

Objective:
To evaluate the impact of axillary lymph node dissection (ALND) and sentinel lymph node biopsy (SLNB) on upper limb (UL) morbidity in breast cancer patients.
Background:
Axillary de-escalation is motivated by a desire to reduce harm of ALND. Understanding the impact of axillary surgery and disparities in operative procedures on postoperative arm morbidity would better direct resources to the point of need and cement the need for de-escalation strategies.
Methods:
Embase, MEDLINE, CINAHL, and PsychINFO were searched from 1990 until March 2020. Included studies were randomized-controlled and observational studies focusing on UL morbidities, in breast surgery patients. The study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The prevalence of UL morbidity comparing SLNB and ALND at <12 months, 12 to 24 months, and beyond 24 months were analyzed.
Results:
Sixty-seven studies were included. All studies reported a higher rate of lymphedema and pain after ALND compared with SLNB. The difference in lymphedema and pain prevalence between SLNB and ALND was 13.7% (95% confidence interval: 10.5–16.8, P<0.005) and 24.2% (95% confidence interval: 12.1–36.3, P<0.005), respectively. Pooled estimates for prevalence of reduced strength and range of motion after SLNB and ALND were 15.2% versus 30.9% and 17.1% versus 29.8%, respectively. Type of axillary surgery, greater body mass index, and radiotherapy were some of the predictors for UL morbidities.
Conclusions:
Prevalence of lymphedema after ALND was higher than previously estimated. ALND patients experienced greater rates of lymphedema, pain, reduced strength, and range of motion compared with SLNB. The findings support the continued drive to de-escalate axillary surgery.
Keywords: axillary lymph node dissection, axillary surgery, breast surgery, lymphedema, pain, quality-of-life, range of motion, sentinel lymph node biopsy, strength, upper limb morbidity
Survival after breast cancer treatment has improved longitudinally as a result of more targeted and personalized treatments.1 This translates to many more breast cancer survivors experiencing long-term adverse consequences of therapy. Axillary treatment can leave patients with symptoms of arm and shoulder pain and/or reduced range of motion (ROM), with adverse impact on activities of daily living, health-related quality-of-life (HRQoL), and the ability to return to work.1 Moreover, axillary radiation and axillary lymph node dissection (ALND) are known to be significant risk factors for development of lymphedema and reduced ROM.1 While the introduction of sentinel lymph node biopsy (SLNB) in the 1990s reduced the number of ALND’s, there remains an important and yet to be quantified degree of arm morbidity associated with SLNB.2
Axillary de-escalation is driven by both a desire to minimize injury and a growing awareness of the oncological safety of axillary conservation.3 Understanding the effect of axillary surgery and differences in surgical intervention on postoperative arm and shoulder morbidity would allow for more effective resource allocation and would reinforce the importance of de-escalation strategies. Furthermore, it is critical to investigate which procedures or treatments are associated with the highest rates of morbidity so that clinicians can counsel patients regarding strategies with improved HRQoL outcomes.
The last systematic review investigating the adverse effects of breast cancer treatment on the upper limb (UL) was published in 2014,1 subsequently many important trials have been published.3–6 Whilst prior systematic reviews of the literature regarding UL morbidity have been performed, due to multiple methodologies of data presentation, the complexity of quantitative assessment through meta-analysis was precluded.1 Other systematic reviews focused on particular outcomes7,8 (eg, lymphedema or pain), medical therapies9 or included nonvalidated outcomes.1 Contemporary studies have improved in quality, including randomized-controlled trials (RCTs) and prospective cohort trials in the last decade, which might alter the results.3,4,6,10,11 In the current meta-analysis, only objective data measured by validated tools for lymphedema, ROM and strength or measured using validated questionnaires for UL function, pain, and HRQoL were included to ensure standardization wherever possible. We appraised data at an individual-study level with raw variables for preoperative to postoperative outcomes representing an internal difference metric which could then be expanded sequentially for study group synthesis. This was made possible by applying meta-analytical outcome weighting to each study and applying inverse variance methodologies. Data was synthesized from validated outcome measures to better characterize the adverse effects after breast cancer treatment on UL morbidity, in particular ALND and SLNB.
METHODS
Search Strategy and Selection Criteria
A systematic literature search was conducted using the databases of Embase, MEDLINE, CINAHL, and PsychINFO from 1990 to March 2020 according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidelines (Supplemental Digital Content 1, http://links.lww.com/SLA/E169). The review was registered with PROSPERO (CRD42020199311). The search terms included keywords as described in Supplemental Digital Content 2, http://links.lww.com/SLA/E170.
Included studies (Supplemental Digital Content 3, http://links.lww.com/SLA/E171) were RCTs and observational studies focusing on UL function in patients treated with breast surgery±additional therapies. Outcomes must be measured using validated tools. Papers that met inclusion criteria were reviewed using PRISMA methodological checklist (Supplemental Digital Content 1, http://links.lww.com/SLA/E169). Case reports, case series, letters, systematic and literature reviews, unpublished or ongoing trials, studies prior to 1990s, non-English studies, posttreatment interventional studies, and studies focusing only on chemotherapy/hormonal therapy were excluded. The articles were uploaded into COVIDENCE (www.covidence.org) which is a web-based screening and data extraction tool. Abstracts and titles were screened independently on COVIDENCE by 2 reviewers (N.A.C.B. and N.K.) and a third reviewer (A.L.) helped arbitrate in case of disputes. Full text screening was completed by NACB/NK and AL/OG.
Data Extraction
Six outcomes were extracted based on the most common findings from reviewed studies (Supplemental Digital Content 4, http://links.lww.com/SLA/E172). Outcomes that were objectively measured for lymphedema, ROM and strength or measured using validated tools for UL function, pain, and HRQoL and studies focusing on ALND and SLNB were included in the review. Adverse effects of treatment were subcategorized based on time-point of data capture and defined as <12 months, 12 to 24 months, and more than 24 months. Methods of outcome reporting is described in Supplemental Digital Content 5, http://links.lww.com/SLA/E173.
Risk of Bias Analysis
Two authors (N.A.C.B. and Y.G.) independently assessed the risk of bias of each study using the Risk of Bias 2 (RoB2) tool and Risk of Bias in Nonrandomized Studies of Interventions (ROBINS-I) tool for RCTs and nonrandomized studies, respectively. Disagreements were resolved by discussion, and when necessary, a third person arbitrated (A.D).
Statistical Analyses
Meta-analysis was performed where possible on the prevalence rates of UL morbidity after ALND and SLNB. Pooled prevalence was calculated with a random effects model and presented with 95% confidence intervals (CI) utilizing the DerSimonian & Laird method as a between‐study variance estimator. Heterogeneity was assessed by the I 2 statistic (<30%—low, 31%–59%—moderate, >60%—high) and the Cochran Q statistic. Analyses were performed using Stata version 15 (Stata Corp LP; College Station, TX). Probability values (P value) ≤0.05 were considered statistically significant.
RESULTS
The initial search yielded 7415 articles (Fig. 1). Nineteen additional articles were identified from existing references and 5 additional articles were identified from other source. Two hundred and seventy-nine articles fulfilled our primary selection criteria. Articles were organized by outcome measure of interest and the 6 most common outcomes (Supplemental Digital Content 4, http://links.lww.com/SLA/E172) were selected, leaving 67 studies focusing on SLNB and/or ALND included in the review (Supplemental Digital Content 6, http://links.lww.com/SLA/E174).
FIGURE 1.
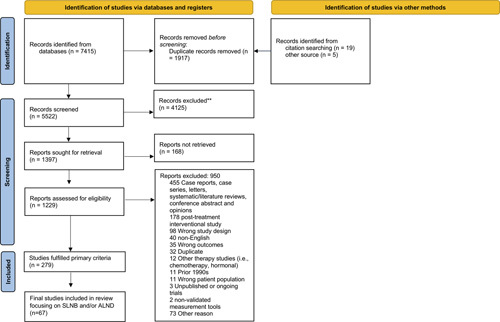
PRISMA flow diagram.
Lymphedema
Rates of Lymphedema After ALND and SLNB
Among 38 studies that reported the prevalence of lymphedema at different time intervals, the pooled estimate for the prevalence of lymphedema after ALND at <12 months (Fig. 2a),3,4,6,11–23 12 to 24 months (Fig. 2b),4,6,11–13,16,22,24–28 and more than 24 months (Fig. 2c)3,4,10–12,29–46 was observed to be 16.5% (16 studies, n=3515, 95% CI: 11–22, I 2= 97.1%, P<0.0005), 24.6% (12 studies, n=1971; 95% CI: 11–38, I 2= 98.3%, P<0.0005) and 23.6% (23 studies, n=5288; 95% CI: 16.4–30.9, I 2= 98.3%, P<0.0005), respectively.
FIGURE 2.
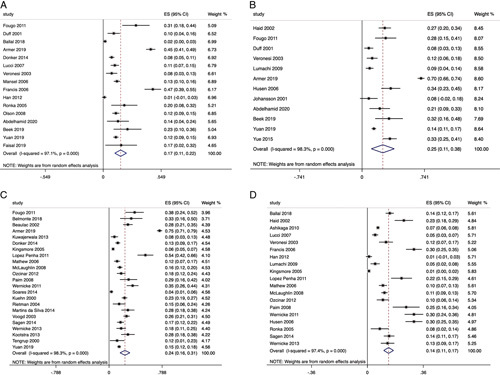
A, Prevalence of lymphedema after ALND at <12 months. B, Prevalence of lymphedema after ALND between 12 and 24 months. C, Prevalence of lymphedema after ALND at more than 24 months. D, Differences of lymphedema prevalence between ALND and SLNB.
The equivalent pooled estimate for the prevalence of lymphedema after SLNB at <12 months,14,15,18–20,47,48 12 to 24 months,16,24–26,49 and more than 24 months31–36,43,44,50 was observed to be 7.5% (6 studies, n=3866; 95% CI: 4.9–10.1, I 2= 79.8%, P<0.0005), 3.7% (4 studies, n=491; 95% CI: 1.8–5.6, I 2= 70%, P<0.0005), and 5.9% (11 studies, n=3136; 95% CI: 3.6–8.1, I 2= 82.8%, P<0.0005), respectively.
There was a statistically significant difference in the prevalence of lymphedema between ALND and SLNB, as illustrated in Fig. 2d (19 studies, n=9381; difference in pooled estimate=13.7%, 95% CI: 10.5–16.8, I 2= 97.4%, P<0.0005). All studies included in the meta-analysis14–16,19,24,25,31,33–37,50 reported higher rate of lymphedema following ALND.
Rates of Lymphedema After ALND and Axillary Reverse Mapping
The prevalence of lymphedema after ALND+axillary reverse mapping (ARM) at <12 months6,11,22,23 and more than 12 months6,11,22,28 was observed to be 3.3% (4 studies, n=657; 95% CI: 1.9–4.7, I 2= 0%, P =0.437) and 6.4% (4 studies, n=762; 95% CI: 1.9–10.9, I 2= 72%, P =0.013), respectively.
Immediate Versus Completion ALND
There was no significant difference in the rate of lymphedema when comparing immediate and completion ALND particularly in long-term follow-up. At 12 and 36 months, patients who underwent immediate ALND had no significant difference in lymphedema rate compared with completion ALND (17.8 vs. 8.6%, P=0.09214; 10.3% vs. 14.3%, P=0.65).30
ALND and Radiotherapy
ALND conferred a higher rate of lymphedema compared with axillary radiotherapy (RT) at 1 (8% vs. 6%, P=0.332), 3 (10% vs. 6%, P=0.08), and 5 (13% vs. 5%, P=0.0009) years.3 At 5 years, this difference was observed to be statistically significant (P=0.0009).3 Similarly, another RCT observed higher rates of lymphedema following ALND and breast irradiation (ALND-breast irradiation=22% vs. ALND=12%).46 Individuals who received ALND and regional lymph node radiation (RLNR) had the greatest 5-year risk of lymphedema (31.2%, Hazard ratio: 0.613, 95% CI: 0.403–0.935, P=0.023)51 when compared with ALND without RLNR (24.6%) and SLNB with RLNR (12.2%, Hazard ratio: 0.285, 95% CI: 0.149–0.545, P=0.0002). In a trial comparing RT versus non-RT, irradiated patients had a higher rate of lymphedema than nonirradiated (14% vs. 3%, P=not significant).52
Factors Increasing Risk of Lymphedema
Significant predictors for lymphedema included ALND (P<0.0001),51 chemotherapy (P<0.0001),51 high body mass index (P<0.0001),51 diabetes (P<0.05),5 palpable tumor (P<0.05),5 weight gain exceeding 10% of baseline value (P<0.001),5 and RLNR (P<0.0001).51 Lymphedema was also associated with a higher number of metastatic axillary lymph nodes (P<0.05),53 radical mastectomy (P<0.05),53 advanced age (P=0.006),50 the presence of seroma (P<0.001),54 and the amount of time passed after the procedure (P<0.05).54
Pain
SLNB and ALND
According to 12 studies that reported the prevalence of pain after ALND at different time intervals, the pooled estimates at <12 months (Fig. 3a),12,16,20,55–57 between 12 and 24 months (Fig. 3b),12,26,36,55,58 and beyond 24 months (Fig. 3c)12,16,24,40,46,59 was 40% (6 studies, n=1335; 95% CI: 23.8–56.2, I 2= 97.8%, P<0.0005), 38.5% (5 studies, n=540; 95% CI: 15.7–61.4, I 2= 96.2%, P<0.0005), and 32.9% (6 studies, n=426; 95% CI: 18.8–47, I 2= 90.9%, P<0.0005), respectively.
FIGURE 3.
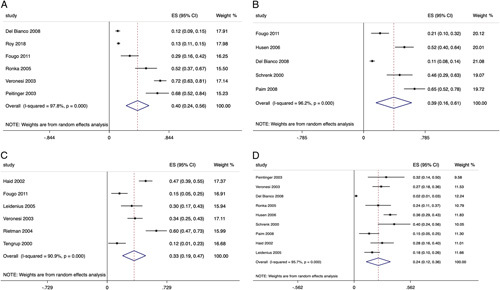
A, Prevalence of pain after ALND at <12 months. B, Prevalence of pain after ALND between 12 and 24 months. C, Prevalence of pain after ALND at more than 24 months. D, Differences of pain prevalence between SLNB and ALND.
In contrast, the pooled estimate for the prevalence of pain after SLNB at any different follow-up intervals was 21.7% (10 studies, n=1039; 95% CI: 13.9–29.5, I 2= 91.8%, P<0.0005).16,20,24,26,36,55,57–59 Nine studies comparing SLNB and ALND found the latter led to greater pain, with the pooled difference estimate of 24.2% (Fig. 3d) (9 studies, n=1788; 95% CI: 12.1–36.3, I 2= 95.7%, P<0.0005).16,20,24,26,36,55,57–59
ROM
Prevalence of Reduced ROM and Flexion After ALND and SLNB
A greater proportion of patients experienced reduced ROM following ALND6,14,21,22,26,27,44,46,58,60,61 compared with SLNB,14,26,44,47,48,60 with a pooled estimate of 29.8% (11 studies, n=826, 95% CI: 17.5–42, I 2= 98.1%, P<0.0005) and 17.1% (6 studies, n=5809, 95% CI: 11.1–23.1, I 2= 96%, P<0.0005), respectively. Similarly, the pooled estimate for prevalence of reduced flexion after ALND20,36,39,40,45,59 and SLNB20,36,48,59 was 27.2% (6 studies, n=662, 95% CI: 15.2–39.2, I 2= 91.4%, P<0.0005) and 20% (4 studies, n=283, 95% CI: 11.5–28.6, I 2= 70.8%, P<0.0005), respectively.
Impact of Radiation on ROM
Reduced ROM was more prevalent in patients receiving axillary, supraclavicular, and/or chest wall RT compared with nonirradiated patients (52% vs. 15%, P<0.01).52 Similarly, a greater rate of reduced ROM was observed when combining ALND and axillary RT compared with ALND only (82% vs. 28%).62 In an RCT comparing ALND and axillary RT, ROM did not differ significantly between the 2 groups (1 years: P=0.29; 5 years: P=0.47).3
Predictors of Reduced ROM
ALND (P<0.001),63 RT (P<0.05),63 and side of dominance (P<0.05)64 were found to be significant predictors of decreased ROM. In addition, increased observation time (P<0.05),53 advanced age (P=0.011),48 radical modified mastectomy (P<0.05),53 higher body mass index (P<0.05),53 chemotherapy (P=0.002),65 presence of tumor-positive lymph nodes (P=0.014),65 expander-implant (P<0.05),65 and the latissimus dorsi flap (P<0.0001)65 were significant risk factors to decreased arm/shoulder function.
Strength
Prevalence of Reduced Strength After SLNB and ALND
The pooled estimate of the prevalence of reduction in any strength (eg, grip, abduction, internal rotators strength) after ALND and SLNB was 30.9% (6 studies, n=825, 95% CI: 15.3–46.5, I 2= 96.5%, P<0.0005)10,36,39,40,43,45 and 15.2% (5 studies, n=437, 95% CI: 5.2–25.2, I 2= 91.8%, P<0.0005),10,36,43,45,48 respectively. The ALND group experienced more strength loss than the SLNB. In both SLNB and ALND, a decrease in strength of shoulder external rotation/abduction and ROM remained 5 to 7 years after surgery.10,45
Predictors and Association With Reduced Strength
Shoulder-arm function/strength 6 weeks following surgery and age were the greatest predictors of long-term shoulder-arm function/strength.45 Women who had surgery on their nondominant side demonstrated a larger loss of grip strength compared with those who had surgery on their dominant side (P=0.001).66 In addition, strength loss was associated with ALND surgery (P=0.046) and having received physical/occupational therapy (P=0.036) during follow-up.60
UL Function
Prevalence of Reduced UL Function
The pooled estimate for the prevalence of reduced UL function after any breast cancer treatment was 34.4%% (3 studies, n=880, 95% CI: 17.2–51.7, I 2= 91.4%, P<0.0005).48,64,67
Association With Worse UL Function
Postmastectomy radiation and chemotherapy resulted in considerably worse (P=0.0093) UL function and HRQoL.68 Women with a history of diabetes (P=0.0249), rheumatoid arthritis (P<0.0001), or shoulder pain (P=0.002), a lower income (P<0.0001), and less health literacy (P=0.0062) were associated with poorer UL function.68
HRQoL
HRQoL Post-SLNB and ALND
Studies comparing SLNB and ALND found that patients who received SLNB experienced better HRQoL than those who had ALND. Compared with global HRQoL scores preoperatively, the global scores postoperatively measured by European Organization for Research and Treatment of Cancer core quality-of-life (EORTC-QLQ-C30) improved by 15% (3 studies, n=155, 95% CI: 4.4–26.1, I 2= 99.9%, P<0.0005) in SLNB and 6% (3 studies, n=92, 95% CI: 0.7–11, I 2=99.8%, P<0.0005) in ALND.57,69,70
Association With HRQoL
Factors associated with poorer level of functioning and HRQoL were stage of disease (P=0.005),71 menopausal status (P=0.031),71 co-morbidities (P=0.032),71 chemotherapy (P=0.009),71 postoperative complications (P=0.02),72 upper-body function (P<0.001),72 greater psychological burden (P=0.001),72 had no confidante for social and emotional support (P<0.01),72 had unmet health care needs (P<0.001),72 and low health self-efficacy (P<0.001).72
Risk of Bias Assessment
Overall, the risk of bias for included RCTs and nonrandomized studies were high or serious (Fig. 4). Risk of bias for individual studies can be found in Supplemental Digital Content 7, http://links.lww.com/SLA/E175 and 8, http://links.lww.com/SLA/E176.
FIGURE 4.
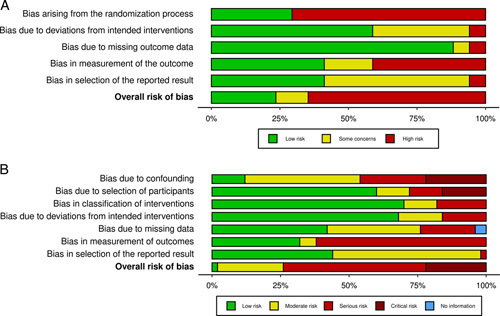
A, RoB2 tool for assessing risk of bias of randomized-controlled trials. B, ROBINS-I tool for assessing risk of bias of nonrandomized studies.
DISCUSSION
The pooled estimates for the short and long-term prevalence of lymphedema are higher than reported in prior systematic reviews.1,7 ALND was observed to have greater rates of lymphedema, pain, reduced strength, and ROM compared with SLNB. There is limited data available on UL function measured by DASH after ALND and SLNB, and there is no standardization in the measurement of UL morbidities making it difficult to compare between different treatments.
Prior systematic reviews focused on specific outcomes such as lymphedema7 or pain8 and medical treatments such as RT and surgery.9 One systematic review1 examined all the adverse effects related to breast cancer treatments, but did not perform a meta-analysis. As far as we know, this is the first systematic review where meta-analysis has been performed to better estimate the prevalence of lymphedema, pain, reduced ROM, and reduced strength following ALND and SLNB at different time intervals where possible.
The pooled estimates of the prevalence of lymphedema after ALND appear to increase with longer follow-up, which is consistent to findings from the review by Hidding et al, 1 although meta-analysis was not performed. In addition, the results are similar to the meta-analysis by DiSipio et al7 in which arm lymphedema increased longitudinally up to 2 years following diagnosis or surgery, at which point it appeared to decline. The authors also estimated 21% incidence of lymphedema after any breast cancer treatment.7 The prevalence of lymphedema after ALND in the current review using objective validated outcomes is higher compared with estimates by DiSipio et al,7 particularly in the long term (>24 mo, 23.6% vs. 18.6%).7 Compared with ALND, it is interesting that the prevalence of lymphedema following SLNB in our meta-analysis decreases with time. In this instance, time may not increase the prevalence of lymphedema; rather, the results may suggest that early lymphedema following SLNB is more prevalent, but it can resolve with time (with or without intervention). The pooled prevalence of pain appears to improve over time and this finding is consistent with the meta-analysis by Wang et al.8
In our current meta-analysis, there is a reduction of lymphedema rate when combining ALND and ARM approach compared with ALND only or SLNB in the first 12 months. Yuan et al,11 which was included in this meta-analysis, introduced a modified ARM approach called iDEntification and Preservation of ARm lymphaTic system (DEPART) that allows a thorough identification of the axillary lymphatic system and hence may further reduce the lymphedema occurrences. The ARM approach has the potential to minimize the rate of lymphedema, but it has not been adopted globally due to the uncertainty of its long-term oncological effects. The concern with the ARM approach is the anatomical crossover variations between breast and arm lymph nodes.28 Therefore, some of the preserved arm lymphatics may introduce the risk of metastasis, which can be a potential pitfall of this technique. Hence, large-scale studies with a longer follow-up period are required to assess the oncological safety of this method.
In comparison to SLNB, ALND patients have a higher rate of lymphedema, pain, decreased strength, and ROM. The current meta-analysis also demonstrates that the addition of axillary radiation to ALND increases the risk of UL morbidity especially lymphedema and reduced ROM which is consistent with a prior systematic review.9 While the type of axillary surgery is important in contributing toward the reduced ROM,43,57,58 arm positioning intraoperatively may also be a factor. The arm positioning for either SLNB or ALND is similar. Regardless of the type of breast cancer surgery they have, many breast cancer patients experience persistent arm/shoulder dysfunction for more than 12 months following surgery.1 Variations in shoulder ROM based on the type of surgery are not fully understood. When shoulder recovery patterns were analyzed by the number of lymph nodes removed, recovery patterns did not differ by the number of lymph nodes.73 This may suggest that arm positioning during the surgery may have an important role in determining the impact on ROM.
De-escalation of axillary surgery is motivated by a desire to reduce UL morbidities associated with ALND and subsequently improve patients’ HRQoL.3 The current meta-analysis adds to the evidence to de-escalate axillary surgery, such as SLNB, or to perform better surgery, such as exploring the ARM approach6 or the LYmphatic Microsurgical Preventive Healing Approach (LYMPHA)74 procedure when appropriate. There is also a need to provide patients and healthcare professionals with more information about the likely outcomes of their treatment. Therefore, resources can be allocated at an appropriate time to manage these life-debilitating morbidities.
There is a paucity of evidence on UL function following ALND and SLNB as indicated by DASH questionnaires. Although DASH was a frequently used patient-reported outcome for UL evaluation, there were few studies assessing UL function following ALND and SLNB. A recent RCT demonstrated that patients who are at increased risk of developing UL complications who received physiotherapy-led structured exercise had improved UL function as measured by DASH questionnaires 1 year following breast cancer treatment compared with usual care, which was proven to be cost-effective.75 The findings from this study support the implementation of an exercise program postbreast cancer treatment, strengthening the need to recognize patients who are at risk and intervene early.
The measurement of UL morbidities following breast cancer treatments is not standardized, making comparisons challenging. Many tools used are subjective, such as questionnaires, which may cause recall bias.2 Our group has found the use of wearable activity monitors helpful as a tool to assess function and UL activities after breast cancer treatment.2 This approach could improve the quality of data in the future when comparing the postoperative outcomes of limb function.
This study has several limitations that should be considered. Language bias might occur as we only included studies published in English. The lack of a universally agreed approach for documenting and assessing shoulder morbidity, making comparisons between treatment types and studies limited. The prevalence of lymphedema, reduced ROM and reduced strength may be under-reported as the outcomes measured by subjective tools were not included in the review. There was significant statistical heterogeneity in the studies included in the meta-analysis so that any interpretations of outcome measures require measured consideration. To mitigate these limitations, we included studies published from non-English speaking countries. Only objective data and data measured by validated tools were included in the meta-analysis to ensure standardization wherever possible. There is an urgent need to standardize the measurement of UL morbidities in future studies to reduce heterogeneity.
CONCLUSION
This systematic review demonstrates that pooled estimates for the short-term and long-term prevalence of lymphedema after ALND are higher than previously estimated. ALND patients were observed to have higher rates of lymphedema, pain, reduced strength, and ROM compared with SLNB. There is an urgent need to develop a standardized tool with updated technology that is easy to use in a clinical setting to assess these morbidities to ensure better comparison between treatments and studies. Much work remains to be done to compare the effects of different breast cancer treatments and compute the costs associated with complications of treatment so that we can provide better support for breast cancer survivors. The findings reinforce the need to continue de-escalating surgical management of the axilla, including expanding the use of axillary irradiation instead of ALND in selected group of patients and exploring lymphatic microsurgery or ARM approach as feasible alternatives and adjuncts.
Supplementary Material
ACKNOWLEDGMENTS
The authors express their gratitude to Ping Wu (MSc, PhD) (Statistician and Data Scientist) for reviewing the data analysis and the manuscript as well as other colleagues from Institute Global Health and Innovation and the Department of Surgery and Cancer, Imperial College London for their support.
Footnotes
N.A.C.B., R.M.K., D.R.L. and A.D. designed the study. N.A.C.B. and R.M.K. designed the study protocol and methodology. N.A.C.B., N.K., O.G., and A.L. screened the studies and interpreted the data. N.A.C.B., Y.G., and A.D. assessed the risk of bias. N.A.C.B. and H.A. analyzed and synthesized the study data. N.A.C.B. prepared the first draft of the manuscript. N.A.C.B., R.M.K., N.K., O.G., A.L., Y.G., A.D., A.D., H.A., and D.R.L. were involved in the critical revision of the draft manuscript. All authors approved the final version.
A.D. is the Chair of the Health Security initiative at Flagship Pioneering UK Ltd and Hutan Ashrafian is the Chief Scientific Officer of Preemptive Medicine and Health Security initiative at Flagship Pioneering UK.
The authors report no conflicts of interest.
Supplemental Digital Content is available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal's website, www.annalsofsurgery.com.
Contributor Information
Nur Amalina Che Bakri, Email: nchebakr@ic.ac.uk.
Richard M. Kwasnicki, Email: richard.kwasnicki07@imperial.ac.uk.
Naairah Khan, Email: naairahkhan25@gmail.com.
Omar Ghandour, Email: mrog96@gmail.com.
Alice Lee, Email: Alice.lee13@imperial.ac.uk.
Yasmin Grant, Email: yasmin.grant14@imperial.ac.uk.
Aleksander Dawidziuk, Email: aleksander.dawidziuk16@imperial.ac.uk.
Ara Darzi, Email: a.darzi@imperial.ac.uk.
Hutan Ashrafian, Email: H.ashrafian@imperial.ac.uk.
Daniel R. Leff, Email: d.leff@imperial.ac.uk.
REFERENCES
- 1.Hidding JT, Beurskens CH, van der Wees PJ, et al. Treatment related impairments in arm and shoulder in patients with breast cancer: a systematic review. PLoS One. 2014;9:e96748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Che Bakri NA, Kwasnicki RM, Dhillon K, et al. Objective assessment of postoperative morbidity after breast cancer treatments with wearable activity monitors: The “BRACELET” Study. Ann Surg Oncol. 2021;28:5597–5609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Donker M, van Tienhoven G, Straver ME, et al. Radiotherapy or surgery of the axilla after a positive sentinel node in breast cancer (EORTC 10981-22023 AMAROS): a randomised, multicentre, open-label, phase 3 non-inferiority trial. Lancet Oncol. 2014;15:1303–1310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Armer JM, Ballman KV, McCall L, et al. Lymphedema symptoms and limb measurement changes in breast cancer survivors treated with neoadjuvant chemotherapy and axillary dissection: results of American College of Surgeons Oncology Group (ACOSOG) Z1071 (Alliance) substudy. Support Care Cancer. 2019;27:495–503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wetzig N, Gill PG, Espinoza D, et al. Sentinel-lymph-node-based management or routine axillary clearance? Five-year outcomes of the RACS Sentinel Node Biopsy Versus Axillary Clearance (SNAC) 1 Trial: Assessment and Incidence of True Lymphedema. Ann Surg Oncol. 2017;24:1064–1070. [DOI] [PubMed] [Google Scholar]
- 6.Abdelhamid MI, Bari AA, Farid MI, et al. Evaluation of axillary reverse mapping (ARM) in clinically axillary node negative breast cancer patients—randomised controlled trial. Int J Surg. 2020;75:174–178. [DOI] [PubMed] [Google Scholar]
- 7.DiSipio T, Rye S, Newman B, et al. Incidence of unilateral arm lymphoedema after breast cancer: a systematic review and meta-analysis. Lancet Oncol. 2013;14:500–515. [DOI] [PubMed] [Google Scholar]
- 8.Wang L, Cohen JC, Devasenapathy N, et al. Prevalence and intensity of persistent post-surgical pain following breast cancer surgery: a systematic review and meta-analysis of observational studies. Br J Anaesth. 2020;125:346–357. [DOI] [PubMed] [Google Scholar]
- 9.Shaitelman SF, Chiang YJ, Griffin KD, et al. Radiation therapy targets and the risk of breast cancer-related lymphedema: a systematic review and network meta-analysis. Breast Cancer Res Treat. 2017;162:201–215. [DOI] [PubMed] [Google Scholar]
- 10.Belmonte R, Messaggi-Sartor M, Ferrer M, et al. Prospective study of shoulder strength, shoulder range of motion, and lymphedema in breast cancer patients from pre-surgery to 5 years after ALND or SLNB. Support Care Cancer. 2018;26:3277–3287. [DOI] [PubMed] [Google Scholar]
- 11.Yuan Q, Wu G, Xiao SY, et al. Identification and preservation of arm lymphatic system in axillary dissection for breast cancer to reduce arm lymphedema events: a randomized clinical trial. Ann Surg Oncol. 2019;26:3446–3454. [DOI] [PubMed] [Google Scholar]
- 12.Fougo JL, Dinis-Ribeiro M, Araujo C, et al. Impact of lymphadenectomy on axillary recurrence and morbidity of the upper limb in breast cancer patients with negative sentinel node. a prospective randomised study. Cir Esp. 2011;89:307–316. [DOI] [PubMed] [Google Scholar]
- 13.Duff M, Hill AD, McGreal G, et al. Prospective evaluation of the morbidity of axillary clearance for breast cancer. Br J Surg. 2001;88:114–117. [DOI] [PubMed] [Google Scholar]
- 14.Ballal H, Hunt C, Bharat C, et al. Arm morbidity of axillary dissection with sentinel node biopsy versus delayed axillary dissection. ANZ J Surg. 2018;88:917–921. [DOI] [PubMed] [Google Scholar]
- 15.Lucci A, McCall LM, Beitsch PD, et al. Surgical complications associated with sentinel lymph node dissection (SLND) plus axillary lymph node dissection compared with SLND alone in the American College of Surgeons Oncology Group Trial Z0011. J Clin Oncol. 2007;25:3657–3663. [DOI] [PubMed] [Google Scholar]
- 16.Veronesi U, Paganelli G, Viale G, et al. A randomized comparison of sentinel-node biopsy with routine axillary dissection in breast cancer. N Engl J Med. 2003;349:546–553. [DOI] [PubMed] [Google Scholar]
- 17.Mansel RE, Fallowfield L, Kissin M, et al. Randomized multicenter trial of sentinel node biopsy versus standard axillary treatment in operable breast cancer: the ALMANAC Trial. J Natl Cancer Inst. 2006;98:599–609. [DOI] [PubMed] [Google Scholar]
- 18.Francis WP, Abghari P, Du W, et al. Improving surgical outcomes: standardizing the reporting of incidence and severity of acute lymphedema after sentinel lymph node biopsy and axillary lymph node dissection. Am J Surg. 2006;192:636–639. [DOI] [PubMed] [Google Scholar]
- 19.Han JW, Seo YJ, Choi JE, et al. The efficacy of arm node preserving surgery using axillary reverse mapping for preventing lymphedema in patients with breast cancer. J Breast Cancer. 2012;15:91–97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Ronka R, von Smitten K, Tasmuth T, et al. One-year morbidity after sentinel node biopsy and breast surgery. Breast. 2005;14:28–36. [DOI] [PubMed] [Google Scholar]
- 21.Olson JA, Jr, McCall LM, Beitsch P, et al. Impact of immediate versus delayed axillary node dissection on surgical outcomes in breast cancer patients with positive sentinel nodes: results from American College of Surgeons Oncology Group Trials Z0010 and Z0011. J Clin Oncol. 2008;26:3530–3535. [DOI] [PubMed] [Google Scholar]
- 22.Beek MA, Gobardhan PD, Klompenhouwer EG, et al. A patient- and assessor-blinded randomized controlled trial of axillary reverse mapping (ARM) in patients with early breast cancer. Eur J Surg Oncol. 2020;46:59–64. [DOI] [PubMed] [Google Scholar]
- 23.Faisal M, Sayed MG, Antonious K, et al. Prevention of lymphedema via axillary reverse mapping for arm lymph-node preservation following breast cancer surgery: a randomized controlled trial. Patient Saf Surg. 2019;13:35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Haid A, Koberle-Wuhrer R, Knauer M, et al. Morbidity of breast cancer patients following complete axillary dissection or sentinel node biopsy only: a comparative evaluation. Breast Cancer Res Treat. 2002;73:31–36. [DOI] [PubMed] [Google Scholar]
- 25.Lumachi F, Basso SM, Bonamini M, et al. Incidence of arm lymphoedema following sentinel node biopsy, axillary sampling and axillary dissection in patients with breast cancer. In Vivo. 2009;23:1017–1020. [PubMed] [Google Scholar]
- 26.Husen M, Paaschburg B, Flyger HL. Two-step axillary operation increases risk of arm morbidity in breast cancer patients. Breast. 2006;15:620–628. [DOI] [PubMed] [Google Scholar]
- 27.Johansson KIC, Albertsson M, Ekdahl C. Arm lymphoedema, shoulder mobility and muscle strength after breast cancer treatment ? a prospective 2-year study. Eur J Physiother. 2001;3:55–66. [Google Scholar]
- 28.Yue T, Zhuang D, Zhou P, et al. A prospective study to assess the feasibility of axillary reverse mapping and evaluate its effect on preventing lymphedema in breast cancer patients. Clin Breast Cancer. 2015;15:301–306. [DOI] [PubMed] [Google Scholar]
- 29.Beaulac SM, McNair LA, Scott TE, et al. Lymphedema and quality of life in survivors of early-stage breast cancer. Arch Surg. 2002;137:1253–1257. [DOI] [PubMed] [Google Scholar]
- 30.Kuwajerwala NK, Feczko C, Dekhne N, et al. Comparison of lymphedema in patients with axillary lymph node dissections to those with sentinel lymph node biopsy followed by immediate and delayed ALND. Am J Clin Oncol. 2013;36:20–23. [DOI] [PubMed] [Google Scholar]
- 31.Kingsmore DB, Hole DJ, Gillis CR, et al. Axillary recurrence in breast cancer. Eur J Surg Oncol. 2005;31:226–231. [DOI] [PubMed] [Google Scholar]
- 32.Lopez Penha TRSJ, Heuts EM, Voogd AC, et al. Prevalence of lymphoedema more than five years after breast cancer treatment. Eur J Surg Oncol. 2011;37:1059–1063. [DOI] [PubMed] [Google Scholar]
- 33.Mathew J, Barthelmes L, Neminathan S, et al. Comparative study of lymphoedema with axillary node dissection versus axillary node sampling with radiotherapy in patients undergoing breast conservation surgery. Eur J Surg Oncol. 2006;32:729–732. [DOI] [PubMed] [Google Scholar]
- 34.McLaughlin SA, Wright MJ, Morris KT, et al. Prevalence of lymphedema in women with breast cancer 5 years after sentinel lymph node biopsy or axillary dissection: patient perceptions and precautionary behaviors. J Clin Oncol. 2008;26:5220–5226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Ozcinar B, Guler SA, Kocaman N, et al. Breast cancer related lymphedema in patients with different loco-regional treatments. Breast. 2012;21:361–365. [DOI] [PubMed] [Google Scholar]
- 36.Paim CR, de Paula Lima ED, Fu MR, et al. Post lymphadenectomy complications and quality of life among breast cancer patients in Brazil. Cancer Nurs. 2008;31:302–309; quiz 310–301. [DOI] [PubMed] [Google Scholar]
- 37.Wernicke AG, Goodman RL, Turner BC, et al. A 10-year follow-up of treatment outcomes in patients with early stage breast cancer and clinically negative axillary nodes treated with tangential breast irradiation following sentinel lymph node dissection or axillary clearance. Breast Cancer Res Treat. 2011;125:893–902. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Soares EW, Nagai HM, Bredt LC, et al. Morbidity after conventional dissection of axillary lymph nodes in breast cancer patients. World J Surg Oncol. 2014;12:67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Kuehn T, Klauss W, Darsow M, et al. Long-term morbidity following axillary dissection in breast cancer patients--clinical assessment, significance for life quality and the impact of demographic, oncologic and therapeutic factors. Breast Cancer Res Treat. 2000;64:275–286. [DOI] [PubMed] [Google Scholar]
- 40.Rietman JS, Dijkstra PU, Debreczeni R, et al. Impairments, disabilities and health related quality of life after treatment for breast cancer: a follow-up study 2.7 years after surgery. Disabil Rehabil. 2004;26:78–84. [DOI] [PubMed] [Google Scholar]
- 41.Martins da Silva RC, Rezende LF. Assessment of impact of late postoperative physical functional disabilities on quality of life in breast cancer survivors. Tumori. 2014;100:87–90. [DOI] [PubMed] [Google Scholar]
- 42.Voogd AC, Ververs JM, Vingerhoets AJ, et al. Lymphoedema and reduced shoulder function as indicators of quality of life after axillary lymph node dissection for invasive breast cancer. Br J Surg. 2003;90:76–81. [DOI] [PubMed] [Google Scholar]
- 43.Sagen A, Kaaresen R, Sandvik L, et al. Upper limb physical function and adverse effects after breast cancer surgery: a prospective 2.5-year follow-up study and preoperative measures. Arch Phys Med Rehabil. 2014;95:875–881. [DOI] [PubMed] [Google Scholar]
- 44.Wernicke AG, Shamis M, Sidhu KK, et al. Complication rates in patients with negative axillary nodes 10 years after local breast radiotherapy after either sentinel lymph node dissection or axillary clearance. Am J Clin Oncol. 2013;36:12–19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Kootstra JJ, Dijkstra PU, Rietman H, et al. A longitudinal study of shoulder and arm morbidity in breast cancer survivors 7 years after sentinel lymph node biopsy or axillary lymph node dissection. Breast Cancer Res Treat. 2013;139:125–134. [DOI] [PubMed] [Google Scholar]
- 46.Tengrup I, Tennvall-Nittby L, Christiansson I, et al. Arm morbidity after breast-conserving therapy for breast cancer. Acta Oncol. 2000;39:393–397. [DOI] [PubMed] [Google Scholar]
- 47.Wilke LG, McCall LM, Posther KE, et al. Surgical complications associated with sentinel lymph node biopsy: results from a prospective international cooperative group trial. Ann Surg Oncol. 2006;13:491–500. [DOI] [PubMed] [Google Scholar]
- 48.De Groef A, Van Kampen M, Tieto E, et al. Arm lymphoedema and upper limb impairments in sentinel node-negative breast cancer patients: a one year follow-up study. Breast. 2016;29:102–108. [DOI] [PubMed] [Google Scholar]
- 49.Golshan M, Martin WJ, Dowlatshahi K. Sentinel lymph node biopsy lowers the rate of lymphedema when compared with standard axillary lymph node dissection. Am Surg. 2003;69:209–211; discussion 212. [PubMed] [Google Scholar]
- 50.Ashikaga T, Krag DN, Land SR, et al. Morbidity results from the NSABP B-32 trial comparing sentinel lymph node dissection versus axillary dissection. J Surg Oncol. 2010;102:111–118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.McDuff SGR, Mina AI, Brunelle CL, et al. Timing of lymphedema after treatment for breast cancer: when are patients most at risk? Int J Radiat Oncol Biol Phys. 2019;103:62–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Hojris I, Andersen J, Overgaard M, et al. Late treatment-related morbidity in breast cancer patients randomized to postmastectomy radiotherapy and systemic treatment versus systemic treatment alone. Acta Oncol. 2000;39:355–372. [DOI] [PubMed] [Google Scholar]
- 53.Nesvold IL, Dahl AA, Lokkevik E, et al. Arm and shoulder morbidity in breast cancer patients after breast-conserving therapy versus mastectomy. Acta Oncol. 2008;47:835–842. [DOI] [PubMed] [Google Scholar]
- 54.Paiva DM, Rodrigues VO, Cesca MG, et al. Prevalence of lymphedema in women undergoing treatment for breast cancer in a referral center in southeastern Brazil. BMC Womens Health. 2013;13:6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Del Bianco P, Zavagno G, Burelli P, et al. Morbidity comparison of sentinel lymph node biopsy versus conventional axillary lymph node dissection for breast cancer patients: results of the sentinella-GIVOM Italian randomised clinical trial. Eur J Surg Oncol. 2008;34:508–513. [DOI] [PubMed] [Google Scholar]
- 56.Roy P, Leizorovicz A, Villet R, et al. Systematic versus sentinel-lymph-node-driven axillary-lymph-node dissection in clinically node-negative patients with operable breast cancer. Results of the GF-GS01 randomized trial. Breast Cancer Res Treat. 2018;170:303–312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Peintinger F, Reitsamer R, Stranzl H, et al. Comparison of quality of life and arm complaints after axillary lymph node dissection vs sentinel lymph node biopsy in breast cancer patients. Br J Cancer. 2003;89:648–652. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Schrenk P, Rieger R, Shamiyeh A, et al. Morbidity following sentinel lymph node biopsy versus axillary lymph node dissection for patients with breast carcinoma. Cancer. 2000;88:608–614. [DOI] [PubMed] [Google Scholar]
- 59.Leidenius M, Leivonen M, Vironen J, et al. The consequences of long-time arm morbidity in node-negative breast cancer patients with sentinel node biopsy or axillary clearance. J Surg Oncol. 2005;92:23–31. [DOI] [PubMed] [Google Scholar]
- 60.Monleon S, Ferrer M, Tejero M, et al. Shoulder strength changes one year after axillary lymph node dissection or sentinel lymph node biopsy in patients with breast cancer. Arch Phys Med Rehabil. 2016;97:953–963. [DOI] [PubMed] [Google Scholar]
- 61.Devoogdt N, Van Kampen M, Christiaens MR, et al. Short- and long-term recovery of upper limb function after axillary lymph node dissection. Eur J Cancer Care (Engl). 2011;20:77–86. [DOI] [PubMed] [Google Scholar]
- 62.Nagel PH, Bruggink ED, Wobbes T, et al. Arm morbidity after complete axillary lymph node dissection for breast cancer. Acta Chir Belg. 2003;103:212–216. [DOI] [PubMed] [Google Scholar]
- 63.Rietman JS, Geertzen JH, Hoekstra HJ, et al. Long term treatment related upper limb morbidity and quality of life after sentinel lymph node biopsy for stage I or II breast cancer. Eur J Surg Oncol. 2006;32:148–152. [DOI] [PubMed] [Google Scholar]
- 64.Kopec JA, Colangelo L, Land S, et al. Relationship between arm morbidity and patient-reported outcomes following surgery in women with node-negative breast cancer: NSABP Protocol B-32. J Support Oncol. 2013;11:22–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Woo KJ, Lee KT, Mun GH, et al. Effect of breast reconstruction modality on the development of postmastectomy shoulder morbidity. J Plast Reconstr Aesthet Surg. 2018;71:1761–1767. [DOI] [PubMed] [Google Scholar]
- 66.Perez CS, das Neves LMS, Vacari AL, et al. Reduction in handgrip strength and electromyographic activity in women with breast cancer. J Back Musculoskelet Rehabil. 2018;31:447–452. [DOI] [PubMed] [Google Scholar]
- 67.Koehler LA, Hunter DW, Blaes AH, et al. Function, shoulder motion, pain, and lymphedema in breast cancer with and without axillary web syndrome: an 18-month follow-up. Phys Ther. 2018;98:518–527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Chrischilles EA, Riley D, Letuchy E, et al. Upper extremity disability and quality of life after breast cancer treatment in the Greater Plains Collaborative clinical research network. Breast Cancer Res Treat. 2019;175:675–689. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Arraras JI, Manterola A, Illarramendi JJ, et al. Quality of life evolution in elderly survivors with localized breast cancer treated with radiotherapy over a three-year follow-up. Breast. 2018;41:74–81. [DOI] [PubMed] [Google Scholar]
- 70.Bogusevicius A, Cepuliene D. Quality of life after sentinel lymph node biopsy versus complete axillary lymph node dissection in early breast cancer: a 3-year follow-up study. Medicina (Kaunas). 2013;49:111–117. [PubMed] [Google Scholar]
- 71.Jassim GA, Whitford DL. Quality of life of Bahraini women with breast cancer: a cross sectional study. BMC Cancer. 2013;13:212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.DiSipio T, Hayes S, Newman B, et al. What determines the health-related quality of life among regional and rural breast cancer survivors? Aust N Z J Public Health. 2009;33:534–539. [DOI] [PubMed] [Google Scholar]
- 73.Min J, Kim JY, Yeon S, et al. Change in shoulder function in the early recovery phase after breast cancer surgery: a prospective observational study. J Clin Med. 2021;10:3416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Johnson AR, Kimball S, Epstein S, et al. Lymphedema incidence after axillary lymph node dissection: quantifying the impact of radiation and the lymphatic microsurgical preventive healing approach. Ann Plast Surg. 2019;82(suppl 3):S234–S241. [DOI] [PubMed] [Google Scholar]
- 75.Bruce J, Mazuquin B, Canaway A, et al. Exercise versus usual care after non-reconstructive breast cancer surgery (UK PROSPER): multicentre randomised controlled trial and economic evaluation. BMJ. 2021;375:e066542. [DOI] [PMC free article] [PubMed] [Google Scholar]