

Abstract
Background:
Higher risk of dementia among racial/ethnic minorities compared to White populations in the U.S. has been attributed to life-course exposures to adverse conditions such as lower educational attainment, but most studies have not considered additional disparities in education quality. We sought to determine the extent to which disparities in dementia would be reduced had different racial groups received the same quality of education, with no change to present disparities in educational attainment.
Methods:
We conducted a literature review to assess whether and how measures of educational attainment and quality are utilized in the development of norms for standard cognitive screening measures. In a separate search of the literature, we identified estimates of relationships between race, education quality and dementia; and calculated the adjusted association between race and dementia had education quality been equalized between Black and White participants.
Results:
Most norms for cognitive measures included educational attainment, but few addressed quality. Our search identified relevant parameter estimates: 44.3% of Black participants and 10.5% of White participants had “limited literacy” (<9th grade reading level, a potential marker of poor education quality), which was associated with a 53% greater hazard of dementia compared with “adequate literacy” (≥ 9th grade reading level) after adjusting for educational attainment. Applying these parameters to a hazard ratio of 1.37 (95%CI: 1.12,1.67) for the risk of dementia comparing Black to White participants, we obtained an adjusted hazard ratio of 1.17 (0.96,1.43), a 54% reduction.
Discussion:
Present studies are limited in their consideration of education quality. Our work using available measures from the literature suggests that if education quality were equalized across groups by race, without changing disparities in attainment, racial disparities in dementia would be reduced by about half. Future work should seek to consistently incorporate education quality in order to better understand the sources of disparities.
Keywords: Cognitive aging, Dementia, Education, Minority health, Social determinants of health
1. Introduction
Higher risk of mild cognitive impairment (MCI) and dementia among racial/ethnic minority populations as compared to non-Hispanic White populations in the United States (U.S.) has been well-documented in the literature (Weuve et al., 2018; Avila et al., 2019). This relationship may be partially explained by disparities in educational experiences, one of the most consistent and robust predictors of cognitive and physical health (Cohen and Syme, 2013; Glymour and Manly, 2008; Hamad et al., 2018). Education is hypothesized to impact cognitive health through improved labor market opportunities, knowledge and skill building, healthy behaviors via school-based resources, and access to advantaged social networks over the lifecourse (Glymour and Manly, 2018). In addition to “downstream” consequences such as fewer occupational opportunities (Fujishiro et al., 2020) and a lack of access to medical care (Zajacova and Lawrence, 2018), fewer years of education is also associated with worse performance on cognitive testing (Bohnstedt et al., 1994; Milani et al., 2019).
Racial/ethnic minority populations have lower levels of educational attainment on average compared to White populations (Everett et al., 2011) and experience substantial barriers in obtaining high-quality education. This can be linked to the lasting impact of policies and practices that collectively uphold structural racism, including government-sanctioned residential segregation and disinvestment in schools (among other public services) particularly in historically redlined or legally segregated areas in the U.S. (Glymour and Manly, 2008; Bailey et al., 2017, 2021) Moreover, racial residential segregation itself—rooted in racist housing and education policies—is associated with worse cognition in later life, potentially functioning through chronic stress and/or depression induced by repeated exposure to adverse social and environmental experiences such as interpersonal discrimination (Barnes et al., 2012; Pohl et al., 2021). Allostatic load due to “toxic stress” from experiencing discrimination based on race has been found to be associated with greater decline in late-life memory trajectory (Zahodne et al., 2019), and any benefit to cognitive reserve from obtaining education was nearly absent among those who experience everyday discrimination (Nkwata et al., 2022).
Returning to the discussion of racial disparities in the educational experience, studies have shown that White individuals experience greater benefits from educational attainment compared to Black individuals in terms of all-cause mortality (Bartle-Haring and Whiting, 2022) and self-reported health (Whiting and Bartle-Haring, 2022). This points to racial disparities even after obtaining comparable “levels” or years of formal education and, potentially, disparities in the quality of education received. Research further suggests that higher education quality is associated with better cognitive functioning and cognitive trajectories (Dotson et al., 2009; Sisco et al., 2015); previous studies that have adjusted for literacy, a potential indicator of early education quality, found attenuated differences in late-life cognition comparing racial/ethnic minorities to White older adults. (Manly, Jacobs, Touradji, Small, Stern) Thus, worse late-life cognition among minoritized populations reflect “mutually reinforcing systems” (Bailey et al., 2021) including structural barriers to obtaining education (particularly high-quality education), downstream consequences of low educational attainment or poor education quality related to cognitive reserve and adult socioeconomic opportunities, as well as the deleterious impact of experiencing discrimination due to race, among other diverging mid-life experiences (Garcia et al., 2018). In the extant literature, however, many studies of cognition adjust for educational attainment (Kennedy et al., 2014) or use education-standardized norms (Crum et al., 1993; Rossetti et al., 2011) to account for educational differences between racial/ethnic groups, while few studies additionally take into account the quality of education. This may leave unexamined many considerable mechanisms via which education influences racial/ethnic disparities in dementia.
Our study has two complementary aims. First, as we are aware of no other comprehensive review of how research studies of race and cognition operationalize education, we aim to document how education is operationalized in studies that developed norms for standard cognitive screening measures among older adults and specifically whether education quality in addition to attainment is considered. We hypothesize that few studies of race and cognition would account for education quality, thus motivating a formal sensitivity analysis to assess the potential impact of unmeasured education quality on observed differences by race in dementia risk. In our second aim, we will examine the extent to which disparities in dementia incidence would be eliminated if education quality were equalized across racial groups, while holding constant educational attainment. We hypothesize that equalizing the quality of education, without changing educational attainment, would potentially eliminate a significant proportion of the racial disparities in dementia risk.
2. Methods
To achieve our two complementary aims, we 1) reviewed the literature to describe how educational attainment and education quality are operationalized in studies of diverse older adults in the U.S. that developed normative data for cognition; then 2) identified relevant parameter estimates from the literature for use in a formal sensitivity analysis to evaluate the role of education quality in explaining the relationship between race and dementia risk.
2.1. Literature review
For our literature review, we searched PubMed and PsychINFO for studies that developed norms for standard cognitive screening measures in diverse populations of older adults in the U.S. using the search terms in Table 1. We included studies published before December 31, 2021 with participants who were community-dwelling, over the age of 45, and from at least two racial or ethnic groups. Among the included studies, we extracted any available information on study population demographics (age, sex, race/ethnicity) as well as if and how education attainment and quality were determined.
Table 1.
Search terms for literature review.
| PubMed | PsycINFO | |
|---|---|---|
| Search Terms | (cogniti*[title] OR dementia [tiab] OR Alzheimer*[tiab]) AND education AND ((white[tiab] OR Caucasian*[tiab]) AND (“non-white”[tiab] OR Black*[tiab] OR “African American*“[tiab] OR Hispanic*[tiab] OR latina*[tiab] OR latino*[tiab] OR latinx*[tiab] OR “Mexican American*“[tiab] OR Asian*[tiab] OR “Pacific Islander*“[tiab] OR “Native American*“[tiab] OR “Alaskan Native*“[tiab] OR “Alaska Native*“[tiab] OR “American Indian*“[tiab] OR “Native Hawaiian*“[tiab] OR indigenous [tiab] OR indian[tiab])) AND (elder*[tiab] OR “older*“[tiab] OR geriatric[tiab] OR senior* [tiab] OR ageing[tiab] OR retire* [tiab] OR aging[tiab] OR “Aged”[Mesh] OR “Aged, 80 and over”[Mesh]) AND (“United States” OR “United States of America” OR American* OR “USA” OR “U.S.A.” OR “U.S.“) AND norm* | (AB(cogniti*) OR TI(cogniti*) OR AB(dementia) OR TI (dementia) OR AB (Alzheimer*) OR TI (Alzheimer*)) AND (AB (education) OR TI(education)) AND (AB(Elder*) OR AB(old) OR AB(older) OR AB(“Aged”) OR AB(“Aged, 80 and over”) OR TI(Elder*) OR TI(old) OR TI(older) OR TI(“Aged”) OR TI (“Aged, 80 and over”)) AND (AB(adult) OR TI(adult)) AND (AB(non-white*) OR AB (Asian*) OR AB(Indian) OR AB (Black*) OR AB(African-American*) OR AB(“African American”) OR AB(“African Americans”) OR AB (Hispanic*) OR AB(Latin*) OR AB(Latina*) OR AB(latino*) OR AB(latinx) OR AB(“Native American*“) OR AB (Polynesian*) OR AB(Alaskan native*) OR AB(Arab*) OR AB (“people of color”) OR AB (POC) OR AB(BIPOC) OR AB (racial minority) OR AB (“visible minority”) OR AB (“people of colour”) OR AB (indigenous) OR AB(race) OR AB(racial) OR AB(ethnic) OR AB(culture*) OR TI(non-white*) OR TI(Asian*) OR TI (Indian) OR TI(Black*) OR TI (African-American*) OR TI (“African American”) OR TI (Hispanic*) OR TI(Latin*) OR TI(Latina*) OR TI(latino*) OR TI(latinx) OR TI(“Native American*“) OR TI (Polynesian*) OR TI(Alaskan native*) OR TI(Arab*) OR TI (“people of color”) OR TI(POC) OR TI(BIPOC) OR TI(racial minority) OR TI(“visible minority”) OR TI(“people of colour”) OR TI(indigenous) OR TI(race) OR TI(racial) OR TI (ethnic) OR TI(culture*)) AND (“United States” OR “United States of America” OR “USA” OR “U.S.A.” OR “U.S.“) AND norm* |
| Exclusion Criteria | Dissertations and conference abstracts, non-English language articles | |
2.2. Sensitivity analysis framework
Following our review of the literature, we conducted a formal sensitivity analysis to examine the extent to which disparities in dementia incidence would be eliminated if education quality were equalized across racial groups, while holding constant educational attainment. Our sensitivity analysis used a framework developed by VanderWeele & Robinson (VanderWeele and Robinson, 2014) to assess causal relationships between race, socioeconomic context, and health outcomes. In this approach, processes leading to racial discrimination are viewed as common causes of race and socioeconomic context. In appropriately adjusted models, covariate coefficients correspond to the effects of these variables on the outcome; the coefficient for race can be interpreted as the health inequality that would remain if the distribution of other covariates across racial groups were set equal to those of the reference group (i.e., setting the confounders for each person to levels randomly chosen from the reference group distribution).
We applied this framework specifically to the context of race, early education quality, and dementia, as illustrated in Fig. 1: P represents the processes giving rise to differences by race in education quality, including historical segregation, present-day systems and institutions that perpetuate racial discrimination, and individual perceptions of race leading to interpersonal racism. This process also gives rise to inequalities in education quality, which are associated with dementia risk (Kaup et al., 2014). Thus, the arrow between P and race represents the relationship between racial discrimination and lower quality of education. This causal structure leads to unmeasured confounding in the relationship between race—which we define to include subjective perception by others as well as lived experience as a member of a particular racial group—and dementia, in which there is a non-causal path through P and education quality. While adjusting for P would block the open non-causal pathway (i.e., adjust for unmeasured confounding) between race and dementia, P is difficult to measure. An alternative solution is to adjust for education quality, which blocks this non-causal pathway as well as a causal pathway between race and dementia (i.e., race → education quality → dementia). Under this alternative solution, findings from our analysis allow us to estimate the proportion of racial disparities in dementia that would be eliminated if education quality were equalized between racial groups. For simplicity, we limited our analysis to comparisons between Black and White participants.
Fig. 1.
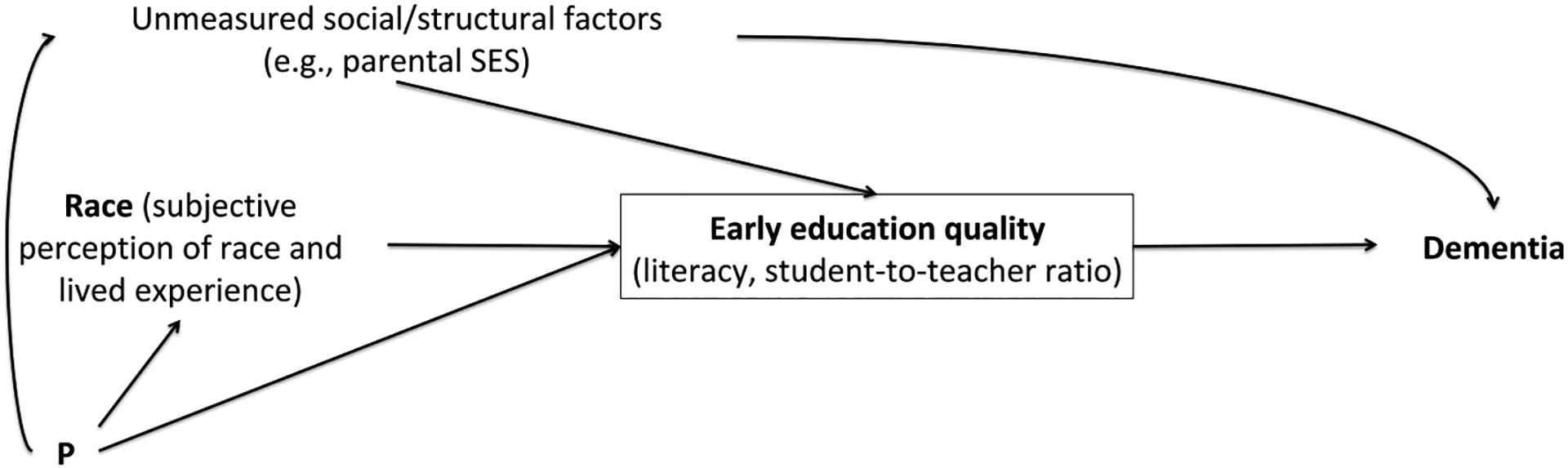
Relationship between race, education quality and dementia. P represents the processes giving rise to differences by race in education quality, including historical segregation, present-day systems and institutions that perpetuate racial discrimination as well as individual perceptions of race.
2.3. Extraction of parameter values
To parameterize our sensitivity analysis, we identified relevant estimates of the relationships between race, education quality and dementia primarily in a separate literature search of studies examining the relationship between education quality (in any form) and dementia risk among diverse populations. This search used the same terms as the above-mentioned literature review, but without limiting the search to only studies of normative data. The parameters that we identified for the sensitivity analysis are as follows: 1) the proportions of White and Black participants with low education quality (pw and pB, respectively), 2) the association between race and incident dementia risk (HRrace-dementia), and 3) the association between education quality and incident dementia risk (HREdQ-dementia) (Table 2).
Table 2.
Definition of parameters used for sensitivity analysis.
| Parameter | Definition | Source of extracted estimate(s) |
|---|---|---|
| pw | Proportion of White participants with low education quality |
Kaup et al., 2014
www.NCES.gov |
| pB | Proportion of Black participants with low education quality | Sisco et al., 2015 |
| HREdQ-dementia | Hazard of dementia for participants with low education quality compared to participants with adequate education quality; low education quality defined as either <9th grade reading level, inadequate literacy according to the National Center for Education Statistics, or having a student-teacher ratio greater than or equal to 29. |
Kaup et al., 2014
Yaffe et al., 2013 |
| HRrace-dementia | Hazard of dementia for Black participants compared to White participants |
Yaffe et al., 2013
Shadlen et al., 2006 |
We identified only one study, the Health, Aging and Body Composition (Health ABC) Study, in which all parameters required for our sensitivity analysis were available. Health ABC is a prospective cohort study of older adults without dementia at enrollment from zip code areas surrounding Memphis, Tennessee and Pittsburgh, Pennsylvania. The outcome of interest, dementia, was adjudicated by an expert committee using any of the following definitions: 1) ≥1.5 standard deviations of decline in the Modified Mini Mental State Examination (3MS) (Teng and Chui, 1987) score (from the participant’s baseline to the most recent visit) compared with the mean change in 3MS score in participants of the same race, 2) having dementia as a primary or secondary diagnosis at admission on hospital records and a 3MS score below 90 (a standard cutoff for diagnosing dementia), or 3) a prescription for a dementia medication (Yaffe et al., 2013). “Likely dementia” was defined similarly, only without the requirement for a 3MS score below 90 in those with an admission diagnosis. Education quality was parameterized as low vs. high education quality, and low education quality was defined as <9th grade reading level (Kaup et al., 2014).
To evaluate the impact on our estimates of parameter values from other studies, we extracted estimates for pw and pB from the National Center for Education Statistics (NCES) (National Center for Education Statistics, 2006) and the Health and Retirement Study (Sisco et al., 2015); “low education quality” was defined as having a student-teacher ratio of 29 or greater (HRS) (Sisco et al., 2015) or a literacy score reflecting “no more than the most simple and concrete literacy skills” (NCES) (National Center for Education Statistics, 2006). We additionally extracted an estimate of HRrace-dementia from the Cardiovascular Health Study (Shadlen et al., 2006). Only Health ABC had available estimates for HREdQ-dementia.
2.4. Sensitivity analysis equation
We applied these parameter values to the sensitivity analysis equation developed by VanderWeele (VanderWeele, 2013; Vanderweele and Onyebuchi, 2011) to calculate the hazard of dementia comparing Black to White participants adjusted for education quality; in other words, the extent to which racial disparities in dementia risk would be eliminated if education quality were equalized across groups:
The above equation estimates a corrected hazard ratio estimate of the inequality in dementia risk between Black and White participants by dividing the observed inequality by the bias factor on the hazard ratio scale for the effect of the unmeasured, binary confounder (here, education quality) on dementia risk, accounting for the prevalence of education quality in each group (VanderWeele, 2013). We repeated this process for each of the HRrace-dementia estimates (including the point estimate and 95% confidence interval [CI]) identified from the literature, using every combination of the other available parameters.
2.5. Necessary assumptions for sensitivity analysis
VanderWeele and Robinson (2014) and VanderWeele (2013) discussed the limitations of such an approach to sensitivity analysis. This approach assumes that the coefficient(s) for our mediator, early education quality, corresponds to the effect of this variable on dementia risk and there is no unmeasured confounding of this relationship. The analog of no unmeasured exposure-outcome confounding (race and dementia risk) is not required in this framework as we do not conceptualize an intervention on our exposure, race, but rather are interested in capturing a “mediated racial inequality measure” (VanderWeele and Robinson, 2014). We assume consistency in potential outcomes when setting education quality according to the distribution observed in the white population and positivity across the distributions of education quality, as well as no model misspecification. Finally, in the sensitivity analysis equation, we rely on simplifying assumptions that our unmeasured variable (education quality) is binary and that our outcome is “relatively rare” such that the hazard ratio is approximately collapsible and the difference method adopted here is valid given our confounding and modeling assumptions (VanderWeele, 2013).
3. Results
3.1. Literature review: operationalization of education
In our literature search, we identified 12 eligible studies that developed norms for measures of global cognition, which were published between 1999 and 2021. Multiple studies generated norms for performance on the Mini Mental State Examination (MMSE)(Pedraza et al., 2012) or a modified version (n = 2) and on the Montreal Cognitive Assessment (MoCA (Rossetti et al., 2011); n = 3), which are two common instruments for measuring global cognition. We found that in 10 out of 12 studies, educational attainment was operationalized as a categorical (e.g. <9 years, 9–11 years, 12 years, 13–15 years, 16+ years) variable. One study binarized educational attainment (0–13 years, >13 years)(Guayara-Quinn et al., 2021) and one used a continuous variable (years) (Casaletto et al., 2015). Overall, only one study adjusted for education quality, using the continuous reading score from the Wide Range Achievement Test (WRAT-3) (Wilkinson, 1993) as a proxy for literacy (Jefferson et al., 2007) (Table 3).
Table 3.
Educational classification and use among studies that developed norms for standard cognitive screening measures with multiple race/ethnicity groups (N = 12).
| Title | First author (Year) | Study population age, sex, race/ethnicity (N) | Measure(s) of cognition | Operationalization of educational attainment (mean years of education if available) | Operationalization of education quality |
|---|---|---|---|---|---|
| Normative data for the Montreal Cognitive Assessment (MoCA) in a population-based sample | Rossetti et al. (2011) | Mean age 50.3 years; 60% female; 34% White, 52% African American, 11% Hispanic, 2% other (N = 2653) | Montreal Cognitive Assessment (MoCA) | <12 years, 12 years, >12 years | N/A |
| Normative performance of healthy older individuals on the Modified Mini-Mental State (3MS) examination according to ethno-racial group, gender, age, and education level | Ryan et al. (2019) | Mean age 74 years; 47.1% White, 39.1% African-American, 13.8% Hispanic/Latino; 56% female (N = 2291)a | Modified Mini-Mental State Examination (3MS) | <9 years, 9–11 years, 12 years, 13–15 years, 16+ years (mean years of education: 12) | N/A |
| Effects of age, gender, education and race on two tests of language ability in community-based older adults | Snitz et al. (2009) | Mean age 77.2 years; 65.2% female; 28.1% African American, 71.9% White (N = 1885) | Animal fluency task, Indiana University Token Test | 0–8 years, 9–12 years, 13+ years (mean years of education: 12.2) | N/A |
| Re-evaluation of psychometric evidence and update of normative data for the Test of Practical Judgment | Guayara-Quinn et al. (2021) | Mean age 79 years; 68% female; 30% Black/African-American, 8% Hispanic, 62% White (N = 348) | Test of Practical Judgment | 0–13 years, >13 years (mean years education: 15) | N/A |
| Neuropsychological performance of Hispanic and non-Hispanic older adults: an epidemiologic survey | La Rue et al. (1999) | Age range 65–97 years; 46.8% female; 45% Hispanic, 55% non-Hispanic white (N = 797) | Fuld Object Memory Evaluation, Digit Span, category naming, clock drawing, Color Trails | 0–6 years, 7–9 years, 10–12 years, > 12 years | N/A |
| Performance of cognitively normal African Americans on the RBANS in community dwelling older adults | Patton et al. (2003) | Mean age 72; 50% African American, 50% White; 62% males (n = 100) | Repeatable Battery for the Assessment of Neuropsychological Status | Less than 8th grade, some high school, completed high school, some college, completed college, some graduate school, completed graduate school | N/A |
| Geriatric performance on an abbreviated version of the Boston naming test | Jefferson et al. (2007) | Mean age 71.9 years; 66.2% female; 12.4% African Americans, 87.6% White (N = 219)b | Boston Naming Test | Less than high school, some college, college grad, less than grad degree, graduate degree | Average WRAT-3 vs. above-average |
| Norms for letter and category fluency: demographic corrections for age, education, and ethnicity | Gladsjo et al. (1999) | Mean age 52 years; 47% female; 53% White, 47% African American (N = 768) | Letter and Category Fluency | 0–11 years, 12–15 years, 16+ years (mean years of education: 14) | N/A |
| Demographically Corrected Normative Standards for the English Version of the NIH Toolbox Cognition Battery | Casaletto et al., 2015 | Mean age 49.1; 63.1% female; 61.5% White, 14.8% African American, 9.6% Hispanic (N = 1038) | NIH Toolbox Cognition Battery | Years (continuous) | N/A |
| Normative data for 8 neuropsychological tests in older blacks and whites from the atherosclerosis risk in communities (ARIC) study | Schneider et al. (2015) | Mean age 71.9; 62.6% female; 44.9% Black, 55.1% White (N = 712) | Delayed Word Recall Test, Logical Memory, Word Fluency Test, Animal Naming, Trail Making Test Part A&B, Digit Symbol Substitution Test | < High school, high school/GED/vocational school, college or graduate/professional school | N/A |
| Normative performance on the executive clock drawing task in a multi-ethnic bilingual cohort: a project FRONTIER study | Menon et al. (2012) | Mean age 61.9 years; 68.7% female; 43% Hispanic, 57% non-Hispanic White (N = 445) | Mini Mental State Examination (MMSE) | 8–13 years, 14+ years (mean years of education: 10.9) | N/A |
| Robust demographically-adjusted normative data for the Montreal Cognitive Assessment (MoCA): Results from the systolic blood pressure intervention trial | Sachs et al. (2021) | Mean age 66.9 years; 35.7% female; 63.1% White, 27.4% Black, 9.5% Hispanic (N = 5338) | Montreal Cognitive Assessment (MoCA) | Less than high school, high school graduate or GED, post-high school or some college, college graduate or higher | N/A |
Demographic and sample size information only includes U.S. participants who participated in the study.
Demographic and sample size information only includes cognitively normal participants who participated in the study.
3.2. Sensitivity analysis
To obtain race-specific proportions of low education quality (pw and pB for White and Black participants, respectively), we operationalized education quality as a binary variable (low education quality vs. adequate education quality) using different definitions from Kaup et al. (2014), Sisco et al. (2015), and the NCES (National Center for Education Statistics, 2006). In Kaup et al. (2014), low education quality was defined based on achieving limited literacy (i.e., <9th grade reading level) as discussed previously. Using this cut-point, 44.3% of Black participants and 10.5% of White participants had “limited literacy” and thus low quality. Sisco et al. (2015) defined low education quality as having a student-teacher ratio of 29 or greater (Black: 71%; White: 33%). The NCES (National Center for Education Statistics, 2006) defined low education quality as having below-basic literacy, i.e. “having no more than the most simple and concrete literacy skills,” which includes being unable to locate “easily identifiable information in short, commonplace prose texts,” locate “easily identifiable information and follow written instructions in simple documents,” or search “a short, simple text to find out what a patient is allowed to drink before a medical test”; being unable to locate numbers and “[use] them to perform simple quantitative operations (primarily addition)” or add the amounts on a bank deposit slip; or being unable to sign a form (Black: 24%; White: 7%).
Next, we obtained estimates for the association between education quality and dementia (HREdQ-dementia) from Health ABC, which, as noted above, defined education quality as <9th grade reading level. These estimates were HR = 1.53 (95% CI: 1.17, 2.00) from Kaup et al. (2014) and HR = 1.70 (95% CI: 1.41, 2.00) from Yaffe et al. (2013) We also obtained estimates for the association between race and dementia (HRrace-dementia) from Health ABC (Yaffe et al., 2013) and the Cardiovascular Health Study (CHS) (Shadlen et al., 2006), which were HR = 1.37 (95% CI: 1.12, 1.67) and HR = 2.0 (95% CI: 1.43, 2.74), respectively (Table 4).
Table 4.
Sensitivity analysis parameter estimates from the literature for relationships between education quality, race, and dementia.
| Race-specific proportions of low education quality | HREdQ-dementia | HRrace-dementia (95%CI) |
|---|---|---|
|
Kaup et al., 2014 (Health ABC) EdQ: limited literacy, <9th grade reading level pB = 0.443 pw = 0.104 www.NCES.gov EdQ: below-basic literacy in 2003a pB = 0.24 pw = 0.07 Sisco et al., 2015 (HRS) EdQ: student-teacher ratio ≥29 pB = 0.711 pw = 0.329 |
Kaup et al., 2014 (Health ABC) Risk of likely dementiab Adjusted for age, sex, race, education, income HREdQ-dementia (95% CI): 1.53 (1.17, 2.00) Yaffe et al., 2013 (Health ABC) Risk of incident dementia Adjusted for: N/A HREdQ-dementia (95% CI): 1.70 (1.41, 2.05) |
Shadlen et al., 2006 (CHS): Adjusted for education, comorbidities, APOE4 HRrace-dementia (95%CI): 2.00 (1.43, 2.74)c Yaffe et al., 2013 (Health ABC): Adjusted for demographics, APOE4, comorbidities, lifestyle HRrace-dementia (95%CI): 1.37 (1.12, 1.67) |
Defined as “having no more than the most simple and concrete literacy skills”, which includes being unable to locate “easily identifiable information in short, commonplace prose texts”, locate “easily identifiable information and follow written instructions in simple documents”, or search “a short, simple text to find out what a patient is allowed to drink before a medical test”; being unable to locate numbers “using them to perform simple quantitative operations (primarily addition)” or add the amounts on a bank deposit slip; or being unable to sign a form (nces.ed.gov/naal/pdf/2006470_1.pdf).
Likely dementia define as “if any of the following criteria were met: (a) record of a hospitalization with dementia listed as a primary or secondary diagnosis, determined through Health ABC adjudication to reflect a chronic, progressive decline rather than an acute change (eg, delirium), (b) a documented prescription for dementia medication, or (c) ≥ 1.5 SD decline in 3MS score from participants’ baseline to last visit compared with the mean 3MS change exhibited by their race-matched peers within the cohort.”
Only included participants with <10 years of educational attainment.
Table 5 shows the results of calculations for HRrace-dementia with every combination of the parameters in Table 4. HRrace-dementia was attenuated in every combination. Using HREdQ-dementia from Kaup et al. (2014) (i.e., education quality defined according to high and low literacy using below 9th grade reading level), HRrace-dementia (risk of likely dementia for Black compared to White participants) adjusted for age, sex, race, education, and income was attenuated from 1.37 (95% CI: 1.12, 1.67) to 1.17 (95% CI: 0.96, 1.43), an attenuation of 54% (i.e., from 37% excess risk to 17% excess risk). The percent attenuation ranged from 29% to 68% based on specifications of the education quality-dementia and race-dementia relationships.
Table 5.
EdQ-adjusted relationship between race and dementia using different combinations of parameter estimates from the literature.
| Race-specific proportions of low education quality | HREdQ-dementia (95% CI) | HRrace-dementia (95%CI) | EdQ-Adjusteda HRrace-dementia (95%CI) |
Percent attenuatedb from EdQ-Adjustment |
|---|---|---|---|---|
| pB = 0.443 pw = 0.104 EdQ = Limited literacy (<9th grade reading level) (Kaup et al.; Health ABC) | 1.53 (1.17, 2.00) EdQ = Limited literacy (<9th grade reading level) (Health ABC) Risk of likely dementia; adjusted for age, sex, race, education, income (Kaup et al., Health ABC) | 2.0 (1.43, 2.74) Adjusted for education, comorbidities, APOE4 (Shadlen et al., CHS) | 1.71 (1.22, 2.34) | 29% |
| 1.37 (1.12, 1.67) Adjusted for age, sex, APOE4, BMI, history of stroke or myocardial infarction, hypertension, diabetes, depression, current smoking, alcohol use, physical activity (Yaffe et al., Health ABC) | 1.17 (0.96, 1.43) d | 54% | ||
| 1.70 (1.41, 2.05) EdQ = Limited literacy (<9th grade reading level) (Health ABC) Risk of incident dementia; unadjusted (Yaffe et al., Health ABC) | 2.0 (1.43, 2.74) | 1.64 (1.17, 2.24) | 36% | |
| 1.37 (1.12, 1.67) | 1.12 (0.92, 1.37) d | 67.6% | ||
| pB = 0.24 pW = 0.07 EdQ = Below-basic literacy (NCES)c | 1.53 (1.17, 2.00) | 2.0 (1.43, 2.74) | 1.84 (1.32, 2.52) | 16% |
| 1.37 (1.12, 1.67) | 1.26 (1.03, 1.54) | 29.7% | ||
| 1.70 (1.41, 2.05) | 2.0 (1.43, 2.74) | 1.80 (1.28, 2.46) | 20% | |
| 1.37 (1.12, 1.67) | 1.23 (1.01, 1.50) | 37.8% | ||
| pB = 0.711 pW = 0.329 EdQ = Student-teacher ratio ≥29 (Sisco et al., HRS) | 1.53 (1.17, 2.00) | 2.0 (1.43, 2.74) | 1.71 (1.22, 2.34) | 29% |
| 1.37 (1.12, 1.67) | 1.17 (0.96, 1.42) d | 54% | ||
| 1.70 (1.41, 2.05) | 2.0 (1.43, 2.74) | 1.64 (1.17, 2.25) | 36% | |
| 1.37 (1.12, 1.67) | 1.13 (0.92, 1.37) d | 64.8% |
Equation used: HRrace-dementia, adjusted for U = HRrace-dementia/[(1+(HREdQ-dementia-1)*pB)/(1+(HREdQ-dementia-1)*pw)]; where pB = proportion of Black participants with low EdQ; pW = proportion of White participants with low EdQ; definition of low EdQ specified for each estimate.
Percent attenuation defined according to percent attenuation in excess risk (HR-1/HR) from the unadjusted to the EdQ-Adjusted HR.
Defined as “no more than the most simple and concrete literacy skills” in the domains of prose, document and quantitative literacy in 2003 (nces.ed.gov/naal/pdf/2006470_1.pdf).
Confidence interval crosses HR = 1.
Using HREdQ-dementia from NCES (National Center for Education Statistics, 2006) (i.e., education quality defined according to below-basic literacy), HRrace-dementia (risk of likely dementia for Black compared to White participants) adjusted for age, sex, race, education, and income was attenuated from 1.37 (95% CI: 1.12, 1.67) to 1.23 (95% CI: 1.01, 1.50), an attenuation of 37.8% (i.e., from 37% excess risk to 23% excess risk). This percent attenuation ranged from 16% to 38% based on specifications of the education quality-dementia relationship as well as the race-dementia relationships.
Finally, when using HREdQ-dementia from Sisco et al. (2015) (i.e., education quality defined according to student teacher ratio ≥ 29), HRrace-dementia (risk of likely dementia for Black compared to White participants) adjusted for age, sex, race, education, and income was attenuated from 1.37 (95% CI: 1.12, 1.67) to 1.13 (95% CI: 0.92, 1.37), an attenuation of 65% (i.e., from 37% excess risk to 13% excess risk); percent attenuation ranged from 29% to 65% based on specifications of the education quality-dementia and race-dementia relationships.
4. Discussion
In this study, we examined the extant literature to evaluate the utilization and operationalization of education measures (attainment and quality) to account for differences in measured cognition between racial/ethnic groups in the United States. Noting a paucity of work adequately incorporating measures of education quality, we performed a sensitivity analysis to quantify the potential reduction or elimination of racial disparities in dementia risk that resulted from making the quality of education comparable between groups, without changing present disparities in educational attainment. Our findings suggest that U.S. Black versus White population disparities in dementia risk would be consistently attenuated after equalizing education quality (i.e., setting the distribution of education quality among Black participants to be that observed among White participants), allowing for variation in the parameter estimates of values identified in the extant literature. While additional research is needed to confirm this finding and to quantify the impact of early-life education quality on dementia risk, our results add support to the critical need to address educational inequality for reasons of public health as well as social justice.
In the literature, education is operationalized as a quantitative, categorical variable in most studies that developed norms for standard cognitive screening measures. Few studies accounted for or operationalized education quality. Studies that developed normative data sources by age and educational attainment generally only considered categorized education level, with the same norms applied across racial/ethnic groups (Crum et al., 1993; Rossetti et al., 2011; Schneider et al., 2015). While this is problematic due to the socioeconomic context-specific nature of educational attainment that often differs by racial/ethnic group, there are also issues with developing normative data by race (Manly et al., 2005). Race-specific norms of cognition may obscure underlying factors contributing to between-group discrepancies, which creates barriers to measuring racial disparities and may imply that underlying differences are biological rather than socially constructed (Pedraza and Mungas, 2008). Developing norms for cognitive testing that consider education quality may contribute to more valid cognitive testing overall and for minority populations in particular. Such norms will provide additional information about the historical context that contribute to poor education quality for many Black Americans, including racist housing and education policies (e.g. redlining and legalized school segregation) with effects that continue to manifest in present-day structural racism.
Previous work has hypothesized that measures of education quality such as literacy are a more accurate reflection of the overall educational experience than years of educational attainment, and that differences in the quality of education greatly contribute to racial and ethnic disparities in late-life cognitive decline (Manly et al., 2005). Manly et al. (Manly, Jacobs, Touradji, Small, Stern) found that after matching Black and White older adults on years of educational attainment, adjusting for WRAT-3 significantly reduced (i.e. attenuated to the null) racial differences in scores for nearly all cognitive tests. This is consistent with findings from our sensitivity analysis showing that equalizing education quality between groups would significantly attenuate the observed racial disparities in dementia risk, even after accounting for differences in educational attainment. We further expanded on the work by Manly et al. (Manly, Jacobs, Touradji, Small, Stern) with the inclusion of a process measure (student-teacher ratio) as well as an outcome measure (9th grade literacy, literacy score), and provided a range of estimates for the extent to which racial disparities in dementia risk could potentially be attenuated after accounting for these measures of education quality. While the latter measure, limited literacy, is likely the consequence of both education quality and attainment along with broader social factors in early-life, it generally reflects a fundamental failure of the education system. Historical and present-day racial discrimination on a systemic level, such as geographic disparities in education quality due to racial segregation and economic factors, and on an individual level, such as differential treatment of children according to ascribed racial identity (Dulin-Keita et al., 2011), perpetuate stark disparities in the access and receipt of high-quality education. In the same study (Manly, Jacobs, Touradji, Small, Stern), the authors noted the importance of not perpetuating the fallacy that residual racial disparities in test performance are due to biological differences; and thus, the need to quantify the substantial proportion of the racial disparities that can be attributed to the educational experience beyond years of educational attainment. In any event, addressing disparities in education quality in addition to or independently of educational attainment is critical to understanding and mitigating health disparities. Future work is critically needed to elucidate the complex relationships among race, educational attainment and quality, and dementia risk.
Our study has several limitations related to our intentionally simplified conceptual model described in Fig. 1. There are likely mechanisms contributing to observed disparities not captured in our model, including subsequent employment opportunities, adulthood socioeconomic status and other sources of unmeasured confounding. Since we sought to determine the effect of education quality on the relationship between race and dementia beyond that of educational attainment, our conceptual model does not take into account the substantial impact of education quality on attainment (Park and Kyei, 2011). As a result, the full attenuation of the relationship between race and dementia may be greater than what we estimated, had we included the impact of education quality on educational attainment in our model. Further, the necessary use of broad comparison groups, Black versus White, may obscure significant heterogeneity within groups and fail to capture disparities in other U.S. racial or ethnic groups. For example, the comparison was not able to not address differences in dementia incidence between foreign-born versus U.S.-born minorities previously identified in the literature (Garcia et al., 2018). Future research should aim to assess the proportion eliminated in racial or ethnic disparities in dementia risk among other minority groups in the U.S., although this would first require estimates of the association between education quality and dementia risk in these populations.
There are several additional limitations due to potential violations of the assumptions for the sensitivity analysis method. First, there was a minor violation of the rare disease assumption, as approximately 18% of the participants in Health ABC developed dementia over follow-up (Yaffe et al., 2013). However, Health ABC was the only study in which all key parameter estimates were available, and the only study that provided an estimate of the association between education quality (with literacy as a proxy) and dementia. Second, potential unmeasured confounding in the studies providing our parameter estimates for HRrace--dementia and HREdQ-dementia would have violated the assumption that the estimates used in the sensitivity analysis are unconfounded. The studies from which we obtained hazard ratio estimates for the sensitivity analysis did not take into account potential birth cohort effects and geographical variation, such as legalized racial segregation during formal schooling experienced by earlier birth cohorts, which may be a source of significant unmeasured confounding in the relationship between race and dementia (HRrace-dementia) (Glymour and Manly, 2008). We also acknowledge that while racial disparities in dementia risk documented in the literature may be biased due to differences in literacy that increase the risk of falsely diagnosing MCI or dementia in minority populations(Parker and Philp, 2004), the use of race-specific criteria for dementia adjudication in Health ABC may have in fact underestimated the risk of dementia for Black compared to White participants. A larger estimate for HRrace-dementia in the sensitivity analysis may have yielded a smaller proportion of disparities eliminated. Finally, there was likely unmeasured confounding of the education quality and dementia relationship (HREdQ-dementia) from the literature by early childhood experiences or cognitive development. These factors may also be a source of measurement error for education quality, as low literacy may be a poor proxy for poor education quality for participants whose low score on literacy tests are partly or fully due to early deprivation in nutrition, lack of familial support, or other adverse exposures in the early developmental period (i.e. reasons not directly related to low education quality). Even if none of the assumptions were violated, it is important to note that our analysis only captures the proportion of racial inequality in dementia risk due to the particular measure of education quality that was used in each iteration of the sensitivity analysis (e.g. student-to-teacher ratio or 9th grade literacy, but not both). Thus, as stated previously, we interpret our results with caution and suggest that education quality may be an underexamined but considerable contributor to inequalities in dementia risk.
Given the significant burden of dementia in the United States and the disproportionate risk among racial/ethnic minorities, there is ample reason to explore the important role of education quality in reducing disparities in cognitive aging. Not accounting for education quality in studies of cognitive decline and dementia among racially diverse populations of older adults perpetuates the lack of information on how to address these disparities. Measuring and operationalizing education quality in addition to educational attainment will enhance our understanding of the relationships between race, education, and dementia, which is particularly important for the development of normative data on cognition that considers early-life socioeconomic context. Developing practical interventions to reduce racial disparities in health outcomes, rather than documenting them, has been discussed at length in the literature (Harper and Strumpf, 2012; Galea and Link, 2013; Galea, 2013). However, policy efforts aimed at reducing these disparities have not been effective(Marmot, 2010; Mackenbach, 2010), and more specific targeting of domains where socioeconomic and racial/ethnic disparities arise may be needed. For example, changes in schooling and education structure may be able to significantly improve early educational achievement among students in low-income areas (Fryer and Dobbie, 2011), which is likely a downstream effect of improving education quality as well as attainment. Finally, literature focusing on disparities in cognition by race/ethnicity without the acknowledgement of broader social and societal contexts places focus on factors that are non-modifiable by late-life, such as educational attainment and employment opportunities, and risks reinforcing fallacious biological essentialism. These historically constructed, systemically unequal opportunites for racial and ethnic minorities in the U.S. lead to stark disparities in life-course health outcomes. In order to take actionable and concrete steps to address the disproportionate burden of dementia among racial and ethnic minorities, it may be more useful to shift the paradigm to instead study critical periods for modifiable social factors across the life-course and develop interventions to redress extant inequalities among older adults.
Acknowledgements
We thank Emily Harrison for thoughtful discussions on framing racial disparities in the context of historical and present-day structures built around race.
Footnotes
Credit author statement
Chelsea Liu: Conceptualization, Software, Formal analysis, Investigation, Resources, Data curation, Roles/Writing - original draft, Writing – review & editing, Visualization, Audrey R. Murchland: Conceptualization, Verification, Formal analysis, Investigation, Resources, Data curation, Roles/Writing - original draft, Writing – review & editing, Visualization. Tyler J. VanderWeele: Methodology, Writing – review & editing, Deborah Blacker: Conceptualization, Writing – review & editing, Supervision, Funding acquisition, Project administration
Declaration of competing interest
The authors have no relevant financial or non-financial interests to disclose.
Data availability
Data will be made available on request.
References
- Avila JF, Vonk JMJ, Verney SP, et al. , 2019. Sex/gender differences in cognitive trajectories vary as a function of race/ethnicity. Alzheimers Dement 15 (12), 1516–1523. 10.1016/j.jalz.2019.04.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bailey ZD, Krieger N, Agénor M, Graves J, Linos N, Bassett MT, 2017. Structural racism and health inequities in the USA: evidence and interventions. Lancet 389 (10077), 1453–1463. 10.1016/S0140-6736(17)30569-X. [DOI] [PubMed] [Google Scholar]
- Bailey ZD, Feldman JM, Bassett MT, 2021. How structural racism works - racist policies as a root cause of U.S. Racial health inequities. N. Engl. J. Med 384 (8), 768–773. 10.1056/NEJMms2025396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barnes LL, Lewis TT, Begeny CT, Yu L, Bennett DA, Wilson RS, 2012. Perceived discrimination and cognition in older African Americans. J. Int. Neuropsychol. Soc 18 (5), 856–865. 10.1017/S1355617712000628. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bartle-Haring S, Whiting R, 2022. Structural racism and the education gradient for early all-cause mortality. SSM Popul Health 17, 101076. 10.1016/j.ssmph.2022.101076. Published 2022 Mar 23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bohnstedt M, Fox PJ, Kohatsu ND, 1994. Correlates of Mini-Mental Status Examination scores among elderly demented patients: the influence of race-ethnicity. J. Clin. Epidemiol 47 (12), 1381–1387. 10.1016/0895-4356(94)90082-5. [DOI] [PubMed] [Google Scholar]
- Casaletto KB, Umlauf A, Beaumont J, et al. , 2015. Demographically corrected normative standards for the English version of the NIH toolbox cognition battery. J. Int. Neuropsychol. Soc 21 (5), 378–391. 10.1017/S1355617715000351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen AK, Syme SL, 2013. Education: a missed opportunity for public health intervention. Am. J. Publ. Health 103 (6), 997–1001. 10.2105/AJPH.2012.300993. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crum RM, Anthony JC, Bassett SS, Folstein MF, 1993. Population-based norms for the Mini-Mental State Examination by age and educational level. JAMA 269 (18), 2386–2391. [PubMed] [Google Scholar]
- Dotson VM, Kitner-Triolo MH, Evans MK, Zonderman AB, 2009. Effects of race and socioeconomic status on the relative influence of education and literacy on cognitive functioning. J. Int. Neuropsychol. Soc 15 (4), 580–589. 10.1017/S1355617709090821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dulin-Keita A, Hannon L, Fernandez JR, Cockerham WC, 2011. The defining moment: children’s conceptualization of race and experiences with racial discrimination. Ethn. Racial Stud 34 (4), 662–682. 10.1080/01419870.2011.535906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Everett BG, Rogers RG, Hummer RA, Krueger PM, 2011. Trends in educational attainment by race/ethnicity, nativity, and sex in the United States, 1989–2005. Ethn. Racial Stud 34 (9), 1543–1566. 10.1080/01419870.2010.543139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fryer R, Dobbie W, 2011. Are high-quality schools enough to increase achievement among the poor? Evidence from the Harlem Children’s Zone. Am. Econ. J 3, 158–187. [Google Scholar]
- Fujishiro K, MacDonald LA, Howard VJ, 2020. Job complexity and hazardous working conditions: how do they explain educational gradient in mortality? J. Occup. Health Psychol 25 (3), 176–186. 10.1037/ocp0000171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galea S, 2013. An argument for a consequentialist epidemiology. Am. J. Epidemiol 178, 1185–1191. [DOI] [PubMed] [Google Scholar]
- Galea S, Link BG, 2013. Six paths for the future of social epidemiology. Am. J. Epidemiol 178, 843–849. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garcia MA, Saenz J, Downer B, Wong R, 2018. The role of education in the association between race/ethnicity/nativity, cognitive impairment, and dementia among older adults in the United States. Demogr. Res 38, 155–168. 10.4054/DemRes.2018.38.6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gladsjo JA, Schuman CC, Evans JD, Peavy GM, Miller SW, Heaton RK, 1999. Norms for letter and category fluency: demographic corrections for age, education, and ethnicity. Assessment 6 (2), 147–178. 10.1177/107319119900600204. [DOI] [PubMed] [Google Scholar]
- Glymour MM, Manly JJ, 2008. Lifecourse social conditions and racial and ethnic patterns of cognitive aging. Neuropsychol. Rev 18 (3), 223–254. 10.1007/s11065-008-9064-z. [DOI] [PubMed] [Google Scholar]
- Glymour MM, Manly JJ, 2018. Compulsory Schooling Laws as quasi-experiments for the health effects of education: reconsidering mechanisms to understand inconsistent results. Soc. Sci. Med 214, 67–69. 10.1016/j.socscimed.2018.08.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guayara-Quinn CG, Nester CO, Katz MJ, et al. , 2021. Re-evaluation of psychometric evidence and update of normative data for the Test of Practical Judgment [published online ahead of print, 2021 Mar 25]. Clin. Neuropsychol 1–24. 10.1080/13854046.2021.1889680. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hamad R, Elser H, Tran DC, Rehkopf DH, Goodman SN, 2018. How and why studies disagree about the effects of education on health: a systematic review and meta-analysis of studies of compulsory schooling laws. Soc. Sci. Med 212, 168–178. 10.1016/j.socscimed.2018.07.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harper S, Strumpf EC, 2012. Social epidemiology: questionable answers and answerable questions. Epidemiology 23, 795–798. [DOI] [PubMed] [Google Scholar]
- Jefferson AL, Wong S, Gracer TS, Ozonoff A, Green RC, Stern RA, 2007. Geriatric performance on an abbreviated version of the Boston naming test. Appl. Neuropsychol 14 (3), 215–223. 10.1080/09084280701509166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaup AR, Simonsick EM, Harris TB, et al. , 2014. Older adults with limited literacy are at increased risk for likely dementia. J Gerontol A Biol Sci Med Sci 69 (7), 900–906. 10.1093/gerona/glt176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kennedy RE, Williams CP, Sawyer P, Allman RM, Crowe M, 2014. Comparison of in-person and telephone administration of the mini-mental state examination in the university of Alabama at birmingham study of aging. J. Am. Geriatr. Soc 62 (10), 1928–1932. 10.1111/jgs.13027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- La Rue A, Romero LJ, Ortiz IE, Liang HC, Lindeman RD, 1999. Neuropsychological performance of Hispanic and non-Hispanic older adults: an epidemiologic survey. Clin. Neuropsychol 13 (4), 474–486. 10.1076/1385-4046(199911)13:04;1-Y;FT474. [DOI] [PubMed] [Google Scholar]
- Mackenbach JP, 2010. Has the English strategy to reduce health inequalities failed? Soc. Sci. Med 71, 1249–1253 discussion 1254. [DOI] [PubMed] [Google Scholar]
- Manly JJ, Schupf N, Tang MX, Stern Y, 2005. Cognitive decline and literacy among ethnically diverse elders. J. Geriatr. Psychiatr. Neurol 18 (4), 213–217. 10.1177/0891988705281868. [DOI] [PubMed] [Google Scholar]
- Manly JJ, Jacobs DM, Touradji P, Small SA, Stern Y, 2002. Reading level attenuates differences in neuropsychological test performance between African American and White elders [published correction appears in J Int Neuropsychol Soc 2002 May;8(4):605]. J. Int. Neuropsychol. Soc 8 (3), 341–348. 10.1017/s1355617702813157. [DOI] [PubMed] [Google Scholar]
- Marmot M, 2010. Fair Society, Healthy Lives: the Marmot Review. Strategic Review of Health Inequalities in England Post-2010. [Google Scholar]
- Menon C, Hall J, Hobson V, Johnson L, O’Bryant SE, 2012. Normative performance on the executive clock drawing task in a multi-ethnic bilingual cohort: a project FRONTIER study. Int. J. Geriatr. Psychiatr 27 (9), 959–966. 10.1002/gps.2810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Milani SA, Marsiske M, Striley CW, 2019. Discriminative ability of montreal cognitive assessment subtests and items in racial and ethnic minority groups. Alzheimer Dis. Assoc. Disord 33 (3), 226–232. 10.1097/WAD.0000000000000310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Center for Education Statistics. National Assessment of Adult Literacy (NAAL). nces.ed.gov/naal/pdf/2006470_1.pdf.
- Nkwata AK, Zhang M, Song X, Giordani B, Ezeamama AE, 2022. Toxic psychosocial stress, resiliency resources and time to dementia diagnosis in a nationally representative sample of older Americans in the health and retirement study from 2006–2016. Int. J. Environ. Res. Publ. Health 19 (4), 2419. 10.3390/ijerph19042419. Published 2022 Feb 19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Park H, Kyei P, 2011. Literacy gaps by educational attainment: a cross-national analysis. Soc. Forces 89 (3), 879–904. 10.1353/sof.2011.0025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Parker C, Philp I, 2004. Screening for cognitive impairment among older people in black and minority ethnic groups. Age Ageing 33 (5), 447–452. 10.1093/ageing/afh135. [DOI] [PubMed] [Google Scholar]
- Patton DE, Duff K, Schoenberg MR, Mold J, Scott JG, Adams RL, 2003. Performance of cognitively normal African Americans on the RBANS in community dwelling older adults. Clin. Neuropsychol 17 (4), 515–530. 10.1076/clin.17.4.515.27948. [DOI] [PubMed] [Google Scholar]
- Pedraza O, Mungas D, 2008. Measurement in cross-cultural neuropsychology. Neuropsychol. Rev 18 (3), 184–193. 10.1007/s11065-008-9067-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pedraza O, Clark JH, O’Bryant SE, et al. , 2012. Diagnostic validity of age and education corrections for the Mini-Mental State Examination in older African Americans. J. Am. Geriatr. Soc 60 (2), 328–331. 10.1111/j.1532-5415.2011.03766. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pohl DJ, Seblova D, Avila JF, et al. , 2021. Relationship between residential segregation, later-life cognition, and incident dementia across race/ethnicity. Int. J. Environ. Res. Publ. Health 18 (21), 11233. 10.3390/ijerph182111233. Published 2021 Oct 26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rossetti HC, Lacritz LH, Cullum CM, Weiner MF, 2011. Normative data for the montreal cognitive assessment (MoCA) in a population-based sample. Neurology 77 (13), 1272–1275. 10.1212/WNL.0b013e318230208a. [DOI] [PubMed] [Google Scholar]
- Ryan J, Woods RL, Britt C, et al. , 2019. Normative performance of healthy older individuals on the Modified Mini-Mental State (3MS) examination according to ethno-racial group, gender, age, and education level. Clin. Neuropsychol 33 (4), 779–797. 10.1080/13854046.2018.1488996. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sachs BC, Chelune GJ, Rapp SR, et al. , 2021. Robust demographically-adjusted normative data for the Montreal Cognitive Assessment (MoCA): results from the systolic blood pressure intervention trial [published online ahead of print, 2021 Sep 1]. Clin. Neuropsychol 1–16. 10.1080/13854046.2021.1967450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schneider AL, Sharrett AR, Gottesman RF, et al. , 2015. Normative data for 8 neuropsychological tests in older blacks and whites from the atherosclerosis risk in communities (ARIC) study. Alzheimer Dis. Assoc. Disord 29 (1), 32–44. 10.1097/WAD.0000000000000042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shadlen MF, Siscovick D, Fitzpatrick AL, Dulberg C, Kuller LH, Jackson S, 2006. Education, cognitive test scores, and black-white differences in dementia risk. J. Am. Geriatr. Soc 54 (6), 898–905. 10.1111/j.1532-5415.2006.00747.x. [DOI] [PubMed] [Google Scholar]
- Sisco S, Gross AL, Shih RA, et al. , 2015. The role of early-life educational quality and literacy in explaining racial disparities in cognition in late life. J. Gerontol. B Psychol. Sci. Soc. Sci 70 (4), 557–567. 10.1093/geronb/gbt133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Snitz BE, Unverzagt FW, Chang CC, et al. , 2009. Effects of age, gender, education and race on two tests of language ability in community-based older adults. Int. Psychogeriatr 21 (6), 1051–1062. 10.1017/S1041610209990214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Teng EL, Chui HC, 1987. The modified mini-mental state (3MS) examination. J. Clin. Psychiatr 48 (8), 314–318. [PubMed] [Google Scholar]
- VanderWeele TJ, 2013. Unmeasured confounding and hazard scales: sensitivity analysis for total, direct, and indirect effects. Eur. J. Epidemiol 28 (2), 113–117. 10.1007/s10654-013-9770-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vanderweele TJ, Onyebuchi AA, 2011. Bias formulas for sensitivity analysis of unmeasured confounding for general outcomes, treatments, and confounders. Epidemiology 22 (1), 42–52. 10.1097/EDE.0b013e3181f74493. [DOI] [PMC free article] [PubMed] [Google Scholar]
- VanderWeele TJ, Robinson WR, 2014. On the causal interpretation of race in regressions adjusting for confounding and mediating variables. Epidemiology 25 (4), 473–484. 10.1097/EDE.0000000000000105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weuve J, Barnes LL, Mendes de Leon CF, et al. , 2018. Cognitive aging in black and white Americans: cognition, cognitive decline, and incidence of alzheimer disease dementia. Epidemiology 29 (1), 151–159. 10.1097/EDE.0000000000000747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whiting R, Bartle-Haring S, 2022. Variations in the association between education and self-reported health by race/ethnicity and structural racism. SSM Popul Health 19, 101136. 10.1016/j.ssmph.2022.101136. Published 2022 Jun 2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wrat-3 Wilkinson GS, 1993. WRAT-3: Wide Range Achievement Test Administration Manual. Wide Range Inc., Washington, DC. [Google Scholar]
- Yaffe K, Falvey C, Harris TB, Newman A, Satterfield S, Koster A, et al. , 2013. Effect of socioeconomic disparities on incidence of dementia among biracial older adults: prospective study. BMJ 347, f7051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zahodne LB, Sol K, Kraal Z, 2019. Psychosocial pathways to racial/ethnic inequalities in late-life memory trajectories. J. Gerontol. B Psychol. Sci. Soc. Sci 74 (3), 409–418. 10.1093/geronb/gbx113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zajacova A, Lawrence EM, 2018. The relationship between education and health: reducing disparities through a contextual approach. Annu. Rev. Publ. Health 39, 273–289. 10.1146/annurev-publhealth-031816-044628. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data will be made available on request.