

Abstract
Background:
Epidural spinal cord stimulation (eSCS) restores volitional movement and improves autonomic function after nonpenetrating and traumatic spinal cord injury (SCI). There is limited evidence of its utility for penetrating SCI (pSCI).
Case Description:
A 25-year-old male sustained a gunshot wound (GSW) resulting in T6 motor/sensory paraplegia and complete loss of bowel and bladder function. Following eSCS placement, he regained partial volitional movement and has independent bowel movements 40% of the time.
Conclusion:
A 25-year-old pSCI patient who, following a GSW resulting in T6-level paraplegia, sustained marked recovery of volitional movement and autonomic function following eSCS placement.
Keywords: Epidural spinal cord stimulation, Gunshot wound, Paralysis, Spinal cord injury, Traumatic injury

INTRODUCTION
Penetrating spinal cord injuries (pSCIs), most often from gunshot wounds (GSWs), comprise one-fifth of all spinal cord injuries (SCIs).[2,7] Although epidural spinal cord stimulation (eSCS) has restored volitional movement and autonomic function in patients with nonpSCIs, there is limited literature regarding its efficacy for pSCI. Here, we demonstrate restoration of volitional movement and autonomic function with eSCS in a paraplegic patient secondary to a T6-level GSW.
CASE DESCRIPTION
History and treatment
A 25-year-old male sustained a GSW to the T6 spine (4/2017); the bullet entered his right shoulder, passed through his lung, and ended up in the T6 vertebrae resulting in paraplegia [Figure 1]. He underwent pneumonectomy, but remained with full motor/sensory paraplegia below the T6 level (i.e., complete motor loss, absent temperature/pain sensation, minimal proprioception, and complete loss of anal and bladder sphincter control). Five years later, he wished to undergo eSCS, but due to the retained missile, he was deemed a poor candidate. Therefore, he first underwent a T5-T7 laminectomy for removal of the retained bullet fragment accompanied by the left-sided facetectomies at T5-T6 and T6-T7, and performance of a T4-T8 pedicle/screw fusion. The bullet, lodged extradurally, was removed along with 40% of the T6 vertebral body [Figure 2]. One month later, an eSCS was placed dorsal to the L1-2 vertebral bodies using intraoperative neuromonitoring (i.e., for stimulation of all muscle groups from the iliopsoas to the anterior tibialis, including the anal sphincter) [Figure 3].
Figure 1:

Sagittal view of thoracic spine preoperative computed tomography. Red arrow indicates bullet location.
Figure 2:

Sagittal view of thoracic spine postoperative computed tomography. Red arrow indicates preoperative bullet location.
Figure 3:
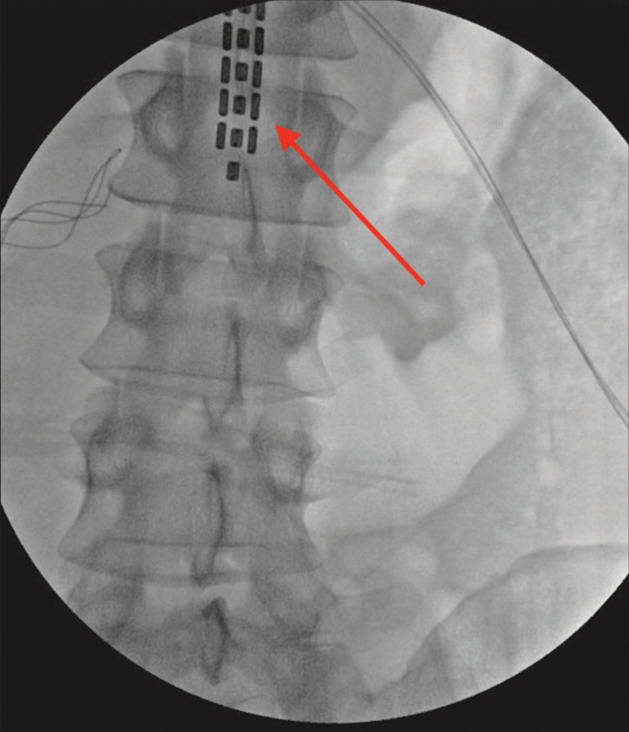
Intraoperative X-ray following epidural spinal cord stimulation placement. Red arrow indicates electrode grid.
Postoperative course and recovery
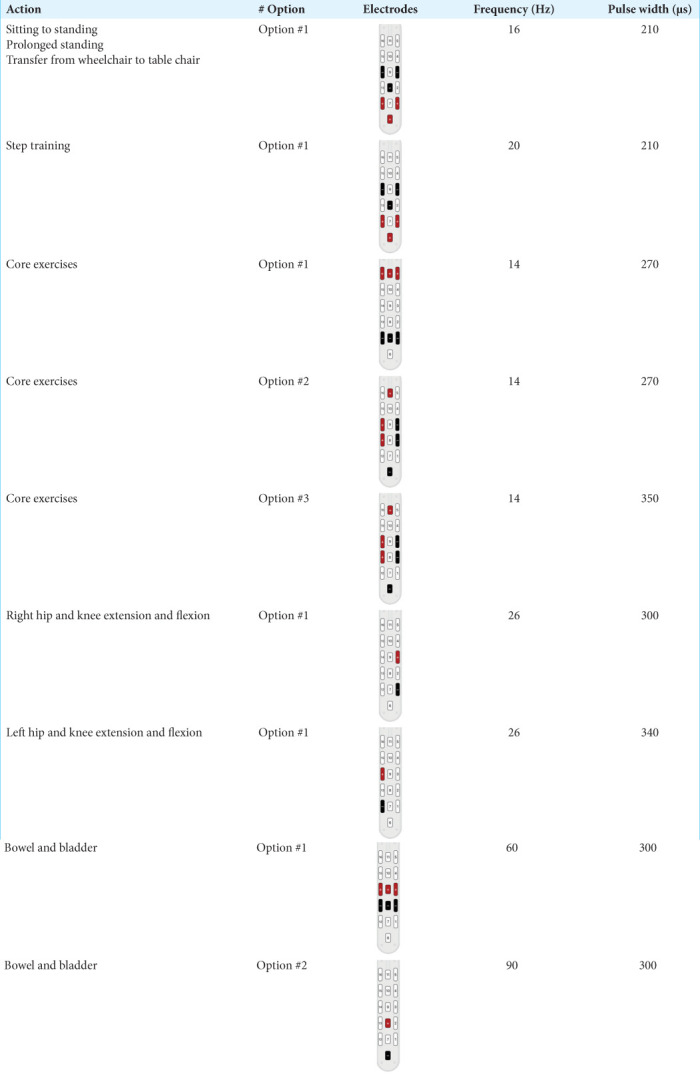
Two days postoperatively, with eSCS turned on, the patient could perform seated knee extension and hip flexion and began physical therapy and walking therapy [Table 1, Videos 1 and 2]. Burst settings of 30 son and 90 s off were utilized for the full awake day 3–4 times/week; these reduced leg spasms and other non-volitional leg movements. Bladder function did not improve, but 40% of the time, he could independently empty his bowels. Further, back pain and other symptoms consistent with complex regional pain syndrome (Type 2) were eliminated.
Table 1:
Stimulation parameters.
First video of patient using epidural spinal cord stimulation along with assisted walking therapy.
Second video of patient using epidural spinal cord stimulation along with assisted walking therapy.
DISCUSSION
Although 80% of patients with blunt spinal cord injuries undergo surgery, only 17% of patients with pSCI have surgery.[1,7] Meta-analyses indicate no difference in recovery between operatively versus conservatively-managed pSCI patients; few in either group show meaningful recovery.[2,4,5,8] eSCS improves autonomic function and restores volitional movement in some SCI patients.[3,5,7] We report a 25-year-old pSCI patient who, following a GSW resulting in paraplegia, sustained marked recovery of function following eSCS placement. We identified four other patients in the literature discussing placement of eSCS for penetrating spinal GSW [Table 2], PRISMA flow diagram is shown in [Figure 4].[3,6] Collectively, these cases suggest that eSCS may possibly have a role in improving outcomes in patients with pSCI; however, further research is necessary to confirm this.
Table 2:
Literature search.

Figure 4:

PRISMA diagram of literature search for previous literature on restoration of volitional movement in gunshot wound patients receiving epidural spinal cord stimulation.
CONCLUSION
This case study shows that a patient with a pSCI attributed to a GSW resulting in total loss of motor and sensory function can benefit from the placement of an epidural spinal cord stimulator.
Footnotes
How to cite this article: Gupta R, Johnson R, Samadani U. Recovery of volitional movement with epidural stimulation after “complete” spinal cord injury due to gunshot: A case report and literature review. Surg Neurol Int 2023;14:68.
Contributor Information
Rishabh Gupta, Email: gupta324@umn.edu.
Reid Johnson, Email: joh18656@umn.edu.
Uzma Samadani, Email: usamadan@umn.edu.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
Dr. Samadani has equity in Oculogica and has received speaking fees from Integra. Abbott and Medtronic have made donations to the J Aron Allen Legacy Foundation, which has donated research money to the laboratory of Dr. Samadani. No other disclosures were reported.
Videos available on:
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Journal or its management. The information contained in this article should not be considered to be medical advice; patients should consult their own physicians for advice as to their specific medical needs.
REFERENCES
- 1.Avila MJ, Martirosyan NL, Hurlbert RJ, Dumont TM. Penetrating spinal cord injury in civilians: Analysis of a national database. World Neurosurg. 2021;146:e985–92. doi: 10.1016/j.wneu.2020.11.059. [DOI] [PubMed] [Google Scholar]
- 2.Bin-Alamer O, Bhenderu LS, Stuebe C, Sagoo NS, Palmisciano P, Haider M, et al. Penetrating spinal cord injury: A systematic review and meta-analysis of clinical features and treatment outcomes. Spinal Cord. 2022;60:845–53. doi: 10.1038/s41393-022-00813-x. [DOI] [PubMed] [Google Scholar]
- 3.Kandhari S, Sharma D, Samuel S, Sharma G, Majumdar P, Edgerton VR, et al. Epidural spinal stimulation enables global sensorimotor and autonomic function recovery after complete paralysis: 1st study from India. IEEE Trans Neural Syst Rehabil Eng. 2022;30:2052–9. doi: 10.1109/TNSRE.2022.3158393. [DOI] [PubMed] [Google Scholar]
- 4.Khorasanizadeh M, Yousefifard M, Eskian M, Lu Y, Chalangari M, Harrop JS, et al. Neurological recovery following traumatic spinal cord injury: A systematic review and meta-analysis. J Neurosurg Spine. 2019;30:683–99. doi: 10.3171/2018.10.SPINE18802. [DOI] [PubMed] [Google Scholar]
- 5.Platt A, Dafrawy MH, Lee MJ, Herman MH, Ramos E. Gunshot wounds to the lumbosacral spine: Systematic review and meta-analysis. Global Spine J. 2022;12:1247–53. doi: 10.1177/21925682211030873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Richardson RR, Cerullo LJ, McLone DG, Gutierrez FA, Lewis V. Percutaneous epidural neurostimulation in modulation of paraplegic spasticity. Six case reports. Acta Neurochir (Wien) 1979;49:235–43. doi: 10.1007/BF01808963. [DOI] [PubMed] [Google Scholar]
- 7.Roach MJ, Chen Y, Kelly ML. Comparing blunt and penetrating trauma in spinal cord injury: Analysis of long-term functional and neurological outcomes. Top Spinal Cord Inj Rehabil. 2018;24:121–32. doi: 10.1310/sci2402-121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Sidhu GS, Ghag A, Prokuski V, Vaccaro AR, Radcliff KE. Civilian gunshot injuries of the spinal cord: A systematic review of the current literature. Clin Orthop Relat Res. 2013;471:3945–55. doi: 10.1007/s11999-013-2901-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
First video of patient using epidural spinal cord stimulation along with assisted walking therapy.
Second video of patient using epidural spinal cord stimulation along with assisted walking therapy.