

The world continues to be entrenched in the COVID-19 pandemic, which has significantly impacted our daily interpersonal interactions, including community response to public emergencies that require bystander cardiopulmonary resuscitation. For healthcare workers on the frontline of COVID-19 care, our reality is a spectrum of disease that ranges from the mildly symptomatic patient to the critically ill, hypoxic, crashing patient. The public reality is “stay at home” orders or newly implemented “safer at home” plans, job losses and coping with the illness and death of family and friends. These events predominate daily routines in this “new normal”, as does a profound sense of fear-for the community and for health care providers. As a cardiac arrest outcomes researcher, I fear how this viral pandemic will threaten our altruistic societal approach to helping victims of cardiac arrest. Bystander cardiopulmonary resuscitation (bCPR) is an essential physical maneuver proven to impart better survival and neurologic recovery for cardiac arrest victims. CPR requires bystanders to come into close proximity with another individual, sometimes even a stranger, at a time when the messaging is to “socially distance”, and fears over SARS-CoV-2 transmission predominate.
Our generation has faced similar fears before-in the community and among healthcare providers. In 1981 the U.S. Centers for Disease Control and Prevention advised the public about a new infectious disease, initially causing pneumonia in homosexual men. This marked the beginning of the Human Immunodeficiency Virus (HIV) pandemic now a historical memory for many, but at the time, events that shocked society and produced overwhelming fear. Misconceptions about disease transmission were prevalent and discrimination against people living with HIV became pervasive. Exaggerated fears that touching someone with HIV might result in transmission of disease became ostracizing, and unsubstantiated fears of acquiring the disease by way of casual contact or touch became as endemic as the disease. We are all presently experiencing a similar fear, with pervasive underpinnings anchored on avoidance and anxiety. Similar to HIV, COVID-19 is heavily affecting disenfranchised communities (e.g. low socioeconomic status, racial/ethnic minorities, undomiciled, and others) that are already prone to poor access to healthcare, lower rates of bCPR and delayed response from emergency medical services.1,2 Confounding pre-existing disparities in rates of bCPR with the fear of an infectious virus that is aerosolized during CPR could have devastating results.
Early findings reported from four Italian provinces heavily affected by COVID-19 were reported in the New England Journal of Medicine.3 In comparison to the previous year, Baldi, et al. reported the incidence of out of hospital cardiac arrest increased by 58%. This is in stark contrast to the provision of bCPR that decreased by 15.6% in a region that had previously reported a bCPR rate of 47%. If we translate similar findings to the U.S., where rates of bCPR are variable and neighborhoods with lower socioeconomic status observe considerably less, we will undoubtedly see a devastating effect. Data from Washington found that in the midst of the pandemic, approximately 10% of cardiac arrest victims responded to by emergency medical services were COVID-19 positive. Assuming a transmission rate of 10% without personal protective equipment, after treating 100 patients, 1 rescuer may become infected.4 Rates of OHCA have been increasing during COVID-19, but those arrests may not be primarily due to the virus and limiting bystander resuscitative measures to protect the rescuer will undoubtedly result in death from cardiac arrest, not necessarily COVID-19.
The American Heart Association has issued an interim guideline on basic life support during COVID-19.5 Recommendations previously endorsed bystander CPR by the public for cardiac arrest victims and in 2010, rescue breaths were removed from the basic life support algorithm in favor of a “hands-only” approach. That being said, even “hands-only” CPR can result in aerosolization of respiratory droplets, and potential fomite transmission of SARS-CoV-2. While evidence is sparse, current COVID-19 recommendations recommend taking caution while still performing bCPR. When providing CPR to an unresponsive person, all efforts should be made to cover the face of the cardiac arrest victim with a cloth to minimize dispersion of respiratory droplets and the rescuer should have face covering as well if possible for increased protection. Rescue breaths should not be provided, and the rescuer should administer guideline concordant chest compressions and placement of an automated external defibrillator as soon as possible. Additional rescuers should remain at a distance, away from the victim’s airway and face, until they are needed to assume CPR when the initial rescuer fatigues. Messaging these suggested precautions and the early data regarding the risk of transmission must be relayed to the public immediately, and educational programs for bCPR should be amended to include this information as a means of keeping the rescuer safe while continuing to encourage bystander provision of basic life support to save lives.
Given the real and potential threat of viral inoculation perceived by the public, rates of bCPR will decline, undoubtedly resulting in more loss of life. There are many reasons why the public fear providing bystander CPR to an unresponsive person: the threat of contracting a deadly viral disease will undoubtedly enter the list of reasons to not render aid. Previous goals to improve rates of bCPR in the community are now in jeopardy as our “new normal” threatens to reduce current U.S. bCPR rates. Declining rates of bCPR are a reality: addressing this issue before it results in more death or neurologic disability is paramount. Cardiopulmonary resuscitation saves lives. It saved lives before this pandemic, and it will save lives after this pandemic. Our task will be to clearly understand the risk to operators, train the public in best practices to maintain one’s personal safety and to allay fears once we are safe to do so (Figure). Waiting for rates of bystander CPR to drop is too late. We must be prepared to educate and empower rescuers in our “new normal”.
Figure:
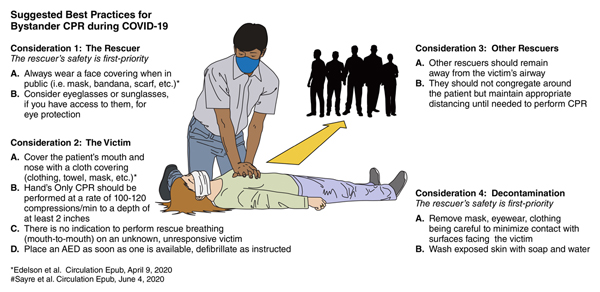
Suggested Best Practices for Bystander CPR During COVID-19
Acknowledgments
Disclosure Statement: Dr. Perman is supported by K23 HL138164 from the National Heart, Lung and Blood Institute. The views expressed in this manuscript represent those of the author, and do not necessarily represent the official views of the National Heart, Lung and Blood Institute.
Footnotes
There are no conflicts of interest to disclose pertaining to this work.
REFERENCES
- 1.Sasson C, Magid DJ, Chan P, Root ED, McNally BF, Kellermann AL, Haukoos JS; CARES Surveillance Group. Association of neighborhood characteristics with bystander-initiated CPR. N Engl J Med. 2012;367:1607–1615. doi: 10.1056/NEJMoa1110700 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kleindorfer DO, Lindsell CJ, Broderick JP, Flaherty ML, Woo D, Ewing I, Schmit P, Moomaw C, Alwell K, Pancioli A, Jauch E, Khoury J, Miller R, Schneider A, Kissela BM. Community socioeconomic status and prehospital times in acute stroke and transient ischemic attack: do poorer patients have longer delays from 911 call to the emergency department? Stroke. 2006;37:1508–1513. doi: 10.1161/01.STR.0000222933.94460.dd [DOI] [PubMed] [Google Scholar]
- 3.Baldi E, Sechi GM, Mare C, Canevari F, Brancaglione A, Primi R, Klersy C, Palo A, Contri E, Ronchi V, Beretta G, Reali F, Parogni P, Facchin F, Bua D, Rizzi U, Bussi D, Ruggeri S, Oltrona Visconti L, Savastano S; Lombardia CARe Researchers. Out-of-Hospital Cardiac Arrest during the Covid-19 Outbreak in Italy. N Engl J Med. April 29, 2020. doi: 10.1056/NEJMc2010418. [Online ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sayre MR, Barnard LM, Counts CR, Drucker CJ, Kudenchuk PJ, Rea TD, Eisenberg MS. Prevalence of COVID-19 in Out-of-Hospital Cardiac Arrest: Implications for Bystander CPR. Circulation. June 4, 2020. doi: 10.1161/CIRCULATIONAHA.120.048951. [Online ahead of print]. [DOI] [PubMed] [Google Scholar]
- 5.Edelson DP, Sasson C, Chan PS, Atkins DL, Aziz K, Becker LB, Berg RA, Bradley SM, Brooks SC, Cheng A, Escobedo M, Flores GE, Girotra S, Hsu A, Kamath-Rayne BD, Lee HC, Lehotzky RE, Mancini ME, Merchant RM, Nadkarni VM, Panchal AR, Peberdy MAR, Raymond TT, Walsh B, Wang DS, Zelop CM, Topjian A. Interim Guidance for Basic and Advanced Life Support in Adults, Children, and Neonates With Suspecte. Interim Guidance for Basic and Advanced Life Support in Adults, Children, and Neonates With Suspected or Confirmed COVID-19: From the Emergency Cardiovascular Care Committee and Get With the Guidelines®-Resuscitation Adult and Pediatric Task Forces of the American Heart Association in Collaboration with the American Academy of Pediatrics, American Association for Respiratory Care, American College of Emergency Physicians, The Society of Critical Care Anesthesiologists, and American Society of Anesthesiologists: Supporting Organizations: American Association of Critical Care Nurses and National EMS Physicians. Circulation. April 9, 2020. doi: 10.1161/CIRCULATIONAHA.120.047463. [Online ahead of print]. [DOI] [Google Scholar]