

Abstract
Introduction:
Cardiovascular comorbidities may predispose to adverse outcomes in hospitalized patients with coronavirus disease 2019 (COVID-19). However, across the United States the burden of cardiovascular comorbidities varies significantly. Whether clinical outcomes of hospitalized patients with COVID-19 differ between regions has not yet been studied systematically. Here, we report differences in underlying cardiovascular comorbidities and clinical outcomes of patients hospitalized with COVID-19 in Texas and in New York State.
Methods:
We established a multi-center retrospective registry including patients hospitalized with COVID-19, between March 15th, 2020 and July 12th, 2020. Demographic and clinical data were manually retrieved from electronic medical records. We focused on the following outcomes: mortality, need for pharmacologic circulatory support, need for mechanical ventilation, and need for hemodialysis. Univariate and multivariate logistic regression analyses were performed.
Results:
Patients in the participating Texas hospitals (n=296) were younger (57 vs 63 years, p-value <0.001), they had a higher BMI (30.3 kg/m2 vs 28.5 kg/m2; p =0.015), and they had higher rates of diabetes mellitus (41% vs 30%; p=0.014). In contrast, patients in the New York State cohort (n=218) had higher rates of coronary artery disease (19% vs. 10%; p=0.005) and atrial fibrillation (11% vs. 5%; p=0.012). Pharmacologic circulatory support, mechanical ventilation, and hemodialysis were more frequent in the Texas cohort (21% vs 13%, p=0.020; 30% vs 12%, p<0.001, and 11% vs 5%, p=0.009, respectively). In-hospital mortality was similar between the two cohorts (16% vs. 18%, p=0.469). After adjusting for differences in underlying comorbidities, only the use of mechanical ventilation remained significantly higher in participating Texas hospitals (Odds Ratios [95%CI]: 3.88 [1.23, 12.24]). Median time to pharmacologic circulatory support was 8 days (IQR: 2, 13.8) in the Texas cohort compared to 1 day (0, 3) in the New York State cohort, while median time to in-hospital mortality was 16 days (10, 25.5) and 7 days (4, 14), respectively (both p<0.001). In-hospital mortality was higher in the late versus the early study phase in the New York State cohort (24% vs 14%, p=0.050), while it was similar between the two phases in the Texas cohort (16% vs 15%, p=0.741).
Conclusions:
Geographical differences, including practice pattern variations and the impact of disease burden on provision of healthcare, are important for the evaluation of COVID-19 outcomes. Unadjusted data may cause bias affecting future regulatory policies and proper allocation of resources.
Keywords: COVID-19, Texas, New York, cardiovascular comorbidities, mortality, clinical outcomes
Introduction
Since its emergence one year ago, Coronavirus Disease 2019 (COVID-19) has spread rapidly worldwide, resulting in over 86 million cases and close to 2 million deaths at the time of writing this manuscript.[1] Underlying cardiovascular comorbidities are important predisposing factors to an unfavorable outcome.[2–5] Large disparities in the burden of cardiovascular comorbidities have been reported between different regions of the US.[6] Texas and New York are states with unique demographic characteristics and prevalence of cardiovascular disease among their residents.[7, 8] Whether clinical outcomes of hospitalized patients with COVID-19 are different between regions in the US has not yet been studied systematically. Our study addresses differences in underlying cardiovascular comorbidities and clinical outcomes of patients hospitalized with COVID-19 in selected hospitals of Texas and New York State.
Methods
Patient population and data collection
We established a multi-center retrospective registry of patients hospitalized with COVID-19 in the states of Texas and New York, from March 15th, 2020 until July 12th, 2020. Participating hospitals included Memorial Hermann Hospital-Texas Medical Center and the Lyndon B. Johnson Hospital in Houston, TX, Christus Spohn Health System in Corpus Christi, TX, Albany Medical Center in Albany, NY, and three United Health Services Hospitals in New York, Wilson Memorial Regional Medical Center in Johnson City, Binghamton General Hospital in Binghamton, and Chenango Memorial Hospital in Norwich. Figure 1 shows the US counties primarily served by the study hospitals and Figure 2 shows the patient distribution at each participating site.
Figure 1:
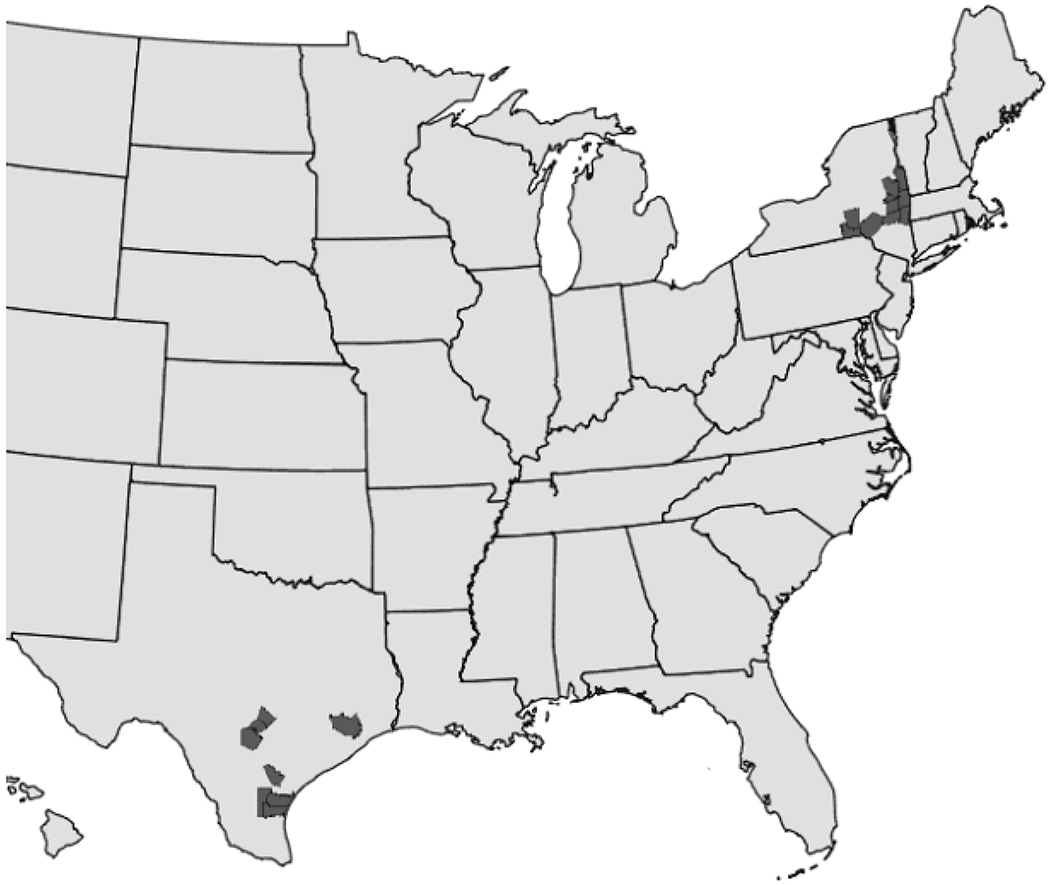
US counties primarily served by the study hospitals including Broome, Albany, Delaware, Waren, Saratoga, Rensselaer, Greene, Columbia, Schenectady, Chenango, and Washington counties in New York State, and Nueces, Jim Wells, Bee, Kleberg, Bexar, Comal, Hays, and Harris counties in Texas.
Figure 2:
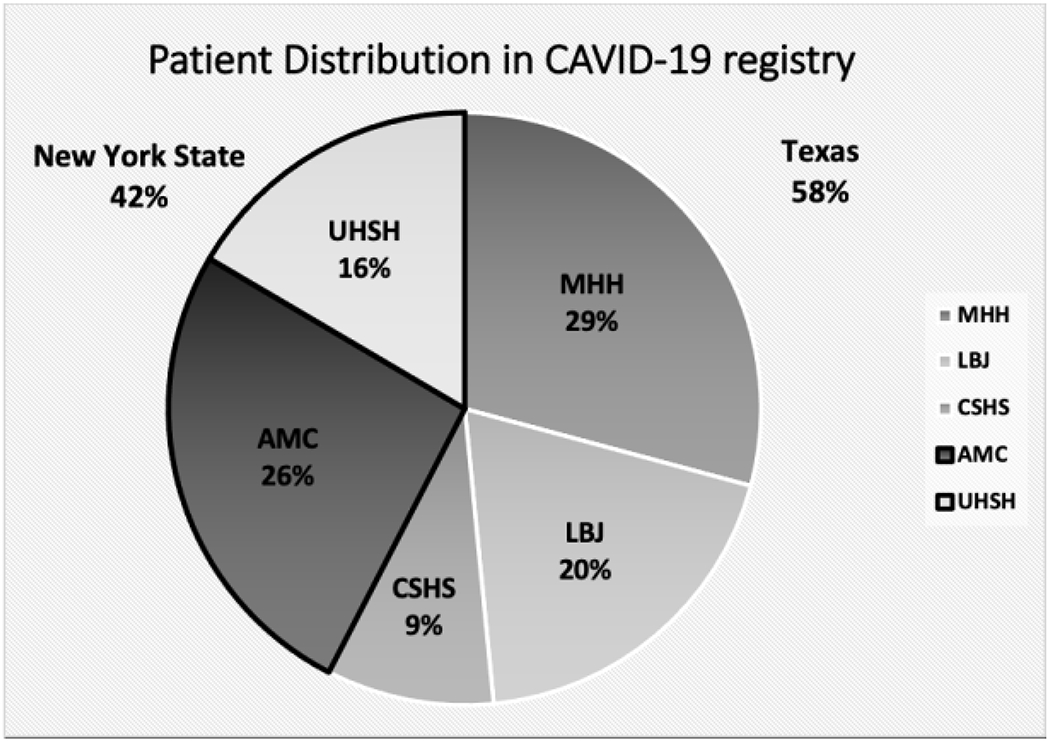
Patients distribution at each participating site. TX: Texas; MHH: Memorial Hermann Hospital- Texas Medical Center; LBJ: Lyndon B. Johnson Hospital; CSHS: Christus Spohn Health System; NY: New York; AMC: Albany Medical Center; UHSH: United Health Services Hospitals including Wilson Memorial Regional Medical Center, Binghamton General Hospital, and Chenango Memorial Hospital.
Hospital registries and hospitalization billing codes were used to identify consecutive patients admitted with COVID-19. All patients had laboratory confirmation of infection with SARS-CoV2. A positive laboratory finding for SARS-CoV-2 was defined as a positive result on real-time reverse-transcriptase-polymerase chain reaction (RT-PCR) assay of nasopharyngeal swab specimens. A diagnosis of COVID-19 was made based on the presence of disease-defining symptoms plus at least one positive RT-PCR assay.
A retrospective review of electronic medical records was performed, and detailed demographic and clinical characteristics, including past medical history, were recorded. Cardiovascular comorbidities were retrieved based on the admission medical records and included hypertension (HTN), diabetes mellitus (DM), dyslipidemia (DLD), coronary artery disease (CAD), heart failure (HF), atrial fibrillation (Afib), and stroke. Outcomes included mortality, need for pharmacologic circulatory support, need for mechanical ventilation, and need for hemodialysis. Pharmacologic circulatory support was defined as the use of vasopressors or inotropic agents for the treatment of shock. Demographic characteristics, cardiovascular comorbidities, and clinical outcomes of patients admitted to participating Texas hospitals were compared to those of patients admitted to participating New York State hospitals. Furthermore, we evaluated the time to the development of adverse clinical outcomes in the Texas versus New York State cohort as an attempt to determine whether the patients were admitted to the hospital at the same point in their illness. In order to evaluate the evolution of practice patterns over time, as care teams became more experienced treating COVID-19 patients, we devided the study period into an early (March 15th- April 30th) and late phase (May 1st- July 12th) and compared clinical outcomes between the two phases in Texas and New York State cohorts.
All data were collected after patients were discharged from the hospital or after patients expired while in the hospital. In order to ensure the accuracy and reproducibility of our data, we abstained from any automated data extraction. We also performed random quality checks, which yielded no errors in abstracted data.
Oversight:
The study was approved by the respective Institutional Review Boards of each participating site (protocol numbers: HSC-MS-20-0286, 20-04-2328, and 2020-063). It was also registered as an observational study at Clinicaltrials.gov on April 6th, 2020 (NCT04335630).
Statistical analysis
Continuous variables were tested for normality of distribution with the Shapiro-Wilk test. Non-normally distributed variables are presented as median values with interquartile ranges and were compared using the Mann-Whitney test. Categorical variables are presented as percentages and were compared using the chi-square test. Multivariable logistic regression analysis was performed to test for significant differences in clinical outcomes after adjusting for underlying demographics and comorbidities. The multivariable logistic regression model was adjusted for age at admission, BMI, Hispanic ethnicity, race, insurance type, and histories of diabetes mellitus, coronary artery disease, atrial fibrillation, and cancer to yield odds ratios (OR) with 95% confidence intervals (95%CI). A two-sided p-value of less than 0.05 was considered statistically significant. All statistical analyses were performed using STATA 15 (StataCorp, College Station, TX).
Results
We identified 514 consecutively hospitalized patients with COVID-19; 296 (58%) in Texas and 218 (42%) in New York State. The median age was 59 years (Interquartile range [IQR] 48-71), 53% were female, and 59% were Caucasians. Cardiovascular comorbidities were prevalent among the study participants, with HTN at 56%, DM at 36%, DLD at 30%, CAD at 14%, and HF at 11%. The median body mass index (BMI) was 29.4 kg/m2 (IQR 25.4-35.5).
Differences in demographic data and baseline cardiovascular comorbidities between patients hospitalized in the participating Texas and New York State hospitals
Table 1 compares the demographic characteristics and baseline cardiovascular comorbidities of patients with COVID-19 admitted to participating Texas versus New York State hospitals. Patients in Texas hospitals were younger (57 vs 63 years, p-value <0.001), had a higher BMI (30.3 kg/m2 vs 28.5 kg/m2; p =0.015), and higher rates of DM (41% vs 30%; p=0.014). In contrast, patients in New York State hospitals were older, had higher rates of CAD (19% vs 10%; p=0.005), and a higher prevalence of Afib (11% vs 5%). More African Americans and Hispanics were present in the Texas cohort compared to the New York State cohort (30% vs 11% and 43% vs 7%, respectively). Of note is also that 22% of patients in the Texas hospitals were uninsured compared to only 1% in the New York State hospitals (p <0.001).
Table 1:
Comparison of demographics and underlying cardiovascular comorbidities of patients with COVID-19 admitted to Texas and New York State hospitals
| Texas (N=296, 58%) | New York State (N=218, 42%) | p-value ** | |
|---|---|---|---|
| Female, n (%) | 165 (56.3) | 103 (48.1) | 0.068 |
| Age, years, median (IQR)* | 57 (47-66) | 63 (51-77) | <.0.001 |
| Age group, n (%) | <.0.001 | ||
| <40 years | 49 (16.6) | 31 (14.2) | |
| 40-49 years | 46 (15.5) | 20 (9.2) | |
| 50-59 years | 77 (26.0) | 37 (17.0) | |
| 60-69 years | 62 (21.0) | 48 (22.0) | |
| 70-79 years | 42 (14.2) | 38 (17.4) | |
| 80+ years | 20 (6.8) | 44 (20.2) | |
| Race, n (%) | <.0.001 | ||
| White | 146 (49.3) | 156 (71.6) | |
| Black | 88 (29.7) | 24 (11) | |
| Asian | 9 (3.0) | 7 (3.2) | |
| Other | 53 (17.9) | 31 (14.2) | |
| Hispanic ethnicity, n (%) | 127 (43.2) | 14 (6.6) | <.0.001 |
| BMI, kg/m2, median (IQR)* | 30.3 (25.9 - 35.9) | 28.49 (24.5 - 34.01) | 0.015 |
| Insurance, n(%) | <0.001 | ||
| Private | 97 (33.0) | 50 (23.1) | |
| Medicare | 65 (22.1) | 93 (43.1) | |
| Medicaid | 14 (4.8) | 49 (22.7) | |
| Uninsured | 65 (22.1) | 3 (1.4) | |
| Positive history of, n (%) | |||
| Hypertension | 174 (58.8) | 112 (51.4) | 0.095 |
| Heart failure | 31 (10.5) | 26 (11.9) | 0.604 |
| Coronary artery disease | 30 (10.1) | 41 (18.8) | 0.005 |
| Atrial fibrillation | 14 (4.7) | 23 (10.6) | 0.012 |
| Stroke | 20 (6.8) | 21 (9.6) | 0.234 |
| Diabetes Mellitus | 121 (40.9) | 66 (30.3) | 0.014 |
| Lung disease | 34 (11.5) | 33 (15.1) | 0.224 |
| Dyslipidemia | 93 (31.4) | 61 (28.0) | 0.400 |
| Cancer | 13 (4.4) | 19 (8.7) | 0.045 |
| Smoking exposure | 87 (33.0) | 65 (30.0) | 0.481 |
IQR = inter-quartile range
p-values from chi-square tests, except for Age and BMI (Mann-Whitney test)
Clinical outcomes of hospitalized patients with COVID-19 in participating Texas and New York State hospitals.
Pharmacologic circulatory support, mechanical ventilation, and hemodialysis were used in 17%, 22%, and 9%, respectively, in the entire cohort. In-hospital mortality was 17% for the entire cohort. COVID-19 patients admitted to the hospitals in Texas were more frequently treated with pharmacologic circulatory support, mechanical ventilation, and hemodialysis than the patients in New York State hospitals (21% vs 13%, p=0.020; 30% vs 12%, p<0.001, and 11% vs 5%, p=0.009, respectively; Table 2). However, in-hospital mortality was similar between the two cohorts (16% vs 18%, p=0.469). After adjusting for differences in underlying comorbidities using a multivariable logistic regression model, only the use of mechanical ventilation remained significantly higher in Texas (OR [95%CI]: 3.88 [1.23, 12.24]; Table 3). No significant differences in the use of pharmacologic circulatory support, hemodialysis or in-hospital mortality were observed (OR [95% CI]: 0.93 [0.28, 3.11], 1.96 [0.56, 6.79] and 1.48 [0.60, 3.66], respectively; Table 3).
Table 2:
Comparison of clinical outcomes of patients with COVID-19 admitted to Texas and New York State hospitals
| Clinical outcomes | Texas (N=296, 58%) | New York State (N=218, 42%) | p-value * |
|---|---|---|---|
| Pharmacologic circulatory support | 59 (20.6) | 27 (12.6) | 0.020 |
| Mechanical ventilation | 85 (29.7) | 25 (11.7) | <.0.001 |
| Hemodialysis | 32 (11.3) | 10 (4.7) | 0.009 |
| In-hospital mortality | 45 (15.6) | 39 (18.1) | 0.469 |
p-values from chi-square tests
Table 3:
Multivariable logistic regression analysis evaluating differences in clinical outcomes of COVID-19 patients admitted to Texas and New York State hospitals † after adjusting for differences in demographics and underlying cardiovascular comorbidities
| Clinical Outcome |
||||
|---|---|---|---|---|
| Regression model (predictor: state) | Pharm. Circ. Support | Mechanical Ventilation |
Hemodialysis | Death |
| Crude logistic, OR (95% CI)‡ | 1.79 (1.09, 2.94) | 3.20 (1.96, 5.21) | 2.58 (1.24, 5.37) | 0.84 (0.56, 1.35) |
| Multivariable logistic, OR (95% CI) * | 0.93 (0.27, 3.12) | 3.88 (1.23, 12.24) | 1.96 (0.56, 6.79) | 1.48 (0.60, 3.66) |
New York was the referent category for all analyses
OR = odds ratio; CI = confidence interval
Model was adjusted for age, bmi, Hispanic ethnicity, race, insurance type, diabetes mellitus, coronary artery disease, atrial fibrilliation, and cancer.
Median time to pharmacologic circulatory support of patients in the Texas cohort was 8 days (IQR: 2, 13.8) compared to 1 day (0, 3) in the New York State cohort (p<0.001). Median time to intubation was not different between the two cohorts (1 [0, 4] vs 0 [0, 5], p=0.430). Comparison of the time to hemodialysis between the two cohorts was not statistically meaningful due to the small number of available data. Median time to in-hospital mortality of patients in the Texas cohort was 16 days (10, 25.5) compared to 7 days (4, 14) in New York State cohort (p<0.001).
Clinical outcomes of hospitalized COVID-19 patients in Texas and New York State cohorts during the early and late study phase.
One hundred seventy nine patients (62%) in the Texas cohort were admitted to the hospital during the early study phase and 110 (38%) during the late study phase. One hundred twenty four patients (58%) in the New York state cohort were admitted to the hospital during the early study phase and 90 (42%) during the late study phase. No significant differences in the use of pharmacologic circulatory support, mechanical ventilation and hemodialysis between the early and late study phase in the Texas and New York state cohorts were noted (Table 3). Although in-hospital mortality was similar in the early and late study phase in the Texas cohort (16% vs 15%, p=0.741), it was higher in the late study phase in the New York State cohort (24% vs 14%, p=0.050; Table 4).
Table 4:
Comparison of clinical outcomes of patients with COVID-19 admitted to Texas and New York State hospitals in early versus late study period
| March-April | May-July | p-value | ||
|---|---|---|---|---|
| Admissions, N (%) | Texas | 179 (62) | 110 (38) | N/A |
| New York | 124 (58) | 90 (42) | N/A | |
| Pharmacologic circulatory support, N (%) | Texas | 35 (20) | 23 (21) | 0.880 |
| New York | 12 (10) | 15 (17) | 0.147 | |
| Mechanical ventilation, N (%) | Texas | 53 (30) | 30 (27) | 0.690 |
| New York | 15 (12) | 10 (11) | 1.000 | |
| Hemodialysis, N (%) | Texas | 19 (11) | 12 (11) | 1.000 |
| New York | 7 (6) | 3 (3) | 0.525 | |
| Death, N (%) | Texas | 29 (16) | 16 (15) | 0.741 |
| New York | 17 (14) | 22 (24) | 0.050 |
Discussion:
Our study draws attention to significant differences in demographics and baseline cardiovascular comorbidities between patients with COVID-19 admitted to a spectrum of hospitals in Texas and in New York State. While pharmacologic circulatory support, mechanical ventilation, and hemodialysis were more commonly used in Texas than in New York, in-hospital mortality was not different. After adjusting for differences in the underlying comorbidities between the patients in the two cohorts, the use of mechanical ventilatory support was less frequent in the New York State cohort.
A high prevalence of cardiovascular comorbidities, including HTN, DLD, DM, CAD, and HF was noted throughout the entire registry. This is in line with reports suggesting that cardiovascular comorbidities predispose to an unfavorable outcome and hospitalization of patients with COVID-19.[2–5] However, the high prevalence of cardiovascular comorbidities may also reflect a lower threshold for admission to the hospital of these patients. The Centers of Disease Control and Prevention (CDC), in their clinical guidance for management of patients with confirmed COVID-19, advise for close monitoring and possible hospitalization of patients with risk factors for severe disease including cardiovascular comorbidities.[9]
Significant differences in demographic characteristics and baseline comorbidities were detected between the patient population hospitalized with COVID-19 in Texas and New York State. Patients in the Texas cohort were younger, more severely obese, and had higher rates of DM. More African Americans and Hispanics were present in the Texas cohort than in the New York State cohort. Of note is that the number of uninsured patients was significantly higher in the Texas cohort than in the New York State cohort (22% vs 1%). However, one of the three hospitals that we studied in Texas is a County hospital with a particularly high prevalence of uninsured patients. We also note that the patients in New York State cohort were older, with higher rates of underlying CAD and Afib. Medicare and Medicaid were the primary insurance plans for two-thirds of the patients hospitalized in participating New York State hospitals. These differences reflect baseline demographic differences in the communities that we studied. [6–8] It is also likely that the different disease burden and time of peak hospitalization rates in the two states contributed to differences in the population characteristics of the infected patients.
Pharmacologic circulatory support, mechanical ventilation, and hemodialysis were more commonly used in the Texas cohort than in the New York State cohort. Although this might suggest that hospitalized patients with COVID-19 in the Texas cohort have a more severe disease course, no significant difference was noted in the in-hospital mortality between the two cohorts. When we adjusted for the differences in the underlying comorbidities between the two cohorts, only the use of mechanical ventilation remained more common in Texas hospitals. This may reflect the reluctance of the older patient population in New York State to give consent to intubation or practice pattern variations between the South and Northeast regions of the US. Our study is the first to report on these practice pattern variations related to COVID-19 treatment. Although, they have not been previously studied in COVID-19 patients, practice pattern variations between the South and Northeast regions of the US, pertaining to the use of mechanical ventilation, vasoactive medications, and hemodialysis, have been described in the literature. In a large nationwide study of over 17,000 patients with idiopathic pulmonary fibrosis, clinicians treating patients in the South region of the US were more likely to offer mechanical ventilatory support compared to the Northeast region.[10] In a different study of over 100,000 adults from 294 US hospitals, use of vasoactive medications post cardiac surgery was significantly more common in the South compared to the Northeast.[11] Furthermore, a study of over 400,000 hospitalizations with dialysis-requiring acute kidney injury in the US, reported more frequent use of hemodialysis in the South than Northeast.[12] Our study findings are in line with the above studies, suggesting that there is regional variation in the use of mechanical ventilation, vasoactive medications, and hemodialysis in the treatment of COVID-19 patients between the South and Northeast regions of the US.
In-hospital mortality of patients with COVID-19 in our registry was 17%. This is similar to the in-hospital mortality rate of 20% that was previously reported in a large multi-center US study of more than 11,000 patients.[13] In addition, in-hospital mortality rates were similar among patients in participating Texas and New York State hospitals. This supports that the standard of patient care provided in the participating Texas hospitals was overall similar to the patient care in the participating New York State hospitals.
In order to evaluate whether COVID-19 patients in participating Texas and New York State hospitals were admitted at about the same point in their illness, we compared the time to the development of adverse outcomes. We observed that the patients in the New York State cohort required pharmacologic circulatory support sooner and died earlier than the patients in the Texas cohort. This suggests that the patients in the New York State cohort may have been admitted at a later point in their illness compared to patients in the Texas cohort, leading to earlier need for interventions and earlier in-hospital mortality.
Our study also evaluated potential differences in the practice patterns over time, as care teams became more experienced in treating COVID-19 patients, by comparing clinical outcomes of patients admitted to the hospital in the early (March 15th-April 30th) versus the late study period (May 1st- July 12th) between the Texas and New York state cohorts. No significant differences in the use of pharmacologic circulatory support, mechanical ventilation, or hemodialysis were identified over time in either of the two cohorts. This may be due to the short time frame that our study examined. Although no difference was noted in mortality between the two phases in the Texas cohort, mortality was higher in the late phase in the New York state cohort. Of note is that on March 25th, 2020 a policy directive from the New York State Department of Health was issued, allowing expedited re-admission or admission of COVID-19 patients in the nursing homes, in an effort to ensure adequate hospital capacity for COVID patients requiring advanced care. [14] Although this nursing home policy might have contributed to the mortality difference, our data did not reveal any difference in the median age or median number of comorbidities between the two phases, which argues against the above hypothesis (median age: 63 [IQR 50.8 - 77] vs 61 [IQR 51 – 76.8] years; p=0.889 and median number of cardiovascular comorbidities: 2 [IQR 0 – 3] vs 1 [IQR 0–3] comorbidities; p=0.372).
Our study has several strengths. First, it is based on a multi-center registry with patients admitted to both tertiary and community hospitals across the states of Texas and New York. This contributed to a diverse patient population, with 53% of the patients being female and 41% non-white. Therefore, the findings of the study are representative of and relevant to all racial and socioeconomic segments of the population. Secondly, all data used in the study were manually abstracted from patients’ electronic health records, yielding thorough reporting of patient history and clinical course. Additionally, missing values represented only less than 10% of the patient data, providing a complete picture of the patient’s clinical course.
Our study also has certain limitations. The retrospective nature of the data collection makes our study prone to biases. We attempted to eliminate selection bias and confounding by using multivariable logistic regression analysis, although residual selection bias is likely. Furthermore, the hospitals that we studied may not be completely representative of hospitals in the rest of each state in terms of equipment, level of care, and the population they serve. In fact, no hospitals from New York city participated in the New York State cohort, as opposed to Texas cohort, which included hospitals in Houston. Lastly, the collection of baseline cardiovascular comorbidities was dependent on appropriate documentation by the primary provider and accurate retrieval of the data by our data collection team. As already mentioned, to eliminate inaccuracies with the data collection, we elected to collect the data by manual chart review and avoid automated data extraction algorithms. Furthermore, we performed random quality checks, which yielded no errors in abstracted data.
Conclusions:
Geographical differences, including practice pattern variations and the impact of disease burden on provision of healthcare, are important for the evaluation of COVID-19 outcomes. Unadjusted data may cause bias affecting future regulatory policies and proper allocation of resources.
Acknowledgements and Funding
Dr. Taegtmeyer’s lab is supported by grants from the United States Public Health Service R01 HL 073162; R01-HL-61483; R01-HL-123627 (to H.T.)
We thank Anna Menezes for expert editorial assistance.
Glossary:
- COVID-19
coronavirus disease 2019
- HTN
hypertension
- DLD
dyslipidemia
- DM
diabetes mellitus
- CAD
coronary artery disease
- HF
heart failure
- Afib
atrial fibrillation
Footnotes
Disclosure Statement: The authors have no conflicts of interest to disclose.
Conflict of Interest
No competing interests exist.
Statement of Ethics
The study complies with internationally accepted standards for research practice and reporting and it was approved by the respective Institutional Review Boards of each participating site (protocol numbers: HSC-MS-20-0286, 20-04-2328, and 2020-063). Since our study involved retrospective review of patients’ medical charts, the need for written informed consent was waived by the IRB.
References:
- 1. Retrieved from: https://coronavirus.jhu.edu/map.html. Date retrieved: 1-5-2021.
- 2.Chen R, Liang W, Jiang M, Guan W, Zhan C, Wang T et al. Risk Factors of Fatal Outcome in Hospitalized Subjects With Coronavirus Disease 2019 From a Nationwide Analysis in China. Chest. 2020;158(1):97–105. doi: 10.1016/j.chest.2020.04.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Williamson EJ, Walker AJ, Bhaskaran K, Bacon S, Bates C, Morton CE et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature. 2020;584(7821):430–6. doi: 10.1038/s41586-020-2521-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Zheng Z, Peng F, Xu B, Zhao J, Liu H, Peng J et al. Risk factors of critical & mortal COVID-19 cases: A systematic literature review and meta-analysis. The Journal of infection. 2020;81(2):e16–e25. doi: 10.1016/j.jinf.2020.04.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Yang J, Zheng Y, Gou X, Pu K, Chen Z, Guo Q et al. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: a systematic review and meta-analysis. International journal of infectious diseases : IJID : official publication of the International Society for Infectious Diseases. 2020;94:91–5. doi: 10.1016/j.ijid.2020.03.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Roth GA, Johnson CO, Abate KH, Abd-Allah F, Ahmed M, Alam K et al. The Burden of Cardiovascular Diseases Among US States, 1990–2016. JAMA cardiology. 2018;3(5):375–89. doi: 10.1001/jamacardio.2018.0385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Prevalence of Heart Disease Among Adults bDC, Risk Factors / Comorbid Conditions, and Place of Residence, Texas 2018. Prepared by Chronic Disease Epidemiology Branch, Health Promotion and Chronic Disease Prevention Section, Texas Department of State Health Services.
- 8.Cardiovascular Disease Mortality in New York State. Results from the New York State Vital Records Death Statistics and the Bureau of Vital Statistics. New York City Department of Health and Mental Hygiene. https://health.ny.gov/diseases/cardiovascular/heart_disease/docs/cvd_mortality.pdf. [Google Scholar]
- 9. https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-guidance-management-patients.html. Accessed on 12/13/2020.
- 10.Rush B, Wiskar K, Berger L, Griesdale D. The use of mechanical ventilation in patients with idiopathic pulmonary fibrosis in the United States: A nationwide retrospective cohort analysis. Respiratory medicine. 2016;111:72–6. doi: 10.1016/j.rmed.2015.12.005. [DOI] [PubMed] [Google Scholar]
- 11.Vail EA, Shieh MS, Pekow PS, Gershengorn HB, Walkey AJ, Lindenauer PK et al. Use of Vasoactive Medications after Cardiac Surgery in the United States. Annals of the American Thoracic Society. 2021;18(1):103–11. doi: 10.1513/AnnalsATS.202005-465OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hsu RK, McCulloch CE, Ku E, Dudley RA, Hsu CY. Regional variation in the incidence of dialysis-requiring AKI in the United States. Clinical journal of the American Society of Nephrology : CJASN. 2013;8(9):1476–81. doi: 10.2215/cjn.12611212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Yehia BR, Winegar A, Fogel R, Fakih M, Ottenbacher A, Jesser C et al. Association of Race With Mortality Among Patients Hospitalized With Coronavirus Disease 2019 (COVID-19) at 92 US Hospitals. JAMA network open. 2020;3(8):e2018039. doi: 10.1001/jamanetworkopen.2020.18039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.New York State Department of Health’s (NYSDOH) Advisory. … www.hurlbutcare.com › images › NYSDOH_Notice.