

Abstract
Background:
Currently there is no laboratory test that can accurately identify children at risk of developing peanut allergy. Utilizing a subset of children randomized to the peanut avoidance arm of the LEAP trial, we monitored the development of epitope-specific (ses-)IgE and ses-IgG4 from 4–11 months to 5 years of age.
Objective:
To evaluate the prognostic ability of epitope-specific antibodies to predict the result of an oral food challenge (OFC) at 5 years.
Methods:
A Bead-Based Epitope Assay was used to quantitate IgE and IgG4 to 64 sequential (linear) epitopes from Ara h 1–3 proteins at 4–11 months, 1 and 2.5 years of age in 74 subjects (38 of them with a positive OFC at 5-years). Specific IgE (sIgE) to peanut and component proteins was measured using ImmunoCAP. Machine Learning methods were used to identify the earliest time point to predict 5-year outcome, developing prognostic algorithms based only on 4–11 months samples, 1-year or 2.5 years, and a combination of them. Data from 74 children were iteratively split 3:1 into training and validation sets and machine learning models were developed to predict the 5-year outcome. A test set (n=90) from an independent cohort was used for final evaluation.
Results:
Elastic-Net algorithm combining ses-IgE and IgE to Ara h 1,2,3 and 9 proteins could predict the 5-year peanut allergy status of LEAP participants with an average validation accuracy of 64% at baseline. Samples taken at 1 year accurately predicted a 5-year OFC outcome with 83% accuracy. This performance remained consistent when evaluated on an independent CoFAR2 cohort with an accuracy of 78% for the 1-year model.
Conclusion:
IgE antibody profiles at 1 year of age are predictive of peanut OFC at 5 years in children avoiding peanuts. If further confirmed, this model may enable early identification of infants who may benefit from early immunotherapeutic interventions.
Keywords: peanut allergy, prognostic biomarkers, sequential epitope, antibody, IgE, IgG4, Bead-Based Epitope Assay
Capsule Summary:
IgE specific to sequential epitopes and component proteins measured at 1 year of age can predict peanut allergy status at 5 years.
Introduction
Peanut allergy is a leading cause of food-related allergic reactions and anaphylaxis [1]. It is one of the leading food allergies causing fatal anaphylaxis, ranking first in the US and second after milk in the UK. As the Learning Early About Peanut Allergy (LEAP) [2] trial demonstrated, early introduction of peanut into the diet of high-risk infants prevents the development of peanut allergy. Some studies report that 20% of infants and young children reacting to peanut will outgrow their allergy, while the rest will experience persistent symptoms throughout their lifetime [3]. These and other studies are strongly supportive of distinct endotypes of peanut allergy, with most patients belonging to the persistent phenotype and a minority to the transient phenotype.
Recent studies measuring levels of immunoglobulins binding sequential (linear) epitopes from milk and peanut allergens using a Bead-Based Epitope Assay (BBEA) revealed their importance for predicting symptomatic allergy. While sequential epitope-specific (ses-)IgE antibodies in infants with persistent food allergy are less pronounced compared to IgE against a whole peanut extract (conformational plus sequential epitopes) during the first year of life, ses-IgEs develop as subjects mature, signaling the establishment of persistent allergy Thus, children developing persistent peanut allergy later in life might have distinct epitope-specific antibody profiles in infancy, but there has been no laboratory test that accurately identifies this subset, which would facilitate the earlier introduction of preventative strategies. BBEA biomarkers have shown great potential in predicting treatment outcomes [5], allergy endotypes [9], and diagnosis [10]. Recently we evaluated the impact of peanut consumption and avoidance on the development of ses-IgE and ses-IgG4 in a subset of 341 high-risk infants who completed the LEAP trial [4]. We found that while subjects had similar baseline ses-IgE and ses-IgG4 profiles irrespective of their allergy status later in life, significant ses-IgE expansion was observed only among children who later became peanut allergic, as determined by an oral food challenge (OFC) at the 5-year visit. In the current study, our goal was to determine whether ses-IgE and ses-IgG4 antibodies measured during the first year of life can be used as a prognostic test, to predict the outcome of a 5-year OFC.
Materials and Methods
Methods are described in detail in the Supplementary Methods in the Online Repository. In brief, we used the subset of children from the avoidance arm of the LEAP trial (NCT00329784, Fig. S1), with peanut allergy (n=38) or no allergy (n=36) outcome at the 5-year OFC and results of IgE specific to Ara h 1,2,3 and 9 proteins (ImmunoCAP, Uppsala, Sweden). For each participant, blood samples were obtained at the baseline study visit (V1), which occurs between 4–11 months of age, at 1 and 2.5 years. The BBEA was used, as described previously [11], to quantify ses-IgE and ses-IgG4 against 64 peptides representing sequential epitopes from Ara h 1 (n = 34), Ara h 2 (n = 16), and Ara h 3 (n = 14) proteins at each time point.
Previous work showed that reactivity to peanut allergens can be explored using various assays, with antibodies recognizing allergens at different tiers, from epitopes to individual component proteins to whole peanut antigens. As such, we developed prognostic models combining 64 ses-IgE and ses-IgG4, specific IgE antibodies to Ara h 1, 2, 3, 8 and 9, collectively referred to as ‘Ara h sIgE’, and IgE to whole peanut extract (‘PN-sIgE’). We used a machine learning (ML) strategy to identify prognostic biomarkers at 4–11 months, 1 and 2.5 years that could predict the 5-year OFC outcome and tested which combination of timepoints and antibodies led to the best performance (Fig. 1A). Of note, we developed models using continuous (quantitative) normalized Median Fluorescence Intensity (MFI) measures of ses-IgE and ses-IgG4, and binary (qualitative) values indicating a presence or absence of an epitope-specific antibody, defined by the MFI above the upper level of the 95% confidence interval (CI) from the background signal. A total of 24 ML models were developed, each starting with a different set of predictors, including ses-IgEs alone and in combinations with ses-IgG4 and sIgEs across three time points (Fig. 1AB).
Figure 1. Development of a predictive model.
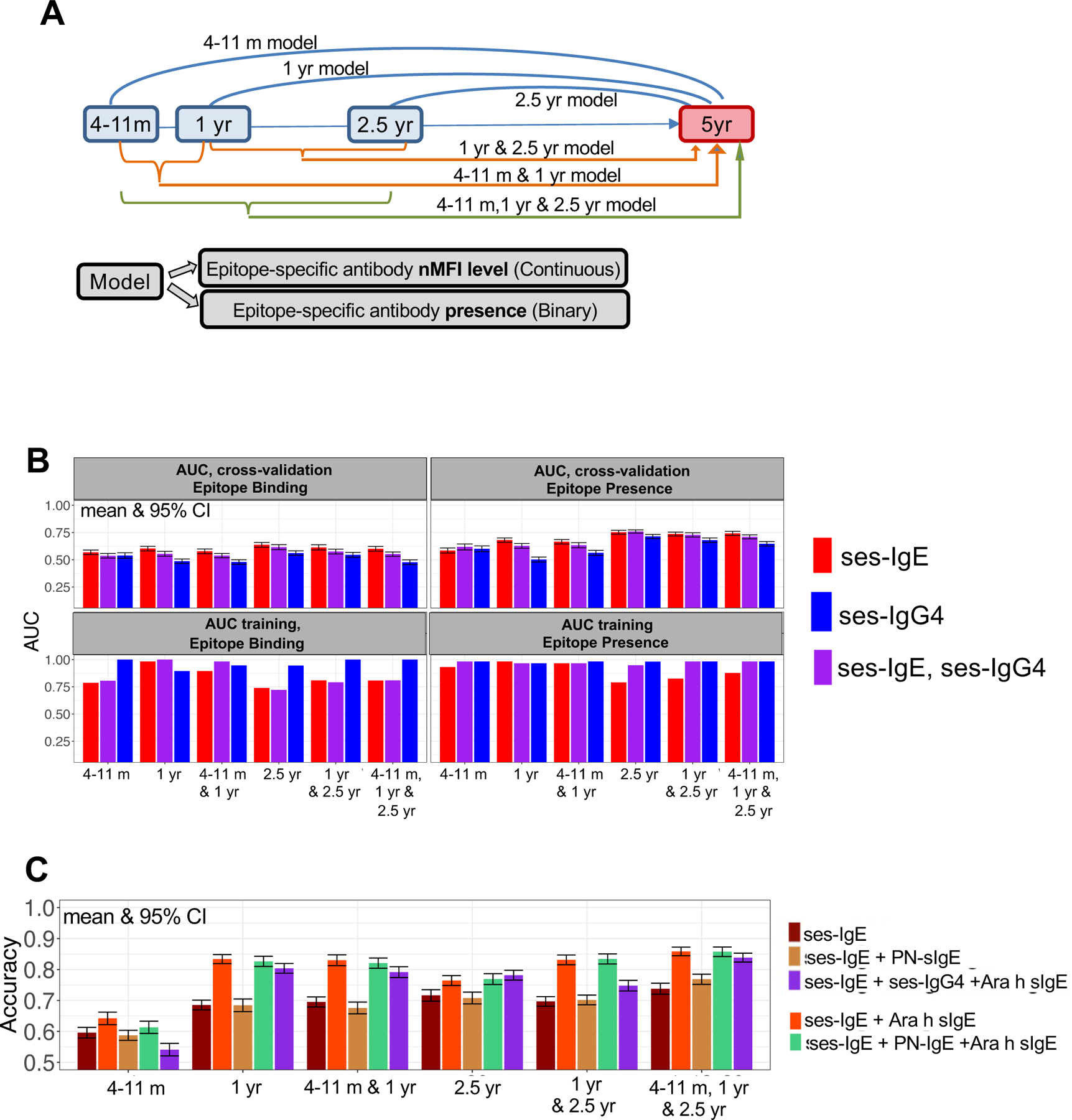
A. Models built to predict 5 year OFC outcomes. B. AUC of models using qualitative and quantitative ses-IgE/ses-IgG4 profiles at different ages and their combinations in cross-validation (top) and training (bottom). C. AUC in cross-validation of models using ses-IgE, ses-IgG4 along with PN-sIgE and Ara h sIgE. Addition of Ara h sIgE, but not PN-sIgE or ses-IgG4, to ses-IgE profiles improves 1 year performance.
To account for the limited sample size, we used a modeling strategy that allowed us to estimate the validation performance for small sample sizes, similar to the approach utilized previously [5]. Briefly, models were developed using 56 randomly selected subjects from the cohort (training set) and performance was validated on the remainder (validation set, n=18); this split was repeated 100 times to produce robust estimates (mean and 95% CI) of the validation performance. Model hyper-parameters were tuned using 5-fold cross-validation within the training set. (Fig.S2).
Ninety subjects from the CoFAR2 (NCT00356174) study [6, 12] were used for external validation (Fig.S1) of our 1-year prognostic model, but was hindered by the differences in the timing of the visits (3–15 months in CoFAR2 vs 12 months in LEAP) and, differences in epitope panel between the two cohorts (50 vs 64). To circumvent the later limitation and based on our observation that maximal correlation between epitope binding decreases with the distance between them, values of ses-IgE to Ara h 1_137, Ara h 1_047, Ara h 2_018 in CoFAR2 were imputed using the closest epitopes from the same protein that were available in the CoFAR’s 50-epitope panel, which were Ara h 1_131, Ara h 1_045, Ara h 2_017. Then the final model estimated using LEAP cohort was applied to the CoFAR2 subjects.
The LEAP and COFAR studies were registered on clinicaltrials.gov (NCT00329784 and NCT00356174) and approved by the local Institutional Review Boards and overseen by the data, safety and monitoring board of NIAID. The LEAP study was approved by the National Research Ethics Service Committee London-Fulham and the COFAR by the IRB of each site. Written informed consent was obtained from the participants’ parent/legal guardian to participate in the study.
Results and Discussion
Seventy-four subjects with available data (Fig.S1) were used for the machine learning. Our computational pipeline indicated that a) simpler qualitative ses-IgE and ses-IgG4 measures produced higher cross-validation performance (Fig.1B) (P<.001), and that while b) inclusion of ses-IgG4 did not significantly improve performance, c) excluding ses-IgE led to significantly (P<.001) lower AUC suggesting that the ses-IgE profile is the key component for predicting a 5-year OFC outcome.
In view of these results, we focused on models including (1) qualitative ses-IgE alone or by adding (2) sIgE to Ara h 1,2,3 and 9 (‘ses-IgE+Ara h sIgE’), (3) peanut-specific IgE (‘ses-IgE+PN-sIgE’) or (4) both sIgE to component proteins and peanut (‘ses-IgE+Ara h sIgE+PN-sIgE’), and (5) including ses-IgG4 (‘ses-IgE+Ara h sIgE+ses-IgG4’). The performance of these models on the validation sets, depicted in Fig.1C, shows that predictive performance is low at 4–11 months but improves with age, with accurate predictions achieved as early as 1 year. At 1 year, ‘ses-IgE+Ara h sIgE’ outperforms all other models with the addition of PN-sIgE being a close second (‘ses-IgE+Ara h sIgE+PN-sIgE’). Though children in this cohort were avoiding peanuts and we would not expect IgG4 to be needed for the predictions, this result is consistent with our previous work [5, 6, 9], where the addition of ses-IgG4 values even in combination with antigen-specific IgEs did not improve the performance. Prognostic biomarkers chosen by the ‘ses-IgE+Ara h sIgE’ model (Fig.2A) are consistent with the second-best performing model that includes PN-sIgE (see Fig.S1 AB). Interestingly, this model contains sIgE to Ara h 9, a component not previously reported to be associated with allergy prognosis. We thus evaluated the impact of excluding Ara h 9 and observed a reduction in both AUC (from 0.92 [95% CI 0.91–0.93] to 0.90 [0.88–0.91], P<.001) and Accuracy (from 83% [82–85%] to 79% [77–81%], P<.001) at 1 year, with similar decreases at other timepoints.
Figure 2. Performance of final ‘ses-IgE+Ara h sIgE’ 5-year prognostic model.
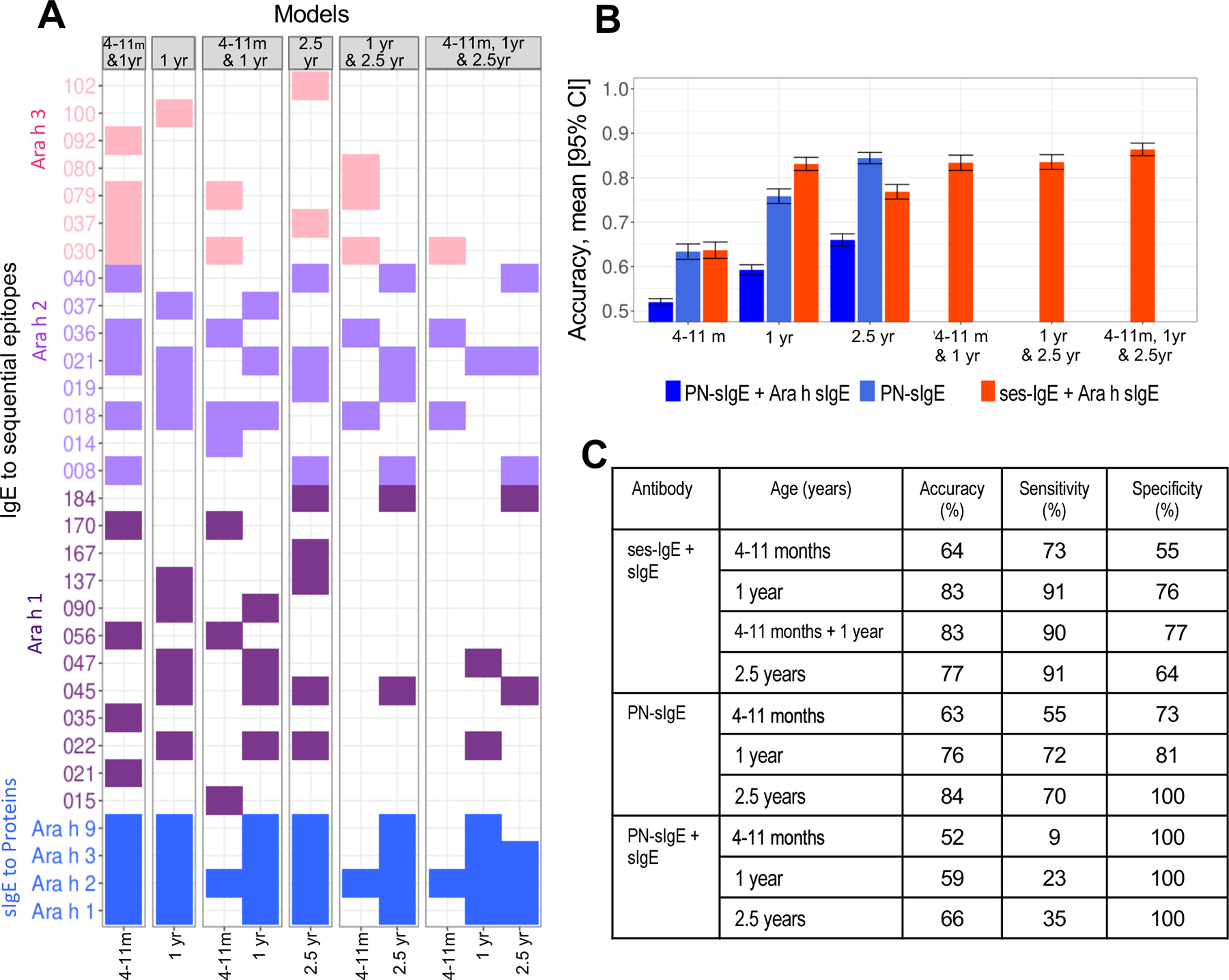
A. Prognostic epitopes identified at each age (or its combination) for the ‘ses-IgE+Ara h sIgE’ model. B-C. Performance in testing set of the ‘ses-IgE+Ara h sIgE’ model and two ImmunoCAP-based criteria: allergic if PN-sIgE ≥0.35 (“PN-sIgE”) or if PN-sIgE ≥0.35 and Ara h 1 and Ara h 2 and Ara h 3 ≥0.35 kUA/L (“PN-sIgE+Ara h sIgE”).
We then compared the performance of our model with that of a simple ImmunoCAP-based cut off of 0.35 kUA/L of sIgE to peanut and/or components (Fig.2BC) [6, 13, 14]. At 4–11 months, our ‘ses-IgE+Ara h sIgE’ model predicts 5-year OFC outcome with an average (validation) Accuracy of 64% [62–66%] which was close to the performance of the cut-off based PN-sIgE (Accuracy=63% [62–65%]). However, at 1 year of age “ses-IgE+Ara h sIgE” model achieves an Accuracy of 83% [82%−85%], significantly superior (P<.001) to the performance of the PN-sIgE-based method (Accuracy of 76% [74%−77%]).
Lastly, we have validated our 1-year ‘ses-IgE+Ara h sIgE’ model using the 3–15 months samples from 90 CoFAR2 participants (29 Allergic and 61 Non-Allergic, Fig.S1) and predicted their allergy status after 4 years of age. The performance was consistent, with an AUC of 0.853 [0.851–0.855], Accuracy of 77.9% [77.5–78.3%], Sensitivity 75.3% [74.7–75.9%], and Specificity 83.3% [82.6–84.0%], thus validating the algorithm’s performance in the LEAP cohort. However, the model excluding sIgE to Ara h 9, which led to lower performance in the LEAP cohort, showed similar performance in CoFAR2 [AUC 85.9% [85.6%−86.1%] and Accuracy 78.5% [78.0%−79.0%]. Of note, the LEAP cohort exhibited higher levels of sIgE to Ara h 9 (and Ara h 2) than the CoFAR2 cohort (Fig.S2C), which may explain why the models with and without Ara h 9 perform similarly on the CoFAR2 subjects.
Several limitations should be noted. This study included only subjects randomized to peanut avoidance arm of the LEAP trial and sample size was further limited by the available sample volumes. Allergy status was determined at the 5-year OFC visit, but some subjects likely developed allergy well before then. We have used a machine learning pipeline with boot-strapping to allow us to estimate performance from a small sample size, which was then validated on an external cohort.
In conclusion
In conclusion, epitope-specific IgE profiles obtained at about 1 year of age in high-risk children avoiding peanut show promising performance as prognostic biomarkers for peanut OFC outcome at 5 years of age. Evaluation of ses-IgE is sufficient to create predictive models without adding ses-IgG4. Models combining ses-IgE and IgE specific to component proteins performed best at predicting allergy status at 5-year OFC, while adding IgE to peanut extract did not improve performance. Our model had comparable prognostic performance when validated on an independent external cohort, despite the need to impute 3 epitopes, which remains a limitation. If our results are confirmed in future prospective studies with larger sample sizes, this test should enable physicians to identify infants likely to develop peanut allergy, allowing them to initiate immunotherapeutic interventions early, which is believed to be more likely to induce permanent tolerance.
Supplementary Material
Acknowledgements:
The authors wish to thank CoFAR investigators Dr. Scott H. Sicherer, Dr. Robert Wood, Dr. Stacie Jones, Dr. Donald Leung, Ms Alice Henning, Dr. Peter Dawson, Dr. Wesley Burks and Dr. Robert Lindblad for sharing the data from the CoFAR2 cohort.
Funding Sources:
This work was supported by the National Institute of Allergy and Infectious Diseases of the National Institutes of Health under Award Number UM1AI109565, NO1-AI-15416, UM1AI109565, HHSN272200800029C, and UM2AI117870; the David H. and Julia Koch Research Program in Food Allergy Therapeutics; and AllerGenis LLC. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Abbreviations
- AUC
Area under the ROC curve
- BBEA
Bead-based epitope assay
- CI
Confidence interval
- CoFAR
Consortium of Food Allergy Research
- LEAP
Learning Early About Peanut
- OFC
Oral food challenge
- OIT
Oral immunotherapy
- Elastic net
Elastic-Net Regularized Generalized Linear Model
- ses-Ig
Sequential epitope-specific immunoglobulin
- sIgE
Specific IgE
Footnotes
Statement of Ethics
The LEAP and COFAR studies were registered on clinicaltrials.gov (NCT00329784 and NCT00356174) and approved by the local Institutional Review Boards and overseen by the data, safety and monitoring board of NIAID. The LEAP study was approved by the National Research Ethics Service Committee London-Fulham and the COFAR by the IRB of each site. Written informed consent was obtained from the participants’ parent/legal guardian to participate in the study.
Disclosures:
Dr Grinek, Dr. Suprun, Mr. Raghunathan, and Dr. Tomalin have nothing to disclose. Dr. Getts is an employee of Genisphere LLC and scientific consultant of AllerGenis LLC; in addition, Dr. Getts has a patent PCT/US15/020715 (WO) pending. Mr. Bahnson has received consulting fees from DBV Technologies and MYOR, and research support from NIAID via the Immune Tolerance Network. Dr. Lack has received research support from the NIAID (NO1-AI-15416 [contract] and UM1AI109565 [grant]), and UK Food Standards Agency; is on the DBV Technologies scientific advisory board; has received a contribution to NIAID contract/grant from Food Allergy Research and Education; has received a contribution to KCL Division of Asthma Allergy & Lung Biology from MRC & Asthma UK Centre; has received the BRC award to Guy’s and St Thomas’ NHS Foundation from the UK Department of Health through NIHR; has received support for pediatric allergy clinical trial’s unit from the National Peanut Board; has received discounted Bamba peanut snack from Osem; and has stock/stock options in DBV Technologies. Dr. Sampson reports grants from Immune Tolerance Network; NIAID/NIH, personal fees from N-Fold LLC, Siolta Therapeutics and DBV Technologies, outside the submitted work; and Mount Sinai has licensed the technology for a bead-based epitope assay for food-allergen epitope analyses to AllerGenis LLC. Dr. Sampson serves as an unpaid Board of Directors member and advisor to AllerGenis LLC. Dr. Suárez-Fariñas received research funding to Mount Sinai by a grant from AllerGenis LLC.
Data Availability Statement:
The data used in this manuscript has been made available as a supplementary table S1.
References:
- 1.Burks AW, Tang M, Sicherer S, Muraro A, Eigenmann PA, Ebisawa M, et al. ICON: food allergy. The Journal of allergy and clinical immunology 2012;129(4):906–20. [DOI] [PubMed] [Google Scholar]
- 2.Du Toit G, Roberts G, Sayre PH, Bahnson HT, Radulovic S, Santos AF, et al. Randomized trial of peanut consumption in infants at risk for peanut allergy. N Engl J Med 2015;372(9):803–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Skolnick HS, Conover-Walker MK, Koerner CB, Sampson HA, Burks W, Wood RA. The natural history of peanut allergy. The Journal of allergy and clinical immunology 2001;107(2):367–74. [DOI] [PubMed] [Google Scholar]
- 4.Suarez-Farinas M, Suprun M, Bahnson HT, Raghunathan R, Getts R, duToit G, et al. Evolution of epitope-specific IgE and IgG4 antibodies in children enrolled in the LEAP trial. The Journal of allergy and clinical immunology 2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Suarez-Farinas M, Suprun M, Chang HL, Gimenez G, Grishina G, Getts R, et al. Predicting development of sustained unresponsiveness to milk oral immunotherapy using epitope-specific antibody binding profiles. The Journal of allergy and clinical immunology 2018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Suprun M, Sicherer SH, Wood RA, Jones SM, Leung DYM, Henning AK, et al. Early epitope-specific IgE antibodies are predictive of childhood peanut allergy. The Journal of allergy and clinical immunology 2020;146(5):1080–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Baker MG, Sampson HA. Phenotypes and endotypes of food allergy: A path to better understanding the pathogenesis and prognosis of food allergy. Ann Allergy Asthma Immunol 2018;120(3):245–53. [DOI] [PubMed] [Google Scholar]
- 8.Jarvinen KM, Beyer K, Vila L, Bardina L, Mishoe M, Sampson HA. Specificity of IgE antibodies to sequential epitopes of hen’s egg ovomucoid as a marker for persistence of egg allergy. Allergy 2007;62(7):758–65. [DOI] [PubMed] [Google Scholar]
- 9.Sackesen C, Suarez-Farinas M, Sillva R, Lin J, Schmidt S, Getts R, et al. A new Luminex-based peptide assay to identify reactivity to baked, fermented, and whole milk. Allergy 2018. [DOI] [PubMed] [Google Scholar]
- 10.Suarez-Farinas M, Suprun M, Kearney P, Getts R, Grishina G, Hayward C, et al. Accurate and reproducible diagnosis of peanut allergy using epitope mapping. Allergy 2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Suprun M, Getts R, Raghunathan R, Grishina G, Witmer M, Gimenez G, et al. Novel Bead-Based Epitope Assay is a sensitive and reliable tool for profiling epitope-specific antibody repertoire in food allergy. Sci Rep 2019;9(1):18425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Sicherer SH, Wood RA, Perry TT, Jones SM, Leung DYM, Henning AK, et al. Clinical factors associated with peanut allergy in a high-risk infant cohort. Allergy 2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.van Veen WJ, Dikkeschei LD, Roberts G, Brand PL. Predictive value of specific IgE for clinical peanut allergy in children: relationship with eczema, asthma, and setting (primary or secondary care). Clin Transl Allergy 2013;3(1):34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Nicolaou N, Murray C, Belgrave D, Poorafshar M, Simpson A, Custovic A. Quantification of specific IgE to whole peanut extract and peanut components in prediction of peanut allergy. The Journal of allergy and clinical immunology 2011;127(3):684–5. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The data used in this manuscript has been made available as a supplementary table S1.