

Abstract
Background:
Social anxiety disorder (SAD) is common, first-line treatments are often only partially effective, and reliable predictors of treatment response are lacking. Here, we assessed resting state functional connectivity (rsFC) at pre-treatment and during early treatment as a potential predictor of response to a novel attention bias modification procedure, gaze-contingent music reward therapy (GC-MRT).
Methods:
32 adults with SAD were treated with GC-MRT. rsFC was assessed with multi-voxel pattern analysis (MVPA) of fMRI at pre-treatment and after 2–3 weeks. For comparison, 20 healthy control (HC) participants without treatment were assessed twice for rsFC over the same time period. All SAD participants underwent clinical evaluation at pre-treatment, early-treatment (week 2–3), and post-treatment.
Results:
SAD and depressive symptoms improved significantly from pre-treatment to post-treatment. After 2–3 weeks of treatment, decreased connectivity between the executive control network (ECN) and salience network (SN), and increased connectivity within the ECN predicted improvement in SAD and depressive symptoms at week 8. Increased connectivity between the ECN and default mode network (DMN) predicted greater improvement in SAD but not depressive symptoms at week 8. Connectivity within the DMN decreased significantly after 2–3 weeks of treatment in the SAD group, while no changes were found in HC over the same time interval.
Conclusion:
We identified early changes in rsFC during a course of GC-MRT for SAD that predicted symptom change. Connectivity changes within the ECN, ECN-DMN and ECN-SN may be related to mechanisms underlying the clinical effects of GC-MRT and warrant further study in controlled trials.
Keywords: social anxiety disorder, resting state fMRI, gaze-contingent music reward therapy, attention bias modification, neuroimaging
INTRODUCTION
Social anxiety disorder (SAD) is one of the most common psychiatric disorders, with a 5–12% lifetime prevalence and high chronicity and impairment (Kessler et al., 2005; Schneier et al., 1994). Current first-line treatments, such as cognitive behavioral therapy (CBT) and serotonin reuptake inhibitors (SSRIs), are only partially effective for most patients (Schneier, 2011; Springer, Levy, & Tolin, 2018), highlighting the need for new interventions addressing novel treatment targets. Biased attention allocation is a characteristic of SAD that has emerged as a promising target of treatment. Among individuals with SAD, visual attention is biased toward socially threatening stimuli, and some controlled trials have shown that, systematic modification of this bias can reduce SAD symptoms (Heeren, Mogoase, Philippot, & McNally, 2015; Lazarov et al., 2018; Lazarov, Pine, & Bar-Haim, 2017).
Gaze-contingent music reward therapy (GC-MRT) is a novel computer-based attention bias modification procedure. It tracks eye gaze as participants view matrices of 16 faces, half with neutral and half with threatening (i.e., disgust) expressions. Participants’ chosen music plays only when gaze is directed at neutral faces but stops when attention is allocated to any of the threat faces (Lazarov et al., 2017). Through this musical reinforcement, participants gradually learn to preferentially allocate their attention to the non-threat (i.e., neutral) faces. In a randomized controlled trial, eight sessions of GC-MRT delivered over a period of four weeks elicited greater clinical improvement than a control condition (Lazarov et al., 2017), and changes in attention allocation were observed beginning with the first week of treatment.
While GC-MRT has been shown to modulate attention to threat assessed at the level of gaze behavior (Lazarov et al., 2017; Shamai-Leshem, Lazarov, Pine, & Bar-Haim, 2021), the neural mechanisms underlying GC-MRT effects remain to be explored. The goal of the present study was to address this gap in knowledge by assessing resting state functional connectivity (rsFC) of neural networks before and at an early stage of GC-MRT in patients with SAD. Prior studies of resting state functional magnetic resonance imaging (rs-fMRI) in SAD have identified abnormalities in networks that underlie threat processing (Prater, Hosanagar, Klumpp, Angstadt, & Phan, 2013), social cognition (Choi, Shin, Ku, & Kim, 2016), and attention (Liao, Chen, et al., 2010) including the executive control network (ECN), the salience network (SN), and the default mode network (DMN). The ECN is engaged by high-level cognitive functions and consists of middle frontal gyrus (MFG), superior frontal gyrus (SFG), inferior frontal gyrus (IFG), orbitofrontal cortex (OFC), inferior and middle temporal gyri (ITG, MTG), and superior and inferior parietal lobe (SPL, IPL) (Shirer, Ryali, Rykhlevskaia, Menon, & Greicius, 2012a, 2012b). Decreased connectivity within the ECN has been reported in SAD and depression and may underlie deficits in cognition and attention that are commonly observed in SAD and depression (Ding et al., 2011), contributing to symptoms such as difficulty concentrating or regulating emotions (Zhao, Swati, Metmer, Sang, & Lu, 2019). The SN, consisting mainly of the amygdala, insula, and dorsal anterior cingulate cortex (dACC), plays a central role in detecting salience, either internally or externally-generated, and directing attention allocation and cognitive response via its functional connectivity with other distributed networks (Menon & Uddin, 2010). The SN may also play a critical role in orchestrating the toggling between ECN and DMN to allocate attentional resources toward whichever network is needed, and in signaling salience to the ECN for cognitive control (Sylvester et al., 2012). A body of research also suggests that anxiety and depressive disorders, including SAD, are characterized by altered rsFC within the DMN (Coutinho et al., 2016; Hamilton et al., 2011; Lucherini Angeletti, Scalabrini, Ricca, & Northoff, 2021; Zhou et al., 2010). The DMN, consisting of parahippocampus/hippocampus, PCC, precuneus, and mPFC, has been implicated in self-referential processing (Qin & Northoff, 2011), mind-wandering (Fox, Spreng, Ellamil, Andrews-Hanna, & Christoff, 2015) and memory (Ward et al., 2014).
No studies to date have explored the relation between rsFC and attention bias modification (ABM) treatment outcomes in SAD, although one study has assessed rsFC measuring low-frequency fluctuations (ALFF) in subthreshold depression participants (H. Li et al., 2016). Findings revealed that ABM treatment significantly reduced the amplitude of ALFF of right anterior insula and right middle frontal gyrus and between right anterior insula and the right insula. In addition, three studies have examined rsFC using an amygdala seed as a predictor or correlate of CBT response, with mixed results (Klumpp, Keutmann, Fitzgerald, Shankman, & Phan, 2014; Whitfield-Gabrieli et al., 2016; Yuan et al., 2016). Yet, a seed-based approach may miss meaningful rsFC changes not hypothesized a priori. Multi-voxel pattern analysis (MVPA) has gained traction in recent years as a data-driven approach to map spatially distributed patterns of brain activation and/or rsFC. This approach examines whole-brain distributed neural activation patterns, leveraging the fact that brain function consists of spatially distributed processes (Davis et al., 2014). MVPA was used as an additional assessment of pre-treatment rsFC in the third study above (Whitfield-Gabrieli et al., 2016), which found that MVPA results were the strongest predictor of CBT outcome in a model that included seed-based rsFC, whole-brain MVPA rsFC, diffusion-weighted MRI fractional anisotropy (FA), and pretreatment clinical severity ratings.
The present study used MVPA with rsfMRI at pre-treatment and after 2–3 weeks of treatment to detect early neural changes that might predict clinical symptom changes after treatment completion (after 8 weeks). This was part of a larger clinical trial designed as an initial step toward clarifying the mechanisms of GC-MRT and optimizing its duration. GC-MRT in the original study (Lazarov et al., 2017) included 8 sessions delivered over 4 weeks (i.e., 2 sessions per week); in the current study, adults with SAD were treated with either a 4-week (8 session) or 8-week (12 session) course of GC-MRT treatment (Supplementary Figure 2). Healthy control (HC) participants were also assessed twice for rsFC over a 2–3 week time interval but did not receive GC-MRT. The present study had three goals. First, we examined whether changes in rsFC from pre-treatment to week 2–3 were associated with changes in clinical features that might be associated with GC-MRT response — namely, severity of social anxiety, depression, anhedonia, and attention control at week 2–3 and at week 8 (when clinical symptom change was expected to be maximal). We hypothesized that in the SAD group, the early change in rsFC within ECN, DMN and between ECN-SN would associated with clinical changes. Second, we compared changes in rsFC from pre-treatment to week 2–3 in SAD to changes in the untreated HC group over the same 2–3 week interval. We expected that in the untreated HC group there would be no significant changes in rsFC over a 2–3 week interval, and so predicted that rsFC changes would be greater in the SAD group. Finally, we also explored pre-treatment rsFC predictors of response to GC-MRT, as measured by SAD symptoms and other clinical features at week 8.
METHODS
Participants
The sample included 44 patients with SAD and 20 HC. All participants underwent a clinical evaluation and an initial resting state MRI scan. Thirty-three SAD and 20 HC participants returned for a second scan 2–3 weeks after the first (The 33 SAD completers had a mean of 4.9 sessions [std: 1.1] over 18.2 days [std: 5.5], the 20 HC had a mean of 18 days [std: 5.8]) before they had the second MRI scan). Eleven SAD participants completed only the pre-treatment MRI scan: Five did not complete a second scan due to scheduling difficulties, and six were dropped due to COVID-19 travel restrictions (Supplemental Figure 1). Tables 1 and 2 summarize demographic information and clinical outcomes of SAD treatment completers and HC. Among the 33 SAD participants, four were in stable pre-existing treatment (supportive psychotherapy (N=1); serotonin reuptake inhibitor pharmacotherapy (N=3)). The New York State Psychiatric Institute Institutional Review Board approved the study, and participants provided written informed consent.
Table 1:
Demographic table for SAD and HC
| SAD | HC | |
|---|---|---|
| N | 33 | 20 |
| Age | 28.06 (6.57) | 28.65 (6.18) |
| Gender (F/M) | 21/12 | 12/8 |
| Race | White 14 (42.4%) | White 10 (50%) |
| Black 6 (18.2%) | Black 6 (30%) | |
| Asian 6 (18.2%) | Asian 4 (20%) | |
| Others 7 (21.2%) | Others 0 (0%) |
Table 2:
Descriptive statistics and paired t-tests of clinical outcomes at pre-treatment, early-treatment- (week 2–3), and week 8.
| Pre-treatment | Early-treatment | Week 8 | Pre - Early | Pre-Week 8 | |||
|---|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | t | p | t | p | |
| LSAS | 86.06 (15.39) | 75.96 (22.64) | 63.24 (28.71) | 2.82 | 0.01 | 4.21 | <0.0001 |
| HAM-D | 6.18 (4.81) | 4.27 (3.66) | 4.33 (4.11) | 2.50 | 0.019 | 2.20 | 0.035 |
| SHAPS | 24.82 (5.55) | 23.94 (5.25) | 23.42 (6.10) | 1.53 | 0.14 | 1.39 | 0.18 |
| ACS | 44.76 (5.91) | N.A. | 47.68 (7.94) | NA | N.A. | −1.46 | 0.16 |
| RSAS | 17.03 (5.96) | 16.41 (7.74) | 15.03 (8.21) | 0.87 | 0.39 | 2.42 | 0.021 |
Note: LSAS: Liebowitz Social Anxiety Scale; HAM-D: Hamilton Rating Scale for Depression; SHAPS: Snaith-Hamilton Pleasure Scale; ACS: Attention Control Scale (not assessed at during treatment); RSAS: Revised Social Anhedonia Scale.
General Procedure
MRI procedures were part of a broader clinical trial assessing mechanisms of GC-MRT and comparing the previously established 4-week (8 sessions) course of treatment (Lazarov et al., 2017) to a course augmented by four additional weekly sessions from week 5 to 8 (Supplemental Figure 2). Hence, SAD participants were randomized to a treatment duration of either 4 weeks or 8 weeks, with randomization stratified by presence or absence of pre-existing medication treatment. All participants underwent clinical evaluation at pre-treatment, early-treatment (week 2–3), and week 8, with measures of social anxiety, attention control, depression, and anhedonia. Depression and anhedonia were assessed due to their potential impact on the GC-MRT process of positive reinforcement. In this study the two groups (4-week vs 8-week) did not differ in symptomatic improvement after 8 weeks (change in LSAS total score at week 8 was −23.68 for the 8-week group and −22.38 for the 4-week group; t= −0.13, df=33, p=0.901), so the groups were pooled for imaging analyses.
GC-MRT
The eye-tracking attention modification task was identical to the one used in our previous study in SAD (Lazarov et al., 2017). During each session of GC-MRT, 30 consecutive 4X4 matrices, each comprising 16 faces (one from each actor), eight with a disgusted facial expression (i.e., socially threatening stimuli) and eight with a neutral one (i.e., neutral stimuli), were presented to participants, with each matrix presented for 24 seconds (see Figure 1 for an example of a single matrix). Before the training session started, patients were asked to choose music that would be used during the session (and after each training session patients rated on a 0–10 scale how much they liked the music played at that session). Next, a 5-point gaze calibration, followed by 5-point validation, was completed. Calibration was repeated if visual deviation was > 0.5 degrees on the X or Y axis of any of the calibration points, and training began only when calibration parameters were achieved. After calibration and validation, the GC-MRT session started, during which the chosen music played contingent on the participants’ gaze -- when the participant fixated on one of the neutral faces the music played, but fixating on any of the threat faces stopped the music. Patients were asked to view each face matrix freely in any way they chose, without additional instructions. Each GC-MRT session was approximately 20 minutes long and used the Eye-Link 1000 plus eye-tracker running Experiment Builder software (SR Research Ltd., Mississauga, Ontario, Canada). Operating distance to the eye-tracking monitor was about 70 cm. The stimuli were presented on a monitor with 1920×1080 pixel resolution.
Figure 1:
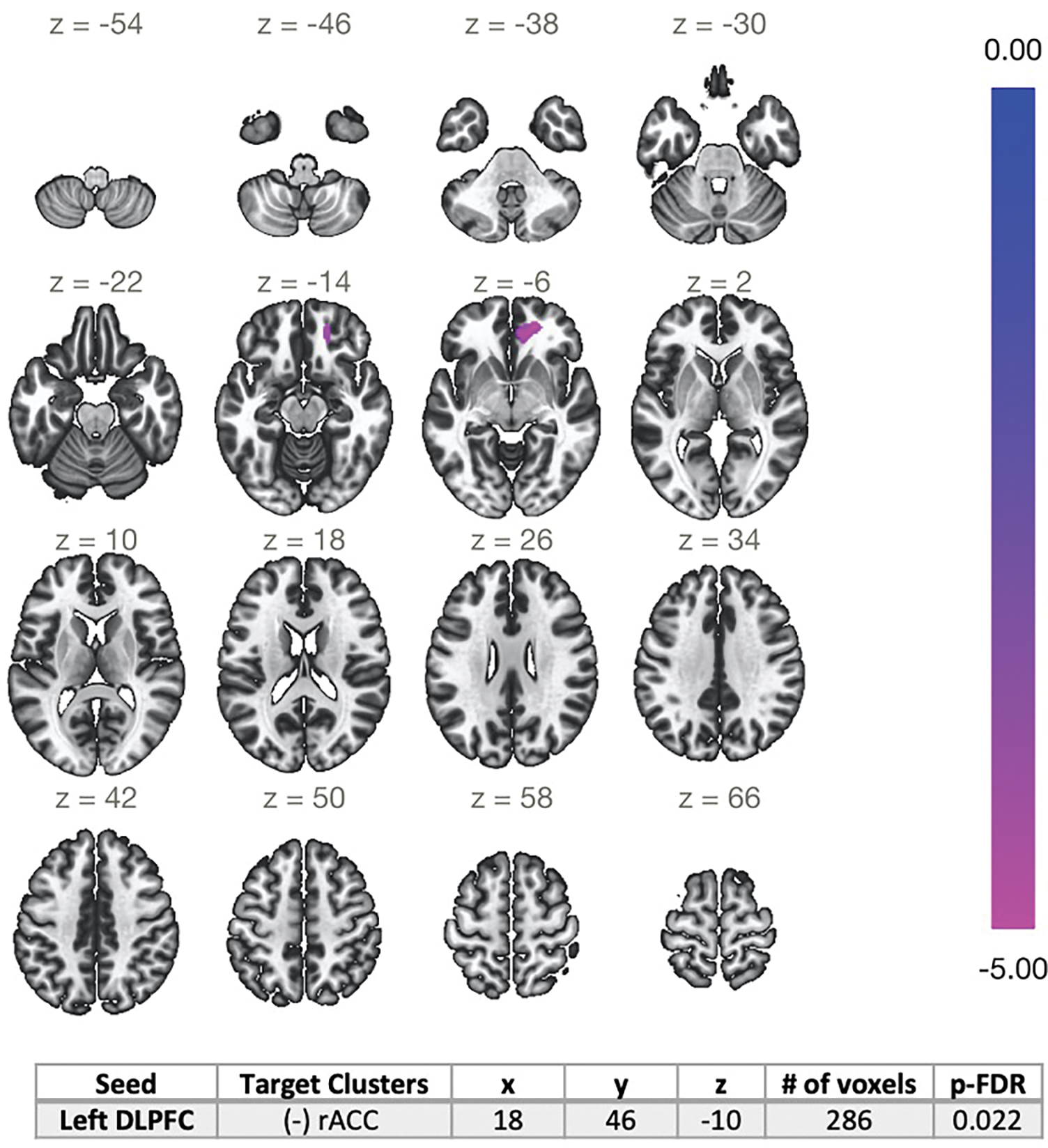
Seed-based whole-brain correlation analysis of changes in rsFC at week 2–3 that were associated with changes in LSAS after week 8 (pre-treatment -Week 8). Left DLPFC was used as the seed. Early decreases in rsFC between the left DLPFC-rACC predicted greater improvement in social anxiety at week 8. rsFC: resting state functional connectivity; LSAS: Liebowitz Social Anxiety Scale; DLPFC: dorsolateral prefrontal cortex; rACC: rostral anterior cingulate cortex [18, 46, −10].
Neuroimaging Procedures
Neuroimaging data acquisition
MRI data were acquired just prior to the first treatment session, and again after 2–3 weeks of treatment. Thirteen participants were scanned using a 3T General Electric MR750, and 20 participants were scanned using a 3T General Electric PREMIER (GE Medical Systems, Waukesha, WI, USA) due to a scanner upgrade that occurred during the trial. A harmonized imaging scanning protocol was used for both scanners. The scanner (indicated as 0/1) was included as nuisance regressors in all the rs-fMRI analysis. For each participant, both sessions used the same scanner. A 32-channel receive-only head coil was used. For each participant a high-resolution T1-weighted 3D BRAVO sequence was acquired using the following parameters: TR=450 mm, Flip angle=12°, field of view=25.6 cm, 256×256 matrix, slice thickness=1 mm. Ten-minute eyes-open resting state scans were acquired with TR=2 sec, TE=30 msec, FA =77°, FOV =22 cm, slice thickness=4 mm, number of volumes=300.
Functional connectivity analysis
Imaging processing is described in the Supplemental Material. We applied MVPA for model-free voxel-wise rsFC analysis using the CONN toolbox (Whitfield-Gabrieli & Nieto-Castanon, 2012). We used this approach to (1) identify regions/seeds where change in rsFC was associated with change in a specific clinical outcome measure in SAD from pre-treatment to week 2–3, or pre-treatment to week 8, and (2) identify regions/seeds of changes in rsFC from pre-treatment to week 2–3 in patients with SAD, within HC only, and in SAD vs. HC. Of the five prespecified clinical measures, only those that changed significantly from pre-treatment to week 2–3 or week 8 were analyzed (i.e., LSAS, HAM-D, and RSAS). To assess the changes in rsFC from pre-treatment to week 2–3, a second F test was carried out comparing within-subject variance across all voxels’ connectivity patterns in SAD and HC, controlling for scanner. Post-hoc analyses were performed using these identified clusters of voxels as seeds in standard seed-to-voxel analyses, and testing the association between seed-to-whole-brain connectivity and clinical outcomes or group by session interaction. Clusters surviving a height threshold of p < .001 and FWE cluster-level threshold of p < .05 were taken for post-hoc analysis. The same threshold was applied for post-hoc seed-to-whole-brain rsFC analysis.
RESULTS
Treatment results
Severity of social anxiety (LSAS), depression (HAM-D) and social anhedonia (RSAS) improved significantly from pre-treatment to week 8 (Table 2). General anhedonia, as assessed by the SHAPS, and attention control, assessed by the ACS, did not change significantly from pre-treatment to either week 2–3 or week 8. In the absence of changes in SHAPS or ACS scores, we were unable to assess the rsFC associated with the hypothesized changes.
The 33 SAD completers and the 11 SAD participants that did not provide a second scan did not differ in age, sex, or baseline clinical measures (LSAS, HAM-D, RSAS, SHAPS, ACS; p>0.05). The 33 SAD completers had an average of 4.9 sessions (std: 1.1) and an average of 18.2 days (std: 5.5) of treatment before they had the second MRI scan.
Across all GCMRT sessions, the mean rating of how much they liked the music was 7.35 (std: 2.10), confirming that the selected music had reinforcement value, as expected.
1. Early rsFC changes predicting symptom improvement
a). In social anxiety symptoms measured by LSAS
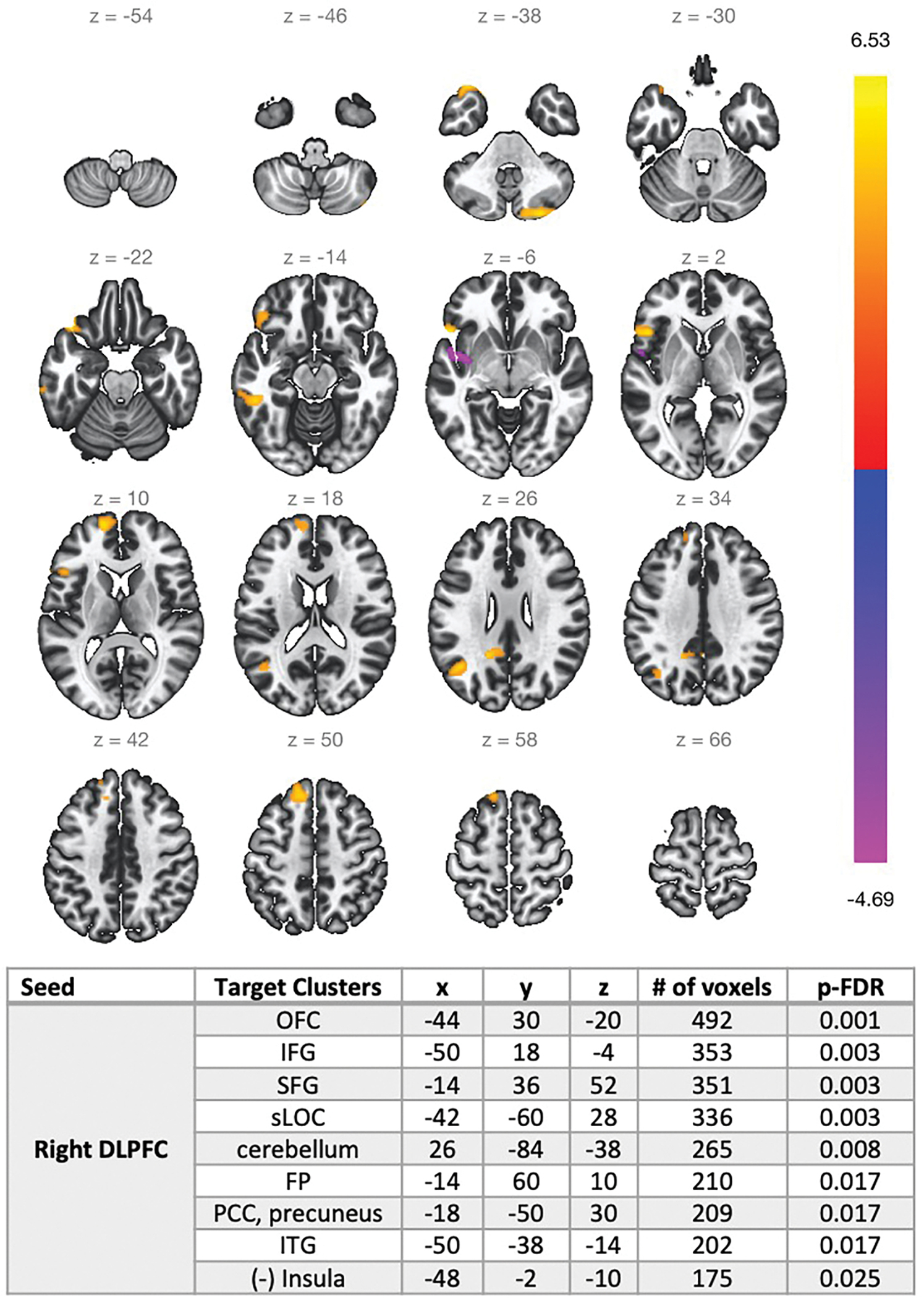
In SAD participants, MVPA analysis revealed two significant clusters, located in the left dorsolateral prefrontal cortex (DLPFC) [−32 48 34] and right DLPFC [28 54 26], with rsFC changes at week 2–3 that predicted change in social anxiety (ΔLSAS at week 8). Spatial localizations of the two brain clusters (left and right DLPFC) were within the executive control network (ECN) (see supplemental Figure 3). Early decreases in rsFC between the left DLPFC- rostral anterior cingulate cortex (rACC) and right DLPFC-Insula, respectively (ECN-salience network [SN]) predicted greater improvement in social anxiety at week 8 (Figure 1, 2). Early increases within the right DLPFC-orbital-frontal cortex (OFC)/superior frontal gyrus (SFG)/inferior temporal gyrus (ITG) (within ECN), and between right DLPFC-PCC/precuneus (ECN-default mode network [DMN]) predicted greater improvement in social anxiety at week 8 (Figure 2). Controlling for level of depression or presence of concomitant medication did not change the findings (see supplemental Figures 6 and 7).
Figure 2:
Seed-based whole-brain correlation analysis of changes in rsFC at week 2–3 that were associated with changes in LSAS after week 8 (pre-treatment -Week 8). Right DLPFC was used as the seed. Early decreases in rsFC between the right DLPFC-Insula, and early increase in rsFC between the right DLPFC -OFC/SFG/ ITG, and between right DLPFC-PCC/precuneus predicted greater improvement in social anxiety at week 8. rsFC: resting state functional connectivity; LSAS: Liebowitz Social Anxiety Scale; OFC: orbitofrontal cortex; DLPFC: dorsolateral prefrontal cortex; IFG: inferior frontal gyrus; SFG: superior frontal gyrus; sLOC: Lateral Occipital Cortex, superior division; FP: frontal pole; PCC: posterior cingulate cortex; ITG: inferior temporal gyrus.
Post-hoc tests assessed whether the rsFC changes that predicted LSAS reduction at week 8 were also associated with early changes in LSAS at week 2–3 (i.e., concurrently with fMRI at early-treatment). The whole-brain connectivity maps with two seeds located in left and right DLPFC were not significantly associated with the LSAS outcome at week 2–3.
b). In depression symptoms measured by HAM-D
In SAD participants, MVPA analysis revealed three significant clusters at week 2–3 that predicted change in depression (ΔHAM-D at week 8), located in the superior lateral occipital cortex (sLOC) [34 −66 24], and posterior inferior temporal gyrus (pITG) (left: [−62 −34 −30] and right [56 −18 −34]). The spatial localization of the three brain clusters (sLOC within visual network, and bilateral pITG within ECN) is displayed in Supplemental Figure 8. Greater improvement in depression at week 8 was predicted by early decrease in rsFC between the left pITG and Insula and between right pITG and ACC (ECN-SN), and early increase in rsFC of bilateral pITG-PFC (within ECN) (Supplemental Figure 9). No significant associations were found with the sLOC seed region.
Post hoc tests assessed whether ΔrsFC was associated with ΔHAM-D assessed concurrently with MRI at week 2–3. For both seed regions, no significant association was found with HAM-D outcome at week 2–3.
c). In social anhedonia symptom measured by the RSAS
The MVPA analysis did not reveal any significant clusters of change in rsFC that were associated with change in RSAS at early-treatment or week 8.
2. Early changes in functional connectivity associated with GC-MRT
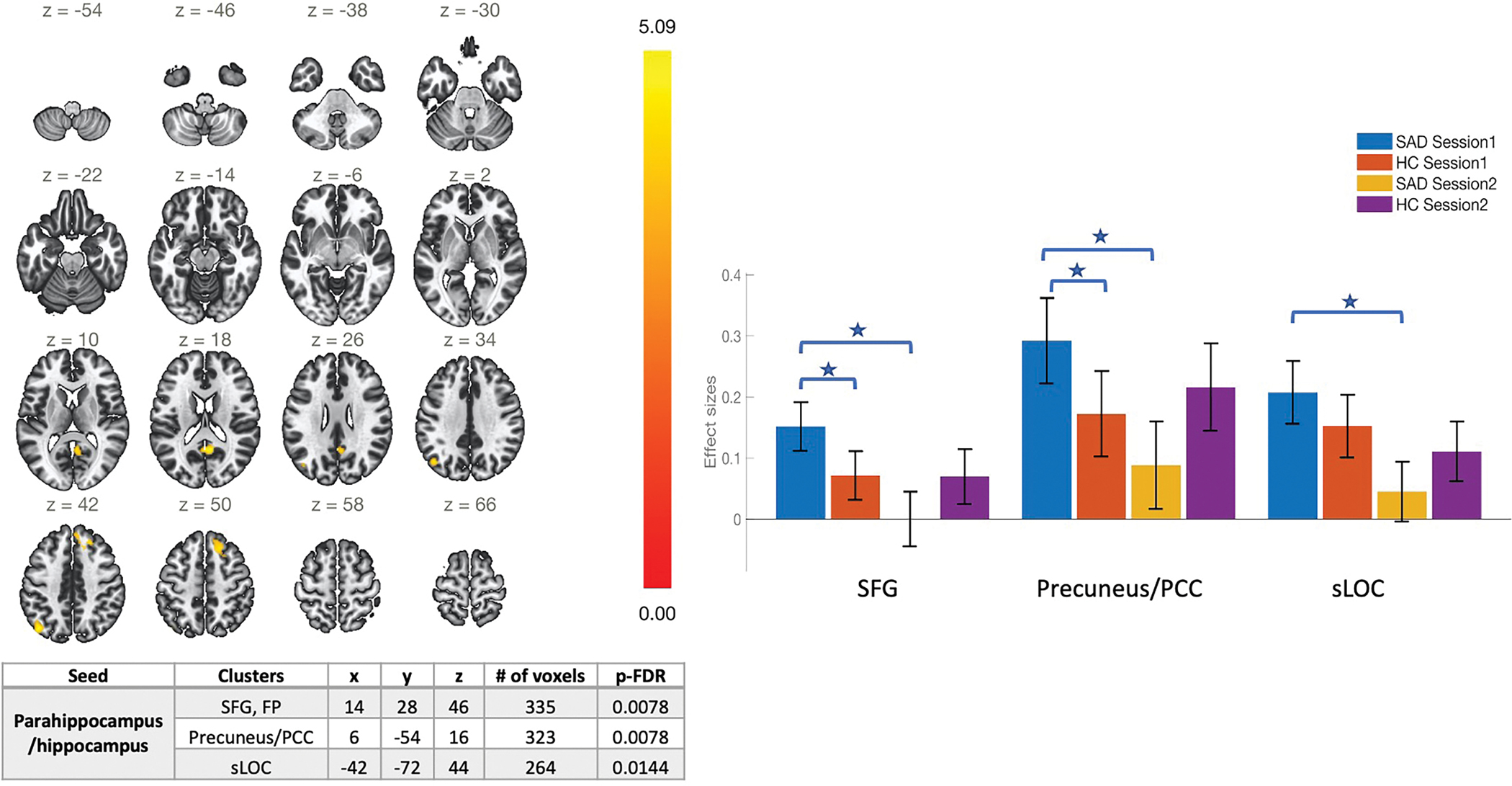
In SAD participants, MVPA analysis of change in rsFC from pre-treatment to week 2–3 revealed one significant cluster in the parahippocampus and hippocampus (HIP) (Supplemental Figure 5). Using this cluster, a seed-based whole-brain correlation analysis of rsfMRI data, corrected for multiple comparisons at cluster level (peak level: p < 0.001, uncorrected; cluster level: p < 0.05 FDR-corrected), showed significant decreases in connectivity within the default mode network (DMN). Specifically, from pre-treatment to week 2–3, there were significant decreases in rsFC (ΔrsFC) of HIP with posterior cingulate cortex (PCC)/precuneus, SFG and sLOC (Figure 3). In HC, MVPA analysis revealed no significant clusters from pre-treatment to week 2–3. Post-hoc analysis also revealed significantly higher within-DMN connectivity (HIP-PCC/precuneus, HIP-SFG) at pre-treatment in SAD, compared with HC. No significant differences were found between HC and SAD at week 2–3 (Figure 3).
Figure 3.
For Parahippocampus/hippocampus (HIP) seed region, connectivity decreased significantly from pre- to early-treatment within the DMN (HIP-PCC/precuneus), and between HIP and SFG. Note: HIP: hippocampus, SFG: superior frontal gyrus, PCC: posterior cingulate cortex; sLOC: lateral occipital cortex, superior division, x y z are MNI coordinates. DMN: default mode network.
To understand whether these early changes in rsFC were associated with changes in clinical symptoms in SAD group, post-hoc tests assessed the association between ΔrsFC in these three pathways and changes in symptom scores (ΔLSAS, ΔHAM-D) concurrently at week 2–3, and later at week 8. No significant associations were found with clinical symptom change at either time point.
3. Pre-treatment rsFC predictive of improvement in social anxiety and depression
The MVPA analysis did not reveal any significant clusters of pre-treatment rsFC that were associated with change in social anxiety or depression at week 8.
DISCUSSION
GC-MRT is a novel computer-based treatment that has been shown to reduce attention to socially threatening stimuli and to improve clinical symptoms in patients with SAD (Lazarov et al., 2017), yet its neural mechanisms of action have not been previously studied. This study used resting state fMRI to investigate changes in intrinsic whole-brain functional network connectivity associated with GC-MRT, and to explore their relationship with improvement in clinical symptoms during treatment. Social anxiety, depression and social anhedonia all improved significantly from pre- to post-treatment in SAD individuals. We identified early changes in brain rsFC (decreased ECN-SN connectivity, and increased connectivity within the ECN, and between ECN and the DMN) that were associated with greater improvement in social anxiety at post-treatment (week 8) and early changes in rsFC within ECN and ECN-SN that were associated with improvement in depression. We also found significantly decreased connectivity within the DMN after 2–3 weeks of treatment in SAD group, while no changes were found in HC over the same time interval. Taken together, these findings suggest that connectivity changes within the ECN and ECN-DMN and ECN-SN may be related to mechanisms of the clinical effects of GC-MRT, warranting further research in randomized controlled trials.
Early changes in rsFC that were associated with improvement in social anxiety included increases within the ECN (right DLPFC-OFC/SFG). Our finding of an early increase in rsFC within the ECN predicting improvement in social anxiety and depressive symptoms is consistent with GC-MRT potentially enhancing attention control, and rsFC may be more sensitive in this regard than our self-report measure of attention control, which did not change during treatment. The increase of rsFC within ECN at this early stage of treatment, at which time improvement in the primary clinical outcome (LSAS) was modest (though statistically significant), suggests that rsFC changes might precede symptomatic response, though this would need to be validated by repeated assessment of rsFC and symptoms at additional time points. Moreover, previous studies have shown that decreased within-ECN connectivity correlated with symptom severity in major depressive disorder (Pan et al., 2020). These results are consistent with our finding that an early increase of rsFC within ECN predicted improvement in depression symptoms.
In addition, we found that an early decrease in ECN-SN rsFC predicted improvement in both social anxiety and depression. The early decrease in ECN-SN rsFC may reflect reduced sensitivity to salience and enhanced cognitive control, which might in turn reduce anxiety and depression (Menon & Uddin, 2010). Compared with healthy controls, SAD patients have been found to exhibit increased connectivity within the SN, possibly related to hypervigilance to external stimuli (Northoff, 2020; Straube, Schmidt, Weiss, Mentzel, & Miltner, 2009). Studies have inconsistent findings on changes of SN and ECN in GAD, SAD and depression, for example, some studies found decreased connectivity between key nodes in the SN and the ECN in GAD (Etkin, Prater, Schatzberg, Menon, & Greicius, 2009; Kim, Gee, Loucks, Davis, & Whalen, 2011), SAD (Liao, Qiu, et al., 2010), and depression (Ellard et al., 2018), while other studies found increased rsFC of SN to ECN in depression (Liu et al., 2021) and this increased ECN-SN was correlated with overall depression severity (W. Li et al., 2017).
We also found that an early increase in ECN-DMN (right DLPFC -PCC/precuneus) rsFC predicted improvement specifically in social anxiety, but not depression. Prior work has shown that better cognitive performance (as measured by working memory and attention tasks) is associated with greater connectivity between the ECN and the DMN, suggesting that these functions may depend upon coupling of these networks (Albert, Potter, Boyd, Kang, & Taylor, 2019; Liang, Zou, He, & Yang, 2016). Moreover, aberrant ECN-DMN connectivity may reflect ongoing rumination, or an underlying bias for control systems to allocate resources towards internal thoughts at the cost of engaging with the external world (Kaiser, Andrews-Hanna, Wager, & Pizzagalli, 2015). Decreased ECN-DMN has been reported in anxiety disorders (Xu et al., 2019). The increased ECN-DMN rsFC we found in SAD may reflect improvement in cognitive functioning, better executive control related to mind-wandering or worry, and less rumination (Sylvester et al., 2012). Finally, the association between increased ECN-DMN rsFC and change in social anxiety but not depression may reflect either true specificity or only that GC-MRT exerted larger effects on social anxiety than depression in our study.
Interestingly, our findings of early changes in brain rsFC (decreased ECN-SN connectivity, and increased connectivity within the ECN, and between ECN and the DMN) that were associated with greater improvement in social anxiety at week 8 were not consistent with findings of previous studies of CBT treatment in SAD (Choi et al., 2016; Prater et al., 2013; Whitfield-Gabrieli et al., 2016). Our study differed in utilizing GC-MRT and in assessing brain changes occurring early in treatment rather than using pre-treatment rsFC to predict treatment outcomes. Additionally, we used a data-driven approach examining the rsFC of all voxels in the brain without an a priori hypothesis of a seed region, while most studies prespecified amygdala as the seed region.
Finally, we found significantly higher connectivity within the DMN at pre-treatment in SAD compared with HC, while after 2–3 weeks of treatment there was decreased connectivity within the DMN in SAD group and no changes were found in HC over the same time interval. One previous study also showed increased DMN activity in socially anxious individuals during reward processing, consistent with high self-focused attention even while engaging with potentially rewarding stimuli (Maresh, Allen, & Coan, 2014). A recent review, however, reported hypoconnectivity within DMN in patients with SAD (Lucherini Angeletti et al., 2021). The discrepancy may relate to the review’s focus on cortical regions and exclusion of the hippocampus from the posterior DMN. Many other studies have included the hippocampus as part of the posterior DMN (Mulders, van Eijndhoven, Schene, Beckmann, & Tendolkar, 2015), as we did. The posterior DMN is implicated in episodic memory retrieval through its connection with temporal structures including the hippocampus (Andrews-Hanna, Reidler, Huang, & Buckner, 2010). The hippocampus is an important brain region implicated in both general anxiety and fear memory.
Our finding that DMN connectivity (HIP-PCC/precuneus/FP) decreased significantly after 2–3 weeks of GC-MRT treatment in patients with SAD suggests that GC-MRT may have early effects on DMN rsFC, and normalized it to the levels of HC. This may relate to the treatment’s effect of redirecting attention away from social threat stimuli that activate self-focused attention, or alternatively to its more general effect of encouraging focused attention on external stimuli. This may also reflect a treatment effect of less social threat memory retrieval via hippocampus connectivity. However, these early FC changes were not associated with symptom changes at either early/during treatment or post-treatment, suggesting that other neural processes that are not captured by resting state measures may be more closely related to symptom change. For example, other studies have shown SAD symptoms were associated with brain activityactivity in fear, reward, attention, or executive control circuitry (Crane, Chang, Kinney, & Klumpp, 2021; Mizzi, Pedersen, Lorenzetti, Heinrichs, & Labuschagne, 2021). Further studies could assess other downstream processes by evaluating pre- to post-treatment fMRI scan, which may be more closely related to symptom change.
This study has several limitations. A key limitation is the absence of a non-GC-MRT SAD group to control for nonspecific changes in rsFC and clinical symptoms over time. The current findings will need to be confirmed in a randomized controlled trial. Additionally, while the week 2–3 assessment of rsFC was designed to detect early brain changes that might precede clinical improvement, improvement in the primary outcome was already statistically significant at week 3, though improvement became much greater at post-treatment. We cannot preclude the possibility that neural changes during the first 2–3 weeks may be related to concurrent symptom change and nonspecific factors. A more fine-grained repeated assessment using rsFC would be needed to clarify the time course of change in rsFC and clinical outcomes. Moreover, we used group-level univariate analysis with relatively small samples and 10 minute resting state scans in this study, thus we cannot make individualized prediction of treatment outcome. Further studies with larger samples and longer scans could use multivariate analysis/machine learning algorithms to handle multidimensional imaging data and predict treatment outcome at the individual level. Although this study found that extending GCMRT duration to 12 sessions did not improve clinical outcome, future research could examine other approaches to optimizing GCMRT, such as by increasing the number of faces (more or less than 16) and the presentation time (24 second per matrix). Finally, further research could collect additional behavioral measures of attention control to better understand the scope of clinical correlates of neural changes associated with GC-MRT.
Conclusion:
This initial attempt to identify early neural predictors of response to GC-MRT treatment found that early changes in rsFC within the ECN, between the ECN and DMN, and between the ECN and SN predicted clinical outcome at post-treatment. Consistent with the aim of GC-MRT to target biased attention to threat, these networks are known to play important roles in attention allocation, salience processing and cognitive control. Our preliminary findings support the value of future controlled trials utilizing rsFC to understand profiles of neural networks involved in the engagement and therapeutic action of GC-MRT in SAD.
Supplementary Material
Financial support:
This research was supported by NIMH grant R61MH116089. Dr. Zhu was supported by K01MH122774 and Brain and Behavior Research Foundation Grant.
Footnotes
Conflict of interest: Over the past 3 years, Dr. Schneier has received research funding from Otsuka Pharmaceuticals and Compass Pathways. Dr. Pizzagalli has received consulting fees from BlackThorn Therapeutics, Boehringer Ingelheim, Compass Pathways, Concert Pharmaceuticals, Engrail Therapeutics, Neurocrine Biosciences, Otsuka Pharmaceuticals, and Takeda Pharmaceuticals; one honorarium from Alkermes, and research funding from NIMH, Dana Foundation, Brain and Behavior Research Foundation, and Millennium Pharmaceuticals. In addition, he has received stock options from BlackThorn Therapeutics. There are no conflicts of interest with the work conducted in this study. All views expressed are solely those of the authors. The other authors have no financial disclosures.
Ethical standards: The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Trial Registration: ClinicalTrials.gov identifier: NCT03415022
Reference:
- Albert KM, Potter GG, Boyd BD, Kang H, & Taylor WD (2019). Brain network functional connectivity and cognitive performance in major depressive disorder. J Psychiatr Res, 110, 51–56. doi: 10.1016/j.jpsychires.2018.11.020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Andrews-Hanna JR, Reidler JS, Huang C, & Buckner RL (2010). Evidence for the default network’s role in spontaneous cognition. J Neurophysiol, 104(1), 322–335. doi: 10.1152/jn.00830.2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Choi SH, Shin JE, Ku J, & Kim JJ (2016). Looking at the self in front of others: Neural correlates of attentional bias in social anxiety. J Psychiatr Res, 75, 31–40. doi: 10.1016/j.jpsychires.2016.01.001 [DOI] [PubMed] [Google Scholar]
- Coutinho JF, Fernandesl SV, Soares JM, Maia L, Goncalves OF, & Sampaio A (2016). Default mode network dissociation in depressive and anxiety states. Brain Imaging Behav, 10(1), 147–157. doi: 10.1007/s11682-015-9375-7 [DOI] [PubMed] [Google Scholar]
- Crane NA, Chang F, Kinney KL, & Klumpp H (2021). Individual differences in striatal and amygdala response to emotional faces are related to symptom severity in social anxiety disorder. Neuroimage Clin, 30, 102615. doi: 10.1016/j.nicl.2021.102615 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davis T, LaRocque KF, Mumford JA, Norman KA, Wagner AD, & Poldrack RA (2014). What do differences between multi-voxel and univariate analysis mean? How subject-, voxel-, and trial-level variance impact fMRI analysis. Neuroimage, 97, 271–283. doi: 10.1016/j.neuroimage.2014.04.037 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ding J, Chen H, Qiu C, Liao W, Warwick JM, Duan X, . . . Gong Q (2011). Disrupted functional connectivity in social anxiety disorder: a resting-state fMRI study. Magn Reson Imaging, 29(5), 701–711. doi: 10.1016/j.mri.2011.02.013 [DOI] [PubMed] [Google Scholar]
- Ellard KK, Zimmerman JP, Kaur N, Van Dijk KRA, Roffman JL, Nierenberg AA, . . . Camprodon JA (2018). Functional Connectivity Between Anterior Insula and Key Nodes of Frontoparietal Executive Control and Salience Networks Distinguish Bipolar Depression From Unipolar Depression and Healthy Control Subjects. Biol Psychiatry Cogn Neurosci Neuroimaging, 3(5), 473–484. doi: 10.1016/j.bpsc.2018.01.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Etkin A, Prater KE, Schatzberg AF, Menon V, & Greicius MD (2009). Disrupted amygdalar subregion functional connectivity and evidence of a compensatory network in generalized anxiety disorder. Arch Gen Psychiatry, 66(12), 1361–1372. doi: 10.1001/archgenpsychiatry.2009.104 [DOI] [PubMed] [Google Scholar]
- Fox KC, Spreng RN, Ellamil M, Andrews-Hanna JR, & Christoff K (2015). The wandering brain: meta-analysis of functional neuroimaging studies of mind-wandering and related spontaneous thought processes. Neuroimage, 111, 611–621. doi: 10.1016/j.neuroimage.2015.02.039 [DOI] [PubMed] [Google Scholar]
- Hamilton JP, Furman DJ, Chang C, Thomason ME, Dennis E, & Gotlib IH (2011). Default-mode and task-positive network activity in major depressive disorder: implications for adaptive and maladaptive rumination. Biol Psychiatry, 70(4), 327–333. doi: 10.1016/j.biopsych.2011.02.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heeren A, Mogoase C, Philippot P, & McNally RJ (2015). Attention bias modification for social anxiety: A systematic review and meta-analysis. Clin Psychol Rev, 40, 76–90. doi: 10.1016/j.cpr.2015.06.001 [DOI] [PubMed] [Google Scholar]
- Kaiser RH, Andrews-Hanna JR, Wager TD, & Pizzagalli DA (2015). Large-Scale Network Dysfunction in Major Depressive Disorder: A Meta-analysis of Resting-State Functional Connectivity. JAMA Psychiatry, 72(6), 603–611. doi: 10.1001/jamapsychiatry.2015.0071 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, & Walters EE (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry, 62(6), 593–602. doi: 10.1001/archpsyc.62.6.593 [DOI] [PubMed] [Google Scholar]
- Kim MJ, Gee DG, Loucks RA, Davis FC, & Whalen PJ (2011). Anxiety dissociates dorsal and ventral medial prefrontal cortex functional connectivity with the amygdala at rest. Cereb Cortex, 21(7), 1667–1673. doi: 10.1093/cercor/bhq237 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klumpp H, Keutmann MK, Fitzgerald DA, Shankman SA, & Phan KL (2014). Resting state amygdala-prefrontal connectivity predicts symptom change after cognitive behavioral therapy in generalized social anxiety disorder. Biol Mood Anxiety Disord, 4(1), 14. doi: 10.1186/s13587-014-0014-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lazarov A, Marom S, Yahalom N, Pine DS, Hermesh H, & Bar-Haim Y (2018). Attention bias modification augments cognitive-behavioral group therapy for social anxiety disorder: a randomized controlled trial. Psychol Med, 48(13), 2177–2185. doi: 10.1017/S003329171700366X [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lazarov A, Pine DS, & Bar-Haim Y (2017). Gaze-Contingent Music Reward Therapy for Social Anxiety Disorder: A Randomized Controlled Trial. Am J Psychiatry, 174(7), 649–656. doi: 10.1176/appi.ajp.2016.16080894 [DOI] [PubMed] [Google Scholar]
- Li H, Wei D, Browning M, Du X, Zhang Q, & Qiu J (2016). Attentional bias modification (ABM) training induces spontaneous brain activity changes in young women with subthreshold depression: a randomized controlled trial. Psychol Med, 46(5), 909–920. doi: 10.1017/S003329171500238X [DOI] [PubMed] [Google Scholar]
- Li W, Wang Y, Ward BD, Antuono PG, Li SJ, & Goveas JS (2017). Intrinsic inter-network brain dysfunction correlates with symptom dimensions in late-life depression. J Psychiatr Res, 87, 71–80. doi: 10.1016/j.jpsychires.2016.12.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liang X, Zou Q, He Y, & Yang Y (2016). Topologically Reorganized Connectivity Architecture of Default-Mode, Executive-Control, and Salience Networks across Working Memory Task Loads. Cereb Cortex, 26(4), 1501–1511. doi: 10.1093/cercor/bhu316 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liao W, Chen H, Feng Y, Mantini D, Gentili C, Pan Z, . . . Zhang W (2010). Selective aberrant functional connectivity of resting state networks in social anxiety disorder. Neuroimage, 52(4), 1549–1558. doi: 10.1016/j.neuroimage.2010.05.010 [DOI] [PubMed] [Google Scholar]
- Liao W, Qiu C, Gentili C, Walter M, Pan Z, Ding J, . . . Chen H (2010). Altered effective connectivity network of the amygdala in social anxiety disorder: a resting-state FMRI study. PLoS One, 5(12), e15238. doi: 10.1371/journal.pone.0015238 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu J, Fan Y, Ling-Li Z, Liu B, Ju Y, Wang M, . . . Li L (2021). The neuroprogressive nature of major depressive disorder: evidence from an intrinsic connectome analysis. Transl Psychiatry, 11(1), 102. doi: 10.1038/s41398-021-01227-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lucherini Angeletti L, Scalabrini A, Ricca V, & Northoff G (2021). Topography of the Anxious Self: Abnormal Rest-Task Modulation in Social Anxiety Disorder. Neuroscientist, 10738584211030497. doi: 10.1177/10738584211030497 [DOI] [PubMed] [Google Scholar]
- Maresh EL, Allen JP, & Coan JA (2014). Increased default mode network activity in socially anxious individuals during reward processing. Biol Mood Anxiety Disord, 4, 7. doi: 10.1186/2045-5380-4-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Menon V, & Uddin LQ (2010). Saliency, switching, attention and control: a network model of insula function. Brain Struct Funct, 214(5–6), 655–667. doi: 10.1007/s00429-010-0262-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mizzi S, Pedersen M, Lorenzetti V, Heinrichs M, & Labuschagne I (2021). Resting-state neuroimaging in social anxiety disorder: a systematic review. Mol Psychiatry. doi: 10.1038/s41380-021-01154-6 [DOI] [PubMed] [Google Scholar]
- Mulders PC, van Eijndhoven PF, Schene AH, Beckmann CF, & Tendolkar I (2015). Resting-state functional connectivity in major depressive disorder: A review. Neurosci Biobehav Rev, 56, 330–344. doi: 10.1016/j.neubiorev.2015.07.014 [DOI] [PubMed] [Google Scholar]
- Northoff G (2020). Anxiety Disorders and the Brain’s Resting State Networks: From Altered Spatiotemporal Synchronization to Psychopathological Symptoms. Adv Exp Med Biol, 1191, 71–90. doi: 10.1007/978-981-32-9705-0_5 [DOI] [PubMed] [Google Scholar]
- Pan F, Xu Y, Zhou W, Chen J, Wei N, Lu S, . . . Huang M (2020). Disrupted intrinsic functional connectivity of the cognitive control network underlies disease severity and executive dysfunction in first-episode, treatment-naive adolescent depression. J Affect Disord, 264, 455–463. doi: 10.1016/j.jad.2019.11.076 [DOI] [PubMed] [Google Scholar]
- Prater KE, Hosanagar A, Klumpp H, Angstadt M, & Phan KL (2013). Aberrant amygdala-frontal cortex connectivity during perception of fearful faces and at rest in generalized social anxiety disorder. Depress Anxiety, 30(3), 234–241. doi: 10.1002/da.22014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Qin P, & Northoff G (2011). How is our self related to midline regions and the default-mode network? Neuroimage, 57(3), 1221–1233. doi: 10.1016/j.neuroimage.2011.05.028 [DOI] [PubMed] [Google Scholar]
- Schneier FR (2011). Pharmacotherapy of social anxiety disorder. Expert Opin Pharmacother, 12(4), 615–625. doi: 10.1517/14656566.2011.534983 [DOI] [PubMed] [Google Scholar]
- Schneier FR, Heckelman LR, Garfinkel R, Campeas R, Fallon BA, Gitow A, . . . Liebowitz MR (1994). Functional impairment in social phobia. J Clin Psychiatry, 55(8), 322–331. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/8071299 [PubMed] [Google Scholar]
- Shamai-Leshem D, Lazarov A, Pine DS, & Bar-Haim Y (2021). A randomized controlled trial of gaze-contingent music reward therapy for major depressive disorder. Depress Anxiety, 38(2), 134–145. doi: 10.1002/da.23089 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shirer WR, Ryali S, Rykhlevskaia E, Menon V, & Greicius MD (2012a). Decoding subject-driven cognitive states with whole-brain connectivity patterns. Cereb Cortex, 22(1), 158–165. doi: 10.1093/cercor/bhr099 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shirer WR, Ryali S, Rykhlevskaia E, Menon V, & Greicius MD (2012b). Decoding subject-driven cognitive states with whole-brain connectivity patterns. Cereb Cortex, 22(1), 158–165. doi: 10.1093/cercor/bhr099 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Springer KS, Levy HC, & Tolin DF (2018). Remission in CBT for adult anxiety disorders: A meta-analysis. Clin Psychol Rev, 61, 1–8. doi: 10.1016/j.cpr.2018.03.002 [DOI] [PubMed] [Google Scholar]
- Straube T, Schmidt S, Weiss T, Mentzel HJ, & Miltner WH (2009). Dynamic activation of the anterior cingulate cortex during anticipatory anxiety. Neuroimage, 44(3), 975–981. doi: 10.1016/j.neuroimage.2008.10.022 [DOI] [PubMed] [Google Scholar]
- Sylvester CM, Corbetta M, Raichle ME, Rodebaugh TL, Schlaggar BL, Sheline YI, . . . Lenze EJ (2012). Functional network dysfunction in anxiety and anxiety disorders. Trends Neurosci, 35(9), 527–535. doi: 10.1016/j.tins.2012.04.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ward AM, Schultz AP, Huijbers W, Van Dijk KR, Hedden T, & Sperling RA (2014). The parahippocampal gyrus links the default-mode cortical network with the medial temporal lobe memory system. Hum Brain Mapp, 35(3), 1061–1073. doi: 10.1002/hbm.22234 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whitfield-Gabrieli S, Ghosh SS, Nieto-Castanon A, Saygin Z, Doehrmann O, Chai XJ, . . . Gabrieli JD (2016). Brain connectomics predict response to treatment in social anxiety disorder. Mol Psychiatry, 21(5), 680–685. doi: 10.1038/mp.2015.109 [DOI] [PubMed] [Google Scholar]
- Whitfield-Gabrieli S, & Nieto-Castanon A (2012). Conn: a functional connectivity toolbox for correlated and anticorrelated brain networks. Brain Connect, 2(3), 125–141. doi: 10.1089/brain.2012.0073 [DOI] [PubMed] [Google Scholar]
- Xu J, Van Dam NT, Feng C, Luo Y, Ai H, Gu R, & Xu P (2019). Anxious brain networks: A coordinate-based activation likelihood estimation meta-analysis of resting-state functional connectivity studies in anxiety. Neurosci Biobehav Rev, 96, 21–30. doi: 10.1016/j.neubiorev.2018.11.005 [DOI] [PubMed] [Google Scholar]
- Yuan M, Zhu H, Qiu C, Meng Y, Zhang Y, Shang J, . . . Lui S (2016). Group cognitive behavioral therapy modulates the resting-state functional connectivity of amygdala-related network in patients with generalized social anxiety disorder. BMC Psychiatry, 16, 198. doi: 10.1186/s12888-016-0904-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhao Q, Swati ZNK, Metmer H, Sang X, & Lu J (2019). Investigating executive control network and default mode network dysfunction in major depressive disorder. Neurosci Lett, 701, 154–161. doi: 10.1016/j.neulet.2019.02.045 [DOI] [PubMed] [Google Scholar]
- Zhou Y, Yu C, Zheng H, Liu Y, Song M, Qin W, . . . Jiang T (2010). Increased neural resources recruitment in the intrinsic organization in major depression. J Affect Disord, 121(3), 220–230. doi: 10.1016/j.jad.2009.05.029 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.