


Abstract
Placenta accreta spectrum (PAS) disorder is one of the most dangerous conditions that can affect pregnancy and its incidence is increasing secondary to rising cesarean section rates worldwide. The standard treatment is frequently elective hysterectomy at the time of cesarean delivery; however, uterine and fertility preserving surgery is becoming more common. In the pursuit of a reduction in blood loss and associated maternal morbidity, occlusive vascular balloons are increasingly used at the time of surgery, usually placed with fluoroscopic guidance. Occlusive balloons placed in the infrarenal aorta have been shown in the literature to be superior in terms of blood loss and hysterectomy rates than those placed more distally, such as within iliac or uterine arteries. We present the first five cases performed in Europe of ultrasound-guided infrarenal aortic balloon placement before cesarean for PAS disorder, and describe the technique we used, which provided reduced blood loss, a clearer operating field and avoided fetal and maternal exposure to radiation and intravenous contrast.
Keywords: Placenta accrete, Placenta accreta spectrum disorder, Placenta percreta, Aortic balloon occlusion, Ultrasound
INTRODUCTION
Placenta accreta spectrum (PAS) disorder is among the most dangerous conditions affecting pregnancy. The increasing incidence is linked to rising cesarean rates.[1] PAS is associated with high morbidity and mortality rates due to massive maternal hemorrhage and its sequelae. Elective hysterectomy is the standard treatment, but in recent years obstetricians and patients increasingly opt for uterus-preserving techniques. To achieve this, endovascular temporary devascularization methods including occlusion balloon placement in bilateral uterine arteries, internal iliac arteries, common iliac arteries, and the infrarenal aorta may be used. These act as intra-arterial ligatures contributing to a clearer operative field, reduced blood loss, and reduced blood transfusion requirement.[2,3] Most insertion techniques are fluoroscopy guided, performed in an angiography suite followed by transfer to the operating room, risking balloon displacement with patient movement. This case series describes our experiences and technique of performing ultrasound (US)-guided prophylactic abdominal aortic balloon occlusion (PAABO) in PAS in the operating room, a procedure previously reported in small numbers in China only.[4,5]
CASE SERIES
We present five women whose pregnancies were complicated by PAS and had a PAABO placed under US guidance by an interventional radiologist in the obstetric operating room immediately before cesarean delivery in our hospital. Optimal delivery time and strategy were decided in our PAS multidisciplinary meeting, involving obstetricians, interventional radiologists, urologists, anesthetists, and transfusion practitioners. Each woman described had previous cesareans and was diagnosed with PAS antenatally. They provided written consent for inclusion in this case series.
Case 1, aged 32 years, with three previous cesareans transferred to our hospital at 28 weeks’ gestation following an antepartum hemorrhage (APH), due to inexperience in managing PAS in her local hospital. Fetal medicine unit (FMU) US, followed by magnetic resonance imaging (MRI), demonstrated placenta percreta with bladder invasion. After severe abdominal pain and further APH episodes, she received corticosteroids and magnesium sulfate for fetal lung maturation and neuroprotection respectively, and a cesarean was performed at 29 + 1 weeks’ gestation. After combined spinal-epidural (CSE) anesthesia was completed, an endovascular balloon was inserted into the infrarenal abdominal aorta preoperatively under US guidance. Cesarean by fundal uterine incision, with resection of the lower uterine segment and adherent placenta, was performed. A 3 cm area of placental invasion into the bladder was excised and the bladder repaired. Total blood loss was 950 mL, 240 mL of which was retransfused through cell salvage, with a further unit of blood given day 1 postnatally. There were no postoperative complications.
Case 2, aged 34, had two previous cesareans. Routine US examination at 20 weeks demonstrated an anterior low placenta. Her antenatal period was uncomplicated. FMU US and subsequent MRI at 36 weeks’ gestation confirmed PAS with high vascularity between the uterine serosa and bladder with very little myometrium inferior to the placental edge.
Cystoscopy with ureteric stenting and US-guided PAABO insertion was performed preoperatively. Elective cesarean with sterilization was performed at 37 + 5 weeks. Despite large bridging vessels between the placenta and bladder serosa, good hemostatic control allowed lower uterine segment resection with adherent placenta, preserving the uterus. Blood loss was 1250 mL, including 940 mL autotransfused following cell salvage.
Case 3, aged 33, with three previous cesareans was diagnosed with placenta previa at 20 weeks’ gestation. FMU US at 30 weeks and MRI confirmed placenta percreta invading the lower uterine myometrium and entire cervix, with parametrial and extrauterine invasion. She received an iron infusion at 32 weeks for mild anemia and corticosteroids pre-delivery. After cystoscopy, which excluded bladder invasion, ureteric stenting and PAABO were performed followed by an elective cesarean-hysterectomy with ovarian conservation at 34 weeks’ gestation. Estimated blood loss was 500 mL with a post-operative hemoglobin of 102 g/L.
Case 4, aged 37, with three previous cesareans transferred to our unit in late pregnancy. Her placenta percreta extended laterally into the left broad ligament, thereby preventing excision. Following US-guided PAABO insertion and cesarean, a subtotal hysterectomy was performed. Total blood loss was 800 mL, no transfusion was required, and there were no post-operative complications.
Case 5, aged 31, had just one previous cesarean. PAS was identified at 20 + 5 gestation, and she was admitted twice with APH, remaining an inpatient until delivery at 31 + 4. On uterine incision, before delivery of her baby, there was brisk and heavy bleeding, which was controlled post-delivery by inflation of the aortic balloon. This allowed placental excision to be performed followed by sterilization and insertion of a Bakri intrauterine balloon. Estimated blood loss was 3000 mL and she received two units of red cells intraoperatively and two units of plasma, with 455 mL blood collected through cell salvage also transfused. Her hemoglobin fell from 105 g/L to 79 g/L.
Description of radiological technique
Our aortic balloon placement technique uses US (GE Logiq S8) to scan the abdominal aorta and its bifurcation in the left oblique coronal plane using the curvilinear probe (C1−5) [Figure 1]. Using compression with the probe, we partially displace the uterus to the right side, which is easier with abdominal muscle relaxation under CSE anesthesia. A C-arm is kept on standby for aortic balloon placement in case US visualization is unsatisfactory; however, this was not needed in our cases.
Figure 1:
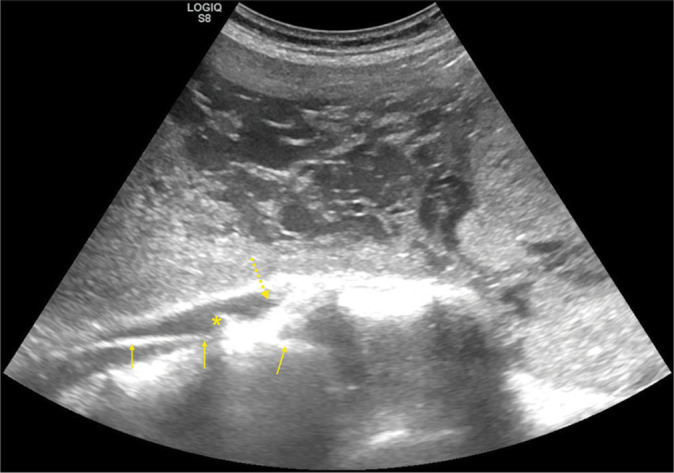
Coronal oblique plane ultrasound image obtained from the left anterolateral aspect with compression to displace the uterus to the right side with the probe after placing an angiographic metallic guidewire via right femoral access showing the guidewire as a linear intravascular reflective structure (yellow arrows) in the infrarenal aorta and right common iliac artery, the location of the aortic bifurcation (asterisk), and the proximal segment of the left common iliac artery (dashed arrows).
The abdomen and right groin are prepared with 2% chlorhexidine in 70% isopropyl alcohol (ChloraPrep, Cardinal Health, Dublin, Ohio, USA) and right femoral retrograde access obtained using US guidance with a linear vascular probe (9L), and an 8F vascular sheath (MeritMedical, South Jordan, Utah, USA) placed. A standard J tipped metallic wire is then inserted and its presence in the aorta confirmed with US. An Atlas balloon measuring either 16 or 18 mm in diameter (depending on aortic measurement on MRI) and 40 mm in length is introduced over the wire and US is used to visualize the balloon movement into the aorta above its bifurcation. The position close to the aortic bifurcation is confirmed using partial non-occlusive expansion of the balloon with 1−2 mL of air, which is seen on US [Figure 2]. When positioning is satisfactory, the guidewire is removed, and a two-way stop cock placed at the guidewire site of the balloon. The vascular sheath and balloon are secured in place with a suture and clear dressings and flushed with 5 mL of heparinized saline (1000 units of unfractionated heparin in 1 L) every 10 min until removal. This procedure takes around 15 min.
Figure 2:
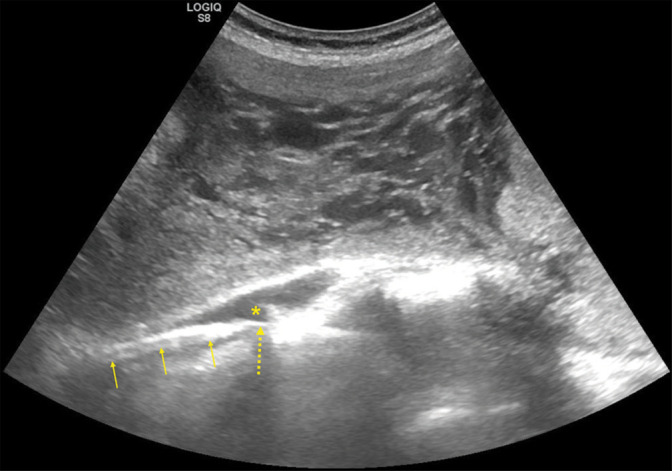
Coronal oblique plane ultrasound image obtained after partial air inflation of an occlusion balloon (yellow arrows) placed over the metallic wire (dashed arrow) just above the aortic bifurcation indicated by the asterisk.
After delivery of the fetus through fundal uterine incision and clamping of the umbilical cord, the balloon is inflated manually with saline (without an inflation device) until minimal resistance is felt to achieve aortic occlusion. The uterus is then closed with the placenta in situ and a decision made whether the placenta can be safely excised, or a hysterectomy required. The balloon inflation cycle involves inflation for 20 min then deflation for 5 min to preserve blood flow to the lower extremities. If a critical step of the surgery is underway like bladder reflection away from the uterus, and bleeding expected on balloon deflation, the balloon is kept inflated for longer, up to a maximum of 40 min. After this the balloon is deflated for 5 min, and the cycle repeated until hysterectomy or uterine closure is complete. Balloon inflation causes a transient increase in blood pressure and the anesthetist is informed every time the balloon is inflated or deflated. After skin closure, the balloon and vascular sheath are removed, and the femoral artery puncture site closed with an 8F Angioseal device (Terumo, Somerset, New Jersey, USA). Doppler examination of tibial arteries in the feet is performed to exclude lower limb embolic complications. None were seen in our patients.
DISCUSSION
The benefit of interventional endovascular radiology techniques in reducing blood loss at cesarean section is well recognized, with intermittent arterial balloon occlusion widely used during high-risk operations.[2,6] Varying levels of efficacy with bilateral internal iliac artery occlusion have been reported in PAS surgery, attributed to the collateral network of blood vessels supplying the uterus, the extent of which increases with more extensive placental invasion.[2,7-9] Multiple studies have demonstrated that bilateral artery or aortic occlusive balloons are most effective in reducing blood loss.[2] They impede blood flow to the placenta more effectively by also reducing blood flow in the obturator, femoral, gluteal, and iliolumbar vessels which supply the placental bed through collaterals.
PAABO performs better than other prophylactic arterial balloon occlusion in terms of blood loss and hysterectomy rates, and the safety of infrarenal PAABO has been demonstrated in a meta-analysis with a reduction in blood loss, blood transfusion requirement, hysterectomy rate, operating time, and post-operative hospital stay when compared with no balloon use.[2,6] In addition, abdominal aortic clamping for 1 h has been demonstrated to be biochemically safe in aneurysm surgery.[10]
Most studies describing PAABO report using fluoroscopy guidance in digital subtraction angiography operating rooms.[2,6,11-13] It has been observed that a lower level of fetal irradiation is required compared with positioning occlusive balloons in internal iliac arteries bilaterally, which requires crossing over the aortic bifurcation twice.[12] Our PAABO insertion method protects the woman and fetus from irradiation and intravenous contrast use completely, with the added logistical benefit of it being performed directly in the obstetric operating room following regional anesthetic.
Insertion of the larger diameter aortic occlusion balloon needs placement of vascular sheaths of either 7 or 8F sizes whereas iliac artery balloon placement can be done through 5F sheaths. However, the latter requires bilateral femoral artery access, while aortic balloons are placed with unilateral femoral access. Thanks to modern vascular closure devices, usage of larger sheaths up to 10F size does not considerably increase access site complications nor prolong operating time.
The most serious complication reported in the literature following PAABO use in PAS surgery is arterial thrombosis, with rates of 0.8−1%.[6,14] A meta-analysis comparing PAABO with more distal balloon occlusion demonstrated a higher rate of thrombosis with the latter, thought in part to be related to a higher degree of blood loss.[2] Studies on aortic clamping duration in abdominal aortic aneurysm or trauma surgeries have shown it to be safe for at least 50 min, and we never exceeded this in our patients.
We use Atlas balloons since they are commonly applied in other interventions in our hospital and are readily available. Any appropriately sized balloon measuring the same as, or 2 mm larger than, the diameter of the infrarenal aorta measured by MRI can be used. Compliant balloons would be safer; and if non-compliant/angioplasty balloons are used, gentle hand inflation instead of an inflation device should be used to prevent aortic dissection/rupture.
Before PAABO use in these five cases, our local audit data since 2005 demonstrated a median blood loss of 2700 mL, with 71% experiencing blood loss >1500 mL. This is consistent with the national median for antenatally diagnosed PAS of 2750 mL.[15] In this series, the average was just 1300 mL, a reduction of over 50% compared to local and national data. As discussed elsewhere, we noticed a significant clinical difference when the aortic balloon was inflated compared to when deflated.[2,12] In comparison to the previous operations without PAABO, the reduced bleeding created a clearer operating field, allowing the surgeons time to carefully divide large areas of bridging vessels and resect the lower uterine segment with minimal blood loss. We did not observe any ischemic or embolic complications. Use of US guided PAABO is now our standard practice and aids placental resection, allowing women the option of uterus and fertility-sparing surgery if desired, and reduces blood transfusion requirement.
CONCLUSION
We present a safe insertion technique for US guided PAABO. This technique has been efficacious when employed in cesarean section for placenta percreta, the most severe form of PAS disorder. Compared with our previous data and that reported in the literature, PAABO use is associated with the lower blood loss and hysterectomy rates, allowing uterine-sparing surgery, with no arterial thrombotic complications in our series. We suggest that US-guided PAABO with prospective auditing of all outcomes should be the gold standard method for achieving uterine devascularization in PAS surgery due to reduced blood loss, rapid insertion speed, insertion ability in the obstetric operating room, and avoidance of fetal and maternal irradiation.
Acknowledgments
We would like to acknowledge the entire PAS multidisciplinary team and give a special thanks to the women who agreed to be part of this case series.
Funding Statement
Financial support and sponsorship
Nil.
Footnotes
How to cite this article: Grewal M, Magro M, Bellam Premnath KP, Bologa S, Otigbah C. Ultrasound-guided prophylactic abdominal aortic balloon occlusion for placenta accreta spectrum disorder: A case series. J Clin Imaging Sci 2023;13:9.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Morlando M, Collins S. Placenta accreta spectrum disorders: Challenges, risks, and management strategies. IJWH. 2020;12:1033–45. doi: 10.2147/IJWH.S224191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Shahin Y, Pang C. Endovascular interventional modalities for haemorrhage control in abnormal placental implantation deliveries: A systematic review and meta-analysis. Eur Radiol. 2018;28:2713–26. doi: 10.1007/s00330-017-5222-0. [DOI] [PubMed] [Google Scholar]
- 3.Zheng W, Dou R, Yan J, Yang X, Zhao X, Chen D, et al. Intra-abdominal aortic balloon occlusion in the management of placenta percreta. Chin Med J. 2022;135:441–6. doi: 10.1097/CM9.0000000000001944. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Chen K, Li F, Jun E, Xie K, Li W, Zhang M, et al. Ultrasound-guided balloon occlusion in 13 cases of dangerous placental previa cesarean section. J Interv Radiol. 2017;26:915–7. [Google Scholar]
- 5.Wei L, Gong G, Chen J, Hou P, Li Q, Zheng Z, et al. Application of lower abdominal aorta balloon occlusion technique by ultrasound guiding during caesarean section in patients with pernicious placenta previa. Zhonghua Yi Xue Za Zhi. 2018;98:930–4. doi: 10.3760/cma.j.issn.0376-2491.2018.12.011. [DOI] [PubMed] [Google Scholar]
- 6.Chen L, Wang X, Wang H, Li Q, Shan N, Qi H. Clinical evaluation of prophylactic abdominal aortic balloon occlusion in patients with placenta accreta: A systematic review and meta-analysis. BMC Pregnancy Childbirth. 2019;19:30. doi: 10.1186/s12884-019-2175-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chou M, Kung H, Hwang J, Chen W, Tseng J. Temporary prophylactic intravascular balloon occlusion of the common iliac arteries before cesarean hysterectomy for controlling operative blood loss in abnormal placentation. Taiwan J Obstet Gynecol. 2015;54:493–8. doi: 10.1016/j.tjog.2014.03.013. [DOI] [PubMed] [Google Scholar]
- 8.Ono Y, Murayama Y, Era S, Matsunaga S, Nagai T, Osada H, et al. Study of the utility and problems of common iliac artery balloon occlusion for placenta previa with accreta. J Obstet Gynaecol Res. 2018;44:456–62. doi: 10.1111/jog.13550. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Levine AB, Kuhlman K, Bonn J. Placenta accreta: Comparison of cases managed with and without pelvic artery balloon catheters. J Matern Fetal Med. 1999;8:173–6. doi: 10.3109/14767059909020484. [DOI] [PubMed] [Google Scholar]
- 10.Westman B, Johansson G, Söderlund K, Wernerman J, Hammarqvist F. Muscle glutathione metabolism during ischemia and reperfusion in patients undergoing aorto-bifemoral bypass surgery. Acta Anaesthesiol Scand. 2006;50:699–705. doi: 10.1111/j.1399-6576.2006.01021.x. [DOI] [PubMed] [Google Scholar]
- 11.Wu Q, Liu Z, Zhao X, Liu C, Wang Y, Chu Q, et al. Outcome of pregnancies after balloon occlusion of the infrarenal abdominal aorta during caesarean in 230 patients with placenta praevia accreta. Cardiovasc Intervent Radiol. 2016;39:1573–9. doi: 10.1007/s00270-016-1418-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Mei Y, Zhao H, Zhou H, Jing H, Lin Y. Comparison of infrarenal aortic balloon occlusion with internal iliac artery balloon occlusion for patients with placenta accreta. BMC Pregnancy Childbirth. 2019;19:147. doi: 10.1186/s12884-019-2303-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Zhu H, Wang S, Shi J, Yao L, Wang L, Chen H, et al. Prophylactic endovascular balloon occlusion of the aorta in cases of placenta accreta spectrum during caesarean section: points from the anaesthesiologist's perspective. BMC Pregnancy Childbirth. 2020;20:446. doi: 10.1186/s12884-020-03136-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wang Y, Jiang T, Huang G, Han X, Chen Z, Liu C, et al. Long-term follow-up of abdominal aortic balloon occlusion for the treatment of pernicious placenta previa with placenta accreta. J Intervent Med. 2020;3:34–6. doi: 10.1016/j.jimed.2020.01.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Fitzpatrick KE, Sellers S, Spark P, Kurinczuk JJ, Brocklehurst P, Knight M. The management and outcomes of placenta accreta, increta, and percreta in the UK: A population-based descriptive study. BJOG. 2014;121:62–71. doi: 10.1111/1471-0528.12405. [DOI] [PMC free article] [PubMed] [Google Scholar]