

Abstract
Peritoneal carcinomatosis, which is the most common malignant process of the peritoneal cavity, originates mostly from colorectal, gastric, and gynaecological malignancies. The differential diagnosis is broad and covers primary peritoneal malignancies, as well as many benign disorders such as endometriosis, and inflammatory and infectious diseases. Peritoneal implants tend to locate in the areas of the physiological stasis of the peritoneal fluid: pelvic peritoneal reflections, right and left paracolic gutters, superior part of the sigmoid mesocolon, ileocolic area, and the right subdiaphragmatic space. The 3 most common imaging findings are ascites, nodular implants, and infiltration of the peritoneal fatty tissue. Several imaging modalities may be applied in patients with peritoneal carcinomatosis. Ultrasound has low sensitivity and specificity, and therefore plays only a marginal role. Computed tomography is the method of choice, due to its availability, cost-effectiveness, and relatively high sensitivity. The sensitivity of magnetic resonance imaging depends on the size of peritoneal implants – in cases of implants larger than 10 mm is comparable to CT. Some studies suggest that PET/CT may be the most sensitive method, yet its usefulness in everyday practice is controversial. The Peritoneal Carcinomatosis Index (PCI) is a scale used to assess the tumour burden in the peritoneum and may serve as a communication tool between clinicians and radiologists. The imaging findings may influence the surgeon’s decision on performing cytoreductive surgery, which may be followed by intraperitoneal chemotherapy (HIPEC or EPIC procedures). The introduction of these therapeutic methods has significantly improved the life expectancy of patients with peritoneal carcinomatosis.
Keywords: oncology, peritoneum, metastases, peritoneal carcinomatosis
Introduction
Every radiologist encounters peritoneal carcinomatosis in his/her daily practice because its most common sources are among the most prevalent types of cancer. Thorough knowledge of peritoneal anatomy, physiology, seeding mechanisms, differential diagnoses, and imaging findings in patients with peritoneal carcinomatosis may lead to a substantial Improvement in the quality of radiology reports.
Peritoneal physiology and circulation of the peritoneal fluid
Peritoneal cavity, peritoneal fluid, and pathways of its circulation
The peritoneal cavity is a potential space located between the parietal and the visceral peritoneum [1,2]. The parietal peritoneum covers the diaphragm, lines the abdominal wall, and secretes peritoneal fluid [1,3]. The visceral peritoneum partially or completely surrounds the viscera. The peritoneum provides mobility of the organs, enables fluid transport and peritoneal dialysis, and hosts immunocompetent cells [2,3]. In healthy individuals, the peritoneal cavity contains 5-20 ml of serosal fluid, formed mostly from the plasma transudate and the ovarian exudate. It enables frictionless movement of the viscera and mediates the exchange of substances and immune cells between the peritoneal cavity and the plasma [3].
The route of circulation of the peritoneal fluid explains the propensity of metastases to occupy certain peritoneal compartments. The fluid accumulated in pelvic recesses moves upward to the subphrenic compartment, preferen-tially via the deeper right paracolic gutter. On the left, this upward movement is blocked by the phrenicocolic ligament. The falciform ligament prevents the mixture of the peritoneal fluid between the right and left subphrenic spaces. Those barriers can be easily forced by a large amount of ascitic fluid [1,2].
Peritoneal metastases – most common sources
Peritoneal carcinomatosis is the most common cause of diffuse peritoneal involvement [4]. Ovarian and gastrointestinal carcinoma have the highest tendency to meta-stasize to the peritoneum. Other causes of peritoneal deposits are carcinomas of the pancreas, breast (the most common extra-abdominal source of peritoneal malignancy), appendix, biliary tract, liver, lung, and genitourinary tract [2].
Imaging findings
Typical findings indicating peritoneal carcinomatosis are ascites, omental and mesenteric infiltration, and scattered peritoneal nodules. Occasionally, bowel or ureteral obstruction may occur [6].
About 70% of patients with peritoneal carcinomatosis present with ascites. Ascites is caused by the obstructed reabsorption of peritoneal fluid at the level of the right subdiaphragmatic lymphatic chain and increased secretion of the intraperitoneal fluid due to VPF secreted by tumour cells [4]. Omental and mesenteric invasion is manifested by increased density and nodular lesions within the omental fat (“the omental cake”). A solid, stellate mass in the mesentery, clustering of the small bowel loops, gastric wall thickening, scalloping of the liver surface, peritoneal thickening (smooth, nodular, or plaque-like), and abnormal peritoneal enhancement are other findings [4]. A sleeve-like pattern of growth along the bowel serosa may also be seen [9].
Peritoneal nodules predominate in the paracolic gutters, the pouch of Douglas, the sigmoid mesocolon, the ileocaecal region, or in the parietal peritoneum along the anterior abdominal wall [4]. Calcification and cystic components may be present [6].
Computed tomography (CT) studies may be falsenegative in cases with multiple, scattered peritoneal micro-nodules [4]. Ascites increases the detection rate of the parietal peritoneal nodules, whereas proper opacification of the bowel lumen and the large amount of the intraperitoneal fat are essential for visualization of visceral peritoneal and mesenteric involvement [6] (Table 1 and Figures 1-3).
Table 1.
Peritoneal implants – most common sites of involvement [2]
| Hepatic ligaments |
| Gallbladder fossa |
| Splenic and hepatic surface |
| Morrison pouch |
| Gastrohepatic ligament |
| Hepatic porta |
| Transverse and the sigmoid mesocolon |
| Paracolic gutters |
| Small bowel mesentery |
| Greater omentum |
| Small bowel serosa |
| Pouch of Douglas and the uterovesical recess in females |
| Rectovesical recess in males |
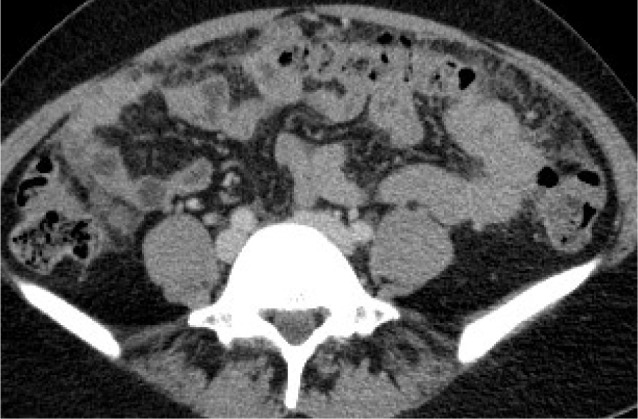
Figure 1.

Female, 61-year-old. Serous ovarian cancer. A) Computed tomo graphy (CT) – small implant in the left paracolic gutter. B) CT – thickened pelvic peritoneum in the pouch of Douglas. C) Axial T2WI. D) DWI (b = 800 s/mm2)
Figure 3.
Female, 42-year-old. Lobular breast cancer. Computed tomography – omental caking
Figure 2.

Female, 78-year-old. Endometrial cancer. A) Computed tomography (CT) – nodular implants in the abdominal peritoneum. B) CT – nodular implants in the greater omentum
The role of diagnostic imaging
The key role of diagnostic imaging of the peritoneal carcinomatosis is to differentiate patients who are surgical candidates from those with extensive disease or unfavourable lesion sites, who should be treated with neoadjuvant or palliative chemotherapy. Proper selection is crucial because major morbidity (23-35% [10]) and mortality (2-4% [10]) associated with cytoreductive surgery may prevail over the potential benefits. Furthermore, preoperative imaging helps to identify suspicious regions that should be biopsied in addition to the routine sampling of the omentum, the diaphragm, and the mesentery and retroperitoneal lymph nodes. Imaging findings combined with measurements of serum CA-125 levels are used to assess the response to chemotherapy and to detect relapse [6,10].
Ultrasound
Ultrasound (US) is often an initial study performed in patients complaining about abdominal distension, but it is inaccurate for staging. Only 69% of peritoneal metastases, 32% of nodal lesions, and 57% of parenchymal metastases are detected by ultrasound. US may be useful for guiding biopsies in patients who need histological validation before chemotherapy [11-15]. On ultrasound, peritoneal implants present as hypo- to isoechoic nodular or plaque-like lesions with colour Doppler flow or as diffuse thickening of the peritoneum. A combination of transabdominal and transvaginal approach is an optimal solution. Several factors influence the sensitivity of ultrasound: the presence of gas hinders the detection of bowel wall and mesenteric implants, whereas ascites improves its performance. However, there are some data suggesting that in selected abdominal regions ultrasound may perform quite well. According to a Chinese study, ultrasound was superior to CT in the detection of pelvic metastases, and splenic and hepatic subcapsular metastases: 92.3% vs. 43.6%, 87.5 vs. 62.5%, and 83.3 vs. 58.3%, respectively. Interestingly, US detected more bowel serosal metastases than CT: 64% vs. 16%, respectively. However, CT proved to be more effective in detecting mesenteric, lateral peritoneal, and omental implants [16]. A Czech study, conducted on a large group of patients with ovarian cancer, showed that combined transvaginal and trans-abdominal ultrasound had good accuracy (91%) in predicting rectosigmoid infiltration. The method was also highly specific (> 0.9) but poor sensitive (< 0.5) in the detection of metastatic involvement of retroperitoneal lymph nodes [17].
Computed tomography
CT is a basic modality for staging and follow-up. Exposure to ionizing radiation and its potential effects are secondary matters in the case of oncologic patients [10]. Owing to technical advances, CT has reached a sensitivity of 79-86% and specificity of 82-89% in the detection of peritoneal involvement [10]; however, when the lesion size is less than 10 mm, the sensitivity drops to 7-28%. The sensitivity of CT, particularly in patients without ascites, depends on the anatomical location of implants. Metastases in the lesser omentum, mesenteric root, left subdiaphragmatic compartment, and small bowel serosa are often missed. Administration of positive oral contrast media may increase the detection of bowel wall implants, but negatively influences the ability to detect calcified metastases [2]. Low tissue contrast, artifacts associated with peristalsis, poor distention of the gastrointestinal tract and the urinary bladder, postoperative anatomical distortion, and small implant size further compromise the detection of peritoneal carcinomatosis [6,11]. A major advantage of CT is its ability to detect pulmonary metastases and lymphadenopathy [10].
Proper contrast enhancement is achieved after injection of around 600 mg of iodine per kg of lean body weight (body mass minus fat). Some centres advocate routine use of hyoscine butyl bromide IV. Arterial phase images should be obtained at 35 s and venous phase images at 70 s. Delayed-phase images after 8-10 min should be obtained if ureteral obstruction is suspected [9].
Magnetic resonance imaging
Due to its relatively high cost and long duration, magnetic resonance imaging (MRI) is rather a second-choice modality. Contrast-enhanced MRI and CT have comparable overall sensitivities (90-95.5% [6,23]); however, MRI can be superior to CT when it comes to the detection of small, sub-centimetre lesions, especially located in the subphrenic area and in the bowel serosa. The accuracy of MRI and CT is similar in relapse detection, although malignant and benign lymphadenopathy cannot be differentiated by both modalities.
Standard MRI protocols include both T1W and T2W images in axial and coronal planes, fat-suppressed T1W and T2W images, and dynamic contrast-enhanced sequences and diffusion-weighted imaging (DWI) [2,6]. Abnormal contrast enhancement of the peritoneum 5 min after contrast agent administration may be an early sign of involvement [8]. Some centres advocate the use of oral contrast media (water or pineapple juice) and intramuscular injection of hyoscine butyl bromide [9,18].
An introduction of DWI to standard pelvic and abdominal protocols in patients with ovarian cancer increased the number of detected lesions in 21-29% of cases. DWI is useful in staging, establishing differential diagnoses and evaluation of the response to therapy. Metastases larger than 5 mm may be detected by DWI-MRI.
Respiratory and cardiac motion artifacts hamper the depiction of subdiaphragmatic and hepatic subcapsular lesions. High DWI signal of normal spleen, lymph nodes, and bowel mucosa may result in false-positive findings. False-negative findings are caused by increased ADC values in cystic, necrotic, and mucinous metastases [2,6]. Another limitation of MRI is insufficient experience in its interpretation among radiologists [8]. As far as correlation between MRI and surgical findings is concerned, MRI performs quite well in the pelvis and central abdomen, but it has low sensitivity in detecting bowel wall involvement [19].
Some studies suggest a relationship between ADC values of peritoneal lesions and response to treatment. Successful chemotherapy potentially causes an increase in ADC values even before a decrease in lesion size. Additionally, high ADC values before treatment may be linked to poor response to chemotherapy. The ability of dynamic contrast-enhanced MRI sequences to differentiate benign from malignant lesions or to assess response to chemotherapy is another subject of studies.
Nuclear medicine
PET/CT predominantly uses a glucose analogue, 18F-FDG, as a radiotracer. It is based on the concept that glucose and similarly 18F-FDG reach highest concentrations in cells with a high metabolic rate (neoplasms, inflammatory lesions, physiological metabolic hyperactivity). Combined with CT imaging, PET allows precise localization of the sites of abnormally increased metabolic activity. Peritoneal implants manifest as focal or diffuse abnormal 18F-FDG uptake in bowel serosa, omental fat, and the peritoneum [6]. Sensitivity of PET/CT ranges between 78 and 97%, and the specificity is about 55-90% [11]. Small, scattered serosal implants mimicking physiological bowel activity, low metabolic rate in mucinous lesions, size of implants below the spatial resolution of the method,and absent uptake in small pulmonary metastases result in false-negative findings. On the other hand, PET/CT may detect nodal metastases before lymphadenopathy occurs.
PET/CT has a sensitivity of 72-100% and specificity of 40-90% in detection of clinically and biochemically silent relapse. Although some studies showed that the addition of PET/CT to routine diagnostic imaging changed staging in 55-64% and influenced clinical decisions in 34-59% of cases [6], findings are inconsistent and it is still debatable if performing PET/CT before CRS has any added value compared to standard imaging [20].
PET/MR combines the advantage of metabolic asses-sment of PET and high soft tissue contrast of MRI. Although data are limited, it is believed that its usefulness is more pronounced in imaging of the local extent of the disease (in cases of cervical and endometrial cancer) than in depicting peritoneal metastases [21].
Which modality should be chosen?
A study conducted on a small group of 15 patients has shown that MRI, PET/CT, and CT were equally effective in detecting peritoneal dissemination; however, the results were of no statistical significance. MRI proved to be the most sensitive modality, whereas PET/CT was the most specific one [22]. Conversely, a study by Low et al. demonstrated a far better performance of MRI compared to CT (per site sensitivity of 95% and 55%, specificity of 70% and 86%, respectively) [23]. Another study suggested that combined MR and CT determine preoperative Peritoneal Carcinomatosis Index (PCI) more precisely than CT alone. These findings were especially true regarding regions 0 (central abdomen), 6 (pelvis), and 3 (left upper abdomen) [24]. A meta-analysis by Laghi et al. showed that it was prudent to regard CT as a first-line imaging modality, although it underestimated the preoperative PCI in 12-33% of cases. MRI reached a sensitivity of 86% and specificity of 88%. When it comes to a comparison between CT and PET/CT, the sensitivity was 66% and 82%, and the specificity was 77% and 93%, respectively [13]. Another study found that in 17.5% of cases CT failed to correctly diagnose the extent of peritoneal carcinomatosis. In patients with PCI 0-20, it overestimated the disease burden in 12.5% and underestimated the extent of the disease in 5%. CT predicted optimal cytoreduction with a sensitivity of 90%, while lapa-roscopy had a sensitivity of 89%, and a combination of both methods increased the sensitivity to 97%. The specificities of those 3 methods were very similar, between 39 and 42% [25].
Relapse may be manifested by miliary nodules and therefore may initially be missed on imaging unless the radiologist is aware of clinical and laboratory findings [8]. PET/CT should be considered in ovarian cancer survivors with rising CA-125 levels and equivocal imaging findings, to detect nodal or extra-abdominal metastases (except in the early postoperative period when findings may be misleading [8]). Imaging findings are often inconsistent with serum marker levels, and patients with extensive intraperitoneal recurrence may show normal marker levels. Some authors suggest performing baseline MRI shortly after the surgery to avoid mistaking normal postoperative findings of peritoneal and bowel serosal thickening and enhancement for disease recurrence. Postoperative changes gradually resolve on subsequent studies, whereas findings related to relapse progress [26].
Differential diagnoses
It is vital to differentiate peritoneal carcinomatosis from other diffuse peritoneal pathologies because some of them require only medical, not surgical, treatment. Conditions that on imaging may mimic peritoneal carcinomatosis are listed in Table 2. Practically, lymphomatosis, tuberculosis, mesothelioma, and pseudomyxoma peritonei are differential diagnoses that should be primarily considered [2] (Figures 4 and 5).
Table 2.
Peritoneal carcinomatosis – differential diagnoses
| 1. Primary peritoneal malignancies | |
| Malignant mesothelioma [5] | |
| Primary peritoneal carcinoma [2] | |
| Desmoplastic small round cell tumour (DSRCT) [5] | |
| Primary peritoneal lymphoma [2] | |
| 2. Desmoid tumour [5] | |
| 3. Solitary fibrous tumour (SFT) [5] | |
| 4. Pseudomyxoma peritonei [6] | |
| 5. Peritoneal lymphomatosis [4] | |
| 6. Carcinoid tumour [5] | |
| 7. Non-malignant conditions | |
| Most common: | |
| Peritoneal tuberculosis [4] | |
| Actinomycosis [6] | |
| Splenosis implants [4] | |
| Endometriosis [6] | |
| Foreign body reaction [7] | |
Figure 4.
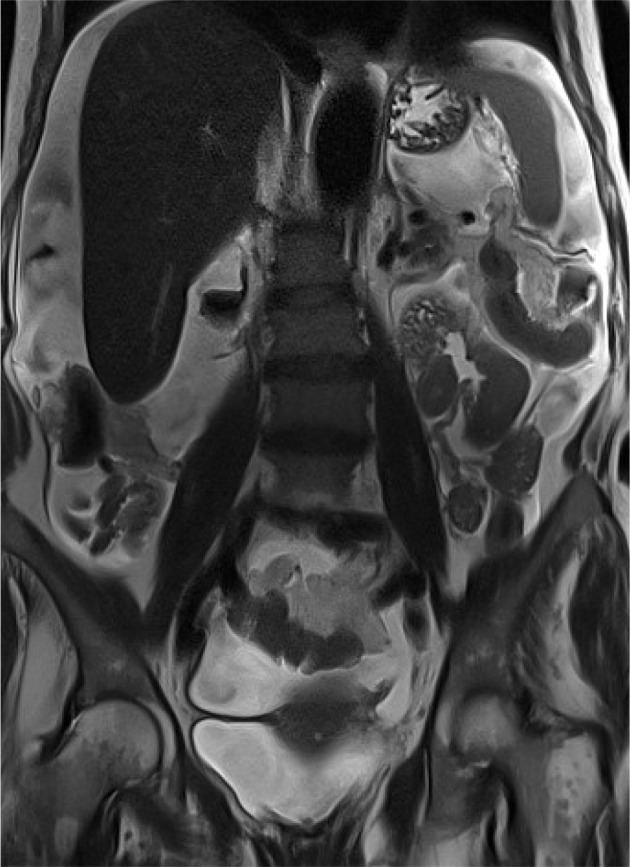
Female, 69-year-old. Primary peritoneal carcinoma. Magnetic resonance imaging, coronal T2WI – massive ascites
Figure 5.
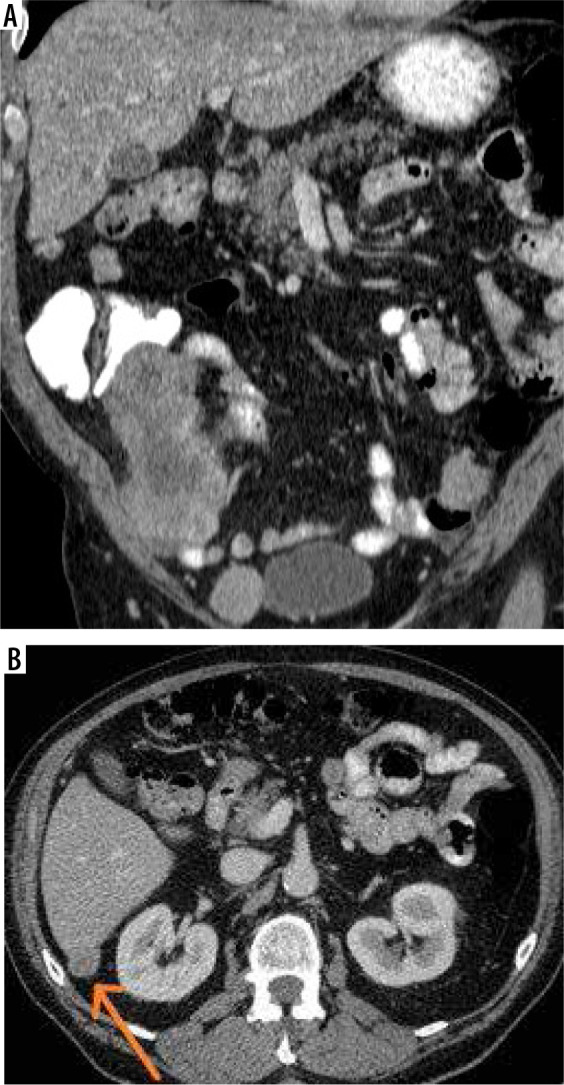
Male, 74-year-old. GIST. A) Computed tomography (CT) – metastatic involvement of the peritoneum. B) CT – subcapsular implant on the liver surface
Treatment methods
Currently, a combination of cytoreductive surgery (CRS) and intraperitoneal chemotherapy (HIPEC or EPIC) is regarded as the best therapeutic option for patients with peritoneal carcinomatosis. The introduction of these methods has significantly improved the life expectancy of patients. Depending on the type of primary malignancy, the increase in survival has been from 3-24 to 40-62 months [27]. Many studies emphasize the benefits of CRS and HIPEC in patients with colorectal carcinoma. Among other malignancies treated by a combination of these methods are ovarian cancer, primary peritoneal carcinoma, neuroendocrine tumours, peritoneal mesothelioma, and gastric cancer.
Unfortunately, these extensive procedures have significant complications like fistula formation, obstruction, and anastomotic leaks [12]. The mortality associated with CRS followed by HIPEC is about 2-4%, and major morbidity ranges 23-35% [10]. The operation should be performed on a carefully selected group of patients in good general condition, in whom optimal cytoreduction is feasible [12].
Cytoreductive surgery
Cytoreductive surgery (CRS) was introduced by Paul Sugarbaker and his team at the Washington Cancer Institute in the 1980s. Its goal is to remove all visible peritoneal deposits by multiple organ resections and peritonectomy procedures [12]. CRS comprises such procedures as pelvic peritonectomy, greater omentectomy, lesser omentectomy, cholecystectomy, multiple resections of the bowel, diaphragmatic stripping, and removal of the liver capsule, sigmoid, rectum, mesorectum, and female genital tract. In cases of splenic involvement, splenectomy is performed [27].
Intraperitoneal chemotherapy
Hyperthermic intraperitoneal chemotherapy (HIPEC) is performed in the operating theatre immediately after the CRS. Chemotherapeutic agents heated up to 41-43°C are instilled into the peritoneal cavity, along with intravenous administration of a complementary agent. The patient is gently moved to provide equal distribution of the fluid in the peritoneal cavity. Finally, after 1-1.5 hours, the fluid is removed and the surgical incision is sutured. Several mechanisms explain the effectiveness of HIPEC. First, high temperature increases cytotoxicity of chemotherapeutic agents and preferentially destroys tumour cells because their mitochondria are more sensitive to hyperthermia. A chemotherapeutic agent (cisplatin, oxaliplatin, or mitomycin C) directly administered into the peritoneal cavity reaches higher concentration than the same agent administered intravenously due to the presence of the peritoneum-plasma barrier [12,28]. Additionally, fluid introduced into the peritoneal cavity during HIPEC is drained by the portal venous system; therefore, the chemotherapeutic agent reaches a high concentration in the liver and may destroy parenchymal micrometastases [29]. Because penetration of the chemotherapeutic agent is limited to 2-5 mm, optimal cytoreduction (R0 and R1 resections) is crucial [12].
EPIC (early postoperative intraperitoneal chemothera-py) consists of several cycles of chemotherapy admini-stered in the early postoperative period directly to the peritoneal cavity through percutaneous catheters [12].
BIPSC/NIPS (bidirectional/neoadjuvant intraperitoneal and systemic chemotherapy) is a novel approach developed in Japan as an attempt to find an optimal solution for patients with gastric cancer. The procedure comprises neoadjuvant systemic and intraperitoneal chemotherapy followed by CRS, HIPEC, and EPIC. The concept is to reduce tumour burden with NIPS, remove remaining macroscopic lesions with CRS and HIPEC and to destroy residual microscopic peritoneal deposits with EPIC [30].
Eligibility to surgery
Before surgery 3 main factors have to be considered: the extent of the peritoneal involvement, the possibility of obtaining complete cytoreduction, and postoperative quality of life [10]. There are no universal criteria for inoperability, and in each case the decision depends on local experience. Therefore, the role of the radiologist is not only to determine disease as resectable or unresectable but also to point out the findings that may pose technical difficulty during surgery [8].
First of all, distant metastases, pleural involvement, and retroperitoneal lymphadenopathy have to be ruled out. This may be accomplished by performing a contrast-enhanced CT of the thorax, abdomen, and pelvis. In problematic cases other imaging modalities like MRI, ultra-sound, and PET/CT may help. It is important to differentiate intraparenchymal liver metastases from subcapsular implants because they are contraindications to surgery except in selected cases of colorectal cancer. Each lesion should be reported (size, location) along with its relation to the bowel wall, ureters, and vessels. It is vital to determine if the small bowel is focally or diffusely involved and whether there are any signs of ileus. Large metastases (> 5 cm) in the bowel serosa or in close proximity to the bowel wall are negative predictive factors because they increase the risk of intestinal obstruction. Enlarged peritoneal, retroperitoneal, and pelvic lymph nodes have to be reported, and any existing hernias should be carefully examined for the presence of tumour deposits [10].
Laparotomy remains the reference standard for the staging of peritoneal carcinomatosis. Exploratory laparoscopy may be performed optionally in patients with ambiguous imaging findings [12]. Diagnostic laparoscopy, however, may reduce the number of unnecessary attempts of CRS by 31% [10].
Contraindications to surgery (Table 3)
Table 3.
Absolute and relative contraindications to surgery
| Absolute contraindications to surgery | Relative contraindications to surgery |
|---|---|
| High PCI score | High BMI |
| Incurable second malignancy | Acute ileus |
| Unresectable metastases | Acute infection |
| Extensive retroperitoneal involvement | Cardiac insufficiency |
| Poor general condition | Hepatic insufficiency |
| Hepatic hilum involvement | Renal insufficiency |
| Mesenteric root involvement | |
| Bladder trigone involvement | |
| Massive small intestine involvement (less than 1.5 m of unaffected bowel) | |
| Lesions penetrating the diaphragm |
PCI – Peritoneal Carcinomatosis Index, BMI – body mass index
The approach may differ depending on the origin of carcinomatosis: primary peritoneal neoplasms are still considered resectable even when they involve both the stomach and colon, as opposed to ovarian and colorectal carcinomatosis [28,31]. Relative contraindications are high BMI, acute ileus, infection, cardiac, hepatic, or renal insufficiency [28].
Despite meticulous radiological workup, at least 20-30% of patients turn out to be inoperable on surgical exploration [10]. The main causes of unresectability are diffuse involvement of the digestive tract, invasion of the root of the mesentery, and miliary peritoneal dissemination [31].
Peritoneal Cancer Index score and its application
Although the PCI was invented as a surgical scoring system, it is applied to preoperatively to determine tumour burden on diagnostic imaging. The initial calculation is revised during surgery. A line connecting the lowest aspects of the costal arches, a line connecting the anterior superior iliac spines, and 2 parallel vertical lines divide the abdomen into 2 segments. The upper jejunum, lower jejunum, upper ileum, and lower ileum are 4 separate segments, while the large bowel is included into corresponding abdominopelvic regions. Each of these 13 sites is carefully examined, and the lesion size in each region is scored on a scale ranging from 0 to 3 points (0 – no visible tumour, 1 – metastases < 5 mm, 2 – metastases 5-50 mm, 3 – implants > 5 cm or confluent) [12,32]. Several studies show different cut-off points on PCI score regarding the feasibility of the surgery [24,27,31] (Figure 6).
Figure 6.
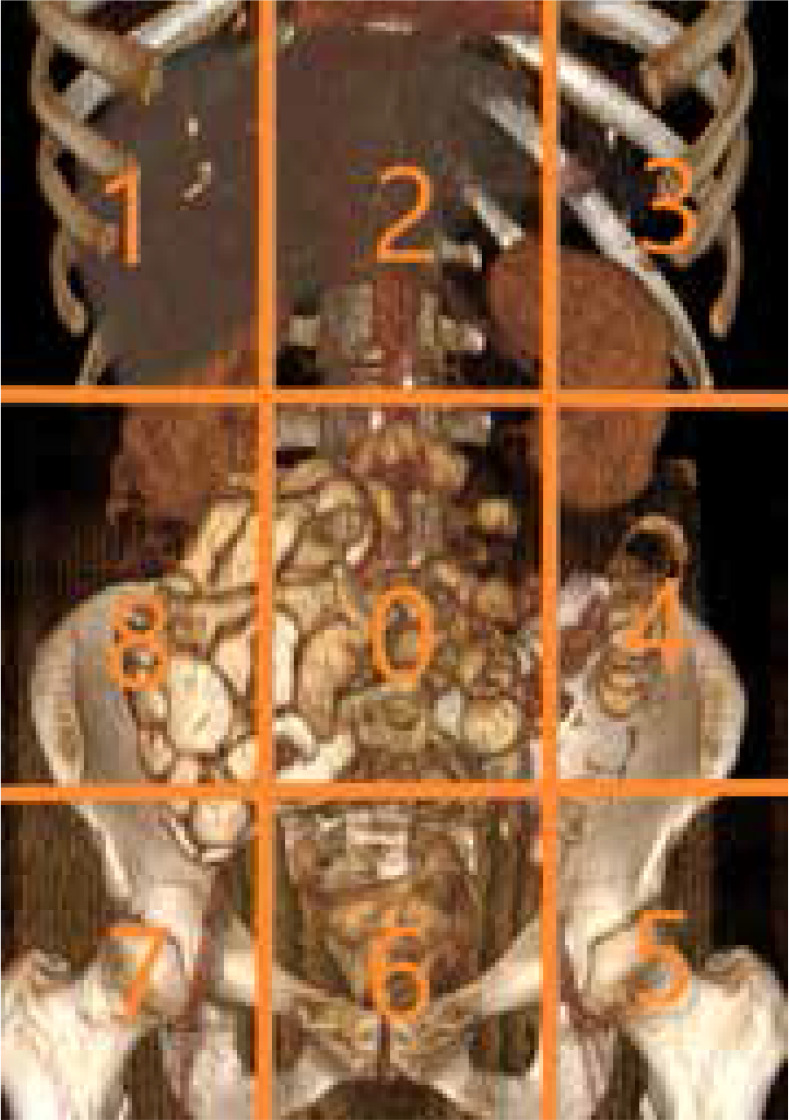
Peritoneal Carcinomatosis Index (PCI) scale. Nine abdominopelvic regions
Conclusions
Preoperative diagnostic imaging plays an important role in determining a patient’s eligibility to cytoreductive surgery and intraperitoneal chemotherapy. A precise radiology report, which covers all crucial findings potentially precluding CRS, prevents unnecessary surgical interventions and associated morbidity and mortality. Alternative treatment like neoadjuvant or palliative chemotherapy may be offered to patients who are not amenable to CRS and HIPEC.
Conflict of interest
The authors declare no conflict of interest.
References
- 1.Tirkes T, Sandrasegaran K, Patel AA, et al. Peritoneal and retroperitoneal anatomy and its relevance for cross-sectional imaging. Radiographics 2012; 32: 437-451. [DOI] [PubMed] [Google Scholar]
- 2.Patel CM, Sahdev A, Reznek RH. Cancer Imaging. CT, MRI and PET imaging in peritoneal malignancy. Cancer Imaging 2011; 11: 123-139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.van Baal JO, Van de Vijver KK, Nieuwland R, et al. The histophysiology and pathophysiology of the peritoneum. Tissue Cell 2017; 49: 95-105. [DOI] [PubMed] [Google Scholar]
- 4.Diop AD, Fontarensky M, Montoriol PF, et al. CT imaging of peritoneal carcinomatosis and its mimics. Diagn Interv Imaging 2014; 95: 861-872. [DOI] [PubMed] [Google Scholar]
- 5.Wasnik AP, Maturen KE, Kaza RK, et al. Primary and secondary disease of the peritoneum and mesentery: review of anatomy and imaging features. Abdom Imaging 2015; 40: 626-642. [DOI] [PubMed] [Google Scholar]
- 6.Ognong-Boulemo A, Dohan A, Hoeffel C, et al. Adnexal masses associated with peritoneal involvement: diagnosis with CT and MRI. Abdom Radiol (NY) 2017; 42: 1975-1992. [DOI] [PubMed] [Google Scholar]
- 7.Elmohr MM, Elsayes KM, Pickhardt PJ. Non-neoplastic conditions mimicking peritoneal carcinomatosis at CT imaging. Br J Radiol 2020; 93: 20200401. doi: 10.1259/bjr.20200401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Nougaret S, Addley HC, Colombo PE, et al. Ovarian carcinomatosis: how the radiologist can help plan the surgical approach. Radiographics 2012; 32: 1775-1800; discussion 1800-1803. [DOI] [PubMed] [Google Scholar]
- 9.Iafrate F, Ciolina M, Sammartino P, et al. Peritoneal carcinomatosis: imaging with 64-MDCT and 3T MRI with diffusion-weighted imaging. Abdom Imaging 2012; 37: 616-627. [DOI] [PubMed] [Google Scholar]
- 10.Dohan A, Hobeika C, Najah H, et al. Preoperative assessment of peritoneal carcinomatosis of colorectal origin. J Visc Surg 2018; 155: 293-303. [DOI] [PubMed] [Google Scholar]
- 11.Kyriazi S, Kaye SB, deSouza NM. Imaging ovarian cancer and peritoneal metastases–current and emerging techniques. Nat Rev Clin Oncol 2010; 7: 381-393. [DOI] [PubMed] [Google Scholar]
- 12.Aherne EA, Fenlon HM, Shields CJ, et al. What the radiologist should know about treatment of peritoneal malignancy. AJR Am J Roentgenol 2017; 208: 531-543. [DOI] [PubMed] [Google Scholar]
- 13.Laghi A, Bellini D, Rengo M, et al. Diagnostic performance of computed tomography and magnetic resonance imaging for detecting peritoneal metastases: systematic review and meta-analysis. Radiol Med 2017; 122: 1-15. [DOI] [PubMed] [Google Scholar]
- 14.Levy MJ, Abu Dayyeh BK, Fujii LL, et al. Detection of peritoneal carcinomatosis by EUS fine-needle aspiration: impact on staging and resectability (with videos). Gastrointest Endosc 2015; 81: 1215-1224. [DOI] [PubMed] [Google Scholar]
- 15.Dadayal G, Weston M, Young A, et al. Transvaginal ultrasound (TVUS)-guided biopsy is safe and effective in diagnosing peritoneal carcinomatosis and recurrent pelvic malignancy. Clin Radiol 2016; 71: 1184-1192. [DOI] [PubMed] [Google Scholar]
- 16.Qi Z, Zhang Y, Dai Q, et al. Peritoneal carcinomatosis in primary ovarian cancer: ultrasound detection and comparison with computed tomography. Ultrasound Med Biol 2017; 43: 1811-1819. [DOI] [PubMed] [Google Scholar]
- 17.Fischerova D, Zikan M, Semeradova I, et al. Ultrasound in preope-rative assessment of pelvic and abdominal spread in patients with ovarian cancer: a prospective study. Ultrasound Obstet Gynecol 2017; 49: 263-274. [DOI] [PubMed] [Google Scholar]
- 18.van ‘t Sant I, van Eden WJ, Engbersen MP, et al. Diffusion-weighted MRI assessment of the peritoneal cancer index before cytoreductive surgery. Br J Surg 2019; 106: 491-498. [DOI] [PubMed] [Google Scholar]
- 19.Garcia Prado J, González Hernando C, Varillas Delgado D, et al. Diffusion-weighted magnetic resonance imaging in peritoneal carcinomatosis from suspected ovarian cancer: diagnostic performance in correlation with surgical findings. Eur J Radiol 2019; 121: 108696. doi: 10.1016/j.ejrad.2019.108696. [DOI] [PubMed] [Google Scholar]
- 20.Lopez-Lopez V, Cascales-Campos PA, Gil J, et al. Use of (18)F-FDG PET/CT in the preoperative evaluation of patients diagnosed with peritoneal carcinomatosis of ovarian origin, candidates to cytoreduction and hipec. A pending issue. Eur J Radiol 2016; 85: 1824-1828. [DOI] [PubMed] [Google Scholar]
- 21.An H, Lee EYP, Chiu K, et al. The emerging roles of functional imaging in ovarian cancer with peritoneal carcinomatosis. Clin Radiol 2018; 73: 597-609. [DOI] [PubMed] [Google Scholar]
- 22.Schmidt S, Meuli RA, Achtari C, et al. Peritoneal carcinomatosis in primary ovarian cancer staging: comparison between MDCT, MRI, and 18F-FDG PET/CT. Clin Nucl Med 2015; 40: 371-377. [DOI] [PubMed] [Google Scholar]
- 23.Low RN, Barone RM, Lucero J. Comparison of MRI and CT for predicting the Peritoneal Cancer Index (PCI) preoperatively in patients being considered for cytoreductive surgical procedures. Ann Surg Oncol 2015; 22: 1708-1715. [DOI] [PubMed] [Google Scholar]
- 24.Dohan A, Hoeffel C, Soyer P, et al. Evaluation of the peritoneal carcinomatosis index with CT and MRI. Br J Surg 2017; 104: 1244-1249. [DOI] [PubMed] [Google Scholar]
- 25.Abdalla Ahmed S, Abou-Taleb H, Ali N, et al. Accuracy of radiologic-laparoscopic peritoneal carcinomatosis categorization in the prediction of surgical outcome. Br J Radiol 2019; 92: 20190163. doi: 10.1259/bjr.20190163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Low RN, Barone RM. Imaging for peritoneal metastases. Surg Oncol Clin N Am 2018; 27: 425-442. [DOI] [PubMed] [Google Scholar]
- 27.Castro-Mesta JF, González-Guerrero JF, Barrios-Sánchez P, et al. Bases and foundations of the treatment of peritoneal carcinomatosis: review article. Medicina Universitaria 2016; 71: 98-104. [Google Scholar]
- 28.Brücher BL, Piso P, Verwaal V, et al. Peritoneal carcinomatosis: cyto-reductive surgery and HIPEC–overview and basics. Cancer Invest 2012; 30: 209-224. [DOI] [PubMed] [Google Scholar]
- 29.Behrenbruch C, Hollande F, Thomson B, et al. Treatment of peritoneal carcinomatosis with hyperthermic intraperitoneal chemotherapy in colorectal cancer. ANZ J Surg 2017; 87: 665-670. [DOI] [PubMed] [Google Scholar]
- 30.Seshadri RA, Glehen O. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in gastric cancer. World J Gastroenterol 2016; 22: 1114-1130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Mohkam K, Passot G, Cotte E, et al. Resectability of peritoneal carcinomatosis: learnings from a prospective cohort of 533 consecutive patients selected for cytoreductive surgery. Ann Surg Oncol 2016; 23: 1261-1270. [DOI] [PubMed] [Google Scholar]
- 32.Jacquet P, Sugarbaker PH. Clinical research methodologies in diagnosis and staging of patients with peritoneal carcinomatosis. Cancer Treat Res 1996; 82: 359-374. [DOI] [PubMed] [Google Scholar]