

STRUCTURED ABSTRACT
Objective:
Examine longitudinal changes in trunk, hip, and knee kinematics in maturing boys during an unanticipated cutting task.
Design:
Prospective cohort study
Setting:
Biomechanical laboratory
Participants:
42 high-school male basketball, volleyball, and soccer athletes
Assessment of Risk Factors:
Trunk, hip, and knee range-of-motion, peak angles, and angles at initial contact during an unanticipated 45° sidestep cutting task were estimated using laboratory-based three-dimensional optoelectronic motion capture. Maturation was classified using a modified Pubertal Maturational Observational Scale (PMOS) into pre-, mid-, or post-pubertal stages.
Main Outcome Measures:
Trunk total range-of-motion (RoM) in frontal, sagittal, and transverse planes; peak trunk flexion, right lateral flexion and right rotation angles; hip total RoM in frontal, sagittal, and transverse planes; hip flexion angle at initial contact; peak hip flexion and adduction angles; knee total RoM in frontal, sagittal, and transverse planes; knee flexion angle at initial contact; peak knee flexion and abduction angles.
Results:
As boys matured, there was a decrease in hip sagittal-plane RoM (49.02° to 43.45°, Benjamini-Hochberg adjusted p-value=0.027), hip flexion at initial contact (29.33° to 23.08°, p=0.018), and peak hip flexion 38.66° to 32.71°, p=0.046), and an increase in trunk contralateral rotation (17.47° to 25.05°, p=0.027).
Conclusions:
Maturing male athletes adopted a more erect cutting strategy that is associated with greater knee joint loading. Knee kinematic changes that increase knee joint loading were not observed in this cohort.
Keywords: knee injuries, change of direction, sport, puberty, biomechanics
Introduction
The risk of anterior cruciate ligament (ACL) injuries increases by up to 70% as boys mature.1 Studies have suggested that this might be due to disproportionate neuromuscular responses to musculoskeletal growth during maturation.2, 3 However, not much is known about the exact neuromuscular responses that increase knee joint loading especially those that occur during cutting movements. Cutting movements are of great interest because the majority of non-contact ACL injuries occur during these change-of-direction, pressing, and evading situations.4, 5 Investigating and understanding the effects of puberty and maturation on cutting technique is necessary because of the significant health, societal, and economic burdens of these devastating injuries. For example, the odds of developing knee osteoarthritis in the ACL-injured knee is four to six times greater compared to the non-injured knee,6 and it costs more than $90,000 USD for each ACL-injured individual to gain a quality-adjusted life year.7 Investigation and understanding the effects of puberty and maturation on cutting technique is necessary to inform injury countermeasures, especially in high risk groups like young athletes.
There is longitudinal evidence suggesting the emergence of kinematics like greater knee abduction angles in maturing females during landing tasks but not in males.8, 9 Knee abduction angles are a modifiable risk factor for ACL injuries and greater angles have been shown to predict non-contact ACL injuries.10 When looking at cutting tasks, a recent study also found that maturing female athletes demonstrated decreased sagittal-plane hip range-of-motion (ROM), decreased peak hip flexion angles, and decreased peak knee flexion angles and abduction angles that are all associated with greater knee joint loading.11 However, no study has longitudinally investigated changes in cutting kinematics in maturing male athletes. To help practitioners identify kinematics associated with greater knee joint loading that emerge across puberty in young male athletes, the objective of this study was to examine longitudinal changes in trunk, hip, and knee kinematics in maturing boys during an unanticipated cutting task.
Methods
Participants
The study is a secondary analysis of data from a cohort study conducted between 2004 to 2008 that investigated trunk and lower limb biomechanics of 1057 (790 female, 267 male) high-school athletes during an unanticipated cutting task.12 Study participants were basketball, volleyball, and soccer athletes representing more than 95% of the high school athletes participating in these respective sports within an entire county in a Midwestern state of the United States of America. Participants had no previous history of knee ligament injuries or surgeries. For this study, only participants with data across two or all three pubertal stages (pre-, mid-, post-pubertal) were included. Investigation protocols were reviewed and approved by the local institutional review board. Written athlete and parent or guardian consent for study participation were obtained prior to study participation. Participants or public partners were not involved in the design, conduct, or interpretation of this study. We conducted an a posteriori power analysis based on data examined at between session reliability of lower limb kinematic estimates,13 and statistically significant changes in knee abduction range-of-motion following a six-week anterior cruciate ligament injury prevention program,14 and determined that a sample size of 13 athletes in each group was adequate to achieve 80% power at α = 0.05 with an effect size of 0.88.
Participants’ weight was measured on a calibrated physician scale and height was measured with a stadiometer. Weight and height were used to calculate Body Mass Index (BMI) as weight (kg) divided by height squared (cm2). A modified Pubertal Maturational Observational Scale (PMOS) was used to classify each participant into 1 of 3 pubertal stages (pre-pubertal or Tanner Stage 1, mid-pubertal or Tanner Stages 2-3, and post-pubertal or Tanner Stages 4-5).15 The PMOS has been shown to provide reliable assessments of pubertal status.2, 16, 17 The PMOS was applied through a parental questionnaire and clinical observations performed by a single investigator. When participants attended multiple sessions from the same pubertal stages, we only included the session with the larger timespan between data collection points. In other words, if a participant attended three testing sessions, two in pre-pubertal and one in mid-pubertal stages, we only considered the pre-pubertal data collected at the earlier date.
Experimental protocol
The three-dimensional optoelectronic motion capture testing protocol and processing procedures were previously described.8, 12 Briefly, thirty-seven retroreflective markers were placed on each participant by the same researcher in the following anatomical locations: sacrum, left posterior superior iliac spine, and sternum and then bilaterally on the shoulder, elbow, wrist, anterior superior iliac spine, greater trochanter, mid-thigh, medial and lateral knee, tibial tubercle, mid-shank, distal shank, medial and lateral ankle, heel, dorsal surface of the mid-foot, lateral foot (fifth metatarsal), and toe (between second and third metatarsals). These markers were tracked by a 10-camera motion analysis system (Eagle; Motion Analysis Corp., Santa Rosa, CA) and two force platforms (AMTI, Watertown, MA). Video and force data were time-synchronized and collected at 240 Hz and 1200 Hz, respectively. Data was then processed using the EvaRT software (v4; Motion Analysis, Santa Rosa, CA) and analyzed in Visual3D (version 4.0; C-Motion, Inc.). Static models were customized for each participant in Visual3D and three-dimensional marker trajectories from each trial were calculated according to the Cardan/Euler rotation sequence and filtered at a cut-off frequency of 12 Hz. The model consisted of eight skeletal segments including the trunk, pelvis, and bilateral foot, shank, and thigh segments. Kinematic analysis was optimized using a global least-squares approach. Sagittal, coronal, and transverse plane joint rotations at the trunk were calculated relative to the lab coordinate system, while hip and knee rotations were calculated and expressed relative to a neutral position where all segment axes were aligned. Initial contact (IC) was defined as the moment the participant jumped forward to land on the force plates and generated a vertical ground reaction force (VGRF) that exceeded 10N. Toe off was calculated after IC when the VGRF falls below 10N.
For the unanticipated cutting task, each participant was instructed to start in an athletic position with feet 36cm apart (Fig. 1). A custom computer program would then cue athletes using a traffic-light system to initiate a forward jump of 40cm to land on 2 separate force platforms. Three hundred milliseconds after the initiation of the forward jump, a randomized arrow (indicating left or right cutting directions) would appear on the monitor directing the participant to perform a 45° sidestep cut in the indicated direction as quickly as possible through a 61cm gate that was placed 2.5 m away.12, 18 Each participant performed six cutting trials (right and left cut direction randomized). Trials were excluded if the participant performed the cut in the wrong direction, performed a crossover cut, or if the entire foot did not land on the force plate. Only left-directed cuts (landing on the right foot and cutting to the left) were analyzed as 93% of the participants were right foot dominant and the effect of limb dominance on cutting biomechanics is still inconclusive as to whether a particular limb is more susceptible to injury 19.
Figure 1 -.
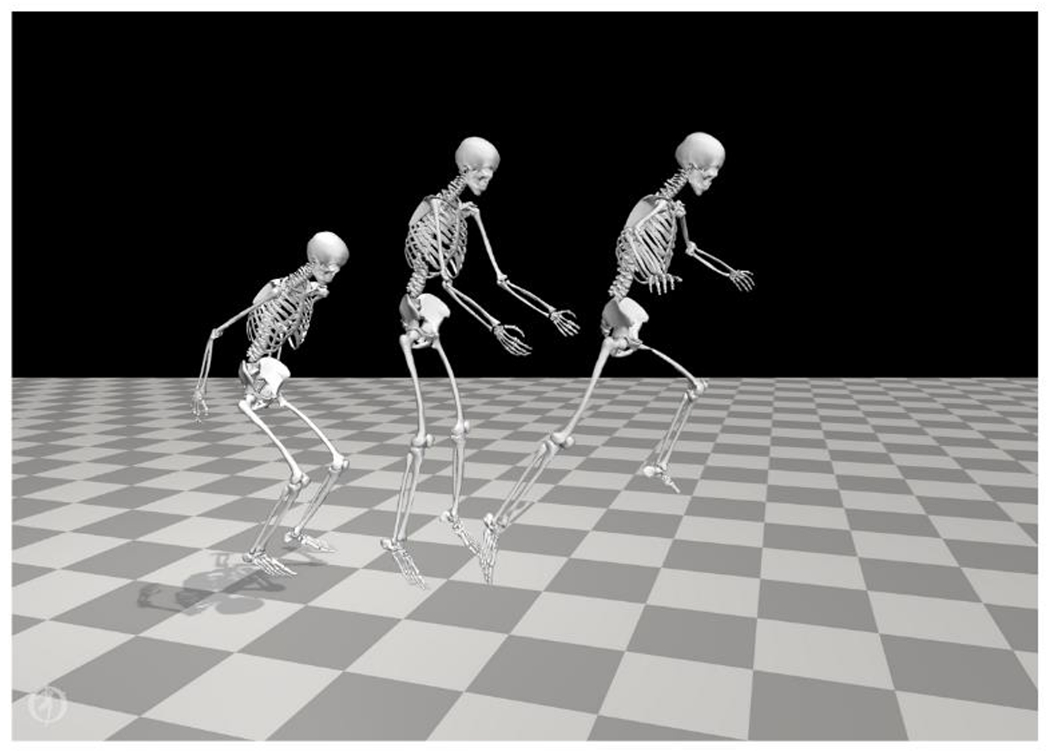
Jump-stop, unanticipated 45° sidestep cutting task
Independent variables
Based on existing reports of trunk and lower limb kinematics associated with increased knee injury risk, the following independent variables were identified for our analyses 12, 20, 21: Trunk total range-of-motion (ROM) in frontal, sagittal, and transverse planes; peak trunk flexion, right lateral flexion and right rotation angles; hip total RoM in frontal, sagittal, and transverse planes; hip flexion angle at initial contact; peak hip flexion and adduction angles; knee total RoM in frontal, sagittal, and transverse planes; knee flexion angle at initial contact; peak knee flexion and abduction angles.
Statistical analyses
Changes in independent variables across three pubertal transitions were compared using linear mixed models and pairwise comparisons (pre- to mid-pubertal, pre- to post-pubertal, and mid- to post-pubertal). For missing data, listwise deletions removed the row of values when an observation was missing, followed by maximum likelihood estimates of the model parameters.22, 23 Linear mixed models have also been successfully used in studies with similar purposes.11, 24 The Benjamini-Hochberg (B-H) method was used to control for the false discovery rate.25 Alpha levels for all statistical tests were set at α ≤ 0.05. Data analyses were performed in R (version 3.6.1 and later, R Foundation for Statistical Computing, Vienna: Austria) using the tidyverse, emmeans, and lm4 packages.
Results
Forty-two boys were included in the analyses (Table 1). These boys may be accounted for in two or three pubertal transitions depending on the number of pubertal stages each boy experienced over the course of data collection. Sixteen boys were accounted for in the pre- to mid-pubertal transition, 26 in mid- to post-pubertal, eight in pre- to post-pubertal, and four across all three stages (Table 2). The average time between measurements was 1.3 years for pre- to mid-pubertal stages, 1.4 years for mid-to post-pubertal stages, and 2.7 years for pre- to post-pubertal stages (Table 2).
Table 1 -.
Participant characteristics in each pubertal group
| Groups | Pre-pubertal (± SD) | Mid-pubertal (± SD) | Post-pubertal (± SD) |
|---|---|---|---|
| n | 20 | 38 | 30 |
| Age, y | 12.3 ± 0.5 | 13.6 ± 1.0 | 15.0 ± 1.2 |
| Height, cm | 158.0 ± 7.9 | 168.7 ± 7.8 | 178.3 ± 7.1 |
| Weight, kg | 48.1 ± 9.4 | 56.2 ± 8.9 | 68.4 ± 9.3 |
| BMI, kg/m2 | 19.2 ± 2.9 | 19.7 ± 2.3 | 21.5 ± 2.5 |
Table 2 -.
Number of complete and missing data per pubertal transition
| Transitions | Pre- to mid-pubertal | Mid- to post-pubertal | Pre- to post-pubertal | |||
|---|---|---|---|---|---|---|
| Pre | Mid | Mid | Post | Pre | Post | |
| Total participants | 20 | 38 | 38 | 30 | 20 | 30 |
| Missing data | 4 | 22 | 12 | 4 | 12 | 22 |
| Complete data | 16 | 26 | 8 | |||
There was a decrease in hip sagittal-plane RoM as boys matured from pre- to post-puberty (means: 49.02° to 43.45°, B-H adjusted p-value = 0.027) (Table 3). There were no statistically significant changes in trunk and knee joint RoM across puberty.
Table 3 -.
Means (°) of joint angles for pre-pubertal, mid-pubertal, and post-pubertal stages and results of linear mixed models analyses comparing pre- to mid-pubertal, mid- to post-pubertal, and pre- to post-pubertal stages.
| Joint | Plane/Movement | Mean (95% CI) | Pubertal Stage | MD (95% CI) | p-value | B-H | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Mid | Post | I | J | ||||||
| RoM (Total) | Trunk | Frontal | 26.88 (24.31, 29.45) | 24.52 (22.61, 26.42) | 23.13 (21.01, 25.25) | Pre | Mid | 2.37 (−0.90, 5.62) | 0.197 | 0.626 |
| Pre | Post | 3.75 (−0.21, 7.28) | 0.035 | 0.189 | ||||||
| Mid | Post | 1.38 (−1.30, 4.07) | 0.433 | 1.000 | ||||||
| Sagittal | 15.01 (12.50, 17.51) | 16.48 (14.62, 18.35) | 17.61 (15.54, 19.68) | Pre | Mid | −1.48 (−4.64, 1.68) | 0.502 | 1.000 | ||
| Pre | Post | −2.60 (−6.03, 0.82) | 0.170 | 0.574 | ||||||
| Mid | Post | −1.13 (−3.73, 1.47) | 0.551 | 1.000 | ||||||
| Transverse | 22.61 (19.52, 25.70) | 25.25 (22.88, 27.62) | 28.07 (25.47, 30.67) | Pre | Mid | −2.64 (−6.37, 1.09) | 0.212 | 0.636 | ||
| Pre | Post | −5.46 (−9.52, 1.40) | 0.006 | 0.054 | ||||||
| Mid | Post | −2.81 (−5.87, 0.23) | 0.075 | 0.337 | ||||||
| Hip | Frontal | 18.62 (16.79, 20.47) | 18.46 (17.18, 19.75) | 18.73 (17.26, 20.21) | Pre | Mid | 0.17 (−2.35, 2.68) | 0.987 | 1.000 | |
| Pre | Post | −0.11 (−2.80, 2.59) | 0.995 | 1.000 | ||||||
| Mid | Post | −0.27 (−2.38, 1.84) | 0.949 | 1.000 | ||||||
| Sagittal | 49.02 (46.04, 52.00) | 43.94 (41.85, 46.02) | 43.45 (41.06, 45.83) | Pre | Mid | 5.08 (−1.00, 9.16) | 0.011 | 0.066 | ||
| Pre | Post | 5.57 (−1.20, 9.95) | 0.001 | 0.027* | ||||||
| Mid | Post | 0.49 (−2.93, 3.91) | 0.937 | 1.000 | ||||||
| Transverse | 18.64 (16.23, 21.05) | 18.46 (16.70, 20.22) | 17.56 (15.59, 19.53) | Pre | Mid | 0.18 (−2.93, 3.29) | 0.990 | 1.000 | ||
| Pre | Post | 1.08 (−2.29, 4.45) | 0.722 | 1.000 | ||||||
| Mid | Post | 0.90 (−1.67, 3.48) | 0.676 | 1.000 | ||||||
| Knee | Frontal | 8.37 (7.44, 9.30) | 8.41 (7.74, 9.08) | 8.07 (7.32, 8.82) | Pre | Mid | −0.04 (−1.27, 1.18) | 0.996 | 1.000 | |
| Pre | Mid | 0.30 (−1.02, 1.62) | 0.849 | 1.000 | ||||||
| Mid | Post | 0.34 (−0.67, 1.36) | 0.696 | 1.000 | ||||||
| Sagittal | 46.35 (43.40, 49.30) | 45.17 (42.94, 47.40) | 45.57 (43.12, 48.03) | Pre | Mid | 1.18 (−2.46, 4.83) | 0.716 | 1.000 | ||
| Pre | Post | 0.78 ( −3.18, 4.74) | 0.884 | 1.000 | ||||||
| Mid | Post | −0.40 (−3.39, 2.59) | 0.944 | 1.000 | ||||||
| Transverse | 21.89 (19.48, 24.30) | 21.19 (19.39, 22.98) | 21.41 (19.42, 23.40) | Pre | Mid | 0.70 (−2.33, 3.73) | 0.842 | 1.000 | ||
| Pre | Post | 0.48 (−2.81, 3.77) | 0.935 | 1.000 | ||||||
| Mid | Post | −0.23 (−2.72, 2.27) | 0.974 | 1.000 | ||||||
| Joint Angle (IC) | Hip | Flexion | 29.33 (26.15, 32.51) | 23.08 (20.72, 25.44) | 22.23 (19.61, 24.86) | Pre | Mid | 6.25 (−2.24, 10.26) | 0.001 | 0.018* |
| Pre | Post | 7.10 (−2.75, 11.45) | <0.001 | 0.054 | ||||||
| Mid | Post | 0.85 (−2.45, 4.15) | 0.810 | 1.000 | ||||||
| Knee | Flexion | 24.36 (20.65, 28.08) | 23.21 (20.27, 26.15) | 24.60 (20.65, 28.08) | Pre | Mid | 1.15 (−3.12, 5.42) | 0.793 | 1.000 | |
| Pre | Post | 0.24 (−2.42, 4.90) | 0.992 | 1.000 | ||||||
| Mid | Post | −1.39 (−4.86, 2.08) | 0.601 | 1.000 | ||||||
| Joint Angle (Peak) | Trunk | Flexion | 41.94 (39.28, 44.59) | 38.75 (36.71, 40.78) | 37.14 (34.91, 39.37) | Pre | Mid | 3.19 (−0.03, 6.41) | 0.05 | 0.245 |
| Pre | Post | 4.80 (−1.29, 8.30) | 0.005 | 0.054 | ||||||
| Mid | Post | 1.60 (−1.03, 4.24) | 0.314 | 0.848 | ||||||
| Lateral Flexion | 18.26 (15.18, 21.35) | 17.04 (14.79, 19.29) | 15.35 (12.83, 17.87) | Pre | Mid | 1.22 (−2.79, 5.23) | 0.745 | 1.000 | ||
| Pre | Post | 2.91 (−1.42, 7.25) | 0.248 | 0.705 | ||||||
| Mid | Post | 1.69 (−1.63, 5.00) | 0.442 | 1.000 | ||||||
| Contralat Rotation | 17.47 (13.77, 21.17) | 21.89 (19.19, 24.58) | 25.05 (22.03, 28.07 | Pre | Mid | −4.42 (−9.21, 0.37) | 0.077 | 0.320 | ||
| Pre | Post | −7.58 (−12.77, 2.40) | 0.002 | 0.027* | ||||||
| Mid | Post | −3.16 (−7.13, 0.80) | 0.142 | 0.511 | ||||||
| Hip | Flexion | 38.66 (35.16, 42.16) | 32.71 (30.14, 35.28) | 32.65 (29.78, 35.52) | Pre | Mid | 5.95 (−1.46, 10.43) | 0.006 | 0.046* | |
| Pre | Post | 6.01 (−1.15, 10.86) | 0.011 | 0.074 | ||||||
| Mid | Post | 0.06 (−3.64, 3.76) | 0.100 | 0.386 | ||||||
| Adduction | 5.72 (3.86, 7.59) | 6.33 (5.02, 7.63) | 6.19 (4.70, 7.68) | Pre | Mid | −0.61 (−3.15, 1.94) | 0.836 | 1.000 | ||
| Pre | Post | −0.47 (−3.21, 2.27) | 0.911 | 1.000 | ||||||
| Mid | Post | 0.14 (−2.00, 2.27) | 0.987 | 1.000 | ||||||
| Knee | Flexion | 56.14 (52.96, 59.32) | 56.75 (54.17, 59.33) | 56.79 (54.02, 59.55) | Pre | Mid | −0.61 (−4.10, 2.87) | 0.906 | 1.000 | |
| Pre | Post | −0.65 (−4.46, 3.16) | 0.912 | 1.000 | ||||||
| Mid | Post | −0.03 (−2.86, 2.79) | 1.000 | 1.000 | ||||||
| Abduction | 7.62 (5.97, 9.26) | 8.28 (6.88, 9.69) | 8.27 (6.79, 9.75) | Pre | Mid | −0.67 (−2.28, 0.95) | 0.584 | 1.000 | ||
| Pre | Post | −0.65 (−2.42, 1.12) | 0.650 | 1.000 | ||||||
| Mid | Post | 0.01 (−1.29, 1.32) | 1.000 | 1.000 | ||||||
Abbreviations: BMI, Body Mass Index; SD, standard deviation; RoM, Range of Motion; I, pubertal stage (control); J, pubertal stage (comparator); Contralat rotation, contralateral rotation or rotation away from intended direction and toward the stance leg; MD, mean difference = I – J; BH, Benjamini-Hochberg adjusted p-value;
, statistical significance (α ≤ 0.05); IC, initial contact.
There was a reduction in hip flexion at initial contact from pre- to mid-puberty (29.33° to 23.08°, B-H adjusted p-value = 0.018) (Table 3). There were no statistically significant changes in knee joint angles at initial contact across puberty.
Boys displayed a reduction in peak hip flexion as they matured from pre- to mid-puberty (38.66° to 32.71°, B-H adjusted p-value = 0.046) and an increase in trunk contralateral rotation from pre- to post-puberty (17.47° to 25.05°, B-H controlled p-value = 0.027) (Table 3). There were no statistically significant changes in peak knee joint angles across puberty.
Discussion
The objective of this study was to examine longitudinal changes in trunk, hip, and knee kinematics in maturing boys during a jump-stop, unanticipated 45° sidestep cutting task. As boys matured, we observed a reduction in hip flexion at initial contact, peak hip flexion, and hip flexion RoM indicating a more erect hip-driven cutting strategy. There was also an increase in peak trunk contralateral rotation. These findings were statistically significant and greater than the typical error between testing sessions, which ranged between 0.9 to 3.2° depending on the variable.13 We did not observe changes in knee kinematics associated with greater knee joint loading, such as greater knee abduction, internal rotation, and flexion.
A reduction in hip sagittal-plane RoM, hip flexion at initial contact and peak hip flexion suggests a more erect cutting strategy associated with greater knee joint loading and ACL injury risk.12, 20, 26 However, decreased hip flexion is also related to shorter task completion times and faster exit velocities.27 Athletes might have developed (instructed or self-directed) a more erect cutting posture to mask and delay their intentions in order to increase their success in pressing and evading situations in sport.28 This reduction in hip sagittal-plane RoM, hip flexion at initial contact and peak hip flexion was only seen in boys as they matured from pre- to mid-puberty, but not as they matured from pre- to post-puberty. Because of the fewer complete data points (Table 2) for pre- to post-pubertal analyses, further research is required to confirm the emergence of this phenomenon. Further investigation is also required to clarify this ‘performance-injury conflict’ to guide the coaching of cutting technique.27
Knee abduction, internal rotation, and flexion angles have a direct influence on the strain and force experienced by the ACL but these changes were not observed in this cohort. In the frontal- and transverse-planes, greater knee abduction and internal rotation angles are commonly observed around initial stance knee contact and is the most common mechanism for ACL injuries.4, 10, 29 In the sagittal-plane, decreased knee flexion indicates preferential contraction of the quadriceps muscle over the hamstring muscle to stabilize the knee joint which leads to greater anterior shear stress on the ACL.30, 31 In comparison, maturing female athletes demonstrated clear increases in peak knee abduction11 which might partially explain why ACL injury incidence is almost two times higher in girls compared to boys of the same age group.1 Additional longitudinal investigation of the effect of maturation on knee biomechanics in a larger cohort of males would be required to further substantiate this finding.
We observed an increase in peak trunk contralateral rotation (rotation away from intended direction and toward the stance leg) but are not certain about the implications of this finding on knee injury risk. There is evidence that rotation of the trunk away from the intended cutting direction is linked to greater ipsilateral knee joint loads but this observation was identified in anticipated cutting conditions.32 Two-dimensional video analyses of ACL injuries also report the trunk to be rotating toward, and not away from, the intended direction at the point of injury.4, 33 Additionally, it is not clear if these observations were made from sidestep, crossover, or a combination of both cutting maneuvers.4, 33 Girls from the same cohort displayed an increase in trunk transverse-plane RoM but not peak trunk contralateral rotation.11 Unlike the relationship between sagittal- and frontal-plane trunk movements and knee injury risk,20, 27 the relationship between trunk transverse-plane movements and knee injuries is not clear. Further studies investigating trunk transverse-plane movements during cutting in ecologically valid settings that consider task- and environmental-constraints may be required.34
There is a paucity of longitudinal studies investigating changes in cutting kinematics across puberty in boys 35 and to our knowledge, this is the first study to do so. Longitudinal studies are important for exploring time-varying risk factors across puberty. We used an unanticipated experimental task to better mimic sporting constraints.36 To reduce measurement error, a single investigator was responsible for marker placement throughout the entire data collection process. There were also some limitations to our study. The unanticipated jump-stop, unanticipated 45° sidestep cutting task that was chosen has inherent limitations and may more relevant for basketball players than volleyball and soccer players. It was chosen, however, because it is easier to standardize across both participants and between study visits within each participant which is important for longitudinal studies. Because we mainly recruited incoming high-school athletes, it meant that most participants presented in the mid- to post-pubertal stages resulting in a smaller sample size for the pre- to post-pubertal group. The discrete variables we used in the analyses do not fully represent the complexity of cutting biomechanical data. Using statistical parametric mapping methods can aid in the objective characterization of waveform features. Kinetic data were also not analyzed and would have afforded further insight into this research question. Participation in exercise-based injury risk reduction programs could have the potential to confound the findings and this was not fully reported by this participant cohort. Inter-session reliability of biomechanical data collection, soft-tissue artefact and marker occlusion may result in inaccuracies during data collection. Finally, it is still not known if the same biomechanical models are valid over time with changing anatomy and morphology.
Changes in cutting kinematics alone will not fully explain the causes of ACL injuries, as these injuries are complex emergent phenomena resulting from multiple non-linear interactions within a web of determinants. Future research should consider intensive longitudinal assessments of multiple injury determinants in a larger cohort. Cutting biomechanics is one such injury determinant, but assessment of biomechanics in a laboratory-based setting is time-consuming and expensive. Inertial measurement units and markerless motion capture are promising alternatives that could be considered because they are cheaper and have shorter data collection and processing times.37
While a more erect cutting strategy is associated with greater knee joint loading, maturing male athletes may have adopted this strategy to improve cutting performance. Knee kinematic changes that increase knee joint loading were not observed in this cohort. Changes in cutting kinematics alone will not fully explain the greater ACL injury risk in maturing males.
Conflict of Interest Disclosure
GDM has consulted with Commercial entities to support application to the US Food and Drug Administration but has no financial interest in the commercialization of the products. GDM’s institution receives current and ongoing grant funding from National Institutes of Health/NIAMS Grants U01AR067997, R01 AR070474, R01AR055563, R01AR076153 and industry sponsored research funding related to brain injury prevention and assessment with Q30 Innovations, LLC, and ElMinda, Ltd. GDM receives author royalties from Human Kinetics and Wolters Kluwer. GDM is an inventor of biofeedback technologies (2017 Non Provisional Patent Pending- Augmented and Virtual reality for Sport Performance and Injury Prevention Application filed 11/10/2016 (62/420,119), Software Copyrighted.) designed to enhance rehabilitation and prevent injuries and has potential for future licensing royalties. The authors acknowledge fund support for this project from the National Institutes of Health grants 5SC3 GM102053 (GDM, TEH, KRF, EP).
Footnotes
Ethical Compliance
This study is exempted from ethical review with a waiver granted by The University of Sydney’s Human Research Ethics Committee. The waiver was granted based on the National Health and Medical Research Council’s (NHMRC) National Statement on Ethical Conduct in Human Research which states that ethical review committees may choose to exempt research from ethical review which meets the following criteria: (a) Is negligible risk research (as defined in paragraph 2.1.7); and (b) involves the use of existing collections of data or records that contain only non-identifiable data about human beings (as defined in paragraph 5.1.22)
REFERENCES
- 1.Sanders TL, Maradit Kremers H, Bryan AJ, et al. Incidence of anterior cruciate ligament tears and reconstruction: a 21-year population-based study. The American Journal of Sports Medicine. 2016; 44(6):1502–1507. [DOI] [PubMed] [Google Scholar]
- 2.Quatman CE, Ford KR, Myer GD, Hewett TE. Maturation leads to gender differences in landing force and vertical jump performance: a longitudinal study. The American Journal of Sports Medicine. 2006; 34(5):806–813. [DOI] [PubMed] [Google Scholar]
- 3.Hewett TE, Myer GD, Ford KR. Decrease in neuromuscular control about the knee with maturation in female athletes. JBJS. 2004; 86(8):1601–1608. [DOI] [PubMed] [Google Scholar]
- 4.Della Villa F, Buckthorpe M, Grassi A, et al. Systematic video analysis of ACL injuries in professional male football (soccer): injury mechanisms, situational patterns and biomechanics study on 134 consecutive cases. British journal of sports medicine. 2020; 54(23):1423–1432. [DOI] [PubMed] [Google Scholar]
- 5.Carlson VR, Sheehan FT, Boden BP. Video analysis of anterior cruciate ligament (ACL) injuries: a systematic review. JBJS reviews. 2016; 4(11):e5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Poulsen E, Goncalves GH, Bricca A, Roos EM, Thorlund JB, Juhl CB. Knee osteoarthritis risk is increased 4-6 fold after knee injury–a systematic review and meta-analysis. British Journal of Sports Medicine. 2019; 53(23):1454–1463. [DOI] [PubMed] [Google Scholar]
- 7.Eggerding V, Reijman M, Meuffels DE, et al. ACL reconstruction for all is not cost-effective after acute ACL rupture. British Journal of Sports Medicine. 2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ford KR, Shapiro R, Myer GD, Van Den Bogert AJ, Hewett TE. Longitudinal sex differences during landing in knee abduction in young athletes. Medicine and science in sports and exercise. 2010; 42(10):1923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Holden S, Boreham C, Delahunt E. Sex differences in landing biomechanics and postural stability during adolescence: a systematic review with meta-analyses. Sports medicine. 2016; 46(2):241–253. [DOI] [PubMed] [Google Scholar]
- 10.Hewett TE, Myer GD, Ford KR, et al. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. The American journal of sports medicine. 2005; 33(4):492–501. [DOI] [PubMed] [Google Scholar]
- 11.Chia L, Myer GD, Hewett TE, et al. When puberty strikes: Longitudinal changes in cutting kinematics in 172 high-school female athletes. Journal of Science and Medicine in Sport. 2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Pappas E, Shiyko MP, Ford KR, Myer GD, Hewett TE. Biomechanical deficit profiles associated with ACL injury risk in female athletes. Medicine and science in sports and exercise. 2016; 48(1):107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ford KR, Myer GD, Hewett TE. Reliability of landing 3D motion analysis: implications for longitudinal analyses. Medicine and Science in Sports and Exercise. 2007; 39(11):2021–2028. [DOI] [PubMed] [Google Scholar]
- 14.Taylor JB, Nguyen A-D, Shultz SJ, Ford KR. Hip biomechanics differ in responders and non-responders to an ACL injury prevention program. Knee Surgery, Sports Traumatology, Arthroscopy. 2020; 28(4):1236–1245. [DOI] [PubMed] [Google Scholar]
- 15.Davies PL, Rose JD. Assessment of cognitive development in adolescents by means of neuropsychological tasks. Developmental Neuropsychology. 1999; 15(2):227–248. [Google Scholar]
- 16.Schlossberger NM, Turner RA, Irwin CE Jr. Validity of self-report of pubertal maturation in early adolescents. Journal of Adolescent Health. 1992; 13(2):109–113. [DOI] [PubMed] [Google Scholar]
- 17.Davies PL, Rose JD. Motor skills of typically developing adolescents: awkwardness or improvement? Physical & occupational therapy in pediatrics. 2000; 20(1):19–42. [PubMed] [Google Scholar]
- 18.Ford KR, Myer GD, Toms HE, Hewett TE. Gender differences in the kinematics of unanticipated cutting in young athletes. Medicine & Science in Sports & Exercise. 2005; 37(1):124–129. [PubMed] [Google Scholar]
- 19.Dos’Santos T, Bishop C, Thomas C, Comfort P, Jones PA. The effect of limb dominance on change of direction biomechanics: a systematic review of its importance for injury risk. Physical therapy in sport. 2019; 37:179–189. [DOI] [PubMed] [Google Scholar]
- 20.Fox AS. Change-of-direction biomechanics: Is what’s best for anterior cruciate ligament injury prevention also best for performance? Sports Medicine. 2018; 48(8):1799–1807. [DOI] [PubMed] [Google Scholar]
- 21.Chia L, de Oliveira Silva D, McKay MJ, Sullivan J, Micolis de Azevedo F, Pappas E. Limited support for trunk and hip deficits as risk factors for athletic knee injuries: a systematic review with meta-analysis and best-evidence synthesis. Journal of Orthopaedic & Sports Physical Therapy. 2020; 50(9):476–489. [DOI] [PubMed] [Google Scholar]
- 22.Beunckens C, Molenberghs G, Kenward MG. Direct likelihood analysis versus simple forms of imputation for missing data in randomized clinical trials. Clinical Trials. 2005; 2(5):379–386. [DOI] [PubMed] [Google Scholar]
- 23.Verbeke G Linear mixed models for longitudinal data, in Linear mixed models in practiceed^eds, Springer, 1997. [Google Scholar]
- 24.Ng L, Rosalie SM, Sherry D, et al. A biomechanical comparison in the lower limb and lumbar spine between a hit and drag flick in field hockey. Journal of Sports Sciences. 2018; 36(19):2210–2216. [DOI] [PubMed] [Google Scholar]
- 25.Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. Journal of the Royal statistical society: series B (Methodological). 1995; 57(1):289–300. [Google Scholar]
- 26.Dempsey AR, Lloyd DG, Elliott BC, Steele JR, Munro BJ. Changing sidestep cutting technique reduces knee valgus loading. The American Journal of Sports Medicine. 2009; 37(11):2194–2200. [DOI] [PubMed] [Google Scholar]
- 27.Dos’Santos T, Thomas C, McBurnie A, Comfort P, Jones PA. Biomechanical determinants of performance and injury risk during cutting: a performance-injury conflict? Sports Medicine. 2021:1–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Brault S, Bideau B, Craig C, Kulpa R. Balancing deceit and disguise: How to successfully fool the defender in a 1 vs. 1 situation in rugby. Human Movement Science. 2010; 29(3):412–425. [DOI] [PubMed] [Google Scholar]
- 29.Kristianslund E, Faul O, Bahr R, Myklebust G, Krosshaug T. Sidestep cutting technique and knee abduction loading: implications for ACL prevention exercises. Br J Sports Med. 2014; 48(9):779–783. [DOI] [PubMed] [Google Scholar]
- 30.Mizuno K, Andrish JT, van den Bogert AJ, McLean SG. Gender dimorphic ACL strain in response to combined dynamic 3D knee joint loading: implications for ACL injury risk. The Knee. 2009; 16(6):432–440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Taylor K, Terry M, Utturkar G, et al. Measurement of in vivo anterior cruciate ligament strain during dynamic jump landing. Journal of Biomechanics. 2011; 44(3):365–371. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Dempsey AR, Lloyd DG, Elliott BC, Steele JR, Munro BJ, Russo KA. The effect of technique change on knee loads during sidestep cutting. Medicine & Science in Sports & Exercise. 2007; 39(10):1765–1773. [DOI] [PubMed] [Google Scholar]
- 33.Stuelcken MC, Mellifont DB, Gorman AD, Sayers MG. Mechanisms of anterior cruciate ligament injuries in elite women’s netball: a systematic video analysis. Journal of Sports Sciences. 2016; 34(16):1516–1522. [DOI] [PubMed] [Google Scholar]
- 34.Song Y, Li L, Hughes G, Dai B. Trunk motion and anterior cruciate ligament injuries: a narrative review of injury videos and controlled jump-landing and cutting tasks. Sports Biomechanics. 2021:1–19. [DOI] [PubMed] [Google Scholar]
- 35.Wild CY, Steele JR, Munro BJ. Why do girls sustain more anterior cruciate ligament injuries than boys? Sports Medicine. 2012; 42(9):733–749. [DOI] [PubMed] [Google Scholar]
- 36.Almonroeder TG, Garcia E, Kurt M. The Effects of Anticipation on the Mechanics of the Knee During Single‐Leg Cutting Tasks: A Systematic Review. International Journal of Sports Physical Therapy. 2015; 10(7):918. [PMC free article] [PubMed] [Google Scholar]
- 37.Chia L, Andersen JT, McKay MJ, Sullivan J, Megalaa T, Pappas E. Evaluating the validity and reliability of inertial measurement units for determining knee and trunk kinematics during athletic landing and cutting movements. Journal of Electromyography and Kinesiology. 2021:102589. [DOI] [PubMed] [Google Scholar]