve = 0.72; for senior author sex analysis, Hosmer-Lemeshow testing for goodness of fit P = 0.08 and area under receiver operating characteristic curve = 0.73.
For first author sex analysis, Hosmer-Lemeshow testing for goodness of fit P = 0.71 and area under receiver operating characteristic curve = 0.83; for senior author sex analysis, Hosmer-Lemeshow testing for goodness of fit P = 0.28 and area under receiver operating characteristic curve = 0.83.
COVID-19 Manuscript Acceptance Rates
Among COVID-19 research manuscripts (all published during the COVID-19 era), we found that 3.2% with male first authors and 2.8% with female first authors were accepted for publication compared with 3.1% with male senior authors and 3.4% with female senior authors (Table E3). We found no association between first or senior author sex and odds of acceptance of COVID-19 research manuscripts.
Sensitivity Analyses
Across all sensitivity cohorts, we found that the COVID-19 era was associated with lower odds of acceptance of non–COVID-19 manuscripts (Table E4). Notably, when all non–COVID-19 submission types (not just original research) were considered, manuscripts with female first, senior, or corresponding authors had lower odds of acceptance (female first author, 0.82 [0.75, 0.90], P < 0.001; female senior author, 0.86 [0.79, 0.90]; P = 0.006; female corresponding author, 0.82 [0.76, 0.88]; P < 0.001).
Discussion
In this study examining the relationship between the COVID-19 pandemic and manuscript submission and acceptance rates among select U.S. pulmonary and critical care journals between 2018 and 2020, we identified several important findings. First, we found that non–COVID-19 research manuscripts were approximately 50% less likely to be accepted during the COVID-19 era, regardless of author sex. Second, women represented less than 40% of first authors and 30% of senior authors of both non–COVID-19– and COVID-19–focused original research submissions, without significant changes observed during the COVID-19 era. Third, among non–COVID-19 research manuscripts, female senior authorship was associated with reduced odds of acceptance compared with manuscripts with male senior authors. These results provide important insights into the potential influence of the pandemic on both sex disparities in academic medicine and on the publication of high-quality research focused on topics unrelated to COVID-19.
The COVID-19 pandemic has led to unprecedented increases in the volume of COVID-19–related research submitted to journals over the past 18 months (22, 34). Interestingly, we found that the pandemic has been associated with decreased acceptance of non–COVID-19–related research among pulmonary and critical care journals, regardless of first or senior author sex. In the face of limited journal space during a public health emergency, journal editors may have shifted their focus to include more COVID-19–related research at the expense of non–COVID-19–related topics. Alternatively, the observed decrease in odds of acceptance of non–COVID-19 manuscripts may also result from differences in the quality of submissions over time or changes in the review and/or editorial processes. Regardless of the mechanism for these findings, it is important for clinicians, scientists, journal editors, policy makers, and academic institutions alike to be aware of the COVID-19 pandemic’s collateral impact on non–COVID-19 research as well, particularly when assessing publication records as a measure for promotion.
In addition, our findings associating author sex with submissions and acceptance rates add to a growing body of literature related to sex disparities in academic publishing. For example, one recent study estimated the percentage of female first authors publishing original research in six high-impact journals to be 37% (35). Similarly, another study found that among critical care literature published between 2008 and 2018, women comprised 31% of first authors and 20% of senior authors (11), despite representing approximately one-third of the critical care workforce worldwide (8). Our study builds upon the findings that, over the past decade, the proportion of manuscripts with female first or senior authors in the field of pulmonary and critical care medicine may have improved slightly, although women still comprise a minority of authors overall.
Several studies published during the early phase of the pandemic demonstrated decreased academic productivity among female physicians and scientists (7, 36). For example, in a recent study published in BMJ, Gayet-Ageron and colleagues evaluated sex disparities in manuscripts submitted to 11 European journals that are part of the BMJ publishing group (including two general medicine journals and nine specialty journals, one of which is focused on pulmonary and critical care) (36). The authors found that women were less well represented in first, senior, and corresponding authorship positions on COVID-19 research manuscripts compared with submissions before the pandemic; however, these sex disparities were most prominent early in the pandemic and narrowed over time (36). Because women take on significantly greater domestic and childcare responsibilities than men do (37), it is not surprising that their academic productivity may have been disproportionately impacted by the pandemic, particularly early on, when stay-at-home orders and school closures were widespread (1). However, in our study focused on North American pulmonary and critical care journals, we found no difference in the proportion of female first or senior authors of non–COVID-19 research manuscripts during the COVID-19 era. These disparate findings raise the possibility that the pandemic differentially affected female physicians and scientists, depending on a variety of factors, including geographic region and/or clinical specialty. For example, pulmonary and critical care physicians have been at the front line caring for hospitalized patients with COVID-19; as such, they had no choice but to find alternative childcare options during school closures, which may have enabled them to continue their academic endeavors simultaneously.
Encouragingly, we found no difference in the odds of acceptance for submitted manuscripts with female versus male first authors. However, among non–COVID-19 manuscripts, we found that those with female senior authors were 15% less likely to be accepted than manuscripts with male senior authors, with an absolute difference of 1.7%. In other words, our findings suggest that for every 1,000 submitted manuscripts with women as senior authors, 17 will be rejected, which would not have been the case if those authors had been men. Similarly, sensitivity analyses including all submitted non–COVID-19 manuscripts (e.g., not limited to original research) showed that manuscripts authored by female first, senior, and corresponding authors were less likely to be accepted than similar manuscripts authored by men. Although a 15% difference in odds of acceptance may not appear substantial, there is no plausible biological explanation for why manuscripts with female senior authors would be accepted less frequently than those with male senior authors. It is also important to consider the cumulative effect of these small differences on women over time, who already lag behind men in reaching senior positions within academic medicine (38, 39). Although these results should be interpreted cautiously, given the limitations of the Genderize database and the small absolute difference observed, it is worthwhile to explore potential mechanisms for these findings.
First, because our findings are from four different journals with distinct editorial teams, they may reflect widespread conscious or unconscious bias during the peer review process rather than discrimination by a given journal. Unconscious bias is an implicit attitude, stereotype, motivation, or assumption that can occur without one’s knowledge, control, or intention (40). Gender bias can occur when women are seen as less qualified than men, despite evidence to the contrary (40, 41). Although academic publishing is purportedly gender neutral, there is growing evidence that the process is decidedly gendered (41–43). For example, most peer reviewers and editors at academic journals are men, despite growing numbers of women in the research workforce (44–47). Women also receive less research funding in science and medicine (41, 48), leading to fewer publications and less visibility as researchers and authors (47). The lack of visibility among women in senior author positions may consciously or unconsciously influence decisions made during the peer review and editorial processes and therefore represents a plausible explanation for our findings. Ultimately, this cycle may lead to fewer invitations as authors, peer reviewers, and editors, together with fewer citations of their own work, further reducing future funding success (19, 20, 41, 48, 49). Potential interventions include real-time data collection that will allow journals to track, analyze, and publish gender statistics for submissions and acceptance (50); implementation of deliberate strategies to improve women’s participation on editorial boards and in the peer review process; and establishment of a double-blind review process to help reduce the impact of both conscious and unconscious bias within academic publishing (41).
Other potential mechanisms for our findings include the possibility that men and women preferentially conduct different types of research (e.g., clinical vs. bench science, observational studies vs. clinical trials) that vary in acceptance rates, depending on journals’ priorities. Furthermore, women remain underrepresented in scholarly activities within academic medicine, particularly those that require invitations for participation (e.g., speaking at and/or chairing conferences, participating in guideline panels and editorial boards) (9, 10, 12–14, 51, 52). Because a substantial number of non–original research manuscripts published by leading journals are by invitation only, it stands to reason that women may be invited to publish these types of manuscripts less frequently than their male colleagues. In addition, the “confidence gap” between men and women may contribute to a reluctance of female scientists to submit editorial or perspective pieces to high-impact journals (11, 53), further contributing to existing sex disparities in academic medicine. Similarly, the relative “overconfidence” of men compared with women may lead reviewers to judge manuscripts submitted by women less favorably, particularly when they include less objective findings such as those in nonoriginal research. Conscious or unconscious bias among peer reviewers or editors who invite reviewers and issue accept or reject decisions on manuscripts may also represent a potential mechanism for sex-based disparities in manuscript acceptance rates.
Limitations
Our study has several limitations. First, we included only four North American pulmonary and critical care journals, which limits the generalizability of our findings. Second, the use of author first name alone to identify author sex is imperfect, and there remains a risk of misclassification of author sex in the Genderize database or manuscripts pertaining to COVID-19. Moreover, we could not track individual authors and account for nonindependence of observations in our analysis. Similarly, we could not ensure that individual manuscripts were not submitted to multiple journals and thus could have been included in our analysis more than once; however, our results were robust to a sensitivity analysis excluding transfers from AJRCCM. Third, world region was only one way to categorize country of author residence. Fourth, residual confounding likely exists despite our adjustment for potential confounders. In addition, because our study considered only original research papers, it is possible that a shift to using research letters for rapid turnaround occurred during the COVID-19 era, which may have impacted our results. The inability to distinguish research letters from letters to the editor in all journals precluded further evaluation of this issue. Fifth, our analysis of acceptance rates relied on the untestable assumption that manuscript assessors (reviewers and editors) remained stable over time. In addition, the true denominator of women pursuing careers as physicians and/or scientists in the field of pulmonary and/or critical care medicine is unknown. Finally, it is possible that the impact of COVID-19 on female physicians and scientists may become more pronounced over time, particularly because the pandemic has extended well beyond our study period ending in December 2020.
Conclusions
Women comprise a minority of first and senior authors among research manuscripts submitted to leading pulmonary and critical care journals; this proportion was not significantly influenced by the COVID-19 pandemic. Our results suggest that female senior authorship of non–COVID-19 research manuscripts was associated with decreased odds of acceptance compared with manuscripts with male senior authors, although no difference in acceptance was seen by first author sex. Importantly, non–COVID-19 research manuscripts were nearly 50% less likely to be accepted during the COVID-19 era, regardless of author sex. Many factors—professional and extraprofessional, external and internal to the authors, intentional and unintentional—likely contribute to a higher percentage of submissions being authored by men than by women. Journals may need to consider strategies to reduce disparities, and academic institutions may need to factor our findings, including lower acceptance rates for non-COVID-19 manuscripts, into promotion decisions.
Acknowledgments
Acknowledgment
The authors acknowledge the help and support of staff and leadership at the American Thoracic Society and American College of Chest Physicians in making these data available.
Footnotes
Supported by resources from the Center to Involve Veteran Involvement in Care, Veterans Affairs Portland Health Care System, Portland, Oregon (C.G.S., K.C.V.) and by funding from the University of Miami Hospitals and Clinics Data Analytics Research Team (H.B.G.).
Author Contributions: H.B.G., K.C.V., and C.G.S. contributed to the conception and design of this study. H.B.G., C.G.S., and D.O. contributed to data acquisition. H.B.G. and D.O. contributed to analysis of data. H.B.G., K.C.V., C.G.S., and C.R.C. contributed to interpretation of the data. All authors contributed to drafting the article for important intellectual content and provided final approval of the version to be published.
This article has a data supplement, which is accessible from this issue’s table of contents at www.atsjournals.org.
Author disclosures are available with the text of this article at www.atsjournals.org.
References
- 1. Cardel MI, Dean N, Montoya-Williams D. Preventing a secondary epidemic of lost early career scientists; effects of COVID-19 pandemic on women with children. Ann Am Thorac Soc . 2020;17:1366–1370. doi: 10.1513/AnnalsATS.202006-589IP. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Godlee F. Covid-19: why we still need more women in academia. BMJ . 2020;371:m4161. [Google Scholar]
- 3. Delaney RK, Locke A, Pershing ML, Geist C, Clouse E, Precourt Debbink M, et al. Experiences of a health system’s faculty, staff, and trainees’ career development, work culture, and childcare needs during the COVID-19 pandemic. JAMA Netw Open . 2021;4:e213997. doi: 10.1001/jamanetworkopen.2021.3997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Myers KR, Tham WY, Yin Y, Cohodes N, Thursby JG, Thursby MC, et al. Unequal effects of the COVID-19 pandemic on scientists. Nat Hum Behav . 2020;4:880–883. doi: 10.1038/s41562-020-0921-y. [DOI] [PubMed] [Google Scholar]
- 5. McCormick CM. Disparities in the toll of the COVID-19 pandemic on publishing: evidence from submissions to Hormones and Behavior. Horm Behav . 2020;124:104814. doi: 10.1016/j.yhbeh.2020.104814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Bell ML, Fong KC. Gender differences in first and corresponding authorship in public health research submissions during the COVID-19 pandemic. Am J Public Health . 2021;111:159–163. doi: 10.2105/AJPH.2020.305975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Andersen JP, Nielsen MW, Simone NL, Lewiss RE, Jagsi R. COVID-19 medical papers have fewer women first authors than expected. eLife . 2020;9:e58807. doi: 10.7554/eLife.58807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Venkatesh B, Mehta S, Angus DC, Finfer S, Machado FR, Marshall J, et al. Women in Intensive Care study: a preliminary assessment of international data on female representation in the ICU physician workforce, leadership and academic positions. Crit Care . 2018;22:211. doi: 10.1186/s13054-018-2139-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Mehta S, Burns KEA, Machado FR, Fox-Robichaud AE, Cook DJ, Calfee CS, et al. Gender parity in critical care medicine. Am J Respir Crit Care Med . 2017;196:425–429. doi: 10.1164/rccm.201701-0076CP. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Mehta S, Rose L, Cook D, Herridge M, Owais S, Metaxa V. The speaker gender gap at critical care conferences. Crit Care Med . 2018;46:991–996. doi: 10.1097/CCM.0000000000003114. [DOI] [PubMed] [Google Scholar]
- 11. Vranas KC, Ouyang D, Lin AL, Slatore CG, Sullivan DR, Kerlin MP, et al. Gender differences in authorship of critical care literature. Am J Respir Crit Care Med . 2020;201:840–847. doi: 10.1164/rccm.201910-1957OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Morton MJ, Sonnad SS. Women on professional society and journal editorial boards. J Natl Med Assoc . 2007;99:764–771. [PMC free article] [PubMed] [Google Scholar]
- 13. Amrein K, Langmann A, Fahrleitner-Pammer A, Pieber TR, Zollner-Schwetz I. Women underrepresented on editorial boards of 60 major medical journals. Gend Med . 2011;8:378–387. doi: 10.1016/j.genm.2011.10.007. [DOI] [PubMed] [Google Scholar]
- 14. Erren TC, Gross JV, Shaw DM, Selle B. Representation of women as authors, reviewers, editors in chief, and editorial board members at 6 general medical journals in 2010 and 2011. JAMA Int Med . 2014;174:633–635. doi: 10.1001/jamainternmed.2013.14760. [DOI] [PubMed] [Google Scholar]
- 15. Wehner MR, Naik HB, Linos E. Gender equity in clinical dermatology—reason for optimism. JAMA Dermatol . 2019;155:284–286. doi: 10.1001/jamadermatol.2018.5283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Wehner MR, Nead KT, Linos K, Linos E. Plenty of moustaches but not enough women: cross sectional study of medical leaders. BMJ . 2015;351:h6311. doi: 10.1136/bmj.h6311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Reed DA, Enders F, Lindor R, McClees M, Lindor KD. Gender differences in academic productivity and leadership appointments of physicians throughout academic careers. Acad Med . 2011;86:43–47. doi: 10.1097/ACM.0b013e3181ff9ff2. [DOI] [PubMed] [Google Scholar]
- 18. Merman E, Pincus D, Bell C, Goldberg N, Luca S, Jakab M, et al. Differences in clinical practice guideline authorship by gender. Lancet . 2018;392:1626–1628. doi: 10.1016/S0140-6736(18)32268-2. [DOI] [PubMed] [Google Scholar]
- 19. Burns KEA, Straus SE, Liu K, Rizvi L, Guyatt G. Gender differences in grant and personnel award funding rates at the Canadian Institutes of Health Research based on research content area: a retrospective analysis. PLoS Med . 2019;16:e1002935. doi: 10.1371/journal.pmed.1002935. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Goldstone K, Edgley C, Mehta S, Leslie K. Peer review for the Canadian Journal of Anesthesia in 2016 and 2017: a retrospective analysis by reviewer and author gender. Can J Anaesth . 2020;67:336–342. doi: 10.1007/s12630-019-01533-2. [DOI] [PubMed] [Google Scholar]
- 21. Else H. How a torrent of COVID science changed research publishing — in seven charts. Nature . 2020;588:553. doi: 10.1038/d41586-020-03564-y. [DOI] [PubMed] [Google Scholar]
- 22. Bauchner H, Fontanarosa PB, Golub RM. Editorial evaluation and peer review during a pandemic: how journals maintain standards. JAMA . 2020;324:453–454. doi: 10.1001/jama.2020.11764. [DOI] [PubMed] [Google Scholar]
- 23. Giustini AJ, Schroeder AR, Axelrod DM. Trends in views of articles published in 3 leading medical journals during the COVID-19 pandemic. JAMA Netw Open . 2021;4:e216459. doi: 10.1001/jamanetworkopen.2021.6459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.American Thoracic Society https://www.atsjournals.org/page/annalsats/instructions.
- 25.American Thoracic Society. https://www.atsjournals.org/page/ajrccm/instructions
- 26.American Thoracic Society. https://www.atsjournals.org/page/ajrcmb/instructions
- 27.World Health Organization. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports
- 28.Demografix ApS. https://genderize.io
- 29. Santamaría L, Mihaljević H. Comparison and benchmark of name-to-gender inference services. PeerJ Comput Sci . 2018;4:e156. doi: 10.7717/peerj-cs.156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Blevins C, Mullen L.http://www.digitalhumanities.org/dhq/vol/9/3/000223/000223.html.
- 31.American Thoracic Society. https://www.atsjournals.org/page/AJRCCM/subject_codes
- 32.United Nations Sustainable Development Goals. https://unstats.un.org/sdgs/indicators/regional-groups
- 33. Bernal JL, Cummins S, Gasparrini A. Interrupted time series regression for the evaluation of public health interventions: a tutorial. Int J Epidemiol . 2017;46:348–355. doi: 10.1093/ije/dyw098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Lapostolle F, Petrovic T, Goix L, Adnet F. Impact of COVID-19 pandemic on non-COVID-19 publications. Resuscitation . 2021;162:102–103. doi: 10.1016/j.resuscitation.2021.02.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Filardo G, da Graca B, Sass DM, Pollock BD, Smith EB, Martinez MA. Trends and comparison of female first authorship in high impact medical journals: observational study (1994–2014) BMJ . 2016;352:i847. doi: 10.1136/bmj.i847. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Gayet-Ageron A, Ben Messaoud K, Richards M, Schroter S. Female authorship of covid-19 research in manuscripts submitted to 11 biomedical journals: cross sectional study. BMJ . 2021;375:n2288. doi: 10.1136/bmj.n2288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Jolly S, Griffith KA, DeCastro R, Stewart A, Ubel P, Jagsi R. Gender differences in time spent on parenting and domestic responsibilities by high-achieving young physician-researchers. Ann Intern Med . 2014;160:344–353. doi: 10.7326/M13-0974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Association of American Medical Colleges https://www.aamc.org/data-reports/faculty-institutions/data/state-womenacademic-medicine-pipeline-and-pathways-leadership-2015-2016.
- 39. Carr PL, Gunn CM, Kaplan SA, Raj A, Freund KM. Inadequate progress for women in academic medicine: findings from the National Faculty Study. J Womens Health (Larchmt) . 2015;24:190–199. doi: 10.1089/jwh.2014.4848. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.National Institutes of Health https://www.niaid.nih.gov/grants-contracts/unconscious-bias-peer-review.
- 41. Lundine J, Bourgeault IL, Clark J, Heidari S, Balabanova D. The gendered system of academic publishing. Lancet . 2018;391:1754–1756. doi: 10.1016/S0140-6736(18)30950-4. [DOI] [PubMed] [Google Scholar]
- 42. Okike K, Hug KT, Kocher MS, Leopold SS. Single-blind vs double-blind peer review in the setting of author prestige. JAMA . 2016;316:1315–1316. doi: 10.1001/jama.2016.11014. [DOI] [PubMed] [Google Scholar]
- 43. Sheltzer JM, Smith JC. Elite male faculty in the life sciences employ fewer women. Proc Natl Acad Sci USA . 2014;111:10107–10112. doi: 10.1073/pnas.1403334111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Lerback J, Hanson B. Journals invite too few women to referee. Nature . 2017;541:455–457. doi: 10.1038/541455a. [DOI] [PubMed] [Google Scholar]
- 45. Rochon PA, Davidoff F, Levinson W. Women in academic medicine leadership: has anything changed in 25 years? Acad Med . 2016;91:1053–1056. doi: 10.1097/ACM.0000000000001281. [DOI] [PubMed] [Google Scholar]
- 46. Wing DA, Benner RS, Petersen R, Newcomb R, Scott JR. Differences in editorial board reviewer behavior based on gender. J Womens Health (Larchmt) . 2010;19:1919–1923. doi: 10.1089/jwh.2009.1904. [DOI] [PubMed] [Google Scholar]
- 47. Nature’s sexism [editorial] Nature . 2012;491:495. [PubMed] [Google Scholar]
- 48. Kaatz A, Gutierrez B, Carnes M. Threats to objectivity in peer review: the case of gender. Trends Pharmacol Sci . 2014;35:371–373. doi: 10.1016/j.tips.2014.06.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Chatterjee P, Werner RM. Gender disparity in citations in high-impact journal articles. JAMA Netw Open . 2021;4:e2114509. doi: 10.1001/jamanetworkopen.2021.14509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Mehta S, Ahluwalia N, Heybati K, Burns KEA, Owais S, Cook DJ, Canadian Critical Care Trials Group Diversity of authors of publications from the Canadian Critical Care Trials Group. Crit Care Med . 2022;50:535–542. doi: 10.1097/CCM.0000000000005284. [DOI] [PubMed] [Google Scholar]
- 51. Metaxa V. Is this (still) a man’s world? Crit Care . 2013;17:112. doi: 10.1186/cc11859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Weinacker A, Stapleton RD. Still a man’s world, but why? Crit Care . 2013;17:113. doi: 10.1186/cc11915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Berg J. Looking inward at gender issues. Science . 2017;355:329. doi: 10.1126/science.aam8109. [DOI] [PubMed] [Google Scholar]