

Abstract
Background:
Motor abnormalities, such as psychomotor agitation and retardation, are widely recognized as core features of depression. However, it is not currently known if motor abnormalities connote risk for depression.
Methods:
Using data from the Adolescent Brain Cognitive Development (ABCD) Study, a nationally representative sample of youth (n=10,835, 9–11 years old), the present paper examines whether motor abnormalities are associated with (a) depression symptoms in early adolescence, (b) familial risk for depression (familial risk loading), and (c) future depression symptoms. Motor abnormalities measures included traditional (DSM) motor signs such as psychomotor agitation and retardation as well as other motor domains such as developmental motor delays and dyscoordination.
Results:
Traditional motor abnormalities were less prevalent (agitation=3.2%, retardation=0.3%) than non-traditional domains (delays=13.79%, coordination=35.5%) among adolescents. Motor dysfunction was associated with depression symptoms (Cohen’s ds=0.02 to 0.12). Familial risk for depression was related to motor abnormalities (Cohen’s ds=0.08 to 0.27), with the exception of motor retardation. Family vulnerability varied in sensitivity to depression risk (e.g., retardation: .53%; dyscoordination: 32.05%). Baseline endorsement of motor abnormalities predicted future depression symptoms at one-year follow-up.
Conclusions:
These findings suggest that motor signs reflect a novel, promising future direction for examining vulnerability to depression risk in early adolescence.
Introduction
Major depressive disorder is one of the leading causes of disability in the world, indicating that depression is both a serious public health concern and economic burden[1]. Although treatments exist, they have modest treatment response rates (approximately ~40–50% remission)[2, 3]. In response to this problem, a growing literature suggests that early identification of this disorder and targeted interventions may reduce the rates and course of depression[4, 5]. Current approaches to assessing risk in depression focus on familial risk, emotion, cognition, or psychosocial factors[6–8]. However, these risk assessments omit motor signs, despite psychomotor slowing and agitation being characteristic features of depression[9] and the sensitivity of motor behaviors signal changes in underlying neural circuitry[10–12]. As a result, motor abnormalities may be a valuable early marker of vulnerability[11, 13]. Indeed, pediatric practice has long depended on the use of early motor milestones as a sensitive marker of disturbances in development[14]. In other psychopathology, such as psychosis, distinct motor abnormalities have served as strong indicators of early vulnerability as well as emerging brain dysfunction[15–22]. There is some evidence to suggest motor abnormalities may predict a severe course of depression in older adults[11, 23–25] and that motor abnormalities show promise for the notion of an early biomarker application[26]. However, it is not known if motor abnormalities are associated with vulnerability for depression in early adolescence. Early adolescence is a critical developmental period where symptoms first emerge, making it an ideal period for identifying markers of vulnerability for the disorder[27, 28]. Unfortunately, the relationship of motor abnormalities to depression in adolescence remains poorly characterized[15]. Additionally, it is not clear which motor signs might be most relevant in adolescence. Finally, motor signs may be a marker that could predict a symptom course starting in early adolescence.
Current neurobiological models of depression suggest that many depression symptoms may be related to a long-term downregulation of dopamine impacting inter-related, parallel circuits (e.g., affective, associative, and motor)[10, 11, 29]. Recent literature also suggests that disturbances in these parallel circuits may have synergistic impacts on clinical deficits across emotion, cognition, and motor behaviors[30]. Regardless of the exact source of the pathophysiology[31], it is clear that any such disturbance may also impact motor behavior, alongside cognitive and affective circuits. As a result, motor signs can be a clinically significant risk marker that should be considered alongside traditional cognitive, heritability, and affective markers.
Among the adult literature, motor signs have been viewed as core components of depression for decades[9]. Extant research highlight the potential for motor abnormalities to be crucial behavioral markers that relate to greater symptom severity[23, 24, 27], worsening course[25, 32], lower quality of life[24], and worse response to antidepressant treatment[33, 34]. However, in developmental literature, it remains unknown whether these motor abnormalities are merely an epiphenomena or reflect a marker of vulnerability for depression[15]. Furthermore, it is not clear if psychomotor agitation and psychomotor retardation are the ideal markers of vulnerability in early adolescence or if other motor markers may be more relevant earlier in development.
Early depression vulnerability may be marked by delays in meeting developmental motor milestones (e.g., sitting upright, rolling over, walking)[35]. Indeed, infants of depressed mothers exhibited developmental motor delays[36, 37], and such delays have predicted symptoms several decades later in adulthood[16, 38]. While these studies provide strong evidence of developmental motor delays as a vulnerability marker, it is not clear if developmental motor delays confer additional sensitivity to vulnerability measures over traditional motor signs or reflect the same general vulnerability. In addition to developmental motor delays, developmental coordination disorder (a childhood movement disorder) has been related to high levels of childhood depression[39, 40] and future depression in adulthood[41, 42]. In a parallel line of work, adults with depression with psychotic features have also shown motor dyscoordination[43], which suggests that dyscoordination may be relevant marker of vulnerability for this disorder. As such, an expanded list of motor abnormalities may be a useful marker of symptoms, onset, or risk.
In addition to a limited set of motor abnormalities, there has been no comprehensive or comparative assessment of motor abnormalities to vulnerability to depression in a single sample. Comparing motor abnormality prevalence across current depression, familial risk for depression, and future depression may indicate whether motor abnormalities reflect inherited mechanisms (familial risk loading for depression) or the presence of active disease processes (current depression)[44]. Though some extant literature suggests the heritability of specific motor signs[27], little is known whether motor abnormalities reflect a stable vulnerability or track early emerging symptoms in adolescence. Examining multiple facets of vulnerability in a single study will thus aid in assessing whether motor abnormalities may be potential psychiatric endophenotypes of depression vulnerability.
Large, representative, and longitudinal samples of adolescents, such as the Adolescent Brain Cognitive Development (ABCD study), provide a unique opportunity to assess the relevance and sensitivity of motor signs to vulnerability to depression. To date, ABCD studies have largely focused on the contribution of health behaviors (i.e., sleep[45], BMI[46], exercise[47, 48]), environment (i.e., stress[49], SES[50, 51]), or individual traits (i.e., familial risk loading[52–54], race[50, 51]) to depression. Far fewer of these studies have examined specific depression symptoms over time[55], and none have examined the potential relationship of motor abnormalities to concurrent depression, familial risk for depression, or future risk for depression. This study leverages the nationally representative samples of young adolescents in the ABCD study to answer several heretofore unanswered questions about the relevance of motor signs in this critical developmental period. First, we determined the prevalence of motor abnormalities in adolescents in general and in those with depression using both traditional (psychomotor agitation, psychomotor retardation) and novel motor measures (developmental motor delays, dyscoordination), thus examining the utility of expanding the traditional motor signs to include developmental motor delays from early life and dyscoordination. We hypothesized that motor signs will be present in adolescence and more prevalent among individuals with emerging depression or risk for depression. Importantly, given the age of the sample and the age window for when depression typically has its onset[56], many individuals in ABCD will have not yet passed through the peak risk window for full depression onset. Therefore, in the current study, we examined depressive symptoms dimensionally and hypothesized that individuals who endorsed a motor sign will have a greater number of depression symptoms. Second, we tested whether motor abnormalities are familial vulnerability factors for depression. This analysis provided insight into which motor abnormalities track emerging symptoms or mechanisms related to inherited risk, and whether motor abnormalities represent a general depression vulnerability endophenotype. We hypothesized that motor signs are related to higher rates of familial vulnerability. Finally, we examined the potential utility of motor abnormalities at baseline to predict depression symptoms at the 1-year follow-up. We expected youth with motor abnormalities at baseline to demonstrate higher rates of depression at follow-up.
Materials and Methods
Participants.
The ABCD study included 21 sites across the United States who collected participants (aged 9–11 years) with a broad demographic diversity range. All research protocols were in line with the ethical guidelines laid out by each respective Institutional Review Board (DOI: 10.15154/1519065). These guidelines included obtaining both the parents’ informed consent and the children’s assent. The ABCD Study aimed to track development from childhood through adolescence to understand factors that may alter healthy development. In the ABCD study, self-assessments were comprehensive and included various measures, such as automated current diagnoses, dimensional assessments of current psychopathology symptoms, and familial risk loading for psychopathology. The present paper takes advantage of this comprehensive approach by examining each of these clinical characterizations of depression vulnerability to examine how each might relate to motor signs. Data was used from ABCD baseline timepoint for motor and baseline depression vulnerability data and one-year follow-up waves for the longitudinal analyses.
Measures.
Youth Psychopathology Assessments.
The Schedule for Affective Disorders and Schizophrenia for School-Age Children, Present and Lifetime Version (K-SADS-PL) is a semi-structured parent-child interview designed to assess present and lifetime psychopathology[57]. K-SADS-PL measures affective and psychotic impairments on both diagnosis-specific and global levels and is highly reliable and well-validated; all questions were asked of each participant. The depression symptoms sum was calculated as a total count of symptoms that were endorsed (current or in the past), resulting in a possible score of 0 to 35[see Supplemental Information (SI), 2]. Additionally, this assessment produces a spectrum of depression diagnoses that are automated and not fully assessed by a clinician. As such, they are not recommended for inclusion in studies. However, such diagnoses show similar patterns of findings as the results below. As a result, we have included these diagnostics in supplemental material, but emphasize caution in their reference and interpretation. For a comparison of specificity, total social anxiety symptoms were also compared to motor symptoms.
Motor Assessments.
Measurements of motor abnormalities are not a central domain of the ABCD study. However, four items within clinical scales assess past and current motor abnormalities. These items include (a) early motor developmental delays (ABCD Developmental History Questionnaire), (b) current symptoms coordination (Child Behavioral Checklist), (c) psychomotor retardation (KSADS), and (d) psychomotor agitation (KSADS), SI. All motor variables were coded dichotomously (absence or presence).
Family History Assessment.
The Family History Assessment Module Screener (FHAM-S[58]) screens for the presence/absence of psychopathological symptoms in first-degree biological relatives and were completed by parents. A total number of first-degree relatives (parents or siblings) endorsed as having depression were used as a proximal measure of familial loading of risk.
Data Analyses.
First, we used a linear regression analyses to examine current depression symptoms to rates of motor abnormalities (i.e., psychomotor agitation, psychomotor retardation, developmental motor delays, dyscoordination) where depression symptoms was the dependent variable and stimulant medication status was a covariate given the impact of stimulants on motor behavior. Confidence intervals were assessed with 1,000 iterations of bootstrapped samples. In developmental symptoms, no correction for current medication was applied and differences were assessed with a chi-square analysis. Second, for the dependent variable of familial risk, general linear models were run for each motor abnormality. Diagnostic test characteristics are reported for all motor measures, Table 2[59]. Third, we tested whether motor abnormalities at baseline predicted depression symptoms at a one-year follow-up in two stepwise regressions. All current symptom analyses excluded individuals on antipsychotics (n=74). Supplemental analyses that included these individuals and did not correct for stimulant medication use yielded similar results (SI). Additionally, post-hoc parallel analyses were conducted for total social anxiety symptoms to examine possible specificity (SI). Finally, for each set of analyses (baseline depression, family history of depression, depression at follow-up) we ran multivariate models that including all motor abnormality variables in order to examine the unique contribution of each motor abnormality to the depression outcome variable. All models described above were considered significant if they passed Bonferroni correction for 4 model comparisons (p<.0125, SI). Analyses were run in SPSS version 27 and visualized in Rv4.0.3.
Table 2.
Test Characteristics of Motor Abnormalities for Detecting Depression Diagnoses
| Motor Abnormalities | Familial MDD History/None | Overall Prevalence | Sensitivity | Specificity | PPV | NPV | OR |
|---|---|---|---|---|---|---|---|
|
| |||||||
| Any motor sign | 1141/2045 | 27.33% | 32.05% | 74.75% | 35.81% | 71.45% | 1.40 |
| 2+ motor signs | 111/166 | 3.17% | 4.39% | 97.33% | 40.07% | 71.45% | 1.67 |
| Psychomotor Agitation | 72/105 | 1.50% | 2.00% | 98.72% | 40.68% | 69.66% | 1.57 |
| Psychomotor Retardation | 19/18 | 0.31% | 0.53% | 99.78% | 51.35% | 69.57% | 2.41 |
| Developmental Motor Delays | 447/680 | 9.58% | 12.21% | 91.61% | 39.66% | 69.78% | 1.52 |
| Dyscoordination | 839/1432 | 19.25% | 23.32% | 82.54% | 36.94% | 71.05% | 1.44 |
Results
Prevalence of Motor Abnormalities and Depression Symptoms in Whole Sample.
In the whole sample, 26.9% of individuals endorsed at least one motor sign and 3% endorsed two or more motor signs: 1.5% endorsed psychomotor agitation, 0.3% endorsed psychomotor retardation, 8.8% endorsed developmental motor delays, and 19.3% endorsed dyscoordination, Table 1. The average depression symptoms endorsed in the whole sample at baseline was 0.74 (StD=2.44) and 0.94 (StD=2.71) at follow up; change in number of symptoms endorsed averaged of 0.41 (StD=3.20). Among individuals who endorsed at least one depression symptom, the average number of symptoms endorsed was 5.97 (StD = 4.08) and 5.79 (StD=4.13) at follow up. For individuals who endorsed at least one symptom at either timepoint, the average change in symptoms was 1.79 (StD=.6.50). Finally, 30.5% of the sample had a first-degree relative with a depression diagnosis.
Table 1.
Demographic Metrics: Prevalence among the whole sample, depression diagnoses, and familial history categories.
| Familial History of Depression |
||||
|---|---|---|---|---|
| Whole Sample | Yes | No | Group Comparison | |
| n=11,870 | n=3639 | n=8230 | Statistics | |
|
|
||||
| Age (Months) -M(StD) | 118.95 (7.46) | 119.03 (7.46) | 118.75 (7.46) | t(11868)=1.92 p=.06 |
| Sex (% Female) | 48.00% | 47.80% | 48.10% | χ2(1)=.14 p=.71 |
| Any Motor Sign | 3186 | 31.35% | 24.85% | |
| Psychomotor Agitation | 180 | 1.30% | 2.00% | χ2(1,11800)=26.04, p=.001 |
| Psychomotor Retardation | 37 | 0.50% | 0.20% | χ2(1, 11800)=9.08, p=.01 |
| Developmental Motor Delays | 1127 | 8.40% | 2.60% | χ2(1, 11662)= 5.62, p=.02 |
| Dyscoordination | 2271 | 23.30% | 17.50% | χ2(2, 11800)=111.08, p<.001 |
Prevalence of Motor Abnormalities and Concurrent Depression Symptoms.
Depression Symptoms and Psychomotor Agitation.
Adolescents who endorsed psychomotor agitation endorsed more depression symptoms, M=1.55, SD=3.84, compared to those who did not endorse Psychomotor agitation, M=0.73, SD=2.41; Cohen’s d=0.34; B=0.08, SE=.02, p<.001.
Depression Symptoms and Psychomotor Retardation.
Adolescents who endorsed psychomotor retardation endorsed more depression symptoms, M=2.51, SD=4.40, compared to those without psychomotor retardation, M=0.76, SD=2.43; Cohen’s d=0.73; B=0.13, SE=0.03, p<.001.
Depression Symptoms and Developmental Motor Milestones Delays.
Adolescents with developmental motor delays endorsed more depression symptoms, M=1.18, SD=3.23, compared to adolescents with no motor delays, M=0.07, SD=2.43, Cohen’s d=0.152; t(11652)=6.07, p<.001.
Depression Symptoms and Dyscoordination.
Adolescents who endorsed dyscoordination endorsed more depression symptoms, M=1.49, SD=3.50, compared to coordinated adolescents, M=0.56, SD=2.07; B=0.12, SE=0.008, Cohen’s d=0.39, p<.001.
Motor Abnormalities Relative Association with Depression Symptoms.
A general linear model with simultaneously entered predictors demonstrated that motor abnormalities overall were related to depression symptoms even after accounting for the variance related to stimulant medication use, F(5,11646)=82.49, r2=.03, p<.001. All four motor variables were related to number of depression symptoms endorsed - psychomotor agitation (B=0.82, 0.41–0.59 95% C.I., t=2.55, SE=0.19, p=.007), psychomotor retardation (B=1.37, 0.56–2.19 95% C.I., t=3.32, SE=0.41, p=.001), developmental motor delays (B=0.43, 0.27–0.99 95% C.I., t=5.45, SE=0.09, p<.001) and dyscoordination (B=0.86, 0.67–1.00 95% C.I., t=15.20, SE=0.06, p<.001).
Motor Abnormalities and Familial Risk for Depression.
Familial Risk and Psychomotor Agitation.
Endorsement of psychomotor agitation related to a greater familial risk for depression, B=0.24, SE=.08, p<.001, Cohen’s d=0.27; psychomotor agitation: M=1.55, SD=3.84; no psychomotor agitation: M=0.73, SD=2.41).
Familial Risk and Psychomotor Retardation.
Psychomotor retardation in youth was unrelated to the number of relatives with a depression diagnosis, B=0.28, SE=0.15, p=.07, Cohen’s d=0.34.
Familial Risk and Developmental Motor Milestones Delays.
Individuals with delayed motor milestones had more first-degree relatives with depression (M=0.47, SD=.759) than individuals who did not experience delays (M=0.40, SD=.727), t(11730)=2.93, p<.001, Cohen’s d=0.082.
Familial Risk and Dyscoordination.
Endorsement of dyscoordination related to familial risk for depression, B=0.22, SE=.029, p<.001, Cohen’s d=0.19. Individuals who endorsed current dyscoordination had more first-degree relatives with depression (M=1.49, SD=2.07) than those who did not endorse dyscoordination (M=0.56, SD=2.867).
Motor Abnormalities Relative Contribution to Depression Familial Vulnerability - Familial Risk Loading.
A general linear model with simultaneously entered predictors demonstrated that motor abnormalities overall were related to familial risk for depression accounting for the variance related to stimulant medication use, F(5,11646)=33.18, p<.001, r2=.013. Three of the four motor variables were each uniquely related to familial risk for depression - psychomotor agitation (B=0.16, 0.036–0.26 95% C.I., t=2.58, SE=0.06, p=.007), developmental motor delays (B=0.06, SE=0.03, p=.02), and dyscoordination (B=0.13, SE=0.02, p<.001), while psychomotor retardation was not (B=0.23, SE=0.17, p=.17). The test characteristics of motor signs in predicting familial vulnerability to depression can be found in Table 2.
Motor Abnormalities and Future Symptoms.
Depression Symptoms at One-Year Follow-Up.
In a stepwise regression, predicting dimensional depression symptoms at follow-up, the first step included baseline symptoms of depression and stimulant uses, and the second step included baseline motor abnormalities (motor agitation, motor retardation, and dyscoordination). The overall model was significant, F(4, 6448)=38.18, p<.001, and the change between steps was significant (F-change(4, 6448)=42.25, r2−change=.011, p<.001), indicating that motor abnormalities predicted depression symptoms at follow-up over and above baseline depression symptoms alone. Baseline depression symptoms significantly contributed to the model (β= .146; t=8.89, partial r=.11, p<.001), and all four motor abnormalities each uniquely predicted follow-up depression symptoms in a second step (dyscoordination: t=2.53, p=.011, β=0.31; partial r=.10; psychomotor retardation: t=6.80, p<.001, β=0.088; partial r=.084; psychomotor agitation: t=2.07, p=.038, β=0.027; partial r=.026), Table 2.
Discussion
Adolescents with motor abnormalities had greater depression vulnerability. Traditional (psychomotor agitation, psychomotor retardation) and novel (developmental motor milestones, dyscoordination) motor signs were related to depression. Similarly, familial risk loading was related to psychomotor agitation, developmental motor delays, and dyscoordination in adolescents. In a prospective model, motor abnormalities predicted future symptoms. Collectively, these analyses suggest that motor abnormalities are sensitive to depression in adolescence[35] and may provide added benefits when combined with the traditional depression risk metrics (i.e., cognitive and affective measures).
All motor abnormalities were endorsed by some adolescents in this sample, but traditional motor measures had a notably low prevalence compared to other motor abnormalities. Developmental motor delays have been reported to have a similar prevalence (7%) [60] to the prevalence in the current sample (9.6%). Similarly, the rates of dyscoordination in the current study (19.25%) was similar to the rate of clinically assessed dyscoordination in previous adolescent studies (27.72%) [61] and populations studies of Canadian children (23%) [62]. Psychomotor agitation and psychomotor retardation among adolescents with a current depression diagnosis in the present study (0.3–3.2%; see SI) were substantially lower than the prevalence among adults with the diagnosis (34–63%) [11, 63–65]. This difference across development may suggest that motor abnormalities develop over the symptom course. Alternatively, psychomotor agitation and psychomotor retardation may be masked by neurodevelopmental processes, such that motor abnormalities become more salient in adulthood. Motor abnormalities may also take alternative forms in adolescence, as dyscoordination had a prevalence of 35.5% among depressed individuals, which was more consistent with the prevalence of adult motor disturbance[39, 40, 42, 66]. Traditional motor measures did, however, show high negative predictive value that may be useful to distinguish individuals without the diagnosis from a larger pool of potential patients. Concurrent symptoms also related to motor abnormalities, consistent with studies that have linked single motor measures to patient symptoms severity in adults[16, 23, 24, 38]. Additionally, supplemental analyses demonstrate that traditional motor metrics (psychomotor agitation and retardation) may have a less specific relationship to depression, as they relate to endorsements of psychomotor agitation, but novel motor measures (dyscoordination and motor milestones) did not show a similar relationship to social anxiety (SI). As a result, the addition of novel motor abnormalities, i.e., dyscoordination, increased sensitivity and specificity to disorder vulnerability beyond traditional measures.
Familial risk loading was related to the endorsement of psychomotor agitation, developmental motor delays, and dyscoordination; it had similar effect sizes to depression symptoms. Thus, motor abnormalities may not reflect the presence of depression alone, but a general depression vulnerability. These findings are consistent with motor abnormalities in infants, children, and adolescents with familial risk for depression[27, 36, 37, 67, 68], but build upon these findings by demonstrating the relevance of multiple motor metrics to familial risk loading in adolescence. However, it is notable that the current study is unable to disambiguate environmental from genetic influences, and more studies (e.g., GWAS, twin studies) are needed to test whether motor abnormalities are potential endophenotypes.
Endorsement of motor abnormalities at baseline predicted future depression symptoms independent of baseline depressive symptoms consistent with adult research[17, 27, 34, 38, 69]. These results provide convincing evidence for the clinical significance of motor abnormalities, even with a relatively short follow-up period of one year. Notably, the age of the sample at follow-up is earlier than the peak onset window for disorder[56], suggesting that motor abnormalities may connote early (and perhaps more chronic) risk for depression. In supplemental analyses[SI;17, 57–59], a discriminant function yielded similar accuracy as a previously published motor discriminant function in adult samples that discriminated healthy individuals from depression at follow-up[64]. Importantly, many of the motor abnormalities provided a unique predictive contribution to the model, suggesting that expanding motor measure may improve sensitivity to predicting future disorder onset and course. The variability of the motor abnormalities in terms of specificity and sensitivity to depression may explain why each motor measure showed an added benefit in classifying individuals as depressed. As a result, motor measurements, both traditional and novel, show promise as early markers of risk for disorder onset and course.
Generally, motor abnormalities were related to depression, but psychomotor retardation had a limited relationship to baseline familial risk, contrary to adult literature, which emphasizes the importance of psychomotor retardation[13, 23, 24, 32, 37, 70–77]. However, these studies often measure psychomotor retardation directly (e.g., actigraphy) rather than via self-reports, which may underestimate the prevalence of this symptom in the ABCD study. Psychomotor retardation did, however, show utility in predicting concurrent and future symptom course at one-year follow-up, highlighting its potential in clinical utility. These latter findings are consistent with reports that psychomotor retardation may highlight a subgroup of the most severe patients or only mark individuals at risk for severe course[17, 27, 34, 38, 69]. Taken together, psychomotor retardation may have limited utility as an early clinical vulnerability feature, but may connote risk for a more severe course and thus warrant early screening to identify those most in need of intervention.
The exact mechanisms of motor disturbance in depression are currently still debated. Some models suggest that hyperactivity in cortical structures, subgenual anterior cingulate cortex and basal lateral amygdala, signals the nucleus accumbens to drive a downregulation of dopamine input to cortical regions in the ventral tegmental area[10, 11, 29, 30]. This hypo-dopaminergic state leads to long-term decrease in dopaminergic gain, which may manifest as decreased volition, movement, and hedonics among other motoric, cognitive, and affective symptoms[30]. Some researchers suggest that reduced metabolism of catecholamine leads to psychomotor agitation type motor signs[11] or reduction of dopamine in particular leads to psychomotor retardation[11, 30]. Others propose that tuning of excitability of these circuits, in general[30] or among interneurons in particular[10], during development will result in motor, cognitive, and affective symptoms. This model suggests that motor signs may be a risk marker that may have sensitivity to depression risk alongside traditional cognitive and affective measures[11]. The current study provides support for this model and suggests that motor may provide additional sensitivity to emerging psychopathology in early adolescence.
Although the study had several notable strengths, it is important to note key limitations. First, these analyses may overestimate the sensitivity of psychomotor agitation and psychomotor retardation as they are included in the symptom sum. However, these motor signs were independent of the measure used to assess risk for this disorder, that also showed a comparable effect size. Second, all of the current motor behavior measures were single items, self-report of motor signs, limiting the sensitivity of motor measures (relative to controlled laboratory assessments) to ones that are salient to participants. This limitation is particularly notable as many motor behavioral measures are readily available, e.g., force variability, velocity scaling [13, 78]. Existing literature demonstrates that behavioral measures are more sensitive at identifying motor symptoms than observation or self-report measures alone [79, 80]. It is also notable that the motor items were included in both self- and parental-reports, and it is possible that parental-reports of motor milestone delays and dyscoordination were less stringent than self-reports of psychomotor slowing and agitation. However, it is also possible that the parental reports may be a more sensitive measure of dyscoordination as their assessment reflects a number of observations of this phenomenon in several of contexts. Additionally, parental report of abnormalities may be biased by parental psychopathology or concerns regarding psychopathology in the child. Next, it is notable that the small effect sizes and test characteristics suggest that self- and parental-reports of motor behavior alone will not be sufficient to assess risk for depression. Instead, motor may confer some additional benefit as a part of a larger risk battery. However, the current effect sizes (Odds Ratios: 1.40–2.41) are within a similar range to other risk markers of depression [81] including: genome wide associations of depression (OR=1.35)[82], single nucleotide polymorphisms/single candidate genes (OR=1.15)[82], severe irritability (OR=1.33)[83], and current parental depression (maternal OR=1.99; paternal OR=1.45)[53]. Finally, although depression in the current paper is treated as a singular outcome, we recognize that the depression is heterogeneous that reflects a number of complex profiles. Future studies should consider examining the specific features of depression rather than aggregating over this heterogenous group.
In conclusion, motor abnormalities show promise as an early marker of vulnerability to depression, as these markers (a) discriminated between individuals with depression and the general population, (b) predicted familial risk loading and (c) prospectively predicted worsening symptoms and onset. This study also demonstrated the utility of expanding motor abnormality metrics beyond psychomotor agitation and psychomotor retardation to increase the sensitivity to a broader set of more developmentally relevant motor issues, including developmental motor delays and dyscoordination.
Supplementary Material
Figure 1. Effect Size of Motor Abnormalities by Current Depression Symptoms and Depression Familial Vulnerability Measures.
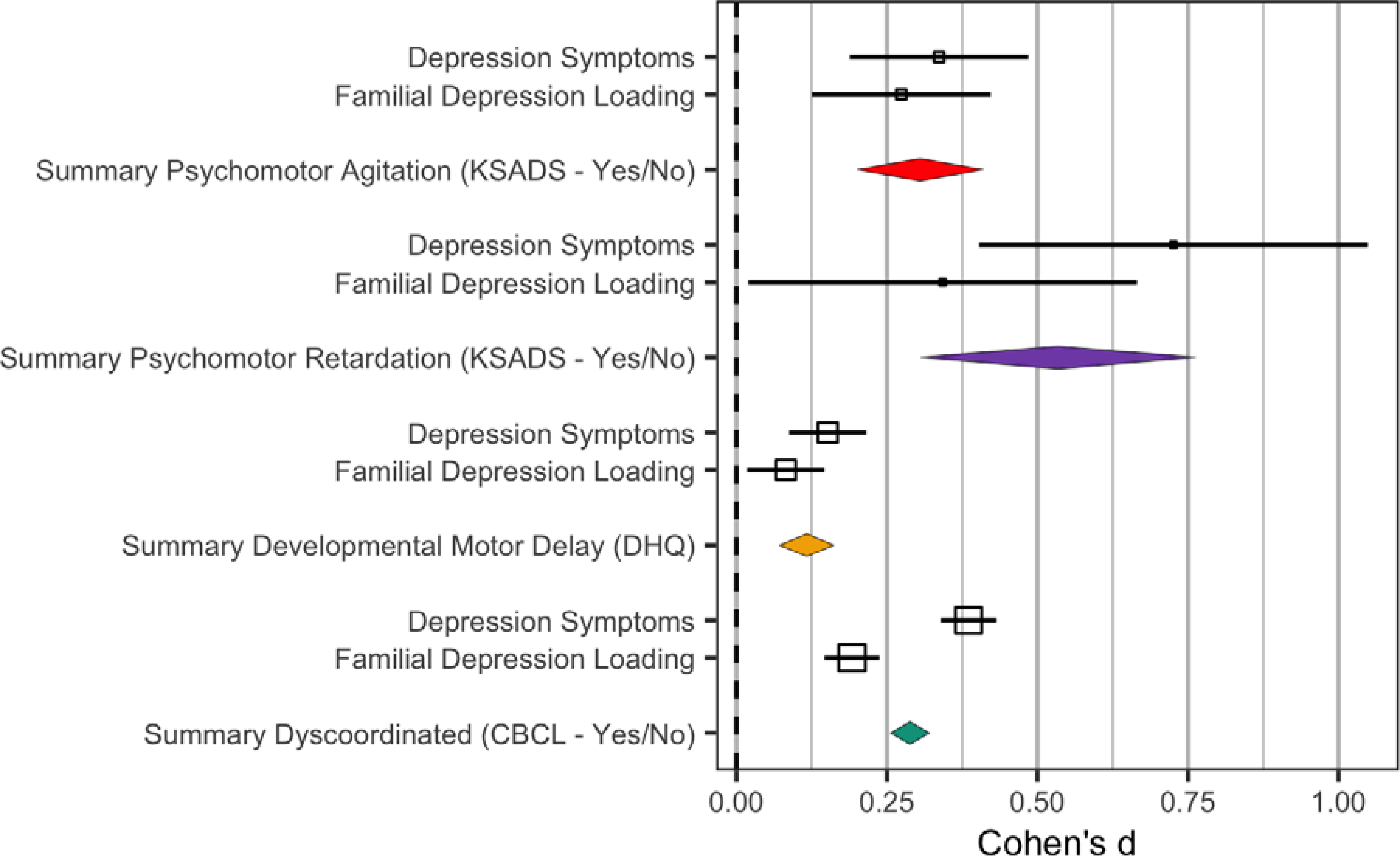
Psychomotor Agitation- Green, Psychomotor Retardation -Yellow, Developmental Motor Delays – Red, Dyscoordination Symptoms -Purple; Effect Sizes above were transformed into calculated in raw, not model-corrected data; Odds Ratios (see Table 2) and standard error were transformed to Cohen’s d using the Michaela package in R; Error bars reflect the standard error; Effect sizes were converted to common values using the R Michaela package [84] and visualized with the metaviz package [85].
Figure 2. Effect Size of Motor Abnormalities at baseline on Depression at 1-Year Follow-Up.
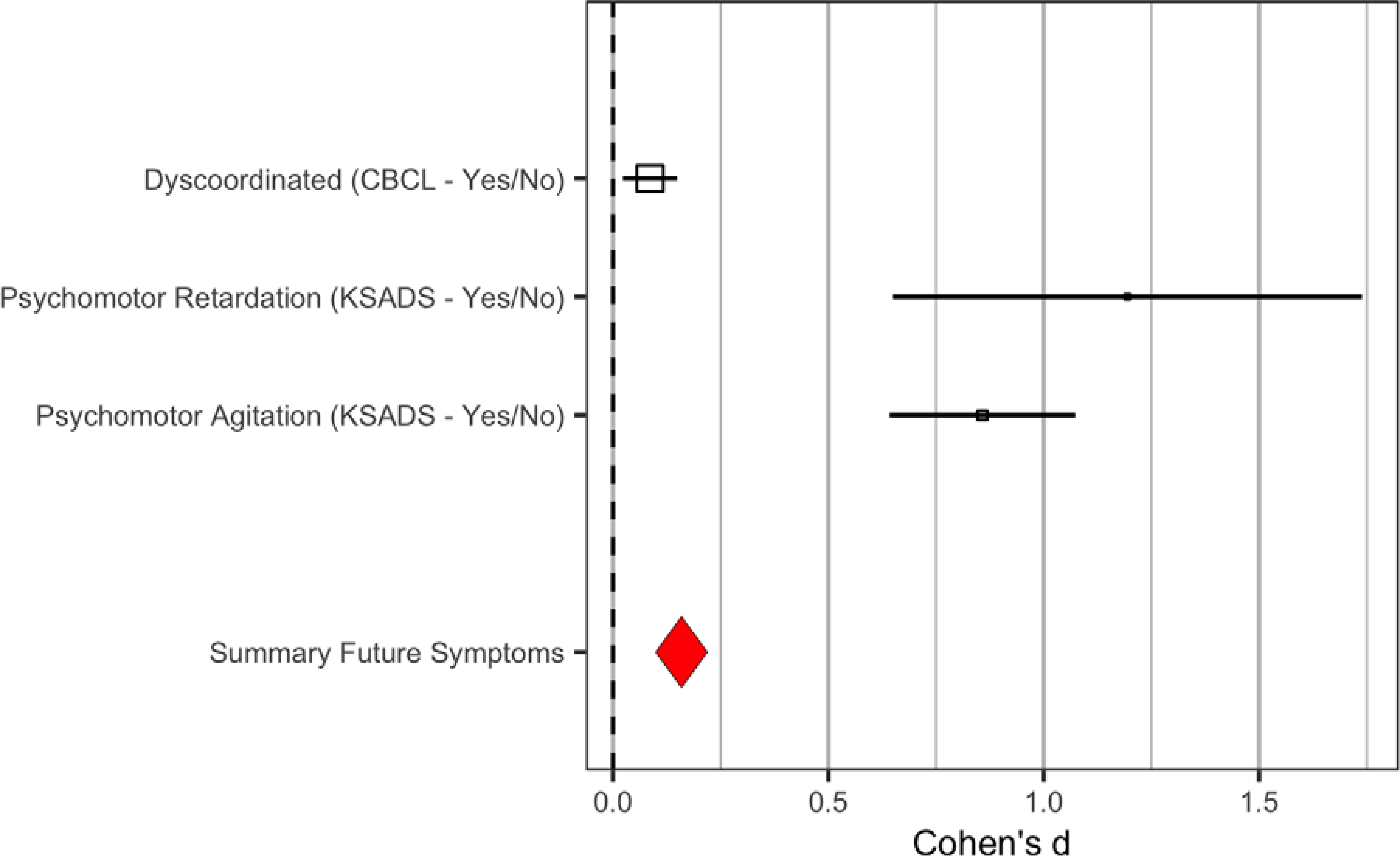
Effect Sizes above are raw, not model-corrected data; Odds Ratios (see Table 2) and standard error were calculated using the Michaela package in R; Error bars reflect the standard error; Effect sizes were converted to common values using the R Michaela package [84] and visualized with the metaviz package [85].
Acknowledgments
This work was supported by the National Institutes of Mental Health (VAM Grant R01MH094650, R01MH112545–01, R01MH103231, R01MH112545, R01MH094650, R01MH118741, R21/R33MH103231; SW Grant Swiss National Science Foundation grants 182469, 184717). Data used in the preparation of this work were obtained from the Adolescent Brain Cognitive Development (ABCD) Study (https://abcdstudy.org), held in the NIMH Data Archive (NDA). This is a multisite, longitudinal study designed to recruit more than 10,000 children age 9–10 and follow them over ten years into early adulthood. The ABCD Study is supported by the National Institutes of Health and additional federal partners under award numbers U01DA041022, U01DA041028, U01DA041048, U01DA041089, U01DA041106, U01DA041117, U01DA041120, U01DA041134, U01DA041148, U01DA041156, U01DA041174, U24DA041123, U24DA041147, U01DA041093, and U01DA041025. A full list of supporters is available at https://abcdstudy.org/federal-partners.html. A listing of participating sites and a complete listing of the study investigators can be found at https://abcdstudy.org/Consortium_Members.pdf. ABCD consortium investigators designed and implemented the study and/or provided data but did not necessarily participate in the analysis or writing of this report. This manuscript reflects the views of the authors and may not reflect the opinions or views of the NIH or ABCD consortium investigators. The ABCD data repository grows and changes over time. DOIs can be found at https://nda.nih.gov/generalquery.html?q=query=studies%20%7Eand%7E%20orderBy=id%20%7Eand%7E%20orderDirection=Ascending.
Footnotes
COMPETING INTERESTS STATEMENT: Authors have no competing interests to disclose related to the current paper, but would like to disclose an unrelated, honoraria that was awarded to Sebastian Walther from Lundbeck, Janssen, and Sunovion.
References
- 1.Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1789–1858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Collins KA, Westra HA, Dozois DJA, Burns DD. Gaps in accessing treatment for anxiety and depression: Challenges for the delivery of care. Clinical Psychology Review. 2004;24:583–616. [DOI] [PubMed] [Google Scholar]
- 3.Tolin DF. Is cognitive–behavioral therapy more effective than other therapies?: A meta-analytic review. Clinical Psychology Review. 2010;30:710–720. [DOI] [PubMed] [Google Scholar]
- 4.Harrington R, Clark A. Prevention and early intervention for depression in adolescence and early adult life. European Archives of Psychiatry and Clinical Neurosciences. 1998;248:32–45. [DOI] [PubMed] [Google Scholar]
- 5.Avenevoli S, Merikangas KR. Implications of High-Risk Family Studies for Prevention of Depression. American Journal of Preventive Medicine. 2006;31:126–135. [DOI] [PubMed] [Google Scholar]
- 6.Pelkonen M, Marttunen M, Aro H. Risk for depression: a 6-year follow-up of Finnish adolescents. Journal of Affective Disorders. 2003;77:41–51. [DOI] [PubMed] [Google Scholar]
- 7.Dobson KS, Dozois DJA. Chapter 1 - Introduction: Assessing Risk and Resilience Factors in Models of Depression. In: Dobson KS, Dozois DJA, editors. Risk Factors in Depression, San Diego: Elsevier; 2008. p. 1–16. [Google Scholar]
- 8.Thapar A, Collishaw S, Pine DS, Thapar AK. Depression in adolescence. The Lancet. 2012;379:1056–1067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.The American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. vol. 5. [Google Scholar]
- 10.Grace AA. Dysregulation of the dopamine system in the pathophysiology of schizophrenia and depression. Nat Rev Neurosci. 2016;17:524–532. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Sobin C, Sackeim HA. Psychomotor Symptoms of Depression. Am J Psychiatry. 1997;154:4–17. [DOI] [PubMed] [Google Scholar]
- 12.Schrijvers D, Hulstijn W, Sabbe BGC. Psychomotor symptoms in depression: a diagnostic, pathophysiological and therapeutic tool. J Affect Disord. 2008;109:1–20. [DOI] [PubMed] [Google Scholar]
- 13.Shankman SA, Mittal VA, Walther S. An Examination of Psychomotor Disturbance in Current and Remitted MDD: An RDoC Study. J Psychiatr Brain Sci. 2020;5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sices L Use of Developmental Milestones in Pediatric Residency Training and Practice: Time to Rethink the Meaning of the Mean. J Dev Behav Pediatr. 2007;28:47–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Damme TV, Simons J, Sabbe B, van West D. Motor abilities of children and adolescents with a psychiatric condition: A systematic literature review. World J Psychiatry. 2015;5:315–329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.van Os J, Jones P, Lewis G, Wadsworth M, Murray R. Developmental Precursors of Affective Illness in a General Population Birth Cohort. Arch Gen Psychiatry. 1997;54:625–631. [DOI] [PubMed] [Google Scholar]
- 17.Emck C, Bosscher RJ, Wieringen PCV, Doreleijers T, Beek PJ. Gross motor performance and physical fitness in children with psychiatric disorders. Developmental Medicine & Child Neurology. 2011;53:150–155. [DOI] [PubMed] [Google Scholar]
- 18.Walker EF. Developmentally Moderated Expressions of the Neuropathology Underlying Schizophrenia. Schizophr Bull. 1994;20:453–480. [DOI] [PubMed] [Google Scholar]
- 19.Mittal VA, Bernard JA, Northoff G. What Can Different Motor Circuits Tell Us About Psychosis? An RDoC Perspective. Schizophr Bull. 2017;43:949–955. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Mittal VA, Walker EF. Movement abnormalities predict conversion to Axis I psychosis among prodromal adolescents. Journal of Abnormal Psychology. 2007;116:796–803. [DOI] [PubMed] [Google Scholar]
- 21.Mittal VA, Tessner KD, McMillan AL, Delawalla Z, Trotman HD, Walker EF. Gesture behavior in unmedicated schizotypal adolescents. J Abnorm Psychol. 2006;115:351–358. [DOI] [PubMed] [Google Scholar]
- 22.Mittal VA, Hasenkamp W, Sanfilipo M, Wieland S, Angrist B, Rotrosen J, et al. Relation of neurological soft signs to psychiatric symptoms in schizophrenia. Schizophrenia Research. 2007;94:37–44. [DOI] [PubMed] [Google Scholar]
- 23.Finazzi ME, Mesquita ME, Lopes JR, Fu I L, Oliveira MG, Del Porto JA. Motor Activity and Depression Severity in Adolescent Outpatients. 2010. 2010. [DOI] [PubMed] [Google Scholar]
- 24.O’Brien JT, Gallagher P, Stow D, Hammerla N, Ploetz T, Firbank M, et al. A study of wrist-worn activity measurement as a potential real-world biomarker for late-life depression. Psychological Medicine. 2017;47:93–102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Vares EA, Salum GA, Spanemberg L, Caldieraro MA, Fleck MP. Depression Dimensions: Integrating Clinical Signs and Symptoms from the Perspectives of Clinicians and Patients. PLoS One. 2015;10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.van de Leemput IA, Wichers M, Cramer AOJ, Borsboom D, Tuerlinckx F, Kuppens P, et al. Critical slowing down as early warning for the onset and termination of depression. PNAS. 2014;111:87–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Leventhal AM, Pettit JW, Lewinsohn PM. Characterizing major depression phenotypes by presence and type of psychomotor disturbance in adolescents and young adults. Depression and Anxiety. 2008;25:575–592. [DOI] [PubMed] [Google Scholar]
- 28.Mittal VA, Wakschlag LS. Research Domain Criteria (RDoC) Grows Up: Strengthening Neurodevelopmental Investigation within the RDoC Framework. J Affect Disord. 2017;216:30–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Obeso JA, Rodriguez-Oroz MC, Stamelou M, Bhatia KP, Burn DJ. The expanding universe of disorders of the basal ganglia. The Lancet. 2014;384:523–531. [DOI] [PubMed] [Google Scholar]
- 30.Robison AJ, Thakkar KN, Diwadkar VA. Cognition and Reward Circuits in Schizophrenia: Synergistic, Not Separate. Biol Psychiatry. 2020;87:204–214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Cullen KR, Gee DG, Klimes-Dougan B, Gabbay V, Hulvershorn L, Mueller BA, et al. A preliminary study of functional connectivity in comorbid adolescent depression. Neuroscience Letters. 2009;460:227–231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Sanders JB, Bremmer MA, Comijs HC, Deeg DJH, Beekman ATF. Gait Speed and the Natural Course of Depressive Symptoms in Late Life; An Independent Association With Chronicity? Journal of the American Medical Directors Association. 2016;17:331–335. [DOI] [PubMed] [Google Scholar]
- 33.Ulbricht CM, Dumenci L, Rothschild AJ, Lapane KL. Changes in Depression Subtypes Among Men in STAR*D: A Latent Transition Analysis. Am J Mens Health. 2018;12:5–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Ulbricht CM, Rothschild AJ, Lapane KL. Functional Impairment and Changes in Depression Subtypes for Women in STAR*D: A Latent Transition Analysis. Journal of Women’s Health. 2015;25:464–472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Beauchaine TP, Constantino JN. Redefining the endophenotype concept to accommodate transdiagnostic vulnerabilities and etiological complexity. Biomark Med. 2017;11:769–780. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Cornish AM, McMahon CA, Ungerer JA, Barnett B, Kowalenko N, Tennant C. Postnatal depression and infant cognitive and motor development in the second postnatal year: The impact of depression chronicity and infant gender. Infant Behavior and Development. 2005;28:407–417. [Google Scholar]
- 37.Vameghi R, Akbari SAA, Sajjadi H, Sajedi F, Alavimajd H. Correlation Between Mothers’ Depression and Developmental Delay in Infants Aged 6–18 Months. Glob J Health Sci. 2016;8:11–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Colman I, Ploubidis GB, Wadsworth MEJ, Jones PB, Croudace TJ. A Longitudinal Typology of Symptoms of Depression and Anxiety Over the Life Course. Biological Psychiatry. 2007;62:1265–1271. [DOI] [PubMed] [Google Scholar]
- 39.Campbell WN, Missiuna C, Vaillancourt T. Peer victimization and depression in children with and without motor coordination difficulties. Psychology in the Schools. 2012;49:328–341. [Google Scholar]
- 40.Draghi TTG, Cavalcante Neto JL, Tudella E. Symptoms of anxiety and depression in schoolchildren with and without developmental coordination disorder. J Health Psychol. 2019:1359105319878253. [DOI] [PubMed] [Google Scholar]
- 41.Poole KL, Schmidt LA, Missiuna C, Saigal S, Boyle MH, Van Lieshout RJ. Childhood motor coordination and adult psychopathology in extremely low birth weight survivors. Journal of Affective Disorders. 2016;190:294–299. [DOI] [PubMed] [Google Scholar]
- 42.Hill EL, Brown D. Mood impairments in adults previously diagnosed with developmental coordination disorder. Journal of Mental Health. 2013;22:334–340. [DOI] [PubMed] [Google Scholar]
- 43.Owoeye O, Kingston T, Scully PJ, Baldwin P, Browne D, Kinsella A, et al. Epidemiological and Clinical Characterization Following a First Psychotic Episode in Major Depressive Disorder: Comparisons With Schizophrenia and Bipolar I Disorder in the Cavan-Monaghan First Episode Psychosis Study (CAMFEPS). Schizophrenia Bulletin. 2013;39:756–765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Raballo A, Poletti M. Advances in early identification of children and adolescents at risk for psychiatric illness. Current Opinion in Psychiatry. 2020;33:611–617. [DOI] [PubMed] [Google Scholar]
- 45.Goldstone A, Javitz HS, Claudatos SA, Buysse DJ, Hasler BP, de Zambotti M, et al. Sleep Disturbance Predicts Depression Symptoms in Early Adolescence: Initial Findings From the Adolescent Brain Cognitive Development Study. Journal of Adolescent Health. 2020;66:567–574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Gray JC, Schvey NA, Tanofsky-Kraff M. Demographic, psychological, behavioral, and cognitive correlates of BMI in youth: Findings from the Adolescent Brain Cognitive Development (ABCD) study. Psychological Medicine. 2020;50:1539–1547. [DOI] [PubMed] [Google Scholar]
- 47.Gorham LS, Barch DM. White Matter Tract Integrity, Involvement in Sports, and Depressive Symptoms in Children. Child Psychiatry Hum Dev. 2020. 25 January 2020. 10.1007/s10578-020-00960-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Karcher NR, Barch DM. The ABCD study: understanding the development of risk for mental and physical health outcomes. Neuropsychopharmacology. 2021;46:131–142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Hoffman EA, Clark DB, Orendain N, Hudziak J, Squeglia LM, Dowling GJ. Stress exposures, neurodevelopment and health measures in the ABCD study. Neurobiology of Stress. 2019;10:100157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Assari S, Boyce S, Bazargan M, Caldwell CH. African Americans’ Diminished Returns of Parental Education on Adolescents’ Depression and Suicide in the Adolescent Brain Cognitive Development (ABCD) Study. European Journal of Investigation in Health, Psychology and Education. 2020;10:656–668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Mennies RJ, Birk SL, Norris LA, Olino TM. The Main and Interactive Associations between Demographic Factors and Psychopathology and Treatment Utilization in Youth: A Test of Intersectionality in the ABCD Study. J Abnorm Child Psychol. 2020. 31 July 2020. 10.1007/s10802-020-00687-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Cai Y, Elsayed N, Barch D. Contributions from resting state functional connectivity and familial risk to early adolescent-onset MDD: Results from the Adolescent Brain Cognitive Development study. PsyArXiv; 2020. [DOI] [PubMed] [Google Scholar]
- 53.Pagliaccio D, Alqueza KL, Marsh R, Auerbach RP. Brain Volume Abnormalities in Youth at High Risk for Depression: Adolescent Brain and Cognitive Development Study. Journal of the American Academy of Child & Adolescent Psychiatry. 2019. 18 October 2019. 10.1016/j.jaac.2019.09.032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Palmer CE, Loughnan RJ, Makowski C, Thompson W, Barch D, Jernigan T, et al. Delineating genetic and familial risk for psychopathology in the ABCD study. MedRxiv. 2020:2020.09.08.20186908. [Google Scholar]
- 55.Funkhouser CJ, Chacko AA, Correa KA, Kaiser AJE, Shankman SA. Unique longitudinal relationships between symptoms of psychopathology in youth: A cross-lagged panel network analysis in the ABCD study. Journal of Child Psychology and Psychiatry. 2020. 2020. 10.1111/jcpp.13256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime Prevalence and Age-of-Onset Distributions of DSM-IV Disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62:593. [DOI] [PubMed] [Google Scholar]
- 57.Kaufman J, Birmaher B, Brent DA, Ryan ND, Rao U. K-SADS-PL. Journal of the American Academy of Child & Adolescent Psychiatry. 2000;39:1208–1208. [DOI] [PubMed] [Google Scholar]
- 58.Rice JP, Reich T, Bucholz KK, Neurnan RJ, Fishman R, Rochberg N, et al. Comparison of Direct Interview and Family History Diagnoses of Alcohol Dependence. 1995. [DOI] [PubMed] [Google Scholar]
- 59.Ranganathan P, Aggarwal R. Common pitfalls in statistical analysis: Understanding the properties of diagnostic tests – Part 1. Perspect Clin Res. 2018;9:40–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Valla L, Wentzel-Larsen T, Hofoss D, Slinning K. Prevalence of suspected developmental delays in early infancy: results from a regional population-based longitudinal study. BMC Pediatrics. 2015;15:215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Sittiprapaporn P Motor Skills Performance of Children. Learning Disabilities, BoD – Books on Demand; 2012. p. 217–238. [Google Scholar]
- 62.Kirby A Overlapping Conditions: Overlapping Conditions Management: Services for individuals with developmental coordination disorder. Children With Developmental Coordination Disorder, London: Wiley. p. 242–265. [Google Scholar]
- 63.Bryan CJ, Songer TJ, Brooks MM, Thase ME, Gaynes BN, Klinkman M, et al. A comparison of baseline sociodemographic and clinical characteristics between major depressive disorder patients with and without diabetes: A STAR⁎D report. Journal of Affective Disorders. 2008;108:113–120. [DOI] [PubMed] [Google Scholar]
- 64.Caligiuri MP, Ellwanger J. Motor and cognitive aspects of motor retardation in depression. Journal of Affective Disorders. 2000;57:83–93. [DOI] [PubMed] [Google Scholar]
- 65.Parker G, Hadzi-Pavlovic D, Brodaty H, Boyce P, Mitchell P, Wilhelm K, et al. Psychomotor disturbance in depression: defining the constructs. Journal of Affective Disorders. 1993;27:255–265. [DOI] [PubMed] [Google Scholar]
- 66.Zhao Q, Ma Y, Lui SSY, Liu W, Xu T, Yu X, et al. Neurological soft signs discriminate schizophrenia from major depression but not bipolar disorder. Progress in Neuro-Psychopharmacology and Biological Psychiatry. 2013;43:72–78. [DOI] [PubMed] [Google Scholar]
- 67.Mehler-Wex C, Kölch M. Depression in Children and Adolescents. Dtsch Arztebl Int. 2008;105:149–155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Kounali D, Zammit S, Wiles N, Sullivan S, Cannon M, Stochl J, et al. Common versus psychopathology-specific risk factors for psychotic experiences and depression during adolescence. Psychological Medicine. 2014;44:2557–2566. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Fried EI, Nesse RM. Depression is not a consistent syndrome: An investigation of unique symptom patterns in the STAR*D study. Journal of Affective Disorders. 2015;172:96–102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Walther S, Höfle O, Federspiel A, Horn H, Hügli S, Wiest R, et al. Neural correlates of disbalanced motor control in major depression. Journal of Affective Disorders. 2012;136:124–133. [DOI] [PubMed] [Google Scholar]
- 71.Cantisani A, Stegmayer K, Bracht T, Federspiel A, Wiest R, Horn H, et al. Distinct resting-state perfusion patterns underlie psychomotor retardation in unipolar vs. bipolar depression. Acta Psychiatrica Scandinavica. 2016;134:329–338. [DOI] [PubMed] [Google Scholar]
- 72.Matthews K, Coghill D, Rhodes S. Neuropsychological functioning in depressed adolescent girls. Journal of Affective Disorders. 2008;111:113–118. [DOI] [PubMed] [Google Scholar]
- 73.Reichert M, Lutz A, Deuschle M, Gilles M, Hill H, Limberger MF, et al. Improving Motor Activity Assessment in Depression: Which Sensor Placement, Analytic Strategy and Diurnal Time Frame Are Most Powerful in Distinguishing Patients from Controls and Monitoring Treatment Effects. PLoS One. 2015;10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Krane-Gartiser K, Henriksen TEG, Vaaler AE, Fasmer OB, Morken G. Actigraphically assessed activity in unipolar depression: a comparison of inpatients with and without motor retardation. The Journal of Clinical Psychiatry. 2015;76:1181–1187. [DOI] [PubMed] [Google Scholar]
- 75.Bracht T, Federspiel A, Schnell S, Horn H, Höfle O, Wiest R, et al. Cortico-Cortical White Matter Motor Pathway Microstructure Is Related to Psychomotor Retardation in Major Depressive Disorder. PLoS One. 2012;7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Razavi N, Horn H, Koschorke P, Hügli S, Höfle O, Müller T, et al. Measuring motor activity in major depression: The association between the Hamilton Depression Rating Scale and actigraphy. Psychiatry Research. 2011;190:212–216. [DOI] [PubMed] [Google Scholar]
- 77.Stange JP, Zulueta J, Langenecker SA, Ryan KA, Piscitello A, Duffecy J, et al. Let Your Fingers Do the Talking: Passive Typing Instability Predicts Future Mood Outcomes. Bipolar Disord. 2018;20:285–288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Damme KSF, Osborne KJ, Gold JM, Mittal VA. Detecting motor slowing in clinical high risk for psychosis in a computerized finger tapping model. Eur Arch Psychiatry Clin Neurosci. 2020;270:393–397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Cortese L, Caligiuri MP, Malla AK, Manchanda R, Takhar J, Haricharan R. Relationship of neuromotor disturbances to psychosis symptoms in first-episode neuroleptic-naïve schizophrenia patients. Schizophrenia Research. 2005;75:65–75. [DOI] [PubMed] [Google Scholar]
- 80.van Harten PN, Walther S, Kent JS, Sponheim SR, Mittal VA. The clinical and prognostic value of motor abnormalities in psychosis, and the importance of instrumental assessment. Neuroscience & Biobehavioral Reviews. 2017;80:476–487. [DOI] [PubMed] [Google Scholar]
- 81.Funder DC, Ozer DJ. Evaluating Effect Size in Psychological Research: Sense and Nonsense. Advances in Methods and Practices in Psychological Science. 2019;2:156–168. [Google Scholar]
- 82.Flint J, Kendler KS. The Genetics of Major Depression. Neuron. 2014;81:484–503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Stringaris A, Cohen P, Pine DS, Leibenluft E. Adult Outcomes of Youth Irritability: A 20-Year Prospective Community-Based Study. Am J Psychiatry. 2009;166:1048–1054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Lam PH, Chiang JJ. michaela—open r package for converting effect sizes. [Google Scholar]
- 85.Schild AHE, Voracek M. Finding your way out of the forest without a trail of bread crumbs: development and evaluation of two novel displays of forest plots. Research Synthesis Methods. 2015;6:74–86. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.