

Abstract
Objective:
This review summarizes the current and previous data on dietary supplement (DS) use collected from participants in the National Health and Nutrition Examination Survey (NHANES), describes the NHANES dietary supplement database used to compute nutrient intakes from DSs, discussed recent developments and future direction, and describes many examples to demonstrate the utility of these data in informing nutrition research and policy.
Background and History:
Since 1971, NHANES, has been collecting information on the use of DSs from participants. These data are critical to national nutrition surveillance and have been used to characterize usage patterns, examine trends over time, assess the percentage of the population meeting or exceeding nutrient recommendations, and to help elucidate the sources contributing nutrients to the diet of the US population.
Rationale:
Over half of adults and about one-third of children in the United States use at least one dietary supplement in the past 30 days. Dietary supplements contribute to the dietary intake of nutrients and bioactive compounds in the US and therefore need to be assessed when monitoring nutritional status of the population and when studying diet-health associations.
Recent Developments:
With the recent development and availability of the Dietary Supplement Label Database (DSLD), a comprehensive DS database that will eventually contain labels for all products marketed in the US, NHANES DS data will be more easily linked to product information to estimate nutrient intake from DS.
Future Directions:
Over time, NHANES has both expanded and improved collection methods. The continued understanding of sources of error in collection methods will continue to be explored and is critical to improved accuracy.
Conclusions:
NHANES provides a rich source of nationally representative data on the usage of dietary supplements in the US.
Keywords: NHANES, monitoring, dietary supplements, supplement labels, epidemiology, nutritional surveillance, nutrition databases
Introduction, background, and history
Nutrition monitoring is important to providing data critical to policymaking, for tracking progress of initiatives, and is used for research purposes. The National Nutrition Monitoring and Related Research Act of 1990 (P.L. 101–445) provided a framework that strengthened national data collection on the US population’s dietary and health related status (1). To accurately assess the dietary intake of a population or large-population groups, nutrients from dietary supplements must be included, not only because of the pervasive use of these products, but also because they can contribute substantially towards intake of nutrients and other bioactive compounds. The National Health and Nutrition Examination Survey (NHANES) is a nationally representative survey designed to assess the health and nutritional status of the US population. NHANES collects data on participants via questionnaires and examinations; including participants usage of DSs. While the process is arduous, it is critical, since NHANES data are used to inform policy and evaluate whether the population is meeting or at risk for exceeding authoritative nutrient recommendations. Additionally, NHANES dietary supplement (DS)7 data are used to characterize usage patterns, examine trends over time, address potential safety issues, and provide insights into the association between nutrients and other bioactives and health outcomes.
NHANES has been consistently collecting data on usage of DSs in the US population since 1971, and data have indicated an increasing trend in usage over time. In NHANES I (1971–74), 32.9% of adults aged 25–74 years and in NHANES II (1976–1980), 34.9% of adults 18–74 years reported the use of at least 1 DS (regularly or irregularly) (2, 3). Data from NHANES III (1988–1994) indicated that 40% of adults aged 20+ years reported using at least 1 DS in the past 30 days, increasing further to 52% in NHANES 1999–2000 (4, 5). The percentage of adult users remained stable over the next decade; in NHANES 2011–2012, 52% of adults took at least 1 DS in the past 30 days (6), with about 45% of adult supplement users taking more than one product (7). Interestingly, the usage pattern differs among infants, toddlers, and children. Briefel et al. found that DS use in general declined significantly among infants and children aged 1–5 years from NHANES I (1971–1974) to NHANES 1999–2000, but remained relatively constant for children and adolescents aged 6–19 years (8).
Many DSs, such as multivitamin-mineral products, contribute 100% or more of recommended daily intake for one or more nutrients. The high doses combined with the high prevalence of use makes collecting and accurately capturing nutrient related information provided by supplements relevant to national nutrition monitoring efforts. Failure to accurately obtain such data could lead to underestimating total nutrient intake for the total population and sub-groups (9, 10). It is also critical to maintain accurate and current DS databases. Collecting information on what supplements are used, and their frequency of use, is only half of the challenge: current and accurate supplement databases that include ingredients and their amounts are the foundation upon which valid intake estimates are based (11). Therefore, this review summarizes DS collection in NHANES since its inception, provides a detailed description of the method currently used to collect DS information in NHANES since 1999 or continuous NHANES, and describes the NHANES DS database that is used to estimate nutrient intakes from DSs. Finally, several examples of studies that have used NHANES data are provided to demonstrate the utility of this invaluable data in nutrition research and informing policy.
The NHANES program
NHANES is conducted by the National Center for Health Statistics (NCHS) of the Centers for Disease Control and Prevention, U.S. Department of Health and Human Services. NHANES is designed to assess the health and nutritional status of the resident, civilian, US noninstitutionalized population through a cross-sectional multi-stage sampling design. Since 1999, NHANES has been continuously collecting data on a sample of approximately 5,000 people per year from 15 counties throughout the United States. Prior to 1999, NHANES was a periodic survey, collecting information over a specified number of years with break years in which no data were collected. NHANES collects data from participants through questionnaires, standardized examinations, and collection of biospecimens. These data are collected via an interview in participants’ homes, at a mobile examination center (MEC), and post-MEC follow-ups. NHANES assesses the nutritional status of participants via 24-hour recalls, targeted food frequency questionnaires (e.g. fish consumption, alcohol use), a questionnaire to assess DS usage, diet and behavior questionnaires, anthropometric measurements, and measurement of nutritional status-related biomarkers (12).
Past and present NHANES dietary supplement data collection methodologies
Although many national surveys have included questions on DSs over time, NHANES is currently the only national survey in the United States that regularly collects detailed information on dietary supplement use and maintains a DS label database to estimate nutrient values for products reported. In addition, linking this information to dietary intake allows the computation of total nutrient intake from diet and DSs in NHANES. The USDA Continuing Survey of Food Intakes by Individuals (CSFII) and the Nationwide Food Consumption Survey (NFCS) have in the past collected information on dietary supplements. The National Health Interview Survey (NHIS) is a household-based survey that collects data on a variety of health topics via household interviews. NHIS has collected and continues to collect valuable information on dietary supplement use, albeit not annually, on a large sample of the US population. Unlike NHANES, NHIS does not collect detailed data on DSs from the product label, or detailed data on dietary intake of foods and beverages, nor does it include a physical examination or biospecimen collection. Details regarding collection of DS use from various national surveys have been described previously (8, 13).
Radimer et al. and Dwyer et al. have described the NHANES DS collection from surveys prior to the early 2000s (13–15) and others have described dietary data collection in general in NHANES (8, 12, 16). This review therefore provides a brief description of past NHANES surveys and focuses on current methods for dietary supplement data collection.
Both NHANES I and NHANES II collected data on dietary supplement use, but they did not collect brand names, and there was no dietary supplement database available at that time with the nutrient content of the products. During NHANES I, participants were asked a question on the use of vitamins and minerals. The response categories were no, taken regularly, or taken irregularly (Table 1). A follow-up question was asked to determine the types of products taken and to classify them into eight categories plus a “miscellaneous” and “prescription unknown” category. These questions were asked at the mobile examination center during the dietary interview, which consisted of a 24-hour recall and food frequency questionnaire. Dietary supplements were collected using similar methodology during NHANES II. The main difference was that the number of categories expanded to 28, with additional categories for “miscellaneous” and “prescription unknown.” Both the NHANES I and NHANES II surveys provided general information on DS use, specifically for vitamins and minerals. Amounts of nutrients in these products were not queried and therefore, nutrient intake from DSs cannot be estimated in NHANES I and II.
Table 1.
Dietary supplement collection in NHANES since 19711
| NHANES I (1971–1974) |
NHANES II (1976–1980) |
NHANES III (1988–1994) |
Continuous NHANES (1999–2006) |
Continuous NHANES (2007–2018) |
|
|---|---|---|---|---|---|
| Age Group | 1–74 y | 6 mo-74 y | 2+ mo | All ages | All ages |
| Mode | Dietary interview in the MEC | Dietary interview in the MEC | Household Interview | Household Interview | Household Interview and Dietary interviews (2) in the MEC and via phone |
| Question | Are you taking vitamins or minerals? (no, taken regularly and taken irregularly). | Are you taking vitamins or minerals? (no, taken regularly and taken irregularly). | Have you taken any vitamins or minerals in the past month? Please include those that are prescribed by a doctor or dentist and those that are not prescribed. Do not include topical vitamins. | Have you used or taken any vitamins, minerals, herbals2 or other dietary supplements in the past 30 Days?3 Include prescription and non-prescription supplements. | Household Interview Have you used or taken any vitamins, minerals, herbals or other dietary supplements in the past 30 days? Include prescription and non-prescription supplements. Dietary Interviews All day yesterday, (day), between midnight and midnight did (you/SP) take any vitamins, minerals, herbals or other dietary supplements?4 |
| Hand card shown with examples? | No | No | No | Yes | Yes |
| Product containers shown to interviewer? | No | No | Yes | Yes | Yes |
| Information recorded from product container | N/A | N/A | Product name and manufacturer information | Product name, form, and manufacturer information | Product name, form, and manufacturer information |
| Referent period | No time frame | No time frame | Past month | Past 30 days3 | Past 30 days Past 24 hours (two 24-hour recalls) |
| Additional data collected | Frequency of use in the past month, amount usually taken when used and how long product taken | Frequency of use in the past 30 days, amount usually taken when used and how long product taken | Frequency of use in the past 30 days, amount usually taken when used, how long product taken, and the reason (s) for taking each product reported. | ||
| Non-prescription antacids containing calcium and/or magnesium collected? | No | No | Yes5 | Yes | Yes |
| Database used to provide nutrient values for the dietary supplement data collected | Not available | Not available | Data base created based on label information in 1996. Database contracted out (not developed or maintained in-house) | NHANES dietary supplement database developed and maintained at NCHS | NHANES dietary supplement database developed and maintained at NCHS |
| Data provided for researchers | 8 categories, plus 1 miscellaneous category and 1 prescription unknown category. | 28 categories, plus 1 miscellaneous category and 1 prescription unknown category. | All products reported and ingredients | All products reported and questions regarding supplement usage patterns NHANES dietary supplement database |
All products reported and questions regarding supplement usage patterns NHANES dietary supplement database |
| Categories | Unknown, prescriptions, | Unknown, prescriptions, | N/A | N/A | N/A |
| Miscellaneous, | Miscellaneous, | ||||
| 1. Multiple vitamins, | 1. Multiple vitamins, | ||||
| 2. Multiple vitamins and minerals, | 2. Multiple vitamins with additional supplements, | ||||
| 3. Iron only, | 3. Multiple vitamins and minerals, | ||||
| 4. Multiple vitamins with iron, | 4. Multiple vitamins and minerals with additional supplements, | ||||
| 5. Vitamins E, A and D, | 5. Iron, | ||||
| 6. Vitamin C, | 6. Multiple vitamins with iron, | ||||
| 7. Calcium, | 7. Iron with additional supplements, | ||||
| 8. Vitamin B | 8. Geritol, | ||||
| 9. Vitamin E, | |||||
| 10. Vitamin E with additional supplements, | |||||
| 11. Vitamin A, | |||||
| 12. Vitamin A with additional supplements, | |||||
| 13. Vitamin D, | |||||
| 14. Vitamin D with additional supplements, | |||||
| 15. Vitamin C, | |||||
| 16. Vitamin C with additional supplements, | |||||
| 17. Calcium, | |||||
| 18. Calcium with additional supplements, | |||||
| 19. Magnesium, | |||||
| 20. Magnesium with additional supplements, | |||||
| 21. Zinc, | |||||
| 22. Zinc with additional supplements, | |||||
| 23. B vitamins/B-complex, | |||||
| 24. B vitamins/B-complex with additional Supplements, | |||||
| 25. Potassium, | |||||
| 26. Potassium with additional supplements, | |||||
| 27. Fluoride, | |||||
| 28. Fluoride with additional supplements |
Some of the contents of the data from this tables have also been provided in the paper by Ahluwalia et al.(12) and Radimer (13)
The word “herbals” was specifically included in the question mid-cycle NHANES 2005–2006. It is important to note that examples of herbal products were included on the hand card since 1999.
For NHANES 1999–2000 the referent period was the “past month”.
The question slightly differs for participants that reported supplements during their household interview. Since this interview utilized dependent interviewing, information from the household or first 24-hour recall if it is the 2nd recall, is used for the dietary interviews. The question reads: “The next questions are about your use of dietary supplements, vitamins, minerals and herbals all day yesterday, (day), between midnight and midnight. This includes prescription and over the counter dietary supplements. During the interview in your home (and our exam center) you reported taking (supplement name). Did you take this supplement yesterday (day). (between midnight and midnight)?”
Only asked for adults (18+ y).
Abbreviations: MEC, mobile examination center; NCHS, National Center for Health Statistics; SP, survey participants
NHANES III (1988–1994) was the first NHANES survey where nutrient information from DSs and amounts consumed were collected. Participants were asked during the home interview if they had taken a dietary supplement in the past month (Table 1). While the question specifically asked only about vitamins and minerals, participants did volunteer other types of information about use of other dietary supplements (i.e., herbals). Participants were also asked how long they had taken each product, how frequently, and how much they usually took. Importantly, participants were also asked to show interviewers the product containers for all dietary supplements taken in the past month. The name and manufacturer of the product was recorded by interviewers. The data on product names and manufacturers were collected to later obtain product labels for information on ingredients and amounts. Unfortunately, due to a lack of resources to edit and process the incoming data, a product label database was not initially constructed. Years after the survey was completed, an external contractor obtained the labels and provided nutrient values for products reported by NHANES participants. However, the label information obtained was from products on the market in 1996, and therefore may not reflect formulations of products on the market during the data collection period (1988–1994). Nonetheless, these data allowed estimation of total nutrient intakes from foods, beverages, and DSs on a nationally representative sample of the US population.
Beginning in 1999, DS usage information was collected from participants during the home interview as in NHANES III. Participants were asked about their use of vitamins and minerals, as well as herbals and other types of DSs in the past 30 days, from here on referred to as the 30-day frequency questionnaire. The interviewer referred participants to a hand card that provided examples (Table 1). Participants were asked to show the dietary supplement bottles/containers to the interviewer, who recorded the name, form, strengths for selected single-nutrient products, and manufacturer electronically into the tablet personal computers. If the container was not seen, the interviewer asked the participants to recall the name of the product taken. Although the percentage of containers actually seen by interviewers differed somewhat between survey cycles, generally containers were seen for over 80% of products reported. The interviewer asked follow-up questions for each product reported, such as how long, how often, and how much of the product was usually taken. Beginning in 2007, NHANES began asking about the motivation(s) for using each product reported, and these procedures have continued since.
In 2007, in addition to the 30-day frequency questionnaire administered in the home, NHANES began asking participants about DS use in each of the two 24-hour dietary recalls, directly following the collection of information on foods and beverages, to allow the calculation of total nutrient intake using the same referent period (14). The first 24-hour dietary recall is collected at the MEC and the second 24-hour dietary recall is collected via phone about 3–10 days later. This provides researchers with the ability to estimate total nutrient intakes and distributions of usual intakes from foods, beverages, and dietary supplements reported by participants using similar methodology. Additionally, collecting supplement use in the past 24 hours as part of the dietary recall in the MEC can help to explain variability in laboratory biomarkers collected during the examination, particularly ones that reflect fairly short-term intake or conditions. For example, if a participant reported very low intake of folate from foods, but serum folate was high, this could be due to folate supplement intake and having information about DS use during this same time period is critical to help explain findings. NHANES employs a “dependent” style of interviewing for both 24-hour dietary recalls, in that the DS product names collected during the home interview are used in the recall interviews. This decreases participant burden and can help reduce measurement error. Participants are asked during the 24-hour dietary recall if they had taken each of the products reported during the home interview in the 24-hour period prior to the interview (midnight to midnight), and how much they took. Any other products taken in that 24-hour period and not reported in the home are also queried. Participants are then asked how much was taken and for how long that product or a similar product had been used. Nonprescription antacids are also collected using a similar methodology to capture intake of calcium and/or magnesium.
The NHANES Dietary Supplement Database
As with dietary assessment in general, a challenge to research on DSs and their links to health outcomes is the difficulty in accurately assessing total intake. Collecting detailed information about each DS used by a participant is very important; however, without a well-maintained composition database, it would not be possible to estimate nutrient intake from these products. The most significant DS-related update from NHANES III to the continuous NHANES is the development and maintenance of the NHANES DS database (NHANES-DSD).
The NHANES-DSD contains label information from prescribed and over-the-counter (OTC) DS products that have been reported by NHANES participants since the NHANES 1999–2000 through the NHANES 2013–2014 survey cycles. This database gets appended with each new NHANES cycle. This includes many types of products such as vitamins, minerals, botanicals, amino acids, fish oils, and fiber supplements. The database currently contains about 12,600 records, which includes new products and reformulations of products. Additionally, NHANES maintains default and generic formulations of products in the NHANES-DSD to assign to participants when not enough information was collected during interviews to identify the product taken or when only strengths of nutrients are known, and not brands. The database also contains label information on nonprescription antacids containing calcium and/or magnesium. One advantage of the NHANES-DSD is that data are maintained for products that may no longer be on the market or have been reformulated, so that outside researchers using the NHANES-DSD to provide nutrient values from DS for their own studies can use appropriate data for relevant years.
Figure 1 describes the process used to collect, maintain, and link product-level data to participants in order to estimate nutrients consumed from dietary supplements (17). The NHANES-DSD requires a significant investment of time and labor to evaluate incoming data, obtain labels from manufacturers, update the information, track constantly changing formulations, and maintain the overall database. Since all NHANES dietary supplement data are released on the NHANES website for use by researchers and policymakers, the data need to be standardized for easier use by researchers. This is because the nutrient data provided on product labels are sometimes listed as compounds that need to be converted into elemental amounts, are in different units (e.g., International Units (IUs) and mcg), or may be in different units compared to the What We Eat in America (WWEIA) - NHANES dietary data (e.g., vitamin D in supplements is reported in IUs and in mcgs for the dietary data).
Figure 1.
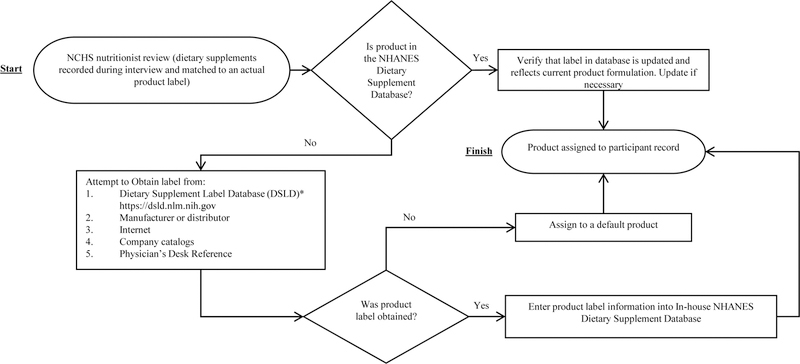
NHANES dietary supplement data processing flow chart
*If label is not in DSLD, NHANES obtains the product label and provides a copy to DSLD for inclusion.
NHANES DS data are released in 2-year cycles and include both the data collected from participants regarding supplement usage and the data from the NHANES-DSD. New, reformulated, generic and default products are appended to the NHANES-DSD for each 2-year NHANES and can be merged with the participant data using a unique DS ID. To use these data, users are encouraged to read the NHANES dietary supplement documentation and analytical guidelines and to review the online dietary tutorial on the NHANES website. More details on NHANES data release can be found elsewhere (12).
Recent Developments
In 1999 at the time NHANES-DSD was constructed, there were no freely available, comprehensive DS composition databases available. However, this is no longer the case. The Dietary Supplement Label Database, (DSLD), a joint project of the NIH Office of Dietary Supplements (ODS) and National Library of Medicine (NLM), is a DS database made available to the public in June 2013, that is continuously updated and to date contains 75,000 labels and label information for products marketed in the United States. NHANES has begun to use DSLD as a resource for product labels. However, since participants sometimes report DSs that are not yet included in the DSLD, some work to obtain these product labels is still necessary. Additionally, correct formulations need to be verified by manufacturers to ensure that the product reported at the time of the survey matches the correct product formulation on the market at that time. The NHANES staff collaborate with ODS to ensure that products reported in NHANES are represented in the DSLD by regularly sending product labels so that they can be included in DSLD. In the future, when DSLD is fully populated, we anticipate that NHANES will be able to use this database to provide nutrient values for DSs taken by NHANES participants.
While the NHANES-DSD and DSLD databases have significantly improved access to information on DS composition since 2012, the nutrient data are derived from labels. Label values can differ from analytically derived values, especially for certain nutrients (18). Beginning in 2005, ODS in conjunction with the Nutrient Data Laboratory of the US Department of Agriculture began a project to analytically test the composition of DSs. These data are available online and can be linked to specific cycles of NHANES to improve estimates of nutrient intake (link, see Andrews et al. this issue of the journal supplement).
Uses of NHANES Dietary Supplement Data
Table 2 describes some of the important uses of the NHANES DS data. The NHANES DS data have been invaluable in characterizing the usage patterns both for the total US population and for subgroups. They have also been used to assess nutrient intake from dietary supplements alone and as part of total nutrient intake. This research is used to inform policy regarding nutrient recommendations.
Table 2.
Key uses of NHANES data on dietary supplements
| Examples of how NHANES dietary supplements data can be used to answer important research questions | |
|---|---|
| Usage patterns by the population and large-population groups | Usage of dietary supplements from a 30-day questionnaire and two 24-hour dietary recalls |
| Usual nutrient intakes from dietary supplements | |
| Total nutrient intake from foods, beverages and dietary supplements on a given day | |
| Usual total nutrient intake from foods, beverages and dietary supplements | |
| Examine motivations for DS use and trends in usage patterns over time | Estimate the top motivations for using dietary supplements and types of dietary supplements |
| Determine if there are differences in why people are using dietary supplements by sociodemographic factors | |
| Examine association of health/wellbeing with DS use, and nutrient intake from DS alone / total nutrient intake from diet and DS | Assess associations between dietary supplement use and biomarkers of exposure to selected nutrients |
| Assess the association between dietary supplement use and health outcomes | |
| Determine the association between baseline dietary supplement use and mortality or morbidity using passive follow-up (i.e., data from the National Death Index, Medicare Claims and Enrollment) | |
| Inform policy | DRI development/updates |
| Evaluating nutrient adequacy of US diet (DGAC) | |
| Intakes in relation to setting or tracking fortification policies | |
Abbreviations: DGAC, Dietary Guidelines Advisory Committee; DS, dietary supplements
Usage patterns by the population and large-population groups
Block et al. were the first to use data from NHANES I to describe vitamin and mineral usage on a nationally representative sample of 11,227 adults aged 25–74 years (2). Understanding and characterizing use previously had been challenging; information was available mostly on specific age groups or specific geographical areas and surveys lacked the statistical power to assess use in nonwhite subgroups (2). NHANES I overcame these limitations and provided more accurate estimates on DS use in the US adult population. At the time, it was possible to assess usage by many demographic variables, including white and black race subgroups. Block et al. found that 22.8% of the US adult population had reported regularly taking a dietary supplement, with usage higher in whites than blacks (24.1% vs. 11.7%) (2). The authors also found that during NHANES I (1971−1974), the most popular DSs used were multivitamins, vitamin C, and vitamin E.
NHANES III provided data that allowed more specific characterization of supplement use on a national level and provided an opportunity for assessment of total nutrient intake and therefore, more accurate evaluation of nutrient exposures in the US population. Ervin et al. provided a detailed look at DS use in the United States during 1988−1994 (19). This report indicated that about 40% of the population 2 months of age and older reported taking at least one DS in the past month. Non-Hispanic whites were more likely to use supplements compared to non-Hispanic blacks and Mexican Americans (43% vs. 30% and 29%). The authors also found that almost 91% of children aged 2 months to 11 years who reported taking a DS, reported taking one product, while about 66% of adults 40 years and older were taking 1 product, and 44% taking more than one product. This report provided strong evidence that a significant proportion of the US population of all ages were taking DSs, and that in certain age groups many were taking multiple products. In another report, Ervin et al. estimated total nutrient intake from diet and DSs and found that while most older adults as a group were not meeting recommendations for calcium, supplement users had higher calcium intake, particularly non-Hispanic white women, than non-users (20). This finding was similar to another report in which a higher percentage of older women (but not men) who were supplement users met recommendations for B-vitamins compared to non-users (21).
Examine trends in usage patterns over time and motivations for DS use
Data from continuous NHANES has provided an opportunity to examine trends in DS over time. This is an essential element in nutrition monitoring, since food sources and lifestyles change over time, and these changes may alter intakes and the nutritional status of the population. For example, it is important to monitor vitamin D status over time, since there were changes in food consumption (especially of vitamin D-fortified foods, with new foods being fortified with the vitamin), increasing use of vitamin D-containing supplements, and changes in recommendations for sun exposure. Since NHANES III, there have been data necessary to assess both vitamin D exposure and vitamin D status in the US population. This includes data on DSs and information on nutrients from labels, estimated vitamin D levels in foods, season of data collection and the geographical location of participants, and measured circulating concentrations of 25-hydroxyvitamin D (22). This approach allows researchers to estimate vitamin D status and exposures of vitamin D in continuous NHANES surveys and to compare to NHANES III to assess changes over time.
Folate nutritional status is another example of how data from NHANES III have been used with continuous NHANES surveys to monitor population intakes and sources of intake of the vitamin pre- and post-fortification of flour in the US food supply. One study found that post-fortification (after 1998), 2.7% of the US population exceeded the Tolerable Upper Intake Level (UL) and that this was specifically confined to groups that were taking folic acid-containing supplements as well as consuming diets with fortified and enriched grain products and ready-to-eat cereals. The UL was also more likely to be exceeded when supplement users were consuming >400µg folic acid from supplements (23). Other NHANES-based studies have estimated total folate intake in women of childbearing age, identifying the fraction of the population at adequate, inadequate, or excessive levels of intake (24, 25). These examples illustrate the importance of NHANES data and its potential to provide snapshots of the population at given times, monitor intakes over time, and provide information on the sources of intake.
Another important research question focuses on the motivations for why people are using DSs. Previously this information was limited, particularly on a nationally representative sample. As a reminder, in 2007 NHANES added questions on the motivations for using each DS reported by participants. In a report by Bailey et al., the authors found that the most common motivations reported by US adults taking DSs were: to improve health (45%), to maintain overall health (33%), for bone health (25%), to supplement the diet (22%) and to prevent health problems (20%) (26). The authors also found that 23% of the products were used based on recommendations of a health care provider (26). This report provided novel findings that helped to elucidate why US adults were taking these products and also the demographic, behavioral, and health characteristics of users.
Examine association of health/wellbeing with DS use, and nutrient intake from DS alone / total nutrient intake from diet and DS
In 2007, NHANES began collecting data on dietary supplement use as part of the two 24-hour recalls. This was in addition to the supplement data collected during the 30-day questionnaire administered in participants’ homes. This recall data makes it possible to estimate total nutrient intake and usual intakes using similar methodologies for foods and DSs, and can thus assess how different dietary assessment methods can affect population estimates of prevalence and intake. For example, Nicastro et al. found that both collection from the 30-day questionnaire and two 24-hour recalls were useful, but the combination of both methods captured a larger percentage of DS users, and that calibration can be used to obtain the most accurate information from each instrument (27). The ability to estimate total nutrient intake is very important in order to assess associations between nutrients and health outcomes. NHANES allows for assessment of intake from DS, foods and beverages and prescription medications. This is especially important for nutrients such as vitamin D and omega-3 fatty acids, in which supplements contribute a significant amount to intake (6, 28). NHANES data also have been used to estimate exposures of many bioactive constituents, such as caffeine from foods and supplements, and their associations with health (29, 30).
NHANES also allows for the assessment of the independent effects of vitamin and mineral supplements on disease risk. The linkage program at NCHS works to provide key information such as administrative data from the National Death Index and Medicare Claims and Enrollment data, linked with NHANES participants, allowing an opportunity to study health outcomes. Bailey et al. used data on supplements from NHANES III linked with follow-up data from the National Death Index to assess if multivitamin-mineral (MVM) and multivitamin use was associated with cardiovascular disease mortality. Although no association was noted between MVM use and CVD mortality overall, a decreased risk of CVD mortality was observed among women who reported using MVM products for over 3 years compared with nonusers (31). NHANES data can also be linked with the Centers of Medicare and Medicaid Services Medicare Claims and Enrollment data to identify targeted health conditions. Medicare Claims and Enrollment data provide information on the prevalence and incidence of many conditions, including chronic degenerative diseases that affect a large percentage of older adults. It is crucial to study the effects of diet and supplements on chronic disease and other health conditions to add to scientific findings to determine how intake may decrease or increase disease burdens (32).
Future Directions
The comprehensive data collected in NHANES offer an opportunity to explore the interplay of genes, nutrition, and environment with health outcomes. NHANES has a biorepository with stored NHANES participants’ blood, urine and DNA, which includes biospecimens from NHANES III (1988–1994) and subsequent NHANES cycles beginning in 1999–2000. More information on the NHANES biospecimen program, including what specimen types are available and the process for using the data is detailed elsewhere (33). Researchers have begun to use the multifactorial complex data collected in NHANES to examine genes-environmental exposures. For example, in a recent publication, Mazidi et al. found that longer telomeres were associated with vitamins and minerals from foods using NHANES data (34).
NHANES has, over time, improved DS collection and adapted to the growing needs of researchers. Although recording information from the label is more accurate than participants’ recalls of the product names, interviewer errors in entry or omissions cannot be ruled out. Photographing the DS container during the interview in the participant’s home would provide information on the exact formulation taken and would reduce the assumptions that currently need to be made when complete and accurate information is not entered by the interviewer. However, an easy, quick, affordable, and operationally feasible device has not been identified for use in NHANES. Barcode scanning would be another option to capture more accurately the DSs used by participants. However, a database would need to be available containing uniquely assigned barcodes for each product. These avenues are being explored in the context of future surveys in NHANES.
Little is known about the measurement error structure and validity of the NHANES DS collection methods. To understand the magnitude of error and the types of error (e.g., random error, systematic error), it would be necessary for validation studies to be conducted. Examples of potential sources of measurement error include: 1) Errors in participants’ recall when reporting all dietary supplements taken, the amount typically taken and the number of days in the past 30 days that the product was taken, 2) Errors in transcribing information from the product label during collection by interviewers, 3) Matching the product reported to the wrong formulation of the product actually taken by the participant, 4) Errors when entering product label information into the database, and 5) Label ingredient amounts differing from what was actually in what was consumed. Future work may include studies to assess NHANES DS collection methods and other methods used to collect dietary supplement use from participants in surveys and studies.
Conclusions
In conclusion, NHANES has been collecting information on dietary supplements since 1971. Over time, NHANES has both expanded and improved collection methods, providing a rich source of nationally representative data to both researchers and policymakers. These data are vital for national nutrition monitoring and can also be used to characterize usage patterns of dietary supplement use in the US population, estimate nutrient intake from supplements, and characterize total nutrient intake from diet and dietary supplements, as well as examine diverse diet-health relationships.
Acknowledgements and Author Contributions:
JJG and JTD designed research; JJG, RLB, NP, AGE, KAH, NA wrote the paper. All authors have read and approved the final manuscript.
Abbreviations used:
- CSFII
the USDA Continuing Survey of Food Intakes by Individuals
- CVD
cardiovascular disease
- DSLD
Dietary Supplement Label Database
- DS
dietary supplement
- IU
International Units
- MEC
mobile examination center
- MVM
multivitamin-mineral
- NCHS
National Center for Health Statistics
- NFCS
the Nationwide Food Consumption Survey
- NHIS
the National Health Interview Survey
- NHANES-DSD
NHANES dietary supplement database
- NLM
National Library of Medicine
- OTC
over-the-counter
Footnotes
Publisher's Disclaimer: Disclaimer: The findings and conclusions in this paper are those of the author(s) and do not necessarily represent the official position of the National Institutes of Health, the Centers for Disease Control and Prevention, or any other entity of the U.S. Government.
Conflicts of interest and funding disclosure: J. J. Gahche, R.L. Bailey, N. Potischman, A.G. Ershow, K.A. Herrick, N. Ahluwalia have no conflicts of interest. J.T. Dwyer has stock in several drug companies, some of which may sell dietary supplements. There is no funding to disclose.
References
- 1.U.S. Congress Pub. L. 101–445. National Nutrition Monitoring and Related Research Act of 1990 Washington, D.C. : 101st Congress, 1990. [Google Scholar]
- 2.Block G, Cox C, Madans J, Schreiber GB, Licitra L, Melia N. Vitamin supplement use, by demographic characteristics. Am J Epidemiol 1988;127:297–309. [DOI] [PubMed] [Google Scholar]
- 3.Koplan JP, Annest JL, Layde PM, Rubin GL. Nutrient intake and supplementation in the United States (NHANES II). Am J Public Health 1986;76:287–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Gahche J, Bailey R, Burt V, Hughes J, Yetley E, Dwyer J, Picciano MF, McDowell M, Sempos C. Dietary supplement use among U.S. adults has increased since NHANES III (1988–1994). NCHS Data Brief 2011:1–8. [PubMed]
- 5.Radimer K, Bindewald B, Hughes J, Ervin B, Swanson C, Picciano MF. Dietary supplement use by US adults: data from the National Health and Nutrition Examination Survey, 1999–2000. Am J Epidemiol 2004;160:339–49. doi: 10.1093/aje/kwh207. [DOI] [PubMed] [Google Scholar]
- 6.Kantor ED, Rehm CD, Du M, White E, Giovannucci EL. Trends in dietary supplement use among US adults from 1999–2012. JAMA 2016;316:1464–74. doi: 10.1001/jama.2016.14403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bailey RL, Gahche JJ, Lentino CV, Dwyer JT, Engel JS, Thomas PR, Betz JM, Sempos CT, Picciano MF. Dietary supplement use in the United States, 2003–2006. J Nutr 2011;141:261–6. doi: 10.3945/jn.110.133025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Briefel RR, Johnson CL. Secular trends in dietary intake in the United States. Annu Rev Nutr 2004;24:401–31. doi: 10.1146/annurev.nutr.23.011702.073349. [DOI] [PubMed] [Google Scholar]
- 9.Bailey RL, Dodd KW, Gahche JJ, Dwyer JT, McDowell MA, Yetley EA, Sempos CA, Burt VL, Radimer KL, Picciano MF. Total folate and folic acid intake from foods and dietary supplements in the United States: 2003–2006. Am J Clin Nutr 2010;91:231–7. doi: 10.3945/ajcn.2009.28427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bailey RL, Dodd KW, Goldman JA, Gahche JJ, Dwyer JT, Moshfegh AJ, Sempos CT, Picciano MF. Estimation of total usual calcium and vitamin D intakes in the United States. J Nutr 2010;140:817–22. doi: 10.3945/jn.109.118539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Heimbach JT. Using the national nutrition monitoring system to profile dietary supplement use. J Nutr 2001;131:1335S–8S. [DOI] [PubMed] [Google Scholar]
- 12.Ahluwalia N, Dwyer J, Terry A, Moshfegh A, Johnson C. Update on NHANES dietary data: focus on collection, release, analytical considerations, and uses to inform public policy. Adv Nutr 2016;7:121–34. doi: 10.3945/an.115.009258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Radimer KL. National nutrition data: contributions and challenges to monitoring dietary supplement use in women. J Nutr 2003;133:2003S–7S. [DOI] [PubMed] [Google Scholar]
- 14.Dwyer J, Picciano MF, Raiten DJ, Members of the Steering Committee National Health Nutrition Examination Survey. Collection of food and dietary supplement intake data: What We Eat in America-NHANES. J Nutr 2003;133:590S–600S. [DOI] [PubMed] [Google Scholar]
- 15.Radimer KL. Methodological issues in assessing dietary supplement use in children. J Am Diet Assoc 2005;105:703–8. doi: 10.1016/j.jada.2005.03.037. [DOI] [PubMed] [Google Scholar]
- 16.Wright JD, Borrud LG, McDowell MA, Wang CY, Radimer K, Johnson CL. Nutrition assessment in the National Health And Nutrition Examination Survey 1999–2002. J Am Diet Assoc 2007;107:822–9. doi: 10.1016/j.jada.2007.02.017. [DOI] [PubMed] [Google Scholar]
- 17.National Center for Health Statistics. National Health and Nutrition Examination Survey, 1999 – 2014 Data Documentation, Codebook, and Frequencies, Dietary Supplement Database September 2014 ed. Hyattsville, MD: National Center for Health Statistics, 2016. [Google Scholar]
- 18.Gusev P, Andrews K, Palachuvattil J, Dang PT, Roseland J, Bailey R, Savarala S, Wu Y, Pehrsson P, Dwyer J. Analytical vitamin content of over-the-counter prenatal multivitamin/mineral products measured for the Dietary Supplement Ingredient Database (DSID). Conference paper presented at the International Vitamin Conference 2014. Washington, DC, May 12–15, 2014. [Google Scholar]
- 19.Ervin RB, Wright JD, Kennedy-Stephenson J. Use of dietary supplements in the United States, 1988–94. Vital Health Stat 11 1999:i–iii, 1–14. [PubMed]
- 20.Ervin RB, Kennedy-Stephenson J. Mineral intakes of elderly adult supplement and non-supplement users in the third national health and nutrition examination survey. J Nutr 2002;132:3422–7. [DOI] [PubMed] [Google Scholar]
- 21.Ervin RB, Kennedy-Stephenson J. B-vitamin intakes of elderly supplement and non-supplement users in NHANES III. J Nutr Elder 2001;21:1–21. doi: 10.1300/J052v21n02_01. [DOI] [Google Scholar]
- 22.Yetley EA. Assessing the vitamin D status of the US population. Am J Clin Nutr 2008;88:558s–64s. [DOI] [PubMed] [Google Scholar]
- 23.Yang Q, Cogswell ME, Hamner HC, Carriquiry A, Bailey LB, Pfeiffer CM, Berry RJ. Folic acid source, usual intake, and folate and vitamin B-12 status in US adults: National Health and Nutrition Examination Survey (NHANES) 2003–2006. Am J Clin Nutr 2010;91:64–72. doi: 10.3945/ajcn.2009.28401. [DOI] [PubMed] [Google Scholar]
- 24.Tinker SC, Hamner HC, Qi YP, Crider KS. U.S. women of childbearing age who are at possible increased risk of a neural tube defect-affected pregnancy due to suboptimal red blood cell folate concentrations, National Health and Nutrition Examination Survey 2007 to 2012. Birth Defects Res A Clin Mol Teratol 2015;103:517–26. doi: 10.1002/bdra.23378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Yetley EA. Monitoring folate status in population-based surveys. Biofactors 2011;37:285–9. doi: 10.1002/biof.176. [DOI] [PubMed] [Google Scholar]
- 26.Bailey RL, Gahche JJ, Miller PE, Thomas PR, Dwyer JT. Why US adults use dietary supplements. JAMA Intern Med 2013;173:355–61. doi: 10.1001/jamainternmed.2013.2299. [DOI] [PubMed] [Google Scholar]
- 27.Nicastro HL, Bailey RL, Dodd KW. Using 2 assessment methods may better describe dietary supplement intakes in the United States. J Nutr 2015;145:1630–4. doi: 10.3945/jn.115.211466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Pludowski P, Holick MF, Grant WB, Konstantynowicz J, Mascarenhas MR, Haq A, Povoroznyuk V, Balatska N, Barbosa AP, Karonova T, et al. Vitamin D supplementation guidelines. J Steroid Biochem Mol Biol 2017. doi: 10.1016/j.jsbmb.2017.01.021. [DOI] [PubMed] [Google Scholar]
- 29.Bailey RL, Saldanha LG, Dwyer JT. Estimating caffeine intake from energy drinks and dietary supplements in the United States. Nutr Rev 2014;72 Suppl 1:9–13. doi: 10.1111/nure.12138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Rybak ME, Sternberg MR, Pao CI, Ahluwalia N, Pfeiffer CM. Urine excretion of caffeine and select caffeine metabolites is common in the U.S. population and associated with caffeine intake. J Nutr 2015;145:766–74. doi: 10.3945/jn.114.205476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Bailey RL, Fakhouri TH, Park Y, Dwyer JT, Thomas PR, Gahche JJ, Miller PE, Dodd KW, Sempos CT, Murray DM. Multivitamin-mineral use is associated with reduced risk of cardiovascular disease mortality among women in the United States. J Nutr 2015;145:572–8. doi: 10.3945/jn.114.204743. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Mues KE, Liede A, Liu J, Wetmore JB, Zaha R, Bradbury BD, Collins AJ, DT G. Use of the Medicare database in epidemiologic and health services research: a valuable source of real-world evidence on the older and disabled populations in the US. Clin Epidemiol 2017;9:267–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.McQuillan GM, McLean JE, Chiappa M, Corporation H, Lukacs SL. National Health and Nutrition Examination Survey Biospecimen Program: NHANES III (1988–1994) and NHANES 1999–2014. Vital Health Stat 2 2015:1–14. [PubMed]
- 34.Mazidi M, Kengne AP, Banach M. Mineral and vitamin consumption and telomere length among adults in the United States. Pol Arch Intern Med 2017;127:87–90. doi: 10.20452/pamw.3927. [DOI] [PubMed] [Google Scholar]