

Abstract
Background:
It is unknown whether increasing attention to police brutality is a source of stress associated with substance use risk among young people.
Methods:
A longitudinal racially/ethnically diverse cohort from Los Angeles, California (n = 1797) completed baseline (2017; mean age: 17.9) and follow-up (2020; mean age: 21.2) surveys assessing level of concern, worry, and stress about police brutality (range: 0 ‘not at all’ – 4 ‘extremely’) and past 30-day nicotine, cannabis, alcohol, other drug, and number of substances used (0–19). Regression models, adjusted for demographic characteristics and baseline substance use, evaluated whether changes in distress about police brutality from 2017 to 2020 were associated with substance use in 2020 overall and stratified by race/ethnicity.
Results:
Distress about police brutality increased between 2017 (mean: 1.59) and 2020 (mean: 2.43) overall. Black/African American and Hispanic/Latino respondents consistently had the highest mean distress levels at both timepoints. In the full sample, each one-unit greater increase in distress about police brutality from 2017 to 2020 was associated with 11% higher odds of cannabis use, 13% higher odds of alcohol use, and 8% higher risk of using an additional substance for the number of substances used outcome. Race/ethnicity-stratified models indicated that greater increases in distress from 2017 to 2020 was associated with substance use among Black/African American, Hispanic, and multiracial respondents in 2020, but not Asian American/Pacific Islander and White respondents.
Conclusions:
Distress about police brutality may be associated with substance use, particularly among certain racial/ethnic minority young people. Further investigation of whether police brutality affects health in disparity populations is needed.
Keywords: Police brutality, Substance use, Alcohol, Tobacco, Marijuana, Cannabis
1. Introduction
Young adult substance use is a major public health concern that may lead to long-term health problems and is a source of racial/ethnic health disparities (Pinedo, 2019). Hence, it is important to understand wide-spanning exposures that may disproportionately impact racial/ethnic minority populations and are salient to young people. The highly publicized killings of Breonna Taylor in March and George Floyd in May 2020 garnered significant attention, public awareness, and civil unrest related to police brutality (i.e., unwarranted or illegal acts of physical, psychological, and sexual violence by law enforcement on civilians) (Alang et al., 2021; Brooks, 2020). Racial/ethnic minority populations remain disproportionately exposed to police brutality, with Black, Latinx, and American Indian/Alaska Native adults being more likely to be killed by police than White adults in the United States (US) (Buehler, 2017; Edwards et al., 2019; GBD, 2019 Police Violence US Subnational Collaborators, 2021; Geller et al., 2014).
While many individuals will not directly experience police brutality in their lifetimes (Edwards et al., 2019), awareness of each incident of police brutality is likely to take an emotional toll on individuals and communities, especially among racial/ethnic minority groups (Bor et al., 2018). Vicarious (indirect) exposure to police brutality, or witnessing or hearing about police brutality through proximal or distal sources, can be harmful to health (Bor et al., 2018; McFarland et al., 2019; Simckes et al., 2021). Similarly, distress about police contact pose unique health risks and might substantially increase after high-profile cases of police brutality or killings (Howard et al., 2022). Racial/ethnic minority groups such as Hispanic and Black Americans worry about police contact at least four times that of White Americans (Graham et al., 2020). In addition, past police contact has been shown to lead to police avoidance and subsequent depressive symptoms (Bowleg et al., 2020).
Incidents of police brutality are examples of race-based trauma (Comas-Diaz et al., 2019), or stressors derived from structural racism that may lead to fear of victimization and increased awareness of inequitable treatment (Alang et al., 2021; Bor et al., 2018). Among youth, these incidents can be described as racialized adverse childhood experiences, or events that are disproportionately harmful to the well-being of youth racial/ethnic minority populations (Jackson, 2021). Experiencing police brutality in any manner, directly or indirectly, can induce psychological stress (Alang et al., 2017; Jackson et al., 2021; Simckes et al., 2021), which may be especially salient among disproportionately impacted communities. Collectively, stressors related to police brutality are best characterized as race-related stress, or stress created by underlying racist institutions and structures, perpetuated by systems (e.g., law enforcement) and social processes (e.g., police brutality) (Williams, 2018). As a race-related stressor, police brutality might differentially affect racial/ethnic minority groups (Alang, 2018; Alang et al., 2017), potentially driving disparities in mental health and health behaviors, such as substance use and misuse (Alang et al., 2021; Comas-Diaz et al., 2019; Williams, 2018).
Given the context of increased media attention to police brutality in recent years, it is possible that distress about police brutality might have increased, with potential consequences for substance use in young people. However, this hypothesis has not been empirically tested in the US. One study found that people who injected drugs in Ukraine who reported being beaten by the police were more likely to engage in risky behavior such as sharing syringes (Strathdee et al., 2010). In Mexico, people who injected drugs and sought treatment were more likely to report experiencing police violence (Werb et al., 2016). Furthermore, in the United Kingdom (UK), youth who experienced police stops were more likely to use substances later in life (Jackson et al., 2022). If younger populations are using substances in the face of stress associated with police brutality, then this will have implications for downstream health outcomes such as substance use disorders and chronic diseases caused by long-term nicotine, cannabis, alcohol, and other drug use. Furthermore, race-related stress associated with increased rates of police brutality in society may exacerbate racial/ethnic disparities in substance use and its associated health outcomes (Williams, 2018).
We examined changes in distress about police brutality from early 2017 to mid 2020, directly after the murders of Breonna Taylor and George Floyd when distress about police brutality may have been heightened (Howard et al., 2022), within a longitudinal study of a diverse cohort of young people from Los Angeles, California. With a history of controversial killings, the police agency in Los Angeles County is one of the largest in the US and is responsible for the shootings of approximately three to four people each month (Levin, 2020). We additionally assessed the extent to which changes in police brutality distress was associated with nicotine, cannabis, alcohol, and other drug use in the overall sample and stratified by race/ethnicity.
2. Materials and methods
2.1. Participants
Data come from an on-going longitudinal cohort study that enrolled youth from ten high schools in Los Angeles County in 2013. Students in 9th grade were asked to provide assent and written or verbal parental consent to participate. Since the baseline survey in 2013, surveys were administered at each six-month follow-up in classrooms during the normal school day. Students absent during the day of assessment were given abbreviated surveys by telephone, Internet, or postal mail. Surveys were administered exclusively online via REDCap starting in 2019, after respondents completed high school. Further details about the study design can be found elsewhere (Leventhal et al., 2015). The University of Southern California Institutional Review Board approved this study.
This study uses data from waves 8 (spring 2017 (January 2017 to June 2017); henceforth referred to as “baseline”) and 10 (spring/summer 2020 (May 2020 to October 2020), “follow-up”). At baseline, 3140 respondents completed the survey. At follow-up, 22.4% of baseline respondents were missing due to attrition, resulting in 2436 participants eligible for this analysis. Of the eligible sample, 1797 participants who had complete exposure and outcome data and were included in the analytic sample. All missing data on covariates (listed below) were assigned using other available information (e.g., demographic information provided at earlier waves).
2.2. Measures
2.2.1. Change in distress about police brutality
At both survey waves, participants rated whether they were “concerned,” “worried,” or “stressed” about “police brutality or unfair treatment of members in your community by law enforcement” at both baseline and follow-up using three Likert-scale items, one for each of the 3 emotional responses. Response options for each item included: 0: “not at all,” 1: “slightly,” 2: “somewhat,” 3: “very,” and 4: “extremely”. A composite mean (range: 0–4) of the three ratings was developed to quantify police brutality concern, worry, and stress as one construct (hereafter referred to as “distress about police brutality”) at each wave. This measure was based on a parallel measure assessing concern, worry, and stress regarding societal discrimination, which showed adequate psychometric properties (Leventhal et al., 2018). To measure internal consistency, Cronbach’s alpha at baseline (α = 0.93) and follow-up (α = 0.95) were estimated, representing excellent internal reliability at both waves. The primary exposure for this study was the change in distress about police brutality between 2017 and 2020 (calculated by subtracting distress about police brutality at baseline from distress at follow-up; range = −4 to 4).
2.2.2. Past 30-day substance use
Past 30-day substance use was measured at both baseline and followup separately for nicotine, cannabis, alcohol, and other drug use (yes/no). Nicotine use included use of any of the following products: cigarettes, electronic cigarettes (with nicotine), IQOS or other heated tobacco devices, snus, nicotine pouches, big cigars, cigarillos, and hookah. Cannabis use included smoking cannabis (with or without blunts), consuming cannabis or THC foods or drinks, dabbing or vaping cannabis concentrates, and using synthetic cannabis. Alcohol use involved drinking at least one full drink (i.e., can of beer, glass of wine, wine cooler, or shot of liquor). Other drugs included misuse of prescription painkillers, stimulant pills, or sedatives, and heroin use. Finally, number of substances used was calculated as a sum of the number of substances used in the past 30 days out of the 19 different substances assessed (range = 0–19). Substance use volume outcomes (i.e., frequency × intensity) were also included as secondary outcomes in supplementary analyses described further below.
2.2.3. Covariates
Several sociodemographic characteristics, assessed at follow-up, were included such as age, sex, race/ethnicity, highest educational attainment, and personal financial status. Sex was assessed using a dichotomized variable (male, female). Race/ethnicity included Black/African American (hereafter, “Black”), Hispanic/Latino, Asian American, Native Hawaiian/Pacific Islander, American Indian/Alaska Native, Middle Eastern, White, Other, and multiracial and was categorized as Black, Hispanic/Latino, Multiracial, Asian American/Pacific Islander (AAPI), White, and another race/ethnicity. Another race/ethnicity included American Indian/Alaska Native and Middle Eastern respondents as well as respondents belonging to other indigenous ethnicities. Highest educational attainment was defined as high school graduate or less and post-secondary education. Participants indicated their personal financial status as 0: “live comfortably,” 1: “meet needs with a little left,” 2: “just meet basic expenses,” and 3: “don’t meet basic expenses.”
2.3. Statistical analysis
2.3.1. Primary analysis
Sociodemographic characteristics, change in distress about police brutality, and substance use outcomes were calculated overall and by race/ethnicity. Differences by race/ethnicity were estimated using chi-square or ANOVA tests. Post-hoc Tukey Kramer tests were used to examine racial/ethnic within-group differences in change in distress about police brutality between baseline and follow-up. Four multivariable logistic regression models estimated unadjusted and adjusted odds ratios (ORs) and 95% confidence intervals (CIs) for associations of increase in distress about police brutality with nicotine, cannabis, alcohol, and other drug use, respectively. Models were adjusted for age, sex, highest educational attainment, and personal financial status at wave 10. To mitigate the possibility of reverse causality, additional covariates for baseline use (never, before-past-30 day, past-30 day) of nicotine, cannabis, alcohol, and other drugs were included, as well as number of substances used (0–19). A subset analysis was conducted that disaggregated nicotine use (i.e., combustible use, e-cigarette use, smokeless tobacco use) and cannabis use (i.e., smoking, vaping, all other use) and estimated the association of change in distress about police brutality and past 30-day use for each category. In addition, negative binomial regression estimated risk ratios (RRs) and 95% CIs for the association between change in distress about police brutality and number of substances used , adjusting for sociodemographic characteristics at follow-up and baseline number of substances used. An additional sensitivity analysis was conducted to include a measure of distress about COVID-19 at wave 10 in each model as a potential confounder. This measure was asked about and coded in the same way as the police brutality measures (0–4).
Next, effect modification was explored for each substance use regression model by including two-way interaction terms between change in distress about police brutality and race/ethnicity to assess whether the magnitude of the associations between change in distress about police brutality and substance use depended on belonging to a specific racial/ethnic group. The joint p-values (see Table 2) indicated that there were no differences between racial/ethnic groups, but meaningful variation by race/ethnicity may have been undetectable due to small sample sizes. Thus, to qualitatively examine effect modification, models were stratified by race/ethnicity to generate stratified-specific ORs or RRs and 95% CIs for associations between change in distress about police brutality and substance use within each racial/ethnic group (i.e., Black, Hispanic/Latino, Multiracial, AAPI, White, another race/ethnicity) for each outcome. Statistical significance was assessed at an alpha level of 0.05, and all analyses were conducted using R version 4.0.5.
Table 2.
Associations between changes in distress about police brutality from 2017 to 2020 and past 30-day substance use in 2020, outcomes overall and by race/ethnicity.
| Stratified by Race/Ethnicity | |||||||
|---|---|---|---|---|---|---|---|
|
| |||||||
| Overall sample | Black/African American | Hispanic/Latino | Multiracial | AAPIa | White | Another race/ethnicityb | |
| Nicotine (OR, 95% CI)c | |||||||
| Unadjusted | 1.05 (0.97, 1.13) | 0.81 (0.53, 1.25) | 1.05 (0.94, 1.17) | 1.20 (0.94,1.53) | 1.10 (0.91, 1.33) | 0.92 (0.74, 1.14) | 1.07 (0.62, 1.85) |
| Adjusted | 1.07 (0.98, 1.16) | 0.78 (0.45, 1.34) | 1.10 (0.98, 1.24) | 1.20 (0.93, 1.55) | 1.01 (0.82, 1.25) | 0.96 (0.72, 1.27) | 1.64 (0.42, 6.34) |
| Cannabis (OR, 95% CI)c | |||||||
| Unadjusted | 1.12 (1.05, 1.20) * | 1.51 (0.99, 2.30) | 1.07 (0.98, 1.17) | 1.16 (0.93, 1.45) | 1.16 (0.98, 1.36) | 1.19 (0.97, 1.45) | 1.72 (0.93, 3.19) |
| Adjusted | 1.11 (1.04, 1.20)* | 1.66 (1.03, 2.67) * | 1.05 (0.96, 1.16) | 1.16 (0.91, 1.47) | 1.09 (0.92, 1.31) | 1.16 (0.93, 1.46) | 1.80 (0.82, 3.96) |
| Alcohol (OR, 95% CI)c | |||||||
| Unadjusted | 1.14 (1.07, 1.22) * | 1.41 (0.97, 2.03) | 1.14 (1.04, 1.24) * | 1.16 (0.94, 1.44) | 1.07 (0.93, 1.24) | 1.20 (0.97, 1.47) | 1.31 (0.79, 2.18) |
| Adjusted | 1.13 (1.05, 1.21) * | 1.51 (1.02, 2.24) * | 1.13 (1.02, 1.24) * | 1.13 (0.88, 1.45) | 1.06 (0.91, 1.24) | 1.17 (0.92, 1.49) | 2.18 (0.65, 7.26) |
| Other Drugs (OR, 95% CI)c | |||||||
| Unadjusted | 1.20 (0.97, 1.49) | 1.60 (0.40, 6.30) | 1.11 (0.85, 1.45) | 1.35 (0.52, 3.54) | 1.57 (0.76, 3.24) | 1.39 (0.78, 2.50) | __________d |
| Adjusted | 1.19 (0.94, 1.50) | d | 1.11 (0.84, 1.47) | 1.32 (0.51, 3.43) | 1.60 (0.79, 3.25) | 1.30 (0.67, 2.51) | __________d |
| Number of substances used (RR, 95% CI)c | |||||||
| Unadjusted | 1.06 (1.01, 1.10) | 1.22 (0.97, 1.54) | 1.05 (0.99, 1.11) | 1.07 (0.94, 1.21) | 1.05 (0.95, 1.17) | 1.04 (0.94, 1.16) | 1.14 (0.86, 1.50) |
| Adjusted | 1.08 (1.04, 1.12) * | 1.35 (1.11, 1.65) * | 1.06 (1.01, 1.12) * | 1.13 (1.01, 1.26) * | 1.05 (0.95, 1.16) | 1.07 (0.98, 1.18) | 1.30 (1.08, 1.56) * |
Asian American/Pacific Islander.
Another race/ethnicity category includes middle eastern and indigenous ethnicities.
Models adjusted for age, sex, race/ethnicity, highest educational attainment, personal financial status, and previous use of categorical substances in Wave 8.
Model did not converge.
P < 0.05.
2.3.2. Supplementary analysis of secondary outcomes
We conducted a supplementary analysis to examine whether change in distress about police brutality was associated with substance use volume. Since frequency and intensity of use measures were not available for all substances in our dataset, we examined only associations between change in distress and past 30-day use volume for: (1) cigarettes (defined as number of days used × the number of cigarettes smoked per typical smoking day); (2) e-cigarettes with nicotine (number of days used × nicotine vaping sessions per vaping day × number of puffs per vaping session), (3) cannabis smoking (number of days used × bowls/joints per cannabis smoking day) or vaping (number of days used × cannabis vaping sessions per vaping day × number of puffs per vaping session), and (4) alcohol (number of days used × drinks per drinking day). We used linear regression to estimate these associations adjusted for age, sex, race/ethnicity, highest educational attainment, personal financial status, and baseline substance use.
3. Results
3.1. Participant characteristics
As shown in Table 1, 60.2% of respondents were female and the majority identified as Hispanic/Latino (54.5%) while the remaining identified as AAPI (20.9%), White (11.3%), multiracial (8.7%), Black (3.4%), or another race/ethnicity (1.2%). Approximately three-fourth of respondents (75.2%) were enrolled in post-secondary education, while 24.8% indicated that their highest education level was high school graduate or less. Nearly half of the sample reported that they live comfortably (45.8%) when asked about their personal financial status, while 30.4% reported that they meet needs with a little left, 20.9% reported that they just meet basic expenses, and 2.7% reported that they do not meet basic needs. The mean age of the analytic sample was 17.9 (SD=0.4) at baseline and 21.2 years old (SD=0.4) at follow-up. The mean change in distress about police brutality (range = −4 to 4) was 0.84 (SD=1.48). About 20% of respondents indicated past 30-day nicotine use, 34.5% indicated past 30-day cannabis use, 57.6% indicated past 30-day alcohol use, and 2.2% indicated past 30-day other drug use. The mean count for past 30-day number of substances used was 1.96 (SD=2.41).
Table 1.
Participant Characteristics at Wave 10 Overall and Stratified by Race/Ethnicity.
| By Race/Ethnicity |
||||||||
|---|---|---|---|---|---|---|---|---|
| Overall sample (n = 1797) | Black/African American (n = 61) | Hispanic/Latino (n = 980) | Multiracial (n = 157) | AAPIa (n = 375) | White (n = 203) | Another race/ethnicityb (n = 21) | P | |
| Age (range = 20.2–23.0), mean ± SD | 21.2 ± 0.4 | 20.0 ± 0.3 | 21.2 ± 0.4 | 21.2 ± 0.4 | 21.2 ± 0.4 | 21.2 ± 0.4 | 21.2 ± 0.3 | < 0.05 |
| Sex, n (%) | < 0.05 | |||||||
| Female | 1081 (60.2%) | 31 (50.8%) | 629 (64,2%) | 99 (63.1%) | 193 (51.5%) | 118 (58.1%) | 11 (52.4%) | |
| Male | 716 (39.8%) | 30 (49,2%) | 351 (35,8%) | 58 (36.9%) | 182 (48,5%) | 85 (41.9%) | 10 (47.6%) | |
| Highest Educational Attainment | < 0.05 | |||||||
| Post-Secondary | 1351 (75.2%) | 43 (70.5%) | 741 (75.6%) | 125 (79.6%) | 242 (64.5%) | 185 (91.1%) | 15 (71.4%) | |
| HS Grad and lower | 446 (24.8%) | 18 (29.5%) | 239 (24.4%) | 32 (20.4%) | 133 (35.5%) | 18 (8.9%) | 6 (28.6%) | |
| Personal Financial Status | 0.23 | |||||||
| Live comfortably | 823 (45.8%) | 25 (41.0%) | 414 (42.2%) | 75 (47.8%) | 194 (51.7%) | 104 (51.2%) | 11 (52.4%) | |
| Meet needs with a little left | 546 (30.3%) | 21 (34.4%) | 316 (32,2%) | 43 (27.4%) | 103 (27.5%) | 58 (28.6%) | 5 (23.8%) | |
| Just meet basic expenses | 376 (20.9%) | 13 (21.3%) | 216 (22.0%) | 34 (21.7%) | 70 (18.7%) | 39 (19.2%) | 4 (19.0%) | |
| Don’t meet basic expenses | 49 (2.7%) | 2 (3.3%) | 32 (3.3%) | 5 (3.2%) | 8 (2.1%) | 1 (0.5%) | 1 (4.8%) | |
| Change in distress about police brutality (range - −4 to 4), mean ± SD | 0.84 ± 1.48 | 0.33 ± 1.54 | 0.77 ± 1.46 | 0.85 ± 1.52 | 0.95 ± 1.44 | 1.12 ± 1.50 | 1.10 ± 1.68 | < 0.05 |
| Past 30-Day Substance Use | ||||||||
| Nicotine (Yes) | 364 (20.3%) | 11 (18.0%) | 197 (20.1%) | 40 (25.5%) | 62 (16.5%) | 48 (23.6%) | 6 (28.6%) | 0.14 |
| Cannabis (Yes) | 620 (34.5%) | 18 (29.5%) | 364 (37.1%) | 55 (35.0%) | 96 (25.6%) | 74 (36.5%) | 13 (61.9%) | < 0.05 |
| Alcohol (Yes) | 1035 (57.6%) | 29 (47.5%) | 579 (59.1%) | 98 (62.4%) | 173 (46.1%) | 145 (71.4%) | 11 (52.4%) | < 0.05 |
| Other Drugs (Yes) | 40 (2.2%) | 1 (1.6%) | 27 (2.8%) | 2 (1.3%) | 4 (1.1%) | 6 (3.0%) | – | 0.38 |
| Number of substances used, mean ± SD | 1.96 ± 2.41 | 1.66 ± 2.37 | 2.14 ± 2.50 | 2.12 ± 2.61 | 1.35 ± 1.93 | 2.17 ± 2.47 | 2.43 ± 2.48 | < 0.05 |
AAPI: Asian American/Pacific Islander
Another race/ethnicity category includes middle eastern and indigenous ethnicities
P-value for chi-square or ANOVA omnibus test for differences by race/ethnicity
Age, sex, and highest educational attainment significantly differed by race/ethnicity (p < 0.05). Cannabis and alcohol use and the number of substances used also differed by race/ethnicity (p < 0.05). For example, AAPI, Hispanic/Latino, Multiracial, and White respondents had lower proportions of past 30-day cannabis use than respondents from another racial/ethnic group. Also, higher proportions of White respondents used alcohol than the five other groups. The number of substances used in the past 30 days was higher for Hispanic/Latino, multiracial, and White respondents, and respondents from other racial/ethnic groups.
Comparisons between participants included in the analytic sample versus those excluded due to study attrition and other factors are reported in Table S2. These data showed that participants excluded differed with respect to each sociodemographic characteristic, nicotine use, and number of substances used (p < 0.05 for each). The analytic sample also differed with respect to sex and race/ethnicity from participants who completed wave 8 but were lost-to-follow-up prior to wave 10 (p < 0.05 for each) and participants who were lost-to-follow-up prior to wave 8 (p < 0.05 for each).
3.2. Changes in distress about police brutality scores from 2017 to 2020
Fig. 1 displays mean changes in distress about police brutality from 2017 to 2020 by race/ethnicity. Overall, the mean distress about police brutality increased between 2017 (1.59) and 2020 (2.43) (data not shown). In 2017, White respondents had the lowest mean for distress about police brutality (1.10), while Black (2.19) and Hispanic/Latino (1.74) respondents had the highest means. From 2017–2020, every racial/ethnic subgroup showed an increase in mean distress about police brutality, with White respondents reporting the greatest change of 1.10 in 2017–2.22 in 2020, for a net increase of 101.8% (p < 0.001). The net change in mean distress about police brutality for the remaining racial/ ethnic group was as follows: 84.5% for another racial/ethnic group (p = 0.009), 67.4% for AAPI (p < 0.001), 54.5% for multiracial (p < 0.001), 44.3% for Hispanic/Latino (p < 0.001), and 15.5% for Black respondents (p = 0.20).
Fig. 1.
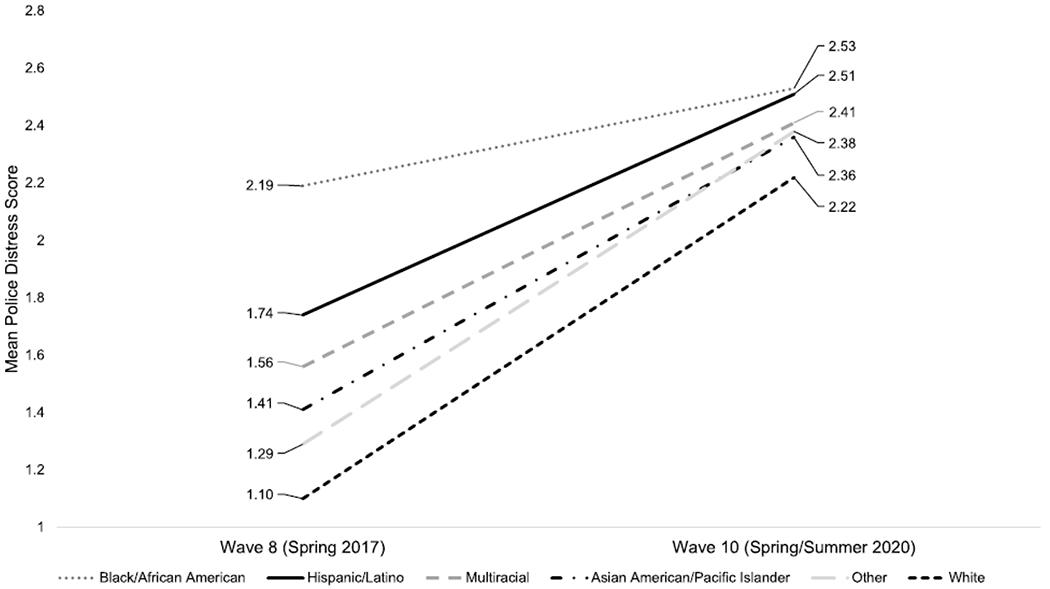
Change in distress about police brutality by race/ethnicity, 2017–2020.
3.3. Associations between changes in distress about police brutality from 2017 to 2020 and substance use in 2020
Table 2 displays associations between change in distress about police brutality and substance use overall and by race/ethnicity. Among the full sample, each single unit increase in distress about police brutality from baseline to follow-up on the five-point scale was associated with 11% (OR: 1.11, 95% CI: 1.04–1.20) higher odds of cannabis use, 13% higher odds of alcohol use (OR: 1.13, 95% CI: 1.05–1.21), and 8% higher risk of using an additional substance (RR: 1.08, 95% CI: 1.04–1.12). Our analysis of specific types of nicotine and cannabis use revealed that increased distress about police brutality from baseline to follow-up was associated with higher odds of cannabis smoking and cannabis vaping (see Table S1). However, increased distress about police brutality from baseline to follow-up was not statistically significantly associated with combustible tobacco, e-cigarette, or smokeless tobacco use. Our results did not change after conducting a sensitivity analysis that included distress about COVID-19 as a potential confounder.
There were no statistically significant interactions between change in distress about police brutality and race/ethnicity for the relationships between distress and substance use outcomes. However, in stratified models we observed associations between change in distress about police brutality and substance use in certain racial/ethnic groups, with associations varying across drug use outcomes. For example, among Black respondents, increased distress about police brutality from baseline to follow-up was associated with higher odds of cannabis use (OR: 1.66, 95% CI: 1.03–2.67) and alcohol use (OR: 1.51, 95% CI: 1.02–2.24). Moreover, increased distress about police brutality from baseline to follow-up resulted in higher risk of using an additional substance (RR: 1.35, 95% CI: 1.11–1.65) among Black respondents. Among Hispanic/Latino respondents, increased distress about police brutality from baseline to follow-up was associated with higher odds of alcohol use (OR: 1.13, 95% CI: 1.02–1.24) and higher risk of using an additional substance (OR: 1.06, 95% CI: 1.01–1.12) Statistically significant associations were observed between increased distress about police brutality from baseline to follow-up and risk of using an additional substance for respondents from another racial/ethnic group (OR: 1.30, 95% CI: 1.08–1.56) and multiracial respondents (OR: 1.13, 95% CI: 1.01–1.26). No statistically significant associations were observed among White and AAPI respondents for any substance use outcomes.
3.4. Supplementary analyses of substance use volume
Supplementary analyses examining change in distress about police brutality and substance use volume revealed that an increase in distress about police brutality from 2017 to 2020 was associated with higher alcohol use volume in 2020 in unadjusted, but not in adjusted models in the overall sample (Table S3). When looking at differences by race/ethnicity, adjusted associations between increased distress about police brutality and alcohol use volume were statistically significant among Hispanic/Latino respondents (β = 0.07, p < 0.05), but not among respondents from other racial/ethnic groups. Associations with substance use volume for cigarettes, e-cigarettes, or cannabis were not statistically significant in any models.
4. Discussion
This study demonstrates two novel findings. First, we found distress about police brutality has increased over the past several years among young people in Los Angeles, California. Second, we found that this increase may be associated with increased risk of substance use, especially within Black and Hispanic/Latino populations.
Patterns of increase in young people’s concern about police brutality from 2017 to 2020 were not equivalent across different race/ethnicity groups in this study. While White respondents had the lowest mean distress about police brutality in 2020 relative to Black respondents, they had the largest increase from 2017 to 2020. Our follow-up assessment took place right after the high-profile killings of Breonna Taylor and George Floyd. These killings were critical in galvanizing change and leading widespread discourse on police brutality in the US, such as through participation in civil rights protests and social movements (e.g., Black Lives Matter). Black and Hispanic/Latino respondents consistently had higher mean distress about police brutality at both baseline and follow-up, compared to all other racial/ethnic groups. This is consistent with prior evidence suggesting that Black and Hispanic/Latino populations report more negative perceptions of and interactions with law enforcement as compared to White populations (Edwards et al., 2019; Weitzer and Tuch, 2004) and extends these results to the current milieu, the population of youth and young adults, and a cohort from a city with an extensive history of publicized police violence.
Change in distress about police brutality was associated with use of cannabis, alcohol, and number of substances in the overall sample; however, race/ethnicity stratified analyses illuminated associations that were statistically significant in a subset of minoritized groups. Among Black and Hispanic/Latino respondents, heightened distress about police brutality during this time was associated with increased risk for substance use in this study. In contrast, we did not find evidence that inter-individual variance in changes in distress about police brutality was associated with substance use outcomes among White and AAPI respondents. One interpretation of this finding is that Black and Hispanic/Latino respondents may use substances in response to distress about police brutality, which is troubling. However, it is possible that the causal mechanisms might be bidirectional in nature. Policing or distress related to policing may lead to substance use through a stresscoping mechanism; however, early substance use, especially among younger racial/ethnic populations, may heighten the risk for additional police encounters and thus lead to more distress about policing. We attempted to mitigate bias related to reverse causality by adjusting for prior substance use at baseline, but reverse causality cannot be ruled out.
Supplementary analyses of substance use volume secondary outcomes indicated that greater increases in distress related to police brutality from 2017 to 2020 were associated with greater total number of past 30-day drinks consumed among Hispanic/Latino respondents, but not among other racial/ethnic groups. We found no other associations between increases in distress and substance use volume for cigarettes, e-cigarettes, or cannabis. Because this was a population-based sample with modest levels of substance use, on average, it is likely that there was insufficient variance in the upper end of the substance use level distribution to detect certain associations. Future research utilizing targeted sampling strategies that include greater proportions of frequent or heavy substance users (e.g., samples in substance use treatment) might be warranted to provide a sensitive test of the association between policing concerns and outcomes indicative of possible problematic substance use.
To our knowledge, only one recent study has evaluated the relationship between any exposure to police contact and substance use in the US. This study found that partner incarceration was associated with past-year illicit and licit drug use (excluding nicotine and alcohol use), and that this association was primarily driven by Black women, compared to White and Hispanic women (Bruns and Lee, 2020). These findings exemplify the effects of vicarious police contact as a race-based stressor. In our study, distress about police brutality was not associated with other drug use, though the magnitude of association implies that an effect may be detected had our analysis had more statistical power. In a study based in the UK, youth who experienced police stops by age 14 were more likely to use illicit drugs at age 17 (Jackson et al., 2022), suggesting that these relationships might also extend internationally. Collectively, these findings corroborate the literature indicating that stressors, particularly ones driven by structural racism, are related to adverse behavioral health outcomes (Anderson et al., 2020; Borrell et al., 2007; Hagle et al., 2021; Mattingly et al., 2020). If distress about police brutality is ultimately deemed to be associated with substance use, then efforts aimed to prevent use is critical, especially among racial/ethnic minority populations, for a couple of reasons. One, the health effects of substance use are alarming, especially the health effects of polysubstance use, or the use of multiple substances (Conway et al., 2013; Liu et al., 2018). Two, these relationships may be driving racial/ethnic disparities in substance use and its downstream health consequences given the plausibility that distress over police violence is unlikely to abate in disproportionately affected communities.
The current findings, alongside the collective evidence base on the devastating impact of exposure to police brutality, should be interpreted within a broader historical and social context. Illicit drug use among racial/ethnic minority groups have been the target of police jurisdiction for decades. For example, the War on Drugs going back to 1973, encouraged the police force to prioritize and target drug users, irrespective of non-drug crime happening in communities (Cooper, 2015). Since then, the gap in racial/ethnic disparities in drug-related arrests and legal treatment have widened (Cooper, 2015), and racial/ethnic minority populations remain disproportionately targeted by the police for drug-related crimes in the US (Acevedo et al., 2019; Rosenberg et al., 2017). Even if police reform were to take place in the future, the long history of police brutality against Black, Hispanic, and other populations could entrench distress over police violence over the long term for many. The conceptual model developed by Simckes et al. (2021) highlights two mechanisms through which policing affects health: (1) direct, personal experience and (2) indirect, vicarious experience (Simckes et al., 2021). While our study does not allow for stratification by experience, both types of experiences can lead to short- and long-term population health effects at the individual, community, and systems levels (Simckes et al., 2021). In Simckes et al.’s conceptual model, these effects include behavior changes such as using substances in the short term, with substantial implications such as developing dependence and other physical health effects in the long-term. At the systems level, disparities in access to treatment opportunities for racial/ethnic minorities may be exacerbated by policing, as policing may disproportionately affect racial/ethnic minorities into developing problematic substance use (Pinedo, 2019; Simckes et al., 2021).
4.1. Limitations
First, our study is observational and includes changes in distress about police brutality contemporaneous with substance use, which precludes definitive casual inferences. Second, the measures of distress about police brutality were created by aggregating items about concern, worry, and stress related to police brutality. Some respondents may be more concerned about police brutality than they are worried or stressed, and this may differ by factors such as race/ethnicity, lived experiences, place, among others. Third, this study did not contain measures of individual-level police or criminal legal system contact, which may affect both distress about police brutality and substance use. This may lead to some residual confounding in our study estimates. Fourth, this study lacked statistical power to detect race/ethnicity × police brutality distress interactions and bivariate associations of police brutality distress with substance use in certain subgroups with smaller sample sizes in race/ethnicity-stratified analyses. We were additionally unable to explore the intersection between race/ethnicity and sex (sex/gender × race/ethnicity × police brutality three-way interactions) because of sample size limitations. Fifth, substance use outcomes were not biochemically confirmed and subject to response biases. Sixth, it is difficult to parse the historical time-period effects from the developmental context because the cohort aged into emerging adulthood during this unique historical period.
Another limitation is the possible influence of selection bias. Respondents missing data or who were lost-to-follow-up differed from the analytic sample in certain sociodemographic and substance use factors, suggesting that missingness may not be completely at random. For example, Black respondents were younger on average than other racial/ethnic groups and it is possible that older Black respondents were loss to follow-up prior to wave 10. However, if attrition were associated with distress about police brutality or substance use, we would expect that our study results underestimate the association between distress and use. Participants excluded from the analytic sample might have also been at greater risk for other adverse outcomes. This missingness could decrease the variability in exposures and outcomes and potentially result in the underestimation of the true magnitude of association between police brutality concern and substance use, suggesting that the estimates presented here might be conservative. Because of the impact of the COVID-19 pandemic and other sources of societal and public health volatility during the follow-up period, many studies (including ours) have been impacted by attrition and other factors that can reduce internal or external validity. Hence, it will be important to take these results in context alongside most population-based observational research conducted during this era in which data collection for certain hard-to-reach populations were unfortunately suboptimal.
5. Conclusions and implications
This study’s finding that increasing distress about police brutality in young people over the past few years was associated with substance use, namely in Black and Hispanic/Latino respondents, and may have implications for health equity moving forward. Our results might be an additional important demonstration that adds to the body of evidence illuminating how structural racism drives population-based racial/ethnic health disparities (Simckes et al., 2021; Williams, 2018), and how it manifests through substance use in young people. Policing continues to perpetuate racial/ethnic health inequities in the US (Alang et al., 2017; Edwards et al., 2019). Systematic targeting of racial/ethnic minority populations by the police is a product of structural racism and a determinant of stress and is liable to perpetuate maladaptive stress-coping mechanisms (e.g., substance use). Thus, interventions and policies aimed to prevent and reduce substance use in young people should recognize police brutality as a determinant of use. It is imperative to address the issue at its core, beginning with the police force to reduce the incidence of police brutality, and further evaluating the range of health consequences police contact may cause (Simckes et al., 2021). Our study focuses on substance use in early life, which might be one of a myriad of possible adverse effects of police brutality that merit further research. This, combined with dismantling components of police institutions that are associated with deleterious health outcomes, and adopting improved, beneficial methods to interacting with individuals and communities, is a step in the right direction for promoting health equity (Simckes et al., 2021). Public health scholars have called for attention to investigate the effects of police brutality on health inequities in the US (Alang et al., 2017; DeVylder et al., 2020), and our study provides evidence that a relationship between distress about police brutality and substance use exists. While the effect sizes across racial/ethnic groups were moderate, addressing these relationships can make a meaningful contribution to public health given that police brutality is a widespread exposure and affects many populations across the US.
Supplementary Material
Role of Funding
Research reported in this publication was supported by grant number K24-DA048160 from the National Institute for Drug Abuse (NIDA) at the National Institutes of Health (NIH) in the United States (US) and grant number R01-CA229617 from the National Cancer Institute (NCI) and NIDA at the NIH in the US. The funders had no role in the design and conduct of the study; collection, management, analysis, or interpretation of the data; or preparation, review, or approval of the manuscript.
Footnotes
CRediT authorship contribution statement
Delvon T. Mattingly, Lauren C. Howard, Evan A. Krueger, Adam M. Leventhal: Designed the study. Lauren C. Howard: Analyzed the data. Delvon T. Mattingly: Drafted the original manuscript. All authors (Delvon T. Mattingly, Lauren C. Howard, Evan A. Krueger, Nancy L. Fleischer, Chanita Hughes- Halbert, Adam M. Leventhal) reviewed and revised the manuscript and approved the final article. Adam M. Leventhal supervised the study.
Declaration of Competing Interest
No conflict declared.
Appendix A. Supporting information
Supplementary data associated with this article can be found in the online version at doi:10.1016/j.drugalcdep.2022.109530.
References
- Acevedo A, Miles J, Panas L, Ritter G, Campbell K, Garnick D, 2019. Disparities in criminal justice outcomes after beginning treatment for substance use disorders: the influence of race/ethnicity and place. J. Stud. Alcohol Drugs 80 (2), 220–229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alang S, 2018. The more things change, the more things stay the same: race, ethnicity, and police brutality. Am. J. Public Health 108 (9), 1127–1128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alang S, McAlpine D, McCreedy E, Hardeman R, 2017. Police brutality and black health: setting the agenda for public health scholars. Am. J. Public Health 107 (5), 662–665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alang S, McAlpine D, McClain M, 2021. Police encounters as stressors: associations with depression and anxiety across race. Socius 7, 2378023121998128. [Google Scholar]
- Anderson RE, Lee DB, Hope MO, Nisbeth K, Bess K, Zimmerman MA, 2020. Disrupting the behavioral health consequences of racial discrimination: a longitudinal investigation of racial identity profiles and alcohol-related problems. Health Educ. Behav 47 (5), 706–717. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bor J, Venkataramani AS, Williams DR, Tsai AC, 2018. Police killings and their spillover effects on the mental health of black Americans: a population-based, quasi-experimental study. Lancet 392 (10144), 302–310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borrell LN, Jacobs DR Jr., Williams DR, Pletcher MJ, Houston TK, Kiefe CI, 2007. Self-reported racial discrimination and substance use in the Coronary Artery Risk Development in Adults Study. Am. J. Epidemiol 166 (9), 1068–1079. [DOI] [PubMed] [Google Scholar]
- Bowleg L, Maria Del Rio-Gonzalez A, Mbaba M, Boone CA, Holt SL, 2020. Negative police encounters and police avoidance as pathways to depressive symptoms among US Black Men, 2015-2016. Am. J. Public Health 110 (S1), S160–S166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brooks O, 2020. Police brutality and blacks: an american immune system disorder. J. Natl. Med Assoc 112 (3), 239–241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bruns A, Lee H, 2020. Partner incarceration and women’s substance use. J. Marriage Fam 82 (4), 1178–1196. [Google Scholar]
- Buehler JW, 2017. Racial/Ethnic Disparities in the Use of Lethal Force by US Police, 2010-2014. Am. J. Public Health 107 (2), 295–297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Comas-Diaz L, Hall GN, Neville HA, 2019. Racial trauma: Theory, research, and healing: Introduction to the special issue. Am. Psychol 74 (1), 1–5. [DOI] [PubMed] [Google Scholar]
- Conway KP, Vullo GC, Nichter B, Wang J, Compton WM, Iannotti RJ, Simons-Morton B, 2013. Prevalence and patterns of polysubstance use in a nationally representative sample of 10th graders in the United States. J. Adolesc. Health 52 (6), 716–723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cooper HL, 2015. War on drugs policing and police brutality. Subst. Use Misuse 50 (8–9), 1188–1194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeVylder J, Fedina L, Link B, 2020. Impact of police violence on mental health: a theoretical framework. Am. J. Public Health 110 (11), 1704–1710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Edwards F, Lee H, Esposito M, 2019. Risk of being killed by police use of force in the United States by age, race-ethnicity, and sex. Proc. Natl. Acad. Sci. USA 116 (34), 16793–16798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- GBD, 2019. Police Violence US Subnational Collaborators, 2021. Fatal police violence by race and state in the USA, 1980-2019: a network meta-regression. Lancet 398 (10307), 1239–1255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Geller A, Fagan J, Tyler T, Link BG, 2014. Aggressive policing and the mental health of young urban men. Am. J. Public Health 104 (12), 2321–2327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Graham A, Haner M, Sloan MM, Cullen FT, Kulig TC, Jonson CL, 2020. Race and Worrying About Police Brutality: The Hidden Injuries of Minority Status in America. Vict. Offenders 15 (5), 549–573. [Google Scholar]
- Hagle HN, Martin M, Winograd R, Merlin J, Finnell DS, Bratberg JP, Gordon AJ, Johnson C, Levy S, MacLane-Baeder D, Northup R, Weinstein Z, Lum PJ, 2021. Dismantling racism against Black, Indigenous, and people of color across the substance use continuum: A position statement of the association for multidisciplinary education and research in substance use and addiction. Subst. Abus 42 (1), 5–12. [DOI] [PubMed] [Google Scholar]
- Howard LC, Krueger EA, Barker JO, Cruz TB, Cwalina SN, Under JB, Barrington-Trimis JL, Leventhal AM, 2022, Young Adults’ Distress About Police Brutality Following the Death of George Floyd. Youth Soc. Advance online publication. [Google Scholar]
- Jackson DB, 2021. The case for conceptualizing youth–police contact as a racialized adverse childhood experience. Am. J. Public Health 111 (7), 1189–1191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jackson DB, Del Toro J, Semenza DC, Testa A, Vaughn MG, 2021. Unpacking racial/ethnic disparities in emotional distress among adolescents during witnessed police stops. J. Adolesc. Health 69 (2), 248–254. [DOI] [PubMed] [Google Scholar]
- Jackson DB, Testa A, Boccio CM, 2022. Police stops and adolescent substance use: findings from the United Kingdom Millennium cohort study. J. Adolesc. Health 70 (2), 305–312. [DOI] [PubMed] [Google Scholar]
- Leventhal AM, Strong DR, Kirkpatrick MG, Unger JB, Sussman S, Riggs NR, Stone MD, Khoddam R, Samet JM, Audrain-McGovern J, 2015. Association of Electronic Cigarette Use With Initiation of Combustible Tobacco Product Smoking in Early Adolescence. JAMA 314 (7), 700–707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leventhal AM, Cho J, Andrabi N, Barrington-Trimis J, 2018. Association of Reported Concern About Increasing Societal Discrimination With Adverse Behavioral Health Outcomes in Late Adolescence. JAMA Pedia 172 (10), 924–933. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Levin S, 2020, “Reign of terror”: A summer of police violence in Los Angeles. The Guardian. https://www.theguardian.com/us-news/2020/sep/06/los-angeles-police-killings-dijon-kizzee-andres-guardado (accessed 23 May 2022). [Google Scholar]
- Liu Y, Williamson V, Setlow B, Cottler LB, Knackstedt LA, 2018. The importance of considering polysubstance use: lessons from cocaine research. Drug Alcohol Depend. 192, 16–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mattingly DT, Fleischer NL, Colston DC, Mezuk B, 2020. Perceived racial discrimination and polysubstance use among African American and Afro-Caribbean adults: Results from the National Survey of American Life. J. Ethn. Subst. Abus 1–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McFarland MJ, Geller A, McFarland C, 2019. Police contact and health among urban adolescents: The role of perceived injustice. Soc. Sci. Med 238, 112487. [DOI] [PubMed] [Google Scholar]
- Pinedo M, 2019. A current re-examination of racial/ethnic disparities in the use of substance abuse treatment: Do disparities persist? Drug Alcohol Depend. 202, 162–167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosenberg A, Groves AK, Blankenship KM, 2017. Comparing black and white drug offenders: implications for racial disparities in criminal justice and reentry policy and programming. J. Drug Issues 47 (1), 132–142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simckes M, Willits D, McFarland M, McFarland C, Rowhani-Rahbar A, Hajat A, 2021. The adverse effects of policing on population health: A conceptual model. Soc. Sci. Med 281, 114103. [DOI] [PubMed] [Google Scholar]
- Strathdee SA, Hallett TB, Bobrova N, Rhodes T, Booth R, Abdool R, Hankins CA, 2010, HIV and risk environment for injecting drug users: the past, present, and future. Lancet 376(9737), 268–284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weitzer R, Tuch SA, 2004. Race and perceptions of police misconduct. Soc. Probl 51 (3), 305–325. [Google Scholar]
- Werb D, Strathdee SA, Vera A, Arredondo J, Beletsky L, Gonzalez-Zuniga P, Gaines T, 2016. Spatial patterns of arrests, police assault and addiction treatment center locations in Tijuana, Mexico. Addiction 111 (7), 1246–1256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams DR, 2018. Stress and the mental health of populations of color: advancing our understanding of race-related stressors. J. Health Soc. Behav 59 (4), 466–485. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.