

Abstract
Technological advances in both genome sequencing and prenatal imaging are increasing our ability to accurately recognize and diagnose Mendelian conditions prenatally. Phenotype-driven early genetic diagnosis of fetal genetic disease can help to strategize treatment options and clinical preventive measures during the perinatal period, to plan in utero therapies, and to inform parental decision-making. Fetal phenotypes of genetic diseases are often unique and at present are not well understood; more comprehensive knowledge about prenatal phenotypes and computational resources have an enormous potential to improve diagnostics and translational research. The Human Phenotype Ontology (HPO) has been widely used to support diagnostics and translational research in human genetics. To better support prenatal usage, the HPO consortium conducted a series of workshops with a group of domain experts in a variety of medical specialties, diagnostic techniques, as well as diseases and phenotypes related to prenatal medicine, including perinatal pathology, musculoskeletal anomalies, neurology, medical genetics, hydrops fetalis, craniofacial malformations, cardiology, neonatal-perinatal medicine, fetal medicine, placental pathology, prenatal imaging, and bioinformatics. We expanded the representation of prenatal phenotypes in HPO by adding 95 new phenotype terms under the Abnormality of prenatal development or birth (HP:0001197) grouping term, and revised definitions, synonyms, and disease annotations for most of the 152 terms that existed before the beginning of this effort. The expansion of prenatal phenotypes in HPO will support phenotype-driven prenatal exome and genome sequencing for precision genetic diagnostics of rare diseases to support prenatal care.
Keywords: Human Phenotype Ontology, HPO, Prenatal phenotyping, Phenopacket, Prenatal diagnosis, Fetal pathology
Introduction
Genetic diagnosis can define fetal prognosis, inform parental decision-making, and guide clinical management during pregnancy and the perinatal period. Congenital anomalies affect 2–4% of all infants and are responsible for 20% of perinatal deaths [Osterman et al., 2015]. The most recent systematic review of prenatal genomic testing with Exome Sequencing (ES) and/or Genome Sequencing (GS), identified 72 reports from 66 studies involving 4350 fetuses with a pooled diagnostic yield of 31% [Mellis et al., 2022]. This represents a compelling justification for the adoption of genomic diagnostics into fetal medicine, but there is still significant room for improvement to facilitate clinical use.
The Human Phenotype Ontology (HPO) is a rich representation of abnormal human phenotypic features including signs, symptoms, laboratory test results, imaging findings, and others. HPO is logically structured as an ontology and enables sophisticated algorithms that support combined genomic and phenotypic analysis in diverse clinical and research applications. Examples include genomic interpretation for diagnostics, gene-disease discovery, mechanism discovery, and Electronic Health Record (EHR) cohort analytics – all of which assist in realizing the promise of precision medicine [Haendel et al., 2018]. The HPO development team has developed free and open community resources consisting of the ontology itself and a comprehensive corpus of phenotype annotations (HPOA) corresponding to each of over 8,400 rare diseases. HPO has become a global standard for the International Rare Disease Research Consortium (IRDiRC) [Lochmüller et al., 2017] and has been translated into more than 10 languages for use in rare disease diagnostic tools [Köhler et al., 2018]. Almost all clinical genetics diagnostic tools now leverage the HPO to encode and compute over patient features in the context of genomic variant classification. Further, by enabling data exchange, HPO unites an ever-growing community of diverse users and contributors across the world, illuminating the natural history of disease, revealing new diseases, supporting patient registries and n-of-1 matchmaking for diagnosis, as well as numerous national genomic initiatives including the 100,000 Genomes Project, the NIH Undiagnosed Diseases Program and Network, the Deciphering Developmental Disorders study, and biobanking programs [Robinson et al., 2008; Köhler et al., 2021]. It has also supported the discovery of genes associated with both previously known and novel human diseases by comparing HPO terms and those of the Mammalian Phenotype Ontology (MP) [Cacheiro et al., 2020; Oellrich et al., 2012].
Accurate and comprehensive phenotyping matters for accurate diagnosis. Many ES and GS pipelines incorporate phenotype analysis into approaches for ranking and interpreting variants, and having a standardized computational resource such as HPO is key to sharing and analyzing both prenatal and postnatal features. Since its inception in 2008, the majority of work on the HPO has been dedicated to describing phenotypes observed postnatally. With the advent of sophisticated methods for prenatal phenotyping and recent successes in the application of next-generation sequencing including ES and GS, an opportunity has arisen to apply HPO-based, phenotype-driven, genomic analysis to prenatal sequencing. For this reason, a group of specialists in multiple disciplines related to prenatal medicine came together over a period of two years to extend HPO resources to better cover the prenatal phenotype. This article describes the result of this work and provides guidelines for using HPO for prenatal phenotyping.
Prenatal phenotyping
Common non-invasive prenatal evaluations in the first trimester include first trimester screening (FTS), non-invasive prenatal testing (NIPT) on cell-free DNA (cfDNA) in maternal serum, and ultrasound for nuchal translucency (NT) measurement and morphological assessment of the fetus. As screening tests, these are designed to identify women with pregnancies at high risk for chromosomal and genetic conditions and congenital anomalies [Carlson and Vora, 2017]. The FTS for aneuploidy risk assessment generally comprises a multiparameter algorithm including maternal age, serum screening (usually pregnancy-associated plasma protein A and free beta-human chorionic gonadotropin), and ultrasonographic measurement of the NT and the crown-rump length (CRL) performed between 11 weeks and 13 weeks 6 days gestational age [Salomon et al., 2013].
The morphological assessment of the fetus is based on ultrasound examination. High resolution ultrasound can potentially detect the majority of severe or lethal fetal structural anomalies in the first trimester scan [Blaas, 2014; Rossi and Prefumo, 2013]. In most countries, a 2nd trimester detailed anomaly scan between 18–22 weeks’ gestation (WG) is standard of care, and with the advances of high resolution ultrasound technologies, it allows detection of the majority of fetal anomalies and assessment of the fetal phenotype at this developmental stage with high precision. Resources available for following up on potentially abnormal findings continue to improve and additional modalities, including magnetic resonance imaging (MRI), computerized tomography (CT-Scan), and 3D/4D ultrasound, are entering the prenatal imaging space [Gray et al., 2019]. The catalog of prenatal phenotypes in HPO, therefore, needs to be extended to include data from these modalities.
There are a number of challenges to fetal phenotypic assessment. Prenatal phenotypes are generally less well characterized than postnatal phenotypes; further, there is a clear difficulty in identifying some organs in the prenatal period (e.g. the skin) and some anatomical structures change significantly in the postnatal period (e.g. the lungs, the cardiovascular system). Fetal phenotypes are observed indirectly by imaging modalities and the clinical information inferred from prenatal imaging is sparse in comparison with that obtained through clinical, behavioral, functional, and pathological phenotyping of the infant after delivery [Filges and Friedman, 2015]. It is substantially more difficult and in some cases impossible in the prenatal period to assess functional anomalies such as seizures, developmental delay, or hearing loss. This is reflected in our assessment that only about 10% of HPO terms are identifiable through imaging modalities in the prenatal setting. A review of HPO terms with a focus on their “identifiability” during prenatal life has confirmed that only a minority are detectable with high sensitivity. Therefore, fetal phenotypes may differ from those classically associated with a newborn, child or adult with the same genetic condition. In addition, a significant proportion of abnormal phenotypes encountered during the antenatal developmental stages may be specific to fetal life since they will lead to embryonic, fetal or perinatal lethality and will have escaped etiological research and clinical delineation so far. This is epitomized by fetal Noonan syndrome where, in the second trimester fetus, pleural effusions and polyhydramnios are common, and the typical pulmonic stenosis is not easily ascertained [Scott et al., 2021]. This was also noted in a cohort of 246 stillborn probands evaluated using ES in which there was an enrichment of loss of function (LOF) variants in genes intolerant to such variation in humans; the LOF variants were was concentrated in genes not previously associated with human disease and 44% of the candidate genes were embryonic lethal in mice [Stanley et al., 2020]. Fetal phenotypes may also represent an incomplete or severe allelic presentation of a phenotype described to occur postnatally, and the diagnosis therefore can remain unrecognized at this stage of development [Filges and Friedman, 2015]. Recent studies on GS/ES amongst sick infants in ICU showed that in a significant proportion of cases an abnormal prenatal phenotype would not be expected in cases where a genomic etiology was identified postnatally [Kingsmore et al., 2019; Meng et al., 2017].
Fetal phenotypes may also evolve over time since the occurrence of symptoms may be specific to the developmental stage [Mone et al., 2021a]. New phenotypes can be observed with increasing gestational age, and phenotypes can resolve (i.e., cystic hygromas or hydrops fetalis may resolve) even in the presence of an underlying genetic disease. A recently published systematic review has shown that during routine third-trimester ultrasound, an incidental fetal anomaly will be found in about 1 in 300 scanned women. This not only includes anomalies missed at the earlier 20 weeks scan but also abnormalities that can only be seen with fetal maturation, such as certain malformations of cortical development, microcephaly, or hydrocephalus; some congenital heart defects; gastrointestinal abnormalities relating to intestinal obstruction; urinary tract abnormalities that change over time such as renal pelvis dilatation; and some skeletal dysplasias [Drukker et al., 2021]. Tracking and real-time updating of the fetal phenotype in combination with the application of genomic testing in prenatal diagnosis has become an active field of research. As a consequence, HPO can support this effort by curation of prenatal phenotypes as available. For example, a finding in the fetal period may sometimes suggest a specific disease and the same finding in a child or adult may not be related to the same disease. This is the case of cardiac rhabdomyomas: when observed in the fetal age they suggest the diagnosis of tuberous sclerosis but when observed in teenagers or adults, alternative diagnoses are more likely [Boitor Borza et al., 2022].
In summary, fetal phenotypes of genetic diseases are often unique and at present are not well understood. We lack knowledge of the natural history of most genetic diseases in the prenatal period. Certain manifestations can occur prenatally but resolve or evolve postnatally. For instance, fetal effusions, polyhydramnios, and contractures can be prenatal manifestations of RASopathies but are not postnatal features of these diseases. In order to extend our understanding of these diseases and their prenatal manifestations, it is essential to create HPO resources to allow comprehensive and precise computational models of fetal phenotypes and to link these features to fetal manifestations of disease.
Prenatal genetic and genomic diagnosis (PD).
In contrast to screening approaches, PD provides diagnostic information as to the etiology and prognosis as well as informing pregnancy, perinatal and neonatal decision-making and management. Fetal aneuploidy and unbalanced chromosomal rearrangements can be identified in about 35% of structurally abnormal fetuses, and chromosomal microarray (CMA) analysis identifies copy number variants in an additional 3–6.5% of cases [Hillman et al., 2013; Wapner et al., 2012]. Altogether, these tests identify a genetic etiology in up to 40% of abnormal fetuses. Until recently, published experience on the diagnostic yield of prenatal ES/GS was limited to relatively small cohorts but suggested the ability of ES/GS to diagnose monogenic disorders in fetuses with normal CMA analysis. Retrospective studies for selected indications and in small patient series using various sequencing approaches show diagnostic yields between 6.5 and 80% [Best et al., 2018]. Targeted exome testing on fetuses with a suspected skeletal dysplasia phenotype showed a diagnostic rate of 81% [Chandler et al., 2018], and in some cases ES/GS reduced morbidity and lowered inpatient costs [Clark et al., 2018; Warburton, 1991; Talkowski et al., 2012; Farnaes et al., 2018]. Two large prospective studies that applied ES to large cohorts of fetuses with structural anomalies were performed in cases where CMA was unrevealing. One prospective study of 610 fetuses with structural anomalies (PAGE) identified a clinically significant genetic variant in 8.5% of cases [Lord et al., 2019]. In the second study, a diagnostic variant was found in 10.3% of fetuses [Petrovski et al., 2019]. Both studies and subsequent studies showed that the diagnostic yield was higher in fetuses with multiple congenital anomalies, skeletal dysplasias and cardiac anomalies [Mone et al., 2021b, 2021e; Lord et al., 2019; Petrovski et al., 2019]. In 3.2% of pregnancies with an isolated increased first trimester nuchal translucency, monogenic etiologies were identified as compared to 25% of pregnancies with non-immunological hydrops. Pathogenic variants in genes of the RASopathy pathways seem to account for the majority of such severe phenotypes [Sparks et al., 2020; Mone et al., 2021b]. When including deep phenotyping throughout pregnancy and postnatally on the initial patients of the PAGE cohort, a genetic diagnosis was obtained in over half of ultrasound detected fetal structural anomalies [Mone et al., 2021a]. A systematic review and meta-analysis of 66 ES/GS studies in fetal structural anomalies representing 4350 fetuses concluded that prenatal exome sequencing provides an additional diagnostic yield of 31% after normal CMA [Mellis et al., 2022]. The diagnostic yield was reported to be significantly higher in clinically pre-selected cases (42% vs. 15%) and differed between phenotypic subgroups ranging from 53% for isolated skeletal abnormalities to 2% for isolated nuchal translucency [Mellis et al., 2022].
HPO Terms and Annotations
In addition to the ontology itself, the HPO project provides HPO annotations (HPOAs) of diseases. For instance, the disease ‘Marfan syndrome’ is characterized by — and therefore annotated to — over 50 phenotypic abnormalities including ‘Aortic aneurysm’ (HP:0004942) (each abnormality is represented by an HPO term). The annotations can have modifiers that describe the age of onset and the frequencies of features. For instance, the phenotypic abnormality ‘Brachydactyly’ (HP:0001156) is rare in ‘Hydrolethalus syndrome’ (3/56 according to a published study referenced in our data), but affects nearly 100% of patients diagnosed with most of the 484 other diseases annotated to this term. This type of information can be used by algorithms to weight findings in the context of clinical differential diagnosis. The Monarch Initiative is additionally creating the Medical Action Ontology (MAxO), a new ontology of clinically relevant actions (e.g., treatments and interventions) to integrate these actions into the HPO disease models for use in clinical decision-making when interpreting variants and performing diagnostics for RDs. A full disease model includes phenotypic features, links to genes and variants, a representation of treatments and other actions, and (if relevant) environmental exposures (Figure 1).
Figure 1. Example attributes of the HPO Disease annotation model (HPOA).
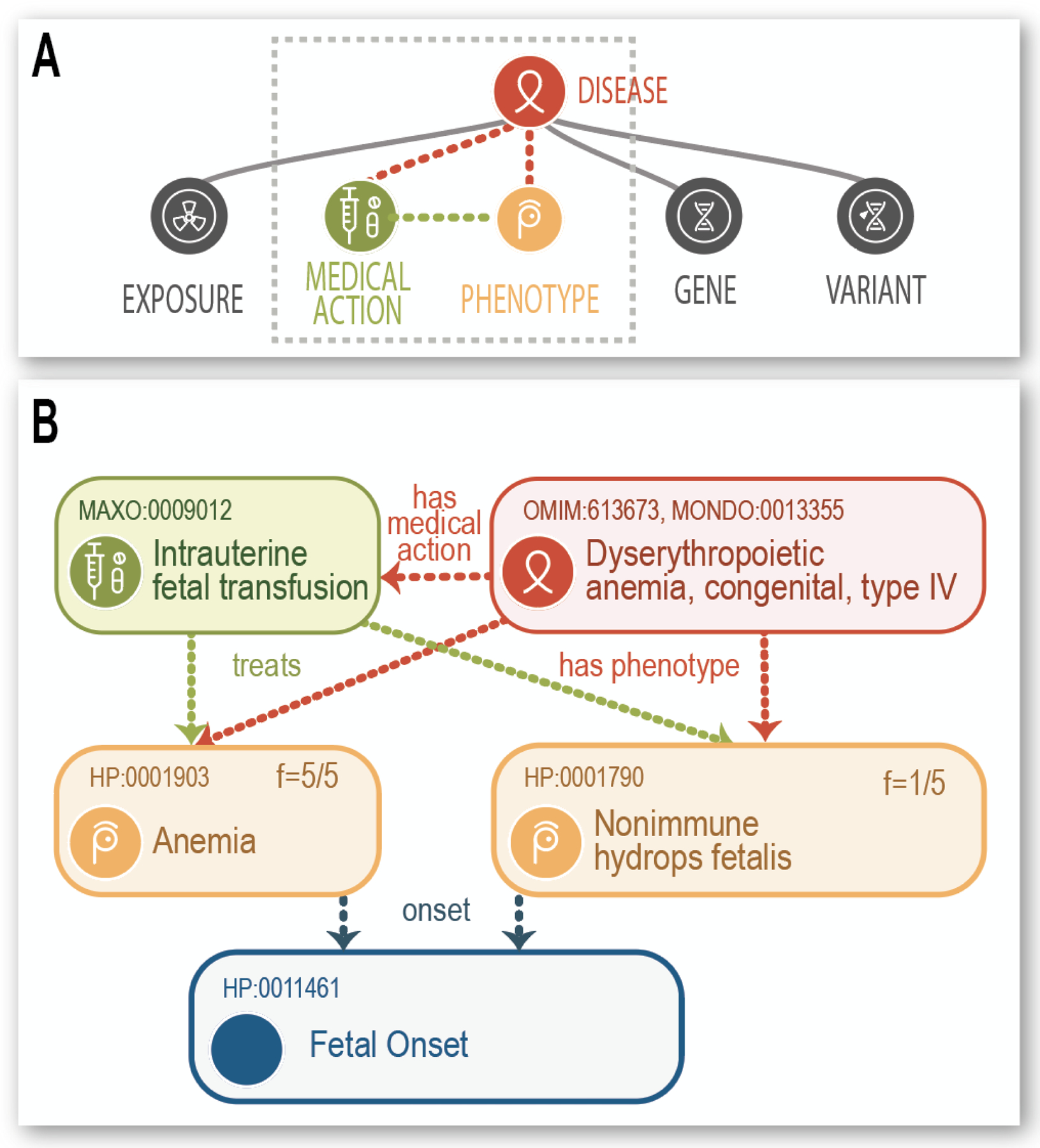
Panel A: Schematic representation of our model of a rare disease. Associated with the diseases are a variety of features. Panel B: This schematic represents one HPO annotation for the disease Dyserythropoietic anemia, congenital, type IV. Published phenotypes include Anemia with Infantile onset REF; all five of the patients with the disease presented this way (shown as f=5/5). An annotation to a treatment (Intrauterine fetal transfusion coded by a MAxO term) is shown; the treatment treats Anemia, as well as Nonimmune hydrops fetalis, a less frequent phenotypic manifestation of the disease.
The description of phenotypic variation has become central to translational research and genomic medicine [Biesecker, 2004; Robinson and Webber, 2014; Robinson, 2012; Deans et al., 2015], and computable descriptions of human disease using HPOAs have become key to a number of genomic diagnostic algorithms. Our group has developed HPO-based software for genomic diagnostics called Exomiser/Genomiser [Robinson et al., 2014; Smedley et al., 2015, 2016] that is widely used by projects such as the NIH Undiagnosed Diseases Program [Bone et al., 2016; Gall et al., 2017] and Genomics England’s 100,000 Genomes project [100,000 Genomes Project Pilot Investigators et al., 2021] [Chief Medical Officer annual report 2016: Generation Genome]. The HPO allows algorithms to ‘compute over’ clinical phenotype data in a wide variety of contexts. The ontological structure of the HPO allows fuzzy phenotype matching (semantic similarity) of sets of individual terms (phenotypic profiles, encoded within HPOAs) [Köhler et al., 2009; Bauer et al., 2012; Schulz et al., 2009]. Additionally, the underlying logical definitions enable HPO terms to be integrated with numerous other resources, such as model organism data [Robinson and Webber, 2014; Doelken et al., 2013; Köhler et al., 2014, 2013; Washington et al., 2009; Mungall et al., 2015].
Prenatal extension of the HPO
The HPO consortium has periodically organized collaborative workshops to revise and extend specific areas such as ophthalmology, immunology, nephrology, and neurology [Lewis-Smith et al., 2021; Haimel et al., 2021; Ong et al., 2020; Gasteiger et al., 2020; Köhler et al., 2019, 2017]. In 2020, we began a series of workshops to expand the representation of phenotypic abnormalities that are observed in the prenatal period. Because of the COVID-19 pandemic, the workshops were conducted by videoconferencing. Participants included experts in perinatal pathology, musculoskeletal anomalies, neurology, medical genetics, hydrops fetalis, craniofacial malformations, cardiology, neonatal-perinatal medicine, fetal medicine, informatics, placental pathology, and prenatal imaging.
Some phenotypic features are only observable in the prenatal period. The HPO groups such terms under a dedicated subontology that descends from the grouping term Abnormality of prenatal development or birth (HP:0001197). Other features such as Preaxial polydactyly (HP:0100258) can be ascertained both pre- and postnatally. The HPO puts such terms underneath the main hierarchy (for instance, the path from Preaxial polydactyly to the root of the ontology is Preaxial polydactyly →Polydactyly →Abnormal digit morphology →Abnormal limb bone morphology → Abnormal appendicular skeleton morphology → Abnormal skeletal morphology → Abnormality of the skeletal system →Abnormality of the musculoskeletal system → Phenotypic abnormality. Specifically prenatal skeletal abnormalities are placed under Abnormal fetal skeletal morphology (HP:0025662), such as Hypoplastic nasal bone (HP:0025707). Because Hypoplastic nasal bone is a subterm (child) of Abnormal skeletal morphology, it is included by searches and phenotypic similarity algorithms such as LIRICAL under both skeletal abnormalities as well as specifically prenatal abnormalities.
Ongoing work is adding annotations to terms that specify the diagnostic modalities by which a phenotypic abnormality can be ascertained. For instance, Inferior crossed fused renal ectopia (HP:0034230) is annotated via the relation ‘is observable through’ to the Medical Action Ontology (MAxO) term prenatal renal ultrasonography (MAXO:0009009). When this work is finished, software will be able to use the annotations to suggest HPO terms and the investigations by which they can be ascertained that are most helpful given a certain differential diagnosis and age of the patient. Additionally, the SUOG European project (www.suog.org) aims to associate fetal ultrasound phenotypes with specific ultrasound planes (or views) and other technical elements (2D, 3D; Doppler mode) to augment the ultrasound examination with the support of semantically derived imaging protocols [Dhombres et al., 2019].
The HPO prenatal workshops added 95 terms to the Abnormality of prenatal development or birth (HP:0001197) sub-hierarchy (for a total of 247) and revised definitions, synonyms, and disease annotations for most of the 152 terms existing before the start of the workshops. 65 terms descend from Abnormalities of placenta or umbilical cord (HP:0001194). Many additional terms were discussed on the GitHub tracker of the HPO project, which currently lists 91 issues with label prenatal/perinatal/neonatal that pertain to term requests for both specifically prenatal features as well as other features that can be observed pre- and postnatally (2022-04-14 release).
Age of onset
The HPOA disease annotations include in some cases information about the age of onset of a disease or of a specific phenotypic feature of the disease. These annotations are intended to specify the range of ages in which individuals with the disease in question tend to develop clinical manifestations, ranging from Antenatal onset (Onset prior to birth; HP:0030674), to Late onset (onset of symptoms after the age of 60 years; HP:0003584). As a part of the series of prenatal workshops, additional terms were added to the Antenatal onset subhierarchy (Figure 2). As gestational age (GA) is described in weeks from the last menstrual period (LMP or WG) during ultrasound examination, we decided to keep this for consistency with ultrasound phenotypes: for example, 8 weeks of embryonic development correspond to 10 WG.
Figure 2. Prenatal onset terms.
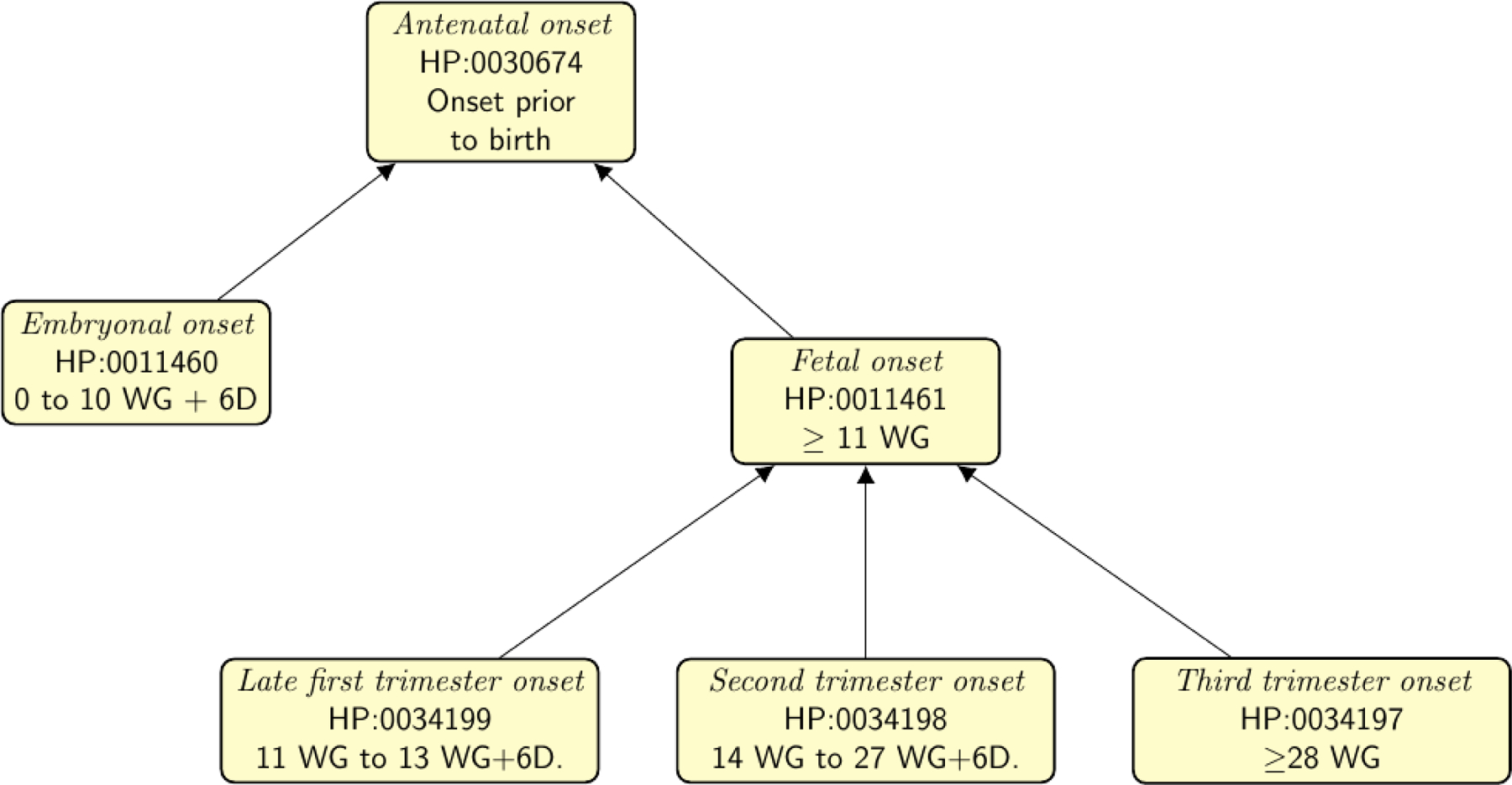
The HPO provides terms to denote the range of onset of diseases or phenotypic features. New terms were added for more granularity in the prenatal period. Prenatal ages are shown as gestational weeks, which are defined as the time from the last menstrual period of the mother. For instance, Embryonal onset refers to a disease or phenotypic feature that is first observed in the 8 weeks following fertilization, which corresponds to 10 weeks of gestation (WG). 13 WG + 6D refers to a gestational age of 13 weeks and 6 days.
HPO-based Phenopackets for computable case reports
The Global Alliance for Genomics and Health (GA4GH) is developing a suite of coordinated standards for genomics for healthcare [Rehm et al., 2021]. The Phenopacket is a new GA4GH standard for sharing disease and phenotype information. A Phenopacket characterizes an individual person or biosample, linking that individual to detailed phenotypic descriptions, genetic information, diagnoses, and treatments. The Phenopacket schema enables comparison of sets of phenotypic attributes from individual patients. Such comparisons can aid in diagnosis and facilitate patient classification and stratification for identifying new diseases and treatments [Jacobsen et al., 2021].
The HPO disease annotations are computational models of disease with information about the full range of phenotypic abnormalities and in many cases the frequencies and typical ages of onset of specific phenotypic features in cohorts of individuals with the disease [Köhler et al., 2021]. In contrast, a Phenopacket represents an individual case report. Phenopackets have been used to support rare-disease diagnostics in the SOLVE-RD project of the European Union [Zurek et al., 2021] and can be used to support a number of additional applications in translational research and computational decision support. Several tools for phenotype-driven genomic diagnostics support the Phenopacket Schema, including Exomiser, LIRICAL, Phen2Gene, and CADA [Peng et al., 2021; Robinson et al., 2014, 2020; Zhao et al., 2020] and we anticipate that more tools will offer Phenopacket support in the future.
Here we show how a Phenopacket might be used to encode clinical data to support exome or genome analysis. We have adapted a case of fetal cataract in which subsequent postnatal investigations revealed additional phenotypic abnormalities that led to a diagnosis of Warburg micro syndrome [Léonard et al., 2009]. Figure 2 provides an explanation and we refer to the online documentation for technical details [Phenopacket-schema 2.0 documentation]. In this example, the Phenopacket provides additional context for the phenotypic abnormalities that goes beyond what could be provided by a simple list of HPO terms. For instance, the age of onset of each feature is provided, and the fact that Microphthalmia was excluded on prenatal sonography is indicated. For prenatal features, the precise age of onset is often difficult to determine, and the “onset” field should be used to report the age of first observation.
As a first application of Phenopacket schema for prenatal medicine, the HPO team is collaborating with the Fetal Sequencing Consortium (FSC; https://www.google.com/url?q=https://www.obgyn.columbia.edu). The FSC includes >30 national and international sites involved in fetal sequencing whose members participate in bi-weekly calls to share data, challenges, and discuss new technologies relevant to sequencing in the perinatal period. The FSC has sequenced >3,000 anomalous and stillbirth probands, finding that 13–26% of fetuses with structural anomalies currently have a causative genotype using American College of Medical Genetics (ACMG) guidelines.
This effort has expanded to the Fetal Genomics Consortium (FGC), with a mission to understand the genetic and phenotypic architecture of fetal anomalies and stillbirth and use this information to inform pre-, peri -, postnatal and maternal care. Phenotypic and genotypic data from across the FGC centers will be integrated, aggregated, and analyzed. This collaboration will leverage the Terra Platform (https://terra.bio/), a cloud-based data ecosystem enabling processing and analysis of genomic data. Integrating phenotype data into analysis in Terra is currently limited, and a goal is to build-out the ability to easily store and run analysis using Phenopackets and associated tools in Terra. This would, for the first time, enable truly integrated genotype and phenotype analyses in one cloud-based platform that is accessible to researchers and clinicians worldwide.
We anticipate that the phenotype-driven analysis will require tuning to particular cohorts, and working with the FGC will: 1) drive new systematic phenotypes in the prenatal space; 2) allow benchmarking of phenotypic driven analysis in a single, large cohort; 3) enable phenotype driven analysis on an existing, widely used platform, Terra.
Discussion
We have presented the work of a group of experts in various fields of fetal medicine to extend the HPO to cover the prenatal phenotypic manifestations of disease. The majority of rare genetic diseases have good phenotypic descriptions and consequently HPOA in children and adults, available in gene-centric form from the HPO consortium and in disease-centric form from Orphanet [Maiella et al., 2018]. However, scant phenotypic data are available for the prenatal period. Prenatal findings of some genetic diseases have only recently begun to be collected in the literature [García Santiago et al., Sarac Sivrikoz et al., 2022], and these annotations have been transferred more slowly to the databases, limiting their computational management. For this reason, the HPO prenatal team has made an effort to include new prenatal HPO terms to support rapid inclusion in databases. Also, detailed ultrasound findings from the ontology developed by the SUOG consortium will continue to support the extension of prenatal HPO terms.
To take full advantage of ontology-based algorithms for translational research in fetal medicine and variant interpretation in prenatal ES/GS analysis, additional clinical data, computational resources, and algorithms will be required. A paucity of data is available about the prenatal manifestations of most Mendelian diseases, and many relevant articles are reports about single cases that are insufficient to understand the scope of variability and the natural history of diseases. Efforts such as the FGC can help distribute datasets in a federated fashion; the use of the GA4GH Phenopacket to code each case in an interoperable and computable fashion should accelerate the computational use of case-level data. Journals in the field are to be encouraged to have authors submit Phenopackets as supplemental material with case reports and articles about cohorts of patients. Innovative ways of encoding phenotype data as a part of the clinical encounter are imaginable. For instance, the fetal femur length is measured as a part of some fetal sonographic examinations. Knowledge of the femur length, the sex and gestational age of the fetus would allow a simple algorithm to determine if Short fetal femur length (HP:0011428) is present or not, which would allow HPO terms to be immediately generated as a part of the fetal sonography evaluation. Furthermore, phenotypes may be refined with new imaging modalities, such as fetal MRI or fetal CT-scan. Comprehensive aggregation of prenatal phenotype and genotype data will permit expansion of the phenotypic spectrum of a disorder, and inform both pre- and postnatal diagnosis.
In humans, information on genes associated with prenatal and neonatal phenotypes is limited and/or not systematically captured in a comprehensive manner. As more prenatal data become available, algorithms for cross-species phenotype matching may become relevant for characterization of novel associations between genes and human diseases with prenatal manifestations [Robinson and Webber, 2014]. Prenatal ES studies have been successful in characterizing previously unrecognized prenatal phenotypes associated with known Mendelian disease genes, and in many cases have leveraged comparisons to embryonic phenotypes in mouse models [Filges et al., 2014; Fujikura et al., 2013; Vora et al., 2017]. Large scale efforts such as the International Mouse Phenotyping Consortium (IMPC) are creating genome- and phenome-wide catalogs of gene function by characterizing new knockout mouse strains across diverse biological systems through a broad set of standardized phenotyping tests [Meehan et al., 2017]. Current estimates are that gene inactivation leads to lethal embryonic or perinatal phenotypes in roughly 30% of gene knockout experiments [Adams et al., 2013]. An additional 13% (198/1751) are associated with subviable phenotypes in which fewer than half the expected number of homozygous pups survive [Dickinson et al., 2016]. Future algorithms for variant interpretation in prenatal genomics will be able to make use of the HPO annotations and their ready comparison to data from other species that is the focus of the Monarch Initiative [Shefchek et al., 2020]. Such analyses could include data on the time course of prenatal manifestations or death, and further allow discrimination between phenotypes leading to prenatal lethality. These early manifestations are part of a wider, postnatal phenotyping spectrum that can be used to improve prioritization of genes and diseases and ultimately care and family planning. Due to the rapidly growing importance of ES/GS for the diagnosis of monogenic disorders in fetal anomaly phenotypes, extension of cross-species algorithms and tools such as Exomiser [Smedley et al., 2015] could support analysis of prenatal phenotypes in genomic diagnostics.
The HPO consortium welcomes the continued participation of the prenatal genomics community in the extension and improvement of HPO resources in this area.
Figure 3.
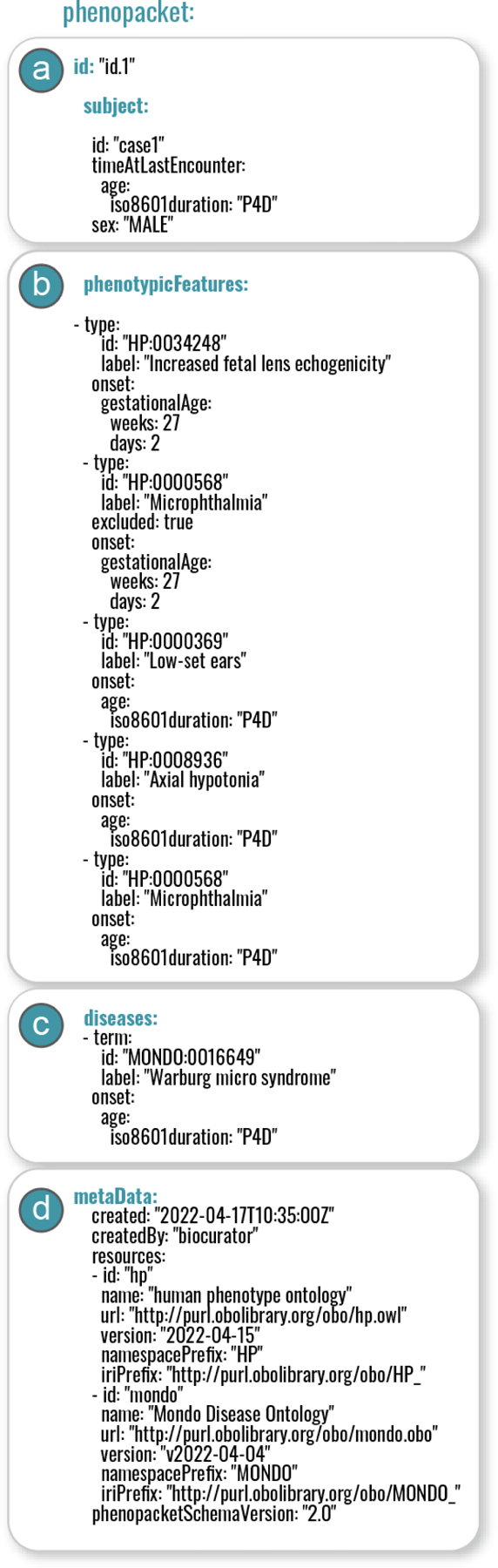
Components of a Phenopacket. (A) The subject message provides basic demographic information; (B) The phenotypicFeatures message consists of a list of phenotypic features (each of which begins with “-type” in YAML format as shown here). The patient was found to have Increased fetal lens echogenicity (HP:0034248) at a gestational age of 27 weeks, at which time Microphthalmia (HP:0000568) was excluded. Postnatal examination at an age of 4 days (represented in iso8601 format as P4D) shows Axial hypotonia (HP:0008936), Low-set ears (HP:0000369), and Microphthalmia (HP:0000568). (C) The disease diagnosis is recorded using a term from the Mondo ontology [Shefchek et al., 2020], Warburg micro syndrome (MONDO:0016649). (D) The metaData message records versions of ontologies used to create the Phenopacket together with other information. Additionally, the Phenopacket schema provides resources to record measurements, biospecimens, and treatments, not shown here.
Funding:
This work was supported by NHGRI [1U24HG011449-01A1 and 2R24OD011883-05A1], NIH Office of the Director (OD), the European Union’s Horizon 2020 research and innovation programme under grant agreement No. 779257 (SOLVE-RD), The European Union’s EIT-Health Innovation programme bp2020-2022, #20062 and #211015 (SUOG-Smart Ultrasound in Obstetrics and Gynecology), FIS-ISCIII PMP21/00063, the Australian Federal Government Medical Research Futures Fund (MRFF) PreGen: Filling the Gap - Antenatal Genomics and Newborn Care: The Translational PreGen Consortium and PI 20/01053. This work has been partly generated within the European Reference Network on Rare Congenital Malformations and Rare Intellectual Disability (ERN-ITHACA). ERN-ITHACA is co-funded by the Health Programme of the European Union.
References
- 100,000 Genomes Project Pilot Investigators, Smedley D, Smith KR, Martin A, Thomas EA, McDonagh EM, Cipriani V, Ellingford JM, Arno G, Tucci A, Vandrovcova J, Chan G, Williams HJ, Ratnaike T, Wei W, Stirrups K, Ibanez K, Moutsianas L, Wielscher M, Need A, Barnes MR, Vestito L, Buchanan J, Wordsworth S, Ashford S, Rehmström K, Li E, Fuller G, Twiss P, Spasic-Boskovic O, Halsall S, Floto RA, Poole K, Wagner A, Mehta SG, Gurnell M, Burrows N, James R, Penkett C, Dewhurst E, Gräf S, Mapeta R, Kasanicki M, Haworth A, Savage H, Babcock M, Reese MG, Bale M, Baple E, Boustred C, Brittain H, de Burca A, Bleda M, Devereau A, Halai D, Haraldsdottir E, Hyder Z, Kasperaviciute D, Patch C, Polychronopoulos D, Matchan A, Sultana R, Ryten M, Tavares ALT, Tregidgo C, Turnbull C, Welland M, Wood S, Snow C, Williams E, Leigh S, Foulger RE, Daugherty LC, Niblock O, Leong IUS, Wright CF, Davies J, Crichton C, Welch J, Woods K, Abulhoul L, Aurora P, Bockenhauer D, Broomfield A, Cleary MA, Lam T, Dattani M, Footitt E, Ganesan V, Grunewald S, Compeyrot-Lacassagne S, Muntoni F, Pilkington C, Quinlivan R, Thapar N, Wallis C, Wedderburn LR, Worth A, et al. 2021. 100,000 Genomes Pilot on Rare-Disease Diagnosis in Health Care - Preliminary Report. N. Engl. J. Med 385: 1868–1880. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Adams D, Baldock R, Bhattacharya S, Copp AJ, Dickinson M, Greene NDE, Henkelman M, Justice M, Mohun T, Murray SA, Pauws E, Raess M, Rossant J, Weaver T, West D. 2013. Bloomsbury report on mouse embryo phenotyping: recommendations from the IMPC workshop on embryonic lethal screening. Dis. Model. Mech 6: 571–579. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bauer S, Köhler S, Schulz MH, Robinson PN. 2012. Bayesian ontology querying for accurate and noise-tolerant semantic searches. Bioinformatics 28: 2502–2508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Best S, Wou K, Vora N, Van der Veyver IB, Wapner R, Chitty LS. 2018. Promises, pitfalls and practicalities of prenatal whole exome sequencing. Prenat. Diagn 38: 10–19. doi: 10.1002/pd.5102. Epub 2017 Jul 25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Biesecker LG. 2004. Phenotype matters. Nat. Genet 36: 323–324. [DOI] [PubMed] [Google Scholar]
- Blaas H-GK. 2014. Detection of structural abnormalities in the first trimester using ultrasound. Best Pract. Res. Clin. Obstet. Gynaecol 28: 341–353. doi: 10.1016/j.bpobgyn.2013.11.004. Epub 2013 Dec 4. [DOI] [PubMed] [Google Scholar]
- Boitor Borza D, Popa Stanila R, Zaharie G, Hasmasanu M, Muresan D. 2022. Fetal cardiac rhabdomyomas as a sonographic sign of tuberous sclerosis complex - a diagnosis not to be missed. A pictorial essay. Med. Ultrason [DOI] [PubMed] [Google Scholar]
- Bone WP, Washington NL, Buske OJ, Adams DR, Davis J, Draper D, Flynn ED, Girdea M, Godfrey R, Golas G, Groden C, Jacobsen J, Köhler S, Lee EMJ, Links AE, Markello TC, Mungall CJ, Nehrebecky M, Robinson PN, Sincan M, Soldatos AG, Tifft CJ, Toro C, Trang H, Valkanas E, Vasilevsky N, Wahl C, Wolfe LA, Boerkoel CF, Brudno M, Haendel MA, Gahl WA, Smedley D. 2016. Computational evaluation of exome sequence data using human and model organism phenotypes improves diagnostic efficiency. Genet. Med 18: 608–617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cacheiro P, Muñoz-Fuentes V, Murray SA, Dickinson ME, Bucan M, Nutter LMJ, Peterson KA, Haselimashhadi H, Flenniken AM, Morgan H, Westerberg H, Konopka T, Hsu C-W, Christiansen A, Lanza DG, Beaudet AL, Heaney JD, Fuchs H, Gailus-Durner V, Sorg T, Prochazka J, Novosadova V, Lelliott CJ, Wardle-Jones H, Wells S, Teboul L, Cater H, Stewart M, Hough T, Wurst W, Sedlacek R, Adams DJ, Seavitt JR, Tocchini-Valentini G, Mammano F, Braun RE, McKerlie C, Herault Y, de Angelis MH, Mallon A-M, Lloyd KCK, Brown SDM, Parkinson H, Meehan TF, Smedley D, Genomics England Research Consortium, International Mouse Phenotyping Consortium. 2020. Human and mouse essentiality screens as a resource for disease gene discovery. Nat. Commun 11: 655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carlson LM, Vora NL. 2017. Prenatal Diagnosis: Screening and Diagnostic Tools. Obstet. Gynecol. Clin. North Am 44: 245–256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chandler N, Best S, Hayward J, Faravelli F, Mansour S, Kivuva E, Tapon D, Male A, DeVile C, Chitty LS. 2018. Rapid prenatal diagnosis using targeted exome sequencing: a cohort study to assess feasibility and potential impact on prenatal counseling and pregnancy management. Genet. Med 20: 1430–1437. doi: 10.1038/gim.2018.30. Epub 2018 Mar 29. [DOI] [PubMed] [Google Scholar]
- Chief Medical Officer annual report 2016: Generation Genome GOV.UK.
- Clark MM, Stark Z, Farnaes L, Tan TY, White SM, Dimmock D, Kingsmore SF. 2018. Meta-analysis of the diagnostic and clinical utility of genome and exome sequencing and chromosomal microarray in children with suspected genetic diseases. NPJ Genom Med 3: 16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deans AR, Lewis SE, Huala E, Anzaldo SS, Ashburner M, Balhoff JP, Blackburn DC, Blake JA, Burleigh JG, Chanet B, Cooper LD, Courtot M, Csösz S, Cui H, Dahdul W, Das S, Dececchi TA, Dettai A, Diogo R, Druzinsky RE, Dumontier M, Franz NM, Friedrich F, Gkoutos GV, Haendel M, Harmon LJ, Hayamizu TF, He Y, Hines HM, Ibrahim N, Jackson LM, Jaiswal P, James-Zorn C, Köhler S, Lecointre G, Lapp H, Lawrence CJ, Le Novère N, Lundberg JG, Macklin J, Mast AR, Midford PE, Mikó I, Mungall CJ, Oellrich A, Osumi-Sutherland D, Parkinson H, Ram’irez MJ, Richter S, Robinson PN, Ruttenberg A, Schulz KS, Segerdell E, Seltmann KC, Sharkey MJ, Smith AD, Smith B, Specht CD, Squires RB, Thacker RW, Thessen A, Fernandez-Triana J, Vihinen M, Vize PD, Vogt L, Wall CE, Walls RL, Westerfeld M, Wharton RA, Wirkner CS, Woolley JB, Yoder MJ, Zorn AM, Mabee P. 2015. Finding our way through phenotypes. PLoS Biol 13: e1002033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dhombres F, Maurice P, Guilbaud L, Franchinard L, Dias B, Charlet J, Blondiaux E, Khoshnood B, Jurkovic D, Jauniaux E, Jouannic J-M. 2019. A Novel Intelligent Scan Assistant System for Early Pregnancy Diagnosis by Ultrasound: Clinical Decision Support System Evaluation Study. J. Med. Internet Res 21: e14286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dickinson ME, Flenniken AM, Ji X, Teboul L, Wong MD, White JK, Meehan TF, Weninger WJ, Westerberg H, Adissu H, Baker CN, Bower L, Brown JM, Caddle LB, Chiani F, Clary D, Cleak J, Daly MJ, Denegre JM, Doe B, Dolan ME, Edie SM, Fuchs H, Gailus-Durner V, Galli A, Gambadoro A, Gallegos J, Guo S, Horner NR, Hsu C-W, Johnson SJ, Kalaga S, Keith LC, Lanoue L, Lawson TN, Lek M, Mark M, Marschall S, Mason J, McElwee ML, Newbigging S, Nutter LMJ, Peterson KA, Ramirez-Solis R, Rowland DJ, Ryder E, Samocha KE, Seavitt JR, Selloum M, Szoke-Kovacs Z, Tamura M, Trainor AG, Tudose I, Wakana S, Warren J, Wendling O, West DB, Wong L, Yoshiki A, International Mouse Phenotyping Consortium, Jackson Laboratory, Infrastructure Nationale PHENOMIN, Institut Clinique de la Souris (ICS), Charles River Laboratories, MRC Harwell, Toronto Centre for Phenogenomics, Wellcome Trust Sanger Institute, RIKEN BioResource Center, MacArthur DG, Tocchini-Valentini GP, Gao X, Flicek P, Bradley A, Skarnes WC, Justice MJ, Parkinson HE, Moore M, Wells S, Braun RE, Svenson KL, de Angelis MH, Herault Y, Mohun T, Mallon A-M, Henkelman RM, Brown SDM, Adams DJ, Lloyd KCK, McKerlie C, Beaudet AL, Bućan M, Murray SA. 2016. High-throughput discovery of novel developmental phenotypes. Nature 537: 508–514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Doelken SC, Köhler S, Mungall CJ, Gkoutos GV, Ruef BJ, Smith C, Smedley D, Bauer S, Klopocki E, Schofield PN, Westerfield M, Robinson PN, Lewis SE. 2013. Phenotypic overlap in the contribution of individual genes to CNV pathogenicity revealed by cross-species computational analysis of single-gene mutations in humans, mice and zebrafish. Dis. Model. Mech 6: 358–372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Drukker L, Bradburn E, Rodriguez GB, Roberts NW, Impey L, Papageorghiou AT. 2021. How often do we identify fetal abnormalities during routine third-trimester ultrasound? A systematic review and meta-analysis. BJOG 128: 259–269. [DOI] [PubMed] [Google Scholar]
- Farnaes L, Hildreth A, Sweeney NM, Clark MM, Chowdhury S, Nahas S, Cakici JA, Benson W, Kaplan RH, Kronick R, Bainbridge MN, Friedman J, Gold JJ, Ding Y, Veeraraghavan N, Dimmock D, Kingsmore SF. 2018. Rapid whole-genome sequencing decreases infant morbidity and cost of hospitalization. NPJ Genom Med 3: 10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Filges I, Friedman JM. 2015. Exome sequencing for gene discovery in lethal fetal disorders--harnessing the value of extreme phenotypes. Prenat. Diagn 35: 1005–1009. doi: 10.1002/pd.4464. Epub 2014 Aug 22. [DOI] [PubMed] [Google Scholar]
- Filges I, Nosova E, Bruder E, Tercanli S, Townsend K, Gibson WT, Röthlisberger B, Heinimann K, Hall JG, Gregory-Evans CY, Wasserman WW, Miny P, Friedman JM. 2014. Exome sequencing identifies mutations in KIF14 as a novel cause of an autosomal recessive lethal fetal ciliopathy phenotype. Clin. Genet 86: 220–228. [DOI] [PubMed] [Google Scholar]
- Fujikura K, Setsu T, Tanigaki K, Abe T, Kiyonari H, Terashima T, Sakisaka T. 2013. Kif14 mutation causes severe brain malformation and hypomyelination. PLoS One 8: e53490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gall T, Valkanas E, Bello C, Markello T, Adams C, Bone WP, Brandt AJ, Brazill JM, Carmichael L, Davids M, Davis J, Diaz-Perez Z, Draper D, Elson J, Flynn ED, Godfrey R, Groden C, Hsieh C-K, Fischer R, Golas GA, Guzman J, Huang Y, Kane MS, Lee E, Li C, Links AE, Maduro V, Malicdan MCV, Malik FS, Nehrebecky M, Park J, Pemberton P, Schaffer K, Simeonov D, Sincan M, Smedley D, Valivullah Z, Wahl C, Washington N, Wolfe LA, Xu K, Zhu Y, Gahl WA, Tifft CJ, Toro C, Adams DR, He M, Robinson PN, Haendel MA, Zhai RG, Boerkoel CF. 2017. Defining Disease, Diagnosis, and Translational Medicine within a Homeostatic Perturbation Paradigm: The National Institutes of Health Undiagnosed Diseases Program Experience. Front. Med 4: 62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gasteiger LM, Robinson PN, Pazmandi J, Boztug K, Seppänen MRJ, Seidel MG, Registry Working Party of the European Society for Immunodeficiencies (ESID). 2020. Supplementation of the ESID registry working definitions for the clinical diagnosis of inborn errors of immunity with encoded human phenotype ontology (HPO) terms. J. Allergy Clin. Immunol. Pract 8: 1778. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gray KJ, Wilkins-Haug LE, Herrig NJ, Vora NL. 2019. Fetal phenotypes emerge as genetic technologies become robust. Prenat. Diagn 39: 811–817. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haendel MA, Chute CG, Robinson PN. 2018. Classification, Ontology, and Precision Medicine. N. Engl. J. Med 379: 1452–1462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haimel M, Pazmandi J, Heredia RJ, Dmytrus J, Bal SK, Zoghi S, van Daele P, Briggs TA, Wouters C, Bader-Meunier B, Aeschlimann FA, Caorsi R, Eleftheriou D, Hoppenreijs E, Salzer E, Bakhtiar S, Derfalvi B, Saettini F, Kusters MAA, Elfeky R, Trück J, Rivière JG, van der Burg M, Gattorno M, Seidel MG, Burns S, Warnatz K, Hauck F, Brogan P, Gilmour KC, Schuetz C, Simon A, Bock C, Hambleton S, de Vries E, Robinson PN, van Gijn M, Boztug K. 2021. Curation and expansion of Human Phenotype Ontology for defined groups of inborn errors of immunity. J. Allergy Clin. Immunol. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hillman SC, McMullan DJ, Hall G, Togneri FS, James N, Maher EJ, Meller CH, Williams D, Wapner RJ, Maher ER, Kilby MD. 2013. Use of prenatal chromosomal microarray: prospective cohort study and systematic review and meta-analysis. Ultrasound Obstet. Gynecol 41: 610–620. [DOI] [PubMed] [Google Scholar]
- Jacobsen JOB, Baudis M, Baynam GS, Beckmann JS, Beltran S, Callahan TJ, Chute CG, Courtot M, Danis D, Elemento O, Freimuth RR, Gargano MA, Groza T, Hamosh A, Harris NL, Kaliyaperumal R, Khalifa A, Krawitz PM, Köhler S, Laraway BJ, Lehväslaiho H, Lloyd KC, Matalonga L, McMurry JA, Metke-Jimenez A, Mungall CJ, Munoz-Torres MC, Ogishima S, Papakonstantinou A, Piscia D, Pontikos N, Queralt-Rosinach N, Roos M, Schofield PN, Siapos A, Smedley D, Smith LD, Steinhaus R, Sundaramurthi JC, Swietlik EM, Thun S, Vasilevsky NA, Wagner AH, Warner JL, Weiland C, Haendel MA, Robinson PN. 2021. The GA4GH Phenopacket schema: A computable representation of clinical data for precision medicine. bioRxiv [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kingsmore SF, Cakici JA, Clark MM, Gaughran M, Feddock M, Batalov S, Bainbridge MN, Carroll J, Caylor SA, Clarke C, Ding Y, Ellsworth K, Farnaes L, Hildreth A, Hobbs C, James K, Kint CI, Lenberg J, Nahas S, Prince L, Reyes I, Salz L, Sanford E, Schols P, Sweeney N, Tokita M, Veeraraghavan N, Watkins K, Wigby K, Wong T, Chowdhury S, Wright MS, Dimmock D, RCIGM Investigators. 2019. A Randomized, Controlled Trial of the Analytic and Diagnostic Performance of Singleton and Trio, Rapid Genome and Exome Sequencing in Ill Infants. Am. J. Hum. Genet 105: 719–733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Köhler S, Carmody L, Vasilevsky N, Jacobsen JOB, Danis D, Gourdine J-P, Gargano M, Harris NL, Matentzoglu N, McMurry JA, Osumi-Sutherland D, Cipriani V, Balhoff JP, Conlin T, Blau H, Baynam G, Palmer R, Gratian D, Dawkins H, Segal M, Jansen AC, Muaz A, Chang WH, Bergerson J, Laulederkind SJF, Yüksel Z, Beltran S, Freeman AF, Sergouniotis PI, Durkin D, Storm AL, Hanauer M, Brudno M, Bello SM, Sincan M, Rageth K, Wheeler MT, Oegema R, Lourghi H, Della Rocca MG, Thompson R, Castellanos F, Priest J, Cunningham-Rundles C, Hegde A, Lovering RC, Hajek C, Olry A, Notarangelo L, Similuk M, Zhang XA, Gómez-Andrés D, Lochmüller H, Dollfus H, Rosenzweig S, Marwaha S, Rath A, Sullivan K, Smith C, Milner JD, Leroux D, Boerkoel CF, Klion A, Carter MC, Groza T, Smedley D, Haendel MA, Mungall C, Robinson PN. 2018. Expansion of the Human Phenotype Ontology (HPO) knowledge base and resources. Nucleic Acids Res [DOI] [PMC free article] [PubMed] [Google Scholar]
- Köhler S, Carmody L, Vasilevsky N, Jacobsen JOB, Danis D, Gourdine J-P, Gargano M, Harris NL, Matentzoglu N, McMurry JA, Osumi-Sutherland D, Cipriani V, Balhoff JP, Conlin T, Blau H, Baynam G, Palmer R, Gratian D, Dawkins H, Segal M, Jansen AC, Muaz A, Chang WH, Bergerson J, Laulederkind SJF, Yüksel Z, Beltran S, Freeman AF, Sergouniotis PI, Durkin D, Storm AL, Hanauer M, Brudno M, Bello SM, Sincan M, Rageth K, Wheeler MT, Oegema R, Lourghi H, Della Rocca MG, Thompson R, Castellanos F, Priest J, Cunningham-Rundles C, Hegde A, Lovering RC, Hajek C, Olry A, Notarangelo L, Similuk M, Zhang XA, Gómez-Andrés D, Lochmüller H, Dollfus H, Rosenzweig S, Marwaha S, Rath A, Sullivan K, Smith C, Milner JD, Leroux D, Boerkoel CF, Klion A, Carter MC, Groza T, Smedley D, Haendel MA, Mungall C, Robinson PN. 2019. Expansion of the Human Phenotype Ontology (HPO) knowledge base and resources. Nucleic Acids Res 47: D1018–D1027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Köhler S, Dölken S, Ruef B, Washington SBN, Westerfield M, Gkoutos G, Schofield P, Smedley D, Robinson PN, Mungall CJ. 2013. Construction and accessibility of a cross-species phenotype ontology along with gene annotations for biomedical research. F1000 Reserach 2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Köhler S, Gargano M, Matentzoglu N, Carmody LC, Lewis-Smith D, Vasilevsky NA, Danis D, Balagura G, Baynam G, Brower AM, Callahan TJ, Chute CG, Est JL, Galer PD, Ganesan S, Griese M, Haimel M, Pazmandi J, Hanauer M, Harris NL, Hartnett MJ, Hastreiter M, Hauck F, He Y, Jeske T, Kearney H, Kindle G, Klein C, Knoflach K, Krause R, Lagorce D, McMurry JA, Miller JA, Munoz-Torres MC, Peters RL, Rapp CK, Rath AM, Rind SA, Rosenberg AZ, Segal MM, Seidel MG, Smedley D, Talmy T, Thomas Y, Wiafe SA, Xian J, Yüksel Z, Helbig I, Mungall CJ, Haendel MA, Robinson PN. 2021. The Human Phenotype Ontology in 2021. Nucleic Acids Res 49: D1207–D1217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Köhler S, Schoeneberg U, Czeschik JC, Doelken SC, Hehir-Kwa JY, Ibn-Salem J, Mungall CJ, Smedley D, Haendel MA, Robinson PN. 2014. Clinical interpretation of CNVs with cross-species phenotype data. J. Med. Genet 51: 766–772. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Köhler S, Schulz MH, Krawitz P, Bauer S, Dölken S, Ott CE, Mundlos C, Horn D, Mundlos S, Robinson PN. 2009. Clinical diagnostics in human genetics with semantic similarity searches in ontologies. Am. J. Hum. Genet 85: 457–464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Köhler S, Vasilevsky NA, Engelstad M, Foster E, McMurry J, Aymé S, Baynam G, Bello SM, Boerkoel CF, Boycott KM, Brudno M, Buske OJ, Chinnery PF, Cipriani V, Connell LE, Dawkins HJS, DeMare LE, Devereau AD, de Vries BBA, Firth HV, Freson K, Greene D, Hamosh A, Helbig I, Hum C, Jähn JA, James R, Krause R, F Laulederkind SJ, Lochmüller H, Lyon GJ, Ogishima S, Olry A, Ouwehand WH, Pontikos N, Rath A, Schaefer F, Scott RH, Segal M, Sergouniotis PI, Sever R, Smith CL, Straub V, Thompson R, Turner C, Turro E, Veltman MWM, Vulliamy T, Yu J, von Ziegenweidt J, Zankl A, Züchner S, Zemojtel T, Jacobsen JOB, Groza T, Smedley D, Mungall CJ, Haendel M, Robinson PN. 2017. The Human Phenotype Ontology in 2017. Nucleic Acids Res 45: D865–D876. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Léonard A, Bernard P, Hiel A-L, Hubinont C. 2009. Prenatal diagnosis of fetal cataract: case report and review of the literature. Fetal Diagn. Ther 26: 61–67. [DOI] [PubMed] [Google Scholar]
- Lewis-Smith D, Galer PD, Balagura G, Kearney H, Ganesan S, Cosico M, O’Brien M, Vaidiswaran P, Krause R, Ellis CA, Thomas RH, Robinson PN, Helbig I. 2021. Modeling seizures in the Human Phenotype Ontology according to contemporary ILAE concepts makes big phenotypic data tractable. Epilepsia 62: 1293–1305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lochmüller H, Torrent I Farnell J, Le Cam Y, Jonker AH, Lau LP, Baynam G, Kaufmann P, Dawkins HJ, Lasko P, Austin CP, Boycott KM, IRDiRC Consortium Assembly. 2017. The International Rare Diseases Research Consortium: Policies and Guidelines to maximize impact. Eur. J. Hum. Genet 25: 1293–1302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lord J, McMullan DJ, Eberhardt RY, Rinck G, Hamilton SJ, Quinlan-Jones E, Prigmore E, Keelagher R, Best SK, Carey GK, Mellis R, Robart S, Berry IR, Chandler KE, Cilliers D, Cresswell L, Edwards SL, Gardiner C, Henderson A, Holden ST, Homfray T, Lester T, Lewis RA, Newbury-Ecob R, Prescott K, Quarrell OW, Ramsden SC, Roberts E, Tapon D, Tooley MJ, Vasudevan PC, Weber AP, Wellesley DG, Westwood P, White H, Parker M, Williams D, Jenkins L, Scott RH, Kilby MD, Chitty LS, Hurles ME, Maher ER, Prenatal Assessment of Genomes and Exomes Consortium. 2019. Prenatal exome sequencing analysis in fetal structural anomalies detected by ultrasonography (PAGE): a cohort study. Lancet [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maiella S, Olry A, Hanauer M, Lanneau V, Lourghi H, Donadille B, Rodwell C, Köhler S, Seelow D, Jupp S, Parkinson H, Groza T, Brudno M, Robinson PN, Rath A. 2018. Harmonising phenomics information for a better interoperability in the rare disease field. Eur. J. Med. Genet [DOI] [PubMed] [Google Scholar]
- Meehan TF, Conte N, West DB, Jacobsen JO, Mason J, Warren J, Chen C-K, Tudose I, Relac M, Matthews P, Karp N, Santos L, Fiegel T, Ring N, Westerberg H, Greenaway S, Sneddon D, Morgan H, Codner GF, Stewart ME, Brown J, Horner N, International Mouse Phenotyping Consortium, Haendel M, Washington N, Mungall CJ, Reynolds CL, Gallegos J, Gailus-Durner V, Sorg T, Pavlovic G, Bower LR, Moore M, Morse I, Gao X, Tocchini-Valentini GP, Obata Y, Cho SY, Seong JK, Seavitt J, Beaudet AL, Dickinson ME, Herault Y, Wurst W, de Angelis MH, Lloyd KCK, Flenniken AM, Nutter LMJ, Newbigging S, McKerlie C, Justice MJ, Murray SA, Svenson KL, Braun RE, White JK, Bradley A, Flicek P, Wells S, Skarnes WC, Adams DJ, Parkinson H, Mallon A-M, Brown SDM, Smedley D. 2017. Disease model discovery from 3,328 gene knockouts by The International Mouse Phenotyping Consortium. Nat. Genet 49: 1231–1238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mellis R, Oprych K, Scotchman E, Hill M, Chitty LS. 2022. Diagnostic yield of exome sequencing for prenatal diagnosis of fetal structural anomalies: A systematic review and meta-analysis. Prenat. Diagn [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meng L, Pammi M, Saronwala A, Magoulas P, Ghazi AR, Vetrini F, Zhang J, He W, Dharmadhikari AV, Qu C, Ward P, Braxton A, Narayanan S, Ge X, Tokita MJ, Santiago-Sim T, Dai H, Chiang T, Smith H, Azamian MS, Robak L, Bostwick BL, Schaaf CP, Potocki L, Scaglia F, Bacino CA, Hanchard NA, Wangler MF, Scott D, Brown C, Hu J, Belmont JW, Burrage LC, Graham BH, Sutton VR, Craigen WJ, Plon SE, Lupski JR, Beaudet AL, Gibbs RA, Muzny DM, Miller MJ, Wang X, Leduc MS, Xiao R, Liu P, Shaw C, Walkiewicz M, Bi W, Xia F, Lee B, Eng CM, Yang Y, Lalani SR. 2017. Use of Exome Sequencing for Infants in Intensive Care Units: Ascertainment of Severe Single-Gene Disorders and Effect on Medical Management. JAMA Pediatr 171: e173438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mone F, Abu Subieh H, Doyle S, Hamilton S, McMullan DJ, Allen S, Marton T, Williams D, Kilby MD. 2021a. Evolving fetal phenotypes and clinical impact of progressive prenatal exome sequencing pathways: cohort study. Ultrasound Obstet. Gynecol 2021 Dec 23. doi: 10.1002/uog.24842. Epub ahead of print. [DOI] [PubMed] [Google Scholar]
- Mone F, Eberhardt RY, Hurles ME, Mcmullan DJ, Maher ER, Lord J, Chitty LS, Dempsey E, Homfray T, Giordano JL, Wapner RJ, Sun L, Sparks TN, Norton ME, Kilby MD. 2021b. Fetal hydrops and the Incremental yield of Next-generation sequencing over standard prenatal Diagnostic testing (FIND) study: prospective cohort study and meta-analysis. Ultrasound Obstet. Gynecol 58: 509–518. doi: 10.1002/uog.23652. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mone F, Eberhardt RY, Morris RK, Hurles ME, McMullan DJ, Maher ER, Lord J, Chitty LS, Giordano JL, Wapner RJ, Kilby MD, CODE Study Collaborators. COngenital heart disease and the Diagnostic yield with Exome sequencing (CODE) study: prospective cohort study and systematic review. Ultrasound Obstet Gynecol 2021. Jan;57(1):43–51. [DOI] [PubMed] [Google Scholar]
- Mone F, McMullan DJ, Williams D, Chitty LS, Maher ER, Kilby MD, Fetal Genomics Steering Group of the British Society for Genetic Medicine, Royal College of Obstetricians and Gynaecologists. Evidence to Support the Clinical Utility of Prenatal Exome Sequencing in Evaluation of the Fetus with Congenital Anomalies: Scientific Impact Paper No. 64 [February] 2021. BJOG 2021. Aug;128(9):e39–e50. [DOI] [PubMed] [Google Scholar]
- Mone F, Stott BK, Hamilton S, Seale AN, Quinlan-Jones E, Allen S, Hurles ME, McMullan DJ, Maher ER, Kilby MD. 2021e. The Diagnostic Yield of Prenatal Genetic Technologies in Congenital Heart Disease: A Prospective Cohort Study. Fetal Diagn. Ther: 1–8. doi: 10.1159/000512488. Epub ahead of print. [DOI] [PubMed] [Google Scholar]
- Mungall CJ, Washington NL, Nguyen-Xuan J, Condit C, Smedley D, Köhler S, Groza T, Shefchek K, Hochheiser H, Robinson PN, Lewis SE, Haendel MA. 2015. Use of model organism and disease databases to support matchmaking for human disease gene discovery. Hum. Mutat 36: 979–984. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oellrich A, Hoehndorf R, Gkoutos GV, Rebholz-Schuhmann D. 2012. Improving disease gene prioritization by comparing the semantic similarity of phenotypes in mice with those of human diseases. PLoS One 7: e38937. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ong E, Wang LL, Schaub J, O’Toole JF, Steck B, Rosenberg AZ, Dowd F, Hansen J, Barisoni L, Jain S, de Boer IH, Valerius MT, Waikar SS, Park C, Crawford DC, Alexandrov T, Anderton CR, Stoeckert C, Weng C, Diehl AD, Mungall CJ, Haendel M, Robinson PN, Himmelfarb J, Iyengar R, Kretzler M, Mooney S, He Y, Kidney Precision Medicine Project. 2020. Modelling kidney disease using ontology: insights from the Kidney Precision Medicine Project. Nat. Rev. Nephrol 16: 686–696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Osterman MJK, Kochanek KD, MacDorman MF, Strobino DM, Guyer B. 2015. Annual summary of vital statistics: 2012–2013. Pediatrics 135: 1115–1125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peng C, Dieck S, Schmid A, Ahmad A, Knaus A, Wenzel M, Mehnert L, Zirn B, Haack T, Ossowski S, Wagner M, Brunet T, Ehmke N, Danyel M, Rosnev S, Kamphans T, Nadav G, Fleischer N, Fröhlich H, Krawitz P. 2021. CADA: phenotype-driven gene prioritization based on a case-enriched knowledge graph. NAR Genom Bioinform 3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Petrovski S, Aggarwal V, Giordano JL, Stosic M, Wou K, Bier L, Spiegel E, Brennan K, Stong N, Jobanputra V, Ren Z, Zhu X, Mebane C, Nahum O, Wang Q, Kamalakaran S, Malone C, Anyane-Yeboa K, Miller R, Levy B, Goldstein DB, Wapner RJ. 2019. Whole-exome sequencing in the evaluation of fetal structural anomalies: a prospective cohort study. Lancet [DOI] [PubMed] [Google Scholar]
- Phenopacket-schema 2.0 documentation.
- Rehm HL, Page AJH, Smith L, Adams JB, Alterovitz G, Babb LJ, Barkley MP, Baudis M, Beauvais MJS, Beck T, Beckmann JS, Beltran S, Bernick D, Bernier A, Bonfield JK, Boughtwood TF, Bourque G, Bowers SR, Brookes AJ, Brudno M, Brush MH, Bujold D, Burdett T, Buske OJ, Cabili MN, Cameron DL, Carroll RJ, Casas-Silva E, Chakravarty D, Chaudhari BP, Chen SH, Cherry JM, Chung J, Cline M, Clissold HL, Cook-Deegan RM, Courtot M, Cunningham F, Cupak M, Davies RM, Denisko D, Doerr MJ, Dolman LI, Dove ES, Dursi LJ, Dyke SOM, Eddy JA, Eilbeck K, Ellrott KP, Fairley S, Fakhro KA, Firth HV, Fitzsimons MS, Fiume M, Flicek P, Fore IM, Freeberg MA, Freimuth RR, Fromont LA, Fuerth J, Gaff CL, Gan W, Ghanaim EM, Glazer D, Green RC, Griffith M, Griffith OL, Grossman RL, Groza T, Auvil JMG, Guigó R, Gupta D, Haendel MA, Hamosh A, Hansen DP, Hart RK, Hartley DM, Haussler D, Hendricks-Sturrup RM, Ho CWL, Hobb AE, Hoffman MM, Hofmann OM, Holub P, Hsu JS, Hubaux J-P, Hunt SE, Husami A, Jacobsen JO, Jamuar SS, Janes EL, Jeanson F, Jené A, Johns AL, Joly Y, Jones SJM, Kanitz A, Kato K, et al. 2021. GA4GH: International policies and standards for data sharing across genomic research and healthcare. Cell Genom 1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robinson PN. 2012. Deep phenotyping for precision medicine. Hum. Mutat 33: 777–780. [DOI] [PubMed] [Google Scholar]
- Robinson PN, Köhler S, Bauer S, Seelow D, Horn D, Mundlos S. 2008. The Human Phenotype Ontology: a tool for annotating and analyzing human hereditary disease. Am. J. Hum. Genet 83: 610–615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robinson PN, Köhler S, Oellrich A, Sanger Mouse Genetics Project, Wang K, Mungall CJ, Lewis SE, Washington N, Bauer S, Seelow D, Krawitz P, Gilissen C, Haendel M, Smedley D. 2014. Improved exome prioritization of disease genes through cross-species phenotype comparison. Genome Res 24: 340–348. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robinson PN, Ravanmehr V, Jacobsen JOB, Danis D, Zhang XA, Carmody L, Gargano M, Thaxton C, Reese J, Holtgrewe M, Koehler S, McMurry JA, Haendel MA, Smedley D. 2020. Interpretable Clinical Genomics with a Likelihood Ratio Paradigm. Genetic and Genomic Medicine [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robinson PN, Webber C. 2014. Phenotype ontologies and cross-species analysis for translational research. PLoS Genet 10: e1004268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rossi AC, Prefumo F. 2013. Accuracy of ultrasonography at 11–14 weeks of gestation for detection of fetal structural anomalies: a systematic review. Obstet. Gynecol 122: 1160–1167. doi: 10.1097/AOG.0000000000000015. [DOI] [PubMed] [Google Scholar]
- Sarac Sivrikoz T, Basaran S, Has R, Karaman B, Kalelioglu IH, Kirgiz M, Altunoglu U, Yuksel A. Prenatal sonographic and cytogenetic/molecular findings of 22q11.2 microdeletion syndrome in 48 confirmed cases in a single tertiary center. Arch Gynecol Obstet 2022. Feb;305(2):323–342. [DOI] [PubMed] [Google Scholar]
- Salomon LJ, Alfirevic Z, Bilardo CM, Chalouhi GE, Ghi T, Kagan KO, Lau TK, Papageorghiou AT, Raine-Fenning NJ, Stirnemann J, Suresh S, Tabor A, Timor-Tritsch IE, Toi A, Yeo G. 2013. ISUOG practice guidelines: performance of first-trimester fetal ultrasound scan. Ultrasound Obstet. Gynecol 41: 102–113. [DOI] [PubMed] [Google Scholar]
- Schulz MH, Köhler S, Bauer S, Vingron M, Robinson PN. 2009. Exact Score Distribution Computation for Similarity Searches in Ontologies. Algorithms in Bioinformatics: 298–309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shefchek KA, Harris NL, Gargano M, Matentzoglu N, Unni D, Brush M, Keith D, Conlin T, Vasilevsky N, Zhang XA, Balhoff JP, Babb L, Bello SM, Blau H, Bradford Y, Carbon S, Carmody L, Chan LE, Cipriani V, Cuzick A, Della Rocca M, Dunn N, Essaid S, Fey P, Grove C, Gourdine J-P, Hamosh A, Harris M, Helbig I, Hoatlin M, Joachimiak M, Jupp S, Lett KB, Lewis SE, McNamara C, Pendlington ZM, Pilgrim C, Putman T, Ravanmehr V, Reese J, Riggs E, Robb S, Roncaglia P, Seager J, Segerdell E, Similuk M, Storm AL, Thaxon C, Thessen A, Jacobsen JOB, McMurry JA, Groza T, Köhler S, Smedley D, Robinson PN, Mungall CJ, Haendel MA, Munoz-Torres MC, Osumi-Sutherland D. 2020. The Monarch Initiative in 2019: an integrative data and analytic platform connecting phenotypes to genotypes across species. Nucleic Acids Res 48: D704–D715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smedley D, Jacobsen JOB, Jäger M, Köhler S, Holtgrewe M, Schubach M, Siragusa E, Zemojtel T, Buske OJ, Washington NL, Bone WP, Haendel MA, Robinson PN. 2015. Next-generation diagnostics and disease-gene discovery with the Exomiser. Nat. Protoc 10: 2004–2015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smedley D, Schubach M, Jacobsen JOB, Köhler S, Zemojtel T, Spielmann M, Jäger M, Hochheiser H, Washington NL, McMurry JA, Haendel MA, Mungall CJ, Lewis SE, Groza T, Valentini G, Robinson PN. 2016. A Whole-Genome Analysis Framework for Effective Identification of Pathogenic Regulatory Variants in Mendelian Disease. Am. J. Hum. Genet 99: 595–606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sparks TN, Lianoglou BR, Adami RR, Pluym ID, Holliman K, Duffy J, Downum SL, Patel S, Faubel A, Boe NM, Field NT, Murphy A, Laurent LC, Jolley J, Uy C, Slavotinek AM, Devine P, Hodoglugil U, Van Ziffle J, Sanders SJ, MacKenzie TC, Norton ME, University of California Fetal–Maternal Consortium, University of California, San Francisco Center for Maternal–Fetal Precision Medicine. 2020. Exome Sequencing for Prenatal Diagnosis in Nonimmune Hydrops Fetalis. N. Engl. J. Med 383: 1746–1756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stanley KE, Giordano J, Thorsten V, Buchovecky C, Thomas A, Ganapathi M, Liao J, Dharmadhikari AV, Revah-Politi A, Ernst M, Lippa N, Holmes H, Povysil G, Hostyk J, Parker CB, Goldenberg R, Saade GR, Dudley DJ, Pinar H, Hogue C, Reddy UM, Silver RM, Aggarwal V, Allen AS, Wapner RJ, Goldstein DB. 2020. Causal Genetic Variants in Stillbirth. N. Engl. J. Med 383: 1107–1116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Talkowski ME, Rosenfeld JA, Blumenthal I, Pillalamarri V, Chiang C, Heilbut A, Ernst C, Hanscom C, Rossin E, Lindgren AM, Pereira S, Ruderfer D, Kirby A, Ripke S, Harris DJ, Lee J-H, Ha K, Kim H-G, Solomon BD, Gropman AL, Lucente D, Sims K, Ohsumi TK, Borowsky ML, Loranger S, Quade B, Lage K, Miles J, Wu B-L, Shen Y, Neale B, Shaffer LG, Daly MJ, Morton CC, Gusella JF. 2012. Sequencing chromosomal abnormalities reveals neurodevelopmental loci that confer risk across diagnostic boundaries. Cell 149: 525–537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vora NL, Powell B, Brandt A, Strande N, Hardisty E, Gilmore K, Foreman AKM, Wilhelmsen K, Bizon C, Reilly J, Owen P, Powell CM, Skinner D, Rini C, Lyerly AD, Boggess KA, Weck K, Berg JS, Evans JP. 2017. Prenatal exome sequencing in anomalous fetuses: new opportunities and challenges. Genet. Med 19: 1207–1216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wapner RJ, Martin CL, Levy B, Ballif BC, Eng CM, Zachary JM, Savage M, Platt LD, Saltzman D, Grobman WA, Klugman S, Scholl T, Simpson JL, McCall K, Aggarwal VS, Bunke B, Nahum O, Patel A, Lamb AN, Thom EA, Beaudet AL, Ledbetter DH, Shaffer LG, Jackson L. 2012. Chromosomal microarray versus karyotyping for prenatal diagnosis. N. Engl. J. Med 367: 2175–2184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Warburton D 1991. De novo balanced chromosome rearrangements and extra marker chromosomes identified at prenatal diagnosis: clinical significance and distribution of breakpoints. Am. J. Hum. Genet 49: 995–1013. [PMC free article] [PubMed] [Google Scholar]
- Washington NL, Haendel MA, Mungall CJ, Ashburner M, Westerfield M, Lewis SE. 2009. Linking human diseases to animal models using ontology-based phenotype annotation. PLoS Biol 7: e1000247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- García-Santiago FA, Martínez-Payo C, Mansilla E, Santos-Simarro F, Ruiz de Azua Ballesteros M, Mori MÁ, Antolín Alvarado E, Nieto Y, Vallcorba I, Tenorio J, Nevado J, Lapunzina P. Prenatal ultrasound findings in Koolen-de Vries foetuses: Central nervous system anomalies are frequent markers of this syndrome. Mol Genet Genomic Med 2021. May;9(5):e1649. doi: 10.1002/mgg3.1649. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhao M, Havrilla JM, Fang L, Chen Y, Peng J, Liu C, Wu C, Sarmady M, Botas P, Isla J, Lyon GJ, Weng C, Wang K. 2020. Phen2Gene: rapid phenotype-driven gene prioritization for rare diseases. NAR Genom Bioinform 2: lqaa032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zurek B, Ellwanger K, Vissers LELM, Schüle R, Synofzik M, Töpf A, de Voer RM, Laurie S, Matalonga L, Gilissen C, Ossowski S, ‘t Hoen PAC, Vitobello A, Schulze-Hentrich JM, Riess O, Brunner HG, Brookes AJ, Rath A, Bonne G, Gumus G, Verloes A, Hoogerbrugge N, Evangelista T, Harmuth T, Swertz M, Spalding D, Hoischen A, Beltran S, Graessner H, Solve-RD consortium. 2021. Solve-RD: systematic pan-European data sharing and collaborative analysis to solve rare diseases. Eur. J. Hum. Genet 29: 1325–1331. [DOI] [PMC free article] [PubMed] [Google Scholar]